


Public health experts turned late to the problem of accidents. Surveying the field after three decades of false starts, William F. Haddon Jr. (1926–1985), Edward Suchman, and David Klein mapped out a sweeping agenda for current and future investigators with their collection Accident Research: Methods and Approaches (1964). Over twenty academic journals including the Journal of the American Medical Association, American Journal of Public Health, American Sociological Review, and Nature reviewed the textbook, which became a crucial reference for university-trained injury prevention specialists.Footnote 1 According to Ross A. McFarland (1901–1976), Professor of Environmental Health and Safety at Harvard, the compilation offered an overdue response from health professionals to the rise of injuries as causes of morbidity and mortality: ‘With the increasing mechanization of our environment and the increasing complexity of our industrial processes, both the individual and the community are exposed to many new hazards at home, at work, in their transportation, and in their recreation’. McFarland, Haddon, and the other contributors to the collection argued that ‘the prevention of accidental death and injury’ deserved as much attention as ‘the control of infectious and degenerative diseases’, priorities which continued to dominate the U.S. medical system.Footnote 2 Within the narrower confines of injury control, moreover, workplace and traffic safety were overrepresented compared with the sites where accidents actually happened.Footnote 3
Although communicable illnesses had declined steeply since the outset of the twentieth century, medical authorities were slow to take up accident prevention. Haddon, Suchman, and Klein proposed multiple reasons for this paradox, complaining that even well-educated people often perceived accidents as unavoidable and unpredictable outcomes of fate or chance rather than events with measurable, modifiable causes. Many otherwise rational Americans allegedly believed accidents were ‘as uncontrollable as the weather’ and defied ‘any kind of systematic study beyond mere tabulation’.Footnote 4 These assumptions, mixed with the political ideals of freedom from coercion, personal responsibility, small government, and ambivalence about social welfare programs, had powerfully constrained the theory and practice of injury control. Haddon and his colleagues asserted that the path forward demanded branching out from safety education and mechanical engineering into physics, chemistry, mathematics, economics, psychiatry, sociology, anthropology, architecture, and city planning.Footnote 5 This interdisciplinary approach would let safety practitioners correct the ‘methodological errors’ of their predecessors and transform accident prevention into a science.Footnote 6
This influential myth about the ‘prescientific’ history of injury control prior to Accident Research papers over significant inflection points.Footnote 7 Haddon and his colleagues were merely the latest generation of experts to apply the logic and methods of epidemiology to injuries. As early as 1942, the American Public Health Association (APHA) and U.S. Public Health Service (USPHS) had gathered data from communities across the country to reveal the manifold causes of home accidents and to inform local safety campaigns. These initial investigations were comprehensive but nonspecific, warning families about all of the dangers of domestic space and recommending general strategies to live safely. This version of accident prevention resembled the ‘new’ public health and treated carefulness, like hygiene, as a learned habit.Footnote 8 Following the landmark article ‘The Epidemiology of Accidents’ (1949), safety professionals shifted from cataloguing hazards and counting cases to quantifying the extent to which isolable risk factors contributed to single accidents and to broader statistical trends. This revised approach to injuries coincided with the consolidation of risk-factor medicine and launched a decadeslong search for ‘magic bullets’ to eliminate specific types of injuries.Footnote 9 The accelerating proliferation of injury data mixed with the patchiness of accident prevention efforts pushed the USPHS to try to rationalise the field during the 1950s. When Haddon recast injuries as the physicochemical outcomes of ‘abnormal energy exchanges’ between bodies and their environments almost a decade later, he joined a dynamic lineage of safety studies and pilot projects.Footnote 10
This essay explains why public health institutions declined to prioritise injury prevention throughout the epidemiological transition of the mid-twentieth century and what made home accidents especially intractable.Footnote 11 From the 1940s to 1980, safety professionals analysed these events with the objective of improving available safety measures. The resulting sets of models, methods, and results, collectively referred to as ‘the epidemiology of accidents’, changed how experts interpreted injuries but did not achieve any lasting consensus about the most effective ways to keep homes safe. Across its different iterations, the epidemiology of accidents involved identifying, classifying, quantifying, and controlling the causes of unintended injuries and acted as what I refer to as a ‘science of attribution’. Like research on the drivers of climate change or the effects of industrial chemicals on community health, the epidemiology of accidents tried to disentangle the complex web of human, object-centred, and environmental factors associated with injuries.Footnote 12 Over the course of the twentieth century, safety experts borrowed models from infectious disease control, risk-factor medicine, and biomechanics to produce scientific data on accidents and to guide their applications. The success of these models as tools to actively prevent home injuries fell short of their promises: despite rising living standards and increased access to emergency medical treatment, the number of deaths from non-motor-vehicle accidents stayed roughly constant from 61,544 in 1941 to 59,058 in 1971.Footnote 13
Combining unpublished correspondence, conference proceedings, and reports from the USPHS; studies of home injuries from public health journals; and safety education resources for practitioners and ordinary Americans, I examine the slippages between the science of accident prevention and the implementation of corresponding safety interventions. Historians including Lukas Engelmann and Mary Morgan have demonstrated how mechanical, visual, mathematical, and conceptual models have defined the epidemiology of contagious diseases, economics, and civil administration over time.Footnote 14 This essay extends this approach to home accidents and argues that the models used to analyse domestic risks held individuals responsible for their own safety, downplayed the structural determinants of injuries, and consistently raised the burden of proof for potential solutions. Experts assumed that each redefinition of the epidemiology of accidents would lead to efficient, scalable strategies for home safety. The replacement of one model with another, however, casts doubt on the methods, evidence, and conclusions of previous research, inducing public health professionals to collect ever-more data on injuries and contributing to a cycle of decision paralysis. From 1940 to 1980, the essence of these data changed considerably from numbers of cases to statistical distributions and probabilities to measurements of physical forces. Safety specialists applied these distinct types of quantification to bring what Ian Hacking has called ‘the taming of chance’ to accidents.Footnote 15 Following Judith Green, who claims accidents were a leftover category of nineteenth-century mortality statistics, I describe the difficulty with which public health authorities confronted unintended injuries.Footnote 16 Overall, this essay lends new insights into the history of home safety and into the fitful transfer of epidemiological reasoning from infectious and degenerative disease to bodily harm.Footnote 17
