


The cost of mental health problems in England has been estimated to exceed £100 billion. Reference McDaid, Park, Davidson, John, Knifton and McDaid1 It is suggested that much of this cost could be mitigated by investments in early prevention interventions – notably, initiatives during key developmental stages of childhood and early adolescence. Schools have been identified as a universal point of access for young people in key developmental stages, which makes them effective platforms for early prevention and mental health promotion. Reference Lee, Barendregt, Stockings, Ferrari, Whiteford and Patton2 Previous studies have found some evidence for the effectiveness of school-based programmes in promoting mental health; Reference Kuyken, Ball, Crane, Ganguli, Jones and Montero-Marin3 however, it has also been noted that such interventions have not been investigated in the UK to the same extent as in other countries, such as the USA. Reference Mackenzie and Williams4 Further, evidence on the cost-effectiveness of such interventions is limited, with few trials including an economic component in the analyses. A review in 2020 Reference Schmidt, Werbrouck, Verhaeghe, Putman, Simoens and Annemans5 found only nine studies (since 2013) of universal mental health interventions for children and adolescents that included an economic evaluation – only three of which took place in the UK. The review highlighted a number of challenges in addressing the cost-effectiveness of interventions, including the lack of cost-related information available. With consideration for the increasing demands on health and social care resources, it is important that cost-effectiveness forms part of the decision-making process with regard to intervention recommendations.
Study objectives
This study aims to evaluate the cost-effectiveness of two school-based interventions, funded by the Department for Education, designed to improve mental health literacy and emotional well-being in year 9 students in England: (a) the Youth Aware of Mental Health (YAM) programme, a universal intervention to improve awareness and promote mental health; Reference Wasserman, Hoven, Wasserman, Wall, Eisenberg and Hadlaczky6 and (b) the Mental Health and High School Curriculum Guide (The Guide), Reference Kutcher, Wei and Morgan7 which aims to increase awareness of mental disorders and their treatments, as well as increasing understanding of how to achieve and maintain mental health, reduce stigma and improve help-seeking efficacy. A description of these programmes are available from the Department for Education. Reference Deighton, Thompson, Humphrey, Thornton, Knowles and Patalay8
The key objectives of this evaluation are: (a) to assess the cost-effectiveness of each of these interventions against usual school provision in terms of improving students’ health-related quality-of-life (HRQoL), as measured by quality-adjusted life-years (QALYs); (b) to assess the cost-effectiveness of YAM relative to usual school provision, with respect to changes in depressive symptoms; and (c) to assess the cost-effectiveness of The Guide relative to usual school provision, with respect to changes in help-seeking behaviour.
Method
This health economic analysis was conducted alongside a three-arm, parallel-group, cluster randomised controlled trial (trial registration number: ISRCTN17631228) designed to evaluate the cost-effectiveness of the YAM programme, The Guide, and usual school provision for year 9 students in England. Recruitment took place between March 2018 and July 2019. Data were collected at three time points: at baseline, at 3–6 months after the start of the intervention and at 9–12 months following the end of intervention (as detailed in the pre-registered statistical analysis plan Reference Boehnke, Deighton, Evans-Lacko, Hayes, Humphrey and Patalay9 ). All questionnaires were completed online.
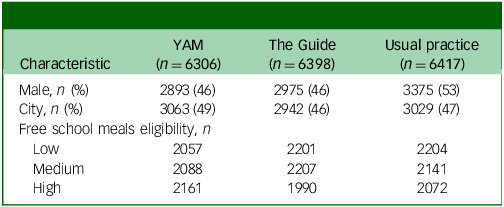
The target population was year 9 students (aged 13–14 years) from 144 secondary schools in England, totalling approximately 8600 participants. Parents/guardians of the pupils in these classes were sent letters informing them of the study. For outcome (effectiveness) data, opt-out consent was used when sending letters to parents/guardians of pupils who were selected by schools to take part. Parents/carers who wished to opt out their children were asked to return an opt-out form to the research team. Pupils whose parents had not opted out of the evaluation were given the option to assent to take part through reading an online information sheet and ticking an online assent form. Any young people that did not provide assent at the baseline survey did not take part in the trial. Data were collected via self-reported questionnaires from participants (staff and students). Financial information relating to intervention delivery, including training, were collected using financial surveys completed by school staff. Participant characteristics are presented in Table 1.
Participant characteristics at baseline (N = 19 121)

