


Forensic mental health services provide specialist treatment to people who pose a serious risk of harm to others in the context of a mental disorder. Reference Whiting, Ryland, Fazel, Focquaert, Shaw and Waller1 The treatment pathway in the UK is based around the secure hospital system, where treatment is provided in low-, medium- and high-secure settings for people detained under civil or criminal proceedings parts of the Mental Health Act 1983. Reference Whiting, Ryland, Fazel, Focquaert, Shaw and Waller1 The pathway is complex and interfaces with many other services.
In England, community forensic mental health services (CFMHS) developed over the past three decades as a community extension to secure hospitals, with emphasis on supporting those leaving secure hospital, Reference Kenney-Herbert, Taylor, Puri and Phull2 addressing long-standing concerns about overly institutionalised care for the forensic population highlighted in the 1992 Reed Report. 3 More recently, NHS England’s New Care Models programme further emphasised community forensic care, as part of goals to provide care in the ‘least restrictive setting, as close to home as possible and with a stronger focus on recovery’. 4
The development of CFMHS in England was rapid and ad hoc, led by local need Reference Latham and Williams5 and with variation in what CFMHS provide, to whom and how services are organised. Reference Judge, Mari-Anne and Fahy6 This may be particularly the case for more peripheral functions, such as advising other services. Reference Kenney-Herbert, Taylor, Puri and Phull2 Two models have typically been described: those in which forensic clinicians work within general mental health services, referred to as integrated services, and those in which they work separately in a parallel service that is operationally distinct from general mental health services. Reference Latham and Williams5,Reference Humber, Adrian, Steve, Thomas and Shaw7 However, there is some variation in how these labels are applied. Reference Kenney-Herbert, Taylor, Puri and Phull2 Further, not all models fit this categorisation, such as ‘outreach’ models whereby in-patient secure hospital teams provide ongoing community care, and a tiered approach whereby functions interfacing with general services range from advice only, through to shared working and full handover of care coordination to forensic services.
Considerable efforts have been made to develop clinical standards for CFMHS in England, Reference Kenney-Herbert, Taylor, Puri and Phull2 which could better facilitate quality oversight, development and research into the effectiveness and resource implications of different components. However, the extent to which consistency has been achieved, or to which early conceptualisations of models remain relevant, is not well understood. This study therefore aimed to examine current provision of CFMHS in England by surveying these clinical services, to understand their population, staffing, treatment provision and organisation.
Method
Data collection
Data for this cross-sectional study were collected via Freedom of Information (FOI) requests. Use of FOI requests is a recognised research method for accessing data held by public institutions. Reference Savage and Hyde8 The information requested (Supplementary Material) was based on previous similar surveys Reference Kenney-Herbert, Taylor, Puri and Phull2,Reference Judge, Mari-Anne and Fahy6 and agreed among the research team, which included community forensic clinicians, of whom one (M.T.) was previously involved in standard-setting work. Reference Kenney-Herbert, Taylor, Puri and Phull2 We asked respondents to summarise their service organisation in a more granular manner than previous descriptions, as either (a) operating as part of secure hospital-based forensic services; (b) a standalone community forensic team that works in parallel with general adult services; (c) forensic clinicians working within non-forensic teams as an integrated service or (d) other.
Relevant mental health teams were identified through a briefing from the Royal College of Psychiatrists, 9 supplemented by a search undertaken by the Nottinghamshire Healthcare NHS Foundation Trust Library and Knowledge service. The FOI requests were then directed to relevant NHS Trusts in March 2023, and followed up in July 2023 for those who had not responded.
Analysis
Data were collated, stored and analysed using PSPP statistical software. 10 Descriptive statistics were used to summarise the data. Chi-squared tests were used to test for associations with different service structures. Structured survey responses were supplemented by referral and policy documentation, which was reviewed to provide more granular detail where necessary. As this scoping exercise did not involve patients or patient data, research ethics approval was not required.
Results
FOI requests were sent to 50 NHS mental health Trusts in England. Forty Trusts (80%) responded. Of these, 31 (78%) have a CFMHS of some description. One Trust reported that they have two services (one of which specialises in forensic intellectual disability) and thus submitted a response for each. Therefore, we describe findings relating to a total of 32 CFMHS.
