


Introduction
The terms ‘silver splits’ and ‘grey divorce’ have been used in reference to the trend towards increasing rates of union dissolution in middle and later life (Alderotti et al., Reference Alderotti, Tomassini and Vignoli2022; Brown & Lin, Reference Brown and Lin2022). In the United States, the divorce rate among those 50 and older doubled from 1990 through 2010 (Brown & Lin, Reference Brown and Lin2022). Since then and prior to the COVID-19 pandemic, the rate attenuated somewhat among those aged 50–64 while continuing to increase among those aged 65 and older (Brown et al., Reference Brown, Lin and Julian2024; Brown & Lin, Reference Brown and Lin2022). In Canada, divorce rates are generally lower (Statistics Canada, 2022a). Yet, beginning in the 1990s, they also increased among those 50 and older before stabilizing during the latter half of the 2000s (Margolis et al., Reference Margolis, Choi, Hou and Haan2019; Statistics Canada, 2023). As well, the average age of Canadians who were separated or divorced as well as the incidence of re-partnering in later life increased, reflecting not only the declines in divorce among younger adults but also the increases in divorce and in reliance on cohabitation as a viable alternative to remarriage among middle-aged and older adults (Schimmele & Wu, Reference Schimmele and Wu2016). However, despite increases in cohabitation rates, whether cohabiting union dissolution rates of older adults also increased over time is less clear. Although older adult cohabiting unions are noted to be more stable and less likely to dissolve than those of younger adults (Brown & Wright, Reference Brown and Wright2017), those in cohabiting relationships have been found to face a significantly greater risk of union disruption than those who are married (Wu & Penning, Reference Wu and Penning2018).
Union dissolution is widely reported to have negative implications for the physical and mental health of those involved (Canady & Broman, Reference Canady and Broman2003). Whether the reverse is true and health influences union dissolution is less clear. Yet poor or declining physical and mental health may also increase dissolution risk by increasing exposure to stressors (such as job loss, declines in income, increased medical and other costs, and enhanced caregiving responsibilities), all of which can increase conflict and strain and undermine union quality (Brown & Wright, Reference Brown and Wright2017; Canady & Broman, Reference Canady and Broman2003; Karraker & Latham, Reference Karraker and Latham2015; Percheski & Meyer, Reference Percheski and Meyer2018; Teachman, Reference Teachman2010; Wilson & Waddoups, Reference Wilson and Waddoups2002; Wolff & Kasper, Reference Wolff and Kasper2006).
To date, relatively few studies have focused on health as a determinant of union dissolution, particularly in middle and later life (Alderotti et al., Reference Alderotti, Tomassini and Vignoli2022; Kalmijn, Reference Kalmijn2026; Karraker & Latham, Reference Karraker and Latham2015; Latham-Mintus et al., Reference Latham-Mintus, Holcomb and Zervos2022; Lin et al., Reference Lin, Brown, Wright and Hammersmith2018). Further, what research has been conducted has tended to focus on the implications of illness onset, particularly of serious or life-threatening physical illnesses such as cancer or stroke. Some report an increased risk of divorce following diagnosis or disability onset among younger or working age adults (Blekesaune & Barrett, Reference Blekesaune and Barrett2005; Singleton, Reference Singleton2012; Syse & Kravdal, Reference Syse and Kravdal2007; Teachman, Reference Teachman2010). Whether a similar pattern holds for middle-aged and older adults is less clear. Karraker and Latham (Reference Karraker and Latham2015) studied the impact of serious physical illness onset (i.e., cancer, heart problems, lung disease, and stroke) on subsequent union dissolution among initially healthy older married couples aged 50 and older at baseline. They found that the onset of wives’ but not husbands’ illness was associated with subsequent union dissolution. However, drawing on a more representative sample of American adults of the same age (i.e., not just healthy individuals), Lin et al. (Reference Lin, Brown, Wright and Hammersmith2018) found that the onset of these conditions among either partner was not associated with union dissolution. More recently, Alderotti et al. (Reference Alderotti, Tomassini and Vignoli2022) found that poor physical health – assessed using the number of limitations to daily activities – was associated with a lower rather than higher likelihood of union dissolution among adults of the same age in Europe.
Studies of the impact of mental health on union dissolution have also tended to focus on specific disorders. In general, those with anxiety, mood, substance abuse, and other psychiatric disorders are reported to be more likely to experience union dissolution (Breslau et al., Reference Breslau, Miller, Jin, Sampson, Alonso, Andrade, Bromet and Kessler2011; Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2017). This includes evidence indicating that declines in mental health (e.g., onset of depression) are associated with union dissolution in middle and later life. A Finnish study of middle-aged married couples (aged 40–64) without psychiatric morbidity at baseline found that for both women and men, the risk of divorce increased significantly following new incidence of psychiatric morbidity (Metsä-Simola et al., Reference Metsä-Simola, Martikainen and Monden2018). As well, a longitudinal study of adults aged 50 and older in the UK on the development of depressive symptoms before, upon and following divorce found that depressive symptoms increased in the 1–2 years before divorce or separation (Tosi & van den Broek, Reference Tosi and van den Broek2020). Findings of a positive impact of depression on union dissolution among older adults across Europe are reported by Alderotti et al. (Reference Alderotti, Tomassini and Vignoli2022).
Overall, while some studies suggest that physical and mental health may be associated with union dissolution in middle and later life, exactly what it is about health decline that increases the likelihood of union dissolution remains unclear. By focusing primarily on the onset of a limited number and range of illnesses, it becomes difficult to know whether the findings are specific to such conditions and to short-term or immediate rather than longer-term or chronic effects. Yet, despite some evidence suggesting that the onset of specific illnesses may be the most problematic (Mojtabai et al., Reference Mojtabai, Stuart, Hwang, Eaton, Sampson and Kessler2017), other evidence suggests that the impact of overall physical and mental health status and more prolonged or chronic illnesses may be equally or more important. For example, in a longitudinal study of individuals aged 18–59 in Europe, Monden and Uunk (Reference Monden and Uunk2013) report a negative impact of self-assessed health on dissolution risks. Moreover, they noted that ‘this selection effect appears to be associated with being in poor self-assessed health for a prolonged period of time rather than by the immediate effect of a health decline’ (p. 103). More recently, Kalmijn (Reference Kalmijn2026) also reports finding a negative impact of declining self-rated health (SRH) on union dissolution among adults aged 18+ in several countries (including Australia, Germany, South Korea, Russia, Switzerland, the UK), but notes that the effect declines significantly with age. This, in turn, is attributed to the more common and normative nature of health problems in later life and the fact that older couples ‘have invested more in the relationship, reducing the risk of dissolution when problems arise’ (p. 80).