The epidemiology of accidents
On 23 October 1936, Commissioner Edward S. Godfrey Jr. (1878–1960) of the New York State Department of Health applauded the American Public Health Association for the rapid decline of infectious diseases since the turn of the century and implored his colleagues to take comparable steps to prevent accidents. Due to improved sanitation and immunisation, injuries had started to account for rising proportions of disability and death relative to illnesses such as typhoid, diphtheria, and tuberculosis. Godfrey complained that this trend had largely escaped the attention of public health practitioners, who ‘tabulated and published’ applicable data but left safety programs ‘entirely to other agencies or to the will of God’. Godfrey emphasised the downstream costs of this complacency: ‘What is the net gain if a child, through breastfeeding and pasteurized milk, is prevented from dying of gastroenteritis if he pulls a stewpan of boiling water off the stove and is fatally scalded?’Footnote 18 He called on doctors, nurses, and state officials to study the ‘epidemiology of accidents’, a science of attribution based on identifying, classifying, quantifying, and controlling the causes of unintended injuries. Despite his appreciation for the environmental causes of disease and the infrastructure used to dispense clean water and food across the country, Godfrey equated accident prevention with education. Public health experts would be charged with teaching Americans, especially women, how to do everyday housework safely and how to avoid injuries themselves.Footnote 19
The medical profession was slow to respond to this appeal and discounted home safety into the 1940s. Even after the APHA appointed Donald Budd Armstrong (1886–1968), the Vice President of the Metropolitan Life Insurance Company, to chair its Subcommittee on Accident Prevention (1942), Armstrong essentially recycled the approach of his previous demonstration project in Framingham, Massachusetts. From 1917 to 1923, MetLife had collaborated with the National Tuberculosis Association to test Framingham residents for tuberculosis, to offer clear guidance on personal hygiene and sanitation, to pasteurise the town’s milk supply, and to treat the sick as ways to trim its expected payouts to policyholders.Footnote 20 Under Armstrong and William Graham Cole, the subcommittee consequently prioritised community outreach and systematic data collection over fixing, modernising, or regulating private homes. Safety authorities had to warn the public about risky practices and conditions, but families were responsible for carrying out their advice. Doctors were only one part of this arrangement. Visiting nurses reviewed the implications of the latest injury trends with their patients and inspected existing housing using standardised checklists.Footnote 21 Statisticians combined these results with regional hospital records to determine significant patterns from year to year.Footnote 22
This focus on measurement and safety education reflected the modest resources of the committee and the ideological convictions of the mid-century United States. For Armstrong and Cole, home accidents were hardships beyond the control of the government. Safety campaigns were seen as community affairs involving ‘education and motivation – at least in a democracy, where the privacy of the home is still respected’. Against the backdrop of the Second World War, the coauthors scoffed, ‘In a totalitarian state, if the authorities can send a man to a prison camp for violating restrictions about listening to foreign broadcasts in his own home, they can probably also jail a man for falling off a rocking chair’.Footnote 23 The APHA continued to conflate strong state intervention with coercion after the war, bracketing the extent to which building codes, access to affordable childcare, financial and technical assistance for costly repairs, and other policies could promote home safety. On the contrary, Armstrong and Cole chalked up most accidents to carelessness or ignorance and overestimated the efficacy of health communication. Although the APHA pushed for survey after survey to compile scientific data on home injuries, its proposals rarely indicated how local officials should act on their findings beyond holding occasional workshops, preparing bulletins, or appearing on television or radio.Footnote 24 The returns on this strategy were disappointing: ‘Health departments on the whole are now doing very little as regards actual or contemplated studies in the home accident field’.Footnote 25
Despite its mission to develop new accident prevention programs, the committee was unable to compete with the rival priorities of the APHA and its members. Speaking out at the ‘Victory Meeting’ of the APHA, Armstrong and Cole emphasised the stakes of the ‘continuing war against accidents on the home front’ and doubled down on their current frameworks for injury control.Footnote 26 The subcommittee unsurprisingly stalled from 1946 to 1949, when its second chairman, Isadore Jay Brightman, invited some safety experts to the annual conference of the APHA.Footnote 27 The session covered well-worn ground. Brightman criticised U.S. health departments for failing to assign funding and personnel to home injuries and advocated for more intensive safety education.Footnote 28 Elisabeth C. Phillips, the Executive Director of the Rochester Visiting Nurse Association, agreed. Unlike ordinary Americans who overlooked domestic risks, a professional nurse could notice a ‘child pick up the knife his sister put down when the telephone rang and the housewife who snatches a tea towel […] to take a boiling pot off an open flame’, turning these common mistakes into ‘on-the-spot’ lessons for the future.Footnote 29 Albert L. Chapman of the USPHS Division of Chronic Diseases felt this outreach might be premature and opposed taking action without epidemiological certainty: ‘It is only when a pattern of accidents points a finger very definitely in the direction of a mechanical or an environmental factor that we should say “that was the cause of the accident”’.Footnote 30 None of these speakers discussed how engineering or enforcement, two staples of industrial and transportation safety, could complement efforts to train Americans to live more cautiously.
