


LEARNING OBJECTIVES
After reading this article, you will be able to:
-
• understand the current challenges in prescribing for severe BPSD and other complexities in management
-
• understand how wider societal and sociological factors shape prescribing in BPSD
-
• appreciate the relevance of palliative care principles in overcoming therapeutic nihilism, reducing distress and improving dementia care.
Behavioural and psychological symptoms of dementia (BPSD) encompass a wide range of symptoms, including aggression and agitation, psychosis, mood disturbance, anxiety, apathy, disinhibition and sleep–wake cycle disruption. The majority of people living with dementia will experience one or more at some point during progression of their disease (Gallop Reference Gallop, Ford and Bowman2025). These symptoms cause significant distress for the individuals, their families and carers, and reflect complex interactions between the severity of dementia, environment, unmet physical or psychological needs, and comorbid medical or psychiatric conditions (Sampson Reference Sampson, White and Leurent2014).
Severe BPSD, associated with risk to self and others, often necessitate urgent intervention, including the use of psychotropics. Despite well-documented risks, antipsychotics in particular remain commonly prescribed (Smith Reference Smith, Petersen and Hayes2025). This article critically explores this issue and the current challenges and complexities faced by clinicians in the management of severe BPSD, with a focus on pharmacological treatment. These include limitations of the current evidence base and related guidelines, as well as sociopolitical contexts and policy frameworks that influence prescribing decisions. We also consider how different paradigms, such as palliative perspectives, can inform balanced and compassionate approaches to the management of severe BPSD.
Defining and measuring ‘severe’ BPSD
Categorising symptom severity
Defining behavioural and psychological symptoms as ‘severe’ is a critical step when considering the need for pharmacological treatment. Many clinicians will approach categorising BPSD severity heuristically as they would with any other psychiatric syndrome, considering the frequency, intensity, impact on the patient, family and other caregivers, and the associated risk to self or others (Gallop Reference Gallop, Ford and Bowman2025). This is inherently subjective as BPSD are fluctuating, episodic and context dependent, and their unstable course makes categorisation difficult (Anantapong Reference Anantapong, Jiraphan and Aunjitsakul2025). The overlap of BPSD with other syndromes, such as hyperactive delirium, and their occurrence in chaotic and busy settings, such as the acute hospital, makes BPSD difficult to quantify in practice (Sampson Reference Sampson, White and Leurent2014; Gallop Reference Gallop, Ford and Bowman2025). Discordant accounts of BPSD and their severity may provide valuable opportunities for identifying situational factors that contribute to symptoms, but this complicates stratification of severity and need for treatment (McKeith Reference McKeith and Cummings2005a).
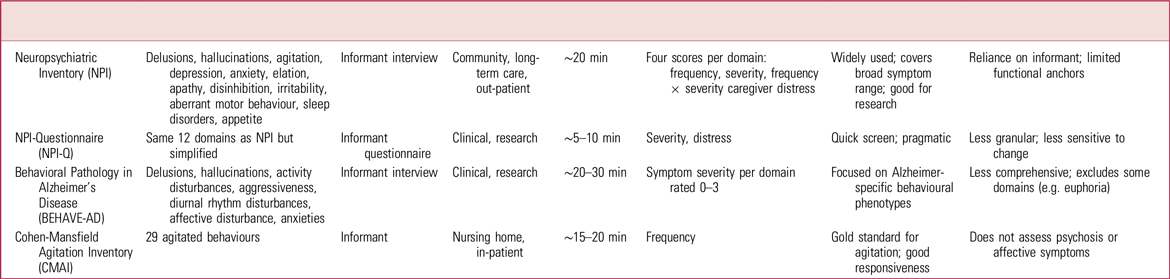
The above challenges have led to the development of validated research instruments such as the Neuropsychiatric Inventory (NPI), Cohen-Mansfield Agitation Inventory (CMAI) and Behavioral Pathology in Alzheimer’s Disease (BEHAVE-AD) rating scale, as summarised in Table 1.
Comparison of instruments for assessing neuropsychiatric symptoms in dementia a

a .Further information on these instruments and more is available from the Dementia Outcomes Measurement Suite at https://www.dementiaresearch.org.au/resources/doms.