This study represents an important first step to address the implications of self-assessed physical and mental health for union dissolution among middle-aged and older Canadians. More specifically, it responds to the lack of evidence regarding the role of overall physical and mental health on union dissolution in middle and later life as well as the need for greater clarity regarding the implications of shorter-term (onset) versus longer-term (ongoing) health problems in the Canadian context. The following research questions are addressed: (1) Are self-rated physical and mental health associated with union dissolution among middle-aged and older Canadians? and (2) To what extent is it declines in health and to what extent is it ongoing poor health that precedes union dissolution?
Methods
Data source and sample
This study was approved by the University of Victoria’s Research Ethics Board (Approval no. 23-0173). It utilized data from the Longitudinal and International Study of Adults (LISA) conducted by Statistics Canada in partnership with Employment and Social Development Canada (ESDC). The LISA was developed to provide information on the impact of changes in the labour market, education, health, and family experiences on people’s lives in Canada. Computer-Assisted Personal Interview (CAPI) software was used to collect information from approximately 34,000 Canadians aged 15+ from more than 11,000 households. The LISA has a stratified multi-stage, multi-phase design with data collection conducted every 2 years (Statistics Canada, 2022b). The target population included those living in Canada’s 10 provinces, including their future children. Excluded populations include those living on reserves and other Aboriginal settlements, official representatives of foreign countries and their families living in Canada, members of religious and other communal colonies, members of the Canadian Armed Forces stationed outside Canada, inmates in correctional facilities, and chronic care patients living in hospitals and nursing homes or other collective dwellings (Statistics Canada, 2022b). These exclusions represent approximately 2 per cent of the overall population (Statistics Canada, 2022b).
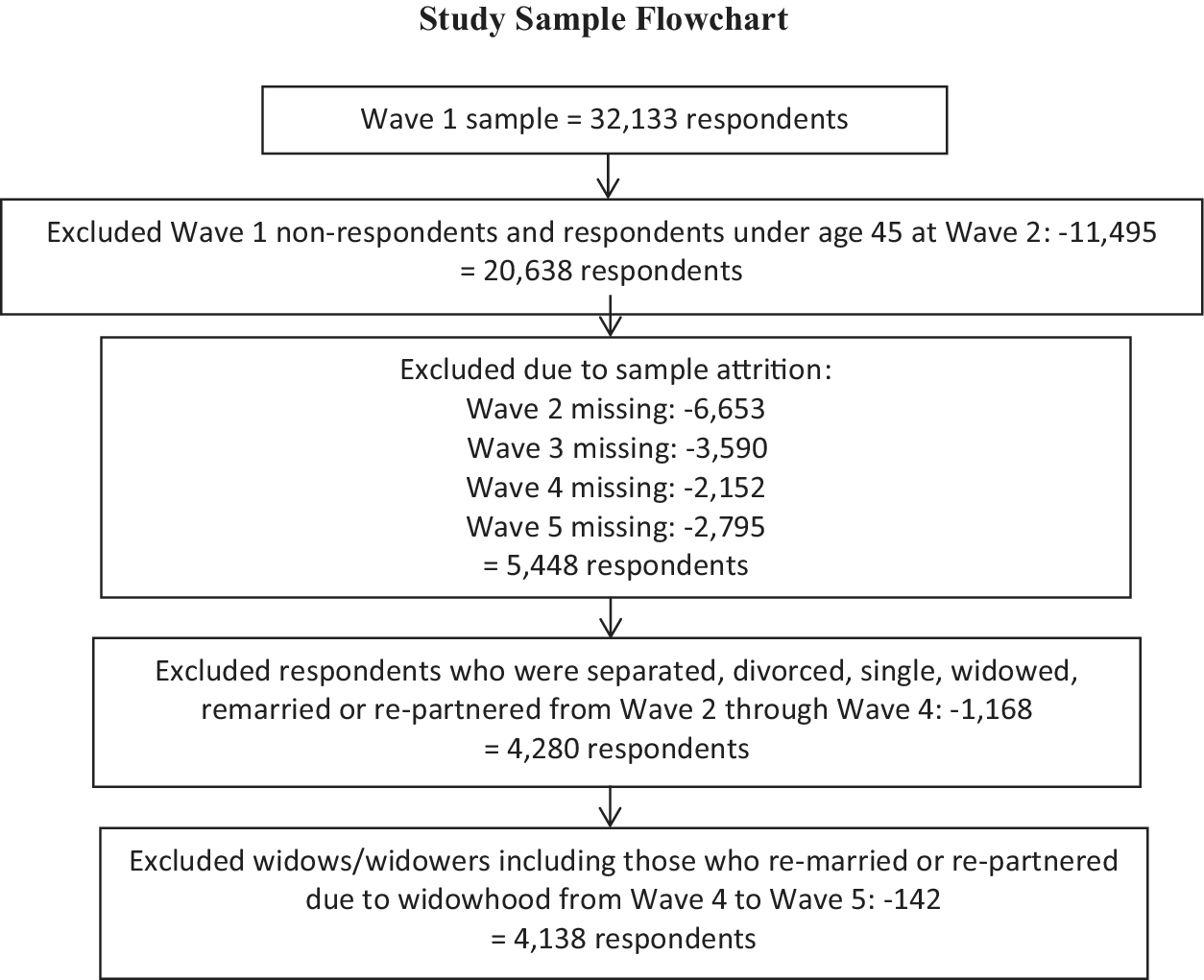
The study utilized the LISA sample of permanent study members (n = 32,133). The sample included respondents aged 45+ who participated in Waves 2 through 5 (W2–W5). W1 responses were excluded due to limitations on the availability of appropriate health-related data. The exclusion of those who did not respond to various waves of the survey generated an initial sample of 5,448 eligible respondents. To ensure a clear temporal ordering between health changes and union dissolution, we further restricted the sample to individuals who remained in the same married or common-law relationship across Wave 2 (W2) and Wave 3 (W3). This design allowed us to measure changes in health status over a two-wave interval while the union was still intact. By measuring health changes while the union was still stable (W2–W3), we were able to more accurately predict the risk of a breakup occurring later (W3–W5), avoiding the confusion of whether a change in health was the cause or the result of a dissolution. Lastly, we excluded those who experienced widowhood in W4–W5. Net of these exclusions (see Figure 1), the analytical sample consisted of 4,138 individuals aged 45+ who were married or living common-law with the same partner at W2 and W3 and whose partner did not die during the period of study.