Environmental approaches to injury prevention accordingly garnered less support from contemporary stakeholders than safety education or new research on ‘human factors’. Along these lines, accident proneness attributed incidents from car crashes to tap water scalds to the temperaments and physical traits of their casualties. At their most extreme, strictly biomedical models of injury tended to downplay the effectiveness of engineering, bureaucratic regulation, and social services as tactics to keep homes safe.Footnote 31 Frederick S. Kent (1917–1995), the eventual chief of the USPHS Home Accident Prevention Unit, warned his colleagues not to miss the risky material conditions associated with many accidents: ‘Our conception of environment has long since expanded from water and sewage facilities to include the home and its multifarious gear and its surroundings’.Footnote 32 If a housewife fell after standing on a chair to reach a cabinet close to the ceiling, for example, Kent asked safety professionals to consider ‘the inaccessibility of the cabinet’ as well as ‘the use of a chair instead of a step-ladder’.Footnote 33 Although Kent acknowledged the importance of collecting comprehensive epidemiological data on accidents, he also pushed county and state health departments to apply their existing knowledge to revise local building codes and to retrofit unsafe housing. Conscientious engineering could eliminate ‘loose rugs or carpeting’, ‘dark or poorly lighted hallways’, and ‘defective heating equipment’ to transform homes into ‘fool-proof’ environments.Footnote 34
Public health practitioners nevertheless resisted the object-based reasoning of sanitary engineers like Kent. In 1938, the APHA Committee on the Hygiene of Housing had published its own guidelines for safe and healthy homes, recommending fire-resistant construction, proper wiring, ventilation for all gas appliances, ample storage space, and stairs with handrails and adequate lighting.Footnote 35 Over the next dozen years, Charles-Edward A. Winslow and his team revised this list for the book Construction and Equipment of the Home (1951). The manual referred builders to the technical specifications of the National Electrical Code, Underwriters Laboratories, and the National Board of Fire Underwriters but asserted that ‘strict conformance’ to these standards would not necessarily protect the public. The committee expressed two broader objectives: to incorporate ‘automatic controls and protective devices to make unsafe practices difficult’ and to make the ‘easy’ and ‘natural’ way of doing something at home ‘as safe as possible’.Footnote 36 Few health departments put these principles into practice. As late as 1949, only fifteen state health agencies had home accident programs; three-fourths did not have any staff assigned to safety; and most stuck to data analysis and education.Footnote 37
The disconnects between behavioural, biological, and technical explanations for injuries led John E. Gordon (1890–1983), Chair of the Harvard Department of Preventive Medicine and Epidemiology, to consolidate the field with his landmark essay ‘The Epidemiology of Accidents’ (1949). Once again chastising his fellow public health experts for applying scientific methods to diseases but not to accidents, Gordon outlined four steps for the investigation of physical risks: describing the status quo with statistics, finding the causes of particular sets of injuries, piloting measures to counteract these causes, and evaluating the chosen interventions using consistent criteria. Gordon drew striking parallels between accidents and contagious illnesses, comparing the declining mortality rates of tuberculosis and non-traffic injuries, the medical timelines of a typhoid fever outbreak and a catastrophic night club fire, and the racial distributions of deaths from whooping cough and accidental suffocation. His position was straightforward: ‘Accidents as a health problem of populations conform to the same biologic laws as do disease processes and regularly evidence a comparable behavior’.Footnote 38 Borrowing from conventional epidemiology, Gordon defined accidents as the outcomes of predictable but unforeseen interactions between the ‘hosts’ who had injuries, the proximate ‘agents’ or objects responsible for these incidents, and the socio-material ‘environments’ where accidents happened. This reconfiguration of the seed-and-soil model of disease offered a handy tool to disentangle the causes of unintentional injuries.Footnote 39 Other researchers soon followed suit, placing a complex multifactor epidemiology at the centre of the next decade of accident prevention.Footnote 40
Quantifying safety: The home demonstration era
The first systematic efforts to apply the new epidemiology of accidents to communities resulted from the philanthropy of the W. K. Kellogg Foundation, which funded several projects on the causes and control of home injuries. The cereal entrepreneur William Keith Kellogg had endowed the charity following the White House Conference on Children (1930) to advance the health and welfare of children and youth.Footnote 41 From 1948 to 1952, the foundation consulted with the USPHS to award $280,000 to the health departments of Kalamazoo, Michigan; Mansfield, Ohio; San Jose, California; and Cambridge, Massachusetts, for home demonstration programs focused on accidents.Footnote 42 At the time, injuries had quietly become the leading cause of death for Americans aged 1 to 34 and had climbed from fifth to fourth overall.Footnote 43 The goals of these pilots were ambitious. The USPHS hoped to gather robust statistics on the health outcomes of home injuries, to measure the relative importance of different causes of injuries, to plan and to test innovative safety strategies and evaluation methods, and to clarify the relationships between public health practitioners and affiliated voluntary associations.Footnote 44 These programs inspired the foundation to allocate additional resources to state-level safety activities and fuelled the home safety movement into the 1950s.Footnote 45
Medical professionals had lofty expectations for these demonstrations. Leonard Board, the Chief of the USPHS Division of Sanitation, looked to the Kalamazoo program to provide the first properly controlled assessment of home injuries and their solutions.Footnote 46 The Subcommittee on Accident Prevention excitedly invited Winston B. Prothro (1911–1991), the Director of the Kalamazoo Health Department, to the 1950 meeting of the APHA to summarise his procedures and initial data. At the start of their campaign, Prothro and his staff had distributed surveys at local schools to set baseline accident rates for their planned interventions. Their multipronged project included in-service training, home visits, educational outreach, and collaborations with nonprofits such as the Boy Scouts and Girl Scouts and aimed to quantify their efficacy.Footnote 47 Following the examples of the National Tuberculosis Association Modern Health Crusade, seasonal clean-up weeks, and swat-the-fly events, officials mobilised the county against accidents with promising results.Footnote 48 Over 2 years, the regional death rate from home injuries fell from 27.1 to 13.5 per 100,000 inhabitants.Footnote 49 This 50% decline led to many similar programs. The USPHS bibliography Home Accident Prevention: Selected References (1956) catalogued thirty-six reports, handouts, and guides related to Kellogg grants.Footnote 50
Safety experts responded to the early success of the Kellogg Foundation initiatives and another comparable survey out of the University of Michigan School of Public Health with the first postwar American conference on home injury prevention. From 1951 to 1952, personnel from the University of Michigan, APHA, USPHS, and National Safety Council (NSC), a nonprofit network of industry leaders committed to occupational and transportation safety, laid out the agenda for the conference. The Steering Committee settled on four intersecting themes: data and statistical methods for studying injuries; the ‘personal and environmental factors’ tied to home accidents; the role of local health departments; and community resources available for injury control.Footnote 51 The members of the committee had unexpected difficulty planning the event, which was repeatedly delayed until January of 1953.Footnote 52 Well into October, Thomas Fansler, the Director of the Home Safety Division of the NSC, objected to replacing scripted papers with an informal ‘bull session’ on the demonstration projects.Footnote 53 The planning team eventually found a compromise between these options, mixing short talks with workshop sessions to foster active conversation. Altogether, the conference set out to modernise home accident prevention and optimistically pointed to the day when its own proceedings would become ‘as obsolete as the profound texts of medieval medicine’.Footnote 54
Otis L. Anderson of the USPHS Bureau of State Services opened the meeting with a call for ‘selective’, ‘economical’ approaches to injuries that would guarantee a ‘fair return on our investment’.Footnote 55 Moving from descriptive to analytical epidemiology, the conference considered how statistics could help experts test and implement ‘specific, rather than general, preventive measures’ for domestic hazards. Iwao M. Moriyama (1909–2006) of the National Office of Vital Statistics cited the extraordinary accomplishments of mass immunization and latched onto the prospect of finding ‘magic bullets’ for sets of injuries with the same causal mechanisms. Unlike the capacious research and education projects of the previous decade, future studies would be designed to strictly differentiate between, for example, burns resulting from ‘defective heating equipment, misuse of flammable liquids, or improper storage of combustibles’.Footnote 56 Following the insights of ‘The Epidemiology of Accidents’ and the trend within postwar biomedicine towards risk-factor analysis, the participants of the conference simultaneously tried to account for the complexity of home injuries and to quantify the extent to which certain human, material, and environmental factors influenced injury patterns. Just as the contemporary Framingham heart study went on to isolate hypertension, overweight, and smoking as significant contributors to cardiovascular disease, so too did postwar safety practitioners break down accidents like falls into clusters of events correlated with distinct risks ranging from icy driveways and rickety stairs to drunkenness and old age.Footnote 57
Reinterpreting accidents as the sums of batches of smaller probabilities led experts to pick apart the methodologies of the home demonstration movement. According to Moriyama and his collaborators, all except two of the community projects discussed at the meeting had relied on nonrandom and possibly unrepresentative samples of local households to estimate baseline injury rates and to test promising countermeasures. Hospital and insurance records, meanwhile, only reported serious injuries and did not document the experiences of different classes, age groups, ethnic and racial identities, occupations, or regions equally.Footnote 58 Until safety professionals settled on a common definition of home accidents and teased out their various causes, the conference participants insisted, the field would continue to produce skewed and partial data.Footnote 59 The results of most of the Kellogg Foundation grants – including the Kalamazoo program – were dismissed as incompatible and unreliable, driving injury researchers to gather new statistics and case reports from scratch.