These measures attempt to quantify BPSD but differ in their focus, structure and utility in defining severity categories (Anantapong Reference Anantapong, Jiraphan and Aunjitsakul2025). Their routine use in real-world clinical settings is also constrained by the need for specialist training and their administration times. There is a short form of the NPI (the NPI-Questionnaire or NPI-Q), which takes 5 min to administer, but it provides limited differentiation of very severe symptom states as it conflates agitation and aggression in a single domain, and symptoms in its highest severity category are defined as ‘extremely distressing, unable to [be] cope[d] with’, which are both subjective constructs. Similarly, although there are subscales for aggression in other neuropsychiatric symptom scales, there is no perfect psychometric measure that is brief and consistently used. This makes it difficult to accurately assess and measure the severity seen in real-world clinical settings. Furthermore, the lack of consistent definition adds to challenges in comparing results and design targeted interventions (Cummings Reference Cummings, Mintzer and Brodaty2015).
Terminology, classification and the medicalisation of dementia
Appraisal of the evidence base for the pharmacological treatment of severe BPSD is made more difficult by inconsistent terminology, the difficulties in quantifying severity (as above) and the nebulous nature of symptoms. Although this article uses the term ‘behavioural and psychological symptoms of dementia’ (BPSD), other authors use terms ranging from ‘neuropsychiatric symptoms’, ‘behavioural symptoms’ and ‘non-cognitive symptoms’ to ‘challenging behaviours’, reflecting the conceptual and lexical ambiguity within the field (Watt Reference Watt, Porter and Tavilsup2024). As these overlapping terms encompass diverse phenomena, from delusions and hallucinations to agitation, apathy and aggression, clinicians may inadvertently overlook relevant studies simply because of variations in terminology. The broad diagnostic category of BPSD also conflates multiple aetiologies, experiences and expressions of unmet need, explaining why no single treatment approach is universally effective (Rose Reference Rose, Lyketsos and Rosenberg2025).
The difficulties of classifying BPSD are indicative of problems that have long dogged dementia research and practice generally. As the contemporary dementia research economy flourished in the late 20th century, various scales and cognitive batteries were devised to better demarcate the problem (Wilson Reference Wilson2017). Dementia poses challenges for classificatory schemes because of its heterogeneous presentation and the subjective nature of the behaviours and experiences associated with it. Nonetheless, certain measures are now used widely and have become integral to research and treatment practices. Classification has traditionally been understood as a key component of medicalisation, a sociological critique contending that circumstances previously perceived by people as normal human circumstances (i.e. later life cognitive decline) have been reclassified as a medical problem and hence brought under medical control. Central to this critique is concern that medicalisation dehumanises people with dementia by always treating their behaviours as pathological, rather than as legitimate human expressions, therefore warranting technical management by medical authorities (Fletcher Reference Fletcher2023). The pharmacological management of BPSD can be interpreted as an example of the medicalisation of dementia. Forms of life at odds with dominant societal interests are kept in check via technical interventions, often administered by medical authority without consent. Establishing classificatory schemes is integral to substantiating that authority.
Current evidence: benefit, harm, efficacy, prospects
Contemporary management of BPSD emphasises holistic, person-centred assessment to identify reversible contributors to distress and prioritises individualised, non-pharmacological interventions as first-line treatment. Pharmacological therapies are reserved for severe distress or risk, and should be used proportionately, with regular review.
However, evidence for both non-pharmacological and pharmacological interventions remains limited by methodological and resource constraints (Rose Reference Rose, Lyketsos and Rosenberg2025). As McKeith cautions, ‘most evidence is flawed in some way and therefore, it is argued, cannot be relied upon. Gazing ever further into the evidence simply increases our sense of uncertainty. When does a benefit in BPSD become a useful one, and how does one measure it?’ (McKeith Reference McKeith2005b). This doubt remains central to current debates on psychotropic use in dementia.
A key limitation of the evidence base is that the benefits of drugs for severe symptoms are often conflated with effects across a broad spectrum of severity. Nevertheless, several trials have attempted to stratify outcomes by severity, suggesting that psychotropic medications may confer greater benefit in more severe cases of agitation and aggression (Box 1). Collectively, these studies suggest that atypical antipsychotics may have a clinically meaningful role in managing severe BPSD, such as agitation and aggression, when symptoms are refractory to non-pharmacological approaches and associated with substantial distress or risk.
Intervention studies that stratify results by severity of behavioural and psychological symptoms of dementia (BPSD)
-
In the Clinical Antipsychotic Trials of Intervention Effectiveness–Alzheimer’s Disease (CATIE-AD), post hoc analyses showed that patients with higher baseline Neuropsychiatric Inventory (NPI) scores – particularly in agitation and psychosis domains – were more likely to demonstrate improvement with antipsychotics, especially in the first 2 weeks, but benefits remained modest and counterbalanced by adverse events (Schneider Reference Schneider, Tariot and Dagerman2006).
