


Introduction
Dementia is an umbrella term encompassing a variety of disorders affecting the brain and causing symptoms that include impaired memory, language, cognitive skills, personality, perception, and overall functioning (World Health Organization, 2023). These impairments can result in profound changes not only for those who have received a diagnosis but also for family and friend care partners. Because each person’s experience with dementia is unique, the journey from recognizing early symptoms to living with a diagnosis varies widely. Systematic reviews consistently report barriers to seeking a dementia diagnosis, such as symptom normalization, fear, stigma, denial, and low perceived need for receiving a diagnosis (Hicks et al., Reference Hicks, Wheatley, Porter, Farina and Banerjee2025; Parker et al., Reference Parker, Barlow, Hoe and Aitken2020). Facilitators include recognition of accumulating symptoms, support from informal networks, and prior knowledge or contact with dementia resources (Hicks et al., Reference Hicks, Wheatley, Porter, Farina and Banerjee2025; Parker et al., Reference Parker, Barlow, Hoe and Aitken2020). Reviews further highlight cultural, linguistic, socioeconomic, and systemic factors influencing timely help-seeking (Hicks et al., Reference Hicks, Wheatley, Porter, Farina and Banerjee2025). Multiple studies have also identified systemic barriers to timely and supportive diagnosis, which included clinicians’ lack of confidence and training (Iliffe et al., Reference Iliffe, Koch, Jain, Lefford, Wong, Warner and Wilcock2012; Mason et al., Reference Mason, Annear, Lo, McInerney, Tierney and Robinson2016), time pressures in primary care (Aminzadeh et al., Reference Aminzadeh, Molnar, Dalziel and Ayotte2012), fragmented services (Wheatley et al., Reference Wheatley, Bamford, Brunskill, Booi, Dening and Robinson2021), and healthcare workforce shortages (Wheatley et al., Reference Wheatley, Bamford, Brunskill, Booi, Dening and Robinson2021). In addition, evidence shows that diagnostic experiences are shaped by social position in society and cultural background. Ethnic minority groups face additional barriers due to stigma, cultural perceptions of dementia, language barriers, and mistrust of health systems (Kenning et al., Reference Kenning, Daker-White and Blakemore2017; Stephan et al., Reference Stephan, Bieber and Hopper2018). Stigma is a powerful influence throughout the diagnostic journey. Fear of labelling contributes to delayed help-seeking (Parker et al., Reference Parker, Barlow, Hoe and Aitken2020; Werner, Reference Werner and Corrigan2014), reluctance to disclose a diagnosis (Karnieli-Miller et al., Reference Karnieli-Miller, Werner, Aharon-Peretz, Sinoff and Eidelman2012), and underuse of supportive services post-diagnosis (Phillipson et al., Reference Phillipson, Jones and Magee2014).
Qualitative research indicates diverse emotional responses to receiving a dementia diagnosis. A recent qualitative study found that individuals who received a diagnosis often experienced a sense of relief, clarity, and validation, as well as apprehension about losing dignity and autonomy (Molvik et al., Reference Molvik, Kjelvik and Selbæk2024). These findings align with earlier work demonstrating that receiving a diagnosis can reduce anxiety and facilitate acceptance among people living with dementia (Wheatley et al., Reference Wheatley, Bamford, Brunskill, Booi, Dening and Robinson2021). However, across other studies, diagnosis was experienced as a complex and often ambivalent milestone. For many, receiving a diagnosis provided validation and explanation for troubling symptoms (Kitwood, Reference Kitwood1997; Molvik et al., Reference Molvik, Kjelvik and Selbæk2024). However, it also carried fear, stigma, and uncertainty about the future (Bacsu et al., Reference Bacsu, Spiteri, Nanson, Rahemi, Webster, Norman and Stone2024; Werner, Reference Werner and Corrigan2014). Those undiagnosed tended to normalize cognitive changes and experience less distress but often missed opportunities to seek support (Molvik et al., Reference Molvik, Kjelvik and Selbæk2024).
The concept of a ’timely’ diagnosis has been contested (Dhedhi et al., Reference Dhedhi, Swinglehurst and Russell2014; Parker et al., Reference Parker, Barlow, Hoe and Aitken2020), with both patients and clinicians recognizing that the ’right time’ depends on the readiness of individuals and families to process the news. Moreover, how a diagnosis is delivered shapes whether it is experienced as empowering or traumatic. Studies of memory clinic interactions highlighted tensions in the disclosure process, particularly when care partners wished to shield the person with dementia from the diagnosis (Karnieli-Miller et al., Reference Karnieli-Miller, Werner, Aharon-Peretz, Sinoff and Eidelman2012). Compassionate, clear, and person-centred communication was identified as critical to support acceptance and adjustment (Bamford et al., Reference Bamford, Lee, McLellan, Poole, Harrison-Dening, Hughes and Exley2018; Molvik et al., Reference Molvik, Kjelvik and Selbæk2024).
Following diagnosis, there is often dissatisfaction with post-diagnostic care. A qualitative study conducted in the UK and Wales identified 20 distinct components of good post-diagnostic support spanning themes such as timely needs assessment, emotional well-being, practical support, and integration of services (Bamford et al., Reference Bamford, Wheatley, Brunskill, Booi, Allan and Banerjee2021). However, inequalities persist in service delivery due to resource constraints, rigid eligibility criteria, and inconsistent professional training (Bamford et al., Reference Bamford, Wheatley, Brunskill, Booi, Allan and Banerjee2021). A consistent theme across international studies is that receiving a diagnosis often marks the beginning of new challenges rather than resolution (Bamford et al., Reference Bamford, Wheatley, Brunskill, Booi, Allan and Banerjee2021; Hevink et al., Reference Hevink, Wolfs, Ponds, Doucet, McAiney, Vedel and de Vugt2023). Many people with dementia and care partners report being left to navigate services alone with little guidance or structured follow-up (Hagan, Reference Hagan2020; Prorok et al., Reference Prorok, Hussain, Horgan and Seitz2017). Research conducted across multiple countries demonstrates both shared challenges and context-specific barriers. In high-income contexts, the challenge is often poor care coordination and lack of continuity (Bamford et al., Reference Bamford, Wheatley, Brunskill, Booi, Allan and Banerjee2021; Wheatley et al., Reference Wheatley, Bamford, Brunskill, Booi, Dening and Robinson2021), while in low- and middle-income settings, limited resources, lack of culturally appropriate tools, and reliance on informal care shape diagnostic processes (Bernstein Sideman et al., Reference Bernstein Sideman, Al-Rousan, Tsoy, Piña Escudero, Pintado-Caipa, Kanjanapong and Possin2022). Across contexts, early and supportive diagnosis and post-diagnosis care is consistently identified as a gateway to better overall care experience, planning, and quality of life.
