


Medium-secure units (MSUs) treat people with complex mental health needs, who also pose a risk of harm to the public. Reference Mills and Davies1 MSUs have two fundamental aims: enable service user recovery while protecting the public. Limited research has demonstrated the effectiveness of MSUs in achieving these aims. Reference Smothers, Hill, Lawrence, Bagshaw and Watt2 Most of the available literature on reoffending is now dated and was published up to 20 years ago, Reference Coid, Kahtan, Gault, Cook and Jarman3 or reliant on historical samples. Reference Hill, Bagshaw, Hewlett, Perham, Davies and Maden4 MSUs are costly, Reference Walker, Amos, Knowles, Batson and Craissati5 but there is little evidence that investment in them has been effective. Demonstrating public protection is difficult to operationalise meaningfully because of the absence of comparison groups and confounding by discharge destinations and exposure to risk.
The single study that has reported the association between discharge destination and reconviction outcomes Reference Hill, Bagshaw, Hewlett, Perham, Davies and Maden4 reported higher reconviction rates for people discharged to prison, but substantial reductions in reconvictions relative to actuarially assessed risk in the sample as a whole. Research using more recent samples is required because of a wide range of policy changes (e.g. the Department of Health’s 2014 report ‘Positive and Proactive Care: Reducing the Need for Restrictive Interventions’ 6 ) likely to have affected the operation and effectiveness of secure services.
The aim of the current study was to build on previous work Reference Hill, Bagshaw, Hewlett, Perham, Davies and Maden4 and provide a similar analysis using data from a more contemporary cohort of service users. Differences between observed and predicted reconviction rates were contrasted between groups discharged to open conditions, prison or further secure care.
Method
Design
The study was a retrospective, secondary analysis of data from service user healthcare records and the Offenders Index (a Home Office database that has records of court disposals relating to standard list offences since 1963 in England and Wales). Outcomes included were (a) any reconviction and (b) violent reconviction, across three follow-up periods (2 years, 4 years and 6 years). Reconviction was coded cumulatively as a binary measure (yes/no). ‘Violent reconviction’ included any conviction categorised under the standard list offence category of ‘violence against the person’, as well as ‘common assault and battery’, ‘affray’, ‘sexual assault’, ‘assault on a constable’ and ‘assaulting a designated or accredited person’. ‘Any reconviction’ consisted of all offence types (including violent offences).
Discharge locations were explored to examine their association with reconvictions. Service users were categorised into three groups based on their discharge pathway from MSU care: open conditions (including community, open care home and open rehab), prison or locked units (including psychiatric intensive care unit/general psychiatric unit, locked rehab and low-, medium- or high-secure units). Twenty-five (12.2%) participants were discharged to prison, 85 (41.5%) were discharged to secure care and 95 (46.3%) were discharged into the community or open conditions.
The Offender Group Reconviction Scale 2 (OGRS-2) Reference Taylor7 was used to provide a continuous numerical score that estimated the per cent probability of reconviction within 2 years. OGRS-2 scores were based purely on official criminal histories and calculated from convicted offences before the date of admission to the MSU. Preadmission histories were used to give an estimate of risk before treatment in the medium-secure hospital, and therefore served as a baseline measure of risk.
Participants
Service users who were discharged from a single MSU in Wales, UK, between 30 July 1999 and 24 November 2017, were followed up through the Offenders Index. Data for 285 cases were collected by the original authors. For this study, 80 were excluded because full conviction histories were unavailable (25 of these cases died during the follow-up period; and were excluded as their Offenders Index files may have been deleted), leaving 205 cases for whom OGRS-2 scores could be calculated, and for whom post-discharge conviction outcomes were available. Of the 205 service users, 177 were male (86%) and 28 were female (14%). Participants ages ranged from 17 to 72 years, with a mean age of 34.5 years. The most common referral source was prison (49.8%) and the least common was police stations (0.5%).
