


Introduction
Thought disorder (TD, also called Formal Thought Disorder or FTD) is a clinically significant symptom dimension of many severe mental illnesses (SMI) [Reference Palaniyappan1, Reference Kircher, Bröhl, Meier and Engelen2]. It presents in two broad forms: disorganization (positive TD), characterized by incoherent, illogical, or tangential speech with difficulty maintaining goal-directed discourse; and impoverishment (negative TD), characterized by reduced speech quantity, poverty of content, and slowed verbal output. TD affects both verbal and nonverbal communicative behavior, and is particularly common in people with psychotic disorders (50–70% in some cohorts [Reference Breier and Berg3, Reference Cuesta and Peralta4]) and mood disorders [Reference Kircher, Bröhl, Meier and Engelen2, Reference Palaniyappan and Wang5, Reference Stein, Lemmer, Schmitt, Brosch, Meller and Fischer6]. TD often precedes and predicts episodic psychotic symptoms (e.g., hearing voices, paranoia) [Reference Dominguez, Saka, Lieb, Wittchen and van Os7, Reference Bearden, Wu, Caplan and Cannon8], yet can persist despite treatment and significantly increase the risk of relapse [Reference Sandini, Zöller, Schneider, Tarun, Armando and Nelson9, Reference Häfner, Maurer and der Heiden10]. The presence of TD typically indicates higher illness severity [Reference Oeztuerk, Pigoni, Wenzel, Haas, Popovic and Ruef11, Reference Roche, Creed, MacMahon, Brennan and Clarke12].
TD is a neglected therapeutic target, with no treatment that specifically addresses TD once it is diagnosed. While TD symptoms (especially disorganization) in the early phases of illness may improve with targeted multimodal early intervention [Reference Pelizza, Leuci, Maestri, Quattrone, Azzali and Paulillo13], over the longer term, both negative and positive TD often persists despite the remission of other psychotic symptoms, contributing to long-term functional impairment and poorer clinical outcomes [Reference Brasso, Bellino, Bozzatello, Del Favero, Montemagni and Rocca14–Reference Liddle17]. Evidence suggests that decline in cognitive, vocational, and functional outcomes [Reference Norman, Malla, Cortese, Cheng, Diaz and McIntosh18–Reference Sigaudo, Crivelli, Castagna, Giugiario, Mingrone and Montemagni21] as well as the disrupted sense of self [Reference Sass and Parnas22] that characterizes illnesses such as schizophrenia are predominantly influenced by persistent TD. Reducing the burden of TD could potentially mitigate social exclusion [Reference de Sousa, Sellwood, Eldridge and Bentall23] and improve quality of life [Reference Rocca, Galderisi, Rossi, Bertolino, Rucci and Gibertoni20].
Several promising preliminary findings targeting communication impairments suggest the potential for targeted intervention [Reference Jimeno24–Reference Joyal, Bonneau and Fecteau27]. However, large-scale trials to understand therapeutic targets (i.e., the cognitive and mechanistic processes behind TD) and test potential treatments are lacking. The measurement of TD per se varies considerably in current practice [Reference Palaniyappan, Sreeraj, Venkatasubramanian and Voppel28, Reference Sreeraj, Voppel, Venkatasubramanian and Palaniyappan29], with the resulting operational heterogeneity itself being a barrier to cumulative knowledge about the participation of people with TD. More importantly, lived experience perspectives remain largely absent in TD research; it is this aspect that we focus on in the current work. We argue that TD research is paradoxically hindered by the systematic, often unexamined noninclusion of those most affected by it, resulting in a biased evidence base that perpetuates therapeutic nihilism. Given the prevalence and pervasiveness of TD in SMI, closing this inclusivity gap is key both to understanding its pathophysiology and to improving overall recovery rates in SMI.
Methodology
We employed a qualitative, experienced-informed methodological approach to examine how current research practices shape the inclusion of individuals with SMI, with a particular focus on those experiencing TD. This approach, grounded in collaborative expertise, integrated two distinct knowledge sources: combined professional research experience (from coauthors with backgrounds in psycholinguistics, psychiatry, neuroimaging, cognitive neuroscience, and clinical trials) and lived experience (from coauthors and network members with personal experience of TD and its impact on social and research participation). This enabled a combined epistemic perspective on how assumptions about capacity, willingness, and communication influence recruitment, consent, and study design processes.
We collected evidence through three methods: (1) Reviewing published literature on eligibility, recruitment, and consent practices in SMI research. Searches were conducted in PubMed by combining variations of the terms (“thought disorder” OR “formal thought disorder” OR “disorganisation” OR “impoverished speech”) with (“clinical trial” OR “research participation” OR “informed consent” OR “decisional capacity” OR “recruitment” OR “exclusion criteria”). Reference lists of included papers were hand searched. No date restriction was applied; publications up to December 2025 were considered. (2) Assessing the alignment of identified practices with empirical evidence on decisional capacity, motivation, and communicative variability in TD, and (3) identifying areas for strengthening current practices and formulating recommendations to support inclusion. These recommendations were iteratively refined through structured discussion with individuals with lived experience of TD, within the DISCOURSE in Psychosis Network, and validated against existing consent and capacity enhancement literature. The resulting recommendations reflect this integrated epistemic process rather than a formal systematic review; we use the term “experienced-informed review” to distinguish this approach. We additionally identified areas in which current practices could be strengthened and formulated corresponding recommendations to enhance supported participation.
Results
Exclusion of people with TD from clinical research operates through at least three interlocking mechanisms. First, ethical and regulatory barriers arise from concerns (often assumed rather than assessed) about decisional capacity and vulnerability, and lead to explicit protocol-level exclusion criteria. Second, methodological barriers emerge from design choices that inadvertently disadvantage people with TD, such as requirements for sustained digital engagement or complex language comprehension. Third, logistical and pragmatic barriers reflect clinician workload, unfamiliarity with supported consent procedures, and implicit gatekeeping (constituting what we term assumptive exclusion below). All three drivers interact and frequently reinforce one another.
