


Schizophrenia typically emerges in late adolescence or early adulthood, with earlier onset in men, and affects approximately 24 million people worldwide (0.32%, or 1 in 300 individuals). Individuals with schizophrenia have a two- to threefold increased risk of premature mortality, mainly due to common somatic conditions such as cardiovascular and metabolic disorders and infectious diseases. 1 Schizophrenia contributed 1.06% of the prevalence of mental health disorders in Romania in 2018, 2 and was responsible for 0.04% of all deaths in 2020. 3
Length of stay determinants
The average length of stay in hospital (HLoS) for patients with schizophrenia varies widely, from a few weeks to several months, being influenced by several factors including disease severity, treatment resistance, comorbidities and socioeconomic factors. The age of the patient (patients older than 50 years remain longer in hospital), marital status (being married serves as a protective factor for long hospitalisation stays) and education level (higher education is associated with shorter hospitalisation) are among the factors associated with HLoS. Reference Chen, Collins, Anderson, McKenzie and Kidd4 In Japan, patients with schizophrenia and psychotic disorder had an average hospital stay of 45.79 days, with age and low Global Assessment of Functioning scores (1–20) significantly (P < 0.001) linked to stays longer than 180 days. Reference Shinjo, Tachimori, Sakurai, Ohnuma, Fujimori and Fushimi5 Other reported factors significantly associated with prolonged hospital stay (>36 days, P < 0.05) include aggressiveness, involuntary admission, polypharmacy and parenteral medication administration. Reference Di Lorenzo, Montardi, Panza, Del Giovane, Saraceni and Rovesti6 Young and unmarried (single, separated, divorced or widowed; 30.6%) patients were factors associated with HLoS in a Chinese cohort. Reference Cheng, Wang, Xu, Zhou, Zhang and Li7 The HLoS reported for a Greek cohort significantly (P < 0.05) increased as the positive subscale (Pearson correlation coefficient, r = 0.481) and the general subscale (r = 0.312) of the Positive and Negative Syndrome Scale (PANSS) increased, and decreased with support from family (r = −0.517) and friends (r = −0.233). Reference Velelekou, Papathanasiou, Alikari, Papagiannis, Tsaras and Fradelos8 Unmarried marital status, treatment resistance and the need for the use of reserve medications (e.g. clozapine) were statistically significantly (P < 0.05) linked with HLoS exceeding 90 days in an African cohort. Reference Goga and Marais9
Research gaps
The scientific literature reporting factors related to hospitalisation of patients with schizophrenia in Romania is limited. Romanian patients with medical hospitalisation under Article 110 of the Romanian Penal Code (person who unjustifiably committed a crime), and hospitalised at the largest medium-security penitentiary hospital in Romania (n = 650), had significantly (P < 0.05) shorter HLoS if they had a higher level of education, were married or cohabiting and were employed on the date of admission. Reference Parfene Banu10 To date, only the study by Parfene Banu has reported HLoS in Romanian forensic psychiatric patients. Reference Parfene Banu10
Aim and objectives
Given the limited research available on the Romanian population, this study aimed to evaluate which socio-clinical factors are associated with HLoS. The primary objective was to identify and quantify the socio-clinical factors influencing HLoS in patients with schizophrenia. The secondary objective was to examine the association of socio-clinical factors with extreme hospital length of stay (XHLoS) in patients with schizophrenia.
Method
Ethical standards
All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on studies on human subjects, and with the Helsinki Declaration of 1975 as revised in 2024. All procedures involving patients were approved by the Ethics Committee of Iuliu Hațieganu University of Medicine and Pharmacy Cluj-Napoca, Romania (approval no. 21 from 27 January 2023), and by the Ethics Committee of County Emergency Hospital of Cluj-Napoca, Romania (application no. 7530 from 16 February 2023). Consent for participation was waived because the study utilised routinely collected health data.
Study design and setting
We conducted a retrospective study of the hospital medical records of patients with schizophrenia hospitalised between January 2018 and December 2022 at the First and Second Psychiatric Clinics of the County Emergency Hospital of Cluj-Napoca, Romania. Our methodology adheres closely to the RECORD statement. Reference Benchimol, Smeeth, Guttmann, Harron, Moher and Petersen11
Participants, measurements and data
Patients with a primary diagnosis of schizophrenia (F20, according to the ICD-10 classification), aged between 18 and 65 years and evaluated at admission and discharge, using either the PANSS/Structured Clinical Interview for Positive and Negative Syndrome (SCI-PANSS) Reference Kay, Opler and Lindenmayer12 or Brief Psychiatry Rating Scale (BPRS), Reference Overall and Gorham13 were eligible for the study. Patients diagnosed with intellectual disability, bipolar disorder, schizoaffective disorder or persistent delusional disorder were excluded. Additionally, those hospitalised under the Mental Health Law without treatment descriptions were excluded.