Structural inequities also impact younger people with dementia, rural populations, and those with lower socioeconomic status. In the Canadian context specifically, these disparities were further exacerbated during the COVID-19 pandemic (Giebel et al., Reference Giebel, Sutcliffe, Darlington-Pollock, Green, Akpan, Dickinson and Gabbay2021; Lemay-Compagnat et al., Reference Lemay-Compagnat, Couturier and Rojas-Rozo2025; McAiney et al., Reference McAiney, Conway, Koch, Middleton, Dupuis, Keller and Boger2021). The COVID-19 pandemic had a disproportionate impact on people living with dementia and care partners in Canada. Service suspensions, delayed assessments, restricted visitor access to long-term care homes, and the widespread shift to virtual care created additional barriers to timely diagnosis and ongoing support (Cetin-Sahin et al., Reference Cetin-Sahin, Godard-Sebillotte and Bronskill2025; McAiney et al., Reference McAiney, Conway, Koch, Middleton, Dupuis, Keller and Boger2021). Social isolation intensified, particularly for those in institutional settings or relying on in-home community supports (Bacsu et al., Reference Bacsu, Spiteri, Nanson, Rahemi, Webster, Norman and Stone2024; Giebel et al., Reference Giebel, Sutcliffe, Darlington-Pollock, Green, Akpan, Dickinson and Gabbay2021), while stigma and social exclusion further affected both diagnosis and care (Bacsu et al., Reference Bacsu, Spiteri, Nanson, Rahemi, Webster, Norman and Stone2024). A recent intersectional analysis demonstrates how overlapping disadvantages (e.g., gender, ethnicity, class) compound these challenges (Hicks et al., Reference Hicks, Wheatley, Porter, Farina and Banerjee2025). Reports from the COGNISANCE (Co-designing Dementia Diagnosis and Post-diagnosis Care) and PriDem (Primary-care Led Post-Diagnostic Dementia Care Program) projects emphasize the importance of ongoing, relational, and personalized post-diagnostic support, including emotional, informational, and practical assistance (Bamford et al., Reference Bamford, Wheatley, Brunskill, Booi, Allan and Banerjee2021; Hevink et al., Reference Hevink, Wolfs, Ponds, Doucet, McAiney, Vedel and de Vugt2023).
Care partners play a central role in seeking and responding to a dementia diagnosis. Diagnosis often marks the point at which care partners assume a formalized advocacy role (Macdonald et al., Reference Macdonald, Martin-Misener, Weeks, Helwig, Moody and MacLean2020; Shi et al., Reference Shi, Wang, Yoo, Karkar and Saha2025). Spousal care partners consistently describe a profound sense of loss of the relationship, identity, and the partner they once knew, while undergoing continuous adaptation in the context of dementia care (Macdonald et al., Reference Macdonald, Martin-Misener, Weeks, Helwig, Moody and MacLean2020). Systematic reviews focusing on spousal/partner care partners identify themes of uncertainty, unpredictability, and the emotional burden of caregiving demands (Macdonald et al., Reference Macdonald, Martin-Misener, Weeks, Helwig, Moody and MacLean2020). Care partners often report needing to ’fight’ for services (Prorok et al., Reference Prorok, Hussain, Horgan and Seitz2017), highlighting gaps between policy commitments and everyday realities of care delivery. While some describe relief in having a diagnosis, many feel overwhelmed by new responsibilities and by the lack of clear support structures. Studies report that care partner well-being and preparedness are deeply intertwined with the quality of the diagnostic process (Gilhooly et al., Reference Gilhooly, Gilhooly, Sullivan, McIntyre, Wilson, Harding and Crutch2016; Prorok et al., Reference Prorok, Hussain, Horgan and Seitz2017). Recent studies emphasize mental health burdens in care partners; for example, a 2025 qualitative study interviewing 25 family care partners found a trajectory of evolving mental health needs over the caregiving journey, with care partners calling for stage-sensitive and personalized supports (Shi et al., Reference Shi, Wang, Yoo, Karkar and Saha2025).
While numerous studies explore either diagnostic experiences or post-diagnostic support, few integrate both perspectives across multiple jurisdictions while triangulating the voices of people living with dementia and care partners. This study is part of the COGNISANCE (Co-designing Dementia Diagnosis and Post-diagnosis Care) project, which is an international research project co-led by teams in Canada, Australia, the Netherlands, the United Kingdom, and Poland. The overall objective of COGNISANCE is to design, implement, and evaluate an awareness campaign that will improve how health and social care providers communicate a dementia diagnosis and support people living with dementia and care partners post-diagnosis. The current study draws from Phase 1 of COGNISANCE (the needs assessment phase), which involved surveys and interviews of people living with dementia, care partners, and people involved with the dementia diagnostic process. The COGNISANCE needs-assessment approach addressed this gap by combining surveys and qualitative interviews across five countries, directly targeting barriers and facilitators to diagnosis and support from both people living with dementia and their care partners (see Hevink et al., Reference Hevink, Wolfs, Ponds, Doucet, McAiney, Vedel and de Vugt2023). Information about the larger study design and procedures is described in the Methods section.
The purpose of this study was to explore: (a) the experiences of the diagnostic process and post-diagnostic support among persons living with dementia and care partners in Canada and (b) the barriers, facilitators, and gaps related to receiving a dementia diagnosis and post-diagnostic support. As such, this study sought to address the following research question: What are the experiences (including gaps, barriers, and facilitators) of the diagnostic process and post-diagnostic support for people with dementia and care partners in Canada?
Methods
Study context and design
This study was part of a broader, multi-phase international project (COGNISANCE) resulting in the Forward with Dementia website and campaign (see: forwardwithdementia.org). The focus of this paper is on the Phase 1 needs assessment that involved interviewing people with dementia and care partners about their experiences with the diagnostic process and post-diagnostic support in Canada. This paper reports on a qualitative descriptive study design, which is suited to capturing participants’ experiences, perspectives, and perceptions in straightforward, descriptive language that closely reflects the data (Sandelowski, Reference Sandelowski2000). Qualitative description is particularly appropriate where the research aims to identify patterns across participants’ experiences without imposing theoretical abstractions and to inform health practice and policy with accessible, practice-relevant findings (Sandelowski, Reference Sandelowski2000). This study was reviewed by and received research ethics clearance from the University of Waterloo (REB #41423), The University of New Brunswick (Horizon Health Network REB #100560, Vitalité Health Network REB #100858, University of New Brunswick REB #057-2019), and McGill University (IRB #A09-B70-20A). All participants provided informed consent verbally.
