


Introduction
Puppets, or the moveable, material representation of human and/or animal characters with materials such as cloth, wood or clay, have been used to entertain children and adults since antiquity. Countries as diverse as Japan, India, Iran and Italy have a history of puppets manipulated with string, rods, hands, and shadows.(Reference Blumenthal1) Presentations can range from the highly professional shows designed to entertain, to educational presentations developed by teachers, librarians, and parents, giving useful information for healthy childhood development.(Reference Abu-Ras, Al-Kubaisi and Idris2–Reference Kröger and Nupponen5) For example, the long-running children’s TV show Sesame Street, popular worldwide, featured two puppets, Bert and Ernie, demonstrating while they had many differences, they could be good friends.(Reference Gikow6,Reference Mares and Pan7)
The combination of puppetry as both theatre, art, and education has the potential to introduce discussion about sensitive topics, social barriers, and uninteresting but important topics that may be difficult with didactic education. Interaction and learning occur organically as observers identify with the different puppets and engage in implicit critical thinking. As an educational tool, puppets have been used around the world to directly and indirectly address a variety of health topics, including oral health in Peru,(Reference Ladera-Castañeda, Córdova-Limaylla and Briceño-Vergel8) adolescent sexuality in India,(Reference Pélicand, Gagnayre and Sandrin-Berthon9,Reference Pattathil and Roy10) suicide prevention in Canadian First Nations, (Reference Jacono and Jacono11) reducing the spread of HIV infection,(Reference Skinner, Metcalf and Seager12) drowning prevention in Spain, (Reference Peixoto-Pino, Barcala-Furelos and Paz-García13) and COVID-19 education with the elderly in China.(Reference Zhu, Liu and Jiang14) Given the wide applicability and acceptability of puppetry and storytelling globally, puppetry based education is uniquely suited to cultural tailoring through the use of local puppeteers, and adaptation of scripts to local languages and cultural norms.(Reference Abu-Ras, Al-Kubaisi and Idris2,Reference Kröger and Nupponen5,Reference Jacono and Jacono11,Reference Skinner, Metcalf and Seager12,Reference Loy and Bautista15–Reference Chandler, Leass, Shegog and Aboul-Enein17)
Nutrition education is an essential cornerstone towards good health. Diets with adequate amounts of protein, complex carbohydrates, fats, and micronutrients can be a challenge to achieve with the bewildering variety of choices available in high-income countries, and the limited selections often available in low-to-middle income countries. Education for all ages provides the basis of the knowledge necessary for a balanced diet. Preschool and school age children can learn about fruits and vegetables, parents can implement strategies for maximising the purchase, preparation and offering of children’s healthy meals and snacks, and adults can learn about local resources. While children may not be responsible for the shopping and preparation of meals, they can be taught about healthy eating, about the importance of eating a variety of foods, and the role of nutrition in maintaining health.
For nutrition educators, cost is often a consideration when considering the development, implementation, and scalability of an intervention. Puppetry may be an attractive medium for educators to engage audiences through, both because of the ease of adoption of puppetry in education, particularly with the use of smaller and less complex puppets and sets, as well as the relatively low cost of implementation.(Reference Blumenthal1–Reference Kröger and Nupponen5)
Puppets hold appeal and attentiveness for both younger and older children, as well as adults given their range of characters from silly, surprising, sophisticated, to mysterious. Thus using them to teach about nutrition makes excellent pedagogical sense. Hand puppets, together with picture books, live demonstrations, and discussions are important strategies for providing children with the basics of nutrition knowledge. The aim of this review was to provide an inclusive description of the nature and extent and the role and application of puppetry interventions in nutrition education and their outcomes and recommendations.