Procedure
Original data collection was conducted as part of wider post-doctoral project Reference Hill8 and was sourced from the Offenders Index, alongside healthcare records. Data for the original research were collected without service user consent and in line with the Confidentiality Advisory Group conditions. The project was also approved by the NHS Research Ethics Committee as well as the Confidentiality Advisory Group (Confidentiality Advisory Group reference: 18/CAG/0090). Additional ethical approval for the current analysis was granted by the Cardiff Metropolitan University School of Sport and Health Sciences Ethics Committee (project reference number: PGT-7622). The procedure for the current study was to separate preadmission convictions from post discharge offences and use preadmission convictions to calculate the OGRS-2 scores for each case. Post-discharge convictions were used to determine cumulative binary post-discharge conviction outcomes (convicted/not convicted) for all possible cases over three follow-up periods (2, 4 and 6 years).
Materials
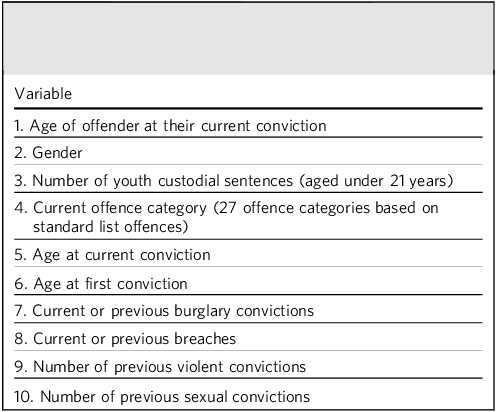
The OGRS-2 is an updated version of the original OGRS, Reference Copas and Marshall9 which uses ten criminogenic and demographic variables to create a probability score (0–100%) of reconviction for any standard offence within 2 years of leaving custody (Table 1). Sound predictive validity of the OGRS-2 has been shown to extend to 4 and 6 years for discharged MSU service users, Reference Hill, Bagshaw, Hewlett, Perham, Davies and Maden10 even though the OGRS model was only originally designed as a risk assessment tool for 2 years following imprisonment. Furthermore, following comparison with other available and established risk assessment tools, the OGRS-2 has been reported as performing similarly to other scales for offending outcome measures, including reconvictions for a combined categories of ‘any offence’ and violence. Reference Coid, Hickey, Kahtan, Zhang and Yang11
Criminogenic and demographic variables used by the Offender Group Reconviction Scale 2 to calculate a score of probability of reconviction

Method of analysis
Analyses were conducted using SPSS version 29 (IBM, Armonk, NY, USA). Receiver operating characteristic curves were used to determine the predictive validity of the OGRS-2 for any offence reconvictions.
One-way analysis of variance (ANOVA) compared preadmission reconviction risk (OGRS-2) between service users discharged to three different discharge pathways (open, locked units and prison).
Hazard ratios with 95% confidence intervals were used to compare any and violent reconviction outcomes between groups discharged to prison, open conditions and locked units. Observed reconviction rates (for any offence) were contrasted with mean predicted reconviction rates (OGRS-2 scores) with 95% confidence intervals separately for groups discharged to prison, open conditions and locked units.
Chi-squared tests were used to examine the associations between discharge pathways and violent reconvictions at 2, 4 and 6 years follow-up.
Results
Only 32 (15.6%) of the service users held remand status at the time of discharge (charged but not yet convicted). This low frequency reduced the likelihood of pseudo-reconviction (convictions for offences committed before psychiatric admission) affecting the results. Data were not analysed separately for remand and convicted cases.
Preadmission risk of reconviction and discharge pathways
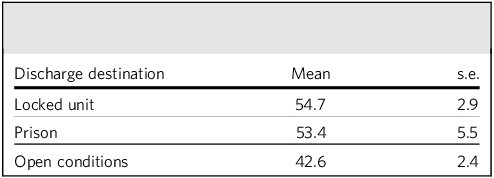
One-way ANOVA was used to determine whether preadmission OGRS-2 scores varied between service users discharged to different pathways. The data conformed with homogeneity of variance assumptions for ANOVA, assessed by Levene’s test for equality of variances (p = 0.075). OGRS-2 scores were compared between all three discharge locations (Table 2). Scores varied between the three pathways (F(2, 202) = 5.401, p = 0.005, η 2 = 0.051). The mean OGRS-2 score was highest for those discharged to locked units, followed by prison, and then open conditions. The only significant contrast in OGRS-2 scores was between the open conditions group and the locked unit group (p = 0.005): mean OGRS-2 scores were significantly lower (mean difference 12.1%) for the group discharged to open conditions.