The SCI-PANSS/PANSS assessment includes 30 items across three categories: positive symptoms (7 items, total score 7–49), negative symptoms (7 items, total score 7–49) and general psychopathology (16 items, total score 16–122), with a bipolar index (the ratio of the positive to the negative score) reflecting the balance between positive and negative syndromes. BPRS consists of 18 items assessing symptoms including emotional detachment, perceptual disturbances and agitation, with scores indicating either no syndrome (0–9), minor syndrome (10–20) or major syndrome (21+). Psychometric evaluation of patients regarding the type of questionnaire was carried out based on the attending physician’s preferences. Evaluations were routinely conducted on the first day of admission and on the day preceding discharge. Percentage score reduction was used in our study by applying the following formula: 100 − ((discharged score)/(admission score)) × 100.
The following data were extracted from medical health records as potential predictors for duration of hospital stay: sociodemographic (e.g. gender, age at diagnosis and hospitalisation, place of residence, employment and marital status, living accommodation, addictions such as systematic current use of tobacco, substances/drugs); family history (e.g. schizophrenia or bipolar affective disorder in the family); comorbidities; symptoms (e.g. experiencing fear in the context of psychotic decompensation; depressive symptoms – observed clinically or measured by PANSS or BPRS; violence at the time of the admission; suicidality – suicidal thoughts, ideation or self-harming behaviours); type of treatment (first- or second-generation antipsychotics, adjuvant therapy); reasons for late discharge (e.g. court-order hospitalisation, comorbid acute infectious diseases or critical situations requiring intensive care); or reasons for early discharge (e.g. discharge on demand, transfer to another healthcare unit). Symptoms related to violence, suicidality, depression and fear were evaluated subjectively by the clinician during routine psychiatric anamnesis at admission. These were routinely documented in the electronic medical records as individual, single-item questions, as part of the standard clinical interview.
Statistical analysis
Sociodemographic and clinical characteristics considered as quantitative variables were summarised using central tendency and dispersion measures, including arithmetic mean with standard deviation or median with interquartile range (IQR, (25th percentile, 75th percentile)), whereas qualitative variables were summarised using absolute and relative frequency. A descriptive analysis was conducted based on complete cases for each variable. We split our cohort based on age into three unbalanced classes: 18–30, 31–40 and 41–65 years. The first age class reflects the age range in which disease onset most frequently occurs, whereas the latter two denote the degree of chronicity and psychopharmacological response.
To test whether the distributions for sociodemographic and clinical qualitative characteristics fit a uniform distribution, we performed a one-sample chi-square test. Because the distribution of HLoS was skewed and over-dispersed (for the multivariable model, α = 0.12, 95% CI [0.10; 0.16]), a negative binomial regression model was used and demonstrated a good fit to the data tested by residual deviance test. First, each independent variable (age range, gender, living arrangements, employment status, marital status, place of residence, schizophrenia in family, bipolar affective disorder in family, cardiac or metabolic comorbidities, depressive symptoms, addictions, antipsychotics therapy, reasons for early discharge (such as discharge on demand or transfer to another healthcare unit)) was included in a univariable negative binomial regression model. Second, potential predictors with an estimated significance level (P < 0.10 Reference Chowdhury and Turin14 ) were then tested in the multivariable negative binomial regression model. Effect sizes of the tested associations were reported using unadjusted and adjusted incidence rate ratios (IRRs) and their corresponding 95% confidence intervals.
XHLoS was defined as exceeding the 95th percentile for HLoS; chi-squared test, Fisher’s exact test or Student’s t-test was used to test the associations between sociodemographic and clinical characteristics with XHLoS.
All descriptive and inferential analyses were performed using R software version 4.4.0 for Windows (The R Foundation, Vienna, Austria, URL: https://cran.r-project.org/bin/windows/base/old/). The significance level for all two-tailed statistical tests was set at α = 0.05.
