


Anorexia of ageing (AA) is defined as a decline in appetite and caloric intake seen with increasing age (Morley, 1997)(Reference Morley1). Despite no single, universally accepted method to identify those with AA, a loss of appetite is thought to directly affect between one in five and one in two older adults. van der Meij et al.(Reference van der Meij, Wijnhoven and Lee2) reported 22% of community-dwelling older adults in the USA exhibited poor appetite, while Vazquez-Valdez and co-workers(Reference Vázquez-Valdez, Aguilar-Navarro and Ávila-Funes3) reported a 30% prevalence of low appetite amongst community-dwelling older adults in Mexico. Prevalence is higher among those in care settings(Reference Donini, Dominguez and Barbagallo4), further increasing to ∼45% of hospitalised older adults(Reference Cox, Morrison and Ibrahim5). A recent meta-analysis from Fernandez et al. (Reference Fernandez, Cipolli and Merchant6) pooled data from 36 studies and over 29 million over-60-year-olds from multiple settings, reporting a global AA prevalence of 23%.
AA gives rise to individual, societal, and economic consequences. Those with AA experience a reduced quality of life(Reference Di Francesco, Pellizzari and Corrà7,Reference Rasheed and Woods8) and increased risk of undernutrition, sarcopenia, and frailty(Reference Landi, Calvani and Tosato9). Low appetite and a resultant reduction in food intake results in insufficient intakes of certain nutrients and foods, such as protein, fibre, and fruits and vegetables(Reference van der Meij, Wijnhoven and Lee2), while both low protein and energy intake contribute to accelerated sarcopenia(Reference Landi, Liperoti and Russo10). Those with AA have an approximate two-fold increased risk of disability(Reference Vázquez-Valdez, Aguilar-Navarro and Ávila-Funes3,Reference Landi, Russo and Liperoti11) and are two-and-a-half times more likely to suffer with sarcopenia(Reference Landi, Liperoti and Russo10). Consequently, those with AA have an 83% higher risk of all-cause mortality(Reference Landi, Liperoti and Lattanzio12). As such, AA can be considered a precursor or ‘pathway’ to frailty and frailty-related outcomes(Reference Merchant, Woo and Morley13). The cost of AA and consequent frailty on healthcare services must also be acknowledged. Research suggests that undernourished adults require three times greater health and social costs compared with adequately nourished adults(Reference Russell and Elia14), while healthcare costs are four times higher for older adults with severe frailty, compared with their fit counterparts(Reference Fogg, England and Zhu15). Given the global ageing population and the current trajectory of an increase in those living with frailty(Reference Fogg, England and Daniels16), addressing AA – its causes and consequences – should be deemed a public health priority.
While the aetiology of AA remains to be fully elucidated, the phenomenon is almost certainly multifactorial. AA likely results from physiological, pathological, and social changes associated with ageing(Reference Wysokiński, Sobów and Kłoszewska17). A greater understanding of the causes of AA will help to develop effective treatment strategies, reducing both the social and economic burden. This review will briefly highlight current knowledge of the aetiology of AA, with a focus on the role of gut hormones.
Aetiology of anorexia of ageing
Appetite control is complex and multifactorial. Consequently, changes in appetite and eating behaviour in later life must be viewed through a multifaceted lens. The role of cognitive, emotional, societal, and environmental inputs and influences cannot be overlooked. For example, it has long been appreciated that widowhood can result in a reduction in energy intake, associated with reductions in mealtime enjoyment, loss of appetite, and loss of interest in food(Reference Rosenbloom and Whittington18). Relatedly, low mood is associated with poor appetite in later life(Reference Cox, Howson and Ibrahim19), with older adults suffering with depression more likely to lose weight(Reference DiPietro, Anda and Williamson20). Further, psychological factors and traits relating to resilience and mood – such as a determination not to ‘give up’ and to ‘be positive’ – have been identified as mediators of social and environmental determinants of eating behaviour(Reference Bloom, Lawrence and Barker21).
However, biological inputs are irrefutably consequential. This is perhaps best argued by highlighting the commonality of age-related weight loss and reductions in food intake across numerous species, from primates(Reference Tardif, Mansfield and Ratnam22) to rodents(Reference Blanton, Horwitz and Murtagh-Mark23), fish, birds, and invertebrates(Reference Christian and Benian24). Colman et al. (Reference Colman, McKiernan and Aiken25) observed mid-life onset of sarcopenia in rhesus macaques, with a muscle mass loss of 20% in later life. This coincides with evidence of declines in dietary intake in rhesus macaques with advancing age(Reference Mattison, Black and Huck26). This preserved trait suggests an evolutionary conservation, highlighting a strong genetic and biological drive for a reduction in appetite in later life.