Individuals with SMI are generally willing to participate in research, often for altruistic reasons [Reference Roberts, Warner and Brody30, Reference Zullino, Conus, Borgeat and Bonsack31]. Nevertheless, many patients likely including those with notable TD – are explicitly excluded from clinical trials [Reference Humphreys32] and many more are never approached. Only one in five “real-world” patients with schizophrenia appear eligible based on explicit exclusion criteria for randomized efficacy [Reference Taipale, Schneider-Thoma, Pinzón-Espinosa, Radua, Efthimiou and Vinkers33] and effectiveness [Reference Lawrence, Bernstein, Perez Coste, Zhao, Wang and Goldberg34] trials. This is worsened by symptom-based exclusion criteria for emerging interventions recruiting community-living patients (e.g., more than minimal disorganization for digital therapeutics [Reference Lakhan, Dorner-Ciossek, Besedina, Dickerson, Hastedt and Isla35, Reference McCall, Hadjistavropoulos and Loutzenhiser36]) that disproportionately affect people with TD. More damagingly, most eligible patients never get invited to participate [Reference Hofer, Hummer, Huber, Kurz, Walch and Fleischhacker37]. For example, although 20% of people with psychosis had ever been approached to consent to contact by clinicians [Reference Patel, Oduola, Callard, Wykes, Broadbent and Stewart38], 65% of those approached agreed to enter a research register; those left out are likely to have a higher burden of TD.
Multiple implicit factors based on subjective clinical impressions shape who gets invited into clinical research. The resulting unacknowledged exclusions constitute “disappearing participants” (e.g., people with cognitive impairment in geriatric research) [Reference Taylor, DeMers, Vig and Borson39]. Compared with the rest of the broader clinical population with psychosis, excluded patients show poorer therapeutic engagement, impaired cognition [Reference Lally, Watkins, Nash, Shetty, Gardner-Sood and Smith40, Reference Kline, Hendel, Friedman-Yakoobian, Mesholam-Gately, Findeisen and Zimmet41], and lower psychosocial functioning [Reference Lally, Watkins, Nash, Shetty, Gardner-Sood and Smith40, Reference Riedel, Strassnig, Müller, Zwack and Möller42, Reference Woods, Ziedonis, Sernyak, Diaz and Rosenheck43]. All of these factors – poor psychosocial functioning [Reference Rocca, Galderisi, Rossi, Bertolino, Rucci and Gibertoni20, Reference Kline, Hendel, Friedman-Yakoobian, Mesholam-Gately, Findeisen and Zimmet41–Reference Evans, Bond, Meyer, Kim, Lysaker and Gibson44], impaired cognition [Reference Skiba, Chinchani, Menon, Lepage, Lavigne and Malla45–Reference Oeztuerk, Pigoni, Antonucci and Koutsouleris49], and poor engagement [Reference McCabe, John, Dooley, Healey, Cushing and Kingdon50] – are more strongly influenced by TD than by other symptoms of psychosis. The most direct evidence for TD-specific gatekeeping comes from Riedel and colleagues who noted that people with TD were seven times more likely to be excluded from trials testing antipsychotic efficacy [Reference Riedel, Strassnig, Müller, Zwack and Möller42] – a ratio not explained by overall illness severity. Lally and colleagues identified “cognitive problems” including incoherent speech were more among people not invited to a lifestyle intervention trial [Reference Lally, Watkins, Nash, Shetty, Gardner-Sood and Smith40].
Beyond interventional trials, the consequences of selective exclusion extend beyond representativeness to compromise both external validity and statistical power. Not approaching people with TD has substantial implications for studies that aim to understand neurobiological mechanisms per se. For example, in the largest and most well-powered study of the neuroanatomy of TD (n = 2008), the median score on the primary TD measure (PANSS P2; scale range 1–7) was 2 (interquartile range: 1–3; patients n = 752), indicating that most patients had no or clinically insignificant TD [Reference Sharkey, Bacon, Peterson, Rootes-Murdy, Salvador and Pomarol-Clotet51]. This low TD score is in keeping with the overall low symptom burden, but highlights the lack of representativeness of people with notable TD even in TD-specific mechanistic studies. The resulting estimates of neural correlates, derived from a range-restricted sample, may not capture the pathophysiological signal most relevant to TD. This attenuates the true effect, inflates required sample sizes to the detriment of further research efforts, and limits generalizability to the population for whom therapeutic targets are most urgently needed.
