


Introduction
Childhood adverse experiences (e.g., abuse and neglect) are common experiences for children and have profound effects on individuals’ lifelong outcomes, including brain development, physical health, and mental health (Danese & Tan, Reference Danese and Tan2014; Teicher & Samson, Reference Teicher and Samson2016). Human brains undergo dramatic reconfiguration during adolescence, and these developing functional networks are highly susceptible to the influence of adversities, which may translate into biological risk for internalizing problems and physical health (Rakesh, Allen, et al., Reference Rakesh, Allen and Whittle2023). Nonetheless, susceptibility to adversity is heterogeneous, with some individuals maintaining adaptive functioning despite early risks. Therefore, investigating the impact of adverse factors and corresponding protective factors on the brain phenotypes of adolescents aged 10 years and older (Sawyer et al., Reference Sawyer, Azzopardi, Wickremarathne and Patton2018) is of significant importance for understanding and addressing potential negative outcomes.
Psychological resilience is conceptualized as the ability to adapt well and cope successfully when facing risk or adversity (Bonanno, Reference Bonanno2008). While psychological resilience has been regarded as a key capacity during childhood and adolescence for coping with adversity (Ungar & Theron, Reference Ungar and Theron2020), its specific impact on sub-dimensions of adverse childhood experiences remains unclear, as does its influence on brain phenotypes. Accordingly, the present study examined whether psychological resilience can buffer the influence of distinct adversity dimensions on resting-state brain network connectivity and how this mechanism influenced physical and psychological well-being concurrently and longitudinally.
The Dimensional Model of Adversity and Psychopathology (DMAP) proposes that distinct dimensions of childhood adversity experience differentially shape neurodevelopment and consequently psychopathology (McLaughlin et al., Reference McLaughlin, Weissman and Bitrán2019). This model identifies two principal dimensions of adversity: threat, including physical, emotional, or sexual abuse, and deprivation, defined as insufficient access to expected nurturing inputs like physical and emotional care. Threat experiences are expected to result in the alteration of biological fear learning systems, leading to impaired emotion regulation (McLaughlin et al., Reference McLaughlin, Weissman and Bitrán2019). In contrast, neglect experiences may lead to excessive synaptic pruning in the association cortex, which undermines cognitive functioning (Sheridan & McLaughlin, Reference Sheridan and McLaughlin2014).
Research on protective factors mitigating childhood adversity effects has grown substantially, yet remains disproportionately focused on environmental factors like supportive parenting (Brody et al., Reference Brody, Gray, Yu, Barton, Beach, Galván, MacKillop, Windle, Chen, Miller and Sweet2017; Cao et al., Reference Cao, Wang, Chen and Zhu2024; Rakesh, Cropley, et al., Reference Rakesh, Cropley, Zalesky, Vijayakumar, Allen and Whittle2021; Whittle et al., Reference Whittle, Vijayakumar, Simmons, Dennison, Schwartz, Pantelis, Sheeber, Byrne and Allen2017) and school climate (Hackman et al., Reference Hackman, Duan, McConnell, Lee, Beak and Kraemer2022; Rakesh, Seguin, et al., Reference Rakesh, Seguin, Zalesky, Cropley and Whittle2021). While the mitigating effects of the external environment on the neurodevelopmental consequences of childhood adversity have been well documented, less attention has been paid to individual-level protective factors. Among these, psychological resilience emerges as a particularly promising yet understudied factor, offering unique and readily implementable intervention opportunities for children facing adversity.
Psychological resilience has been conceptualized through multiple distinct perspectives in the literature. The capacity-oriented perspective conceptualizes psychological resilience not merely as a stable trait (Ahern et al., Reference Ahern, Ark and Byers2008), but more broadly as the capacity to adapt to stress and maintain functioning under adversity (Schultze-Lutter et al., Reference Schultze-Lutter, Schimmelmann and Schmidt2016). Although psychological resilience demonstrates trait-like characteristics, accumulating research demonstrates that it develops and fluctuates across the lifespan (Chen et al., Reference Chen, Liang, Yang, Gao and Zhang2022) and can be enhanced through targeted interventions (İme & Ümmet, Reference İme and Ümmet2024; Yuan, Reference Yuan2021). These findings suggest that psychological resilience is a modifiable capacity rather than a fixed predisposition, a perspective that is now widely recognized in the research community. Under this perspective, psychological resilience is typically regarded as an individual-level protective factor (Poole et al., Reference Poole, Dobson and Pusch2017a, Reference Poole, Dobson and Pusch2017b) and is commonly assessed through validated instruments like the Connor-Davidson Resilience Scale (Connor & Davidson, Reference Connor and Davidson2003). By contrast, the outcome-focused perspective defines psychological resilience as an observable phenomenon characterized by the maintenance or rapid recovery of adaptive functioning following adversity (Kalisch et al., Reference Kalisch, Russo and Mueller2024). Process-oriented perspectives further emphasize psychological resilience as “a dynamic process involving complex interactions across biological, psychological, social, and ecological systems that collectively enable individuals to preserve or enhance mental well-being when experiencing significant risk factors” (Ungar & Theron, Reference Ungar and Theron2020).
Emerging research adopting the capacity-oriented perspective has investigated how psychological resilience protects children facing adversity. Higher psychological resilience has been shown to mitigate or even eliminate the detrimental effects of adversity on psychological and physiological outcomes, including depression (Poole et al., Reference Poole, Dobson and Pusch2017b), anxiety (Poole et al., Reference Poole, Dobson and Pusch2017a), physical health (Wojujutari et al., Reference Wojujutari, Alabi and Emmanuel2019), epigenetic aging (Harvanek et al., Reference Harvanek, Fogelman, Xu and Sinha2021), and cortisol levels (Sun et al., Reference Sun, Lunkenheimer and Lin2023). Despite these findings, the extent to which the buffering role of psychological resilience is specific to particular sub-dimensions of childhood adversity, rather than generalizing across adversity types, remains unclear. More importantly, the neural underpinnings of this protective effect are poorly understood. A recent systematic review indicates that psychological resilience is associated with region-specific resting-state connectivity, including lower OFC-precuneus connectivity (Zhang et al., Reference Zhang, Rakesh, Cropley and Whittle2023). However, few studies have examined psychological resilience at the level of large-scale functional brain networks, with only one study reporting reduced coupling between the salience (SN) network and both the default mode (DMN) and frontoparietal (FPN) networks (Zhang et al., Reference Zhang, Rakesh, Cropley and Whittle2023). Clarifying the neurodevelopmental underpinnings of psychological resilience at the level of functional brain networks in the context of adversity and psychopathology could inform the development of more targeted interventions for children exposed to adversity.