Biological systems influence both hedonic and homeostatic processes of appetite control. Hedonic influences include palatable cues, particularly taste and smell, from foods that activate neural reward pathways(Reference Saper, Chou and Elmquist27). The taste, sight, and smell of food stimulate flavour centres in the brain which result in a reward value(Reference Rogers and Hardman28,Reference Rolls29) . Sensory function is known to diminish with ageing(Reference Brenowitz, Kaup and Lin30), and reductions in sense of smell and taste were indeed implicated in appetite loss (Reference Schiffman31,Reference Aschenbrenner, Hummel and Teszmer32) . However, it is now argued that chemosensory impairments are not related to reduced eating pleasure nor the risk of undernutrition(Reference Arganini and Sinesio33,Reference Tomić-Obrdalj, Palfi and Keser34) . Nonetheless, with large heterogeneity in sensory function in older adults and the impact this may have on eating behaviour(Reference Giles, Zannidi and Clegg35), taste, smell, and food texture are important considerations for understanding and addressing low appetite and undernutrition(Reference Giles, Zannidi and Clegg35).
Homeostatic control of appetite refers to mechanisms that match energy intake to energy requirements, alongside maintaining nutrient status. Involving both tonic and episodic inputs, homeostatic appetite regulation is controlled by metabolic, hormonal, and neuronal sensing and signalling from peripheral tissue to the central nervous system to influence eating behaviour(Reference Campos, Port and Acosta36–Reference Neary, Goldstone and Bloom38).
Tonic signals are enduring, with a stable influence over appetite and not fluctuating between or within days(Reference Hopkins, Kristine and Anna37). These signals convey information regarding energy availability, energy stores, and energy needs from body tissues and cellular metabolism to the brain(Reference Beaulieu, Hopkins and Blundell39). A comprehensive discussion of tonic homeostatic control of appetite and energy intake is beyond the scope of this piece; for such, readers are directed to some excellent reviews on this topic (Reference Blundell, Gibbons and Beaulieu40–Reference Hopkins, Gibbons and Blundell42). Briefly, resting metabolic rate (RMR)(Reference Caudwell, Finlayson and Gibbons43), activity energy expenditure(Reference Hopkins, Duarte and Beaulieu44) and total daily energy expenditure (TDEE)(Reference Piaggi, Thearle and Krakoff45) are all associated with energy intake, indicating energy requirement is a strong, tonic determinant of appetite and eating behaviour(Reference Blundell, Gibbons and Beaulieu40). However, the strength of such relationships in older adults is less well understood. Hopkins et al. (Reference Hopkins, Casanova and Finlayson46) showed that TDEE predicted energy intake in a cohort of 590 over 50-year-olds. Physical activity also predicted energy intake, but not when adjusting for TDEE(Reference Hopkins, Casanova and Finlayson46). In younger adults, a J-shaped relationship between physical activity and energy intake is largely accepted(Reference Beaulieu, Hopkins and Blundell39,Reference Mayer, Roy and Mitra47) , but this has yet to be determined in older adults and our research group has previously postulated a deviation from such a relationship in later life(Reference Crabtree, Cox and Lim48).
A relationship between TDEE and energy intake independent of physical activity could indicate that RMR is driving this association. RMR is primarily determined by fat-free mass(Reference Ravussin, Lillioja and Anderson49). Fat-free mass (FFM) is associated with daily energy intake in younger(Reference Blundell, Caudwell and Gibbons50,Reference Hopkins, Finlayson and Duarte51) and older adults(Reference Hopkins, Casanova and Finlayson46), with Hopkins and colleagues showing the mediating effect of RMR on this relationship(Reference Hopkins, Finlayson and Duarte51). In addition to the cross-sectional evidence of Hopkins et al. (Reference Hopkins, Casanova and Finlayson46), Johnson and co-workers(Reference Johnson, Holliday and Mistry52) induced a 1.2 kg increase in FFM in older adults through a 12-week resistance training programme, observing a subsequent and related increase in appetite and daily energy intake of 133 kcal. In contrast, FM appears not to be an independent predictor of energy intake, in younger (49, 50) nor older adults(Reference Hopkins, Casanova and Finlayson46). This is despite the anorexigenic action of the hormone leptin, which is released from adipose tissue proportional to adiposity, signalling energy storage to the brain and exerting influence on feeding(Reference Havel53). However, the influence of leptin on eating behaviour appears particularly potent during periods of energy deficit and is less effective at limiting energy surplus and weight gain with overfeeding(Reference Ravussin, Edwin and Gallop54). In addition, with high levels of adiposity, the negative feedback action of leptin in the brain appears blunted(Reference Morton, Cummings and Baskin55,Reference Schwartz, Woods and Porte56) . Nonetheless, leptin concentration has been shown to be higher in older adults(Reference Johnson, Shannon and Matu57), which may contribute to AA.