Methods
Selection criteria
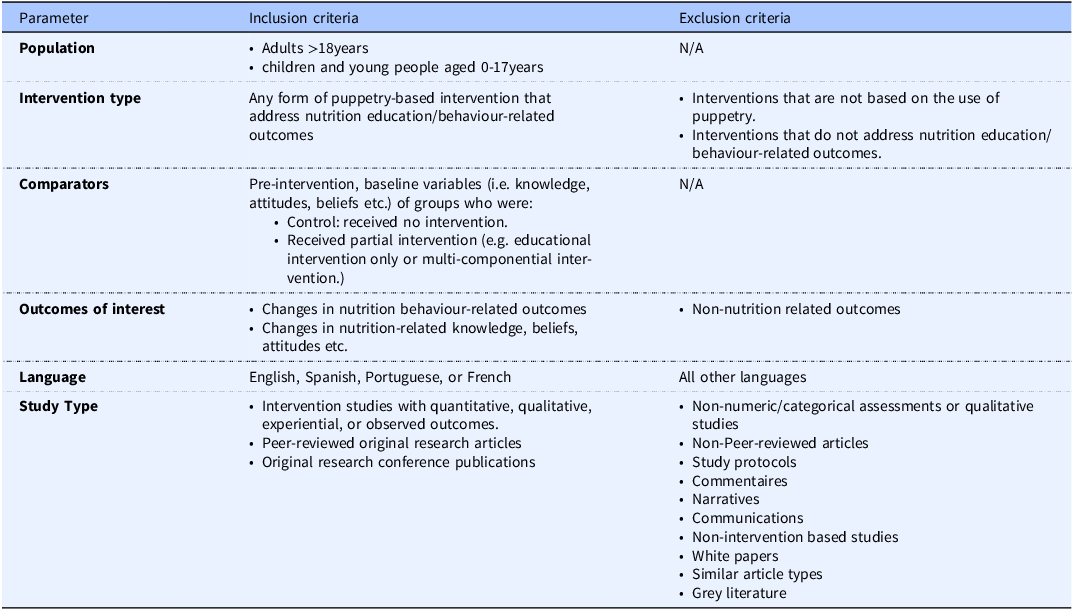
The Population, Intervention, Comparison, Outcomes, and Study (PICOS) design guidelines(Reference Higgins, Thomas and Chandler18) were incorporated to develop the research question: ‘‘Do adults and children populations of all age groups’ (P) that are offered puppetry-based interventions (I) have improved nutrition-related outcomes (O) compared with those that do not participate in puppetry-based interventions(C)?’ and subsequent inclusion and exclusion criteria (see Table 1). Peer-reviewed articles published in the English language were included. Interventions reported outside traditional peer-reviewed articles were excluded in this review. The search was conducted in the summer of 2025, and the results communicate the literature published between 1980 and July 2025, given a robust longitudinal review of the state of puppetry assisted interventions in nutrition education.
PICOS criteria for inclusion and exclusion of studies

Search strategy
This review used the PRISMA-ScR extension for scoping review guidelines; there was no pre-registration or protocol submitted.(Reference Tricco, Lillie and Zarin19) A search was conducted using eight academic databases and a combination of subject heading keywords, terms, phrases, and Boolean operators were used (see Table 2). Search strategies were adapted in accordance with the indexing systems of each respective database used (see supplemental material). Two of the authors [B.A.E. and N.B.] conducted the searches for relevant articles. Author [B.A.E] utilised Rayyan QCRI software(Reference Ouzzani, Hammady and Fedorowicz20) to assist in the screening process. All retrieved articles were screened for relevance to the topic. In addition, reference lists from retrieved articles were also manually searched to identify any additional publications that satisfied the eligibility criteria. Titles and abstracts were screened for relevancy, and potentially relevant journal abstracts were reviewed by two authors [N.B. and B.A.E.]. Potential articles for inclusion in this review were evaluated independently for relevance, merit, and inclusion/exclusion criteria. Articles accepted for inclusion were individually reviewed by each author. Any disagreement was resolved by consensus. Figure 1 provides the PRISMA flowchart leading to selected articles for this review (see Figure 1). We explored the characteristics of interventions, target audiences, and outcomes and tabulated the included studies. Given that methodological quality assessment is not a prerequisite for scoping reviews, we did not appraise the included studies.(Reference Peters, Marnie and Tricco21)