-
The Citalopram for Agitation in Alzheimer Disease Study (CitAD) enrolled only patients with high NPI agitation scores; reductions in agitation, irritability and anxiety with citalopram were comparable to improvements seen in ‘severe symptom’ cohorts receiving antipsychotics in other trials (Porsteinsson Reference Porsteinsson, Drye and Pollock2014).
-
The dementia antipsychotic withdrawal trial (DART-AD), a deprescribing randomised controlled trial, also suggested that patients with more severe BPSD were more likely to benefit from continued treatment, in contrast to those with milder symptoms (Ballard Reference Ballard, Hanney and Theodoulou2009).
-
The Halting Antipsychotic Use in Long-Term Care (HALT) trial provides further context for this, demonstrating that discontinuing risperidone in prior responders was associated with an increased short-term risk of relapse, supporting continued treatment in some severe cases (Brodaty Reference Brodaty, Aerts and Harrison2018).
Antipsychotics, adverse outcomes and confounding factors
The harms associated with antipsychotic use have been widely publicised (Mok Reference Mok, Carr and Guthrie2024), but literature on the magnitude of harms is nuanced. Schneider et al’s meta-analysis, which underpinned the US Food and Drug Administration’s original 2005 black box warning for atypical antipsychotics, concluded that there was a 1% increase in the absolute risk of death with treatment (which translated to a number needed to harm of 100, compared with a number needed to treat between 9 and 25) (Schneider Reference Schneider, Dagerman and Insel2005). It was also postulated that if excess mortality was primarily related to the initiation rather than the continuation of antipsychotic treatment, then the periods surrounding commencement and withdrawal may be the times of greatest risk (Taylor Reference Taylor, Barnes and Young2025).
A more recent population-based matched cohort study concluded that antipsychotic use was associated with increased risk of multiple adverse outcomes, such as pneumonia, stroke and all-cause mortality (Mok Reference Mok, Carr and Guthrie2024). However, neither Schneider et al nor Mok et al stratified their analyses by symptom burden and they were unable to control for the type or severity of BPSD. Studies that do stratify show that mortality in dementia increases with BPSD severity and that, even without medication, people with severe agitation and aggression have a significantly elevated baseline risk of death (Bränsvik Reference Bränsvik, Granvik and Minthon2021). Evidence from acute hospital settings further shows that severe BPSD are strongly prognostic of premature mortality, with symptoms such as activity disturbances (such as pacing and wandering), aggression and eating disturbance conferring up to a 74% increased risk of death (Sampson Reference Sampson, White and Leurent2014). It has also been suggested that the apparent excess mortality associated with antipsychotics is attenuated after adjusting for confounders such as age, psychiatric history, dementia severity and delirium (White Reference White, Leurent and Lord2017). Taken together, these studies suggest a double jeopardy for clinicians: although antipsychotics are associated with increased risk, so is non-treatment and persistence of severe symptoms.
Other psychotropics and novel interventions
Other classes of psychotropic show little benefit in severe BPSD. Cognitive enhancers (cholinesterase inhibitors and memantine) demonstrate only small effect sizes in alleviating BPSD and have limited utility in acute situations (Taylor Reference Taylor, Barnes and Young2025). Mood stabilisers such as valproate have not shown benefit, and benzodiazepines are generally best avoided outside of emergency sedation because of their association with cognitive impairment and falls (Taylor Reference Taylor, Barnes and Young2025). Systematic and narrative reviews similarly emphasise the lack of consistent clinically meaningful benefits (Barnes Reference Barnes, Banerjee and Collins2012).
The immediate prospects for new BPSD treatments are poor. Rare exceptions include 5-HT2A receptor antagonists such as pimavanserin (currently in phase 3 trials for Alzheimer’s psychosis) and brexpiprazole (Aga Reference Aga2025). Evidence for these remains preliminary, based on limited randomised controlled trial (RCT) data, and not specific to severe BPSD. The development of novel treatments for BPSD is complicated by additional issues. These include significant ethical challenges in conducting RCTs of new (and potentially toxic) agents in a population with limited capacity to consent, difficulties in defining what constitutes a categorical response to treatment and ongoing disagreement among professionals regarding preferred treatments (Sink Reference Sink, Holden and Yaffe2005). Clinicians may feel that they work under similar conditions of clinical equipoise when deciding what to prescribe for an individual presenting with severe BPSD such as aggression.