Mean Offender Group Reconviction Scale 2 scores for each discharge location

OGRS-2 predictive validity
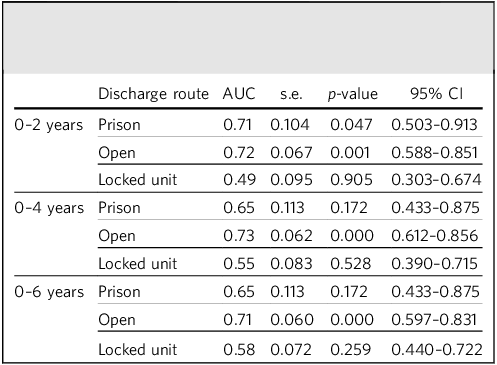
Receiver operating characteristic analysis was used to determine whether the OGRS-2 was a valid predictor of reconvictions for each of the three discharge destinations over time, and the results of these analyses are presented in Table 3. The predictive validity of the OGRS-2 varied between discharge routes: the OGRS-2 was able to discriminate between service users who were reconvicted against those not reconvicted when they were discharged to open conditions at all follow-up points. The OGRS-2 also showed significant predictive validity for the prison discharge route, but only in the initial 2-year follow-up period. OGRS-2 showed no predictive validity for service users who were discharged to locked units throughout the 6-year follow-up period.
Predictive power of the Offender Group Reconviction Scale 2 to predict any offence reconvictions up to 6 years post-discharge from medium-secure care

AUC of 0.5 indicated no relationship between OGRS-2 score and reconvictions; AUC of 1 would have indicated perfect predictive validity. AUC, area under the curve; OGRS-2, Offender Group Reconviction Scale 2.