2020 PRISMA scR flow diagram.

Electronic databases used with relevant search period and terms

Results
A total of 25 intervention studies (see Table 3) that met the eligibility criteria was included in this review. The search dates applied were from January 1, 1980 through July 31, 2025, and the reviewed studies were published between 1979,(Reference Bertrand and Bertrand22) and 2025(Reference Abdelrahman, Hashem and Abo-Seif23) with slightly less than half of the publications (n = 10) during the 2010s.(Reference Sharma, Chuang and Hedberg24–Reference Setiana, Handayani and Suminar33) The research studies were conducted in 13 different countries, with six in Indonesia,(Reference Setiana, Handayani and Suminar33–Reference Murdani, Nanda and laili38) seven in the USA,(Reference Sharma, Chuang and Hedberg24,Reference Fitzgibbon, Stolley and Schiffer25,Reference Goodwin, Marsh and Roberts28,Reference Byrd-Bredbenner, Marecic and Bernstein39–Reference Wright, Wylie-Rosett and Lukoscheck42) two in the Netherlands,(Reference Bevelander, Engels and Anschütz26,Reference de Droog, van Nee and Govers29) and one in each of the following countries – Brazil, India, Colombia, the Philippines, Bolivia, Spain, France, Egypt, and Ecuador.(Reference Pélicand, Gagnayre and Sandrin-Berthon9,Reference Bertrand and Bertrand22,Reference Abdelrahman, Hashem and Abo-Seif23,Reference Alessi, Yassin and Leite27,Reference Romo and Abril-Ulloa30–Reference Martinez, Johannsen and Gertner32,Reference Arora, Kumar and Deep43,Reference Perez-Rodrigo and Aranceta44)
Summary of literature search (N = 25)

BMI, Body mass index; PA, physical activity; RCT, randomised control trial.
Sample sizes and participant characteristics
The target populations varied and included different age groups. Most interventions (n = 19) were aimed at preschool and school-aged children.(Reference Abdelrahman, Hashem and Abo-Seif23–Reference Goodwin, Marsh and Roberts28,Reference Glorioso, Narciso and Avilla31,Reference Setiana, Handayani and Suminar33,Reference Permanasari, Khoirahman and Utami35–Reference Kumbhar45) Other studies concentrated on specific subgroups, including toddlers,(Reference Alessi, Yassin and Leite27,Reference de Droog, van Nee and Govers29) diabetic children,(Reference Pélicand, Gagnayre and Sandrin-Berthon9) adolescents,(Reference Glorioso, Narciso and Avilla31) mothers of stunted children,(Reference Darawati, Yunianto and Sulendri36) of children with stunting (short height for age), preschool teachers,(Reference Usfar, Budiman and Lan34) pregnant women,(Reference Martinez, Johannsen and Gertner32) and women of reproductive age.(Reference Bertrand and Bertrand22) Sample sizes varied widely, ranging from small pilot studies (e.g., n = 12, n = 14) to larger trials (e.g., n = 2000 households, n = 1857 students).