The ‘risk factor’ model of home accidents set aside sweeping debates over the relative importance of human and material factors to delve into topics including child safety, accident proneness, lead poisoning, and nursing homes.Footnote 60 At the same time, this framework tended to study safety concerns in isolation instead of charting the interactions between them. The shift from the ‘shot-gun approach’ of analysing several types of home injuries at once to the ‘rifle approach of hitting major problems’ made public health interventions more cost-efficient and measurable but could also make them more reductive.Footnote 61 The actual solutions applied to these hazards, furthermore, did not always reflect the complexity or specificity of their causes. Most safety programs still revolved around educational television, radio, news stories, displays, and handouts; home inspection checklists; and in-service training for health practitioners.Footnote 62 These methods hardly deviated from those of the past 15 years and conflated mass participation with productivity. The conference proceedings affirmed, ‘The number of pamphlets distributed, or of accident hazards noted, may be useful in indicating activity, but does not measure the effectiveness of the program’.Footnote 63
At the end of the Michigan conference, its Steering Committee looked ahead to future meetings about home injury prevention but missed the central paradox of its sessions. Even as accident statistics became more comprehensive, mathematically precise, and probabilistic, the preferred strategies for controlling the risks of domestic space stayed the same. The mismatch between descriptive, quantitative studies of the epidemiology of accidents and contemporary safety campaigns widened over time. The University of Michigan survey of Washtenaw County and the second wave of Kellogg demonstration projects after 1953 illustrate these trends. The Washtenaw study, for instance, won a grant from the National Institutes of Health to interview 2,500 randomly selected families and to inspect their homes.Footnote 64 The survey set the standard for later attempts to measure the demographic, behavioural, material, and social factors associated with home injuries. The Washtenaw procedures manual supplied two hundred pages of tiered questions and code lists to turn the personal experiences and environments of its respondents into stacks of punch cards. Along these lines, two columns from the questionnaire recorded the activity happening at the moment of a recorded accident, and another eight indicated the type and condition of the kitchen stove.Footnote 65 The study accordingly opened up countless opportunities for safety engineering. Families who reported accidents were more likely to have ‘lever-blade’ can openers, temporary housing, and stoves with rear-mounted controls than others, tracing a path from education to targeted renovations and repairs (Figure 1).Footnote 66
Comparison from Washtenaw survey of kitchens with and without reported accidents (1953).

The Washtenaw survey answered several longstanding questions. First, home accidents were frequent: Washtenaw residents had around six per year, 1% of which qualified as ‘major’ incidents involving medical treatment, property damage, or disability. This rate differed widely based on age and gender. Young children had far more accidents than adults, and women over fifteen had twice as many accidents as men of the same age because they were expected to perform most of the housework.Footnote 67 Whereas homemakers were ordinarily cut or burned in the kitchen or fell down the stairs, husbands with jobs outside the home were hurt doing yardwork or slipping on the driveway.Footnote 68 The study similarly tried to determine the everyday activities, products, and infrastructure responsible for injuries. Children playing, cooking, tidying up the kitchen, laundry, and home repairs accounted for 60% of these incidents, a pattern which also drew attention to objects such as knives, architectural glass, staircases, irons, toys, and pressure cookers.Footnote 69 Other sections of the survey moved from room to room mapping potential causes of accidents. Only 30% of the inspected households had working fire extinguishers; 40% stored knives with other kitchen implements; 50% had stairs without handrails; 70% did their laundry with risky wringer washers; and 95% kept toxic chemicals indoors.Footnote 70 These results underlined the extent to which Americans put themselves at risk and pointed to product safety laws, affordable childcare, and home improvement grants as worthwhile interventions.