Study sample flowchart.

Figure 1. Long description
At the top, the initial sample is 32,133 respondents. The first box below excludes Wave 1 non-respondents and those under age 45 at Wave 2, removing 11,495 and leaving 20,638 respondents. The next box excludes due to sample attrition: Wave 2 missing 6,653, Wave 3 missing 3,590, Wave 4 missing 2,152, Wave 5 missing 2,795, leaving 5,448 not excluded. The following box excludes respondents who were separated, divorced, single, widowed, remarried, or re-partnered from Wave 2 through Wave 4, removing 1,168 and leaving 4,280 respondents. The final box excludes widows or widowers, including those who remarried or re-partnered due to widowhood from Wave 4 to Wave 5, removing 142 and resulting in a final sample of 4,138 respondents.
Measures
To assess union dissolution, respondents were asked about their marital status at each wave. Those whose (0) unions (common-law or married) remained intact from W2 through W5 (2014–2020) were compared to (1) those whose unions had ended (i.e., they reported being separated, divorced, or single or as having established a marriage or common-law relationship with someone new in W4 or W5 – 2018–2020). To ensure the internal consistency of our dissolution measure, we performed a manual audit of all respondents reporting a new union start date between W2 and W5. We cross-referenced start dates with partner identifiers and union history to distinguish between (a) those marrying a pre-existing common-law partner, (b) those re-partnering following spousal bereavement, and (c) those re-partnering following a separation or divorce. Individuals in group (b) were excluded from the sample, while only those in group (c) were coded as experiencing union dissolution. This case-by-case verification ensures that our results are not confounded by bereavement-related transitions.
In this study, SRH change from W2 to W3 was assessed by drawing on responses to the question: ‘In general, would you say your health is excellent, very good, good, fair, or poor?’ SRH is widely used and has been found to have high reliability and predictive and concurrent validity as a measure of perceived overall health status (Zajacova & Dowd, Reference Zajacova and Dowd2011). Previous research has been consistent in linking it to various objective measures of physical health (including the onset of chronic conditions) as well as physician assessments of health and mortality (Latham & Peek, Reference Latham and Peek2013; Schnittker & Bacak, Reference Schnittker and Bacak2014). Further, prior evidence suggests that physical functioning tends to be the main driver of SRH, particularly among older adults and those reporting fair or poor SRH (Benyamini et al., Reference Benyamini, Leventhal and Leventhal2003; Monden & Uunk, Reference Monden and Uunk2013). For both waves, responses were dichotomized in a manner consistent with previous studies: (0) fair/poor and (1) good/very good/excellent health (Percheski & Meyer, Reference Percheski and Meyer2018; Zajacova & Dowd, Reference Zajacova and Dowd2011). A three-category independent variable was then created comparing those whose (1) SRH worsened from W2 to W3 and (2) those reporting fair/poor health in both waves to those (0) who reported either good/very good/excellent health in both waves or improved health from W2 to W3 (reference category) with respect to subsequent union dissolution.
Mental health status during W2 and W3 was assessed using the Kessler Psychological Distress Scale (K10, Kessler et al., Reference Kessler, Andrews, Colpe, Hiripi, Mroczek, Normand, Walters and Zaslavsky2002). The scale consists of 10 questions about anxiety and depressive symptoms that a person experienced in the most recent 4-week period. Items are measured on a 5-point scale such that final scores range from 10 to 50. Higher scores indicate higher levels of psychological distress. Reliability coefficients obtained for the scale in the current study were α = 0.81 (W2) and α = 0.83 (W3). Once again, responses were dichotomized, comparing those who reported (0) low or mild distress (a score of 10–24) to those with (1) moderate or high distress (a score of 25–50) (ABS, 2012). For the analyses, those with (1) increased distress from W2 to W3 and those with (2) chronic moderate or high distress in both waves were compared to those who had (0) chronic low or mild distress or decreased distress from W2 to W3 (reference).
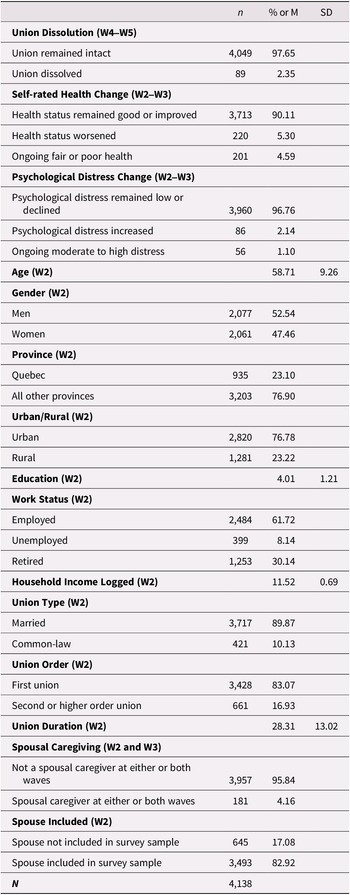
Several demographic, socioeconomic, and union context variables known to be associated with health and union dissolution were included as controls. Demographic indicators included age (coded in years), gender (0 = men, 1 = women), province of residence (0 = non-Quebec, 1 = Quebec), and urban/rural residence (0 = urban, 1 = rural). Previous studies have shown that residence in Quebec is strongly associated with both health and union dissolution in middle and later life. For example, residence in Quebec has been found to be positively associated with self-rated physical and mental health of older adults (Margolis et al., Reference Margolis, Chai, Verdery and Newmyer2022). As well, profound differences have been documented in marital and cohabitation patterns, with residents of Quebec being less likely to be married and more likely to cohabit than those living elsewhere in Canada. As well, previous research, including studies focusing on middle and later life union dissolution, point to greater marital but not cohabiting union dissolution in Quebec than other provinces (Wu & Penning, Reference Wu and Penning2018). Socioeconomic indicators included the highest level of education completed (ranging from 1 = no formal education through 6 = university credential above a bachelor’s degree), work status (0 = employed, 1 = unemployed, 2 = retired), and household income (logged) before taxes (reference year of 2013). Next, union context was assessed based in part on union type (0 = married, 1 = common-law). Union order (0 = first union, 1 = second or higher order union), current union duration (in years) as well as spousal caregiving (0 = non-spousal caregiver or non-caregiver, 1 = spousal caregiver at either or both waves) were also included. Lastly, because the LISA conducted interviews with all members of selected households, a control variable was also included to indicate whether one’s spouse/partner was also in the study sample (0 = not included; 1 = included) to control for the likelihood of correlated responses. Descriptive statistics for all variables used in the analyses are reported in Table 1.