Type of studies and details intervention
The systematic review includes various study designs that assess interventions. Most of the studies (n = 15) were quasi-experimental pre–post interventions.(Reference Bertrand and Bertrand22,Reference Abdelrahman, Hashem and Abo-Seif23,Reference Goodwin, Marsh and Roberts28–Reference Glorioso, Narciso and Avilla31,Reference Setiana, Handayani and Suminar33,Reference Permanasari, Khoirahman and Utami35–Reference Byrd-Bredbenner, Marecic and Bernstein39,Reference Wright, Wylie-Rosett and Lukoscheck42,Reference Arora, Kumar and Deep43,Reference Kumbhar45) The review included several randomised controlled trials,(Reference Bevelander, Engels and Anschütz26,Reference Martinez, Johannsen and Gertner32,Reference Fitzgibbon, Stolley and Schiffer40,Reference Nicklas, Lopez and Liu41) multiple pilot studies,(Reference Sharma, Chuang and Hedberg24,Reference Fitzgibbon, Stolley and Schiffer25,Reference Usfar, Budiman and Lan34,Reference Perez-Rodrigo and Aranceta44) and one mixed-methods study.(Reference Alessi, Yassin and Leite27)
Overall, the interventions employed in the included studies differed in their delivery, duration, and specific components. The length of interventions in the review had a wide range, from a single brief exposure to programmes with puppet content to those that spanned several years. The shortest interventions included a single lesson(Reference Bevelander, Engels and Anschütz26,Reference Wright, Wylie-Rosett and Lukoscheck42,Reference Kumbhar45) and a 5-minute video.(Reference Glorioso, Narciso and Avilla31) Others had content that lasted for several days or weeks. Common durations were 6 weeks(Reference Sharma, Chuang and Hedberg24,Reference Goodwin, Marsh and Roberts28,Reference Byrd-Bredbenner, Marecic and Bernstein39) and 14 weeks.(Reference Fitzgibbon, Stolley and Schiffer25,Reference Fitzgibbon, Stolley and Schiffer40) Some studies carried out interventions over several months, such as 3–7 months,(Reference Romo and Abril-Ulloa30) 8 months,(Reference Bertrand and Bertrand22) and monthly visits.(Reference Martinez, Johannsen and Gertner32) The longest intervention reported lasted one year.(Reference Perez-Rodrigo and Aranceta44) A few studies gave the number of sessions instead of a timeframe, noting three sessions,(Reference Permanasari, Khoirahman and Utami35) four sessions,(Reference Anggraini, Nisa and Hasina37) and a summer camp format.(Reference Pélicand, Gagnayre and Sandrin-Berthon9)
The use of puppetry was diverse and was done in various ways across studies, such as hand puppets for nutrition lessons,(Reference Fitzgibbon, Stolley and Schiffer25,Reference Fitzgibbon, Stolley and Schiffer40) finger puppets for storytelling,(Reference Setiana, Handayani and Suminar33,Reference Permanasari, Khoirahman and Utami35) puppet theatre,(Reference Alessi, Yassin and Leite27) puppet videos,(Reference Glorioso, Narciso and Avilla31) and as a tool in nutrition or therapeutic counselling.(Reference Pélicand, Gagnayre and Sandrin-Berthon9,Reference Darawati, Yunianto and Sulendri36) Interventions were held in various settings, including schools,(Reference Bevelander, Engels and Anschütz26,Reference Alessi, Yassin and Leite27,Reference Byrd-Bredbenner, Marecic and Bernstein39,Reference Arora, Kumar and Deep43,Reference Perez-Rodrigo and Aranceta44) community centres,(Reference Bertrand and Bertrand22) summer camps,(Reference Pélicand, Gagnayre and Sandrin-Berthon9) and household.(Reference Martinez, Johannsen and Gertner32) Many studies combined puppet-based education with other strategies, such as physical activity,(Reference Romo and Abril-Ulloa30,Reference Fitzgibbon, Stolley and Schiffer40) cooking workshops,(Reference Perez-Rodrigo and Aranceta44) parent education,(Reference Sharma, Chuang and Hedberg24,Reference Fitzgibbon, Stolley and Schiffer25) and environmental changes like menu modifications.(Reference Perez-Rodrigo and Aranceta44)