Comparison of reconviction rates between discharge pathways
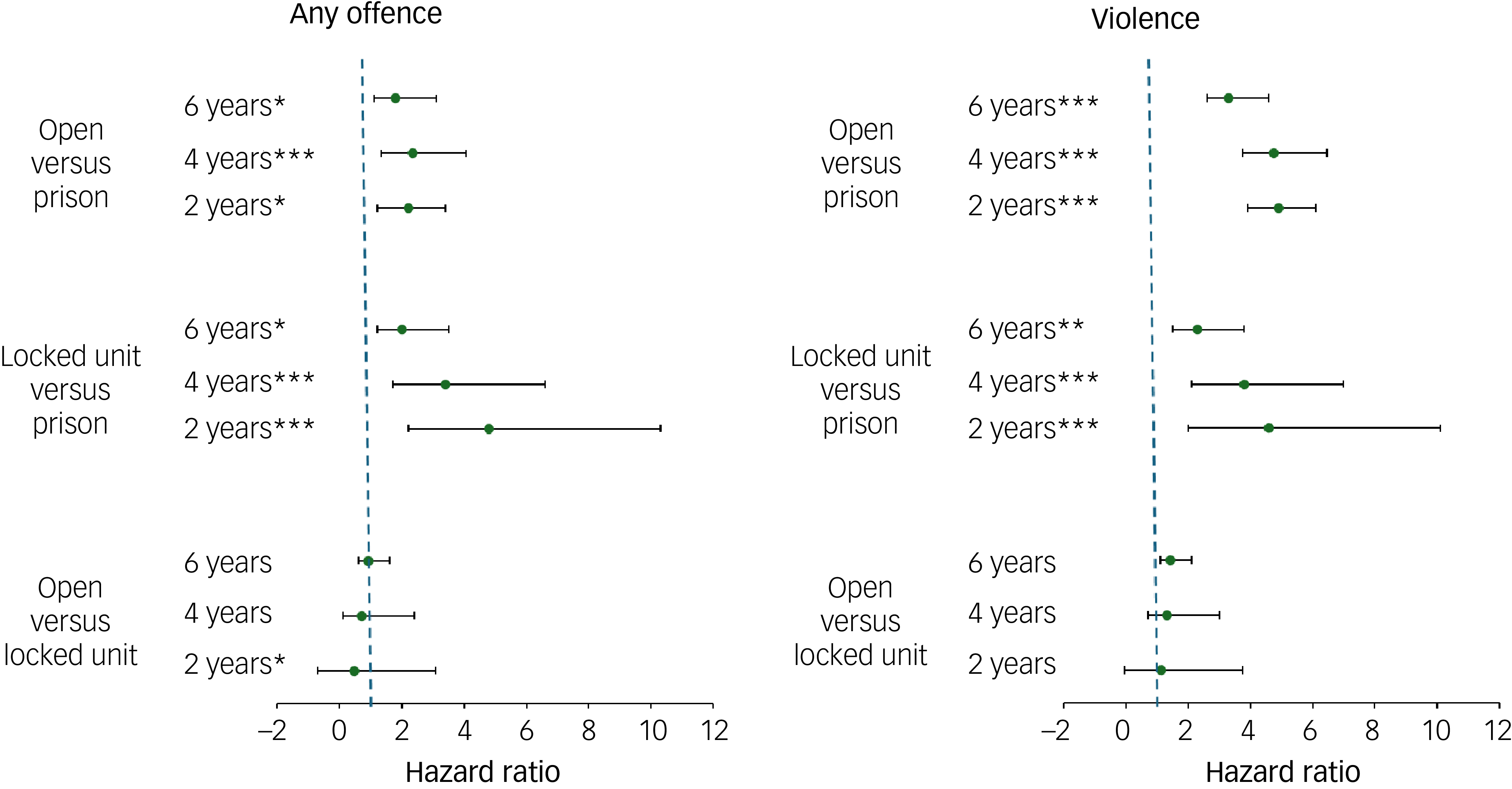
Hazard ratios with 95% confidence intervals were calculated to reflect all possible contrasts amongst the discharge pathways at each of the follow-up points (Fig. 1). Service users transferred to prison had reconviction outcomes more frequently than those transferred to locked units or open conditions at all three follow-up points. Reconvictions for people discharged to locked units remained lower than open conditions at all three follow-up points, but this difference decreased progressively at 4 and 6 years.
Hazard ratios with 95% confidence intervals for any and violent reconvictions at 2, 4 and 6 years follow-up. Service users were discharged to open, prison or locked psychiatric conditions. Significant associations between discharge location and conviction outcome are indicated. *p < 0.05, **p < 0.01, ***p < 0.005.

Service users transferred to prison had more frequent reconviction outcomes, for both any and violent offences, than those transferred to either locked units or open conditions at all three follow-up points. Violent reconvictions (but not any offences) were more frequent among people discharged to locked units than the open conditions group at all three follow-up points.