Results
Characteristics of the evaluated cohort
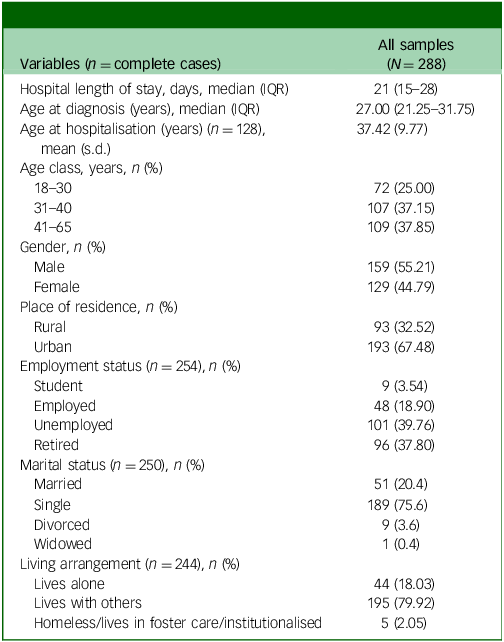
During the study period, a sample of 288 patients with a single hospital admission fitted the inclusion criteria and were evaluated. The participants had a similar distribution in terms of gender (P = 0.0771) but not in terms of age class (P = 0.0110). The majority of patients (75%) were older than 30 years (Table 1). For those patients with schizophrenia included in the current study, the mean age at hospitalisation was 37.42 years (s.d. = 9.77 years) and the length of hospitalisation ranged from 8 to 157 days.
Sociodemographic characteristics of the studied sample
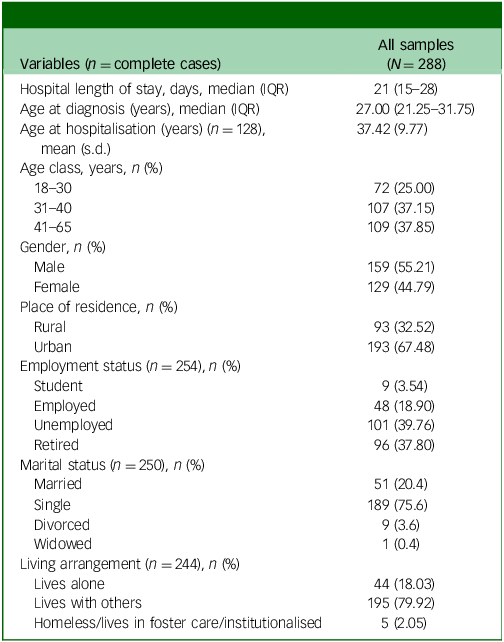
Continuous variables data were summarised as either arithmetic mean (standard deviation) or median interquartile range (IQR, Q1–3), with Q1 being the first quartile and Q3 the third (inclusive ranges); categorical variables were summarised using n (%).
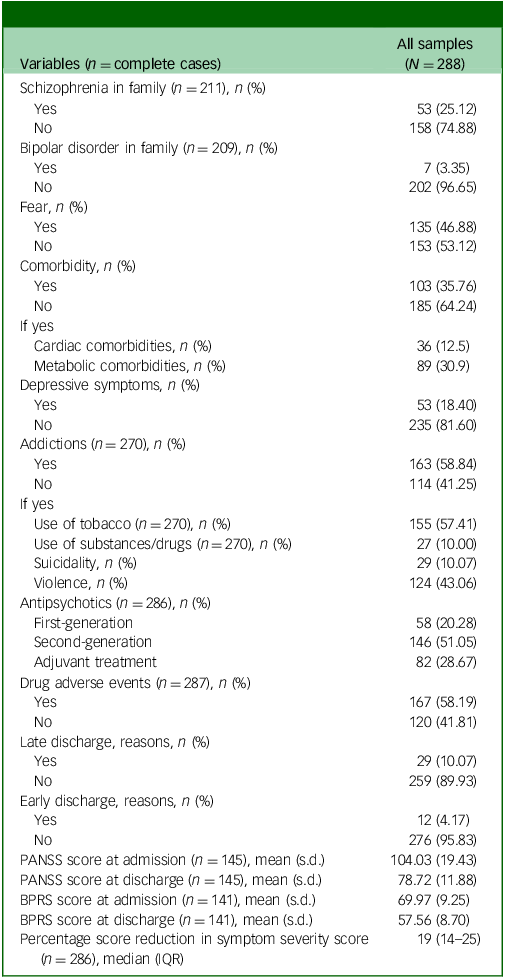
Table 2 shows the clinical characteristics of the study cohort. A quarter of the patients had schizophrenia in their family, and the majority showed addictions (such as tobacco or use of substances/drugs), suicidality or violence preceding hospitalisation. Of the total samples studied, 145 (50.70%) patients were assessed with the PANSS scale and 141 (49.30%) with the BPRS scale. The median percentage reduction from baseline in symptom severity scores was 19% (Table 2). A reduction greater than 10% in severity scores measured with PANSS or BPRS was observed in 272 (95.11%) patients.