Sample characteristics (n = 4,138)

Table 1. Long description
Beginning at the top, union dissolution from wave 4 to wave 5 shows 4,049 unions remained intact (97.65 percent) and 89 dissolved (2.35 percent). Next, self-rated health change from wave 2 to wave 3: 3,713 reported good or improved health (90.11 percent), 220 worsened (5.30 percent), and 201 had ongoing fair or poor health (4.59 percent). Psychological distress change from wave 2 to wave 3: 3,960 remained low or declined (96.76 percent), 86 increased (2.14 percent), and 56 had ongoing moderate to high distress (1.10 percent). Age at wave 2 shows mean 58.71 years, standard deviation 9.26. Gender at wave 2: 2,077 men (52.54 percent), 2,061 women (47.46 percent). Province at wave 2: 935 Quebec (23.10 percent), 3,203 all other provinces (76.90 percent). Urban/rural at wave 2: 2,820 urban (76.78 percent), 1,281 rural (23.22 percent). Education at wave 2: mean 4.01, standard deviation 1.21. Work status at wave 2: 2,484 employed (61.72 percent), 399 unemployed (8.14 percent), 1,253 retired (30.14 percent). Household income logged at wave 2: mean 11.52, standard deviation 0.69. Union type at wave 2: 3,717 married (89.87 percent), 421 common-law (10.13 percent). Union order at wave 2: 3,428 first union (83.07 percent), 661 second or higher order union (16.93 percent). Union duration at wave 2: mean 28.31 years, standard deviation 13.02. Spousal caregiving at wave 2 and wave 3: 3,957 not a spousal caregiver (95.84 percent), 181 spousal caregiver (4.16 percent). Spouse included at wave 2: 645 not included (17.08 percent), 3,493 included (82.92 percent). At the bottom, total sample size is 4,138.
Note: Weighted percentages (%), means (M), and standard deviations (SD); unweighted Ns.
Source: Longitudinal and International Study of Adults (LISA), W2–W5 (2014–2020).
Data analysis
Two main sets of logistic regression analyses were conducted: (1) a model with SRH status change and (2) a model with psychological distress change as the focal independent variable. Both models adjusted for all control variables. Analyses were conducted using Stata 15 with relevant weight factors (i.e., the LISA wave 5 all-waves longitudinal weight – AWRPW_W5) applied. These weights were designed to ensure the sample was representative of the 2012 Census population living in the 10 provinces (Statistics Canada, 2022b). Due to some evidence of heteroskedasticity, robust standard errors were used (White, Reference White1980). Missingness was minimal with most variables having no missing cases. The variable with the greatest number of missing cases was higher order union (1.2%). Consequently, listwise deletion was used, resulting in 3.3 per cent of all cases being dropped from the analyses.
Results
The vast majority (97.65%) of individuals who were married or in common-law relationships in waves 2 and 3 (2014–2016) remained in these relationships during waves 4 and 5 (2018–2020). The fact that only 2.35 per cent (n = 89) reported that their earlier unions had dissolved during subsequent waves is consistent with evidence suggesting that middle and later life union dissolution remains a relatively rare occurrence. With regard to overall health, almost 10 per cent reported that their SRH either decreased from W2 to W3 (5.30%) or remained poor/fair (4.59%) throughout this period. At the same time, somewhat fewer individuals reported either increased psychological distress (2.14%) or continuing moderate/high levels of psychological distress (1.10%) from W2 to W3.
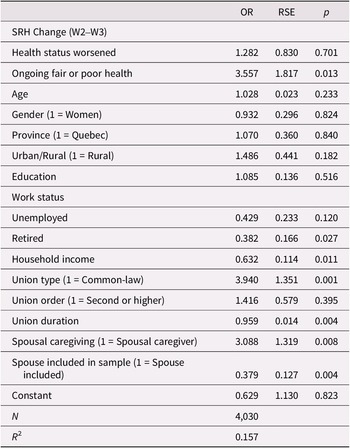
Table 2 reports logistic regression results for analyses of the relationship between changes in SRH and union dissolution. Compared to those experiencing continuing good/very good/excellent health or improved SRH from W2 to W3, those whose SRH declined during this period did not report a greater likelihood of subsequent union dissolution (in W4 or W5). However, those who experienced ongoing fair/poor SRH (in both W2 and W3) had a greater likelihood of union dissolution in W4 or W5 (OR = 3.56; p = .013). With SRH taken into account, none of the demographic variables was significantly related to union dissolution. In terms of socioeconomic variables, education was unrelated whereas respondents who were retired (OR = 0.38; p = .027) and those reporting higher household incomes (OR = 0.63; p = .011) had a lower likelihood of later union dissolution. Union context also assumed importance. Respondents in a common-law relationship were more likely than those in a marital relationship to see their unions subsequently dissolve (OR = 3.94; p = .001). However, union order – whether a first or subsequent union – was unrelated. Additionally, those who were spousal caregivers in either or both waves reported a greater likelihood of subsequent union dissolution than non-caregivers or other types of caregivers (OR = 3.09; p = .008). Conversely, those reporting longer duration unions (OR = 0.96; p = .004) and whose spouse was also surveyed (OR = 0.379; p = .004) were less likely to report experiencing union dissolution during the study period.