YAM, Youth Aware of Mental Health programme; The Guide, Mental Health and High School Curriculum Guide.
Details of the study are reported in Deighton et al. Reference Deighton, Hayes, Thompson, March, Thornton and Santos10 A full description of the trial design is presented in the trial protocol, Reference Hayes, Moore, Stapley, Humphrey, Mansfield and Santos11 and the analyses plan was registered on Open Science Framework. Reference Boehnke, Deighton, Evans-Lacko, Hayes, Humphrey and Patalay9 Health economic analysis was conducted in line the Consolidated Health Economic Evaluation Reporting Standards reporting guideline. Reference Husereau, Drummond, Petrou, Carswell, Moher and Greenberg12 The analysis was conducted from a public health and social care perspective, including the costs of service use and intervention delivery.
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human participants were approved by the University College London Research Ethics Committee (approval numbers 6735/009 and 6735/014).
Outcome measures
In addition to the primary outcomes reported in the main analysis – the Short Mood and Feelings Questionnaire for YAM, Reference Angold, Costello, Messer, Pickles, Winder and Silver13 and the General Help-Seeking Questionnaire for The Guide, Reference Wilson, Deane, Ciarrochi and Rickwood14 – this health economic analysis analysed the self-reported quality-of-life scores, using the Child Health Utility 9D (CHU9D) Index. QALYs were calculated using preference weights estimated by Stevens. Reference Stevens15 One QALY represents a year at full health. All models were adjusted for baseline costs and outcome measures. All instruments used have been validated for the age group in this study. Covariate measures included socioeconomic status, measured using level (low, medium, high) of free school meal eligibility in each participating school; school location and setting (rural versus urban), and any previous implementation of universal mental health programmes before involvement in this trial.
Costs
Service use costs
Service use data were collected using a short form of the Client Service Receipt Inventory (CSRI), Reference Beecham16 which were completed by students at baseline and at each of the two follow-ups. The CSRI collected information on the use of school, health (including hospital) and social services by students because of concerns about their thoughts, feelings or behaviour. To better facilitate recall, the questions were framed in terms of frequency since ‘the beginning of the school year’, with a multiple-choice style response. For example, the student would be asked ‘Since the beginning of the school year, have you seen [a teacher] because of worries about your thoughts, feelings or behaviour?’, with the options of responding ‘once per day’, ‘once per week’, and so on. See the Technical Report 17 for the full questionnaire. Given that both follow-up surveys were conducted over a period of 3 months, the amount of time that passed between the ‘start of the school year’ and the follow-up was not a set length of time. To ensure consistency between student responses, and allow comparability between pre- and post-intervention periods, these frequencies were converted to annual estimates.
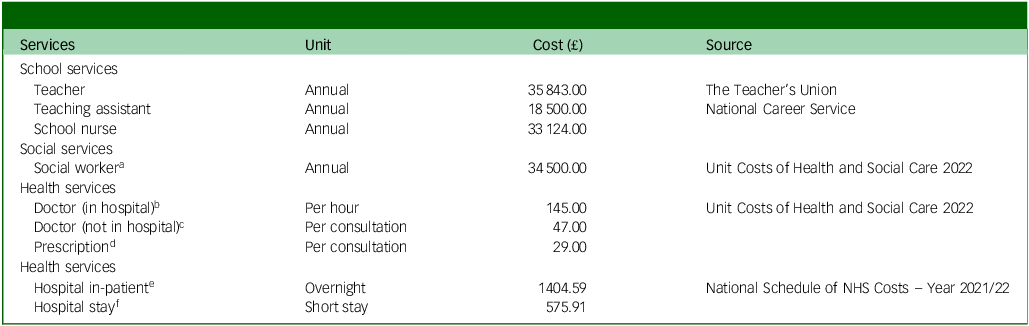
Cost of service use was calculated by combining service use with relevant unit costs. Unit costs were sourced from the latest version of publicly available publications, primarily from NHS Reference Costs, 18 and the Unit Costs of Health and Social Care. Reference Jones, Weatherly, Birch, Castelli, Chalkley and Dargan19 Further information on hourly rates for school staff and social workers were obtained from The Teacher’s Union and the Office of National Statistics. See Table 2 for details. Although the CSRI included a question on the use of prescription medication, information on specific type or duration of prescribed medications was not collected in the interest of privacy. Students instead were asked to indicate whether they have been prescribed medication to address emotional concerns during the study period. Where students reported the affirmative, we include a one-off cost of issuing the prescription.
Service unit costs