Measured parameters
The parameters measured in the systematic review are varied. They included outcomes based only on knowledge,(Reference Glorioso, Narciso and Avilla31,Reference Setiana, Handayani and Suminar33–Reference Permanasari, Khoirahman and Utami35,Reference Arora, Kumar and Deep43) assessments that combined knowledge, attitude, and behaviour,(Reference Pélicand, Gagnayre and Sandrin-Berthon9,Reference Bertrand and Bertrand22,Reference Martinez, Johannsen and Gertner32, Reference Byrd-Bredbenner, Marecic and Bernstein39, Reference Perez-Rodrigo and Aranceta44) and specific dietary and consumption measures.(Reference Sharma, Chuang and Hedberg24,Reference Bevelander, Engels and Anschütz26–Reference de Droog, van Nee and Govers29,Reference Anggraini, Nisa and Hasina37) Some studies focused on anthropometric and health outcomes, including body mass index (BMI), physical activity, and dietary intake details.(Reference Fitzgibbon, Stolley and Schiffer25,Reference Romo and Abril-Ulloa30,Reference Fitzgibbon, Stolley and Schiffer40) Other studies evaluated metrics related to caregivers, such as maternal knowledge, feeding practices, and household nutrient intake.(Reference Martinez, Johannsen and Gertner32,Reference Darawati, Yunianto and Sulendri36)
Knowledge and psychosocial outcomes
The most consistent positive findings appeared in studies measuring knowledge gain and psychosocial involvement. Multiple studies showed significant improvements in nutrition knowledge after puppet-based interventions.(Reference Abdelrahman, Hashem and Abo-Seif23,Reference Glorioso, Narciso and Avilla31,Reference Setiana, Handayani and Suminar33,Reference Permanasari, Khoirahman and Utami35,Reference Darawati, Yunianto and Sulendri36,Reference Wright, Wylie-Rosett and Lukoscheck42–Reference Kumbhar45) Additionally, Pélicand et al. (Reference Pélicand, Gagnayre and Sandrin-Berthon9) found that puppets helped children with diabetes express emotions better and develop more positive attitudes. Byrd-Bredbenner et al. (Reference Byrd-Bredbenner, Marecic and Bernstein39) noted modest improvements in specific food attitudes. On the other hand, some studies did not find any significant change in knowledge,(Reference Bertrand and Bertrand22,Reference Goodwin, Marsh and Roberts28,Reference Byrd-Bredbenner, Marecic and Bernstein39) indicating that knowledge gains are not guaranteed and might rely on other factors in implementation such as peer attitudes.
Behavioural and dietary outcomes
The results for actual behaviour and dietary intake showed more variation with several studies reporting positive results. For instance, Romo and Abril-Ulloa(Reference Romo and Abril-Ulloa30) found a significant reduction in the consumption of sugar-sweetened beverages and a reduction in screen time. Darawati et al. (Reference Darawati, Yunianto and Sulendri36) noted better nutrient intake among mothers, and three studies observed increased fruit and vegetable consumption in children.(Reference Anggraini, Nisa and Hasina37,Reference Murdani, Nanda and laili38,Reference Nicklas, Lopez and Liu41) Alessi et al. (Reference Alessi, Yassin and Leite27) also reported greater acceptance of functional foods. However, other studies found no significant changes in dietary intake,(Reference Sharma, Chuang and Hedberg24,Reference Fitzgibbon, Stolley and Schiffer40) vegetable consumption,(Reference de Droog, van Nee and Govers29) or candy consumption.(Reference Bevelander, Engels and Anschütz26) Goodwin et al. (Reference Goodwin, Marsh and Roberts28) showed a notable decrease in the calories selected by children but no change in macronutrient composition or their ability to identify high-fibre foods.