Logistic regression of union dissolution (W4–W5) on self-rated health change (W2-W3)
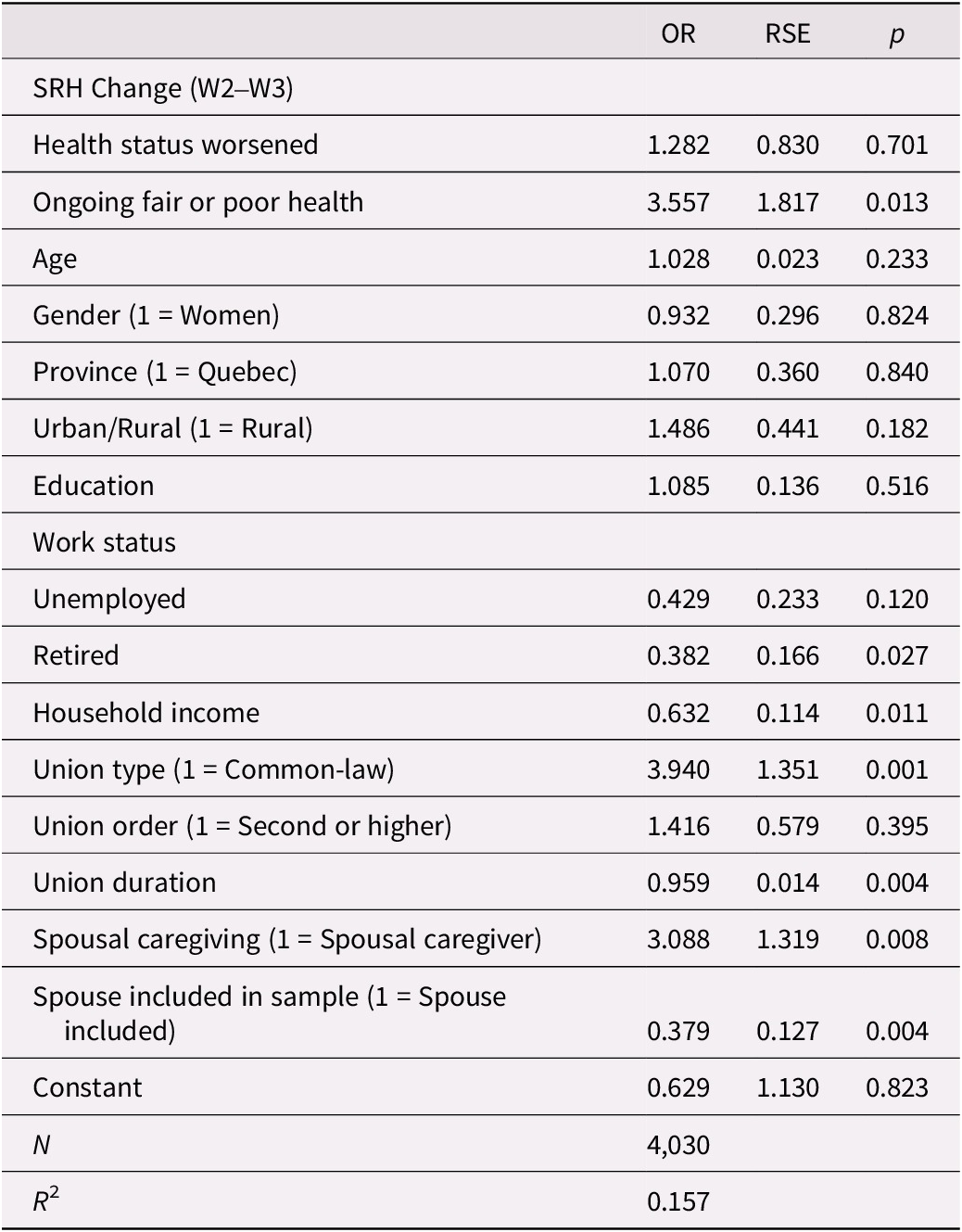
Table 2. Long description
The table presents logistic regression results addressing the impact of self-rated health change from W2 to W3 on union dissolution during W4 and W5, with predictors, odds ratios, robust standard errors and p values listed in each column. The first section covers SRH Change from W2 to W3, with subrows for health status worsened (odds ratio 1.282, robust standard error 0.830, p-value 0.701) and ongoing fair or poor health (odds ratio 3.557, robust standard error 1.817, p-value 0.013). Age is listed with odds ratio 1.028, robust standard error 0.023, p-value 0.233. Gender (1 equals women) shows odds ratio 0.932, robust standard error 0.296, p-value 0.824. Province (1 equals Quebec) has odds ratio 1.070, robust standard error 0.360, p-value 0.840. Urban/Rural (1 equals rural) is odds ratio 1.486, robust standard error 0.441, p-value 0.182. Education is odds ratio 1.085, robust standard error 0.136, p-value 0.516. Work status is followed by unemployed (odds ratio 0.429, robust standard error 0.233, p-value 0.120) and retired (odds ratio 0.382, robust standard error 0.166, p-value 0.027). Household income is odds ratio 0.632, robust standard error 0.114, p-value 0.011. Union type (1 equals common-law) is odds ratio 3.940, robust standard error 1.351, p-value 0.001. Union order (1 equals second or higher) is odds ratio 1.416, robust standard error 0.579, p-value 0.395. Union duration is odds ratio 0.959, robust standard error 0.014, p-value 0.004. Spousal caregiving (1 equals spousal caregiver) is odds ratio 3.088, robust standard error 1.319, p-value 0.008. Spouse included in sample (1 equals spouse included) is odds ratio 0.379, robust standard error 0.127, p-value 0.004. The constant is odds ratio 0.629, robust standard error 1.130, p-value 0.823. At the bottom, N equals 4,030 and R squared equals 0.157. Notes clarify OR as odds ratios and RSE as robust standard errors. Source is the Longitudinal and International Study of Adults, W2 to W5 (2014 to 2020), with AWRPW underscore W5 weight applied.
Note: OR, Odds Ratios; RSE, Robust Standard Errors.
Source: Longitudinal and International Study of Adults (LISA), W2–W5 (2014–2020).
AWRPW_W5 weight applied.