Predicted versus observed reconviction rates (any offence)
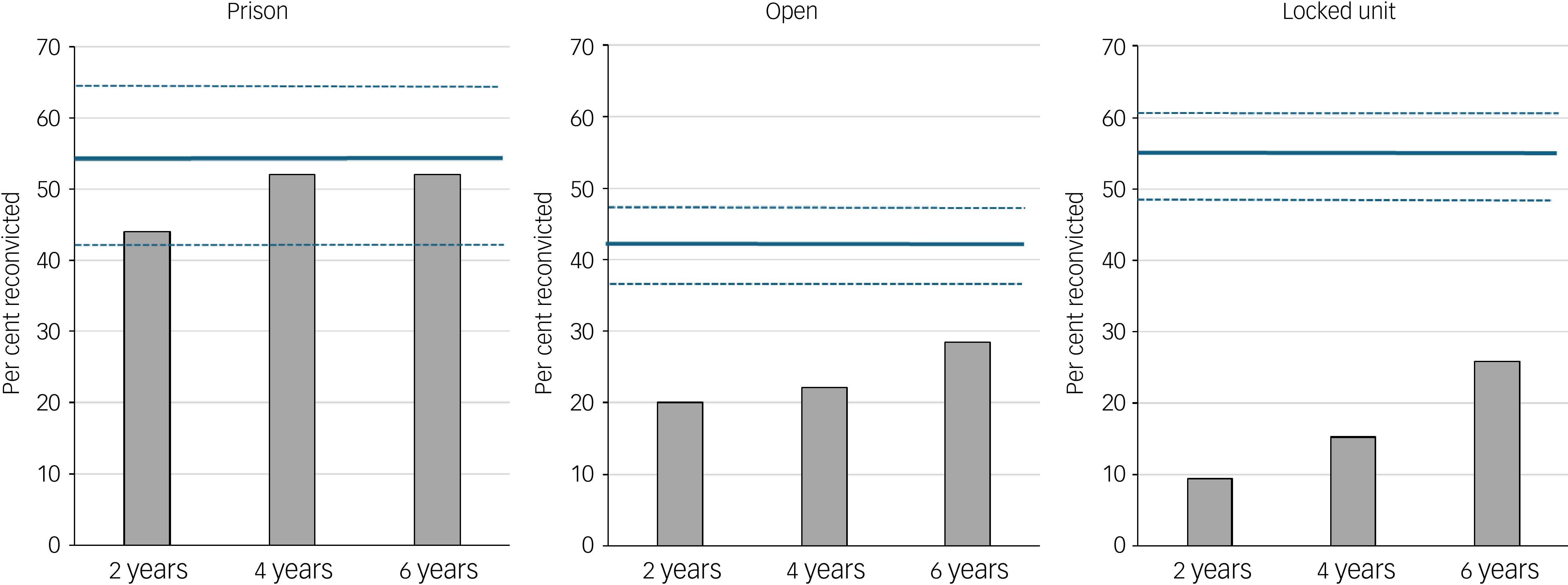
Figure 2 presents reconviction rates at 2, 4 and 6 years follow-up, cross-tabulated with discharge locations, for any offence reconvictions. Reconviction rates were highest for those discharged to prison throughout the entire follow-up period (6 years). Lowest reconviction rates were observed for service users transferred to locked units, and intermediate rates were observed for those discharged into open (unlocked) conditions. Figure 2 also presents predicted reconviction rates (mean OGRS-2 scores) for each of the three discharge destination groups, as well as 95% confidence intervals. The confidence intervals indicate the predicted range of reconviction rates for each of the discharge groups; observed reconviction rates below the lower 95% confidence interval boundary indicated a significant reduction in reconvictions relative to the OGRS-2 model. It was clear from Fig. 2 that reconviction rates for the group discharged to prison were within the OGRS-2 confidence intervals; there was no reduction in reconvictions. In contrast, the observed reconviction rates for the service users discharged to both open conditions and locked units were substantially below predicted reconviction rates across the whole follow-up period, suggesting that treatment in medium security plus onward placement in either open conditions or locked units was associated with significant reductions in reoffending.
Reconviction rates for any offence for three discharge locations and three follow-up periods following discharge form medium security. Solid horizontal lines show predicted reconviction rates (mean OGRS-2 scores), and hatched lines show lower and upper bounds for 95% confidence intervals. OGRS-2, Offender Group Reconviction Scale 2.