Given that brain maturation was supported by large-scale network reconfiguration rather than particular regions (Bressler & Menon, Reference Bressler and Menon2010), research on childhood adversity and its protective factors should focus less on singular brain regions and more on large-scale functional networks. Most prior studies have focused on connectivity between specific brain regions such as the amygdala and prefrontal cortex (Cheng et al., Reference Cheng, Mills, Miranda Dominguez, Zeithamova, Perrone, Sturgeon, Feldstein Ewing, Fisher, Pfeifer, Fair and Mackiewicz Seghete2021; Herzberg et al., Reference Herzberg, McKenzie, Hodel, Hunt, Mueller, Gunnar and Thomas2021; Liu et al., Reference Liu, Song, Zhou, Huang, Zhang, Wang, Zhu, Lan, Yang and Zhao2023). However, large-scale network alterations remain understudied, with limited work focusing on the DMN, FPN, and SN networks (Chahal et al., Reference Chahal, Miller, Yuan, Buthmann and Gotlib2022; Cao et al., Reference Cao, Wang, Chen and Zhu2024; Rakesh, Allen, et al., Reference Rakesh, Allen and Whittle2023; Rakesh, Seguin, et al., Reference Rakesh, Seguin, Zalesky, Cropley and Whittle2021). Beyond the three core neurocognitive networks, dysfunction in the ventral attention (VAN) and somatomotor (SMN) networks is also frequently observed in depression and anxiety disorders (Liu et al., Reference Liu, Xu, Zhang, Jiang, Li and Luo2019; Ray et al., Reference Ray, Bezmaternykh, Mel’nikov, Friston and Das2021). Moreover, broader rsFC alterations during adolescence have been reported as a pathway linking childhood adversity to later depression (Rakesh, Kelly, et al., Reference Rakesh, Kelly, Vijayakumar, Zalesky, Allen and Whittle2021). To this end, we aim to explore how sub-dimensions of childhood adversity relate to large-scale brain network connectivity among Chinese adolescents and how psychological resilience may exert a protective effect.
In summary, the present study aimed to investigate the neural substrates of childhood threat and deprivation and to explore how psychological resilience might buffer these relationships. The study further examined whether psychological resilience moderates the association between adversity and brain network connectivity linked to current symptoms and whether these brain features predict mental health changes over six months. By integrating cross-sectional and longitudinal analyses, this study provides a comprehensive understanding of the neurobiological substrates of adversity-related vulnerability and resilience as both state-dependent neural correlates of current mental health and prospective predictors of symptom change over time, thereby informing the identification of neural features relevant for clinical treatment. We hypothesized that specific adversity dimensions would relate to distinct connectivity patterns but that psychological resilience would act as a general protective factor across both abuse and neglect. Finally, we hypothesized that higher psychological resilience would weaken the link between adversity and poor mental health through these neural pathways, whereas lower psychological resilience would leave individuals more vulnerable to negative outcomes.
Methods
Participants
Ninety-four rural Chinese children from 10 to 14 years old in Chinese primary schools (48 boys and 46 girls) participated in this study. These children often experience multiple adversities, including economic hardship, parental absence or limited care, poor family support and inadequate supervision, restricted access to educational and mental health resources, and higher rates of abuse and neglect (Fan & Wang, Reference Fan and Wang2023; Fellmeth et al., Reference Fellmeth, Rose-Clarke, Zhao, Busert, Zheng, Massazza, Sonmez, Eder, Blewitt, Lertgrai, Orcutt, Ricci, Mohamed-Ahmed, Burns, Knipe, Hargreaves, Hesketh, Opondo and Devakumar2018; Zhang et al., Reference Zhang, Liu and Long2021)
At baseline (T1), participants completed demographic questionnaires and assessments of childhood adversity, psychological resilience, and mental health symptoms, including somatization, anxiety, and depression. Immediately following the behavioral assessments, participants underwent magnetic resonance imaging (MRI) scans. Six months later (T2), participants completed follow-up questionnaires assessing somatization, anxiety, and depression symptoms. No participants reported neurological or psychiatric disorders in the past 6 months. Two participants were excluded from the study due to excessive head motion during image scanning (with a maximum displacement over 5 mm). Thus, the final analysis included 92 participants, aged between 10.01 and 14.12 years (46 boys and 46 girls, M = 11.80 years, SD = 0.72). All participants gave written informed consent and were compensated for the involvement. Study procedures were approved by the Faculty of Psychology at Beijing Normal University (IRB No. 202003260031).
Measures
Participants completed measures of demographic information, childhood adversity, and psychological resilience at baseline (T1), and reported somatization, anxiety, and depression symptoms at both T1 and T2 (6-month follow-up).
Childhood adversity
The Childhood Trauma Questionnaire (CTQ) (Bernstein et al., Reference Bernstein, Stein, Newcomb, Walker, Pogge, Ahluvalia, Stokes, Handelsman, Medrano, Desmond and Zule2003) is a validated self-report questionnaire (e.g., I was punished with a belt, a board, a cord, or some other hard object) used to assess five types of adversities experienced during childhood: emotional, physical, and sexual abuse, as well as emotional and physical neglect. In line with prior study (Cao et al., Reference Cao, Wang, Chen and Zhu2024), sexual abuse was not assessed in this study due to the sensitive nature of the topic in Chinese elementary schools, which limited reliable and ethical measurement. Participants rate the items on a 5-point scale ranging from “Never True” to “Very Often True.” To analyze the different effects of abuse and neglect, we summed the scores of physical and emotional abuse, hereafter referred to as “abuse,” and averaged the scores of physical and emotional neglect, hereafter referred to as “neglect” (Rakesh, Allen, et al., Reference Rakesh, Allen and Whittle2023). The Cronbach’s α was .840 and .787 for the abuse and neglect dimension, respectively.