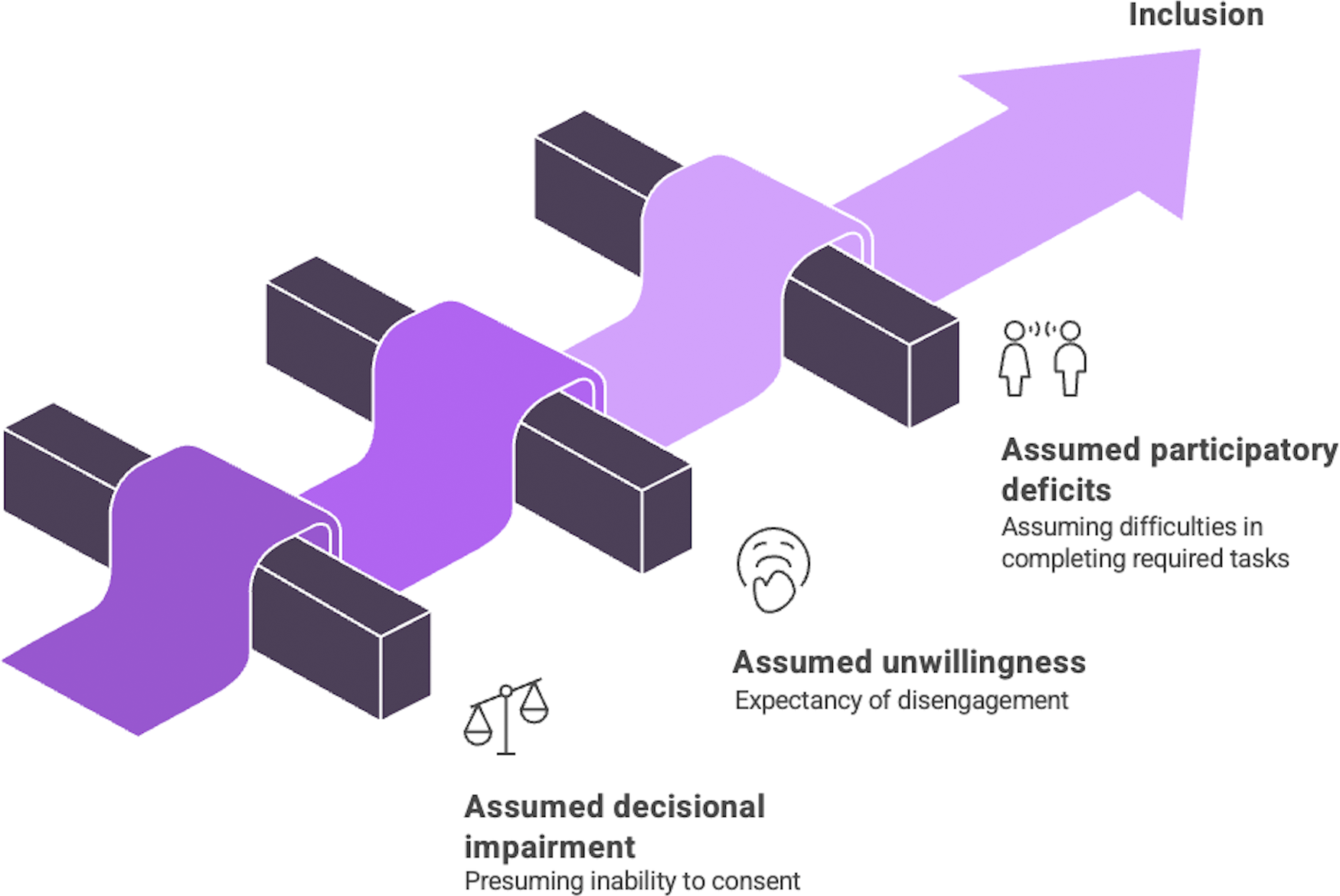
To make clinical research in SMI truly generalizable, we should address the biased practices that lead to the systematic exclusion of people with TD. Based on our professional research experience and lived experience, we find the key barriers are not evidence based but stem from flawed assumptions about capacity, willingness, and communication. We call this phenomenon assumptive exclusion, which creates several major, and often intersecting, barriers to participation that we describe next (Figure 1).
Assumptive exclusion affecting the enrolment of people with thought disorder in clinical research arises from flawed assumptions about capacity, willingness, and abilities. Figure made using napkin.ai.

A supported inclusion package recommended as a basic minimum for studies recruiting people with SMI and thought disorder (TD)
Tier 1 (Essential: applicable to all studies):
-
• Replace diagnosis-based exclusion with function-based assessment.
-
• Use simplified consent materials (e.g., for English, Flesch–Kincaid Grade ≤7 and equivalent readability for other languages; short sentences; no metaphorical/abstract language in information sheets; visual/multimedia aids).
-
• Administer a brief standardized capacity screen (e.g., UBACC) for participants meeting the trigger criteria outlined in Section “Incorporate capacity assessment”.
-
• Train all research personnel in TD-aware communication (minimum: 2-hour session covering assessment and accommodation strategies).
-
• Always include a lived experience consultant in study design and to review materials.
-
• Designate a single study point of contact throughout the study period.
Tier 2 (Enhanced: for studies involving complex/high-risk procedures):
-
• Administer full capacity assessment if capacity is uncertain after Tier 1 screen.
-
• Offer alternative consent formats: pre-recorded video summary; FAQ prompt sheet; advanced consent window.
-
• Document and report accommodations used (to improve the evidence base for supported inclusion).
-
• Allow multiple consent sessions and permit a support person.
Assumptive exclusion
Assumed lack of decision-making capacity
People with SMI, including those with TD, are often excluded from research on the basis of assumed impairments in decision-making capacity (DMC) for research. Patients are frequently perceived to lack capacity, even when they are capable [Reference Muroff, Hoerauf and Kim52]. This perceived actual capacity gap has resulted in unjustified exclusion of people with SMI across various trials [Reference Humphreys32, Reference Humphreys, Blodgett and Roberts53, Reference Harris, Hanson, Leskela, Billig, Padilla-Martinez and Boyd54]. Disorganization (positive TD) is most likely to impede comprehension of consent materials and underpin perceptions of poor communicative competence. Several studies have established that diagnostic labels such as disorganized schizophrenia should not be automatically linked to decisional impairment for research [Reference Spencer, Shields, Gergel, Hotopf and Owen55–Reference Kovnick, Appelbaum, Hoge and Leadbetter60]. Although symptoms such as TD can influence DMC [Reference Spencer, Gergel, Hotopf and Owen56, Reference Howe, Foister, Jenkins, Skene, Copolov and Keks61–Reference Schachter, Kleinman, Prendergast, Remington and Schertzer63], most studies in a systematic review of association between symptoms and research-related decisional impairment reported no or only weak correlations [Reference Spencer, Shields, Gergel, Hotopf and Owen55]. Thus, as with diagnostic labels, no single symptom, including TD, should be taken to indicate impaired research decisional capacity (see also Appelbaum [Reference Appelbaum64] and Dunn [Reference Dunn, Candilis and Roberts65]). In contrast, cognitive impairment, particularly short-term memory deficits [Reference Palmer, Dunn, Appelbaum and Jeste66–Reference Kaup, Dunn, Saks, Jeste and Palmer68], is a stronger predictor of decisional impairment than TD [Reference Spencer, Shields, Gergel, Hotopf and Owen55, Reference Appelbaum64, Reference Kaup, Dunn, Saks, Jeste and Palmer68–Reference Palmer and Jeste72]. Importantly, these memory difficulties are remediable [Reference Kaup, Dunn, Saks, Jeste and Palmer68, Reference Palmer, Savla, Roesch and Jeste69], and once addressed, capacity in patients with schizophrenia can be retained over time [Reference Palmer, Savla, Roesch and Jeste69, Reference Stroup, Appelbaum, Gu, Hays, Swartz and Keefe73]. Decisional impairment for research is best considered “temporal, identifiable, and responsive to interventions” [Reference Calcedo-Barba, Fructuoso, Martinez-Raga, Paz, Sánchez de Carmona and Vicens74].