Clinical characteristics of the studied sample
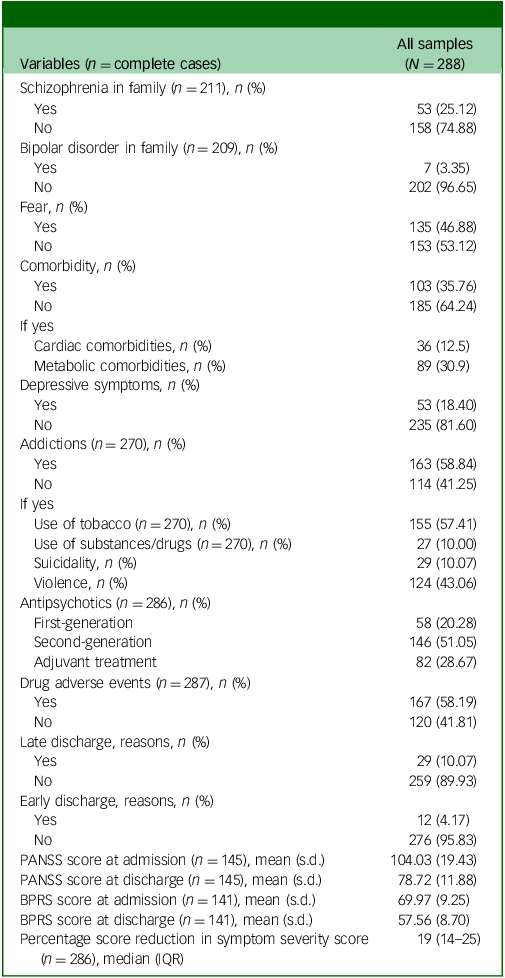
PANSS, Positive and Negative Syndrome Scale; BPRS, Brief Psychiatric Rating Scale. Continuous variables data were summarised as either arithmetic mean (standard deviation) or median (interquartile range (IQR), Q1–3), with Q1 being the first quartile and Q3 the third (inclusive ranges); categorical variables were summarised using n (%). Late discharge reasons: court-order hospitalisation, comorbid acute infectious diseases, critical situations requiring intensive care; early discharge reasons: discharge on demand, transfer to another healthcare unit.
In the evaluated cohort, one cardiac comorbidity was observed in 25 patients (8.63%), 2 in 5 patients (1.74%), 3 in another 5 patients (1.74%) and 4 comorbidities in one (0.35%). Sixty-two patients (21.53%) had one metabolic comorbidity, 24 (8.33%) had 2, and 3 (1.04%) had 3.
Among metabolic comorbidities, the most frequent were obesity (37, 12.94% of patients) followed by mixed dyslipidaemia (26, 9.03%), type 2 diabetes mellitus (12, 4.17%) and folic acid deficiency (12, 4.17%). Other metabolic comorbidities included hypertriglyceridaemia (9 patients, 3.13%) and vitamin B12 deficiency (5 patients, 1.74%).
Of the 277 patients with self-declared addiction, 137 (49.46%) reported one addiction with 26 (9.39%) reporting 2.
Ninety-seven (33.80%) patients reported one adverse effect of medication (n = 287), 2 were reported by 50 patients (17.42%), 3 by 16 patients (5.57%), 4 by 2 patients (0.70%) and 5 by the remainder. The most prevalent adverse effects were muscle stiffness (95 out of 278 patients, 33.10%), tremor (58 patients, 20.28%), tachycardia (74 patients, 25.78%) and akathisia (22 patients, 7.67%).
Twenty-five patients (8.68%) had one reason for late discharge, 3 (1.04%) had 2 and one (0.35%) had 4. Reasons for late discharge included court decisions (4 patients, 1.39%), acute infection (22 patients, 7.64%) and critical situations requiring intensive care (7 cases, 2.43%). Eleven patients (3.82%) had one reason for early discharge and one patient (0.35%) had 2. Three patients were discharged on demand (1.04%) and 10 (3.47%) were transferred to other healthcare units.