Current influences on prescribing
Macro- and micro-contexts: political economics and clinician–patient dynamics
Historically, the management of BPSD can be interpreted within the broader political economic context of industrialising nations seeking to manage growing populations of older people whose behaviour was understood as imperilling the modern state. As societies became more reliant on wage labour and state welfare, and family structures were disrupted, older people described as ‘senile’ were increasingly seen as a burden on public resources (Boyer Reference Boyer2016). Gerontologists have theorised this creation of a burdensome older population as a process of ‘structured dependency’ (Townsend Reference Townsend1981).
Early practical interventions relied on institutionalisation in asylum and workhouse systems, which lasted in various forms until the mid-20th century, when mass deinstitutionalisation released people whose symptoms were deemed safely manageable in the community, partly owing to pharmacological advances (Balbuena Rivera Reference Balbuena Rivera2024). However, despite major pharmacological intervention, the population with severe BPSD have remained in the historical model of institutionalisation and are still significantly over-represented in institutions (Anantapong Reference Anantapong, Jiraphan and Aunjitsakul2025). They are a hangover of institutionalising psychiatry, yet are nonetheless subject to newer pharmaceuticalising psychiatry. This historical account situates the contemporary institutional treatment of severe BPSD vis-à-vis the state. From a sociological perspective, the chequered histories of many contemporary institutions and the genealogy of modern population governance provide important context for understanding institutional responses to BPSD. However, this perspective does not contradict the lived experience of BPSD as a form of human suffering, nor the corresponding ethical and clinical impulse to alleviate that suffering wherever possible through medical care.
Within this macro-political economic system, continued prescribing in BPSD at a micro-level is shaped by complex interactions between clinician, patient and other contextual factors (Fig. 1). Patient factors such as demographics, prior response to non-pharmacological strategies, and the severity and type of symptoms, particularly aggression, agitation and psychosis, strongly influence psychotropic use (Jones Reference Jones, Petersen and Walters2020). Practitioner and system influences, including clinical judgement, experiential knowledge (such as pain recognition), workload and institutional culture, also influence prescribing practices (Graham Reference Graham, Fielding and Beattie2022). Sociological perspectives highlight how these dynamics reflect broader expectations that each clinical encounter should yield a pharmacological intervention (Smith Reference Smith, Petersen and Hayes2025), playing out within and informed by the political economic pressures described above.
Factors influencing prescribing for behavioural and psychological symptoms of dementia (BPSD).

Clinical guidelines: prescribing and deprescribing
Formal guidelines also play a role in determining prescribing practices. However, once again, these are often undermined by variability and classificatory uncertainty. Numerous guidelines have attempted to clarify best practice and inform decision-making (a summary of international guidelines is given in the supplementary material, available online at https://doi.org/10.1192/bja.2026.10211). Clinicians are expected to follow local guidelines, and inevitably approaches in different jurisdictions vary, reflecting ongoing contradictions in the evidence base.
Most guidelines recommend pharmacological approaches only when there is ‘severe’ agitation, distress or significant risk. However, this is not always operationalised, instead relying on doctors’ individual judgements. Prescribers often feel there is insufficient guidance and clarity in making these judgements, particularly given potential treatment harms (Gray Reference Gray, Moniz-Cook and Reichelt2022). With a mounting focus on deprescribing, recommendations to wean and cease medications are inconsistent regarding review intervals and rates of dose reduction, and may appear perfunctory when trying to urgently treat acute symptoms. There is also considerable inconsistency in recommendations for preferred psychotropic agents and in what order they should be trialled. Some guidelines (an international Delphi process and Canadian clinical practice guidelines; Kales Reference Kales, Lyketsos and Miller2019; Hatch Reference Hatch, Seitz and Bruneau2025) offer stepped hierarchies of medications, whereas others (American Psychiatric Association; Reus Reference Reus, Fochtmann and Eyler2016) centre on targeting symptoms. There remains considerable disagreement over best treatment for individual BPSD, for example in the treatment of agitation, whether citalopram or an antipsychotic should be trialled first (Taylor Reference Taylor, Barnes and Young2025). There are also differences in recommendations for and against use of antidepressants and cognitive enhancers.