Nonetheless, this imposing collection of accident statistics had little impact on the ways public health professionals worked to prevent home accidents. After completing its study, the University of Michigan team concluded, ‘The nature of the injuries indicated that fundamental approaches to alleviation might well rest largely with the homemakers themselves’.Footnote 71 Despite the plausible cases for social services and government regulation of consumer technology and infrastructure, the Washtenaw program again resorted to safety education to protect regional homes. The health department correspondingly conducted a 120-day trial where public health nurses visited participating households every 2 weeks to fill out a ‘Home Hazard Check-List’ and ‘Home Safety Calendar’. These resources mobilised their users to identify and to correct dangerous conditions and to painstakingly record the causes and effects of any accidents that happened at home. A checklist copied as a reference for the Washtenaw survey contained an entry dated August 6 for a gas stove with a broken pilot light. The machine was leaking carbon monoxide, and the sample form noted that a technician had been contacted to fix the stove on August 12. The calendar, meanwhile, provided space for families to keep track of the location, time, type, inciting action, and physical and economic outcomes of every injury during the trial period.Footnote 72 This labour-intensive approach was effective, lowering the accident rate for the study group from 5.5 to 1.2 incidents per person per year.Footnote 73
The initial, calculable achievements of the home demonstration era failed to translate over longer time scales and larger geographical areas, and comparable initiatives disappeared once the Kellogg Foundation stopped funding accident prevention. Although the Washtenaw survey offered compelling evidence to hire more travelling nurses and to test whether or not subsidies for home improvement projects could reduce some injuries, its investigators mused, ‘Perhaps home safety is not a purchasable commodity’. The Washtenaw report advocated for strict building codes, routine housing inspections, fireproof construction, and safer consumer goods but did not propose any solutions to make these proven countermeasures more widely available.Footnote 74 Even the Washtenaw pilot, which pared these options down to expert inspections and safety training and relied on the cooperation of motivated homemakers, only assisted 95 families for 4 months.Footnote 75 Many accident prevention programs consequently fell back on the blanket outreach of the previous decade. The San Jose, CA, and California State campaigns, for example, combined educational material for teachers, professors, state officials, and extension agents; displays and announcements for holidays and fire prevention week; continuous media coverage; and do-it-yourself home safety questionnaires and checklists.Footnote 76 Commenting on the inability of the California State Department of Health to help other officials do more to control injuries, Gilbert Rhodes conceded, ‘Unfortunately, lack of staff time has meant that numerous requests have had to be left unfilled’.Footnote 77 The home demonstration movement, then, sought to turn communities into laboratories to isolate and to combat specific hazards but fixated on the accumulation of ever-more granular data.Footnote 78
Unmet expectations at the U.S. Public Health Service
Although the U.S. Public Health Service launched its home accident program fewer than 5 years after the APHA, the national government stayed on the sidelines of injury prevention until the 1950s. Under the leadership of sanitary engineer Frederick Kent and nursing specialist Madeline Pershing (1906–1988), the USPHS confined itself to compiling and distributing safety education resources and to delivering technical assistance to projects outside the agency. From 1947 to 1950, Kent and Pershing collaborated with the APHA and National Publicity Council to prepare exhibits and portfolios for public health professionals, who could then pass on helpful materials to their own communities.Footnote 79 The USPHS not only operated as a clearinghouse for the logistical information necessary to administer local safety projects but also provided advice to the public. The booklet ‘There’s No Place Like Home’ illustrated the causes of accidents with a drawing of a house filled with dangerous situations. These object lessons ranged from children taking pills from an unlocked medicine cabinet to adults falling down the stairs, using electrical devices in the bathtub, and dropping lit cigarettes on the floor (Figure 2).Footnote 80 Kent and Pershing insisted on the preventability of home accidents but left potential interventions to ‘local government and private voluntary organizations’.Footnote 81
Drawing of risky behaviours and conditions from USPHS home accident prevention booklet (1950).

The overreliance of the USPHS on businesses, nonprofits, and municipal health boards resulted from the precarious position of home injury prevention in the agency and the policies governing its official interactions with nonstate institutions. Over the first decade of the USPHS home accident section, Kent and his overtaxed staff were unceremoniously transferred within the Bureau of State Services from the Division of Sanitation to its short-lived ‘Special Projects’ Division and finally to the new Division of Special Health Services.Footnote 82 The second-class size and status of the program influenced its mission, which left out costly initiatives to counteract the effects of ‘housing quality’ on injuries or to advocate for laws regulating building construction and consumer products.Footnote 83 Whereas Americans had already taken decisive steps to pass and to enforce sweeping and sometimes intrusive rules for infectious disease control, workplace and transportation safety, and the healthfulness of foods, drugs, and cosmetics, this logic was not applied to home injuries.Footnote 84 The strategic choice to set aside the social, economic, and political dimensions of these accidents had serious downsides. The USPHS reinforced the tendency to think of home injuries as problems of improper education or faulty engineering rather than as the results of complex social systems. Within this framework, the USPHS staff who worked on private standards committees could voice their opinions on safety guidelines but did not have the authority to dictate industry decisions.Footnote 85 The search for more and more scientific ways to quantify risks and to assess safety programs reflected the deeper ambivalence of the state as well as the advantages of epidemiological methods.
Against the backdrop of the home demonstration movement and the rising demand for community safety programs, the USPHS compiled its own list of known hazards, activities, and references related to injuries. This multiyear project led to Home Accident Prevention: A Guide for Health Workers (1953), which set out to ‘extend the frontiers of preventive medicine’ into the private sphere and, eventually, to train every civic-minded American to be ‘his own health worker in the prevention of accidents’.Footnote 86 Like the previous manuals of the APHA Committee on the Hygiene of Housing, the USPHS guide promoted homes set up to minimise the risks of falls, collisions, shocks, and house fires; constructed using durable and flame-resistant materials; and outfitted with appliances able to meet the standards of Underwriters Laboratories (UL) and the American Gas Association.Footnote 87 Kent and Pershing also documented how mental states; blindness, deafness, chronic illnesses, and other impairments; accident proneness; and age contributed to injuries.Footnote 88 Although the handbook drew on the expertise of architects, engineers, and medical practitioners to describe these factors, its practical solutions centred on instructing families to keep themselves safe with state-of-the-art practices and equipment. Unsurprisingly, the USPHS was less willing to spearhead stricter laws and expanded social services to help members of the public actually follow its advice.
The next several chapters of the guide covered specific classes of injuries and provided modules for safety campaigns with few resources and personnel. The section titled ‘Accidents Due to Falls’, for example, described the leading causes of falls and proposed safety measures including keeping walkways clear; designing staircases with adequate lighting, level steps, and handrails; marking abrupt changes of elevation; storing belongings less than 6 feet off the floor; and using stepstools for housework. Most of the community programs from the chapter were educational, bringing together interested residents to discuss fall prevention, to review local accident reports, and to watch safety films. The handbook also emphasised cooperation between government agencies, companies, and nonprofits. Kent and Pershing prodded public health officials to coordinate with commercial retailers to advertise non-skid wax and traction strips.Footnote 89 The guide similarly invited electrical inspectors to explain the role of private standards institutions like UL and to remind citizen-consumers to buy certified devices.Footnote 90 Writing to Kent about the overwhelming scope of the manual, Charles Spangler of the Communicable Disease Center wryly joked, ‘If one attempted to carry out all of the suggestions made in this Guide he would probably have to quit work’.Footnote 91
Public health experts believed the epidemiology of accidents would narrow down this unwieldy array of risks and prospective safety strategies. Apologising for the breadth of Home Accident Prevention and the labour intensiveness of its advice, Kent and his team nevertheless committed to listing ‘all the safety features we know of’ until the Washtenaw program could identify ‘the major environmental factors’ affecting contemporary families and quantify their influence on ‘accident causation’.Footnote 92 Safety training and physical rehabilitation, Kent asserted, were only two dimensions of home safety, which had to strike a balance between ‘education’ and ‘protection’. As Halbert Dunn of the National Office of Vital Statistics had indicated three years earlier, analytical epidemiology would hypothetically help public health officials pinpoint the objects responsible for accidents and move away from the unscientific model of traditional safety campaigns.Footnote 93 These aspirations were overoptimistic. The inconsistent procedures of the home demonstration movement kept experts from agreeing on the principal causes of injuries and the ideal means to counteract these causes.