The gut, gut hormones and appetite control
The sensing of acute fluctuations in energy and nutrient status provides episodic signals to influence appetite. Much of this sensing occurs in the gut in response to feeding, and this is one potential physiological site where appetite control inputs may differ in later life. The role of the gut, and specifically gut-derived hormones, in appetite has been reviewed comprehensively elsewhere(Reference Gribble and Reimann58–Reference Holliday, Horner and Johnson60). In brief, the secretion of hormones from the gastrointestinal tract communicates acute nutrient status to other organs of the body. Following food ingestion, nutrients are sensed in the gut by enteroendocrine cells, releasing gut-derived hormones, such as GLP-1, PYY and CCK(Reference Gribble and Reimann58). These hormones act via the circulation, vagus nerve, and brain stem, stimulating anorexigenic pathways found primarily in the arcuate nucleus of the hypothalamus. As such, they signal an inhibitory feedback loop that terminates feeding and prevents or delays the reoccurrence of food ingestion. Conversely, the hunger hormone ghrelin is secreted during periods of abstinence from feeding. Surging before food ingestion and signalling via the circulation and vagus nerve to stimulate orexigenic pathways in the arcuate nucleus of the hypothalamus, it is thought to act as a ‘trigger’ for ingestive behaviour. With food ingestion, ghrelin secretion is suppressed, reducing hunger and favouring satiation and satiety. In such a manner, this endocrine communication relays gastrointestinal nutrient status to the brain, providing episodic signals that align with food intake throughout a day.
Gut hormone responses to feeding in older adults
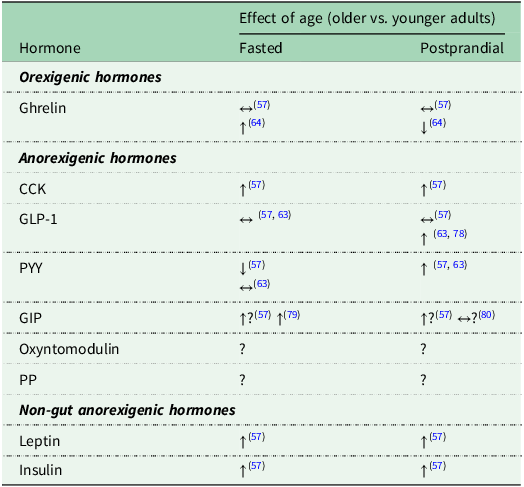
There is now compelling evidence that gut hormones respond differently to food ingestion in later life, especially in those exhibiting AA. A comprehensive meta-analysis by Johnson et al.(Reference Johnson, Shannon and Matu57), showed circulating concentrations of some appetite-related hormones differ between younger and older adults. Older individuals demonstrated elevated fasting and postprandial concentrations of CCK, along with a tendency towards increased PYY secretion. However, CCK data should be interpreted with caution. Cross-reactivity with the structurally-similar and much more abundant gastrin renders the validity of some assays questionable(Reference Rehfeld, Feinle-Bisset and Rehfeld61). Few studies have directly compared ghrelin concentrations between older and younger adults; while meta-analysis showed no significant age-related differences, it was deemed that more evidence was needed(Reference Johnson, Shannon and Matu57). Non-significant elevated GIP concentrations were observed in older adults, in both fasted and postprandial states; but these findings were derived for just four studies. No significant age-related differences were identified for GLP-1, but again, data were limited (7 studies) and of high heterogeneity. This evidence base has since been expanded, with Giezenaar et al.(Reference Giezenaar, Lange and Hausken62) demonstrating greater postprandial increases in GLP-1 concentration in older versus younger men after the consumption of drinks of varying energy and macronutrient content. Table 1 summarises age-related differences in gut hormones in the fasted and postprandial states.