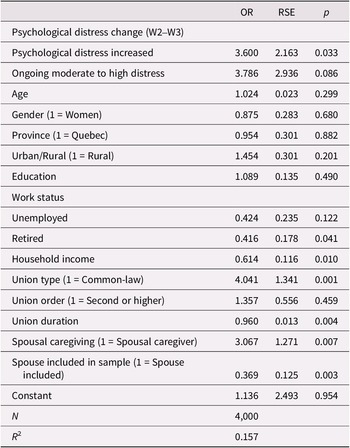
Table 3 reports the results obtained for the relationship between changes in psychological distress and the likelihood of union dissolution. Compared to those with continuing low levels of psychological distress or decreased psychological distress from W2 to W3 (reference category), those reporting increased psychological distress were more likely to experience subsequent union dissolution (OR = 3.60; p = .033). A similar, albeit non-significant, trend was evident among those who experienced comparatively high levels of psychological distress in both W2 and W3 (OR = 3.79; p = .086). In concert with the SRH results, none of the demographic characteristics emerged as significantly related. Once again, however, respondents who were retired (OR = 0.42; p = .041), who reported higher household incomes (OR = 0.61; p = .010), who reported longer duration unions (OR = 0.96; p = .004), and whose spouse also participated in the LISA survey (OR = 0.37; p = .003) had lower odds of experiencing union dissolution. Also, like the SRH results, those in a common-law relationship (OR = 4.04; p = .001) as well as spousal caregivers in either or both W2 and W3 reported a greater likelihood of union dissolution than non-caregivers or other types of caregivers (OR = 3.07; p = .007). With these factors taken into account, whether the union was a first or subsequent union was not significant.
Logistic regression of union dissolution (W4–W5) on psychological distress change (W2-W3)
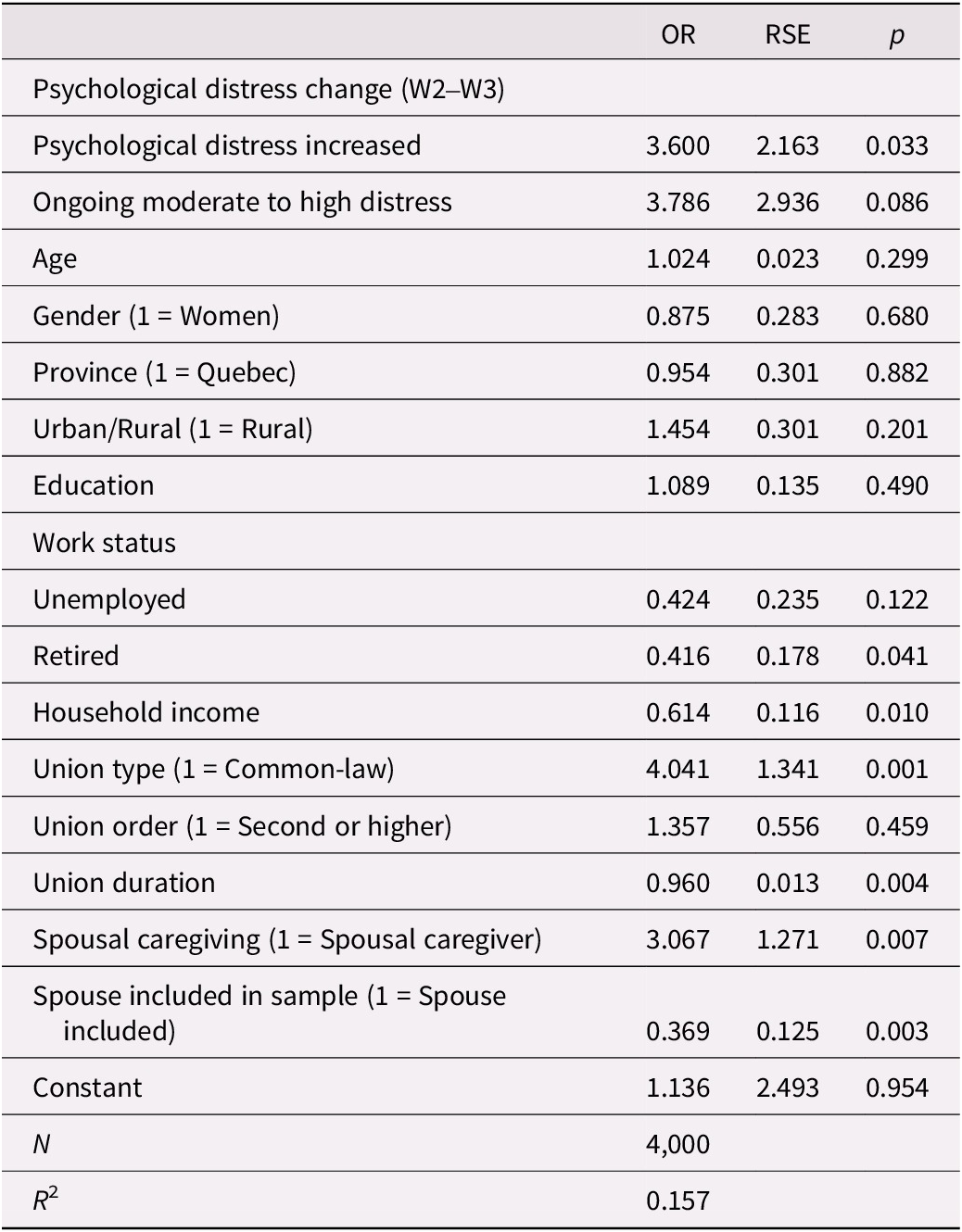
Table 3. Long description
The table presents logistic regression results for for the impact of psychological distress change from W2 to W3 on union dissolution between W4 and W5, with predictors listed in the first column and corresponding odds ratios, robust standard errors, and p values in the next three columns. From top to bottom, the variables are: psychological distress increased (odds ratio 3.600, robust standard error 2.163, p value 0.033), ongoing moderate to high distress (3.786, 2.936, 0.086), age (1.024, 0.023, 0.299), gender coded as 1 equals women (0.875, 0.283, 0.680), province coded as 1 equals Quebec (0.954, 0.301, 0.882), urban or rural coded as 1 equals rural (1.454, 0.301, 0.201), education (1.089, 0.135, 0.490), unemployed (0.424, 0.235, 0.122), retired (0.416, 0.178, 0.041), household income (0.614, 0.116, 0.010), union type coded as 1 equals common-law (4.041, 1.341, 0.001), union order coded as 1 equals second or higher (1.357, 0.556, 0.459), union duration (0.960, 0.013, 0.004), spousal caregiving coded as 1 equals spousal caregiver (3.067, 1.271, 0.007), spouse included in sample coded as 1 equals spouse included (0.369, 0.125, 0.003), and constant (1.136, 2.493, 0.954). The sample size is 4,000 and R squared is 0.157. Odds ratios greater than 1 indicate increased odds of union dissolution, while values less than 1 indicate decreased odds. Statistically significant predictors at p less than 0.05 include psychological distress increased, retired, household income, union type, union duration, spousal caregiving, and spouse included in sample.