Reconvictions and discharge pathways (violent offences)
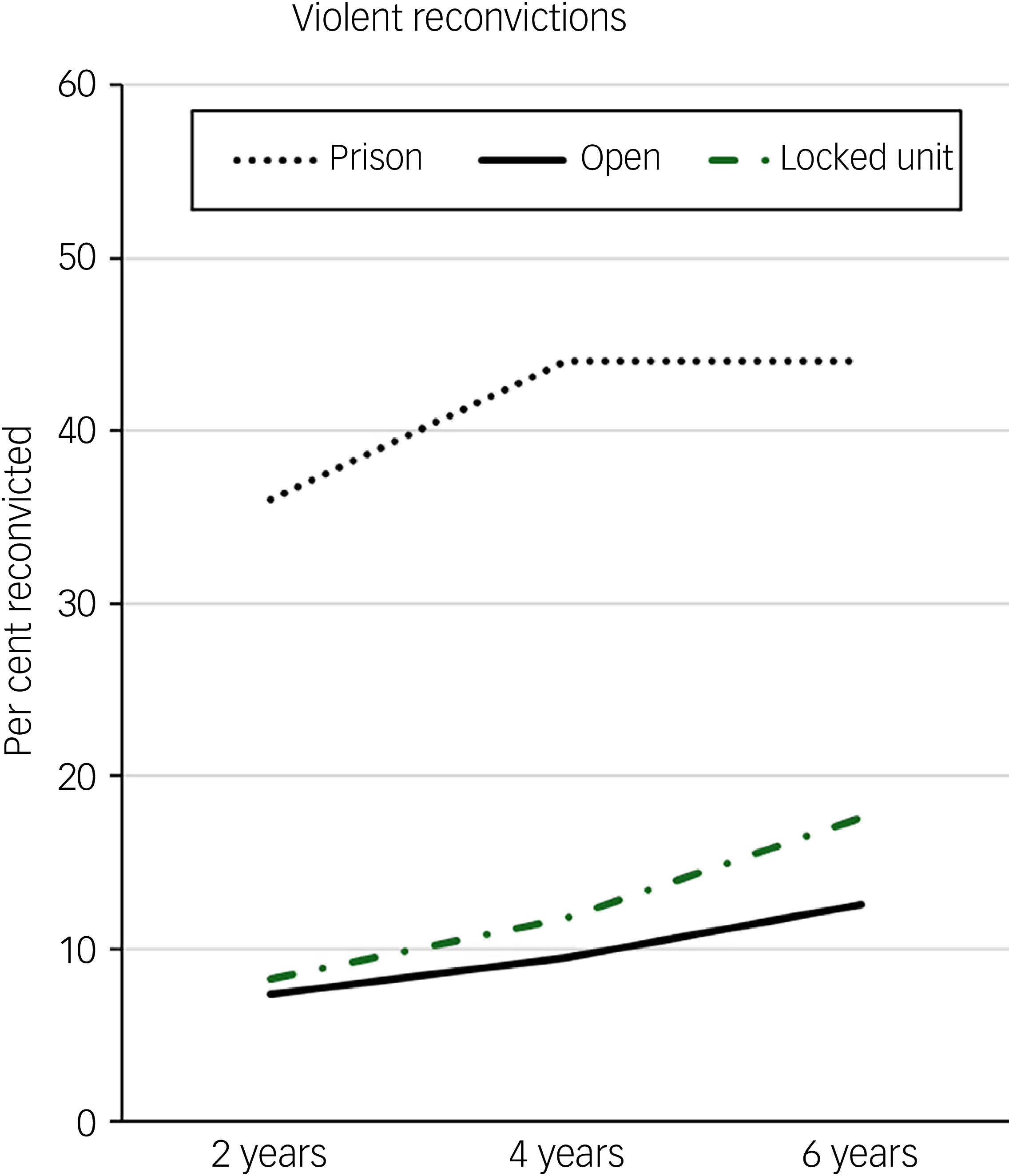
Violent reconviction rates for the three discharge groups across the 6-year follow-up period are presented in Fig. 3. The percentage of service users reconvicted for violent offences was highest for those discharged to prison across the three time periods. The percentage of service users reconvicted were low across open conditions and locked unit discharge pathways.
Reconviction rates for violent offences for three discharge locations and three follow-up periods following discharge from medium security.

When comparing open conditions and locked units, there was no association between pathway and violence convictions at 2 years (χ 2(1, n = 180) = 0.047, p = 0.828), 4 years (χ 2(1, n = 180) = 0.249, p = 0.617) or 6 years (χ 2(1, n = 180) = 0.885, p = 0.347) follow-up. There were, however, significant associations between discharge location and violent reconviction when comparing open conditions with prison at 2 years (χ 2(1, n = 120) = 14.04, p < 0.001), 4 years (χ 2(1, n = 120) = 16.987, p < 0.001) and 6 years (χ 2(1, n = 120) = 12.570, p < 0.001) follow-up. Significant associations were also found at 2 years (χ 2(1, n = 110) = 11.981, p < 0.001), 4 years (χ 2(1, n = 110) = 12.996, p < 0.001) and 6 years (χ 2(1, n = 110) = 7.433, p = 0.006) follow-up when comparing locked units and prison.