Anthropometric and health outcomes
Evidence for the impact on physical health measures was inconsistent. Fitzgibbon et al. (Reference Fitzgibbon, Stolley and Schiffer25) found a significant difference in BMI changes between groups. This result was backed by Romo and Abril-Ulloa,(Reference Romo and Abril-Ulloa30) who reported significant improvements in BMI-for-age. In contrast, other studies found no significant effects on BMI,(Reference Fitzgibbon, Stolley and Schiffer40) anthropometry, or anaemia rates.(Reference Martinez, Johannsen and Gertner32)
Main recommendations from included studies
The main recommendations from the studies highlighted the need for careful evaluation of health education programmes.(Reference Bertrand and Bertrand22) They also stressed the importance of developing engaging materials that are suitable for different age groups.(Reference Anggraini, Nisa and Hasina37,Reference Byrd-Bredbenner, Marecic and Bernstein39,Reference Arora, Kumar and Deep43) Interdisciplinary collaboration across different settings, especially between schools and parents, was indicated as crucial.(Reference Setiana, Handayani and Suminar33,Reference Perez-Rodrigo and Aranceta44) Several studies recommended using puppets as an effective tool in both therapeutic and educational environments.(Reference Pélicand, Gagnayre and Sandrin-Berthon9,Reference Permanasari, Khoirahman and Utami35,Reference Darawati, Yunianto and Sulendri36) A recurring theme is the need for culturally tailored family-centred interventions.(Reference Fitzgibbon, Stolley and Schiffer25,Reference Fitzgibbon, Stolley and Schiffer40) Additional suggestions included incorporating specific topics into school curricula(Reference Glorioso, Narciso and Avilla31) and menus,(Reference Alessi, Yassin and Leite27) and designing programmes that consider strong social influences, like peer modelling.(Reference Bevelander, Engels and Anschütz26) In terms of research, recommendations indicated a focus on long-term effectiveness, sustainability, and cost-effectiveness were proposed.(Reference Sharma, Chuang and Hedberg24,Reference Romo and Abril-Ulloa30,Reference Martinez, Johannsen and Gertner32)
Discussion
The existing body of nutrition education programmes incorporating puppetry remains limited, with only 25 evaluated interventions over nearly 45 years identified for the purposes of this scoping review. Nonetheless, these studies span 13 countries, multiple age groups, and a range of settings, indicating that puppetry has been applied across diverse educational, nutrition-focused and cultural contexts. Across the studies, puppetry-based interventions most consistently improved nutrition knowledge,(Reference Abdelrahman, Hashem and Abo-Seif23,Reference Setiana, Handayani and Suminar33–Reference Darawati, Yunianto and Sulendri36,Reference Wright, Wylie-Rosett and Lukoscheck42–Reference Kumbhar45) however, several studies did not detect significant knowledge gains.(Reference Bertrand and Bertrand22,Reference Martinez, Johannsen and Gertner32,Reference Byrd-Bredbenner, Marecic and Bernstein39) Pélicand et al. (Reference Pélicand, Gagnayre and Sandrin-Berthon9) used puppets to facilitate emotional expression among children with diabetes, highlighting how puppetry can support psychosocial skills alongside content learning. The overall heterogeneity in design and measurement means that improvements in knowledge are promising but not yet definitive.