Confusion around the technical definition, categorisation, and measurement of ‘home accidents’ led to the Uniform Definitions of Home Accidents Conference of 1957. Participants from the NSC, APHA, and USPHS critically reevaluated the existing systems of the NSC and the International Classification of Diseases (ICD), which sorted injuries based on location. The NSC scheme included traffic, workplace, home and farm, and public accidents and split these groups apart using types of injuries (e.g. burns) and their proximate causes (e.g. boilers).Footnote 94 The ICD and USPHS separated transportation from non-transportation accidents and then accounted for the agent of the injury and where the injury took place.Footnote 95 Neither of these longstanding frameworks explained how to count nonfatal accidents, to demarcate the boundaries of domestic space, or to analyse how multiple interwoven factors contributed to most accidents. These shortcomings seriously compromised the usefulness of available injury data and threatened to invalidate the quantifiable results of future home safety initiatives: ‘It is not enough to say that a program is being designed to prevent accidents without specifying in definite terms the kinds of accidents and the level of severity concerned’.Footnote 96
Unlike the ICD and similar injury reporting systems, the Uniform Definitions Conference did not try to categorise accidents.Footnote 97 Returning to the epidemiological theories of John Gordon, Iwao Moriyama and his colleagues set out to consolidate ‘the entire subject of accidents’ with the model of ‘accident sequences’.Footnote 98 This scheme added time to the older framework of hosts, agents, and environments and reimagined accidents as multidimensional processes rather than as instantaneous events with thin contexts. Home accidents did not ‘just happen’ – ‘suddenly, without warning, and without much rhyme or reason’ – but were predictable outcomes of the ‘operation of well-known physical laws (combustion, pull of gravity, interaction of forces, etc.)’ following from risky actions and conditions.Footnote 99 The conference participants consequently broke accidents down into four layers: the ‘background factors’ affecting the probability of injury or property damage, the ‘initiating factors’ behind a specific incident, the ‘intermediate factors’ driving a chain of events towards a harmful endpoint, and the ‘immediate factors’ or ‘trigger mechanism’ at the exact moment of the accident (Figure 3).Footnote 100 Shocks involving hair-dryers, for example, sometimes happened when these machines were knocked into a bathroom sink but were also tied to contexts such as operating electrical devices around water, unreliable shut-off switches, and fleeting distractions like a telephone ringing down the hall.
Diagram of accident sequences from Uniform Definitions of Home Accidents Conference (1958).

Accident sequences stitched together human and engineering factors but unfortunately overlooked the social, economic, and political determinants of safety. Public health authorities asserted that home injury prevention was only possible with the cooperation of ‘alert, trained, unhandicapped adults’ who had the resources and motivation to keep themselves ‘reasonably safe’.Footnote 101 Automatic fail-safes would protect these idealised citizen-consumers from momentary lapses of attention and unexpected mechanical failures. Along these lines, safety professionals had two overlapping roles: to decrease the ‘accident susceptibility’ of ordinary Americans and the ‘accident potential’ of their housing and infrastructure.Footnote 102 This two-pronged approach was cohesive but tended to flatten the ‘environmental’ causes of injuries to physical conditions like darkness, ice, frayed wiring, and cluttered stairs. The final report of the conference pointed out the ways improper housekeeping could lead to accidents but did not address how the unequal division of domestic labour based on class and gender or the cost of safer appliances and safety equipment might contribute to injuries. Most experts perceived middle-class, white, suburban families as the intended target of accident prevention and discounted the challenges of home safety as a day-to-day practice.Footnote 103 At any point from the most remote causes of an accident to the ‘point of no return’ where harm became inevitable, the report affirmed, ‘control may be restored’ and ‘the flow of events reversed’.Footnote 104
Despite these early efforts to systematise injury prevention, government programs to control home accidents declined from the late 1950s to 1960s. Under the leadership of Ralph Longaker and James L. Goddard, the USPHS temporarily budgeted $55,000 per year for housing rehabilitation, released two handbooks condensing its Guide for Health Workers, and founded the National Clearinghouse for Poison Control Centers (1957).Footnote 105 The agency continued to view its role as coordinating the flow of expertise between safety experts, corporations, nonprofits, and health departments. Funding for new projects, meanwhile, shifted towards motor vehicle injuries. Even after the USPHS finally cobbled together its Division of Accident Prevention in 1961 and increased its annual budget from $318,000 to $4,350,000 over the following decade, the agency allocated less than 25% of these totals to non-transportation accidents.Footnote 106 The few home safety projects within this portfolio focused on the collection and interpretation of injury statistics and the timely delivery of emergency services.Footnote 107 Public health professionals reacted differently to these changes. Ross McFarland and Albert Chapman directed their colleagues to look more closely at the ‘physical, physiological, and psychological status of people who have accidents’.Footnote 108 William Haddon and other practitioners of the coalescing field of biomechanics, conversely, devised the energy transfer theory of injuries, casting accidents as technoscientific problems with technoscientific solutions.