Discussion
The current analysis provides updated evidence (1999–2017) to add to a limited literature base evaluating reconviction outcomes of medium-secure service provision. Reconviction rates were lower than expected for service users discharged to open conditions and locked units based on estimates calculated by the OGRS-2 actuarial risk assessment tool. Reconviction rates were consistent with expected estimates for service users discharged to prison. The current findings imply the crucial role of discharge pathways for both public protection and maintaining the effects of medium-secure care. Further investigation into the implications of returning service users to prison settings would be informative to help inform policy and clinical decision-making.
The results show similar trends in reconviction outcomes based on different discharge locations relative to a national sample of service users discharged from medium security between 1997 and 1998, Reference Hill, Bagshaw, Hewlett, Perham, Davies and Maden4 despite multiple changes to the landscape of forensic care based on new laws and updated policies in the interim. High reconviction outcomes for those returning to prison was unsurprising, as prisons have been widely criticised as criminogenic rather than rehabilitative institutions. Reference Cullen, Jonson and Nagin12,Reference Duwe and Clark13 Individuals with severe mental illness who are released from prison also tend to show poor reoffending outcomes. Reference Fazel, Fimińska, Cocks and Coid14,Reference Igoumenou, Kallis, Huband, Haque, Coid and Duggan15 The frequency of remission to prison has doubled over recent decades in the UK, Reference Doyle, Coid, Archer-Power, Dewa, Hunter-Didrichsen and Stevenson16 and has prompted concern regarding the effectiveness of schemes designed to divert people from criminal justice into mental health services. Reference Birmingham, Awonogun and Ryland17 Reasons for this increase in the remission of individuals to prison include increased bed pressures and the limited capacity of the forensic mental health estate, as well as changes in UK health service policy that encourage the timely return of individuals to prison for whom treatment in hospital is no longer required or where no effective treatment is available. 20
The predictive validity of static actuarial risk assessment tools (like the OGRS-2) will be diminished by effective risk management; closer supervision or continued detention of people at high risk of further offending will restrict their exposure to risk. For instance, services might be more likely to discharge those at highest risk of further offending into secure settings (locked units) and disrupt the contribution of cases at highest risk to reconviction statistics. There is some evidence from the current data that the secure service was doing this, as the OGRS-2 scores for people discharged to locked units and prisons were significantly higher than for the group discharged to open conditions. Decisions regarding discharge routes were therefore informally aligned with OGRS-2 scores (to some degree), and this tool could therefore potentially be employed to supplement information contributing to discharge and rehabilitation planning before discharge from medium-secure services.
We observed that the OGRS-2 initially retained predictive validity for cases discharged to prison, but showed no predictive validity for people discharged to locked units throughout the follow-up period. This difference indicated that the prison discharge route was ineffective at preventing reoffending among people with a higher risk for reoffending. In contrast, the combination of low reconviction rates and the absence of predictive validity for the OGSR-2 in the group discharged to locked units showed that this route was effective in reducing reconvictions for those at higher risk.
Legal decision-making regarding whether a convicted person should be directed to prison or forensic mental health services are not informed directly by their risk for future offending according to OGRS-2 criteria. Instead, this is determined in each case by a court judge advised by two psychiatrists. The role of psychiatric advice in this instance is to determine whether the convicted person satisfies criteria for detention under the Mental Health Act 1983; if they do not, then the judge will ‘hand down’ an alternative sentence (depending on severity of the offence(s)), which might include prison. Furthermore, prisoners may be transferred (on the basis of two psychiatric opinions) to forensic mental health services if their mental state deteriorates such that it warrants in-patient treatment. It is important to note that judges’ decisions and psychiatric opinion were unlikely to be informed by OGRS-2 risk assessments. The elevated mean OGRS-2 scores for people discharged to locked services (see Fig. 2) may reflect informal appraisal of general criminogenic risk (like the OGRS-2 criteria) or the influence of historical factors on patient behaviour while in services, or these factors may be associated with poor patient recovery, only further empirical work will address this issue.