Behavioural, anthropometric, and dietary outcomes were more mixed. Several studies found intervention impacts on anthropometrics,(Reference Fitzgibbon, Stolley and Schiffer25,Reference Romo and Abril-Ulloa30) fruit and vegetable intake,(Reference Anggraini, Nisa and Hasina37,Reference Murdani, Nanda and laili38,Reference Nicklas, Lopez and Liu41) acceptance of functional foods,(Reference Alessi, Yassin and Leite27) and improvements in macronutrient intake,(Reference Goodwin, Marsh and Roberts28) while others did not have comparable findings on similar metrics such as BMI and weight,(Reference Fitzgibbon, Stolley and Schiffer25,Reference Bevelander, Engels and Anschütz26) and dietary intake.(Reference Sharma, Chuang and Hedberg24,Reference de Droog, van Nee and Govers29) While these findings align with broader evidence that multifaceted nutrition education and physical activity interventions can influence weight trajectories,(Reference Zhou, Ren and Yin46–Reference Kihm49) some of the reviewed puppet-based interventions were not powered or designed to detect long-term anthropometric effects.(Reference Fitzgibbon, Stolley and Schiffer25,Reference Romo and Abril-Ulloa30,Reference Martinez, Johannsen and Gertner32,Reference Fitzgibbon, Stolley and Schiffer40)
A key theme across puppetry-based interventions included in this review is the importance of active engagement and the applications of social learning. Interventions that include experiential components such as taste testing, role-play, or interacting with characters appear particularly effective. Both puppetry-based educational videos and live shows improved knowledge or nutrient intake through framing abstract health messages and concepts in ways that the audience found relatable and emotionally resonant.(Reference Pélicand, Gagnayre and Sandrin-Berthon9,Reference Abdelrahman, Hashem and Abo-Seif23,Reference Sharma, Chuang and Hedberg24,Reference Alessi, Yassin and Leite27,Reference Glorioso, Narciso and Avilla31,Reference Darawati, Yunianto and Sulendri36,Reference Anggraini, Nisa and Hasina37,Reference Nicklas, Lopez and Liu41,Reference Arora, Kumar and Deep43,Reference Kumbhar45) However, few studies reported specifically how puppet characters were developed, scripted, or adapted to reflect participants’ culture, identities, languages, or social environments,(Reference Sharma, Chuang and Hedberg24,Reference Alessi, Yassin and Leite27,Reference de Droog, van Nee and Govers29,Reference Romo and Abril-Ulloa30–Reference Permanasari, Khoirahman and Utami35,Reference Anggraini, Nisa and Hasina37,Reference Murdani, Nanda and laili38,Reference Kumbhar45) even though arts-based health literature suggests that culturally grounded characters and narratives can strengthen identification and message relevance.(Reference Abu-Ras, Al-Kubaisi and Idris2–Reference Kröger and Nupponen5,Reference Jacono and Jacono11,Reference Skinner, Metcalf and Seager12,Reference Chandler, Leass, Shegog and Aboul-Enein17,Reference Darawati, Yunianto and Sulendri36) Incorporation of additional methodological information in future interventions on puppet type, character design, and scripting decisions would help further elucidate how these elements influence both audience engagement and intended intervention outcomes.
Another educational approach across the studies reviewed is the frequent use of puppetry to introduce or reinforce nutrition information or nutrition related behaviour combined with other multi-component aspects in support of the intervention (such as teacher- or parent-led activities, take-home materials, or environmental modifications) intended to support behaviour change.(Reference Abdelrahman, Hashem and Abo-Seif23–Reference Fitzgibbon, Stolley and Schiffer25,Reference Alessi, Yassin and Leite27,Reference Romo and Abril-Ulloa30,Reference Martinez, Johannsen and Gertner32,Reference Usfar, Budiman and Lan34,Reference Darawati, Yunianto and Sulendri36–Reference Murdani, Nanda and laili38,Reference Nicklas, Lopez and Liu41,Reference Perez-Rodrigo and Aranceta44) This aligns with broader behaviour-change models that emphasise layering information, skills practice, social support, and structural changes to influence diet-related behaviours.(Reference Rinderknecht and Smith50–Reference Browne, Minozzi and Bellisario54) Within this framework, puppetry-based interventions may be particularly well suited for capturing attention and engaging the audience, modelling dialogue about complex topics and concepts, and lowering barriers to participation across diverse audiences and participant age groups; however, additional intervention components are needed to sustain and translate outcomes from puppetry-based interventions into everyday food choices.