Sampling and recruitment
Purposive sampling was used to recruit participants who had direct experience with the dementia diagnostic process, either as a person living with dementia or as a care partner. Purposive sampling is a non-probability approach whereby participants are intentionally selected because they possess characteristics or experiences relevant to the research question (Palinkas et al., Reference Palinkas, Horwitz, Green, Wisdom, Duan and Hoagwood2015). This approach is appropriate for qualitative descriptive studies where the goal is to maximize the relevance and richness of information rather than statistical representativeness (Palinkas et al., Reference Palinkas, Horwitz, Green, Wisdom, Duan and Hoagwood2015). Participants were recruited across three Canadian provinces (New Brunswick, Quebec, and Ontario) using social media, research networks, and in-person recruitment at key community locations. Recruitment channels included posts through the COGNISANCE project’s Canadian networks, local Alzheimer Society chapters, and community partner organizations. Participants were invited to take part in interviews via social media and local networks. Data collection took place between 2020 and 2022, during the COVID-19 pandemic, which shaped the context and content of participants’ experiences.
Data collection procedure
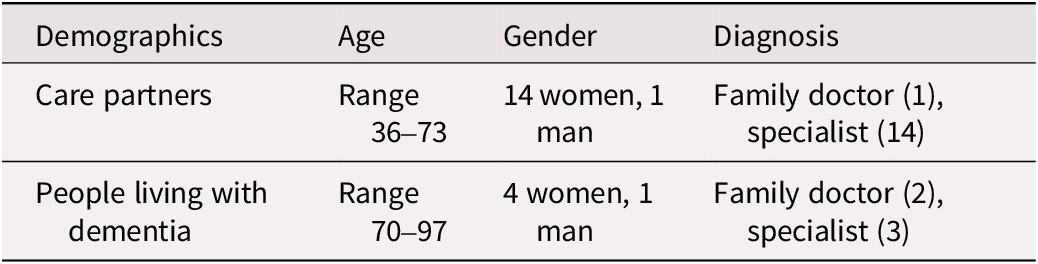
Semi-structured interviews and focus groups were conducted virtually through Zoom with 5 people living with dementia and 15 care partners (see Table 1). A semi-structured topic guide was created with questions about the dementia diagnostic experience and perceived gaps, facilitators, and barriers to diagnostic and post-diagnostic care. A total of 20 individuals participated in the study. Of the five persons with dementia (four women and one man; ages ranging from 70 to 97), two participants had their diagnosis delivered by a family doctor and three participants had their diagnosis delivered by a specialist. Of the 15 care partners (14 women and one man; ages ranging from 36 to 73), most expressed that the person they care for had their diagnosis delivered by a specialist instead of a family doctor. The time since diagnosis ranged from 2 months to 2 years, with an average of 13 months. Of care partners, 11 provided care to a parent with dementia, 2 to a spouse, 2 to a friend, and 1 to an uncle/aunt. All participants in this study identified as white English-speakers, and the majority indicated that their country of origin was Canada. Participants were predominantly recruited from urban and suburban settings.
Demographic characteristics of participants
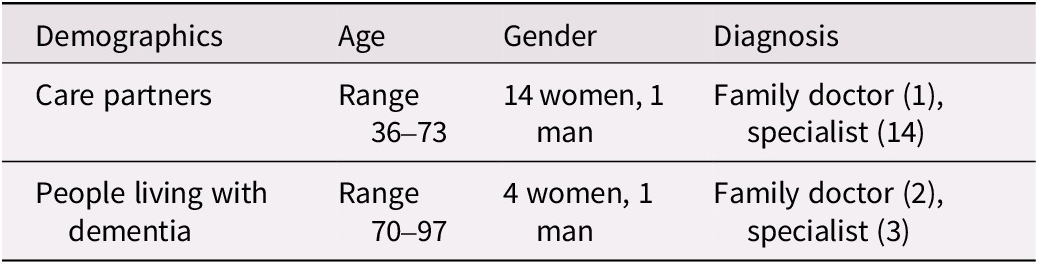
Table 1.
Table 1.The table has four columns labeled Demographics, Age, Gender, and Diagnosis. The first row lists Care partners with age range 36 to 73, 14 women and 1 man, diagnosed by family doctor 1 and specialist 14. The second row lists People living with dementia with age range 70 to 97, 4 women and 1 man, diagnosed by family doctor 2 and specialist 3.
Data analysis
Audio recordings from interviews were transcribed verbatim, cleaned, and anonymized. As the overall sample size was small, and consistent with a qualitative descriptive design, interviews were not analysed with the goal of statistically comparing answers between groups. Rather, transcripts were inductively analysed as a whole to examine overall experiences with the diagnostic and post-diagnostic process. Qualitative content analysis was conducted following the approach described by Elo and Kyngäs (Reference Elo and Kyngäs2008), which outlines a systematic process of preparation, organization, and reporting. This approach permitted both careful fidelity to the data and meaningful abstraction into categories. The analysis was primarily inductive, meaning categories were derived from the data itself rather than imposed from a predetermined framework. However, given that the broader COGNISANCE study was designed to examine barriers, facilitators, and gaps in diagnostic and post-diagnostic care, the analysis was also oriented by these constructs as sensitizing concepts (Elo & Kyngäs, Reference Elo and Kyngäs2008). This reflects what Elo and Kyngäs (Reference Elo and Kyngäs2008) describe as a hybrid inductive-deductive approach, wherein the research question provides a broad orienting structure while categories emerge from the data. Barriers were understood as factors that impeded access to timely, coordinated, and supportive care; facilitators were understood as factors that promoted positive diagnostic and post-diagnostic experiences; and contextual factors were understood as conditions that shaped how participants experienced the diagnostic journey, including pandemic-related disruptions.
The lead analyst (EC) began by reading all transcripts to develop familiarity with the data and to record initial impressions in a reflexive journal. Line-by-line open coding was then conducted, generating descriptive codes that remained close to the language of participants. Codes were subsequently grouped into categories through an iterative process of comparison and discussion with the broader research team. NVivo software (Miles et al., Reference Miles, Huberman and Saldaña2014) was used to organize and manage the data throughout this process. The research team reviewed identified categories iteratively to ensure that they were grounded in the data and reflected the range of participants’ experiences. Final categories were agreed upon through team consensus. Direct quotations are used throughout to illustrate and support the analytic categories and to maintain transparency.
Interviewer journals were maintained throughout data collection and analysis. These journals served as a space for reflexive notetaking, recording the interviewer’s observations, impressions, and analytical thoughts during and following interviews. Journal entries were shared with the research team during peer debriefing sessions and were reviewed alongside transcripts during analysis to ensure the team remained attentive to contextual nuances and researcher influence on the data (Lincoln & Guba, Reference Lincoln and Guba1985).
