


Highlights
-
• Unique program: The OEGTP standardized testing criteria, panel gene curation and testing protocols.
-
• Diagnostic success: A 20.8% yield in 983 individuals was achieved with next-generation sequencing over 2 years.
-
• Clinical impact: Post-test outcomes emphasized clinical benefits of genetic testing in epilepsy, fostering provider engagement and genetics literacy province wide.
Introduction
Epilepsy is a chronic neurological disorder characterized by recurrent seizures, affecting approximately 75 000 adults and 15 000 children in the province of Ontario, Canada.Reference Bowen, Snead, Chandra, Blackhouse and Goeree1,Reference Ng, Maxwell and Yates2 The cause of epilepsy is heterogeneous though genetics plays a significant role, especially in those with an early age of onset, a positive family history or associated co-morbidities.Reference Myers, Johnstone and Dyment3 Accurate genetic diagnosis can direct treatment, better inform prognosis, limit further investigations and interventions and improve surveillance measures.Reference Myers and Mefford4,Reference Demos, Guella and DeGuzman5 A genetic diagnosis will also inform and enable accurate genetic counseling, provide prenatal testing options and psychosocial benefits to the individual and their families.Reference Vears, Dunn, Wake and Scheffer6 Given these significant impacts on both the individuals, families and the healthcare system, accessing timely and accurate genetic services remains of importance in improving the diagnostic process in epilepsy.
Next-generation sequencing (NGS) technologies have transformed genetic testing in epilepsy clinics by enabling high-throughput, cost-effective and high-precision analysis of multiple gene panels with approximately 15%–20% diagnostic yield.Reference Sheidley, Malinowski and Bergner7–Reference Lee, Karp and Zapata-Aldana10 In addition to diagnostic yield, a broader health system impact of NGS testing needs to be considered. While there have been considerable efforts toward a standardized curation of epilepsy-related genes,Reference Helbig, Riggs and Barry11 no clear information exists regardingthe optimal implementation of multigene panels in specific healthcare settings.
To better understand the regional landscape of multigene panel testing in epilepsy in a publicly funded provincial system, the Ontario Ministry of Health and Long-Term Care (MOHLTC) Laboratories and Genetics Branch established the Ontario Epilepsy Genetic Testing Program (OEGTP) in 2020.Reference Dyment, Prasad and Boycott12,Reference Jain, Andrade and Donner13 The program oversees multigene panel testing for epilepsy in the province, which is performed by a single reference laboratory funded by the MOHLTC (London Health Sciences Centre [LHSC] Molecular Genetics Laboratory) for epilepsy genetic testing in the province and is managed by a steering committee with wide representation from across the province that includes regulatory, clinical and laboratory stakeholders. This work summarizes the results from the initial two years (2020–2022) of the OEGTP in a cohort of over 1000 epilepsy patients tested through the province of Ontario. In addition to the diagnostic yield, we describe the various health system impact measures based on the systematic collection and review of pre- and post-test health and patient management information. Overall, the study underscores the importance of integrating genomics into epilepsy care, while highlighting the unique potential of the first of its kind OEGTP model to gather health system evidence for optimization of genomic diagnostic pathways in the care of patients with epilepsy.
Materials and methods
OEGTP – makeup and mandate of steering committee
The OEGTP steering committee comprises of two geneticists, one genetic counselor, two epileptologists (neurologists with specialized epilepsy training), three molecular geneticists, two molecular technologists and one MOHLTC representative and is co-chaired by a diagnostic laboratory specialist and a clinical specialist involved in care of patients with epilepsy (i.e., epileptologist, neurologist, geneticist). The clinicians and laboratory scientists are from five separate academic health sciences centers in Ontario (in London, Ottawa, Toronto, Kingston, Hamilton), ensuring representation from almost all mid- to large-sized healthcare facilities with epilepsy treatment programs in the province. The committee met quarterly in the first year of implementation and has been meeting at least annually thereafter to perform its mandate.
The committee coordinates the ongoing curation of the multigene panels and active optimization of testing requirements based on updated evidence from literature, as well as feedback from the end-users. Its mandate also covers management of optimal access to testing by ensuring genetics literacy in ordering providers, promoting awareness of epilepsy genetics among healthcare professionals and delivering evidence-based guidelines for the streamlined use of NGS technologies in epilepsy.