Note: OR, Odds Ratios; RSE, Robust Standard Errors.
Source: Longitudinal and International Study of Adults (LISA), W2–W5 (2014–2020).
AWRPW_W5 weight applied.
Discussion and conclusions
Despite numerous studies on the implications of union dissolution for declines in health, there has been relatively little attention paid to the reverse – that is, the implications of changes in health for subsequent union dissolution. This is particularly true in the Canadian context. In addition, what longitudinal studies have been conducted have generated contradictory results. As well, they have focused on the implications of the onset of a limited number and range of specific and often life-threatening conditions and thus, the short-term rather than continuing effects of health decline. Given these research gaps, this study drew on data from several waves of the Canadian LISA to explore the effects of stability and changes in SRH and psychological distress reported during W2 or W3 (2014 to 2016) on marital and cohabiting union dissolution reported during W4 or W5 (2018 to 2020) among middle-aged and older adults.
A key finding of this study was that those whose SRH declined over the two-year period captured during earlier waves of the study did not differ in their risk of subsequent union dissolution from those reporting either improved or continuing good to excellent health during this same period. In contrast, those who reported continuing fair or poor SRH over the two consecutive waves were significantly more likely to see their unions dissolve in two subsequent waves. This lends support to previous research conducted among younger and middle-aged adults suggesting that experiencing poor overall health for a prolonged period may be more detrimental to union stability than the more immediate effect of health decline (Monden & Uunk, Reference Monden and Uunk2013). As noted by these authors, short-term declines in health may well be transitional and thus, may have less adverse impact on some of the risk factors for union dissolution such as economic well-being, intensive caregiving, and interpersonal stress levels. Alternatively, it could be that in the short term, a partner’s illness may also enhance one’s feelings of obligation to provide support and care, thereby limiting union dissolution. At the same time, an individual who is faced with the onset of health problems may consider continued access to support and care as one of the benefits of staying in the union (e.g., Lillard & Panis, Reference Lillard and Panis1996). Thus, the increased risk of union dissolution could be offset by short-term decisions to not pursue or to postpone dissolution to avoid doing so when health problems first emerge. Finally, it could also be the case that while illness onset may increase the short-term likelihood of union dissolution for some, it might reduce the likelihood for others.
Somewhat different findings were obtained when the impact of psychological distress was assessed. In this case, those reporting increased psychological distress early on were more likely to report subsequent union dissolution with a similar, albeit non-significant, trend evident among those who experienced continuing high levels of psychological distress. These findings suggest that when it comes to mental health, problems that are more proximal in time (onset) may be the most likely to undermine union stability. This is generally consistent with findings reported by Metsä-Simola et al. (Reference Metsä-Simola, Martikainen and Monden2018). Their study of Finnish married couples aged 40–64 showed that the risk of divorce was greatest immediately after the onset of psychiatric morbidity. It then declined but persisted at a higher level compared to those with no psychiatric morbidity.
Although our findings reveal the importance of both physical and mental health for union dissolution in middle and later life, they also point to a need for research that addresses the implications of both dimensions on subsequent union dissolution simultaneously. Past research has tended to focus on each of these dimensions in separate analyses. Yet our findings suggest that not only are both relevant but that their relationship with subsequent union dissolution may differ somewhat. Of course, physical and mental health are also related to one another (Williams et al., Reference Williams, Di Nardo and Verma2017), raising the possibility that our results reflect confounded measurement. This is particularly so since we drew on SRH – a measure said to reflect individuals’ perceptions of overall health or functioning (i.e., physical, mental, and social) – to address physical health (Williams et al., Reference Williams, Di Nardo and Verma2017). However, as noted, prior evidence suggests that physical health tends to be the main driver of SRH among older adults and those reporting fair or poor SRH (Benyamini et al., Reference Benyamini, Leventhal and Leventhal2003; Monden & Uunk, Reference Monden and Uunk2013). When modelled simultaneously (results not reported), once again we found that decreased SRH was not significantly associated with subsequent union dissolution, whereas the impact of continuing fair/poor SRH was reduced (OR = 2.70; p = .076). Similarly, the impact of increased psychological distress was also reduced (OR = 2.80; p = .075), whereas the impact of ongoing moderate to high distress was not significant. On the one hand, this could be interpreted as evidence that when focused on individually, each picks up some of the effects of the other on union dissolution. However, it could also be an indication of a sequential process – for example, one in which psychological distress also serves as a mechanism through which chronic fair or poor SRH health affects union dissolution. The direction of the relationship between physical and mental health remains unclear (Williams et al., Reference Williams, Di Nardo and Verma2017) and was not possible to explore further with the data we had. However, it will be important for future research to direct attention to the entire process through which physical and mental health affect union dissolution.