From accident sequences to biomechanics
Around the same time as the home demonstration movement, another group of safety practitioners took up mechanical engineering to shield drivers and passengers from high-speed collisions. Following the pilot Hugh DeHaven (1895–1980), who attributed most fatalities from crashes to unsafe ‘structural environments’, these investigators tried to minimise the damage when accidents did happen.Footnote 109 The surgeon John Paul Stapp, for example, experimented with animals and propulsion sleds to test the physiological effects of rapid deceleration.Footnote 110 DeHaven similarly proposed ways to ‘package’ bodies inside cars to reduce the 600,000 injuries per year involving speeds slower than forty miles per hour.Footnote 111 The historian of technology Lee Vinsel has shown how this agenda broadened from improving the ‘crashworthiness’ of motor vehicles to pushing for federal regulation of automobiles and roadways.Footnote 112 This transition from preventing risks to controlling the likelihood and severity of injuries across the different phases of accident sequences gradually crossed over to home safety. Physicians such as Julian Waller (1932–2022) contended that the makeup of housing and consumer products not only caused accidents but also impacted the degree of physical trauma related to their use and misuse. Case reports and epidemiological studies about architectural glass, unsafe toys, and flammable fabrics indicated the extent to which measures like tempering sliding glass doors or fireproofing furniture could protect Americans who passed the ‘point of no return’.Footnote 113
The resulting effort to control the physical outcomes of accidents rested on the ‘energy transfer’ theory of injuries. Mostly neglecting the complementary projects of postwar sanitary engineers to design spaces and equipment with fewer risks, the traffic safety specialist William Haddon denounced the term ‘accident’ and reinterpreted injuries as the effects of ‘abnormal energy exchanges’ between bodies and their surroundings. This physicochemical approach to injuries would allow public health to move past the epidemiology of accidents, which Haddon believed had overstated the causal complexity of injuries and led to the proliferation of ‘trivia’ about particular risk factors and their statistical distribution. Drawing together impacts, burns, shocks, asphyxiation, poisoning, and irradiation as comparable types of damage at the cellular and tissue levels, Haddon emphasised the commonalities between different injuries.Footnote 114 At the same time, he applied the model of accident sequences to break down injury control into four processes: stopping dangerous accumulations of energy, containing the release of this energy, keeping individuals away from sites of energy exchange, and mitigating the outcomes of these exchanges on their casualties.Footnote 115 Children could be protected from the thermal energy of space heaters, for example, if these devices were replaced with central heating; built with automatic thermostats and emergency shut-off switches; set up away from play areas and walkways; and equipped with heat-resistant grates. According to Haddon, preventing accidents was only one aspect of the mission to keep Americans safe.
Biomechanics and the science of abnormal energy exchanges provided the conceptual basis for the landmark collection Accident Research: Methods and Approaches (1964). Haddon and his coeditors complained about the ‘older literature’ centred on ‘counting’ injuries and categorising their ‘manifold factors’ and set out to reconfigure injury prevention using physics and chemistry.Footnote 116 Despite his scepticism about traditional epidemiological studies of accidents, Haddon referred to this research to explain how specific types of energy could be destructively released into their sociotechnical environments. Rather than treating slippery floors or running down the stairs as root causes of injuries, Haddon analysed the ways these objects and actions could lead to unintended exchanges of kinetic energy. Unlike its countless sources, this energy had measurable effects on the body and was a necessary and sufficient cause of physical harm, closing the conceptual gap between the etiologies of accidents and infectious diseases.Footnote 117 For Haddon and his collaborators, the reasons why bones were more or less likely to break under certain circumstances mattered as much as whether fractures resulted from collisions, falls, or violence. Haddon correspondingly rejected the assumption ‘that accidents are largely – even exclusively – a problem of human behavior’ and pushed for fail-safe engineering and efficient emergency services as the most promising means to control injuries.Footnote 118 Against the receptive backdrop of the political controversy around Ralph Nader and his classic Unsafe at Any Speed (1965), public health professionals paid increasing attention to the principles of biomechanics and to transportation safety.Footnote 119
These trends motivated the USPHS to try to expand its authority over accidents during the mid-1960s. Sketching the narrow scope of its activities to justify its unprecedented budget request for the 1966 fiscal year, the restructured Division of Accident Prevention called on the Surgeon General and the Department of Health, Education, and Welfare (DHEW) to spend $30 million over ten years for a 250,000 square-foot Accident Prevention Research Laboratory with 1,000 staff.Footnote 120 This state-of-the-art installation would permit the agency to modernise its work based on the goals, methods, and equipment of contemporary biomechanics. The proposal for the site included a test track, driving simulators, motion capture assemblies to study collisions, workshops to reengineer risky technology, and biomedical laboratories to investigate physical trauma.Footnote 121 Before the agency could move forward with the centre, however, DHEW Secretary Anthony Celebrezze objected to its cost. His office invited the USPHS to appoint a task force to plan a ‘more modest initial phase’ for its anticipated future injury control programs.Footnote 122 Under the leadership of James Goddard and Ross McFarland, this team advised DHEW to allocate $10 million and 380 personnel to the facility. Unless the agency provided the resources to unravel the ‘crazy-quilt’ of almost three decades of injury data, ‘man must continue to submit to the tyranny of accidents – just as he once did for disease’.Footnote 123
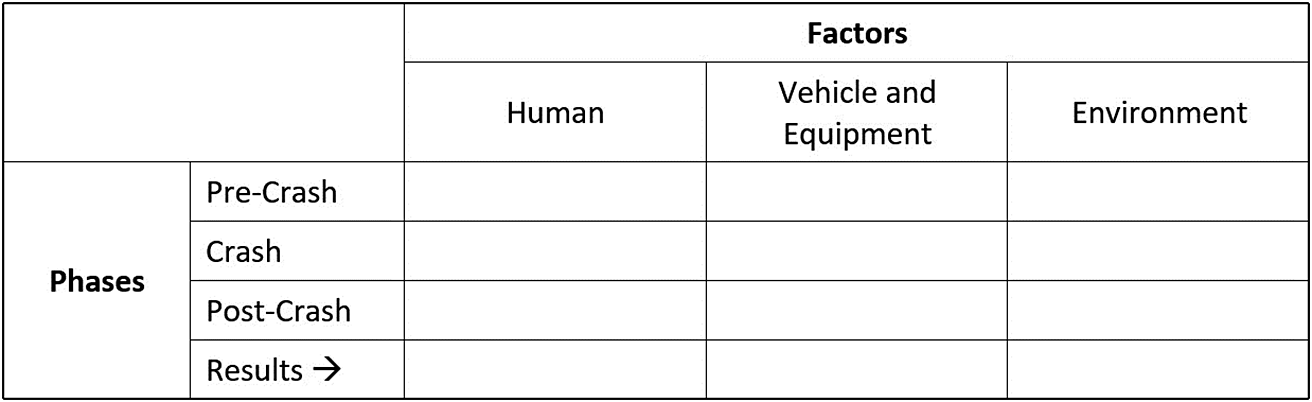
This reasoning failed to convince DHEW, which unexpectedly rejected the scaled-down proposal from the task force and shunted the USPHS out of the safety movement for the next 20 years.Footnote 124 Without the counterweights of the Kellogg Foundation and the USPHS, injury control shifted decisively from domestic space to transportation systems and from community education to mechanical fail-safes. Haddon contributed to these trends throughout the 1970s, when he reintegrated the conventional epidemiology of accidents into his model of abnormal energy exchanges to formulate the Haddon matrix. This influential scheme broke down motor vehicle crashes into human, vehicle and equipment, and environment factors and charted the compounding results of these factors before, during, and after a collision (Figure 4). The Haddon matrix stretched the dimensions of epidemiological analysis over time and led Haddon to expand his earlier scheme of four injury prevention strategies to a set of ten countermeasures.Footnote 125 Despite the applications of this framework to home safety, Haddon and his colleagues overwhelmingly focused on car crashes, especially the deadly ‘second impacts’ when people collided with the interiors of their vehicles. Although injury specialists such as Haddon, Waller, and Susan Baker often referred to home accidents to explain their methods, the risks of housing and consumer products faded into the background.Footnote 126
Haddon matrix after highway safety article from The Journal of Trauma (1972).