Methods to enhance rigour
Strategies consistent with Lincoln and Guba’s (Reference Lincoln and Guba1985) trustworthiness framework were employed throughout this study to ensure credibility, dependability, transferability, and confirmability. Credibility refers to confidence in the accuracy of the findings and their reflection of participants’ perspectives (Lincoln & Guba, Reference Lincoln and Guba1985). Credibility was enhanced through researcher triangulation, wherein multiple members of the research team were involved in data analysis and interpretation. Regular peer debriefing sessions were conducted throughout analysis, during which the lead analyst presented categories to the research team for critical review and discussion. These sessions supported reflexivity and helped identify potential analytical blind spots. Interviewer journals were also reviewed collectively during debriefing to examine how interviewer positionality may have shaped the data collection and interpretive process. Direct quotations from participants are included throughout the findings to anchor interpretations in the data and allow readers to assess the plausibility of the analysis.
Dependability, or the stability and consistency of the analytical process over time, was supported by maintaining a clear and documented audit trail throughout the study (Lincoln & Guba, Reference Lincoln and Guba1985). This included records of coding decisions, team discussions, and revisions to the categorization scheme. The Methods section of this paper provides a sufficiently detailed account of the analytical process to support dependability assessments by external readers. Transferability refers to the degree to which findings may be applicable to other contexts or populations (Lincoln & Guba, Reference Lincoln and Guba1985). To support transferability, thick description of the study context, participant characteristics, and analytical process is provided throughout the methods and findings sections.
Confirmability, or the degree to which the findings reflect participants’ experiences rather than researcher bias, was supported through the reflexive journaling process, iterative peer debriefing, and the use of an explicit, documented analytical process (Lincoln & Guba, Reference Lincoln and Guba1985). The involvement of multiple team members in reviewing and challenging interpretations throughout analysis further supported confirmability. Regarding the use of triangulation in this study: triangulation was employed as an analytical strategy, specifically researcher triangulation, wherein multiple team members independently engaged with the data and collaboratively reviewed emerging categories. It is important to note that triangulation was not used to compare or contrast the perspectives of people living with dementia with those of care partners, as the sample size precluded meaningful between-group comparisons. Rather, the intent was to ensure that the diversity of experiences across all participants was captured and that no single analytical perspective dominated interpretation. Points of convergence and divergence noted in the findings section therefore reflect patterns across participants’ accounts, not systematic group comparisons.
Findings
A qualitative content analysis of the interview data yielded a descriptive understanding of the range of experiences shaping the dementia diagnostic and post-diagnostic journey among participants. Three overarching categories were identified: (a) facilitators of a positive experience, (b) barriers impeding access and continuity of care, and (c) the pervasive impact of the COVID-19 pandemic. These findings reflect insights from both people living with dementia and care partners. Where relevant, convergences, and divergences across participants’ accounts are noted.
Facilitators
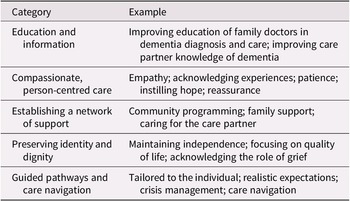
Participants identified several elements that contributed to more positive diagnostic and post-diagnostic experiences. The primary facilitators included: (a) access to education and information; (b) compassionate, person-centred care; (c) strong support networks; (d) the preservation of personhood; and (e) structured care navigation and planning. These facilitators were consistently highlighted by both people living with dementia and care partners. An overview of identified facilitators is presented in Table 2 and explored in more detail through the presentation of relevant excerpts below.
Summary of facilitators to a positive diagnostic and post-diagnostic experience
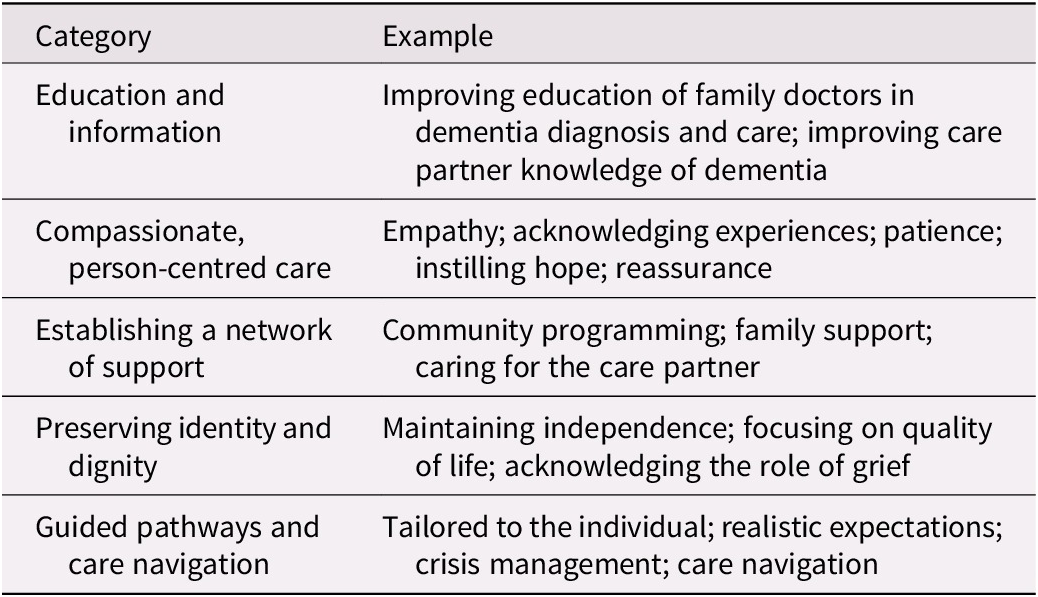
Table 2. Long description
The table has two columns labeled Category and Example. From top to bottom, the first row lists Education and information with examples including improving education of family doctors in dementia diagnosis and care and improving care partner knowledge of dementia. The second row is Compassionate, person-centred care with examples such as empathy, acknowledging experiences, patience, instilling hope, and reassurance. The third row is Establishing a network of support with examples including community programming, family support, and caring for the care partner. The fourth row is Preserving identity and dignity with examples maintaining independence, focusing on quality of life, and acknowledging the role of grief. The fifth row is Guided pathways and care navigation with examples tailored to the individual, realistic expectations, crisis management, and care navigation.
Education and information
Several participants discussed how improving the knowledge of those involved in the care of people living with dementia could facilitate a more positive diagnostic experience. This included education of healthcare providers, such as family doctors and other primary healthcare providers, as well as education for family and friend care partners. Improving the knowledge base of primary health care providers was a recurrent concept, with participants describing a need for better training in dementia recognition and communication. It is worth noting that different types of clinicians involved in diagnosing dementia, including family physicians, neurologists, geriatricians, and nurse practitioners, bring different professional backgrounds and knowledge bases to the diagnostic encounter. Participants’ comments often did not distinguish between these roles; rather, they pointed to a broadly felt need for improved communication skills, emotional attunement, and awareness of available community supports across all professionals involved in the diagnostic process.