People with TD are likely to be subjected to compulsory treatments [Reference Georgaca, Machaira, Stamovlasis, Peppou, Papachristou and Arvaniti75] on the basis of poor disease insight [Reference Monteiro, Silva and Louzã76–Reference Subotnik, Ventura, Hellemann, Zito, Agee and Nuechterlein78], higher risk of treatment nonadherence [Reference Ortiz, Higuchi, Noto, Joyce, Correll and Bressan79], and reduced DMC for treatment [Reference Iozzino, Martella, Picchioni, Wancata, Appelbaum and Mandarelli80]. Clinicians and researchers are often unwilling to approach the compulsorily treated people for research studies on the assumption of absent research DMC [Reference APPELBAUM81, Reference Josiassen, Xavier, Dietterich, Harner, Filmyer and Houpt82]. Such heuristics are problematic as the cognitive and functional demands of consenting to research may differ from those required for treatment decisions. In particular, studies have shown that a greater proportion of acute and severely unwell patients with schizophrenia retain research DMC, even when they lack treatment DMC (51% vs. 31% in a head-to-head comparison [Reference Spencer, Gergel, Hotopf and Owen56]). A critical difference between the two concepts is the role of disease insight. Unlike the decision to accept a proposed treatment, the decision to take part in a research study need not require one’s awareness, acceptance, and in many cases, the attribution of symptoms to an illness label. In empirical studies, insight has emerged as the key determinant of treatment decisions [Reference Spencer, Shields, Gergel, Hotopf and Owen55, Reference Calcedo-Barba, Fructuoso, Martinez-Raga, Paz, Sánchez de Carmona and Vicens74, Reference Marcó-García, Ariyo, Owen and David83, Reference Owen, David, Richardson, Szmukler, Hayward and Hotopf84], but does not play a prominent role in research decisions [Reference Spencer, Shields, Gergel, Hotopf and Owen55, Reference Spencer, Gergel, Hotopf and Owen56]. In contrast, the ability to retain novel study-related information over a period of time is more critical for research-related decisional impairment [Reference Spencer, Gergel, Hotopf and Owen56]. Thus, blanket presumption of impaired research capacity due to involuntary treatment status is not supported by extant literature.
Assumed unwillingness to participate
Clinicians often perceive people with TD to have poor therapeutic engagement [Reference Lysaker, Davis, Buck, Outcalt and Ringer85, Reference Cavelti, Homan and Vauth86]; people with TD are often excluded from therapies where such engagement is a key ingredient (e.g., cognitive behavioral therapy [Reference Palmier-Claus, Griffiths, Murphy, Parker, Longden and Bowe87], group metacognitive training [Reference Moritz, Woodward and Balzan88]) even if these are likely to benefit TD [Reference Fekete, Vass, Balajthy, Tana, Nagy and Oláh89, Reference Shryane, Drake, Morrison and Palmier-Claus90]. People with impoverished speech (negative TD) are more likely to limit expressive participation, creating the misleading impression of unwillingness. These assumptions, part of “first impressions” [Reference Fauviaux, Parisi, Marin, Vattier, Lozano-Goupil and Mrabet91], may deter clinicians from recruitment efforts. When approached, people with SMI agree to take part in research studies in comparable numbers to other patient groups [Reference Patel, Oduola, Callard, Wykes, Broadbent and Stewart38, Reference Robotham, Waterman, Oduola, Papoulias, Craig and Wykes92–Reference Edlinger, Deisenhammer, Fiala, Hofer, Kemmler and Strauss95], due to altruism and an expectancy of psychosocial benefits [Reference Roberts, Warner and Brody30, Reference Zullino, Conus, Borgeat and Bonsack31, Reference Kaminsky, Roberts and Brody96, Reference Roberts, Warner, Hammond and Hoop97]. Illness severity shows no associations with perceived benefits [Reference Dunn, Palmer, Keehan, Jeste and Appelbaum98] and only modest associations with perceived harms [Reference Roberts, Warner, Hammond and Hoop97]. Candillis and colleagues noted that people with schizophrenia unwilling to participate in a hypothetical drug trial had comparable severity of TD to a group that was willing to take part [Reference Candilis, Geppert, Fletcher, Lidz and Appelbaum99], refuting the assumption that TD signals unwillingness. Wu and colleagues observed more TD burden among patients with a higher willingness to participate in a hypothetical treatment study, likely due to the higher relevance of the benefits of the proposed treatment (a hypothetical agent for memory enhancement) [Reference Wu, Liao, Chen and Lan100]. Unlike research decisional impairment, willingness to participate does not vary with cognitive functioning [Reference Wu, Liao, Chen and Lan100, Reference Dunn, Kim, Fellows and Palmer101]; instead, it depends on the patient’s perceived risks of participation [Reference Roberts, Warner and Brody30, Reference Dunn, Kim, Fellows and Palmer101–Reference Roberts, Warner, Brody, Roberts, Lauriello and Lyketsos103] and the presence of research safeguards [Reference Kim, Ryan, Tsungmey, Kasun, Roberts and Dunn104–Reference Roberts, Warner, Anderson, Smithpeter and Rogers106]. The assumption that people with TD may be unwilling for research has no empirical support.