Psychological resilience
The 10-item Connor-Davidson Resilience Scale (CD-RISC) is a widely used scale for assessing an individual’s resilience and their ability to cope with adversity (e.g., can deal with whatever comes), and is widely used among Chinese children and adolescents (Connor & Davidson, Reference Connor and Davidson2003; Chen et al., Reference Chen, Liang, Yang, Gao and Zhang2022). In this study, we utilized the Chinese version of the CD-RISC, which consists of items rated on a scale from 0 (“not true at all”) to 4 (“true nearly all of the time”). A higher CD-RISC score then indicates a greater psychological resilience. The Cronbach’s α was .908.
Somatization symptoms at T1 and T2
The abbreviated version of the Children’s Somatization Inventory (CSI), consisting of the six most frequently endorsed items (i.e., headache, stomachache, nausea, tiredness, sore muscles, feeling weak), was used to assess physical health in children and adolescents (Garber et al., Reference Garber, Walker and Zeman1991). Participants rated the items on a 4-point scale ranging from “Almost Never” to “Almost Always.” A higher score on the CSI indicates worse physical health. The Cronbach’s α was .840 and .836 at baseline and six months later, respectively.
Anxiety at T1 and T2
Anxiety symptoms were measured using the self-report Chinese version of the Generalized Anxiety Disorder Scale (GAD-7) (Liu, Yang et al., Reference Liu, Zhang and Cai2017). The GAD-7 consists of seven items about worry or somatic tension during the last two weeks (e.g., worrying too much about different things). Each item scored from 0 (not at all) to 3 (nearly every day), with total scores ranging from 0 to 21. The higher scores indicate higher severity of anxiety disorders. The Cronbach’s α was .934 and .923 at baseline and six months later, respectively.
Depression at T1 and T2
Depressive symptoms were assessed with the Chinese version Center for Epidemiological Studies – Depression (CES-D) scale (e.g., not being able to shake off the blue) (Chen, et al., Reference Chen, Yang and Li2009; Radloff, Reference Radloff1977). As a screening instrument (not a clinical diagnostic measure), the CES-D assesses the frequency of depressive symptoms (e.g., “not being able to shake off the blues”) experienced during the past week. The scale comprises 13 items, and participants self-rate their degree of experience using a 4-point scale: “rarely or never” (less than 1 day), “not too often” (1-2 days), “sometimes or half the time” (3-4 days), and “most of the time” (5-7 days). A higher CES-D score indicates the presence of more depressive symptoms. The Cronbach’s α was .855 and .755 at baseline and six months later, respectively.
Control variables
The biological sex, age, and subjective socioeconomic status (subjective SES) of the adolescents were treated as covariates and controlled for in all subsequent analyses. In the longitudinal analyses, baseline symptoms (depression, anxiety, or somatization, depending on the outcome variable) were also controlled for to account for initial individual differences. Subjective SES was assessed using the MacArthur ladder tool (Operario et al., Reference Operario, Adler and Williams2004), which presented a 10-rung ladder, with 1 representing the lowest socioeconomic position and 10 the highest.
MRI acquisition and data preprocessing procedures
MRI data were acquired using the Siemens 3.0T scanner (Magnetom Trio Trim syngo, Germany). Resting-state fMRI data were acquired with a T2*sensitive echo-planar imaging (EPI) sequence with these parameters: TR = 2000 ms; TE = 30 ms; flip angle = 90°; voxel size = 3 × 3 × 4 mm3; 0.6 mm skip, 180 volumes. During the resting-state scanning, participants were asked to keep their eyes open and remain still. T1-weighted structural images were obtained through a 3D sagittal magnetization-prepared rapid gradient echo (MPRGE) with a total of 192 slices by the following parameters: TR = 2,530 ms; TE = 3.45 ms; inversion time (TI) = 1100ms; FA = 7°; FOV = 100 × 100 mm2; acquisition matrix = 256 × 256; bandwidth (BW) = 190Hz/Px; slice thickness = 1 mm; no gap.
Functional MRI preprocessing was conducted using fMRIPrep v20.2.1(Esteban et al., Reference Esteban, Markiewicz, Blair, Moodie, Isik, Erramuzpe, Kent, Goncalves, DuPre, Snyder, Oya, Ghosh, Wright, Durnez, Poldrack and Gorgolewski2019). The standard preprocessing pipeline in fMRIPrep was followed, which included skull stripping, slice time correction, susceptibility distortion correction, functional-anatomical co-registration, and calculation of confounding time series per participant. The data was then spatially smoothed using a 6 mm full-width-at-half-maximum isotropic Gaussian kernel. ICA-based Automatic Removal Of Motion Artifacts (AROMA) was used to clean up data using the non-aggressive regression setting. Following fMRIPrep preprocessing, the first 10 volumes of functional images were discarded due to participants’ adaptation to scanning noise and signal equilibrium. Subsequently, the whole-brain masked rs-fMRI data were detrended, band-pass filtered (0.009−0.08 Hz), nuisance regressed, and standardized with Nilearn’ image.clean_img (version 0.10.1). The nuisance regressors were obtained from fMRIPrep, including the Friston-24 head-motion parameters, and signals from white matter (WM) and cerebrospinal fluid (CSF). Consistent with previous adolescent resting-state functional connectivity studies of adversity, we excluded participants whose maximum framewise displacement value exceeded 5 mm and then the mean frame-to-frame displacement (FD) for all participants was less than 0.5 mm (Rakesh, Allen, et al., Reference Rakesh, Allen and Whittle2023).