Description and organisation
A variety of names have been adopted for services: community forensic team/service (n = 13, 41%), specialist community forensic mental health team/service (n = 7, 22%), community forensic mental health team/service (n = 6, 19%), outreach and liaison service (n = 4, 13%), intensive recovery support (n = 1, 3%) and integrated community forensic psychological pathway (n = 1, 3%). Summary descriptions of these services were either being part of secure hospital-based forensic services, i.e. operating as an extension of these services regardless of referral source, rather than a standalone team (n = 19, 59%); or standalone services working in parallel with general services (n = 13, 41%). Physical team bases also varied, with 15 (47%) operating out of a secure hospital unit environment and eight (25%) having access to their own separate community clinical base (either solely, or in addition to other bases). Others use shared community sites or non-clinical/administrative settings. For most services (n = 20, 63%), the geographical catchment area for the community forensic team mapped directly to that of the NHS Trust; however, ten services reported a larger catchment area (31%) and two (6%) reported a smaller catchment area.
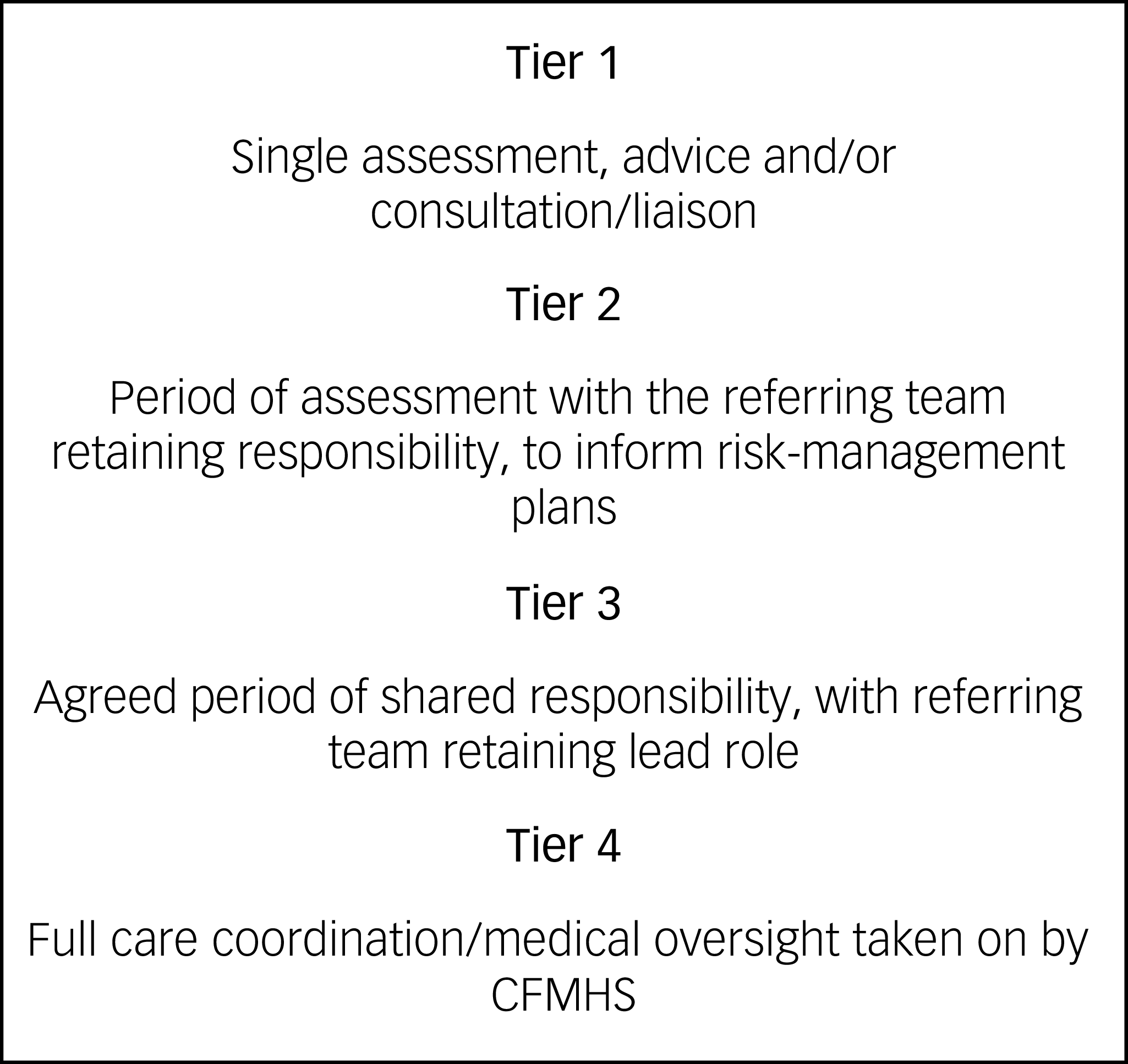
Descriptions of the role of services illustrated a range of functions not captured by structured responses, including ‘in-reach’ services to forensic wards, and Trust-wide ‘scaffolding and advice’. Of the nine services that provided this level of detail on their operating model, six described tiered referral responses, typically with levels of service from advice to handover of care (Fig. 1).