Care partners also expressed a strong need to be equipped with anticipatory guidance about dementia progression and practical caregiving strategies. For example, one participant, reflecting on the time when their parent was diagnosed, stated:
If you were talking to me a year ago, I would have been very stressed or upset because I didn’t know what was going on. But now I got all my ducks in a row but I’m always willing to learn more. I did my homework … Participant 5, care partner
This quote exemplifies the shift in confidence and preparedness resulting from access to targeted information. The care partner illustrates the stark contrast between the confusion and anxiety of early encounters with the healthcare system and the empowerment that followed once they were better informed.
Compassionate, person-centred care
Participants highlighted the importance of empathy, active listening, and emotional attunement by healthcare professionals. Compassionate care was characterized by validation of the individual’s and care partner’s experiences, instillation of hope, and acknowledgement of grief and uncertainty. For example, one participant stated,
Just be kind, caring, and compassionate. And keep saying “we are going through this together”. You’re not alone in this. Letting her know that she’s supported in it. Participant 8, care partner
This quote illustrates the importance of recognizing shared experiences and providing emotional reassurance. Importantly, this kind of co-navigating, supportive presence was identified as key not only at the moment of diagnosis but as an ongoing feature of care relationships. The ongoing nature of this relational connection – what has been described in the literature as relational continuity – refers to an enduring therapeutic relationship between a patient, their family, and a consistent care provider that fosters trust and enables coordinated, personalized care over time (Haggerty et al., Reference Haggerty, Reid, Freeman, Starfield, Adair and McKendry2003). In the context of dementia care, this continuity is particularly important as needs evolve and trust between the care team and the family becomes foundational to effective support. Another care partner shared:
It would have been nice to have gotten a phone call as soon as you got home, just to say, checking in. Just wanna see how you’re doing. Participant 1, care partner
The absence of this type of follow-up left the family feeling isolated, underscoring the significance of relational continuity in post-diagnostic support. Participants living with dementia reinforced these sentiments. When asked what the diagnosing clinician could do to support them, one participant shared:
[The physician] could be reassuring that it is not a death sentence. [The physician] could emphasize the services that are available. [The physician] could explain a bit more about what the process of the disease is, like the progression and what things I would be able to expect. Again, I think highlighting the services that could make it a little easier for myself and my spouse would be where I would be focusing. Participant 4, person living with dementia
Establishing a network of support
Participants emphasized the value of being connected to both formal community resources (e.g., Alzheimer Society programmes) and informal networks (e.g., family, friends). These connections were seen as vital to emotional resilience and practical day-to-day functioning. As one care partner stated:
I really think that the doctor should have a folder of information. Maybe referrals to the Alzheimer’s Society or local community resources for the person. And a little bit about what to expect. The doctor should be plugged in to what’s available out there. Participant 13, care partner
This quote reveals the expectation that clinicians serve not only as diagnosticians but also as connectors, ensuring families have immediate and relevant pathways to support at the point of diagnosis.
Preserving identity and dignity
The importance of upholding personhood throughout the diagnostic and post-diagnostic period was emphasized by both people living with dementia and care partners. Clinicians and care partners who maintained a focus on the individual’s quality of life, acknowledged grief, and supported independence were viewed positively. Care partners and people with dementia often reported feeling grief-stricken and hopeless when receiving a diagnosis and acknowledging and normalizing these feelings were seen as important contributions to a positive experience. For example, one care partner reflected:
[The physician] was very honest and open and said I do not know how this will affect [her]. Participant 1, care partner
The candor expressed by the provider in this case helped the care partner feel respected and included in an uncertain journey. This acknowledgement of uncertainty, rather than false reassurance, modelled a kind of honest, dignified engagement that was highly valued by participants. The desire expressed by participants to be treated as a whole person, not merely a patient, reflects the core tenet of personhood.
Guided pathways and care navigation
Having a structured care plan tailored to individual needs was repeatedly identified as a facilitator. Several participants noted that having a knowledgeable advocate or navigator – someone familiar with both the healthcare system and available community and social services – would reduce confusion and delay. While participants sometimes referred specifically to social workers as potential navigators, the broader concept they described was of a care coordinator role that could bridge service silos across the interdisciplinary team. Such a role might involve collaboration among social workers, primary care providers, specialist physicians, nurse practitioners, and community support workers, each contributing different knowledge, coordinated by a consistent person who could guide families through the system. As one care partner shared:
I think if there was one [thing], it could have been very helpful in terms of what to expect. And measures to put in place ahead of time. Possibly someone, I don’t know if it would be a social worker or some kind of medical consultant, that could kind of guide them through the process. Participant 11, care partner
Another echoed this idea:
Somebody who knows all the branches from what’s available privately to publicly to government agencies. Somebody who can liaison with all of those different entities and work with families. Participant 13, care partner
Both care partners reflect a desire for a consistent, informed presence to guide them through the complexity of dementia care.
Barriers
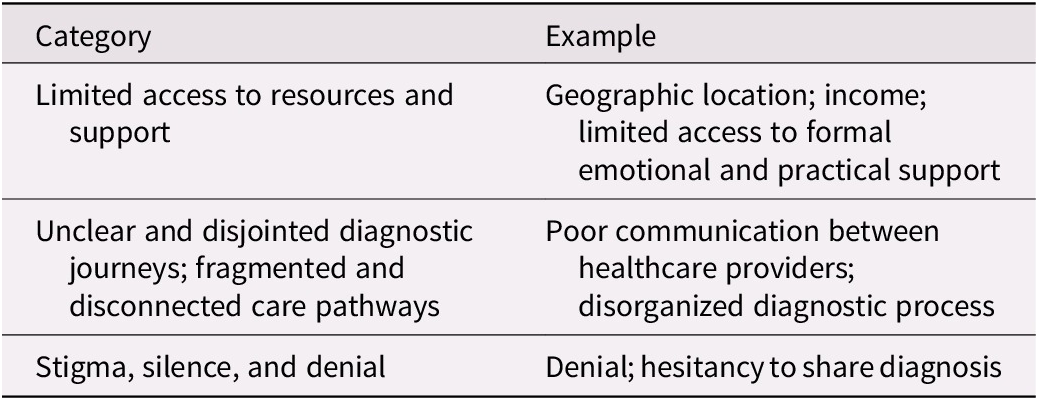
Participants also identified several challenges that hindered access to supportive, timely, and integrated care. Barriers included: (a) limited access to resources and support, (b) unclear and disjointed diagnostic journeys and fragmented and disconnected care pathways, and (c) stigma, silence, and denial. A summary of these barriers is presented in Table 3.