OEGTP – design of epilepsy panels
The initial creation of evidence-based epilepsy gene panels for appropriately selected epilepsy patients was guided by the recommendations of a working group appointed by the Genetic Testing Advisory Committee, which had a mandate to review the clinical utility and validity of genetic tests and provide advice to the MOHLTC on the provision of genetic testing in Ontario.Reference Jain, Andrade and Donner13 Using the principles outlined by the National Institutes of Health funded ClinGen resource (https://www.clinicalgenome.org), more specifically the ClinGen Epilepsy Gene Curation Expert Panel’s guidance,Reference Helbig, Riggs and Barry11 the working group developed a “made in Ontario” tailored set of gene panels for epilepsy testing in a way that maximizes clinical validity (appropriateness) and actionability (benefit), by defining and determining parameters.Reference Dyment, Prasad and Boycott12
The first iteration of NGS panel options encompassed the following categories: (1) focal epilepsy (14 genes), (2) progressive myoclonic (20 genes), (3) early infantile epileptic encephalopathy (51 genes), (4) childhood-onset (45 genes), (5) brain malformation (44 genes), (6) actionable (22 genes) and (7) comprehensive panel (167 genes) (https://www.lhsc.on.ca/pathology-and-laboratory-medicine/ontario-epilepsy-genetic-testing-program). The panel content was reviewed and curated on a periodic basis by the steering committee. All genetic testing services were conducted at the provincial reference laboratory within the of Molecular Diagnostics Program, Verspeeten Clinical Genome Centre, Department of Pathology and Laboratory Medicine at LHSC in London, Ontario.
OEGTP – testing and ordering eligibility criteria in Ontario, Canada
Clinical eligibility criteria for epilepsy genetic testing in Ontario had been previously described by the Genetic Testing Advisory Committee.Reference Jain, Andrade and Donner13 The ordering providers included a board-certified medical geneticist, or epileptologist, or a neurologist with at least 6 months of training in epilepsy. Additional specialties were considered with a requirement for completing the “Project ECHO Ontario, Epilepsy Across the Life Span” educational course. This program was delivered by a team of adult and pediatric epileptologists, geneticists and genetic counselor and laboratory specialists and included didactic sessions on the clinical criteria for genetic testing, pre- and post-test counseling and epilepsy gene panel selection. The program was based on the original hub-and-spoke model created for management of hepatitis C in New Mexico and incorporates a case-based learning program to improve engagement and access to care, called “Extension for Community Healthcare Outcomes” (ECHO).Reference Arora, Thornton and Murata14
Patient recruitment and testing process
Samples recruited from October 2020 to November 2022 from patients meeting the eligibility criteria for genetic testingReference Jain, Andrade and Donner13 were included in this study. The cohort included both pediatric and adult patients with epilepsy, from the neurology or genetics clinics of tertiary care/academic health centers, community hospitals and other neurology or primary care practices across Ontario, ordered by practitioners fulfilling the above criteria. The OEGTP NGS panel testing required adherence to specific clinical criteria to ensure that all referred patients exhibited clinical indications of suspected genetic forms of epilepsy. Physicians were asked to complete a questionnaire confirming that the age of onset, seizure type and electroclinical syndrome aligned with the criteria for genetic epilepsy diagnosis (Epilepsy Test Questionnaire in Supplementary Material 1). The requisition form included a selection of seven distinct NGS panels to be chosen based on clinical indication following recommendations from the OEGTP. Additionally, physicians were required to complete a post-test questionnaire (Management Impact form) to assess the clinical implications of the genetic testing results (Management Impact Form in Supplementary Material 1). The laboratory periodically recontacted the providers for pending forms to improve the response rate.
Specimens were received in the form of either extracted DNA or underwent DNA isolation from peripheral blood at the Molecular Genetics Laboratory (LHSC) using standard protocols using the MagNA Pure system (Roche Diagnostics, Laval, QC, Canada). Subsequently, DNA quantification was carried out by measuring absorbance with a DTX 880 Multimode Detector (Beckman Coulter, Brea, CA, USA).