Example of four-tier community forensic mental health service (CFMHS) model describing interface with referring service.

Staffing and patient ratios
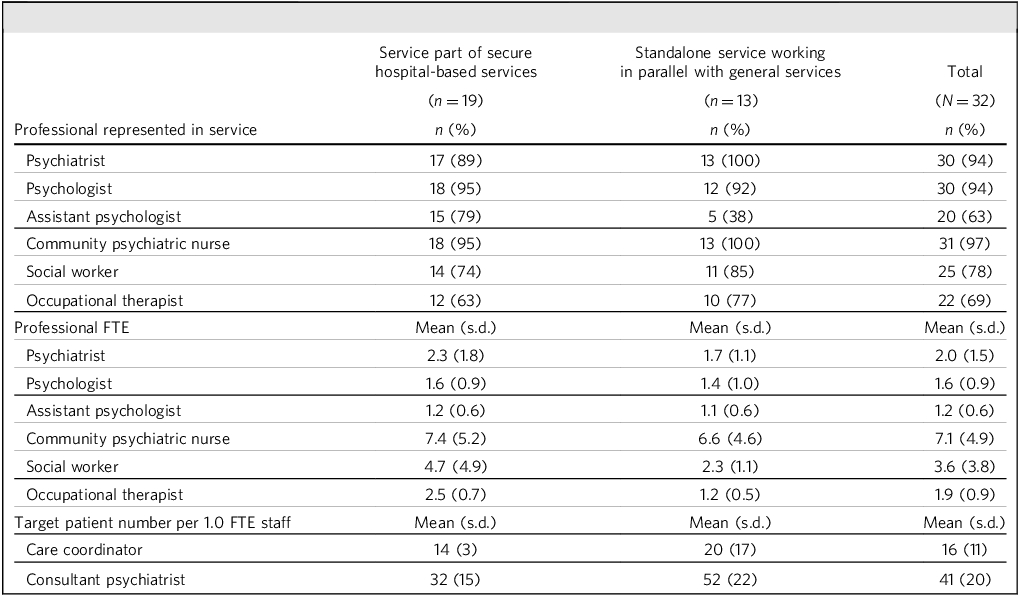
Table 1 summarises the clinician composition of included services. Almost all services reported having designated input from psychiatrists, psychologists and community psychiatric nurses, with variation in the presence of input from social workers, assistant psychologists and occupational therapists. In the two services in which there is no specific psychiatric time embedded in the community team, medical oversight is from the in-patient consultant psychiatrist. There was significantly higher occupational therapy provision in those services that were described as being operationally integrated with secure hospital services rather than standalone parallel teams (χ 2 = 11.37, P ≤ 0.001). Other professionals represented were education, training and employment workers in seven services (22%), speech and language therapists in four services (13%) and pharmacists in three services (9%). Seven services (22%) had peer support workers with lived experience. Where a specific target caseload per full-time equivalent staff member was reported (n = 26 services), these targets typically ranged from 10 to 20 for care coordinators (with one outlier reporting 70), but were more variable for consultants, ranging from 15 to 90. These did not significantly vary by service description.
Clinical professional composition of community forensic services

FTE, full-time equivalent.
Referral criteria and processes
All but one service reported specific policies or guidelines regarding referral procedures into the CFMHS, and most (n = 29, 91%) use a referral form. All services accept referrals from in-patient forensic services, and 12 (38%) reported that the CFMHS automatically accepts patients discharged from these services. Around two-thirds (n = 20, 63%) accept referrals from general adult community mental health teams, 56% (n = 18) accept referrals from non-secure in-patient services and just over half (n = 17, 53%) accept referrals for people in prison. Three-quarters (n = 24, 75%) accept patients with a primary diagnosis of a personality disorder. Twenty-six services (81%) mandate structured risk assessment for entry into the service, in most cases using the Historical, Clinical, Risk Management Scale-20 (HCR-20). Other structured assessments utilised include Risk for Sexual Violence Protocol (RSVP), Spousal Assault Risk Assessment (SARA) Guide, Sexual Violence Risk-20 (SVR-20), Structured Assessment of Protective Factors for Violence Risk (SAPROF) and local Trust risk assessment measures.