Summary of barriers to a positive diagnostic and post-diagnostic experience
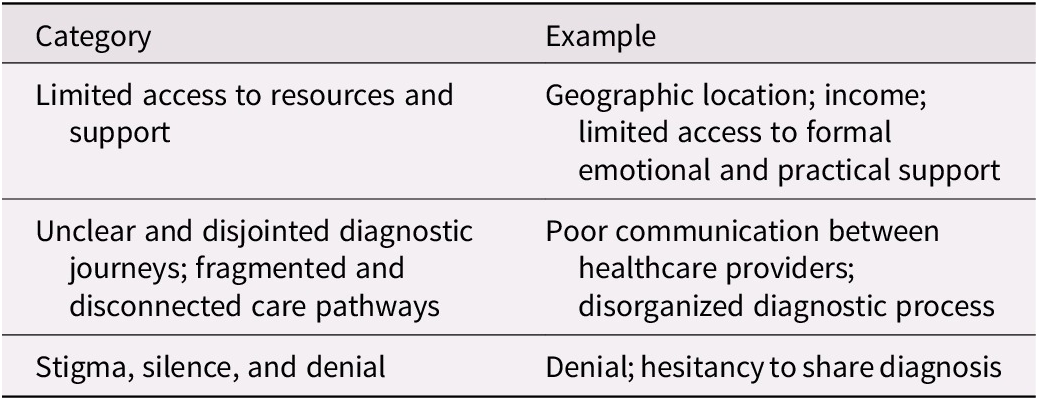
Table 3. Long description
The table has two columns labeled Category and Example. The first row lists Limited access to resources and support with examples including geographic location, income, and limited access to formal emotional and practical support. The second row lists Unclear and disjointed diagnostic journeys; fragmented and disconnected care pathways with examples such as poor communication between healthcare providers and a disorganized diagnostic process. The third row lists Stigma, silence, and denial with examples including denial and hesitancy to share diagnosis.
Limited access to resources and support
Access to supports was a key issue for many participants. While all participants in this study identified as white English-speaking Canadians, they nonetheless raised concerns about systemic barriers to support that would disproportionately affect those from other backgrounds or circumstances. Participants raised the issue of geographic barriers, noting that those in more rural or remote settings face reduced access to specialized dementia services and community supports. Income was also raised as a barrier, with participants describing how the costs associated with private services, medications, and care coordination placed burdens on families. Being unable to access needed supports after a diagnosis led to feelings of frustration and abandonment. For example, one participant shared:
It’s been very, very difficult to know what support is available and of course the pandemic has not helped. So, what I think when I hear the word support, I feel frustration and confusion because I don’t know where to turn. And it’s hard to know what services are available and how to tap into them, and this has been greatly impacted by the pandemic. Participant 11, care partner
Another participant shared,
To be honest with you when I see that word ‘support’, it brings anger. Because the word ‘support’ really comes from family. I don’t see any real major support coming from the system per-say. The public system, even private system support is very difficult to secure. So, it means added responsibility for families. Participant 7, care partner
This perspective reframes support as a familial obligation rather than a societal or institutional responsibility, pointing to structural gaps in formal care infrastructure.
Unclear and disjointed diagnostic journeys; fragmented and disconnected care pathways
A key barrier to a positive diagnostic and post-diagnostic experience was a lack of continuity of care. This included poor communication across the care continuum between healthcare providers, as well as a generally disorganized diagnostic process that resulted in additional stress, confusion, and distress for participants. Many care partners described a healthcare system that lacked integration. Poor communication between providers, reliance on families to coordinate care, and inconsistent messaging led to confusion and burnout. As one care partner discussed:
I’m still actually quite lost. It seems really fragmented. Like, you know, he can go to a physiotherapist, if I make the appointment and take him and he can go he can get home healthcare if I know enough to know he needs it in the middle of a pandemic and make the arrangements. It seems like there should be some (…) overarching agency that would tell me these things instead of me having to figure out painfully on my own. Participant 11, care partner
Another care partner noted,
[The diagnostic process] was robotic. You can tell they’re exhausted emotionally from telling every[one]- they’re telling families hour after hour after hour. So, I had a lot of questions, but again I had to resort to google. Participant 5, care partner
The reliance on self-directed research left care partners feeling abandoned during critical moments. Several participants described the diagnostic process as rushed, unclear, or emotionally distressing. The absence of comprehensive follow-up or explanation often left families unsupported:
There was no discussion of ‘okay as a family these are some of the supports that you will need, and here’s some organizations that can help you’ – there was none of that. So, there’s a follow up in six months’ time, my mother refused. She would not go back. So that’s that. Participant 7, care partner
People with dementia also discussed their experience receiving a diagnosis. For one participant, they felt as if the process was not adequately explained to them:
So, when I’m in the chair, I’m thinking “oh my god, I’ve got dementia”. So, you start, you know, your brain is going around and around thinking “what symptoms did I show? What made them do this?” And that they hadn’t told me. Participant 1, person living with dementia
This quote emphasizes the importance of person-centred diagnostic processes, and how not involving people with dementia in their care can serve as a barrier to a positive diagnostic experience.
Stigma, silence, and denial
Stigma was identified as negatively impacting the diagnostic and post-diagnostic support experiences for people with dementia. People with dementia and care partners both described experiences of the diagnosing clinician not directly disclosing the diagnosis to the person with dementia, which in some cases perpetuated self-stigma and discouraged help-seeking. As one care partner details:
No one actually ever gave her the diagnosis of dementia [at first]. Her family physician just put her on medication. She went home, she looked up that medication, she saw that it was for dementia, she got very upset, she didn’t want to take it… [the specialist] brings us all back together and my mum was saying things to him like ‘well my mother lived till she was 103 and she didn’t have any dementia or anything’ and he said ‘well you’re not gonna live to 103. You have dementia’. And it was just terrible. It was a terrible situation, and when we left my mum was in the back seat, I was driving, and she was so quiet. It just killed me. So anyway, I didn’t think it was handled very well at all and it was a terrible experience really. Participant 7, care partner
This was identified by participants as both self-stigma (internalized stigma about one’s diagnosis) and a general societal stigma that exists around the topic of dementia. Participants reported reluctance to share the diagnosis and discomfort with how professionals handled disclosure. For example, one person with dementia who was interviewed shared,
I do have difficulty telling people that [I have dementia]. That’s a really hard thing for me. They don’t know what to do and they treat you differently and I don’t like that. Participant 3, person living with dementia
the experience for some care partners. The indirect or passive delivery of such life-changing information further eroded trust in the care system. One participant reflected,
It was very difficult [to talk] about dementia in front of my mother, because she was in denial that she had it. Participant 13, care partner
Impacts of COVID-19
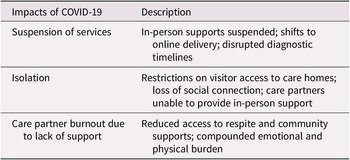
Because this project was conducted during the COVID-19 pandemic, participants frequently described how it disrupted diagnostic and support services. Participants reported (a) suspension of services, (b) social isolation, and (c) care partner burnout due to lack of support (see Table 4). The pandemic compounded existing system-level challenges and created additional emotional and logistical burdens, operating at multiple levels: systemically, through the suspension of services and the shift to virtual care; organizationally, through restricted access to institutional care settings; and interpersonally, through the profound disruption of social and familial connections that form the foundation of everyday dementia care.