NGS targeted panel testing
Gene sequencing was performed using a custom, in-house designed NGS panel protocol.Reference Kerkhof, Rastin, Schenkel, Lin and Sadikovic15 Sequence capture probes were designed for KAPA HyperCap target enrichment encompassing 167 genes linked to epilepsy (Roche Sequencing Solutions, Inc., Santa Clara, CA, USA). These probes were designed to provide full coverage of all targeted coding regions, along with 20 bp of the 5’ and 3’ flanking intronic regions and untranslated regions (UTRs). Additionally, 100 bp surrounding the 24 Single Nucleotide Polymorphism (SNP) targets of the Agena iPLEX Pro Exome QC panel were included in the design. The detailed gene content of the epilepsy NGS panels is described in Supplemental Table 1 (in Supplementary Material 2). Library preparation was carried out using KAPA HyperChoice Chemistry (KAPA HyperCap Workflow v3, Roche Sequencing Solutions, Inc.), followed by sequencing on either NextSeq 550 or MiSeq instruments (Illumina, San Diego, CA, USA), in accordance with standard protocols. Sequencing was performed with a mean 200× coverage in order to enable accurate sequence variant, copy number variant (CNV) and mosaicism detection.
NGS alignment, variant identification and sample fidelity
Sequence alignment and coverage distribution were performed using NextGene software version 2.4.2.3 (SoftGenetics, LLC., State College, PA, USA) with standard alignment settings, as previously described.Reference Schenkel, Kerkhof and Stuart16 Variants were filtered at a 10% allelic fraction threshold. Subsequently, BAM and VCF files were imported into Geneticist Assistant version 1.8.1 (SoftGenetics, LLC) for databasing and variant quality assessment, focusing on read depth, allelic fraction and read balance.
CNV calling was performed using an in-house developed methodology involving quantile normalization of the read depth as previously described,Reference Schenkel, Kerkhof and Stuart16,Reference Kerkhof, Schenkel and Reilly17 with the following modifications: Read depth reports were generated with DNAcopy and exomeCopy R (v3.5.1) packages before normalization. The normalization results were binned by 10 bp and segmented to merge neighboring bins within an average normalized value of 0.1. Segments with ratio thresholds exceeding 1.35 (for duplications) or falling below 0.65 (for deletions) were flagged for manual review. Regions potentially affected by homologous sequence interference were subjected to more stringent ratio thresholds for review (greater than 1.15 for duplications or less than 0.85 for deletions).
The NGS targeted panels also encompass coverage for the 21 SNPs and 3 sex markers of the Agena iPLEX Pro Exome QC panel to evaluate sample fidelity. The Agena panel is processed on each stock DNA specimen according to the manufacturer’s recommendations and in parallel with the KAPA HyperCap workflow. The results of both assessments are compared to ensure expected sex and SNP matching as part of the sample fidelity evaluation.
Targeted testing for familial variants
The familial variant testing was conducted using either Sanger sequencing for sequence variants or multiplex ligation-dependent probe amplification (MLPA) for CNVs in duplicate, following standard laboratory protocols. The proband’s DNA was used as a positive control. In instances where a commercial MLPA kit was unavailable or more than three familial variants needed investigation simultaneously, targeted NGS was carried out as described above, with all non-familial variants filtered out.
Variant interpretation and diagnostic yield assessment
Variants were interpreted by a certified molecular geneticist in accordance with American College of Medical Genetics (ACMG) guidelines.Reference Richards, Aziz and Bale18 Variants classified as pathogenic (P), likely pathogenic (LP) or variants of unknown significance (VUS) were included in the reports.
For the proband results, findings were categorized into four main groups: (i) molecular diagnosis, (ii) possible molecular diagnosis, (iii) uncertain or (iv) negative. A molecular diagnosis was established by the presence of one (for autosomal dominant [AD]) or two (for autosomal recessive [AR]) P/LP variants within a single gene or following the confirmation of a de novo VUS variant in a clinically related AD gene. A possible diagnosis was categorized by the presence of two VUS in an AR gene or a single P/LP variant in a clinically relevant AR gene or following the confirmation of a VUS to be de novo variant in an AR gene. Both sequence and CNVs are routinely and simultaneously reported. Cis versus trans status of multiple variants in the same gene was not available to report based on proband-only testing but was available if follow-up familial testing was performed. Similarly, presumed de novo status could be ascertained through parental testing using Sanger, MLPA or NGS, depending on the specific variant under investigation. Paternity was not confirmed during familial testing during the period of the reported cohort, but this capability was later added to the process based on the suggestions by the steering committee. An uncertain result encompassed any other VUS, while a negative result indicated the absence of reportable variants or a single reported VUS in an AR gene.