Summary of age-related differences in circulating gut hormones. (Adapted from Dagbasi et al. 2024)

↔ no difference between older vs. younger adults; ↑ greater concentration in older vs. younger adults; ↓ lower concentration in older vs. younger adults; ? unclear effect of age. CCK, cholecystokinin; GLP-1, glucagon-like peptide 1; PYY, peptide tyrosine-tyrosine; GIP, glucose-dependent insulinotropic polypeptide; PP, pancreatic polypeptide.
However, earlier studies may have overlooked key nuances due to their design. Specifically, grouping all older adults together without accounting for appetite status may obscure important differences in gut hormone profiles. Given that approximately 30% of community-dwelling older adults experience AA, it is likely that study samples include individuals with both preserved and diminished appetite. This may mask any dysregulation in gut hormone metabolism that is exclusively seen in those exhibiting altered appetite control. Additionally, due to difficulty in recruiting those with low appetite, in part because of health-related barriers, many studies may have inadvertently underrepresented those with low appetite. These limitations have likely contributed to an incomplete understanding of how ageing influences gut hormone responses.
This issue was recently addressed by comparing gut hormone responses among younger adults, older adults with preserved appetite, and older adults identified as having low appetite(Reference Dagbasi, Warner and Catterall63,Reference Holliday, Warner and Hulston64) . Using a novel four-criteria ‘phenotyping’ method, older adults were considered to be exhibiting low appetite if they met two of the following: low-weight (BMI < 23 kg⋅m−2(Reference Crabtree, Cox and Lim48,Reference Winter, MacInnis and Wattanapenpaiboon65) , a score of <15 on the Simplified Nutritional Appetite Questionnaire(Reference Lau, Pek and Chew66), habitual energy intake <75% of estimated daily total energy requirements (TER;(Reference Cederholm, Jensen and Correia67)); a laboratory-measured ad libitum lunch intake of <25% of estimated TER (based on a typical lunch energy intake of ∼27% of total energy intake in UK adults(Reference Pot, Hardy and Stephen68)).
Circulating concentrations of ghrelin (total), PYY, and GLP-1 were measured in the fasted state and in response to a 450 kcal, nutrient-balanced porridge meal(Reference Dagbasi, Warner and Catterall63). Blood samples, along with measures of subjective appetite, were taken before eating and at regular intervals for four hours after the meal. An ad libitum pasta-based lunch meal was then provided. Comparisons were made between younger adults and all older adults, and between younger adults, older adults with a ‘healthy’ appetite, and older adults exhibiting low appetite. This design enabled distinction between differences that appear to be a function of ageing per se, and differences that appear unique to older adults with low appetite.
Data revealed no difference in ghrelin response between older adults and younger adults(Reference Dagbasi, Warner and Catterall63). However, when comparing younger adults, older adults with a healthy appetite, and those exhibiting low appetite, ghrelin was suppressed to a markedly and significantly greater extent in older adults exhibiting low appetite than in younger adults. This was not seen in older adults with a healthy appetite, who showed an almost identical ghrelin profile to younger adults. Similarly, no differences were observed in PYY response between all older adults and younger adults; but there was a marked trend towards a greater response in older adults exhibiting low appetite, compared with younger adults and older adults with a healthy appetite. There was a difference observed in GLP-1 response between all older adults and younger adults, with younger adults experiencing a more rapid elevation in plasma concentrations, while older adults had a delayed but prolonged elevation. However, when comparing the response of younger adults with older adults with a healthy appetite and older adults exhibiting low appetite, this apparent age-related difference was exclusive to those exhibiting low appetite. No difference was observed between young adults and older adults with a healthy appetite(Reference Dagbasi, Warner and Catterall63).
It is unlikely that any single appetitive gut hormone uniquely drives appetite control, and indeed, numerous hormones all change with a degree of synergy in response to feeding. So, while measuring individual hormone responses is common in this field, it is likely to be the gut hormone profile and interplay between hormones that exert appetite control. In appreciation of this, Dagbasi and co-workers(Reference Dagbasi, Warner and Catterall63) calculated an ‘anorexigenic response score’, as a composite of the responses of ghrelin, PYY, and GLP-1. Anorexigenic response score – expressed as net area-under-the-curve for the postprandial period – did not differ between younger and older adults. However, the score was significantly greater for older adults exhibiting low appetite compared with both younger adults and older adults with a healthy appetite. From these data, we concluded that older adults exhibiting low appetite have augmented gut hormone responses to feeding and this may be a causal mechanism of AA(Reference Dagbasi, Warner and Catterall63).