Summary of the impacts of the COVID-19 pandemic
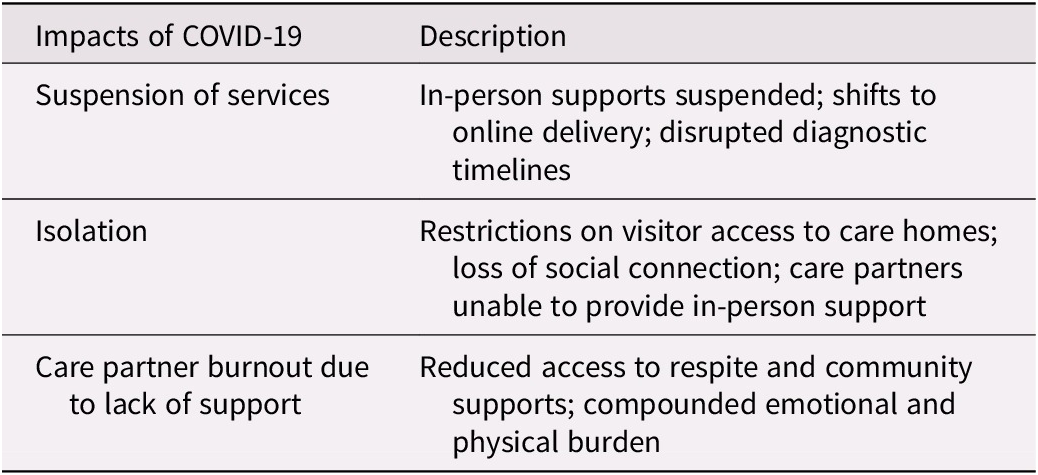
Table 4. Long description
The table has two columns. The left column lists impacts of COVID-19, the right column provides descriptions. First row: Suspension of services, described as in-person supports suspended, shifts to online delivery, disrupted diagnostic timelines. Second row: Isolation, described as restrictions on visitor access to care homes, loss of social connection, care partners unable to provide in-person support. Third row: Care partner burnout due to lack of support, described as reduced access to respite and community supports, compounded emotional and physical burden.
Suspension of services
Due to restrictions associated with the COVID-19 pandemic, many in-person supports for people with dementia and care partners were suspended or transitioned to alternative delivery methods. As one care partner discussed:
There wasn’t anybody, the services were all suspended. Even bloodwork and stuff, like he needed medical care done so unless we took him to the emergency room, those things would have not been able to happen. Participant 5, care partner
Another care partner spoke about how the pandemic impacted assessment and diagnosis:
If they were still living in their home, and receiving services in the home, a lot of those could have been impacted by the COVID outbreak … There were delays in assessments and onsite visits for social workers. Participant 6, care partner
Isolation
During the height of pandemic restrictions, many communities implemented restrictions on access to institutional care settings, preventing care partners from visiting. As one care partner shared:
There was initially no access to anything… I couldn’t even see him for months. That was extremely difficult because his dementia was worsening during that time. Participant 11, care partner
Another care partner stated:
My father is in a senior care home, so they do limit the people who can come in and visit. I mean the basic need for human companionship was just not being met. Participant 14, care partner
Care partner burnout due to lack of support
The pandemic surfaced challenging emotions about navigating one’s own health and the health of others at a time when access to supports were cut off. As one care partner reported:
We’re going through this with my mum at the worst possible time. Participant 13, care partner
Another care partner spoke to the challenges of coping with living with dementia during the pandemic and discussed how physical distancing requirements and mask mandates made their situation even more difficult. They shared,
He has trouble recognizing people of course… with the masks on it’s even worse, for him to realize who’s in front of him. And I’m grateful because if he got COVID, he’s just frail, it would just take him. Participant 14, care partner
Discussion
This study explored the lived experiences of persons living with dementia and care partners in Canada during their diagnostic and post-diagnostic journey, as part of the COGNISANCE project’s international efforts to enhance and improve the process of dementia diagnosis and post-diagnosis support. The findings reveal a complex interplay between systemic, organizational, and interpersonal factors that shaped participants’ experiences. While facilitators such as education, compassionate care, and care navigation enhanced experiences, systemic fragmentation, stigma, and the COVID-19 pandemic introduced persistent barriers. These insights have direct implications for the design of person-centred, coordinated, and accessible dementia care strategies across jurisdictions.
The facilitators identified, such as access to education, person-centred communication, and structured care navigation, resonate strongly with existing literature emphasizing the value of supportive, clear, and empathetic diagnostic processes (Dhedhi et al., Reference Dhedhi, Swinglehurst and Russell2014; Prorok et al., Reference Prorok, Hussain, Horgan and Seitz2017). Participants articulated that emotional attunement and relational continuity from providers played an essential role in reducing uncertainty and psychological burden (Haggerty et al., Reference Haggerty, Reid, Freeman, Starfield, Adair and McKendry2003). These findings echo prior research suggesting that early, honest, and hopeful communication is associated with better adjustment to diagnosis and care planning (Bunn et al., Reference Bunn, Goodman, Sworn, Rait, Brayne, Robinson and Iliffe2012; Phillipson et al., Reference Phillipson, Jones and Magee2014).
The category of preserving identity and dignity aligns with Kitwood’s (Reference Kitwood1997) person-centred dementia care model and has been reinforced by more recent research on the centrality of identity preservation and autonomy in dementia support (Beuscher & Grando, Reference Beuscher and Grando2009; Swaffer, Reference Swaffer2016). Participants valued care approaches that treated people living with dementia not solely as patients but as individuals with unique needs, histories, and agency. The desire for advocates and navigators further reflects a growing recognition that dementia care must be relational, not merely transactional (Gilhooly et al., Reference Gilhooly, Gilhooly, Sullivan, McIntyre, Wilson, Harding and Crutch2016). At an interpersonal level, this means clinicians and care navigators building genuine, sustained relationships with individuals and families. At an organizational level, it requires systems that enable continuity of professional relationships rather than episodic, disconnected encounters. At a systemic level, it calls for policy frameworks that embed person-centred principles into the structures of dementia care funding and delivery.