Network analysis of the functional connectivity network
Mean time series were extracted from 100 predefined cortical parcels in native space according to the Schaefer atlas (Schaefer et al., Reference Schaefer, Kong, Gordon, Laumann, Zuo, Holmes, Eickhoff and Yeo2018). These regions were organized into seven functional networks: visual (VN), SMN, dorsal attention (DAN), VAN, limbic (LN), FPN, and DMN networks (Thomas Yeo et al., Reference Thomas Yeo, Krienen, Sepulcre, Sabuncu, Lashkari, Hollinshead, Roffman, Smoller, Zöllei, Polimeni, Fischl, Liu and Buckner2011). Functional connectivity between regions was estimated by calculating the Pearson correlation between their mean time series. All correlation coefficients were then transformed using Fisher’ r-to-z method. Within-network connectivity was quantified by averaging all pairwise correlations within a network (e.g., FPN-FPN), whereas between-network connectivity was obtained by averaging correlations between ROIs of one network and those of other networks (e.g., FPN-DMN) (Cao et al., Reference Cao, Wang, Chen and Zhu2024).
Statistical analysis
Linear regression models were first used to investigate whether experiences of abuse or neglect were associated with differences in brain network connectivity, controlling for age, gender, subjective SES, and the other dimension of experience (e.g., neglect or abuse). The false discovery rate adjustment (p < 0.05) was considered for multiple comparisons (Benjamini & Hochberg, Reference Benjamini and Hochberg1995). Within-network analyses (7 connectivities) and between-network analyses (21 connectivities) were corrected separately.
Moderation analyses were conducted to examine the moderation effect of psychological resilience, controlling for age, gender, and subjective SES. To investigate whether the moderation effect was specific to abuse or neglect, we also covariated neglect and the interaction term between neglect and resilience in abuse models, and vice versa. FDR correction was separately applied to the 7 within-network and 21 between-network connectivities. Simple slope analyses were conducted to examine whether the relationship between childhood adversity and network connectivity significantly deviates from zero at 0.5 SD above the mean, at the mean itself, and 0.5 SD below the mean score of psychological resilience.
If there was a significant moderation model, moderated mediation effect models were used to test how abuse or neglect influenced concurrent and six-month-later somatization, depression, and anxiety symptoms through brain network connectivity at different levels of psychological resilience. All longitudinal models were adjusted for corresponding baseline symptom severity (depression, anxiety, or somatization symptoms) depending on the outcome variable. The moderation analysis and moderated mediation analysis were performed using the PyProcessMacro - a Python implementation of Andrew F. Hayes’ PROCESS Macro.
Results
Descriptive statistics and correlation analysis
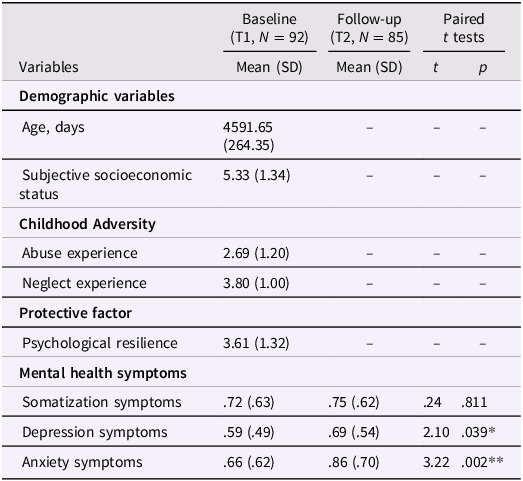
The descriptive statistics of demographic and psychological variables are shown in Table 1. There was a significant positive and moderate association between abuse and neglect (r = .36, p = .0004). The experience of more abuse was found to be associated with higher concurrent somatization, depression, and anxiety symptoms (r = .28, .48, .50, p = .01, .000, .000), as well as higher depression and anxiety symptoms six months follow up (r = .33, .26, p = .002, .02). In contrast, the experience of more neglect was associated with higher concurrent and six-month follow-up depression symptoms (r = .41, .36, ps < .0001).
Descriptive statistics of demographic and psychological variables
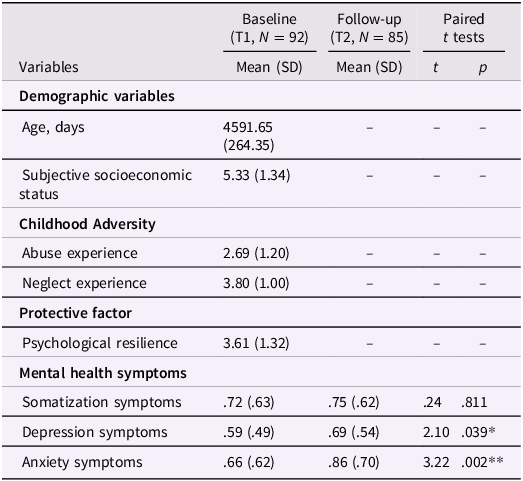
Table 1. Long description
The table presents descriptive statistics of demographic and psychological variables, comparing baseline and follow-up data. It includes variables such as age, subjective socioeconomic status, abuse experience, neglect experience, psychological resilience, and mental health symptoms like somatization, depression, and anxiety. The table has four main sections: demographic variables, childhood adversity, protective factors, and mental health symptoms. Each section lists the mean and standard deviation for baseline and follow-up periods, along with paired t-test results. Notable trends include significant associations between abuse and neglect experiences with various mental health symptoms.
Note. Dashes (—) indicate variables not measured at T2. For somatization symptoms, the follow-up sample size was N = 84 due to missing data. *p < .05, **p < .01.
Abuse, neglect, and within/between-network connectivity
As shown in Figure S1, the results of linear regression analysis indicated that abuse experience was not significantly associated with any specific network connectivity controlling for age, gender, SES, and neglect after correction for multiple comparisons. Similarly, no significant results were found in the neglect model. Results remained consistent when excluding participants with mean FD > 0.2 mm.