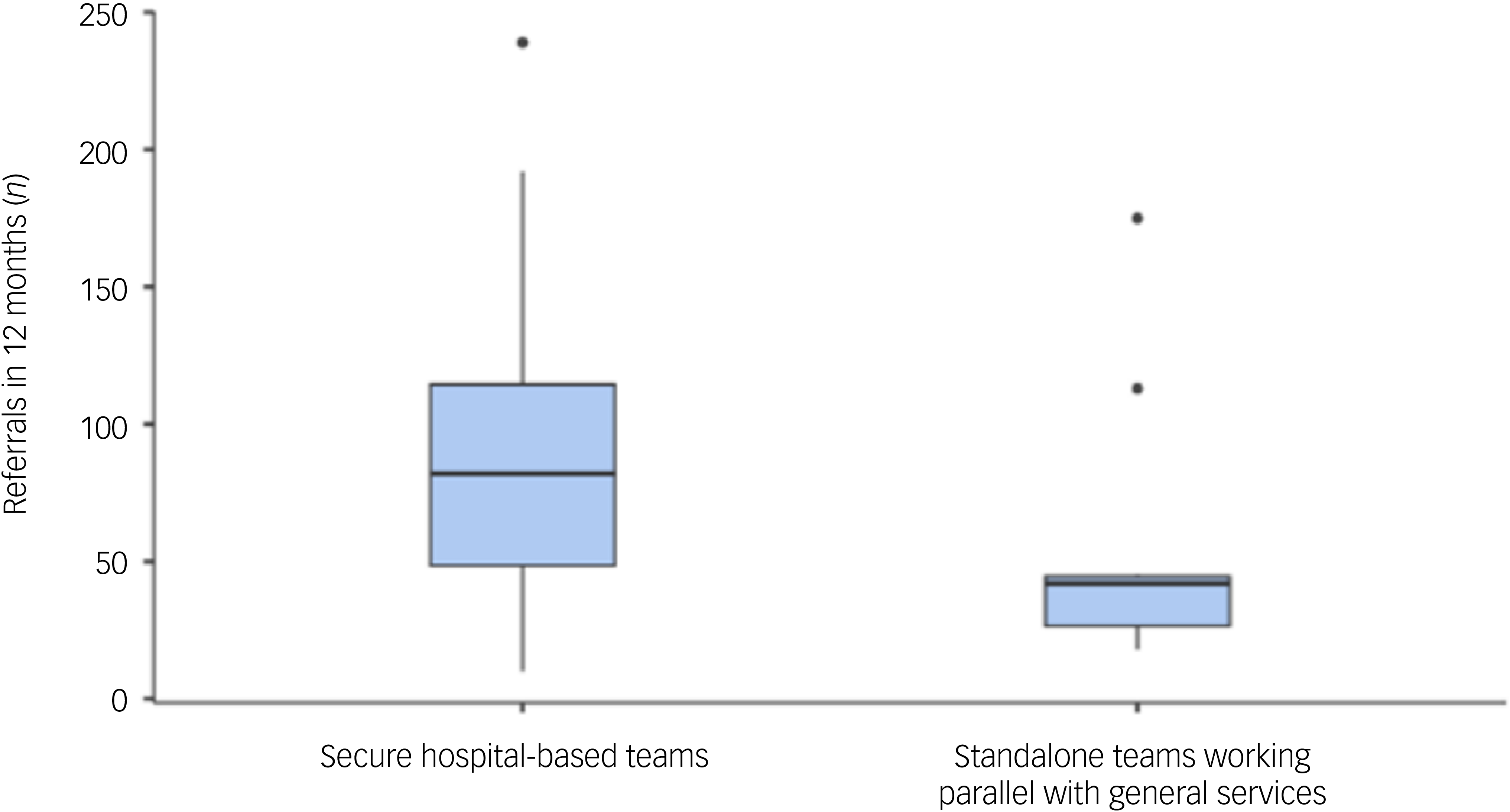
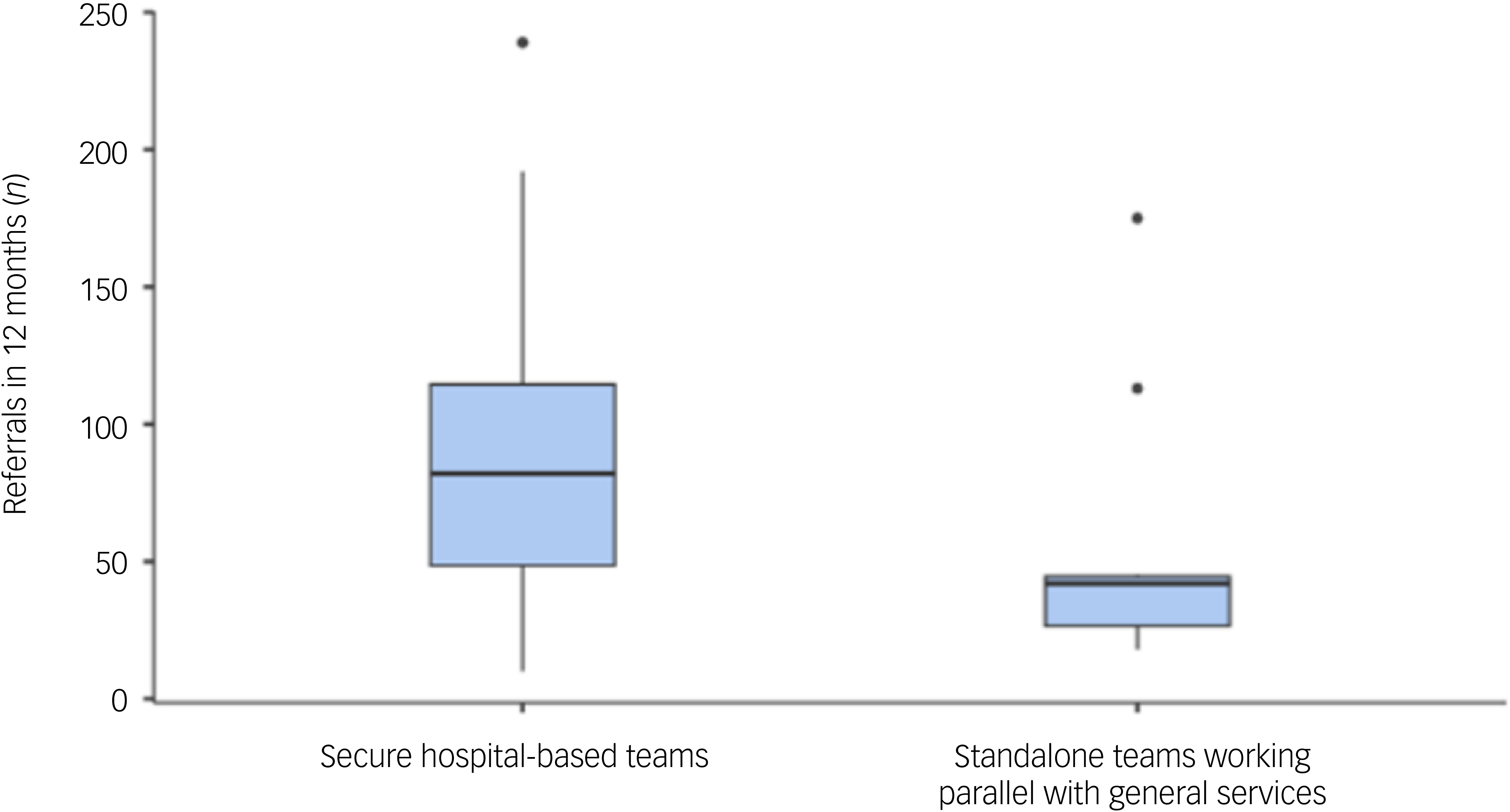
In the 12 months from January to December 2022, the number of referrals received by services ranged widely, from 10 to 239 patients (mean 79, s.d. 59), and was significantly more for those services operating as part of secure hospital teams compared with standalone teams (χ 2 = 4.85, P ≤ 0.028) (Fig. 2). Acceptance rates for individual services ranged from 15 to 100% (mean 62%, s.d. 28). Of the two services with 100% acceptance rates, one was a service operating as part of secure hospital services and only accepting forensic in-patients requiring community follow-up, whereas the other was a standalone service that accepted referrals from both general and forensic services. Overall, there was no significant difference in acceptance rates between service types.
Box plot showing range, median and interquartile range of number of referrals in 12 months to community forensic mental health services, by service type.
Legal status
Four services (13%), all of which operate as part of secure hospital services, do not have any informal patients under the care of the team (i.e. patients not subject to any community supervision frameworks of the UK Mental Health Act 1983). All services accept patients under the expected relevant legal frameworks, i.e. community treatment orders and conditionally discharged patients. With regards to the long-term management of patients subject to special restrictions under Section 41 of the Mental Health Act 1983, Reference Jewell, Cocks, Cullen, Fahy and Dean11 managed in the community under the conditional discharge framework, 12 services (38%) reported that these patients would remain under the care of the CFMHS, whereas 20 (63%) reported that there would be a step-down pathway to move toward transfer to a general community mental health team when the risk management was deemed to no longer require specialist forensic involvement.