Multivariabile negative binomial model
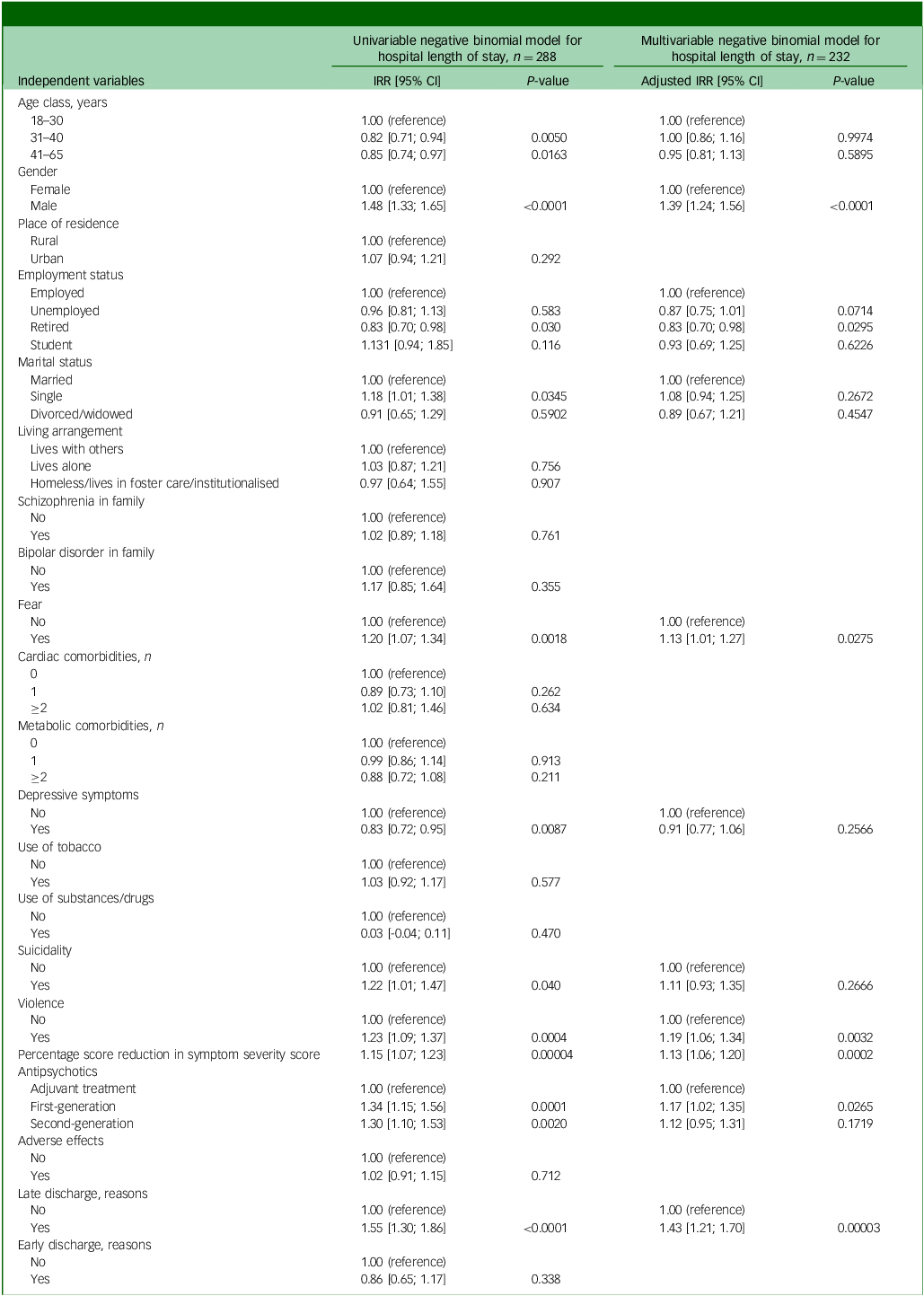
Age class, gender, retired employment status, marital status, depressive symptoms, fear, suicidality, violence, percentage reduction score, antipsychotic treatment type and reasons for late discharge were significantly associated with HLoS in univariable regression models (Table 3).