The inflexibility of static actuarial risk assessment tools (e.g. the OGRS-2) prevents detection of dynamic change in risk resulting from intervention, and has been the source of extensive criticism of this approach to risk assessment. Reference Douglas and Skeem18 However, the inflexible nature of actuarially assessed risk may confer substantial benefits for evaluating service effectiveness. The ability for services to disrupt the correspondence between predicted risk and observed outcomes could be a useful tool in assessing their effectiveness for selectively reducing reoffending in those at high risk.
Strengths and limitations
The current study provides contemporary evidence of reconviction outcomes for a cohort of patients discharged by medium-secure services in the UK. The use of the OGRS-2 model as a control for preadmission risk to estimate the impact of the service on reconviction outcomes helps to improve from the past research tendency to use purely descriptive evaluations of outcomes.
The results are reliant on data from a single medium-secure service based in Wales, limiting the generalisability to services in England, which has different policies and statutory legislation.
Reasons for remission to prison were not collected, which may have been because of sufficient recovery from mental health problems, lack of suitability of psychiatric treatment or pressure for space in medium-secure care with limited capacity. Further research is needed to examine remittance of service users to prison and factors influencing this decision-making process, particularly when considering the impact this seems to have on public protection.
The current study was limited by reliance on data from the Offenders Index. In some instances, offending behaviour may not have been reported or reached threshold for conviction, leading to an underestimate of true criminal behaviour following medium-secure care. Service users may have returned to hospital for care and treatment if risk behaviours escalated, as opposed to being managed through the criminal justice system. 19
Low reconviction rates in people retained in secure care may simply reflect their limited exposure to risk for reconviction (risk exposure is maximised by being in open conditions), and extending the follow-up period to capture data when people have been fully discharged from all in-patient services is needed to address this possibility. The current study also had no access to the release dates for those transferred to prison, and it is safe to assume that this group would have been at reduced risk for reconviction by virtue of continuing detention, at least initially. The current findings for those transferred to prison may therefore actually underestimate the negative effect of this discharge route, because of this group’s reduced time at risk. Future studies should try to factor in the amount of time people spend ‘at risk’ during the follow-up period, although compiling this fine-grain data would be very challenging and resource intensive.
About the authors
Ava Maidment was an MSc forensic psychology student at the Department of Applied Psychology at Cardiff Metropolitan University, Cardiff, UK. Charlotte Hill was a PhD student at the Department of Applied Psychology at Cardiff Metropolitan University, Cardiff, UK. Joseph Lloyd Davies is a senior lecturer in applied psychology at the Department of Applied Psychology at Cardiff Metropolitan University, Cardiff, UK. Daniel Lawrence is a senior lecturer in applied psychology at the Department of Applied Psychology at Cardiff Metropolitan University, Cardiff, UK. Ruth Bagshaw was a senior lecturer in applied psychology at the Department of Applied Psychology at Cardiff Metropolitan University, Cardiff, UK. Andrew Watt is a reader in applied psychology at the Department of Applied Psychology at Cardiff Metropolitan University, Cardiff, UK.
Data availability
The data that support the findings of this study are available from the corresponding author, A.W., upon reasonable request.
Acknowledgement
The authors acknowledge the help and support of the staff of The Caswell Clinic (Bridgend) for their advice and guidance when accessing information.
Author contributions
All authors made substantial contributions to the conception, analysis and drafting of the manuscript. A.W. and R.B. were most involved in developing the conception of the work. C.H., A.M., J.L.D. and A.W. drafted early versions of the manuscript, and D.L. helped to refine the work in relation to changing policy.
Funding
This work was funded by a European Social Fund (KESS2: CMK215) grant awarded to A.W. and R.B.
Declaration of interest
None.

 Open access
Open access
eLetters
No eLetters have been published for this article.