


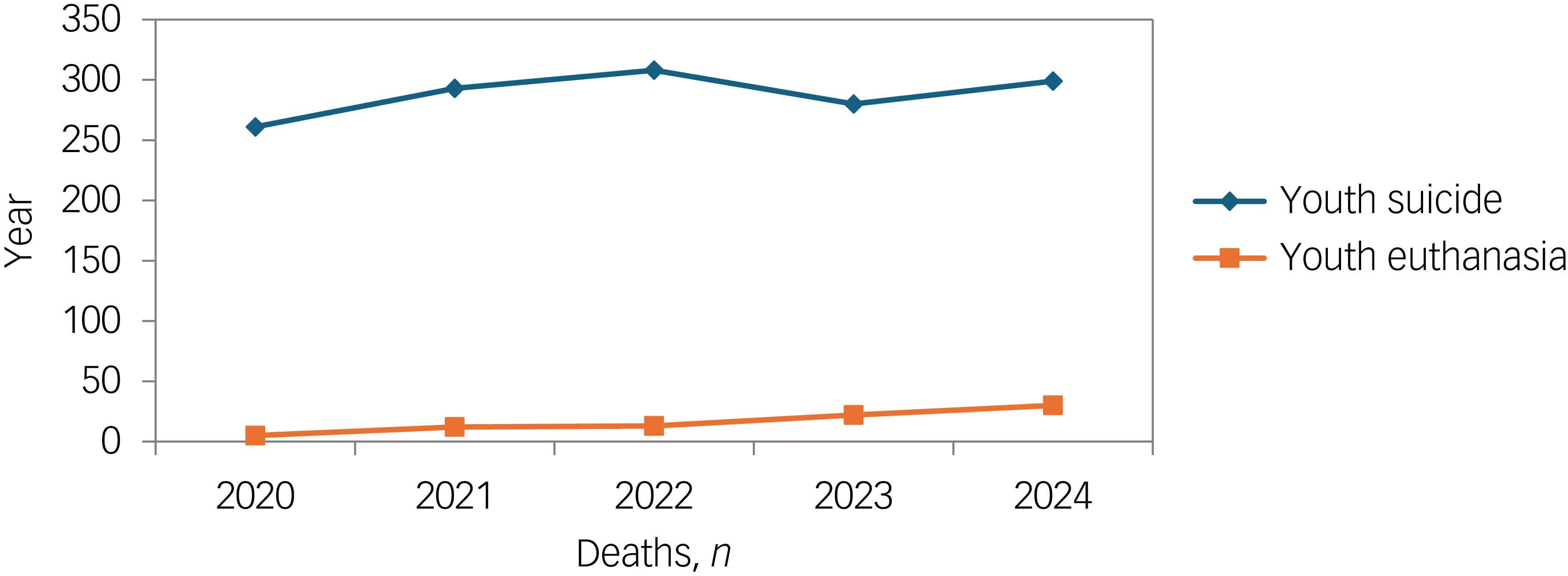
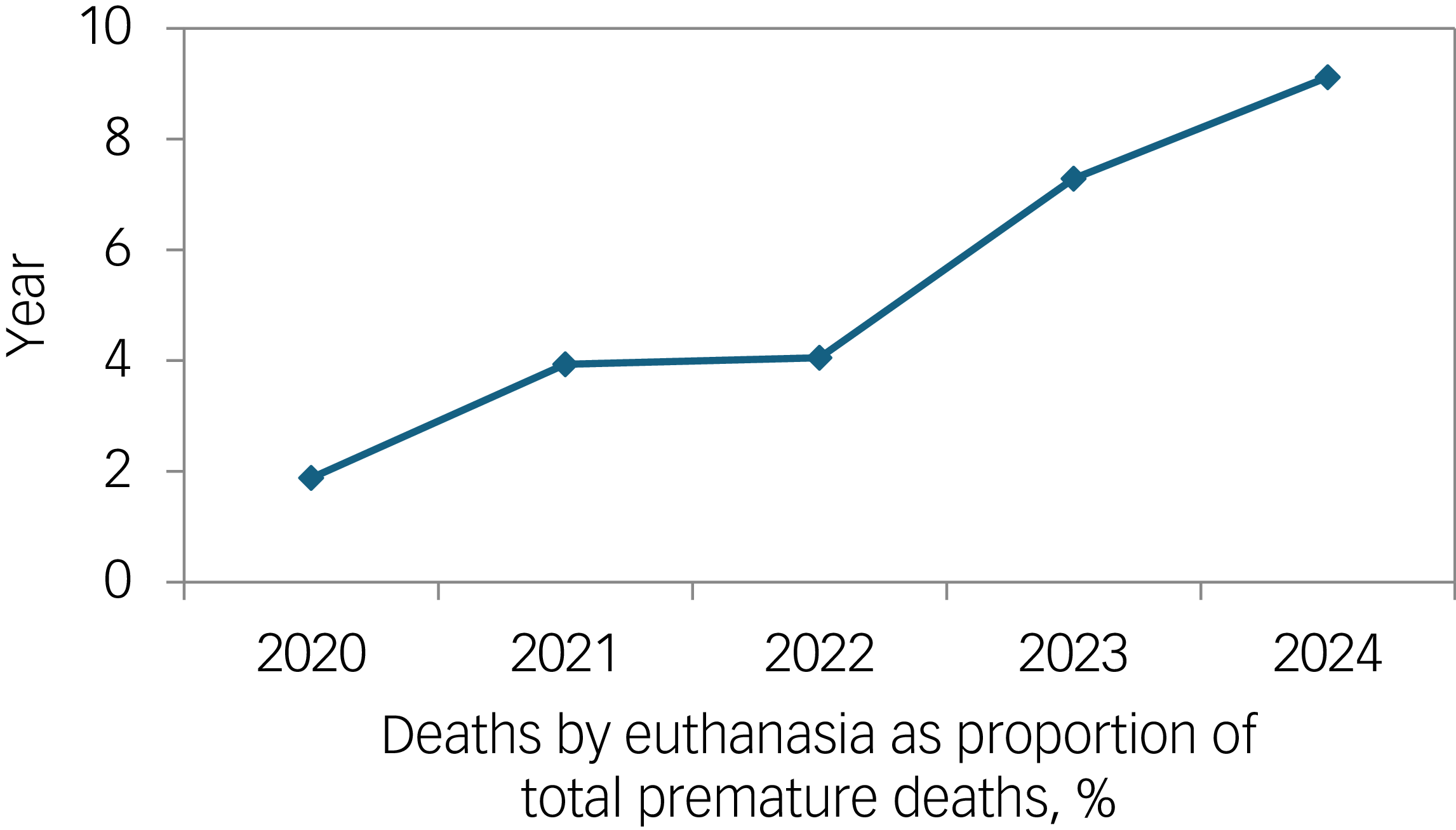
In The Netherlands, euthanasia or medical assistance in dying (MAID) for mental suffering in youth – once a rare and cautious practice – has expanded rapidly, now including young adults and even minors. Between 2020 and 2024, the number of euthanasia procedures for individuals under 30 rose from 5 to 30, a sixfold increase, representing over 9% of all premature deaths (suicide + assisted dying) in that age group 1,2 (Figs 1 and 2). The ensuing public debate has been lively, with a section of the press presenting a romanticised ‘human interest’ approach to youth euthanasia, supported by a small group of professional proponents, giving rise to the so-called Werther effect. Reference Huisman3


Elsewhere, we and others have discussed extensively how the moral, clinical and legal debate surrounding psychiatric euthanasia has evolved in The Netherlands, including discussions about fluctuating capacity, relative autonomy, what constitutes unbearable suffering, relational dynamics, prognostic uncertainty and non-maleficence/beneficence. Reference van Os and Denys4–Reference van Os, van Rooij and Komrad7 Here, we wish to focus specifically on the increasingly common use of a novel epidemiological argument that has taken centre stage in the media: that euthanasia for mental suffering in young people is necessary to prevent a violent or lonely suicide.
The suicide prevention argument in The Netherlands was most notably advocated by a retired psychiatrist, who admitted in a national newspaper to having performed euthanasia 12 times in 11 months, including young people and minors. Reference Bos and Haan8 Introducing deterministic terminology like calling patients ‘mentally terminal’, Reference Oosterhoff9 the retired psychiatrist argued that refusing assisted dying to a suicidal patient can be catastrophic in the case of a ‘false-negative’ event. Reference Oosterhoff10 The prevention argument has received sympathetic and emotionally charged media coverage. Reference Efting11,Reference van Hintum12 There is anecdotal evidence that, as a result, clinicians in The Netherlands are increasingly faced with demands by young people – and sometimes their families – that euthanasia is indicated in order to prevent a suicide.