OEGTP database
The results from the OEGTP database for NGS testing, follow-up familial test results and pre- and post-test questionnaire responses were stored in an internally curated database at LHSC for further analysis and reference.
Statistical analysis
The standard chi-square test of independence was employed to evaluate the association between the reported diagnostic results in the post-test questionnaires and variables available from the data included in the test requisition. The complete list of features included in the pre-test questionnaires/requisitions can be found in Supplementary Material 1.
Results
During the period from October 2020 to November 2022, a total of 1254 tests were conducted. Among these, 996 probands, representing 983 unique cases, were referred for testing using the NGS panel (Figure 1). Additionally, 258 samples in 133 distinct families were referred for targeted testing of a known variant. Clinicians provided responses to 571 completed post-test questionnaires for NGS probands, a response rate of 58.1% for unique cases (excluding add-on testing).
Schematic of samples in Ontario Epilepsy Genetic Testing Program (OEGTP) database from October 2020 to November 2022. In total, there were 1254 patients tested (1241 unique cases). 996 probands were tested by next-generation sequencing, and 258 familial samples were reported. 13 next-generation sequencing (NGS) cases were “add ons” meaning that after a sample was reported with the requested targeted subpanel as negative, an additional requisition was received requesting an expanded panel be reported. 571 post-test questionnaires were received following the reporting of results.

Patient information and NGS panel results
Data from the requisitions revealed that the most referred seizure type was focal, followed by generalized seizures (Figure 2A). The predominant age of onset was between 1 and 16 years of age (n = 606, 61.3%, Figure 2B). The Comprehensive Epilepsy panel, encompassing 167 genes, was the most frequently requested panel (n = 674), accounting for 67.7% of all NGS requests (Figure 3). Additionally, targeted subpanels such as focal epilepsy (n = 36, 3.6% of tests), progressive myoclonic (n = 13, 1.3%), early infantile (n = 57, 5.7%), childhood-onset (n = 76, 7.6%), brain malformation (n-42, 4.2%) and actionable (n = 15, 1.5%) were utilized, along with custom requests involving any combination of panels or genes (n = 83, 8.3%).
Clinical and demographic information of reported next-generation sequencing probands. (A) Type of seizure and (B) age of seizure onset as reported by the Ontario Epilepsy Genetic Testing Program pre-test questionnaire, available in Supplementary Material 1.

Next-generation sequencing (NGS) test distribution by subpanel of all NGS samples. 996 NGS tests were reported (983 unique cases and 13 samples that received an additional, expanded “add-on”’ report following a negative result from a smaller subpanel at the request of a clinician). The majority (67.7%) of requests are for the epilepsy comprehensive panel.

In this cohort, a total of 1626 variants were identified as P/LP/VUS, including 212 P/LP variants reported (13% of all variants), and a comparable frequency of missense, frameshift and nonsense variants was observed (Figure 4B). Notably, 16% of the reportable P/LP variants were CNVs, encompassing sub-exonic, exon-level or gene-level deletion/duplications (Table 1). A list of CNVs detected is provided in Table 1, and a visualization of some examples is shown Figure 5. VUS were reported in 1414 of 1626 of all variants (87%; Figure 4A).
Variants detected by next-generation sequencing (NGS) panel. (A) 1626 total variants were reported by NGS testing (n = 996 reports), with the majority of them being classified as variants of unknown significance (VUS). Note that “add-on”cases where the same variant was included in the original and updated request were only counted once. (B) A breakdown of the types of pathogenic/likely pathogenic variants reported (VUS excluded). A roughly equal distribution of missense, frameshift and nonsense variants was detected, and 16% of the reportable pathogenic/likely pathogenic variants were copy number variants (CNVs). Other variants included inframe deletions and duplications. Benign or likely benign variants are not reported but are available upon request.

Copy number variants (CNVs) detected by next-generation sequencing (NGS). Each colored line represents a different patient. Samples normalized to a ratio of 1 represent normal diploid copy number, whereas regions normalized to 1.5/0.5 are representative of a heterozygous duplication/deletion, respectively. (A) Shows a section of chromosome 16. The patient represented by the red line has a full gene duplication of NDE1. The patient represented by the green line has a full gene deletion of PRRT2. (B) Shows a section of chromosome 22. The targeted NGS panel can also detect subgene or sub-exon-level CNVs. The patient represented by the yellow line has a deletion of DEPDC5 exon 30.