The barriers described in our findings, particularly fragmented care pathways, lack of follow-up, and emotional detachment from providers, point to systemic shortcomings that contribute to negative care experiences. These concerns reflect the broader literature on inequitable access to dementia care in Canada, particularly for those in rural, lower-income, or linguistically diverse communities (Lemay-Compagnat et al., Reference Lemay-Compagnat, Couturier and Rojas-Rozo2025). Prior studies have similarly reported that the diagnostic process can be experienced as abrupt or disjointed, especially when providers fail to communicate clearly or offer immediate follow-up resources (Iliffe et al., Reference Iliffe, Koch, Jain, Lefford, Wong, Warner and Wilcock2012; Karnieli-Miller et al., Reference Karnieli-Miller, Werner, Aharon-Peretz, Sinoff and Eidelman2012). The described reliance on self-navigation, Google searches, or informal networks underlines the unmet need for structured post-diagnostic supports, consistent with other recent findings (Bamford et al., Reference Bamford, Lee, McLellan, Poole, Harrison-Dening, Hughes and Exley2018).
Stigma and denial were also identified as prominent barriers, influencing both personal disclosure and systemic communication practices. As shown in other qualitative studies, societal stigma and internalized fear of dementia often delay diagnosis and limit openness (Aminzadeh et al., Reference Aminzadeh, Molnar, Dalziel and Ayotte2012; Werner, Reference Werner and Corrigan2014). Participants’ accounts of diagnosis being withheld or discovered indirectly suggest a continued discomfort among some healthcare providers in delivering such news, underscoring the urgency of improved training and guidance in dementia disclosure across professional roles (Mason et al., Reference Mason, Annear, Lo, McInerney, Tierney and Robinson2016).
The COVID-19 pandemic exacerbated many of the pre-existing challenges in dementia care delivery. At a systemic level, the suspension of non-urgent health services across Canada and the rapid shift to virtual care created new access barriers and delayed assessments for many families (Cetin-Sahin et al., Reference Cetin-Sahin, Godard-Sebillotte and Bronskill2025). At an organizational level, restrictions on visitor access in long-term care settings severed critical relational ties between care partners and people with dementia, compromising both care quality and the emotional well-being of both groups. At an interpersonal level, social isolation intensified feelings of loneliness, grief, and burnout, particularly among care partners who lost access to community-based respite and peer support. These findings align with emerging pandemic-era literature highlighting the disproportionate impact of COVID-19 on individuals with dementia and their families (Bacsu et al., Reference Bacsu, Spiteri, Nanson, Rahemi, Webster, Norman and Stone2024; Giebel et al., Reference Giebel, Sutcliffe, Darlington-Pollock, Green, Akpan, Dickinson and Gabbay2021; McAiney et al., Reference McAiney, Conway, Koch, Middleton, Dupuis, Keller and Boger2021). Importantly, this study reinforces the interdependence between emotional, informational, and structural supports; facilitators such as compassionate care or structured planning cannot be effective in isolation but must be part of a coordinated, person-centred system that adapts to evolving needs.
While findings of this study reinforce results from other studies in terms of facilitators to a positive diagnosis process and better adjustment to diagnosis and care planning (Bunn et al., Reference Bunn, Goodman, Sworn, Rait, Brayne, Robinson and Iliffe2012; Phillipson et al., Reference Phillipson, Jones and Magee2014), this study makes novel contributions by presenting insights directly from people living with dementia alongside their care partners in the Canadian context. It further extends the literature by situating findings within a multi-level contextual framework that spans interpersonal, organizational, and systemic influences, including the specific disruptions introduced by COVID-19 in Canada.
Limitations
Several limitations of this study should be acknowledged. First, the sample was drawn from only three Canadian provinces (New Brunswick, Ontario, and Quebec) which may not fully capture the diversity of experiences across the broader Canadian population. Provinces vary substantially in their healthcare structures, dementia services, and language policies, and experiences in other provinces, such as British Columbia, Alberta, or the territories, may differ meaningfully. Second, all participants in this study identified as white English-speaking Canadians; the barriers associated with racialized identity, Indigenous heritage, language minority status, and other intersecting dimensions of identity were not directly represented in these data (Hicks et al., Reference Hicks, Wheatley, Porter, Farina and Banerjee2025). Future research should intentionally recruit from more diverse populations to address this gap. Third, while participants were recruited from across three provinces, most were from urban and suburban settings, and the perspectives of those in rural or remote communities, who face distinct access barriers, are likely underrepresented. Finally, this study was conducted during the COVID-19 pandemic, and some experiences described may be specific to that context and less generalizable to the post-pandemic period.
Conclusion
This study examined the experiences of people living with dementia and care partners in Canada navigating the diagnostic and post-diagnostic journey, with the goal of identifying barriers, facilitators, and contextual influences that shape those experiences. Findings underscore that while a dementia diagnosis can provide clarity and access to support, the experience is often shaped by systemic barriers, inequities, stigma, and gaps in post-diagnostic care. Positive experiences occur when diagnosis is delivered with compassion, when individuals and families are treated as partners, and when there is continuity of support beyond the diagnostic event. Negative experiences arise when diagnosis is delayed, poorly communicated, or followed by inadequate support. The COVID-19 pandemic amplified these challenges at systemic, organizational, and interpersonal levels.
These findings carry clear implications for policy, practice, and research. For policy, results underscore the need for a coordinated national dementia strategy that includes sustained funding for post-diagnostic support, care navigation services, and supports for care partners. For practice, clinicians across professional roles would benefit from training in compassionate diagnosis communication, knowledge of available community resources, and relational care approaches. For research, future studies should prioritize the inclusion of racialized, Indigenous, and rural communities in Canada to ensure that strategies emerging from this work are equitable and broadly applicable. Results from this project have already informed subsequent phases of the COGNISANCE project, including the development of an informational tool and web resource, Forward with Dementia.
Data availability statement
Data will be made available upon reasonable request.
Acknowledgements
The authors would like to acknowledge the contributions of Research Assistants Melissa Koch, Laura Rojas Rozo, Luke MacNeill, and Evgeny Neiterman for their assistance in conducting this study, as well as the entire COGNISANCE International Consortium for their support with the overall programme.
Financial support
The authors received funding through the 2019–2022 Horizon 2020 Joint Programme Neurodegenerative Disease (JPND) transnational call: ‘Multinational Research Projects on Health and Social Care for Neurodegenerative Diseases’ for the project ‘CO-Designing Dementia Diagnosis and Post-Diagnostic Care’ ‘COGNISANCE’ HESOCARE-329-098.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.

 Open access
Open access