Psychological resilience as a moderator of relationships between abuse/neglect and within/between-network connectivity
To examine whether psychological resilience may moderate the unique effects of abuse or neglect on functional connectivity, we tested the role of psychological resilience as a moderator in all within- and between-network connectivities. As shown in Figure 1A, only the associations between abuse experience and limbic-somatomotor (LN-SMN) connectivity (β = −.06, s.e. = .02, FDR p = .04) as well as limbic-ventral attention network (LN-VAN) connectivity (β = −.06, s.e. = .02, FDR p = .04) were significantly moderated by psychological resilience. Results were similar when excluding participants with mean FD > 0.2 mm (LN-SMN connectivity: β = −.06, s.e. = .02, FDR p = .03; LN-VAN connectivity: β = −.06, s.e. = .02, FDR p = .03). As shown in Figures 1B and 1C, simple slopes found that higher abuse was associated with greater LN-SMN (β = .07, se = .03, p = .02) and LN-VAN (β = .09, se = .03, p = .007) connectivity in individuals with lower psychological resilience. No significant association between abuse and functional connectivity was found in those with average and higher levels of psychological resilience (p > .05). In contrast, the relationship between neglect experience and functional connectivity was not significantly moderated by psychological resilience.
Moderation of the relation between abuse or neglect experience and brain network connectivity by psychological resilience. (A). Chord diagrams of the connectivity between the LN and both the SMN and the VAN that were signifcantly predicted by the abuse and psychological resilience interaction terms. The color of the line represents the significance of the p-value (dark line: FDR p < .05; gray line: FDR p > .05) and the thickness of the line represents the -log10 FDR p-value (thicker lines indicate larger p-values). (B–C). Abuse experience was positively associated with both LN-VAN connectivity (B) and LN-SMN connectivity (C), controlling for neglect experience, in participants with lower psychological resilience (0.5 SD below the mean and smaller). However, this association was not observed in participants with moderate (0.5 SD above or below the mean) or high (0.5 SD above the mean or greater) levels of psychological resilience. LN, limbic network; SMN, somatomotor network; VAN, ventral attention network; VN, visual network; DAN, dorsal attention network; DMN, default mode network; FPN, frontoparietal network.
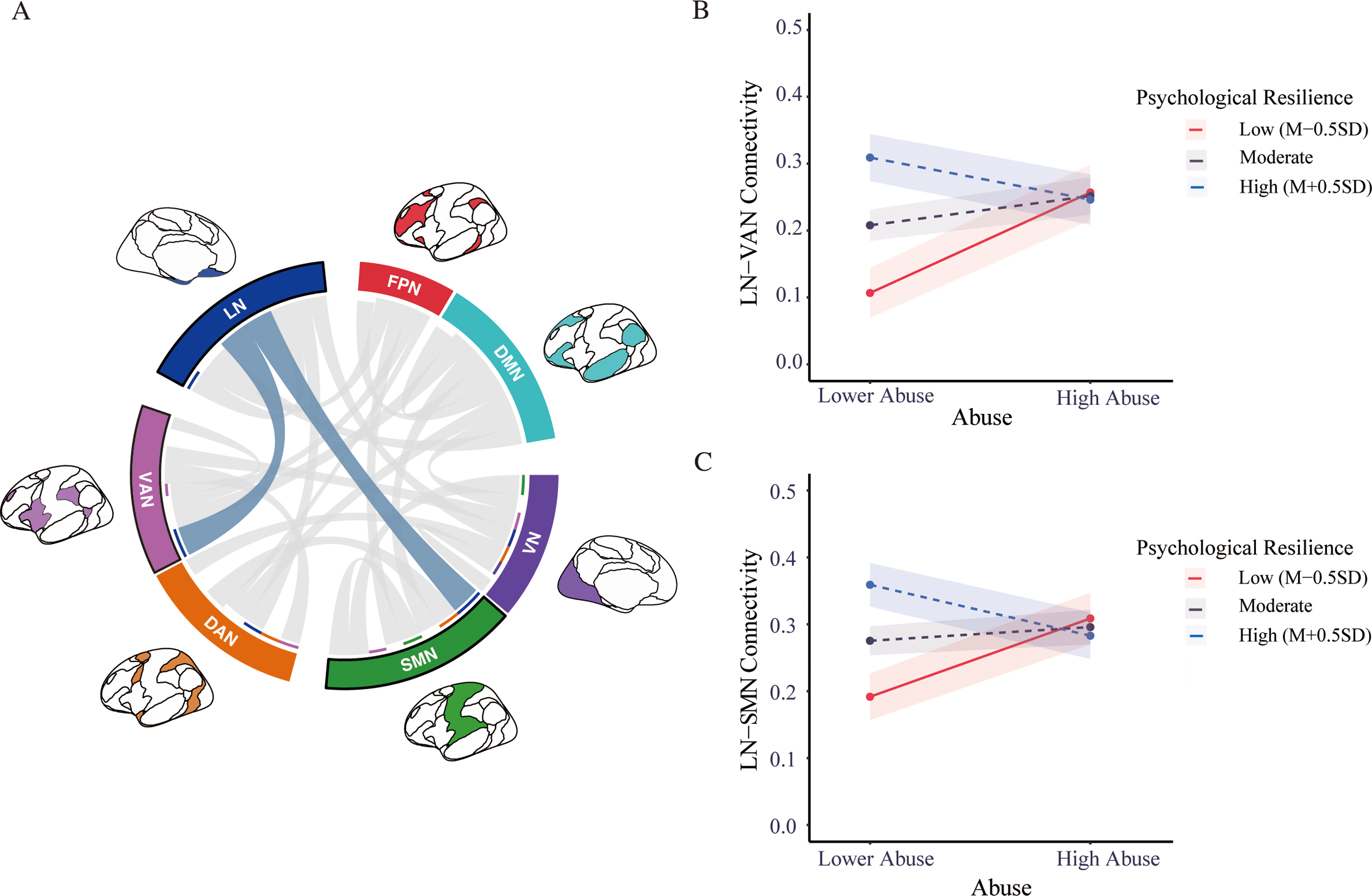
Figure 1. Long description
The chord diagram illustrates the connectivity between the limbic network (LN) and both the somatomotor network (SMN) and the ventral attention network (VAN), significantly predicted by the interaction of abuse and psychological resilience. The color of the lines represents the significance of the p-value, with dark lines indicating FDR p-value less than 0.05 and gray lines indicating FDR p-value greater than 0.05. The thickness of the lines represents the negative log of the FDR p-value, with thicker lines indicating larger p-values. The two line graphs show the relationship between abuse experience and LN-VAN connectivity (b) and LN-SMN connectivity (c), controlling for neglect experience. In participants with lower psychological resilience, abuse experience is positively associated with both LN-VAN and LN-SMN connectivity. However, this association is not observed in participants with moderate or high levels of psychological resilience. All values are approximated.