Copy number variants (CNVs) detected using in-house developed algorithm from NGS panels

AD = autosomal dominant; AR = autosomal recessive; LP = likely pathogenic; NGS = next-generation sequencing; P = pathogenic; VUS = variant of uncertain significance. Individual #40 had two separate CNVs, involving SNAP29 and TCF4 genes. $: Confirmed by microarray as having 15q11.2q13 microduplication syndrome.
Diagnostic yield
Overall, 75% (743/983) of probands had at least one reportable variant (VUS/LP/P), and 19.2% (189/983) had at least one P/LP variant reported. The diagnostic rate reported by the laboratory, comprising both molecular and possible molecular diagnoses, for all unique samples (excluding add-on requests) was 20.8% (204/983) (Figure 6A). The early infantile epileptic encephalopathy panel yielded the highest diagnostic rate at 26.7% (15/57), followed by custom requests at 23.7% (19/83) (Figure 6B). However, the comprehensive panel resulted in the highest absolute number of diagnostic results (148/674; 22.1%) (Figure 6B). Correspondingly, the comprehensive panel also presented the highest (65.6%) proportion of uncertain results.
Next-generation sequencing (NGS) epilepsy panel diagnostic rates (n = 983 unique proband reports). A molecular diagnosis was defined as the presence of 1 or 2 pathogenic or likely pathogenic (P/LP) variants in a single gene, depending on the mode of inheritance of the associated disorder, or a confirmed de novo variants of unknown significance (VUS) in an autosomal dominant gene. A possible diagnosis was defined as two VUS in a clinically related autosomal recessive (AR) gene or 1LP/1P variant in an AR gene. An uncertain result is any VUS that does not fit into prior categories. Negative results identified no reportable variants (benign or likely benign variants are not reported but are available upon request) by NGS. (A) NGS test results for the collective database found a combined molecular/possible diagnostic rate of 20.8%. (B) NGS test results using the same classification system broken down by subpanel.

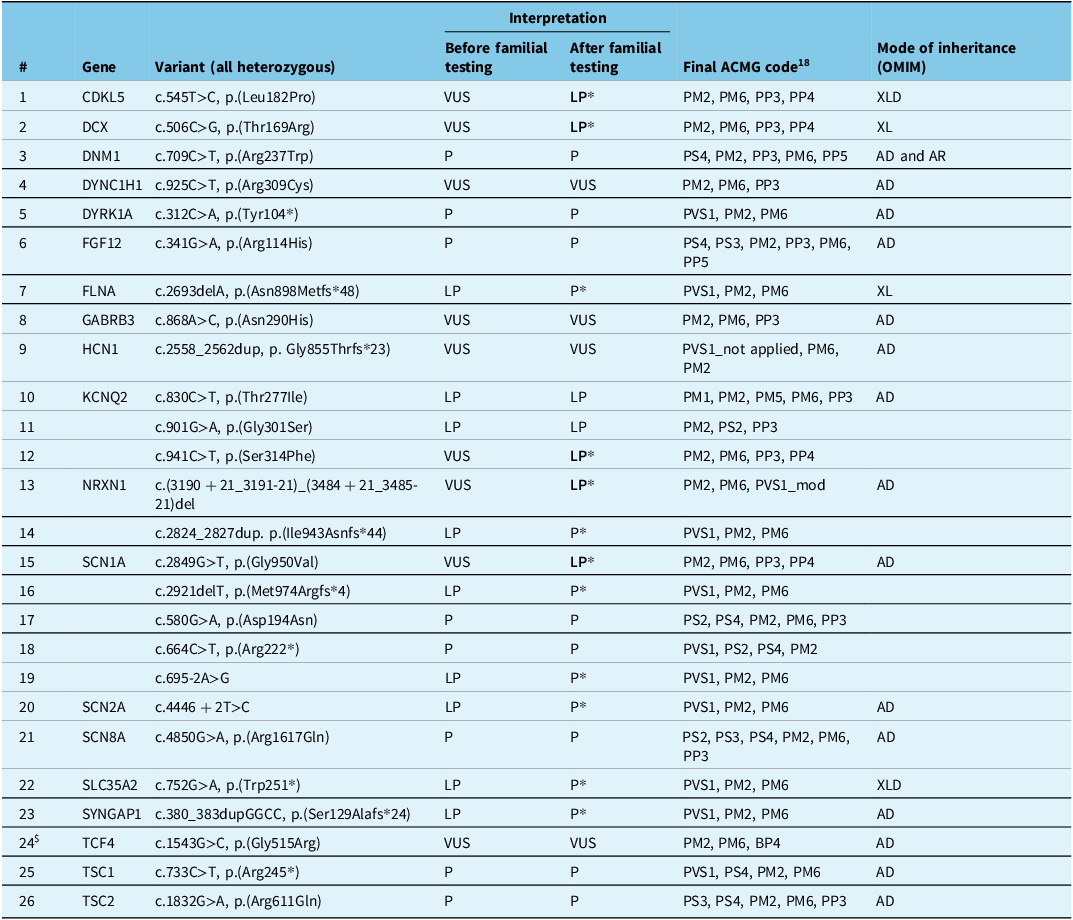
Subsequent familial testing identified 26 assumed de novo variants (but without confirmation of paternity and maternity) (Table 2), with five of these variants identified in SCN1A, three in KCNQ2 and two in NRXN1, while the remaining variants were distributed across unique genes. Seven (out of 9) LP variants were confirmed to be P after parental testing. Five (out of 9) VUS were reclassified as LP based on the de novo criteria (PM6) and additional clinical information for gene-disease correlation (PP4).Reference Richards, Aziz and Bale18 Clinical information was missing in some cases with presumed de novo VUS. As a result, some of these variants could still be reclassified as LP if the patient’s clinical features match the genetic diagnosis. For a complete summary of familial testing outcomes and variant segregation, refer to Supplemental Table 2 (in Supplementary Material 2).