Service and treatment provision
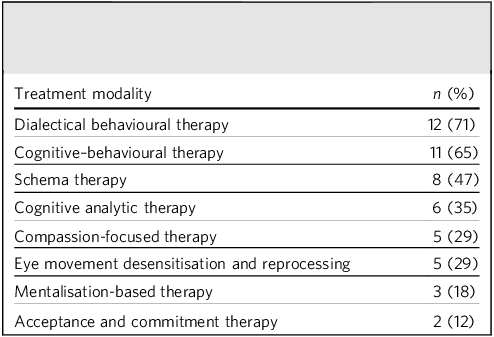
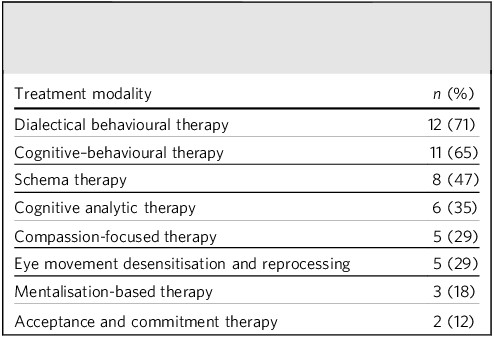
All services endorsed case management as a core role of their service, alongside, in most cases, liaison with justice agencies (n = 27, 84%). Psychological interventions were provided by nearly all services (n = 30, 94%); however, the modality of treatment offered varied between services (see Table 2 for data for the 17 services that provided this information). Some services also reported offering more generic psychoeducation (n = 4, 24%) or offence-related interventions (n = 6, 35%). Around a third (n = 11, 34%) specified that some additional treatment is provided through outside agencies, such as substance misuse treatment.
Psychological interventions provided by 17 community forensic mental health services that provided this information
Out-of-hours provision
Fourteen services (44%) stated that there is a specific arrangement for out-of-hours provision for the service, and the remainder operated a service between 09.00 h and 17.00 h, Monday to Friday only. Thirteen services provided information on the out-of-hours arrangements, and this took a variety of forms, with eight services operating their own on-call cover, and others accessing Trust-wide out-of-hours or crisis services.
Discussion
This study provides a contemporary overview of CFMHS in England. By submitting Freedom of Information requests to 50 NHS Trusts, we have examined service organisation, function, referral criteria and aspects of operations. A core finding is the demonstration that a simple binary description of CFMHS as either being integrated with general mental health services or existing in parallel to them, no longer maps sufficiently well to practice. A more relevant categorical distinguisher instead appears to be whether services are primarily extensions of secure hospital teams, although this is also an oversimplification. CFMHS continue to vary, and we discuss here three key areas of heterogeneity, with implications for future service development and research.
First, despite the existence of national service standards, Reference Kenney-Herbert, Taylor, Puri and Phull2 CFMHS in England vary widely in core aspects, including their operational integration with secure in-patient and general adult services, clinician composition and even service name. This aligns with findings from the Royal College of Psychiatrists’ standards report, which also noted significant divergence in CFMHS models across regions. Reference Kenney-Herbert, Taylor, Puri and Phull2,4 Variation likely reflects local commissioning arrangements, and the development of services ad hoc in response to local need. However, such variation in fundamental characteristics can also contribute to ongoing ambiguity regarding service roles and remits, evidenced elsewhere in our findings, and complicate the development of coherent referral pathways. The limited information available on out-of-hours provision suggested this was also heterogenous. This is an area of further complexity in terms of the interface with general services, and approaches to crisis care themselves vary. Reference Dalton-Locke, Johnson, Harju-Seppänen, Lyons, Sheridan Rains and Stuart12
Second, there was marked variation between CFMHS in the practice of accepting referrals from different clinical settings, with a considerable minority of CFMHS not accepting referrals from community or in-patient general adult services, and only around half of CFMHS accepting referrals directly from integrated mental health teams in prison. The latter finding is concerning, given the well-recognised challenges associated with managing serious mental illness on release from prison Reference Hopkin, Evans-Lacko, Forrester, Shaw and Thornicroft13 and evidence that mental illness is a key risk factor for reoffending and reincarceration. Reference Jones, Manetsch, Gerritsen and Simpson14 This would seem an issue in urgent need of consistency and standardisation. Such variation in approach to referrals from different clinical settings likely contributes to uncertainty among referrers about what CFMHS provide. This is further demonstrated by the wide range of acceptance rates by CFMHS, with a lower bound of 15%. Such differences will be linked to variation in local commissioning arrangements and their evolution in the past decade, with, for example, the focus of NHS England’s Mental Health Secure Care Programme on reducing length of stay in secure hospital and therefore emphasising community support for those leaving these settings.