Assumed lack of participatory ability
People with TD, owing to their speech and language disturbances (both positive and negative TD), may have low participation in life situations in which knowledge, ideas, or feelings are exchanged [Reference Eadie, Yorkston, Klasner, Dudgeon, Deitz and Baylor107, Reference Langdon, Coltheart, Ward and Catts108]. Because participation is central to research endeavors, recruiters may implicitly exclude such individuals. However, the relationship between TD and communicative participation is not fixed. Patients with TD who have participated in linguistic research describe the experience as validating and meaningful, irrespective of TD severity [Reference Delgaram-Nejad, Archer, Chatzidamianos, Robinson and Bartha109]. Many aspects of language comprehension, alignment, and communicative functioning are relatively preserved in TD (109–113) [Reference Çokal, Zimmerer, Varley, Watson and Hinzen110–Reference Sharpe, Schoot, Lewandowski, Öngür, Türközer and Hasoğlu114]. While complex language (e.g., figurative language [Reference Bambini, Arcara, Bosinelli, Buonocore, Bechi and Cavallaro115] and grammatically complex sentences [Reference Elleuch, Chen, Luo and Palaniyappan116]) poses difficulties for some patients, core comprehension remains intact for many. Furthermore, impaired syntactic comprehension shows high variability, with many people demonstrating strong receptive language skills despite disorganized or reduced speech. TD can also fluctuate; communicative impairments vary over time, influenced by emotional states [Reference Docherty, Evans, Sledge, Seibyl and Krystal117], and by relapsing/remitting phases of illness [Reference Häfner, Maurer and der Heiden10, Reference Zaher, Diallo, Achim, Joober, Roy and Demers118, Reference de Winter, Vermeulen, Couwenbergh, van Weeghel, Hasson-Ohayon and Mulder119]. This episodic course distinguishes TD from major neurocognitive disorders or aphasia and creates opportunities to mitigate communication challenges, as we discuss later.
In summary, the practice of assumptive exclusion explains the substantially reduced inclusivity of people with TD in clinical research. These assumptions, combined with workloads [Reference Rønne, Arnfred, Gæde, Cleal and Jørgensen120] and resource constraints [Reference Jones and Cipriani121], result in substantial discretion in patient selection, turning recruitment of people with TD into a street-level bureaucracy [Reference Lipsky122]. To address this, we propose moving from a deficit-based model that excludes, to a support-oriented framework that adapts, includes, and finally represents this critical population. The accommodations described next are designed to address barriers arising from either dimension of TD, recognizing that they often coexist in the same individual and that the relative burden may fluctuate over time. Where these dimensions differ in their implications for specific recommendations, this is noted.
Discussion
Our framework to improve the inclusion of people with TD as participants in research studies on SMI is centered on explicit capacity assessment (addressing 4.1), enhanced consenting and information exchange (addressing 4.2), targeted training/education (addressing 4.3), and reflexive institutional practices (a systemic solution).
Incorporate capacity assessment
A number of empirical studies have explored the means by which decisional capacity for research can be assessed [Reference Gillies, Duthie, Cotton and Campbell123, Reference Dunn, Nowrangi, Palmer, Jeste and Saks124] and enhanced [Reference Appelbaum64, Reference Dunn, Candilis and Roberts65, Reference Carpenter, Gold, Lahti, Queern, Conley and Bartko70, Reference Flory and Emanuel125, Reference Harmell, Palmer and Jeste126] for people with SMI who are likely to have TD. To avoid the considerable variations in inferring decisional impairment based on professional intuition [Reference Kim, Caine, Swan and Appelbaum127–Reference Di Fazio, Morena, Piras, Piras, Banaj and Delogu129], a brief, study-specific assessment should be incorporated in the informed consent process [Reference Weissinger and Ulrich130] (for a detailed review of various instruments, see [Reference Dunn, Nowrangi, Palmer, Jeste and Saks124]). One notable resource is the UCSD Brief Assessment of Capacity to Consent (UBACC [Reference Jeste, Palmer, Appelbaum, Golshan, Glorioso and Dunn131]), a brief (5–10 min), well-validated tool that covers both understanding and appreciation aspects of decision making [Reference Hamilton, Phelan, Chin, Wyman, Lambrou and Cobb132]). Importantly, assessors (e.g., research assistants) must be trained in administering the brief tools [Reference Dunn133]. To reduce assessment burden, the short research capacity assessment could be reserved for situations where decisional impairment for research is suspected rather than presuming incapacity based on diagnosis.
To operationalize “suspected decisional impairment for research” without reproducing subjectivity, we propose one of the following conditions to be met in order to trigger a study-specific capacity assessment: (1) the participant is currently subject to involuntary psychiatric treatment; (2) the participant is unable to comprehend some of the instructions in the most recent clinical encounter; or (3) the participant has been assessed to have decisional impairment for an unrelated task (e.g., financial decisions). Importantly, none of these triggers constitutes grounds for automatic exclusion; they are grounds for structured assessment. Routinely practicing this for all studies involving people with TD could explicitly remind clinicians of the sliding scale notion of capacity [Reference Appelbaum and Grisso134], that is, decisional capacity is not a fixed trait but varies with the nature and complexity of the proposed procedures.