Variants reported as assumed de novo based on familial testing, resulting in upgrade in classification and diagnostic confirmation in 5/9 VUS. In all cases (except #24), samples from both biological parents were tested; in some cases, extended family members were available

AD = autosomal dominant; AR = autosomal recessive; LP = likely pathogenic; P = pathogenic; VUS = variant of uncertain significance; XLD = X-linked dominant; XL = X-linked recessive. *:cases in “after familial testing” resulted in variant reclassification. $: Only one parent tested.
Post-test diagnostic outcome assessment
The post-test questionnaire included two questions. The first inquired about clinicians’ assessment of the reported result, categorizing them as either (i) diagnostic, (ii) non-diagnostic or (iii) uncertain (involving a VUS). The average clinician-reported diagnostic rate in the returned questionnaires was 16% (92/571), the Early Infantile panel exhibited the highest percentage of clinician-reported diagnostic rate at 28% (10/36) (Figure 7).
Ontario Epilepsy Genetic Testing Program (OEGTP) management impact form diagnostic responses by panel (n = 571). Following testing, clinicians were asked to respond to the reported test result in a post-test questionnaire and indicate if the result was in their opinion: diagnostic, non-diagnostic or if a variant of unclear clinical significance was identified. The average reported diagnostic rate across all panels was 17.2%. The Early Infantile panel reported the highest percentage of diagnostic findings (27.8%).

The second question in the post-test questionnaire asked clinicians to indicate if the testing resulted in any change in patient management and, if so, to select the specific change in management (see questionnaire in Supplementary Material 1). From this, 47% (267/571) of patients were reported to have some form of management benefit post-testing as defined by the ordering provider (Figure 8). Of those cases with reported change in management, the majority of them (70%) received a non-diagnostic or VUS genetic testing result. Excluding cases where the only management change applied to referrals of family members for testing, 24.3% (139/571) of patients underwent a direct change in management: most frequently referrals to other specialists and additional imaging/testing. Medication changes or ketogenic diet institution were reported in 22 (4%) cases, from which the majority 15 (68%) received a diagnostic molecular test result.
Ontario Epilepsy Genetic Testing Program (OEGTP) management impact form change in management responses by panel (n = 571). Following testing, clinicians indicated on the post-testing questionnaire if the OEGTP test results led to a change in management of their patient. If applicable, it is possible to select multiple responses. Collectively, 24.3% of patients were reported to have some change in management following testing, with ∼ 4% reporting a direct change in patient treatment. Familial testing for parents, cascade diagnostic or prenatal testing was observed in 23.8% of cases.