These data appear to vindicate the approach of identifying older adults who exhibit appetite suppression. Simply comparing older adults with younger adults would have failed to observe differences in ghrelin and PYY that appear unique to those exhibiting low appetite(Reference Dagbasi, Warner and Catterall63). Conversely, findings would have erroneously identified differences in GLP-1 response between younger adults and older adults, when in fact, the data of this study would suggest this is not an effect of ageing per se, but unique to those exhibiting low appetite. This would have resulted in misplaced conclusions regarding gut hormone responses in later life and the likely role of appetitive gut hormones in the aetiology of AA.
Of note, 54% of older adults classified using the phenotyping model were identified as exhibiting low appetite(Reference Dagbasi, Warner and Catterall63). This is substantially higher than prevalence statistics for AA in community-dwelling older adults of ∼ 15–30%(Reference van der Meij, Wijnhoven and Lee2,Reference Vázquez-Valdez, Aguilar-Navarro and Ávila-Funes3,Reference Cox, Morrison and Ibrahim5) . This could indicate the underreporting of mild anorexia in later life, suggesting more older adults than is currently acknowledged may be experiencing low appetite. The observation of gut hormone dysregulation in those who may have ‘mild’ anorexia indicate a benefit of earlier detection to enable intervention prior to more severe anorexia and consequent undernutrition.
Dagbasi and co-workers(Reference Dagbasi, Warner and Catterall63) interrogated the novel phenotyping model to assess appropriateness and utility for future research in this field. Using the anorexigenic response score as the outcome of interest, regression analysis determined the efficacy of the model for identifying those exhibiting low appetite(Reference Dagbasi, Warner and Catterall63). The phenotyping model explained 48% of the variance in anorexigenic response score(Reference Dagbasi, Warner and Catterall63). Interestingly, stepwise regression showed that the model with the strongest predictive power included SNAQ score, habitual dietary intake, and laboratory ad libitum energy intake, with BMI not adding to the strength of the model. This is perhaps less surprising than one might initially think, given that BMI is not associated with protein-energy undernutrition(Reference van der Pols-Vijlbrief, Wijnhoven and Schaap69), and risk of undernutrition is prevalent in ∼25% of older adults with a BMI > 25 kg/m−2(Reference Sulmont-Rossé, Van Wymelbeke-Delannoy and Maître70). In addition, BMI is a poor predictor of mortality in older people, likely due to the crudity of the measure in its inability to discern body composition(Reference Chang, Beason and Hunleth71). Refinement of the model could include the use of lean mass as an alternative to BMI, to account for the composition of body mass. This phenotyping approach appears to be a robust method, and could prove beneficial for implementation in research in this field. Future research should look to confirm this by monitoring changes in dietary intake and body composition over time in those phenotyped as exhibiting low appetite and those phenotyped as having a ‘healthy’ appetite. If acting as an effective method for identifying early risk of AA, it could be hypothesised that those phenotyped as exhibiting low appetite will be at greater risk of developing undernutrition and experiencing unwanted weight loss and muscle loss.
Only part of the puzzle
Based on these observations, it can be proposed that a dysregulation of the gut hormone responses to feeding is a mechanism of AA, but not the mechanism. As previously mentioned, AA is multifactorial and it is likely that those experiencing AA will do so because of multiple and differing mechanisms, which may work synergistically or in isolation. Indeed, even the nature and manifestation of AA itself are not uniform. In qualitative research exploring AA, older individuals use discrete narratives of the experience that can be broadly outlined as increased or early feelings of satiety, or a general disinterest in food(Reference Cox, Morrison and Robinson72). These narratives are not always consistent with perceptions of what appetite is or should be to the individual, whether a predominantly pleasure-seeking experience driving a desire to eat or a sensation that reflects underlying homeostatic mechanisms controlling energy intake and requirements. This inconsistency is interesting and may suggest that fundamental changes to biological mechanisms are a primary driver of AA rather than behavioural factors. Instead, eating behaviour may be more influential in the way older people adapt (or maladapt) to AA and thus upon consequent health trajectories(Reference Cox, Morrison and Robinson72).
The presence of discrete AA manifestations, which potentially have differing underlying mechanisms, is important to consider when designing further investigation. Certainly, gut hormone dysregulation would align with feelings of increased satiety described by some older adults, which is important, yet we acknowledge it does not explain the full spectrum of the phenomenon. Other biological mechanisms for AA, such as the potentially appetite-suppressive effects of age-related inflammation(Reference Sánchez-Sánchez, Guyonnet and Lucas73,Reference Pourhassan, Babel and Sieske74) , alongside impaired sensory function with ageing, indicate a broad spectrum of potential underpinning elements. Thus, gut hormone dysregulation should currently be considered a key part of the wider puzzle that is AA as it is currently defined.