The review highlights important gaps in the current evidence base. First, there is limited use of standardised, validated measures of dietary intake, psychosocial constructs, and anthropometric outcomes, which complicates cross-study comparison. Second, most interventions in this review assessed outcomes immediately or shortly after the puppetry-based intervention, with relatively few studies incorporating longer-term follow-up. Therefore, it remains uncertain whether observed gains in knowledge or short-term changes in diet-related behaviour are sustained over time. Third, almost none of the included interventions utilised a control group or explicitly compared different puppet formats, story styles, or degrees of audience participation, even though emerging applied-puppetry and arts-based health research suggests that these design choices may influence engagement and effectiveness
Future research should therefore prioritise more rigorous study designs, including randomised or well-controlled quasi-experimental trials; transparent methodological designs describing puppet design, script development, and intervention implementation processes; and incorporation of longer follow-up timeframes to capture maintenance of behaviour change. Studies that explicitly test puppetry as a standalone component as compared to puppetry-based interventions that are developed in combination with other educational strategies would help to determine whether puppets primarily act as a tool to capture the interest of and engage the audience, or whether puppetry can be utilised in nutrition education intervention settings to facilitate positive impacts on nutrition- and health-related knowledge, attitude, and behaviour outcomes.
Finally, this review underscores the potential for puppetry-based nutrition education to be integrated into broader health promotion and disease prevention programmes. Existing evidence from related fields, including oral health, sexual health, general health behaviours, and mental health promotion, suggests that puppets can facilitate dialogue, enhance recall of key messages, and support emotional processing among children and adults.(Reference Abu-Ras, Al-Kubaisi and Idris2,Reference Ladera-Castañeda, Córdova-Limaylla and Briceño-Vergel8,Reference Chandler, Leass, Shegog and Aboul-Enein17,Reference Alosail, Alwadi and Alroweilly55,Reference Synovitz56) Leveraging these constructs within well-designed, theoretically-based, and culturally tailored nutrition interventions may contribute to creatively addressing challenges in engaging diverse populations and translating nutrition knowledge into sustainable dietary change.
Conclusion
This scoping review identified 25 nutrition education interventions that incorporated puppetry over nearly 45 years, indicating both a long-standing interest in utilising puppetry as an educational approach, and a relatively small, fragmented evidence base. Overall, the studies suggest that puppetry-based interventions support gains in nutrition knowledge and psychosocial engagement, whereas evidence for consistent effects on dietary behaviour and anthropometric outcomes remains limited and mixed. Puppet-based activities were typically implemented as part of multi-component interventions delivered to a wide range of populations and settings; while this approach reflects practical realities, it also complicates attribution of effects specifically to the use of puppetry in the intervention setting. There is a clear need for methodologically robust research studies that utilise standardised outcome measures, include longer follow-up time frames, and systematically report and provide assessment and evaluation on decisions about puppet type, character design, script development, cultural tailoring, and degree of audience participation. Such work would clarify when, for whom, and under what conditions puppetry-based nutrition interventions add unique value in improving nutrition knowledge as well as anthropometrics and dietary behaviour. Given the demonstrated ability to engage participants and to open dialogue around health topics in other domains, puppetry-based interventions remain a promising strategy to implement in nutrition education initiatives.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/jns.2026.10102.
Data availability statement
All data generated and analysed during this review are included in the published review article.
Acknowledgements
None.
Author contributions
BHA-E: Writing – review & editing, Writing – original draft, Visualisation, Validation, Supervision, Project administration, Methodology, Investigation, Conceptualisation.
NB: Writing – review & editing, Writing – original draft, Formal analysis, Data curation, Visualisation, Validation.
MJ: Writing – review & editing, Writing – original draft, Formal analysis, Data curation, Visualisation, Validation.
SAA: Writing – review & editing, Writing – original draft, Formal analysis, Data curation, Visualisation, Validation.
PJK: Writing – review & editing, Writing – original draft, Formal analysis, Visualisation, Validation, Methodology.
SG: Writing – review & editing.
ED: Writing – review & editing, Writing – original draft, Formal analysis, Validation, Methodology.
Financial support
The authors received no financial support for the research, authorship, and/or publication of this article.
Competing interests
There was no declaration of interests.
Ethical statement
No ethical oversight was found to be necessary for this review and, therefore, no institutional review board was obtained.






 Open access
Open access