Third, there remains variation in the approach to conditionally discharged patients subject to restriction by the Ministry of Justice, with around 60% of services being geared toward progressing this patient group to step-down to general mental health services. This mirrors other work finding that around a third of all conditionally discharged patients were managed by general mental health services in one English NHS Trust. Reference Adesola, Saleem, Kelbrick, Halim and Nkire15 This specific issue is central to the function of CFMHS; has important resource, service capacity and risk-management ramifications; and is an area of uncertainty and increasing discussion. Reference Saleem, Kelbrick, Halim, Adesola, Nkire and Ansari16
Implications for research and service development
Although some variation in specific local arrangements is inevitable and appropriate, the extent to which the core structure and function of CFMHS in England continues to vary by area suggests that there is a further need for central standardisation. Referral pathways and the approach to the management of conditionally discharged patients may be especially important. The extent of current heterogeneity in core elements of CFMHS organisation and practice is a potential barrier to national benchmarking and service evaluation. Further, despite no longer being a nascent model, the findings suggest that CFMHS continue to lack a consistent core identity for what service they should be providing and to whom. Efforts to standardise may therefore need to begin with consultation to achieve consensus on what CFMHS are, and to what they should aspire in terms of key outcome measures and patient and carer experience.
Currently, there is a limited evidence base to underpin efforts to standardise models or provide evidence for the best practice elements, or ‘active ingredients’ of CFMHS. This deficit is not unique to the community part of forensic mental health services. Reference Tully, Hafferty, Whiting, Dean and Fazel17 Addressing this shortfall would need to involve drawing upon increasingly well-developed research methods for examining complex health service interventions. Reference Skivington, Matthews, Simpson, Craig, Baird and Blazeby18 This should include careful consideration of issues such as the fidelity of model implementation and relevant outcome measures. To what extent, for example, fuller integration with general mental health teams improves continuity of care and collaboration, Reference Mohan, Slade and Fahy19 or to which hybrid models Reference Mohan and Fahy20 mitigate concerns about fragmentation from wider mental health services, Reference Khosla, Davison, Gordon and Joseph21 remain important questions for empirical exploration. Internationally, community services and evidence are likewise mixed. Reference Natarajan, Srinivas, Briscoe and Forsyth22–Reference Beis, Graf and Hachtel24 In the USA, a forensic assertive community treatment approach has evolved as best practice, with some evidence for improved forensic outcomes such as days in prison. Reference Goulet, Dellazizzo, Lessard-Deschênes, Lesage, Crocker and Dumais25 Understanding of effectiveness has, however, similarly been hampered by a lack of standardisation in structure and operation. Reference Lamberti and Weisman26
A related, overarching question is the weighting given to the mixed roles of CFMHS. Currently, service standards in England describe the first core function as being to provide case management for people who ‘present a significant risk of serious harm to others related to their mental disorder, particularly those leaving secure care, for whom the risk is best managed by specialist forensic mental health services’. Reference Kenney-Herbert, Taylor, Puri and Phull2 Core common elements of CFMHS directly address this role, such as having risk thresholds for access, comprehensive care planning and joint working across sectors. Reference Wark and Gredecki27 However, one potential source of model variation is how secondary functions such as providing ‘liaison, advice, specialist interventions, educational and skills development’ to general mental health services are achieved, and the extent to which these functions are emphasised by individual services. The findings of this study are timely in the context of renewed consideration of the provision of community psychiatric care in England, particularly for those with complex needs and experiencing severe and enduring mental illnesses. Reference Smith28 A recent independent mental health homicide investigation made recommendations around the appropriate distribution of resources to meet the needs of patients with serious mental illness, with consistency in the oversight of care. 29 The boards responsible for planning and coordinating local services in England have also recently been asked by NHS England to review whether arrangements are sufficiently developed in terms of assertive community models of care. 30 Although the potential resurgence of, for example, assertive outreach teams Reference Firn, Hindhaugh, Hubbeling, Davies, Jones and White31 are not a substitute for CFMHS, clarification and standardisation of the functions of CFMHS needs to be approached in the context of this evolving community landscape.