Governance and regulation of prescribing
Policy also plays an important role in shaping prescribing practices. Over the past 15 years, multiple initiatives in multiple countries have sought to curb psychotropic prescribing, especially antipsychotics, for BPSD. The impact on clinician attitudes has been mixed, from cautious support to heightened anxiety and fear of litigation (Wood-Mitchell Reference Wood-Mitchell, James and Waterworth2008). The latter may have caused ‘prescribing displacement’, with reductions in one drug class offset by rises in others. For example, following the Food and Drug Administration’s boxed warning regarding atypical antipsychotics in 2005 (extended to all antipsychotics in 2008), overall atypical antipsychotic use for dementia declined but prescriptions for opioids and anti-epileptic agents increased (Rubino Reference Rubino, Sanon and Ganz2020). Similarly, Sultana et al (Reference Sultana, Fontana and Giorgianni2016) found divergent responses in the UK and Italy: although prescriptions for risperidone and olanzapine decreased after regulatory warnings, these reductions were offset by rises in quetiapine and typical antipsychotic use. Notably, the UK experienced an initial decline in prescribing following the first safety alert, but this was short-lived, with rates rising again until subsequent warnings were issued. In Italy, by contrast, antipsychotic prescribing continued to increase despite similar regulatory interventions. Collectively these findings suggest that regulatory measures appear to have prompted transient or compensatory changes rather than sustained reductions in psychotropic use in old age psychiatry (Langford Reference Langford, Chen and Roberts2020). This suggests that regulation alone cannot address the practical realities of managing severe behavioural disturbances.
Clinical judgement and the ‘chemical restraint’ discourse
Although enhanced prescribing governance and regulation of potentially inappropriate medications are essential, they must be accompanied by the development of evidence-based alternatives for severe BPSD. The Australian Halting Antipsychotic Use in Long-Term Care (HALT) trial demonstrated that structured, person-centred and deprescribing interventions can safely reduce antipsychotic use and improve well-being among nursing home residents with mild-to-moderate BPSD (Brodaty Reference Brodaty, Aerts and Harrison2018). However, this trial did not assess outcomes in individuals with severe BPSD, who often require intensive care within specialist mental health services. Consequently, contemporary deprescribing trajectories for individuals with severe symptoms remain poorly supported by evidence.
In this context, a UK national audit of antipsychotic prescribing in dementia (Barnes Reference Barnes, Banerjee and Collins2012) found that agitation and distress – likely overlapping constructs – were the primary target symptoms in the majority of cases, suggesting that alleviation of suffering rather than behavioural control is typically the principal driver of prescribing. These findings indicate that antipsychotic use in dementia is often grounded in thoughtful clinical judgement, even as they highlight the need for more systematic identification of remediable contributors to distress and for regular review of ongoing treatment in light of the fluctuating nature of BPSD. Nevertheless, this evidentiary gap has since intersected with an increasingly polarised and charged policy and legal discourse, with some advocates describing antipsychotic prescribing as ‘elder abuse’ and ‘behavioural euthanasia’ (Cain Reference Cain, Chejor and Porock2023). In some jurisdictions, medications used for BPSD are considered chemical restraints within the mantle of restrictive practices. Contemporary definitions of chemical restraint refer to the use of medication for the primary purpose of influencing behaviour, excluding treatment for a diagnosed mental disorder. These definitions vary across jurisdictions, and the status of dementia within restrictive-practice legislation remains inconsistently interpreted, leaving clinicians uncertain about the legal basis for urgent pharmacological intervention.
Pharmacological treatment: an persistent default response
Despite widespread concern and controversy regarding inefficacy and harms, the pharmacological treatment of BPSD remains commonplace. Much has been written of the need for high-quality tailored social and psychological support as a preferable alternative to pharmacological treatments (Fletcher Reference Fletcher2023). However, to function in the contemporary political economy of dementia, a generalised non-pharmacological approach would require, at a minimum, substantial levels of high-quality staffing. This would necessitate considerable expense, if not the reorganisation of capitalist societies to recentre sustainable social reproduction wherein older people are valued beyond their capacities for economic production. Between greatly increasing expenditure, instigating revolution or prescribing medication, the last has remained a default response to BPSD. It is difficult to envision a significant transformation of this situation.
Potential ways forward: the role of palliative principles in severe BPSD?
So what future options might be feasible? There is increasing recognition that BPSD, particularly agitation and aggression, contribute significantly to the suffering of people with dementia, place a substantial burden on carers and are associated with poor prognosis and increased mortality (Sampson Reference Sampson, White and Leurent2014; Tannenbaum Reference Tannenbaum, Boltz and Ilyas2022). This supports a role for palliative, holistic approaches addressing physical, psychological, social and spiritual needs in the management of severe, treatment-refractory BPSD (Veldwijk-Rouwenhorst Reference Veldwijk-Rouwenhorst, Smalbrugge and Zuidema2021). BPSD can be incorporated into advance care planning in a manner similar to other distressing symptoms that occur across the dementia trajectory, rather than being confined to end-of-life care, and palliative approaches may also support policy imperatives to reduce antipsychotic use (van der Steen Reference van der Steen, Radbruch and Hertogh2014). Importantly, severe BPSD most commonly occur in moderate to severe stages of dementia and may attenuate in the terminal phase. Accordingly, the application of palliative principles to BPSD should not be equated with end-of-life care, but rather understood as a means of proportionate, distress-focused intervention earlier in the disease course.