A significant association was observed between the age of onset and diagnostic findings (chi ^ 2 (degrees of freedom = 2, N = 557) = 21.43, p = 2.22E-5), indicating a higher diagnostic rate among individuals with an onset of < 1 year of age (Supplemental Table 3 in Supplementary Material 2).
Discussion
The OEGTP model encompasses many unique elements, such as incorporating input from multiple experts from provincial centers across specialties within an oversight committee, who then provides a regular review process to improve all aspects of implementation by periodic curation of both panel gene content and the testing process, from tailoring the requisition form to implementing variant resolution strategies. The collection of post-test clinician-reported outcomes that highlight clinical benefits, the inclusion of a community-centered training program to educate providers and improve access and the implementation of an NGS panel with CNV detection capabilities were other unique features of the OEGTP that allowed the program to set a provincial standard for integration of genetic testing in epilepsy care. A programmatic, centralized approach can streamline future research initiatives aimed at enhancing diagnostic rates, such as expanded genomic and epigenomic analyses.
Establishment of the OEGTP and implementation of routine NGS panel testing resulted in a diagnostic yield with a direct management impact in a significant proportion of patients with epilepsy. In this comprehensive analysis of the genetic basis of epilepsy in a large cohort of 983 individuals with diverse phenotypes, we demonstrate the diagnostic efficacy along with clinical impact. We identified a molecular diagnostic/possible diagnostic in 20.8% of probands, a rate consistent with previous studies utilizing targeted NGS panels.Reference Mercimek-Mahmutoglu, Patel and Cordeiro19–Reference Carvill, Heavin and Yendle21
The most ordered clinical testing for epilepsy includes chromosomal microarray (CMA) and NGS testing, with a significant proportion of patients (∼20%) having both tests ordered.Reference Burk, Kaneko and Quindipan22 While there is evidence that NGS (large panels or exome sequencing) has a higher diagnostic yield than CMA in pediatric epilepsy, many medical providers add CMA to the diagnostic process, especially if the patient also has a developmental disability, based on the 2010 American College of Medical Genetics guidelines.Reference Miller, Adam and Aradhya23 A more recent publication by ACMG recommends the use of whole exome sequencing (WES) or whole genome sequencing (WGS) as a first or second tier (after CMA) test for patients with developmental disabilities (including epilepsies).Reference Manickam, McClain and Demmer24 In addition, cost-effectiveness analysis supports a step-wise approach with WES or NGS-panel as first tier and, if negative, CMA for patients with epilepsy of unknown etiology.Reference Sánchez Fernández, Gaínza-Lein, Lamb and Loddenkemper25 An NGS-based test capable of detecting gene-level CNVs, such as the OEGTP panel, further enhances the diagnostic yield of NGS by combining the two approaches, making it the optimal first-tier testing option for this population.
Similarly to our previous findings in hereditary cancer,Reference Schenkel, Kerkhof and Stuart16,Reference Bhai, Levy and Rooney26 mitochondrial disordersReference Levy, Kerkhof and Belmonte27 and neuromuscular disorders,Reference Volodarsky, Kerkhof and Stuart28 we demonstrate that a custom NGS assay that includes CNVs detection significantly increased the diagnostic yield in patients with epilepsy, with 16% of all reported pathogenic variants being large sub-exon, exon and multigene deletions and duplications (Table 1). Some of these CNVs involved the deletion or duplication of a gene within a known microdeletion or microduplication genomic region, such as a PRRT2 gene deletion within 16p11.2, while the majority were novel, highlighting the advantage of a comprehensive NGS-based CNV analysis. For cases involving larger CNVs, microarray testing was recommended to confirm the extent of the deletion or duplication, contributing to the complete and accurate identification of the underlying genetic diagnosis.
Limitations of this study include its retrospective design and potential sampling or response bias, given the 58% response rate to the management impact forms. However, the use of standardized forms for both pre- and post-test processes facilitated the uniform collection of data across subjects and centers, providing a reasonable snapshot of the provincial landscape.