Public health experts eventually found themselves on the sidelines of the campaign to protect citizen-consumers at home. The National Commission on Product Safety (1968–1970), the precursor to the Consumer Product Safety Commission (CPSC), featured physicians, public health practitioners, and employees of the DHEW and USPHS but looked to other stakeholders for its actual recommendations. When Senate staffer and later Chairman of the Federal Trade Commission Michael Pertschuk (1933–2022) remembered the parties responsible for the turn from industry self-regulation to government authority over risky goods, medical professionals did not even make the list.Footnote 127 After the CPSC set up its Bureau of Epidemiology to track and to analyse product-related injuries, moreover, critics of the agency repeatedly contested its data collection and risk assessment methods. New statistics and equations tended to open debates instead of resolving them and sometimes distracted regulators from formulating standards or recalling or banning dangerous items from the market. The readiness of the CPSC to act on its findings nevertheless contrasted starkly with the tepid approach of the USPHS. Whereas prior government-backed studies of home accidents had uncovered ‘academically interesting’ but ‘relatively useless’ patterns, the work of the CPSC had immediate and measurable effects on U.S. communities.Footnote 128 The pursuit of epidemiological precision, some observers indicated, had slowed the translation of injury research into policy.
Conclusion
Reflecting on the shift from conventional accident prevention to modern injury control during the 1970s, Julian Waller wrote a satirical fable expressing why safety had once been the ‘ugly duckling’ of public health. Since the turn of the century, experts had supposedly tried to decrease accidents with ‘monotonous moralistic mumbling about acts of God’, ‘carelessness’, and ‘sinful behavior’. Biomechanics, fail-safes, and emergency medicine promised to lead the field out of this metaphorical Dark Age: ‘A band of wisest gurus came around. They were called scientists. And they said, “Accident Prevention has only one attribute because of poor nutrition, not congenital deformity. If you wish it to mature you must stop feeding it prescientific garbage”’.Footnote 129 According to Waller, injury control had finally become a coequal branch of public health alongside the control of infectious and chronic diseases. The launch of the Injury Control and Emergency Health Services Section of the APHA (1972) and the proliferation of research on injuries offered reasons for optimism about the directions of home and traffic safety. At the same time, internal disagreements between public health professionals over the epidemiology of accidents and the repeated failures of public health institutions and the government to designate enough resources to injury prevention impeded its progress. Injury science added new tools to identify, to classify, to measure, and to counter the numerous factors related to home accidents but did not turn the resulting flood of information into long-term, scalable interventions. Epidemiology, risk analysis, and biomechanics methodically attributed injuries to specific causes but – at least for home safety – revised the terms of accident prevention from what to do about accidents to how to collect and to interpret injury data.
The histories of home safety and the epidemiology of accidents complicate progressive narratives about the efforts of public health authorities to reduce injuries during the twentieth century, underscoring the disconnects between scientific models and the applications of these models. Like other sciences of attribution, the epidemiology of accidents strove to quantify the absolute, relative, and cumulative impacts of the assortment of causal factors associated with unintended injuries. The ‘new’ public health, risk-factor medicine, and biomechanics provided multiple methods to achieve this objective but were less successful at putting their theoretical and mathematical insights into practice. Until the mid-1960s, home accident prevention often boiled down to directing homemakers to find and to remove familiar domestic hazards and to buy safe goods. As the burdens of proof for systems-level countermeasures ratcheted upwards and safety specialists turned to the less contested and more straightforward task of improving road safety, home injuries largely remained a personal responsibility. Even after the Consumer Product Safety Act of 1972 authorised the CPSC to regulate the market with mandatory safety standards, warnings about dangerous products, and recalls, the role of the state was narrowly construed as one of education and enforcement. The social infrastructure designed to protect Americans from communicable illnesses, environmental toxins, and the physical risks of public and corporate spaces was rarely extended to private homes.
Groups including the National Center for Injury Prevention and Control (NCIPC) and the Johns Hopkins Center for Injury Research and Policy (CIRP) have piloted an array of accessible, cost-effective, evidence-based programs to prevent home injuries, but these programs are still confined to a small handful of communities. The Community Aging in Place – Advancing Better Living for Elders (CAPABLE) initiative, for example, helps disabled seniors renovate their homes to lower the risk of falls, trains them to fall safely, and provides on-site assistance from nurses and physical therapists. Despite a decade of results demonstrating the efficacy of the program, however, CAPABLE only covers thirty sites and a few thousand participants nationally.Footnote 130 Public health experts have also had trouble tightening outmoded laws concerning the safety of rental properties, prescription medication, cars, firearms, and consumer products.Footnote 131 Although safety practitioners have challenged policymakers and the public to reimagine U.S. society with ‘zero tolerance for the occurrence of preventable injuries’, the healthcare system, research centres, and the government allot thousands of times more money to cancer and heart disease than to injuries.Footnote 132 The epidemiological dream of discovering ‘magic bullets’ for the leading causes and effects of accidents has trapped us into a false choice between searching for ideal, quantifiable solutions and settling for imperfect ones. Injuries are neither too expensive nor too complex to be controlled. Accident research will continue to reinvent itself, but the mission of home safety cannot wait for the ‘science’ of injuries to be settled.
Acknowledgements
The author would like to thank Lukas Engelmann, John Nott, Michael Healey, and the other participants of the Data and Disease in Historical Perspective workshop for their feedback on this project. The author would also like to thank Sue Baker, Wendy Shields, and the three anonymous reviewers for helping strike a balance between the interests and prior knowledge of public health practitioners and historians of medicine.
Disclosures
The author has no conflicts of interest to disclose.




 Open access
Open access