A fundamental element of all CFMHS is the assessment of risk at the point of referral/assessment. How mental health services understand the concept of risk, and its assessment and management, has also been subject to recent wider scrutiny and recommendations. 29,Reference Fazel and Lennox32 At the point of interface with CFMHS, there is increasing potential for standardisation and improving consistency, clarity and transparency. Although evidence for risk assessment tools used by forensic services is mixed, Reference Ogonah, Seyedsalehi, Whiting and Fazel33 advances in statistical approaches to risk prediction have now made simpler, scalable and probabilistic assessments of risk more accessible. Reference Whiting, Glogowska, Mallett, Maughan, Lennox and Fazel34 There could be a role for such approaches in improving the identification and referral of those people under the care of general adult mental health services who are most likely to benefit from assessment by CFMHS, but this role in referral and assessment pathways needs development. Such approaches need to be considered in the context of defining with greater clarity the extent to which the role of CFMHS includes reaching out into general mental health services to reduce violence risk before a first serious offence occurs, and clinicians exporting their skills to assist non-forensic colleagues in formulating clinical risks and potential strategies to mitigate these. There is considerable potential for improved prevention where risk sits below the threshold that would warrant a forensic service assuming responsibility for care. For example, one in ten people who present to early intervention in psychosis services perpetrate violence in the first year after contact. Reference Whiting, Mallett, Lennox and Fazel35 Guidance to general adult services on use of these straightforward probabilistic tools may be a useful part of lower-tier interventions, such as ‘advice only’, or as part of multi-professional meetings.
Limitations
This survey was exploratory in nature, and data are limited to the 80% of Trusts who responded. Interpretation of quantitative data around referrals and staffing is limited by incomplete information on catchment area population to contextualise findings, and the limited granularity on certain aspects of staffing, such as understanding how psychiatric input is provided in practice (e.g. the amount of ringfenced time for community patients in hybrid models where psychiatrists are also based on hospital units). Details of specific commissioning and funding arrangements were also not collected, which is of direct relevance to aspects of structure and function, including staffing.
Data on multidisciplinary staffing provision were not contextualised in terms of the caseload numbers for the service. Therefore, this only provides information on variation in the size of clinical teams in absolute terms, rather than the intensity of resource available per patient. The information collected on caseload numbers for psychiatrists and care coordinators was also simplistic. Limits on caseloads has been one way in which CFMHS have been distinguished from general community services, Reference Humber, Adrian, Steve, Thomas and Shaw7 although evidence for the benefits of intensive case management approaches (with caseloads lower than 20) over standard case management is limited. Reference Dieterich, Irving, Bergman, Khokhar, Park and Marshall36 Different study designs are required to properly examine this aspect, with more granular information on frequency and nature of contacts and support provided rather than numbers alone. Reference Happell, Hoey and Gaskin37
In conclusion, CFMHS continue to vary both in core functions, such as the long-term approach to patients subject to special restrictions, and in the extent to which secondary functions are emphasised and operationalised, such as the interface with services in non-forensic hospitals, prisons and the community. Although this variation can be explained in part by local needs and commissioning, improved consensus and consistency would support both quality assurance and the development of an empirical evidence base. Renewed and alternative centralised approaches from relevant national bodies are likely required to move toward such standardisation.
About the authors
Marie Williams is a Research and Evidence Assistant at Nottinghamshire Healthcare NHS Foundation Trust, Nottingham, UK. Leah Wooster is a Consultant Forensic Psychiatrist at Birmingham and Solihull Mental Health NHS Foundation Trust, Birmingham, UK. Mark Taylor is a Consultant Forensic Psychiatrist at Nottinghamshire Healthcare NHS Foundation Trust, Nottingham, UK. John Tully is an Honorary Consultant Forensic Psychiatrist at Nottinghamshire Healthcare NHS Foundation Trust, Nottingham, UK; and Clinical Associate Professor in Forensic Psychiatry at the School of Medicine, University of Nottingham, UK and the Institute of Mental Health, Nottingham, UK. Daniel Whiting is an Honorary Consultant Forensic Psychiatrist at Nottinghamshire Healthcare NHS Foundation Trust, Nottingham, UK; and Clinical Associate Professor in Forensic Psychiatry at the School of Medicine, University of Nottingham, UK and the Institute of Mental Health, Nottingham, UK.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1192/bjb.2026.10236
Author contributions
All authors conceived the study. M.W. collected and analysed the data. All authors interpreted the data. D.W. and M.W. drafted the manuscript. All authors critically revised the manuscript.
Funding
There was no specific funding for this work.
Declaration of interest
None.



 Open access
Open access
eLetters
No eLetters have been published for this article.