Personalized medicine is rapidly evolving in the field of epilepsy. A genetic diagnosis narrows the scope of medications used in certain epilepsies, as exemplified by a diagnostic result with a LP variant in SLC2A1, resulting in a change in treatment strategy. Disease causing variants in SLC2A1 are associated with glucose transporter 1 (GLUT1) deficiency disorder, which is targeted successfully with institution of ketogenic diet.Reference Alter, Engelstad and Hinton29 There were further examples of diagnostic results involving SCN1A-related disorders, where sodium channel blocking agents are avoided to prevent seizure exacerbationReference Wirrell, Tinuper, Perucca and Moshé30 and agents such as stiripentol are considered first-line treatment options following diagnosis,Reference Wirrell, Laux and Franz31 as well as in KCNQ2-related encephalopathy, where sodium channel blockers are preferred.Reference Volodarsky, Kerkhof and Stuart28,Reference Alter, Engelstad and Hinton29
As for future directions, the OEGTP will continue to keep up with the advances in epilepsy genetic testing. Recent studies have demonstrated an increased diagnostic rate with WES among epilepsy patients, offering the additional advantage of identifying novel genetic causes.Reference Costain, Cordeiro, Matviychuk and Mercimek-Andrews8,Reference Helbig, Farwell Hagman and Shinde34 With the expanding list of genes associated with epilepsy and the rapid pace of novel gene discovery, WES or other genome-wide methods may complement current diagnostic approaches for syndromic epilepsy. Ontario Health’s Provincial Genetics Program has recently begun issuing “Genetic Testing Recommendation Documents” for various indications, including neuromuscular diseases and neurodevelopmental disorders, to delineate the appropriate stages for implementing genome-wide sequencing in the diagnostic process. The program also recently endorsed the use of genome-wide sequencing (WES or WGS) as a first-tier diagnostic option in the diagnosis of rare genetic conditions with updated criteria and eligibility (https://www.ontariohealth.ca/providing-health-care/clinical-guidelines-standards/genetics-guidelines). Finally, emerging research demonstrates diagnostic utility of DNA methylation analysis in patients with genetically unsolved pediatric epilepsies, even after extensive genomic profiling including WES and WGS.Reference LaFlamme, Rastin and Sengupta35 The OEGTP now has the infrastructure and experience to utilize a programmatic approach to adapt to rapidly changing landscapes and implement the most clinically relevant technology for epilepsy patients in Ontario.
The integrated, dynamic and responsive approach of OEGTP to epilepsy genetic testing, coupled with continued genetic education, could empower healthcare providers to consider genetic testing early in their diagnostic algorithm, confidently order the optimal genetic test with relevant follow-up, ultimately interpret the results and counsel patients accurately.
Conclusion
The OEGTP was established through collaboration among clinical, laboratory and regulatory stakeholders. This partnership created a comprehensive and effective solution that was able to integrate seamlessly into the provincial healthcare system. By enhancing diagnostic capabilities and patient care for syndromic epilepsies, the program ensures a coordinated and impactful approach to delivering high-quality, system-responsive healthcare.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/cjn.2025.69
Acknowledgments
We thank the epilepsy community, the patients and their families, without whom our work would not be possible. We also acknowledge the geneticists, neurologists, epileptologists, pediatricians, family physicians, genetic counselors and all other healthcare providers who have utilized OEGTP panels to care for their patients.
Author contributions
TBB, KJ, LBL, OJ, SH, ANP, DAD, OCS and BS, as past and present members of the OEGTP, contributed to study design, working group creation, clinical standardization and NGS panel design; TBB, DAD, BS and LCS contributed to manuscript writing and editing; TBB and LCS prepared the tables, LCS, CR, JT, JK and PB contributed to data analysis, result generation and prepared the figures; all authors revised the manuscript.
Funding statement
The authors did not receive support from any organization for the submitted work.
Competing interests
The authors, ANP and KJ, receive research support from “Expert testimony for Canadian Medical Protective Association” and “New Investigator Fund Grand Hamilton Health Sciences,” respectively. ANP also serves on an advisory board for “Trofinetide Advisory Board, Acadia Pharma.” KJ received an honorarium for educational writing for the “Project ECHO Epilepsy across the Lifespan/Epilepsy Genetics.” KJ participates in committee and advocacy groups: “Standing Committee Member Ontario Provincial Epilepsy Network (OPEN) Advisory Committee”; “Standing Committee Member Epilepsy Module International Child Neurology Teaching Network”; “Standing Committee Member Co. Lead EEG training Canadian League against Epilepsy, Canadian Epilepsy Teaching Network”; and “Standing Committee Member Ontario Epilepsy Genetic Testing Program Steering Group.”












 Open access
Open access