Incidence rate ratios and confidence intervals (95% CI) from unadjusted and adjusted negative binomial regression models
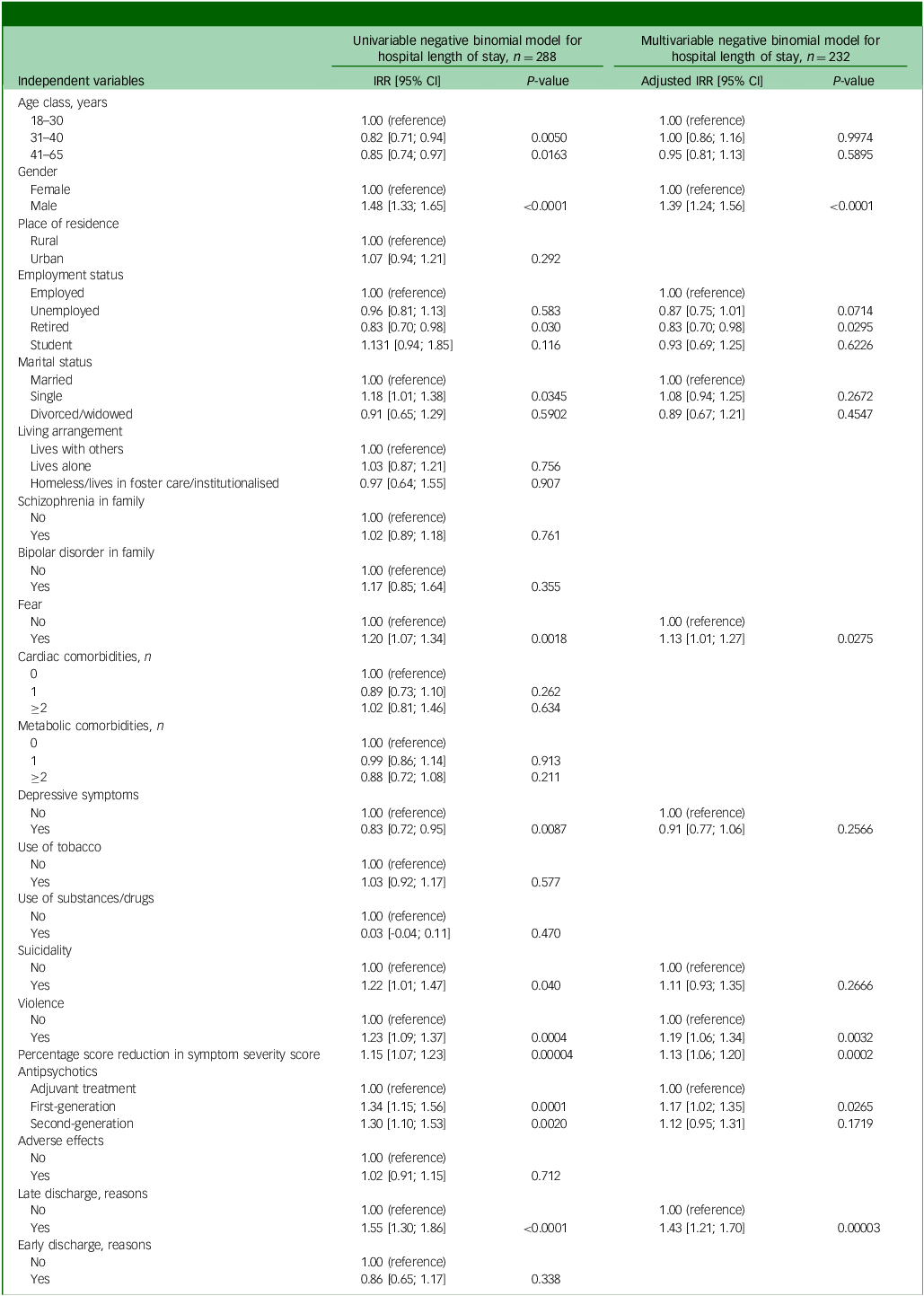
IRR, incidence rate ratio. Percentage score reduction, measured using the Positive and Negative Syndrome Scale or Brief Psychiatric Rating Scale, was scaled so that the regression coefficient reflected a change of 10%. Late discharge reasons: court-order hospitalisation, comorbid acute infectious diseases, critical situations requiring intensive care; early discharge reasons: discharge on demand, transfer to another healthcare unit.