Moderated mediation model: predicting concurrent and six-month follow-up somatization, depression, and anxiety symptoms
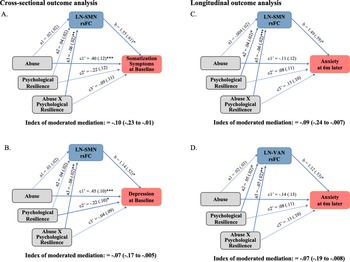
Due to the significant moderation effect of psychological resilience on the relationship between abuse and LN-SMN as well as LN-VAN connectivity, further analyses were performed to investigate moderated mediation models. These models aimed to examine how abuse influenced the cross-sectional and six-month-later somatization, anxiety, and depression symptoms through LN-SMN and LN-VAN connectivity at different levels of psychological resilience. As shown in Figures 2A and 2B, moderated mediation analyses revealed that only among individuals with low psychological resilience, greater LN-SMN connectivity significantly mediated the association between childhood abuse and increased concurrent somatization (the standardized index of moderated mediation = −0.10, 95% CI [−0.23, −0.01]) as well as increased depression symptoms (index = −.07, [−.17, −.005]). This mediation pathway was non-significant at moderate-to-high psychological resilience levels. The results remain consistent among participants with FD < 0.2 mm. Similarly, greater connectivity in both LN-SMN (index = −.09, [−.24, −.007]) and LN-VAN (index = −.07, [−.19, −.008]) mediated the association between childhood abuse and six-month follow-up anxiety only among individuals with low psychological resilience levels (see Figures 2C and 2D). The results were no longer significant when excluding participants with FD > 0.2 mm.
Moderated mediation analysis. (A–B) LN-SMN connectivity mediated the association between abuse experience and concurrent somatization symptoms and depression symptoms when psychological resilience was low. (C–D) LN-SMN connectivity and LN-VAN connectivity mediated the association between abuse experience and six-month follow-up anxiety symptoms when psychological resilience was low. In the concurrent analysis, the models controlled for gender, age, and subjective socioeconomic status. Additionally, neglect experience and the interaction term between neglect experience and psychological resilience were also included as covariates in the analysis. The longitudinal analysis model was similar to the cross-sectional analysis, with the additional control for corresponding baseline symptoms. Results are B (standard error); *p < 0.05, **p < 0.01, ***p < 0.01. LN, limbic network; SMN, somatomotor network; VAN, ventral attention network.
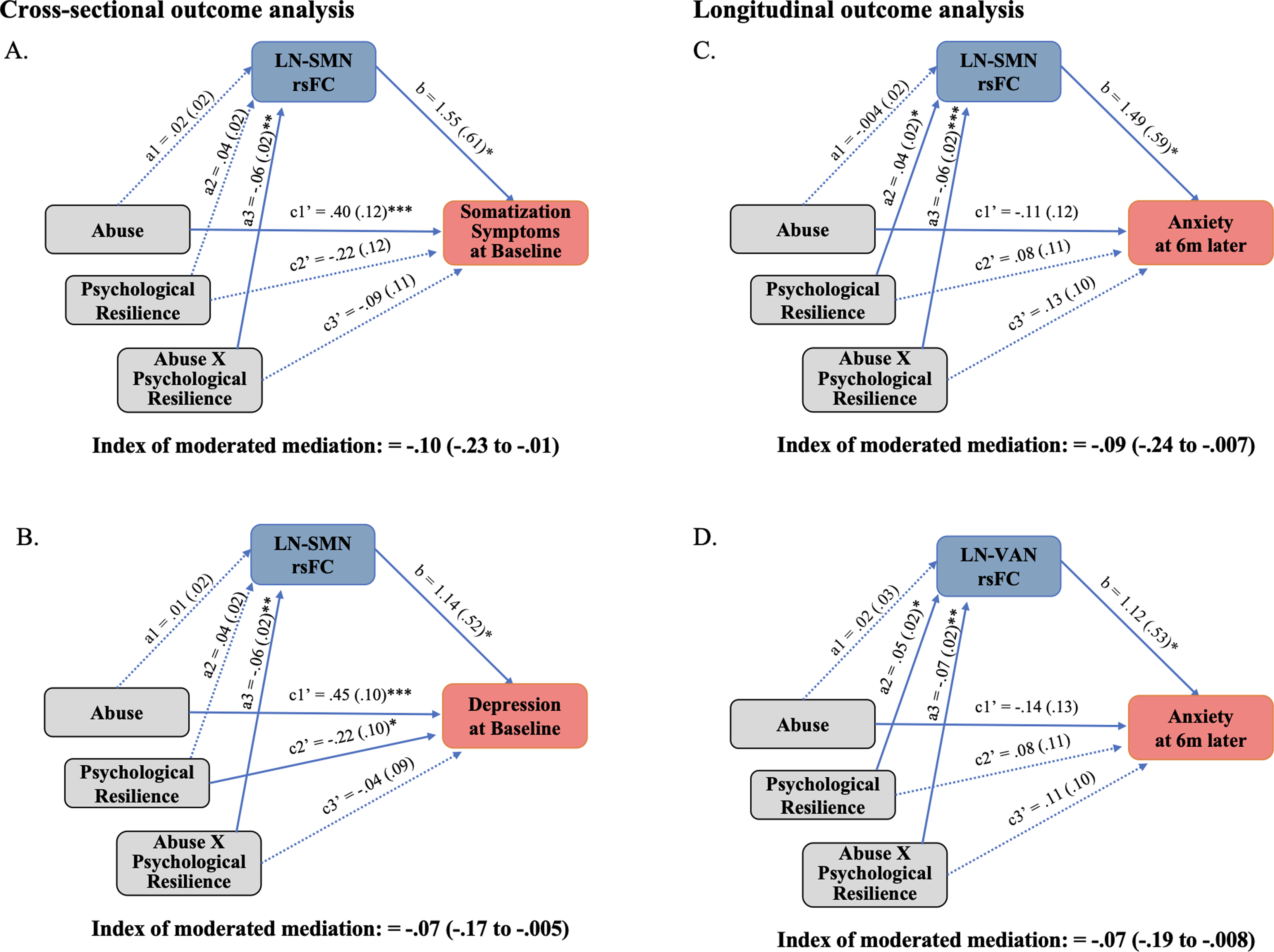
Figure 2. Long description
The flowchart illustrates a moderated mediation analysis examining the relationship between abuse, psychological resilience, and mental health outcomes. It includes four sub-diagrams labeled A, B, C, and D. Each sub-diagram shows paths between abuse, psychological resilience, brain network connectivity, and various mental health outcomes. Abuse and psychological resilience interact to influence brain network connectivity, which in turn affects somatization symptoms, depression symptoms, and anxiety symptoms. The paths are annotated with coefficients and significance levels, indicating the strength and direction of these relationships. The analysis controls for various factors such as gender, age, socioeconomic status, and baseline symptoms.