Enhanced consenting and information exchange
The “understanding” component of research decisional capacity is the most affected element in TD (especially in positive TD), and lack of retention of information is seen as the key cognitive problem behind this failure [Reference Spencer, Gergel, Hotopf and Owen56]. The use of enhancements, that is, aids to simplify (e.g., multimedia cues [Reference Jeste, Palmer, Golshan, Eyler, Dunn and Meeks135], improving comprehension [Reference Dunn, Lindamer, Palmer, Schneiderman and Jeste136]) and reinforce the key procedural information (e.g., via repetition [Reference Palmer and Jeste72, Reference Palmer, Cassidy, Dunn, Spira and Sheikh137], iterative feedback [Reference Stiles, Poythress, Hall, Falkenbach and Williams138]) has been shown to be of benefit (also see [Reference Dunn, Candilis and Roberts65, Reference DuBois, Bante and Hadley139, Reference Dunn and Jeste140] for a review). Shorter and more readable consent forms with simple illustrations that are easy to read, providing information using short and grammatically simple sentences, avoiding ambiguities and metaphorical expressions, and enabling the use of participants’ dominant language [Reference Hodgins, Mouslih, Rukh-E-Qamar and Titone141] are essential general principles to overcome TD-related syntactic and pragmatic comprehension issues (see Supplementary Appendix 1 for an example). Reading ease of most consent forms appears to be poor [Reference Mathew142]; intentional “easing” of the text materials used in clinical research (e.g., using participant feedback, lived experience experts’ input [143], and employing readability indices [Reference Flesch144]) is required to achieve this goal. Options such as advanced consent when TD burden is low, consent to contact at the time of program entry, or proxy consenting [Reference Kim, Karlawish, Kim, Wall, Bozoki and Appelbaum145] (including the use of subject advocates [Reference Stroup and Appelbaum146]) when TD is high may be an option for certain studies, though this may be feasible only for studies that rely on routinely collected information, rather than those involving active data-giving exercises.
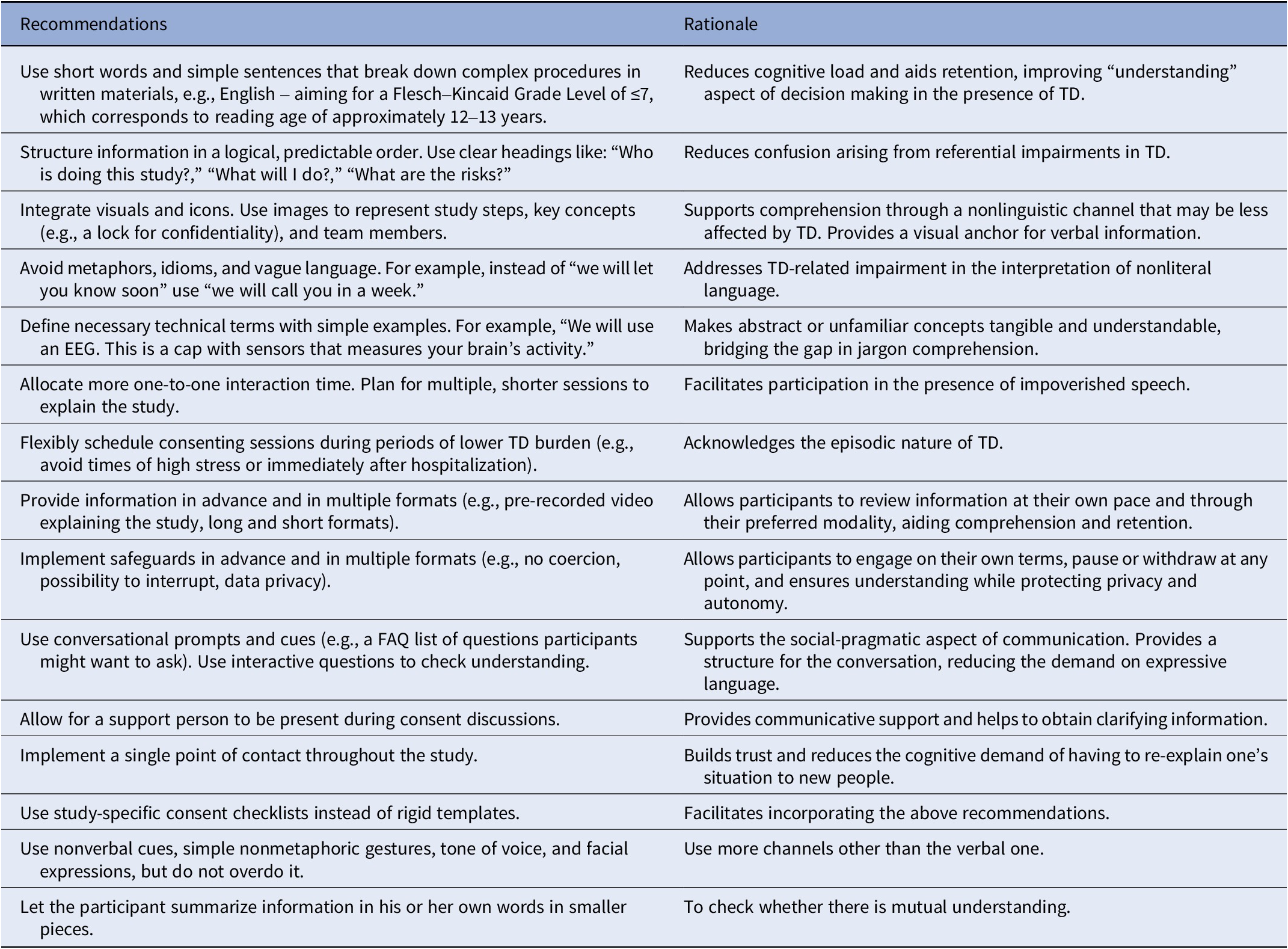
An extensive review of various interventions to enhance research decisional capacity concluded that the key ingredient is the allocation of more one-to-one interaction time [Reference Flory and Emanuel125]. In particular, for patients with TD and impoverished speech (reduced verbal output, often monosyllabic and slow responses that are not elaborate and spontaneous), conversational convergence can be achieved if there is sufficient time for an interaction (see Hodgins and colleagues for further elaboration [Reference Hodgins, O’Driscoll and Titone147]). Providing a set of questions that are expected in a specific context (i.e., prompts or cues) is a technique used as part of social skills training in the presence of TD [Reference Kopelowicz, Liberman and Zarate148–Reference Wong and Woolsey151]; this approach of “frequently asked questions” can be used for consenting procedures to increase engagement (Supplementary Material S1). Such communication accommodations are important because informed consent is not a yes or no response; it is a process rather than a document (note similar considerations in aphasia [Reference Penn, Frankel, Watermeyer and Müller152, Reference Stein and Brady Wagner153] and autism research). Providing pre-recorded information about key procedures in simple language that can be accessed at participants’ own pace (e.g., see Supplementary Material S2 – video link) also increases the contextual information that facilitates exchanges in the presence of impoverished speech [Reference Jimeno24]. Study teams should be able to offer more than one session for explaining research procedures, allow for accompanying persons if required, and be flexible to schedule them during periods when participants are less affected by TD (e.g., not immediately after hospitalization). These accommodations need to be clearly communicated to those who make the first contact for recruitment. A more detailed list of these approaches, adapted from the recommendations made by Working to increase Inclusivity in Research Ethics [Reference Beck, MacKenziem, Kirby, McDonald, Moura and Breitenfeldt154] can be found in Table 1.