A palliative approach is not inherently an anti- or pro-pharmacological approach. When BPSD prove refractory to non-pharmacological strategies (Anantapong Reference Anantapong, Jiraphan and Aunjitsakul2025), antipsychotics, sedatives and analgesics, such as opioids, used for effect on pain and sedation, may be the only effective means of reducing anxiety and distress, and enabling carers to safely provide care. Some authors argue for their role in the ablation of suffering within dignity-prioritising frameworks, where relief is valued above prolongation of life at all costs (Treloar Reference Treloar, Crugel and Prasanna2010). In this framing, psychotropics become instruments of compassion, ensuring patients are not condemned to endure states of unbearable distress for the sake of marginal life extension. Importantly, adopting a palliative perspective does not automatically imply an end-of-life approach and abandonment of other therapeutic goals, including preservation of cognitive function and meaningful engagement.
Palliative sedation
One emerging treatment approach is the use of palliative sedation in cases of extremely severe, treatment-refractory BPSD. To our knowledge, the literature is limited to a single study describing the experiences of Dutch clinicians and family members (Veldwijk-Rouwenhorst Reference Veldwijk-Rouwenhorst, Smalbrugge and Zuidema2021). This work reflects a specific cultural and healthcare context, shaped by euthanasia legislation, a national guideline on palliative sedation and a long tradition of advance care planning in geriatric care, which may limit generalisability to other countries. Intermittent palliative sedation refers to the temporary and reversible lowering of consciousness, often for hours or days, to relieve acute, refractory symptoms such as agitation or psychosis. By contrast, continuous palliative sedation involving sustained sedation until death is a distinct intervention that should be considered when all other options, including intermittent sedation, have failed (Veldwijk-Rouwenhorst Reference Veldwijk-Rouwenhorst, Smalbrugge and Zuidema2021). Intermittent sedation must be trialled first and continuous sedation only after multidisciplinary review, consultation with families and with an old age psychiatrist.
Palliative care versus acute psychiatric treatment: a false dichotomy?
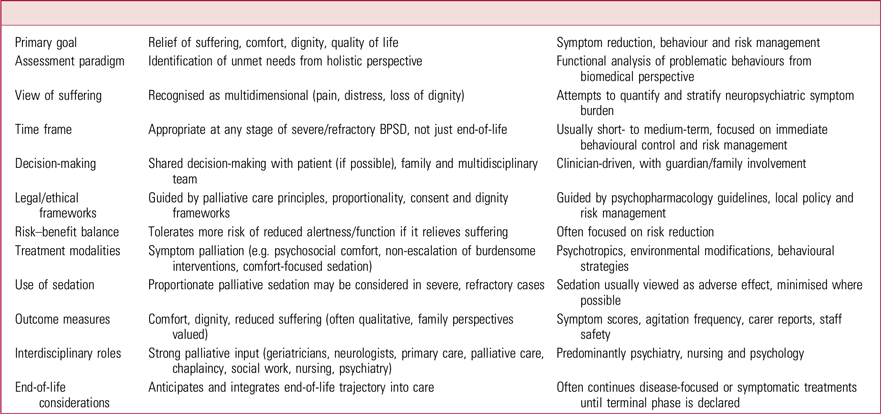
The purported philosophical differences between a holistic palliative care approach and an acute psychiatric response (a medical model) are outlined in Table 2. However, this false ideological dichotomy oversimplifies the real-world complexities surrounding care for people with dementia, not least persistent uncertainty regarding the scope of palliative care involvement, which has traditionally been conflated with end-of-life care. Again, classificatory difficulties regarding dementia can cause trouble here. Conventional definitions of ‘end of life’ are often less applicable in advanced dementia, given its prolonged, fluctuating and unpredictable trajectory (Browne Reference Browne, Kupeli and Moore2021). Individuals experiencing severe BPSD often do not display traditional indicators of end-of-life presentations (Gallop Reference Gallop, Ford and Bowman2025), and recognising when a patient is actively dying remains a significant challenge (Roach Reference Roach, Lovell and Macfarlane2023).