The chi-square goodness-of-fit test showed no statistical evidence of lack of fit (residual deviance) 225.85, d.f. = 215, P = 0.2923), suggesting an adequate fit of the multivariable negative binomial model to the data. In the adjusted regression model, the following explanatory variables remained independent predictors of HLoS: retired due to disability, fear, violence, percentage score reduction (P = 0.0002), first-generation antipsychotic treatment and reasons for late discharge (Table 3; adjusted IRR (aIRR)). Fifteen patients had XHLoS, defined as hospitalisation of at least 47 days (Supplementary Fig. 1 available at https://doi.org/10.1192/bjo.2025.10973), representing 5.2% of the total sample. Most patients with XHLoS were men (Supplementary Table 1), with more frequent fear symptoms and suicidality at admission (Supplementary Table 2).
Discussion
The median HLoS in our unbalanced age cohort (75% of patients were >30 years old, P = 0.0110) was 21 days, with wide variation in length of stay (range 8–157 days). Around 60% of patients experienced adverse effects from antipsychotic treatment, with muscle stiffness, tremors and tachycardia being the most prevalent. Additionally, the type of antipsychotic treatment was associated with HLoS (P = 0.0265). Multivariable regression analysis revealed that gender, being retired, experiencing fear in the context of psychotic decompensation, experiencing violence in the context of psychotic decompensation, percentage score reduction in symptom severity scores, second-generation antipsychotics and reasons for late discharge were independent predictors of HLoS.
Factors linked with length of hospitalisation
The evaluated cohort had a balanced gender distribution (Table 1) and a mean age of ∼37 years, similar to the characteristics reported for patients with multiple hospital admissions in Romania. Reference Crișan and Pop15 Most of the evaluated patients lived in a city (Table 1), which may reflect a tendency of rural patients to seek medical care closer to home, limiting access to a university hospital. Only a small proportion of participants were employed (Table 1), because chronic illness progression reduces work capacity and often leads to early retirement. Most patients were single but lived with others (Table 1), consistent with findings reported by Desalegn et al, Reference Desalegn, Girma and Abdeta16 after accounting for cultural differences.
The length of hospitalisation in our cohort aligns with the findings reported by Gonçalves-Pinho et al. Reference Gonçalves-Pinho, Ribeiro and Freitas17 Most of the patients in our cohort were users of tobacco, substances or drugs, a finding consistent with previous studies. Reference Dervaux, Baylé, Laqueille, Bourdel, Le Borgne and Olie18–Reference Lähteenvuo, Batalla, Luykx, Mittendorfer-Rutz, Tanskanen and Tiihonen20
Violence towards others, or suicidality (self-directed), was commonly observed in our cohort (Table 2). A third of the patients reported at least one adverse medication effect, with muscle stiffness being the most frequent, particularly among women, which is consistent with the adverse effects of antipsychotics reported in the literature. Reference Khelfi, Azzouz, Abtroun, Reggabi and Alamir21,Reference Mathews, Gratz, Adetunji, George, Mathews and Basil22 A small proportion of patients had prolonged hospitalisation due to an acute infectious disease, resulting in outcomes similar to those reported by Lyketsos et al, who noted that somatic comorbidities can extend psychiatric in-patient stays. Reference Lyketsos, Dunn, Kaminsky and Breakey23
Within this clinical and sociodemographic context, multivariable analysis identified several factors associated with HLoS. Men had a hospital stay 39% longer than women after adjusting for other covariates, a finding consistent with some previous studies Reference Ochoa, Usall, Cobo, Labad and Kulkarni24,Reference Abel, Drake and Goldstein25 but opposite to other studies which found that women experienced longer stays. Reference Gonçalves-Pinho, Ribeiro and Freitas17,Reference Tseliou, Johnson, Major, Rahaman, Joyce and Lawrence26 Patients who were retired had an estimated 17% shorter expected HLoS than those employed (aIRR = 0.83, 95% CI [0.70; 0.98]). A similar pattern, with shorter HLoS, was also observed among unemployed patients, in line with findings reported by Ajnakina et al. Reference Ajnakina, Stubbs, Francis, Gaughran, David and Murray27 This finding may reflect the financial burden placed on the healthcare system when patients lack insurance, leading to accelerated discharge.
Patients who experienced fear or those who were violent – both prevalent in our cohort – had significantly longer expected HLoS compared with patients without such manifestations, a result consistent with other evidence considering that the presence of such symptoms is associated with delayed stabilisation. Symptom reduction, as reflected in the percentage reduction score, was also linked to longer hospitalisation. This finding supports the clinical rationale that patients with higher severity at admission require more time to achieve significant improvement, a relationship well established in the literature. Reference Velelekou, Papathanasiou, Alikari, Papagiannis, Tsaras and Fradelos8,Reference Goga and Marais9 The expected HLoS was 17% longer in patients treated with first-generation antipsychotic drugs compared with those administered adjuvant treatment, reflecting differences in treatment response and management complexity.