Recommendations for enhanced consenting in studies focused on TD

Targeted training
Investing in training research staff on capacity assessment, open engagement, and visibility in clinical spaces has significantly improved consent procedures and successfully recruited a conventionally excluded sample of continuously hospitalized patients with SMI for a genetic study [Reference Josiassen, Xavier, Dietterich, Harner, Filmyer and Houpt82]. In addition, to directly counter the assumptive exclusion, targeted sessions can be planned for both frontline clinicians and research teams throughout the study period. Clinicians often rely on subjective impressions of TD due to limited linguistic training and time constraints, leading to inconsistent assessments of communicative ability.
Integrating structured TD assessment tools and training, co-developed with lived experience experts, must move beyond deficit focus to practical, evidence-based skills to foster engagement in the presence of TD (see [Reference McCabe, John, Dooley, Healey, Cushing and Kingdon50, Reference Pilnick, Trusson, Beeke, O’Brien, Goldberg and Harwood155] for example).
Institutional accommodations
Institutional Review/Ethics Boards often mandate that patients with SMI be recruited for research through initial contact by their treating clinicians. This approach is common across jurisdictions, with physicians making the first approach at many institutions [Reference Zullino, Conus, Borgeat and Bonsack31, Reference Roberts, Warner, Brody, Roberts, Lauriello and Lyketsos103, Reference Golay, Baumann, Jenni, Do and Conus156]. Some study designs rely on treating clinicians to assess eligibility [Reference Howard, de Salis, Tomlin, Thornicroft and Donovan157] or to identify participants across the spectrum of TD [Reference Yoon, Mayer, Berro, Brazis and Kantrowitz158, Reference Deckler, Ferland, Brazis, Mayer, Carlson and Kantrowitz159]. For such studies, collecting data as a by-product of routine healthcare visits, having a single point of contact throughout the study period, and sending text message reminders regarding research interviews may facilitate the participation of people with TD.
Relying on clinicians alone to identify participants with TD introduces two types of selection bias. First, TD is often an “invisible” problem as patients do not complain about being “thought disordered.” Subtle TD often goes undetected during brief clinical interactions, affecting studies that focus on people with TD identified via clinical referrals. On the other hand, as discussed earlier, assumptive exclusion precludes the more severely affected individuals from being referred. Reducing reliance on clinical referrals can potentially reduce selection bias [Reference Howard, de Salis, Tomlin, Thornicroft and Donovan157, Reference Tranberg, Due, Rozing, Jønsson, Kousgaard and Møller160] that arises from the conflation of therapeutic engagement and factors related to therapeutic uncertainty [Reference Jones and Cipriani121] with research participation willingness [Reference Howard, de Salis, Tomlin, Thornicroft and Donovan157] and ensure samples that are more representative of the full spectrum of TD. Institutional support for preconsent screening (see [Reference Callard, Broadbent, Denis, Hotopf, Soncul and Wykes161] for example) can remove this barrier, especially in the presence of electronic health record infrastructure and consent to contact procedures [Reference Patel, Oduola, Callard, Wykes, Broadbent and Stewart38, Reference Robotham, Waterman, Oduola, Papoulias, Craig and Wykes92]. Another approach is the use of “third-sector referrals,” for example, employment centers, community organizations, support groups, advocacy groups (e.g., see Bosco and colleagues [Reference Bosco, Gabbatore, Gastaldo and Sacco162]), and through past research participants (e.g., see Yoon and colleagues [Reference Yoon, Mayer, Berro, Brazis and Kantrowitz158]).
Researchers anticipating ethics board concerns about including participants with TD should address the following explicitly in their protocols: (1) specify the capacity assessment instrument and triggers (as in Section “Incorporate capacity assessment”), demonstrating that inclusion is based on assessed rather than assumed capacity; (2) describe the consent accommodations planned (simplified materials, multiple sessions, supported consenting options) with reference to published evidence for their efficacy; (3) include a monitoring plan that is proportionate to the study risk and adapted for participants with TD (e.g., structured check-in calls using a single named contact rather than complex questionnaires); and (4) build the research governance team with lived experience advisors. At the institutional level, common barriers to implementing these approaches include variability in IRB/REC familiarity with supported consent procedures, limited staff time, and absence of reimbursement for additional consent sessions. We recommend that funders and institutions treat enhanced consent procedures as legitimate cost items in grant budgets, and that research ethics frameworks clarify that the use of supported consent is the preferred practice when recruiting people with SMI.