Although superficially convincing, it may be argued that this position exemplifies a questionable emotional inversion of compassion turned into coercion. By dissecting the underlying epidemiological assumptions we can determine to what degree this claim holds empirical or ethical weight.
The epidemiological landscape of suicide
Suicide, even among high-risk psychiatric groups, remains statistically rare. Among those with treatment-resistant depression, the annual risk is roughly 0.5%, or 5% over a decade. Reference Bergfeld, Mantione, Figee, Schuurman, Lok and Denys13 In psychiatric populations, even the presence of suicidal ideation predicts suicide poorly, with a pooled positive predictive value of only about 4% and an annual suicide risk of roughly 0.3–0.5% among those expressing such thoughts. Reference McHugh, Corderoy, Ryan, Hickie and Large14
Therefore, even in severely ill and suicidal groups, the base rate problem dominates: most do not die by suicide. Any policy equating psychiatric assisted dying with suicide prevention implicitly assumes we can accurately identify, ex ante, the minority who otherwise would have died. This assumption is empirically untenable.
The recent study by Schweren and colleagues on 353 young people (<24) who applied for psychiatric assisted dying at the Dutch Euthanasia Expertise Centre found that: 47% of applicants withdrew their request, 45% were rejected, 3% died by assisted dying and 4% died by suicide during the evaluation process, translating to an annual suicide risk of around 2.9%. Reference Schweren, Rasing, Kammeraat, Middelkoop, Werner and Mérelle15 So in this group explicitly requesting euthanasia, the annualised suicide rate is about fivefold higher than in other high-risk psychiatric populations – but still far from universal, meaning most do not die by suicide, even after requesting assisted dying.
Euthanasia as suicide prevention: the evidence fails
Empirically, there is no population-level evidence that assisted dying reduces suicide mortality. A systematic review by Doherty and colleagues found no consistent reduction in suicide rates in countries that legalised assisted dying; in some, suicides even increased. Reference Doherty, Axe and Jones16 In The Netherlands, despite growing numbers of psychiatric euthanasia cases, suicide among young women continues to rise. 1
Testing the ‘preventive’ hypothesis: an epidemiological model
Let us treat youth euthanasia-as-prevention as a diagnostic test problem, in which ‘test positive’ is deemed ‘irremediably ill with a rational death wish’ and ‘test negative’ is not deemed eligible.
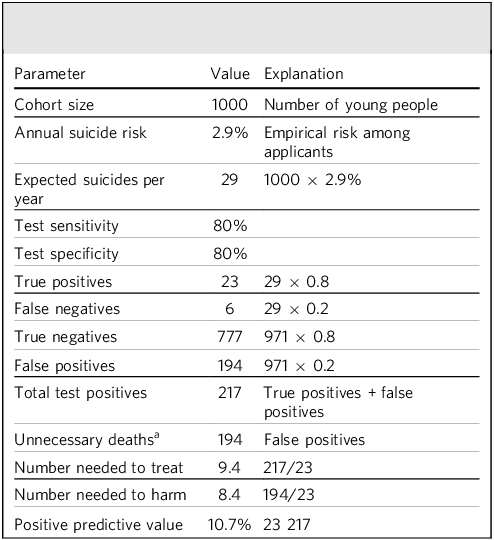
To test the ‘youth euthanasia-as-prevention’ hypothesis under more realistic conditions, we employ a model using the empirical annual suicide risk of 2.9% observed among Dutch youth who applied for psychiatric assisted dying. Reference Schweren, Rasing, Kammeraat, Middelkoop, Werner and Mérelle15 We assume optimistic test parameters – a sensitivity of 80% and specificity of 80% – and a cohort of 1000 young people.
Table 1 shows the basic epidemiological parameters that can be derived from these data. As is standard in clinical epidemiology, both the number needed to treat (NNT) and the number needed to harm (NNH) are rounded up to the nearest whole person, since one cannot treat – or in this case, end the life of – a fraction of an individual. Applying this convention yields an NNT of 10 and an NNH of 9, under these optimistic assumptions. In other words, approximately ten young people would need to undergo assisted dying to ‘prevent’ one suicide, and nine would die without a preventive purpose being served as a direct consequence of the intervention. The positive predictive value (PPV) is 10.7% – meaning fewer than one in ten people deemed suicidal would actually have died by suicide without intervention.
Epidemiological parameters of psychiatric euthanasia as a preventive intervention

a In this context, ‘unnecessary’ means deaths that do not serve any preventive purpose.