Although not our primary focus, another notable outcome of the study is that the negative impact of continuing fair/poor SRH and the onset of psychological distress on union dissolution appears to hold even when both marital and cohabiting unions are considered together. This is so despite controlling for the fact that cohabiting unions are more likely than marital unions to dissolve in middle and later life. In the past, most studies of the relationship between health and union dissolution restricted their focus to marital unions only (e.g., Karraker & Latham, Reference Karraker and Latham2015; Latham-Mintus et al., Reference Latham-Mintus, Holcomb and Zervos2022; Lin et al., Reference Lin, Brown, Wright and Hammersmith2018 – Alderotti et al., Reference Alderotti, Tomassini and Vignoli2022 is an exception). Yet cohabitation has become increasingly prevalent among middle-aged and older adults and with it, a need to focus on the impact of physical and mental health on these unions as well. On the one hand, there are reasons to expect that these factors will impact union dissolution in a similar fashion among marital and cohabiting unions. For example, it has been noted that in later life, cohabitation appears to serve as a long-term alternative rather than a short-term prelude to marriage (Brown & Wright, Reference Brown and Wright2017), thereby suggesting the similarity of marital and cohabiting unions in middle and later life. If this is the case, one could infer that there should be little difference in the impact of health or other factors on union dissolution within these unions. On the other hand, there are also reasons to suggest that cohabiting unions may be more likely than marital unions to dissolve when confronted with either or both partners’ health problems (Kalmijn, Reference Kalmijn2026). For example, even if considered an alternative to and on par with marriage, cohabiting unions may lack many of the formal and informal role obligations and expectations that attend marriage. This includes the caregiving obligations traditionally associated with marriage (Brown & Wright, Reference Brown and Wright2017; Penning & Wu, Reference Penning and Wu2019). In fact, older cohabitors appear less likely to provide care to their partners than older married spouses (Noël-Miller, Reference Noël-Miller2011). Although sample size limitations precluded our ability to do so, there is a clear need for research that compares the role of physical and mental health declines and chronic ill health on union dissolution among both married and cohabiting unions.
Several other limitations should also be acknowledged when reviewing our findings. First, sample attrition is a concern in any longitudinal study. Previous research conducted using the LISA has found lower levels of attrition among middle-aged and older than younger adults and our analyses used survey weights to try and minimize its effect on our estimates (Benhin et al., Reference Benhin, Rouleau, Shahid and Simard-Duplain2022). Nevertheless, it is possible that attrition was more common among those in poorer health as well as among those whose unions dissolved compared to those in better health and whose unions remained intact. If those in poorer health were the most likely to see their unions dissolve, we may have under-estimated the negative impact of health changes on union outcomes. Second, the number of waves of data available for analysis was limited, thereby restricting our ability to conduct more fine-grained analyses of the short- and long-term implications of health on union dissolution.
A third limitation is the limited number of observed union dissolutions (n = 89) as well as of the number of respondents (n = 56) who experienced an increase in psychological distress. Small cell sizes can reduce the statistical power of a model to detect true differences, potentially increasing the risk of Type II errors. However, several factors mitigate these concerns in the current study. First, the effect sizes observed for these health transitions were substantial; for instance, increased psychological distress was associated with more than a threefold increase in the odds of dissolution (OR = 3.600, p = 0.033). Following the power calculation framework for logistic regression established by Hsieh, Bloch, and Larsen (Hsieh et al., Reference Hsieh, Bloch and Larsen1998), larger effect sizes require smaller sample sizes to achieve adequate power. The fact that these associations reached statistical significance despite the relatively infrequent nature of the event suggests that the study was sufficiently powered to detect the magnitude of the effects present in this population. The fact that our findings appear consistent with those reported for the USA and other western countries based on analyses of large-scale longitudinal panel data (e.g., Kalmijn, Reference Kalmijn2026) also lends credibility to the validity of our findings.
The limited number of unions that dissolved also prohibited more detailed analyses (e.g., comparisons of marital and cohabiting union dissolution). Further, although the survey included couples, there was an insufficient number whose unions had dissolved for couple-specific analyses. Finally, many of those in the study were already married for a long period prior to the first wave, with the result that long-term marriages were most heavily represented in the analytic sample. In fact, the average union duration reported at W2 was over 28 years. If health decline has more adverse effects on shorter duration unions, the fact that the sample was biased towards long-term unions could once again mean that the adverse effects of health decline on union dissolution have been under-estimated.
Despite some limitations, this study sheds light on the likely implications of changes in health for union stability in middle and later life in the Canadian context. Although exploratory, it shows that experiencing poor health appears to be detrimental to union stability, albeit somewhat differently depending on the health indicator involved. Despite the clear need for further research into this complex relationship, this is a finding with significant social and policy implications. For example, to the extent that long-term physical as well as emerging mental health problems destabilize intimate relationships, the result may be a significant loss of access to social support and care at a stage of life when it is often needed the most and when other relationships are increasingly unlikely to be able to compensate. This, in turn, could further increase demand for long-term residential care options. Policies and other strategies directed towards preventing chronic illness and mental health problems and limiting their adverse effects on individuals as they age may enhance union stability and reduce the likelihood of union dissolution and its implications. This will assume increasing importance as the population ages and as we see increases in both the absolute number and proportion of older Canadians experiencing poor health and union instability.
Data availability statement
Data used in this project were provided by Statistics Canada and accessed through the University of Victoria Research Data Centre, a part of the Canadian Research Data Centre Network (CRDCN). The data include Waves 1 through 5 (2012–2020) of the Longitudinal and International Study of Adults (5144_LISA-ELIA_AllYears). Because of the confidential nature of these microdata, they cannot be shared. Researchers in Canada working at one of CRDCN’s member institutions can access the data at no additional cost to the researcher. Other researchers pay cost-recovery to access the data. Access to the data is subject to a background check and research approval process. The protocols for data access, including fees for researchers at non-CRDCN institutions, can be found on the CRDCN website (https://crdcn.ca).
Acknowledgements
We would like to acknowledge the contributions of Zheng Wu, PhD (deceased) towards acquiring the funding for this work. We also thank Dr Feng Hou for analytical feedback and Bodhin Kidd, BA for help in identifying relevant literature.
Author contributions
S.B. and M.P. jointly conceptualized and drafted the initial and revised versions of the manuscript. G.L. and S.B. carried out the analyses. All authors reviewed drafts and approved the final version of the manuscript.
Financial support
This study was supported by a grant from the Social Sciences and Humanities Research Council of Canada (SSHRC) Insight Grants Program (#435-2017-0057), 2017–2024. This research was conducted at the University of Victoria Research Data Centre, a part of the Canadian Research Data Centre Network (CRDCN). This service is provided through the support of the Canada Foundation for Innovation, the Canadian Institutes of Health Research, the Social Sciences and Humanities Research Council, and Statistics Canada as well as through the support of the University of Victoria and Province of British Columbia. All views expressed in this work are our own.
Competing interests
The authors declare that they have no competing interests.

 Open access
Open access