Theorised differences between a palliative and psychiatric approach in treatment of behavioural and psychological symptoms of dementia (BPSD)

Clinicians may experience difficulty distinguishing BPSD from related syndromes, including terminal agitation or delirium that may occur at any point in the dementia trajectory. This complexity is compounded by factors such as frailty overlap, the ongoing effects of psychotropic medication (O’Shea Reference O’Shea, Timmons and Kennelly2015) and inconsistent use of pain assessment tools. Although instruments such as the Abbey Pain Scale provide structured methods for evaluating pain in dementia, they are not direct measures of suffering and often fail to distinguish between physical and psychological distress, both of which may be profound in advanced dementia and BPSD (Treloar Reference Treloar, Crugel and Prasanna2010). Another challenge is the assessment of suffering itself. This is a difficult construct to define and measure and as a result is rarely considered in clinical trials, limiting the evidence base. There are validated quality-of-life (QoL) scales for use in dementia, but self-report measures are less applicable in advanced disease stages (Browne Reference Browne, Kupeli and Moore2021) and there is often discordance between the QoL ratings given by individuals with dementia and those offered by their carers (Römhild Reference Römhild, Fleischer and Meyer2018). Most major RCTs of antipsychotics in BPSD (e.g. CATIE-AD, CitAD, DART-AD, HALT: Box 1) focused primarily on symptom reduction (e.g. NPI, CMAI, Clinical Global Impressions scale) and adverse events (e.g. mortality, cerebrovascular risk), but not quality of life as a primary or even secondary outcome. In observational studies, an association has been reported between worse QoL in people with BPSD who are prescribed antipsychotics, but these do not account for BPSD severity (Ballard Reference Ballard, Hanney and Theodoulou2009). Taken together, these challenges impede the targeted delivery of palliative care for BPSD.
A broader ethical and legal issue is widespread concern that labelling psychotropic medications as ‘palliative’ risks legitimising indiscriminate prescribing and normalising sedation as care, adding to current concerns about medication overuse. Palliative sedation remains a socially sensitive practice and may be conflated with opioid overuse, premature death or even assisted dying (van der Steen Reference van der Steen, Radbruch and Boer2016). Regarding BPSD specifically, there is the additional ethical consideration that the person most affected is also unlikely to be able to consent to the treatment. Increasing public and political debate about assisted dying underscores the need for ethical vigilance and the development of unambiguous, safe and compassionate frameworks for clinical practice. Although some people with dementia may benefit from deprescribing, this should not preclude those with severe BPSD from access to palliative treatment that relieves their suffering.
A combined palliative–psychiatric model
What might a palliative model of care for severe BPSD look like? Ideally, it would be collaborative, needs-based and introduced early in the illness trajectory. There is currently no universally agreed palliative framework for severe BPSD, but palliative principles are increasingly incorporated into broader dementia care models. Palliative care specialists are also recognising BPSD as an important target for improving quality of life in people with dementia (van der Steen Reference van der Steen, Radbruch and Boer2016). This recognition underscores the value of collaboration between palliative care and dementia specialists, including old age psychiatrists, neurologists and geriatricians, whose combined expertise is essential for addressing complex behavioural, psychological and existential distress. A truly integrative model would draw on the strengths of different disciplines: psychiatry contributing formulation-based understanding, psychopharmacological expertise and risk management; and palliative care offering holistic assessment, communication frameworks, and a sustained focus on comfort and dignity. An interdisciplinary model of care (Fig. 2) would enable targeted symptom management, informed risk–benefit decision-making and meaningful involvement of families (Gallop Reference Gallop, Ford and Bowman2025).
Interdisciplinary model of care for people with severe behavioural and psychological symptoms of dementia (BPSD).

Care should emphasise early integration of palliative principles, as evidence suggests that patients and families derive the greatest benefit when palliative care is holistic, formulation-driven and tailored to their individual needs. This provides a structured means of understanding distress, identifying sources of support and co-producing plans to alleviate suffering. A needs-based approach also shifts the focus from disease staging and prognostication (which, as we have seen, is a recurrent classificatory struggle in BPSD) towards the dynamic prioritisation of care goals (Browne Reference Browne, Kupeli and Moore2021). These goals may evolve, with life prolongation and maintenance of cognitive abilities and function serving as mechanisms to maximise dignity and comfort, and more than one goal may apply simultaneously. Ultimately, a palliative approach does not aim to hasten death or prolong life, but to improve the quality of both. When integrated with psychiatric expertise, it offers a humane and hopeful paradigm that may help counter therapeutic nihilism among clinicians confronted with severe and persistent suffering in dementia (Rose Reference Rose, Lyketsos and Rosenberg2025).