Testing these parameters under different scenarios can serve as an impression of the boundaries of these estimates. For example, assuming an annual suicide risk of 5% instead of 2.9% still would yield an NNT of 6, an NNH of 5 and a PPV of 17.4%. Likewise, assuming 70% for sensitivity and specificity instead of 80% would yield an NNT of 16, an NNH of 15 and a PPV of 6.5%.
Thus, even under generous assumptions, and realistic sensitivity scenarios thereof, the ‘preventive’ justification for assisted dying is not convincing. The intervention eliminates far more lives than it plausibly saves. In real-world conditions – where predictive accuracy is poorer and substitution effects are uncertain – the ratio of iatrogenic to prevented deaths would likely be higher.
Proportionality and subsidiarity
Epidemiology of prevention demands proportionality: the heavier the intervention, the stronger the evidence of benefit needs to be. Assisted dying, being irreversible, demands near-perfect certainty that recovery or treatment is impossible – yet the uncertainty is maximal. Moreover, the criterion of subsidiarity requires demonstration that all less invasive alternatives have failed. In psychiatric youth, this is almost never the case: the Comprehensive Resource Model of trauma therapy, relational continuity and social rehabilitation remain underprovided. Reference van Os and Denys4
Recent analyses Reference Tuffrey-Wijne, Curfs, Hollins and Finlay17,Reference Tuffrey-Wijne, Curfs, Finlay and Hollins18 show that many euthanasia requests from young people with autism or intellectual disability arise not from medical treatment futility but from social exclusion, overstimulation and lack of supportive care. The suffering is real, but its determinants are social. Labelling such pain ‘medical’ in order to satisfy euthanasia law introduces structural ableism – an observation echoed in 2024 by the United Nations Committee on the Rights of Persons with Disabilities, which urged The Netherlands to revise its legislation for insufficient protection of vulnerable citizens. 19
Cost analyses of assisted dying indicate the moral hazard: assisted dying is cost-saving compared with prolonged care. Reference Trachtenberg and Manns20 Framing death as resource efficiency may betray the medical ethos. When systems fail to provide continuity, relational safety and inclusion, assisted dying risks becoming a systemic shortcut to compensate for social neglect. Reference Perry21
False positives, false negatives and moral asymmetry
In our model, false negatives – those few who might still die by suicide despite rejection – are numerically and ethically dwarfed by the large number of false positives, young people who would die through the intervention itself, without a preventive purpose being served. Thus, false negatives – refusing euthanasia to someone who later dies by suicide – are tragic but allow time, re-evaluation and recovery for those at risk. False positives – granting assisted dying to someone who might have lived – constitute irreversible iatrogenic death. In preventive logic, such asymmetry dictates maximal restraint.
Fragmentation of suicide ethics in psychiatry
An underexamined ethical consequence of framing assisted dying as suicide prevention is that it implicitly creates two categories of suicide within psychiatric practice: one that clinicians are professionally obligated to prevent and another that they are authorised to facilitate. This bifurcation fundamentally destabilises the moral coherence of psychiatry, whose core mission has historically been to respond to suicidal despair with care, containment and accompaniment rather than with the provision of lethal means. Once suicide is reclassified as a legitimate clinical outcome under certain conditions, the distinction between prevention and causation becomes ethically untenable. The profession is then placed in the paradoxical position of both opposing and prescribing death in response to similar expressions of despair.
When prevention becomes collusion
When suicide prevention morphs into medicalised facilitation of death, prevention logic collapses into complicity. The preventive claim – ‘better assisted dying than a violent suicide’ – assumes a causal substitution that cannot be empirically or ethically established. It risks transforming demoralised youth into ‘false positives’ of a system that mistakes despair for autonomy.
From a strictly epidemiological standpoint, that facts are that: (a) suicide remains a rare outcome, even among those requesting assisted dying; (b) predictive accuracy for suicide is low; positive predictive value in youth is <20%; and (c) no evidence exists that assisted dying reduces suicide rates; in any realistic model, around 10 young people die for each suicide theoretically prevented by assisted dying.
Therefore, the argument that youth euthanasia prevents suicide appears to be scientifically unfounded and morally inverted. True suicide prevention lies not in medical facilitation of death but in restoring relational continuity, trauma-informed care and societal inclusion. Compassion without critical reasoning risks becoming cruelty by proxy.
About the author
Jim van Os is Professor of Psychiatric Epidemiology and Public Health at Utrecht University Medical Centre, Utrecht, The Netherlands.
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Funding
This work received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.

 Open access
Open access
eLetters
No eLetters have been published for this article.