The missing voices
An important lacuna in SMI research, in general, and TD research, in particular, is the missing voice of people with lived experience of TD in research studies. Despite the growing integration of lived experience expertise in mental health research elsewhere (e.g., see [Reference Jones, Atterbury, Byrne, Carras, Brown and Phalen163, Reference Molloy, Kilcoyne, Belcher and Wykes164]), most studies on TD do not involve people with lived experience of TD or loved ones/family members as research partners. Of 231 primary studies included in 7 systematic reviews focused on TD (1 on cognitive features [Reference Bora, Yalincetin, Akdede and Alptekin165], 2 on linguistic features [Reference Elleuch, Chen, Luo and Palaniyappan166], 2 on brain imaging [Reference Cavelti, Kircher, Nagels, Strik and Homan167, Reference Sumner, Bell and Rossell168], and 2 on communication interventions [Reference Jimeno24, Reference Joyal, Bonneau and Fecteau27]), none reported active and explicit involvement of Lived Experience expertise in the design, implementation, and dissemination of research. Thus, at a time where coproduction of randomized trials is taking off at a rapid pace elsewhere [Reference Molloy, Kilcoyne, Belcher and Wykes164, Reference Goldsmith, Morshead, McWilliam, Forbes, Ussher and Simpson169], and the concept of “nothing about us without us” [Reference Charlton170] changing public perceptions about conditions such as autism [Reference Hoekstra, Girma, Tekola and Yenus171], a seat at the tables where research is planned and produced remains aspirational for people with lived experience of TD (see Supplementary Material S3).
Coproducing SMI research with people having lived experience of TD requires infrastructure that fosters outreach beyond the conventional “clinic-based” models of psychiatric research [Reference Jones, Callejas, Brown, Carras, Croft and Pagdon172]. This can lead to the selection of meaningful outcomes, especially for clinical trials, reduce assessment burden (e.g., using self-report instruments, recorded spontaneous narratives), enhance the consent process, reinforce relational power, and educate researchers and clinical teams about willingness to participate in research. The key ingredients for collaboration in this regard include the establishment of long-term local coproduction partnerships and platforms fostering experiential science. The experientially driven cowritten recommendations presented earlier emerged from one such collaboration fostered by the DISCOURSE in Psychosis network.
Meaningful partnership with people with lived experience of TD (PLE) should be embedded across the full research cycle, not treated as an after-thought or add-on. At the stage of priority setting, PLE can contribute to developing research questions that meaningfully address TD, ensuring that studies address burdens that matter to those most affected. During materials development, PLE input is directly linked to the consent tools described in this article: PLE can assess whether consent forms achieve the readability and clarity targets (Table 1) and codevelop the FAQ prompt sheets and video summaries described in Section “Enhanced consenting and information exchange”. At the recruitment stage, PLE can enhance outreach to ensure representative samples and engage with peer support groups or advocacy organizations – thus widening access beyond clinical referral pathways. In outcome selection, coproduction ensures that primary outcomes include measures of communicative participation and quality of life that are meaningful from a PLE perspective, and not only symptom assessments. Finally, at dissemination, PLE can help translate findings into accessible formats for patient communities, close the feedback loop, and advocate for the policy changes needed to sustain supported inclusion practices. These contributions require adequate resourcing: PLE should be remunerated fairly and supported with training and preparation time.
Counterarguments
We acknowledge that there are contexts in which the non-inclusion of people with TD may be scientifically justified or ethically required. Where a trial outcome depends on a task that is incompatible with severe disorganization (e.g., paradigms requiring reliably organized verbal and nonverbal behavior), or where safety monitoring mandates real-time verbal communication that cannot be adequately supported in the presence of notable communicative impairment, exclusion may be appropriate. It will be appropriate for institutions and ethics committees to expect sound reasoning for this exclusion, and a consideration of alternatives that facilitate inclusion. The supported inclusion framework advocated here does not argue for inclusion at any cost; it argues that the current default of “exclusion without systematic assessment” should be reversed in favor of “inclusion with appropriate support,” and that the burden of justification should lie with exclusion, not inclusion.
Conclusion
In conclusion, the systematic noninclusion of people with thought disorder from research is not a neutral oversight but an active barrier to scientific progress and therapeutic innovation. Not including their voices means missing out on unique experiential expertise and leads to less representative studies. To dismantle this barrier, we must move beyond flawed assumptions and replace assumptive exclusion with a framework of supported inclusion. By embracing enhanced consent procedures, reflexive institutional practices, and most critically, the leadership of those with lived experience, we can generate a more valid and equitable evidence base. But without the support of funders and institutions acknowledging the need for extra resources and flexibility, the proposed supported inclusion framework risks becoming another mandate that places moral responsibility on individual actors without dismantling the systemic disincentives that make assumptive exclusion the easier option. Ultimately, the path to understanding and effectively treating thought disorder is paved not by excluding those it affects, but by intentionally and respectfully including them.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2026.12211.
Data availability statement
No new data were generated or analyzed in this study. Data sharing is therefore not applicable to this article.
Acknowledgments
The authors acknowledge the contributions of the DIALOG project collaborators and thank them for their scientific discussions and support.
Author contribution
LP contributed to conceptualization, supervision, writing – original draft, visualization, reviewing, and editing. SB, VB, MB, ODN, HG, RG, VH, NH, RJ, GK, TK, CMK, SR, KDS, IES, SXT, DT, AV, TW, and IZ contributed to concept development, reviewing, and editing. EBL contributed to visualization, reviewing, and editing.
Financial support
This work was supported by the Wellcome Trust (grant number 314138/Z/24/Z) as part of the DIALOG project.
Competing interests
LP reports support from the Fonds de Recherche du Québec–Santé and the Monique Bourgeois Foundation, an investigator-initiated grant from Otsuka Canada, royalties from the SPMM Course and Oxford University Press, speaker fees from Janssen Canada and Otsuka Canada, and an editorial stipend from CMA Journals, and serves on the editorial board of the Journal of Psychiatry & Neuroscience. AV reports a NARSAD Young Investigator Grant from the Brain & Behavior Research Foundation. GK reports grants from the Sidney R. Baer, Jr. Foundation, the National Institute of Child Health and Human Development, and DARPA/Department of Defense, as well as travel support from Central European University and an unpaid steering committee role with DISCOURSE in Psychosis. SXT reports funding from the Brain and Behavior Research Foundation (grant no. 30975) and the NIH K23 MH130750 award.
TK reports a contract with AbbVie related to proteomics kits.
All other authors declare no conflicts of interest.



 Open access
Open access
Comments
No Comments have been published for this article.