Discussion
The present study aimed to investigate the general or specific effect of psychological resilience in mitigating the impact of distinct adversity dimensions on resting-state functional connectivity in children and adolescents. This study also aimed to explore how this buffering mechanism affects both mental and physical health, both concurrently and longitudinally. Our findings suggest that higher psychological resilience can disrupt or attenuate the neurobiological pathways linking childhood adversity to poor mental health outcomes. Specifically, when psychological resilience was low, childhood abuse influenced current somatic and depressive symptoms via LN-SMN connectivity, and it also affected future anxiety symptoms after six months through a combination of LN-SMN and LN-VAN connectivity. However, when psychological resilience was moderate to high, these neurobiological pathways were not significant. Furthermore, childhood neglect did not significantly impact resting-state connectivities, regardless of the level of resilience. These findings emphasized psychological resilience as a modifiable neuroprotective factor that specifically mitigates the effects of abuse (but not neglect) through functional connectivity pathways, providing valuable insights for early intervention strategies.
Our findings challenge the hypothesis that psychological resilience functions as a generalized protective factor, instead revealing dimension-specific buffering effects with respect to distinct dimensions of childhood adversity. Specifically, we demonstrate that psychological resilience mitigates the neural impact of childhood abuse, but does not offer significant protection against childhood neglect, regardless of resilience level. This study advances beyond traditional environmental protective factors (e.g., supportive parenting (Brody et al., Reference Brody, Gray, Yu, Barton, Beach, Galván, MacKillop, Windle, Chen, Miller and Sweet2017; Cao et al., Reference Cao, Wang, Chen and Zhu2024; Rakesh, Cropley, et al., Reference Rakesh, Cropley, Zalesky, Vijayakumar, Allen and Whittle2021; Whittle et al., Reference Whittle, Vijayakumar, Simmons, Dennison, Schwartz, Pantelis, Sheeber, Byrne and Allen2017), school climate (Hackman et al., Reference Hackman, Duan, McConnell, Lee, Beak and Kraemer2022; Rakesh, Seguin, et al., Reference Rakesh, Seguin, Zalesky, Cropley and Whittle2021) to emphasize the potential of individual psychological resilience as an intervention target. Moreover, we extend previous research that treated childhood adversity as a uniform construct (Poole et al., Reference Poole, Dobson and Pusch2017a, Reference Poole, Dobson and Pusch2017b), highlighting that psychological resilience selectively protects against abuse-related impacts based on the nature of the adversity. This specificity likely stems from the differential characteristics of abuse and neglect. While childhood abuse, characterized by intermittent and unpredictable traumatic events, may accelerate cortico-limbic maturation (Beck et al., Reference Beck, Whitmore, MacSweeney, Brieant, Karl, Lange, Westlye, Mills and Tamnes2024) and heighten susceptibility to stress-related psychopathology (Rakesh, Allen, et al., Reference Rakesh, Allen and Whittle2023), psychological resilience helps buffer these effects through enhanced cortico-limbic regulation (Gupta et al., Reference Gupta, Love, Kilpatrick, Labus, Bhatt, Chang, Tillisch, Naliboff and Mayer2017). In contrast, childhood neglect, involving chronic deprivation of cognitive, emotional, and material resources, may exceed the compensatory capacity of resilience. The dimension-specific nature of psychological resilience underscores the necessity for tailored intervention strategies. For childhood abuse, strengthening psychological resilience emerges as a promising intervention approach. However, to address the neurodevelopmental consequences of neglect, interventions should focus on alleviating chronic environmental deprivation through cognitive enrichment, material resource provision, and sensitive caregiving training (McDermott et al., Reference McDermott, Norton and Mackey2023).
Greater intrinsic connectivity between LN and VAN/SN significantly correlated with childhood abuse in children with lower psychological resilience. This connectivity also indirectly influenced anxiety symptoms six months later in these children. This finding aligns with the DMAP model, which posits that abuse experience may lead to modifications in neural systems responsible for salience processing and emotion regulation (McLaughlin et al., Reference McLaughlin, Weissman and Bitrán2019). The LN network encompasses the temporal pole (TP), as well as the orbitofrontal cortex (OFC), involving emotion regulation, reward processing, and motivation (Catani et al., Reference Catani, Dell’Acqua and Thiebaut De Schotten2013). The VAN/SN network, encompassing regions like the parietal operculum, frontal operculum, lateral prefrontal cortex, and parietal-temporal-occipital association area, is integral to detecting and responding to salient stimuli (Han & Marois, Reference Han and Marois2014). According to Beck’ cognitive model of emotional disorders (Beck et al., Reference Beck, Emery and Greenberg2005), the LN-VAN/SN connectivity correlated with childhood adversity may indicate that children in adversity have enhanced biased attention deficits and enhanced biased schema. The Triple Network Model of psychopathology further posits that this hyperconnectivity may interact with the aberrant FPN network’ engagement and the default network’ disengagement (Menon, Reference Menon2011). Such disruptions in network dynamics may compromise cognitive control and result in inappropriate assignment of emotional saliency to mundane events, thereby contributing to anxiety problems.