What next for research in this space?
Recent findings of amplified gut hormone responses to feeding in those older adults with low appetite has advanced our understanding but also raised several interesting questions to address. Firstly, such responses were observed for GLP-1, PYY and ghrelin. However, there are numerous other gut-derived hormones which exert appetitive effects, such as cholecystokinin (CCK), oxyntomodulin, pancreatic polypeptide (PP), and glucose-dependent insulinotropic polypeptide (GIP). Identifying responses of these hormones to feeding in older adults with low appetite would provide a thorough profile of the appetitive gut hormones.
Enhanced gut hormone responses to food intake may reflect an increased sensitivity of the gut to nutrients in some older individuals. This heightened responsiveness could contribute to disrupted hormone regulation and diminished appetite, potentially due to the gut overreacting to nutritional stimuli. This theory has been posed and discussed in detail elsewhere(Reference Dagbasi, Fuller and Hanyaloglu75). In brief, research is needed to enhance our understanding of any changes in nutrient transit, sensing, digestion, and absorption – as well as changes in gut function and physiology – in older adults with AA(Reference Dagbasi, Fuller and Hanyaloglu75). A first step may be to determine if the observed augmented gut hormone response is common to all nutrients or is nutrient-specific. The test meals of Dagbsi et al.(Reference Dagbasi, Warner and Catterall63) and Holliday et al.(Reference Holliday, Warner and Hulston64) were a mixed-nutrient meals; it may be of interest to explore gut hormone responses to carbohydrate, fat and protein specifically in older adults exhibiting low appetite. Once it is identified whether any amplified gut hormone response is common to all nutrients or is nutrient-specific, specific, targeted nutrient sensing and signalling pathways can be explored.
The findings of augmented gut hormone responses to feeding in older adults exhibiting low appetite are limited to cross-sectional observation. Consequently, it could be argued that these altered gut hormone responses may be a consequence of low appetite or weight loss, rather than a cause. It was demonstrated that BMI was not a predictor of anorexigenic response score – a composite of GLP-1, PYY, and ghrelin responses – which would indicate that low BMI, at least, is not driving dysregulated hormone responses(Reference Dagbasi, Warner and Catterall63). Those with a high BMI were not included, and hence it cannot be determined that a relationship between BMI and gut hormone response is not present in older adults at higher BMI values. Given that dysregulated or differing hormone responses are observed with excess adiposity in younger adults (e.g., in PYY(Reference Batterham, Cohen and Ellis76), and in ghrelin(Reference Shiiya, Nakazato and Mizuta77)), this may also be prevalent in later life. Nonetheless, longitudinal observation is needed to confirm the direction of the relationship between low appetite and amplified gut hormone responses.
In conclusion, contemporary evidence indicates that amplified gut hormone responses to feeding is observed in older adults with low appetite, but may not be present in those with a ‘healthy’, unaffected appetite. As such, gut hormone dysregulation appears not simply a function of ageing, but may be a fundamental driver of AA. Further research is needed to substantiate this, both in terms of direction of causality and the deeper underpinning mechanisms for a hypersecretory response to nutrient ingestion. However, it must be appreciated that broader evidence of the characteristics of AA indicate strong influence of social factors, sensory decline, and biological systems other than gut hormones. This supports the notion of different mechanisms, aetiology, and manifestations of AA, which aligns with the multifactorial complexity of appetite control. The potential for different ‘types’ of AA needs further consideration, as it will influence not only our understanding of the underlying mechanisms, but also the identification of at-risk populations and associated risk factors, and future treatment strategies.
Acknowledgements
The authors would like to acknowledge co-authors of previous work integral to the content of this review. Specifically, we would like to thank Aygul Dagbasi and Jordan Warner.
Author contributions
AH conceived the idea for the review. AH, MB, and NJC wrote the manuscript. All authors have read and approved the final version of the manuscript.
Financial support
No external funding was received for the conductance of this research. Matthew Barrett is the recipient of a Newcastle University Faculty of Medical Sciences PhD Studentship Award.
Competing interests
The authors declare no conflicts of interest.
Ethical statement
Ethical approval was not required for this review.

 Open access
Open access