Conclusion
The treatment of severe BPSD remains profoundly challenging and there is a gap between policy idealism and the lived reality of severe BPSD. Treatment advances are constrained by significant gaps in the evidence base, including the need for research that helps clinicians define severe or extreme categories of BPSD in a valid, reliable and clinically practical way. Policy frameworks can restrict clinical judgement and individualised treatment, and persistent structural and staffing limitations within the aged care sector also complicate care. Although regulatory oversight and public scrutiny of psychotropic use in dementia are important for promoting safer practice, they also create significant ethical and legal tensions for clinicians. This article intends to be provocative rather than polemical, inviting necessary debate about approaches to severe BPSD, while fully acknowledging the significant micro- and macro-constraints at play.
Combining psychiatric, neurological and geriatric approaches with those of palliative care could offer a more hopeful and practicable basis for clinicians to work from. Maintaining an open mind and genuine dialogue is essential as we explore new paradigms to reduce suffering while balancing the inherent risks of treatment (Rose Reference Rose, Lyketsos and Rosenberg2025). These are difficult but important conversations with families that cannot be resolved by shifting responsibility onto patients or carers. As professionals, we must remain willing to manage risk, complexity and uncertainty, not retreat from them, particularly when the goal is to reduce suffering in people with dementia and their families (McKeith Reference McKeith and Cummings2005a). As Harwood et al (Reference Harwood, Thiyagarajan and Bhadelia2025) remind us, people experiencing BPSD have the same right to a good life and death as any other individual. Recognising this right reframes our clinical and ethical responsibilities, challenges therapeutic nihilism and affirms that dignity, comfort and relief of suffering be treated as legitimate outcomes of care, not as failures of treatment.
MCQs
Select the single best option for each question stem
-
1 The main challenge in the use of instruments like the Neuropsychiatric Inventory to score neuropsychiatric symptoms is that:
-
a scales are only used in research settings, not clinically
-
b scales take time to administer and they remain subjective as to what is ‘severe’
-
c validated scales are expensive to purchase and require frequent updating
-
d repeatedly administering scales over serial reviews changes the utility of the results
-
e their interpretation is complicated when used in combination with other scales, e.g. the Geriatric Depression Scale and Dementia Quality of Life instrument.
-
-
2 As regards clinical guideline recommendations for prescribing in BPSD:
-
a clinical guidelines vary in their recommendations regarding approach to prescribing and medication choice
-
b pharmacological treatment should be determined based on target symptoms rather than a stepped hierarchy
-
c an antidepressant should be trialled before an antipsychotic
-
d cognitive enhancers should be trialled before an antipsychotic
-
e risperidone and olanzapine are equally effective if an antipsychotic is required.
-
-
3 Which of the following reflects a sociological critique on policy considerations that shape treatment decisions?
-
a most studies looking at BPSD response to antipsychotics do not stratify by symptom severity
-
b numerous terms used to denote BPSD make it challenging to review all research relating to the topic
-
c policy relating to restricted or monitored use of one medication can sometimes lead to ‘prescribing displacement’, with increased prescriptions of another
-
d an increased focus on wage labour together with expanded state welfare programmes contribute to the view that an ageing population is a burden on society and their behaviours must be managed
-
e international guidelines vary regarding their recommended approach to selecting a medication for the treatment of BPSD.
-
-
4 Which of the following is not currently a limitation in the application of palliative principles in people with dementia?
-
a the prognostic effects of BPSD are under-recognised
-
b the limited evidence base, for example few studies on BPSD have looked at palliative care outcomes such as quality of life
-
c palliative sedation may be conflated with opioid overuse, premature death or even assisted dying
-
d BPSD may be difficult to distinguish from related syndromes, including terminal agitation or delirium
-
e emerging medications like pimavanserin and brexpiprazole in BPSD reduce the need for palliative care input.
-
-
5 For psychiatrists treating people with BPSD, a palliative approach:
-
a offers a different treatment paradigm focusing on person-centred, needs-based care
-
b subtly signals to family that the patient is imminently dying, to ease into end-of-life conversations
-
c circumvents legal frameworks to reduce antipsychotic prescription
-
d provides legal protection in the event of death
-
e reduces therapeutic nihilism by justifying increased psychotropic use.
-
MCQ answers
-
1 b
-
2 a
-
3 d
-
4 e
-
5 a
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bja.2026.10211.
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Acknowledgement
All ideas in this article came from the authors. ChatGPT for MacOS (OpenAI, San Francisco, California, USA; https://chat.openai.com) was used for review of grammar and flow.
Author contributions
N.C. developed the main conceptual ideas and outline of the manuscript. All authors contributed to writing and review.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.





 Open access
Open access
eLetters
No eLetters have been published for this article.