Taken together, our results indicate that both sociodemographic characteristics (gender, employment status) and clinical features (fear, violence, comorbidities, treatment type and baseline severity) directly influenced the length of hospitalisation in our cohort.
In line with the results reported for the whole cohort, although this subgroup comprised a small number of patients, more men than women had an extreme duration of hospitalisation (Supplementary Table 1). Our results are similar to others reported. Reference Goga and Marais9,Reference Chung, Chang, Oh and Yoon28 Fear, suicidality and the presence of reasons for late discharge are reported more frequently in patients with XHLoS than in those with non-XHLoS (Supplementary Table 2), a finding consistent with results reported by Pompili et al. Reference Pompili, Amador, Girardi, Harkavy-Friedman, Harrow and Kaplan29 and Chong et al. Reference Chong, Wahab, Muthukrishnan, Tan, Ch’ng and Yoong30
Limitations of the study
Although this study adhered to current scientific standards, several limitations should be considered. First, all patients were admitted to a single acute psychiatric ward focused on short-term stabilisation rather than prolonged hospitalisation. Discharge decisions depended not only on symptom improvement but also on the resolution of immediate risk and the feasibility of continued care within out-patient or social support services, thereby limiting hospitalisation duration and external validity.
Second, psychometric assessments were conducted by different psychiatrists without standardised instruments, introducing heterogeneity and subjectivity in symptom and severity evaluation, including negative, depressive and suicidal symptoms. A prospective design using standardised tools and a single examiner would have yielded more consistent assessments.
Third, many patients had multiple comorbidities requiring specialised treatment; however, potential pharmacokinetic interactions between psychotropic and somatic medications were not assessed due to incomplete medical records, despite their potential impact on length of stay.
Fourth, treatment with generic psychotropic medications approved based on bioavailability data, without further validation in controlled trials, may have influenced treatment response and hospitalisation duration.
Finally, reliance on routinely collected health data entails the risk of incomplete documentation and reporting bias, particularly for self-reported substance use. Given the small, geographically limited sample, findings should be interpreted cautiously and validated in larger external cohorts to establish generalisability and clinical relevance.
In conclusion, our results indicate that hospital length of stay in patients with schizophrenia is influenced by demographic, clinical and treatment-related factors. Unemployed or retired status was associated with shorter stays, whereas male gender, fear or violence during psychotic decompensation, reasons for late discharge, greater symptom reduction and first-generation antipsychotic treatment were linked with longer stays. Extreme hospitalisation (>47 days) was more likely in men with fear during decompensation, suicidal ideation and delayed discharge. These findings should be interpreted cautiously, and further studies with larger, standardised cohorts are needed.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2025.10973
Data availability
The data supporting the findings of this study are available from the first author, R.P., upon request. The data-set analysed and reported in this study is part of ongoing PhD research conducted by R.P.
Author contributions
R.P. contributed to conceptualisation, data curation, funding acquisition, investigation, methodology, project administration, resources and writing – original draft. M.I. contributed to data curation, formal analysis, software, visualisation and writing – original draft. I.V.M. contributed to conceptualisation, investigation and validation. C.A.C. contributed to conceptualisation, methodology and supervision. E.P. contributed to data curation and investigation. S.D.B. contributed to conceptualisation, data curation, formal analysis, funding acquisition, methodology, project administration, supervision, validation and writing – review and editing. All authors provided their final approval for the version to be published.
Funding
The first author received funding from Iuliu Hațieganu University of Medicine and Pharmacy Cluj-Napoca (project no. 645/51, dated 11 January 2024) for doctoral research projects. The funding source played no role in the study’s design, data collection, analysis, interpretation, manuscript preparation or the decision to submit it for publication. The funding source did not influence the study’s findings and conclusions.
Declaration of interest
The authors confirm that there are no conflicts of interest or significant financial support that could have influenced this work. All authors have read and approved the manuscript, and no eligible contributors have been omitted. The order of authorship has been mutually agreed upon. Intellectual property considerations have been addressed and no issues prevent publication, including timing, in accordance with institutional regulations.



 Open access
Open access
eLetters
No eLetters have been published for this article.