Interestingly, the study found that abuse was also linked to greater resting state functional connectivity between LN and SMN networks in children with lower psychological resilience. This observation partially aligns with existing literature demonstrating similar connectivity patterns in individuals exposed to lower SES, where greater connectivity within and between SMN networks has been consistently reported (Rakesh, Zalesky, et al., Reference Rakesh, Zalesky and Whittle2021). The SMN network includes somatosensory (postcentral gyrus) and motor (precentral gyrus) regions and extends to the supplementary motor areas (Ruan et al., Reference Ruan, Bludau, Palomero-Gallagher, Caspers, Mohlberg, Eickhoff, Seitz and Amunts2018). The SMN network undergoes earlier maturation and is the primary gradient pattern of brain network functional organization in childhood, which may facilitate detecting associations with adversity (Dong et al., Reference Dong, Margulies, Zuo and Holmes2021). More importantly, we found that SMN-LN hyperconnectivity was a neurobiological pathway linking abuse to concurrent somatic symptoms, depression, and anxiety symptoms six months later. These findings are consistent with emerging evidence positioning the SMN network as a transdiagnostic hub for psychopathology (Kebets et al., Reference Kebets, Holmes, Orban, Tang, Li, Sun, Kong, Poldrack and Yeo2019). In addition, previous research suggests that the SMN network contributes to shaping executive function and prefrontal cortex development (Rosen et al., Reference Rosen, Amso and McLaughlin2019; Rakesh, Zalesky, et al., Reference Rakesh, Zalesky and Whittle2021). The present results may suggest that during early adolescence, when the prefrontal cortex is still maturing, the more developed SMN network may be a key and alternative pathway linking childhood abuse to mental health outcomes through its connections with the LN network. Thus, the predominant focus on the FPN, DMN, and SN networks as core neurocognitive systems, while valuable, may limit our comprehension of how childhood adversity influences neurodevelopment. Future studies would benefit from examining the associations from a more holistic perspective.
Our results found no associations between neglect and brain network connectivity. Existing research has consistently found that neglect is associated with delayed brain structure maturation (Rakesh, Whittle, et al., Reference Rakesh, Whittle, Sheridan and McLaughlin2023). However, there are conflicting results regarding the brain function (Beck et al., Reference Beck, Whitmore, MacSweeney, Brieant, Karl, Lange, Westlye, Mills and Tamnes2024; Herzberg et al., Reference Herzberg, McKenzie, Hodel, Hunt, Mueller, Gunnar and Thomas2021). The participants in our study were rural children characterized by poverty and experiences of being left behind. The pervasive and chronic nature of neglect in this population may explain the discrepancies from previous studies on institutionalization or extreme physical neglect (Fellmeth et al., Reference Fellmeth, Rose-Clarke, Zhao, Busert, Zheng, Massazza, Sonmez, Eder, Blewitt, Lertgrai, Orcutt, Ricci, Mohamed-Ahmed, Burns, Knipe, Hargreaves, Hesketh, Opondo and Devakumar2018).
The study has several limitations. First, the cross-sectional design restricts our ability to draw directional or causal conclusions regarding the relationships among adversity, psychological resilience, and neuroimaging measures. To address this issue and to avoid imposing assumptions about causal directionality, we conducted additional exploratory analyses using the associational variable analysis (AVA) framework, which provides an alternative approach for interpreting associations in nonexperimental cross-sectional data (Weems, Reference Weems2025). These exploratory analyses were consistent with the main findings, suggesting that when psychological resilience was low, SMN-LN served as an associational variable in the relationship between childhood threat and depression as well as somatization (see Supplementary Materials). Future longitudinal research with larger and more diverse samples is essential to capture the long-term developmental trajectories of these associations. Second, employing retrospective self-report questionnaires to measure adversity exposure in children may induce recall bias (Danese & Widom, Reference Danese and Widom2020). Third, sexual abuse constitutes a distinct subtype of childhood adversity with potentially unique neurobiological correlates (Crum et al., Reference Crum, Flanagan, Vaughan, Aloi, Moran-Santa Maria, Back, Brady and Joseph2021), and its omission restricts the breadth of adversity assessed in the present study. Future studies should incorporate all subscales alongside more objective adversity records. Fourth, while our sample size is comparable to prior neuroimaging studies, the detection of small moderated mediation effects may still be limited. The lack of significant findings under a more stringent head-motion criterion of FD > 0.2 mm constitutes an additional limitation. Future studies should employ larger cohort samples and apply more rigorous motion-control methods to more robustly test the relationships.
In conclusion, this study advanced the understanding of how psychological resilience interacts with childhood adversity to influence brain network connectivity. The unique and specific role of psychological resilience was identified in mitigating the impact of adversity dimensions on brain functional connectivity, particularly between LN, VAN/SN, and SMN networks. This protective effect may influence both short- and long-term psychological and physical well-being. These findings provide guidance for developing interventions that promote well-being after adverse childhood experiences.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579426101564.
Data availability statement
The datasets are available from the corresponding author upon reasonable request.
Funding statement
This project was funded by the STI 2030-Major Projects 2021ZD0200500, National Natural Science Foundation of China (32471116), and National Natural Science Foundation of China (32130045).
Competing interests
The authors report no biomedical financial interests or potential conflicts of interest.
Pre-registration statement
This study was not pre-registered. Data collection for the present project began prior to the widespread adoption of pre-registration practices in this research area. The study hypotheses and analytical approach were theory-driven and informed by prior empirical work, and all analyses reported in the manuscript were conducted as described.




 Open access
Open access