NHS, National Health Service.
a. Social worker (adult services), cost per working hour (including qualifications).
b. Consultant psychiatric, cost per working hour (including qualifications).
c. General practitioner, including direct care staff costs (with qualification costs), 9.22 min average per consultation.
d. Prescription costs per consultation, general practitioner (actual cost).
e. Child and Adolescent Mental Health Services, admitted patients.
f. Other mental health disorders, treated by a non-specialist mental health service provider.
Intervention costs
The cost of the interventions includes training costs for teachers (where relevant), and delivery costs:
-
(a) Training costs consist of costs of instructors – including travel and accommodation where applicable – and training materials such as posters, booklets and associated postage costs. These data were collected directly from the intervention team.
-
(b) Data on delivery costs were collected from schools, which reported the amount of time teachers spent on training, preparation and delivery of interventions. It also includes any extra time teachers spent with students as a direct result of the intervention. The teacher’s hourly rates were based on information provided in the finance surveys.
Given the different models for YAM and The Guide, different cost items apply to each intervention. Full details on cost items are included in Table 3. It is assumed that cost per student in the usual school provision group is zero.
Cost items of interventions

YAM, Youth Aware of Mental Health programme; The Guide, Mental Health and High School Curriculum Guide.
Cost-effectiveness analysis
The key research question for this analysis asks whether YAM and The Guide are cost-effective, compared with usual school provision, in terms of HRQoL, at 3–6 months after the start of intervention and at 9–12 months following the end of the intervention. Cost-effectiveness was measured using the incremental cost-effectiveness ratio (ICER), and assessed relative to thresholds typically used by the National Institute for Health and Care Excellence (NICE), which range from £20 000 to £30 000 per QALY gained. Interventions with an ICER below this range are generally considered to be cost-effective.
Cost-effectiveness was conducted from a public health and social care perspective, whereby the costs relating to health and social services, plus school services, were included. Societal costs – such as those resulting from reduced productivity (e.g. parents taking time away from work) – were not included in our analyses because of an absence of data. We also carried out a sensitivity analyses using a public health perspective, in which only costs incurred through use of public health services were included; costs of social services (including those relating to school services) are excluded.
Statistical analysis
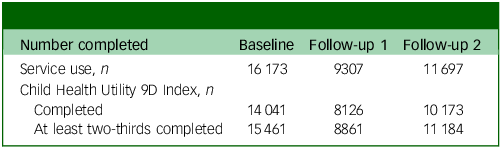
Students that provided responses to HRQoL and CSRI items at baseline and at at least one point of follow-up were included in the analyses. Outcomes relating to HRQoL were estimated with responses to the CHU9D questionnaire. For a QALY score to be calculated, all nine items on the questionnaire must be completed. Missing data – which were assumed to be missing at random – were imputed for responses that completed at least two-thirds of the items. The imputation method is detailed in Deighton et al. Reference Deighton, Hayes, Thompson, March, Thornton and Santos10 Responses with more than a third of items unavailable were excluded from analyses. A sensitivity analysis was conducted using only responses with complete CHU9D answers.
Differences in costs and outcomes between groups (each intervention against control) was first tested using standard parametric tests. The effect of the intervention on costs and effects were assessed using mixed-effects linear regression models to account for school-level clustering. In addition to the covariates specified in the analysis plan – baseline costs and outcomes, socioeconomic status – we also included the school location and setting, existence of prior interventions and gender as part of the model.
Cost-effectiveness was assessed with the ICER – calculated as the ratio of differences in costs and difference in outcomes. A net-benefit approach was employed, with net benefit calculated as:
 $NB = \lambda \left( {{E_I} - {E_{UP}}} \right) - \left( {{C_I} - {C_{UP}}} \right)$
$NB = \lambda \left( {{E_I} - {E_{UP}}} \right) - \left( {{C_I} - {C_{UP}}} \right)$
where NB is net benefit and λ is willingness to pay (WTP) for one unit of improvement in outcomes (e.g. one QALY). EI and EUP are the effects of the intervention group and the usual practice group, respectively. CI and CUP are the costs of the intervention group and the usual practice group, respectively. WTP values of £20 000 and £30 000 per QALY gained were considered, in line with the NICE guidelines. Reference McCabe, Claxton and Culyer20 Cost-effectiveness acceptability curves were constructed using non-parametric bootstrapping to address uncertainty.
All analyses were run with Stata (version 18 for Windows 10; StataCorp LLC, Texas, USA; https://www.stata.com/).
Sensitivity analysis
In addition to the complete case analysis, we examined the cost-effectiveness of the interventions from a public health perspective – that is, only costs directly incurred by the public health sector were included – to explore the potential effect of practices in one sector (here, education) on another (health).
Results
A total of 19 121 year 9 students provided responses for questionnaires at the baseline – 6306 for YAM, 6398 for The Guide and 6417 for usual school provision. At baseline, complete service use data was available for 16 173 students. At the first follow-up, this data was available for 9307 students. For outcome measures, 14 041 students completed the CHU9D at baseline, 8126 students at first follow-up and 10 173 at second follow-up. See Table 4 for data completeness.
Data completeness (N = 19 121)

Costs
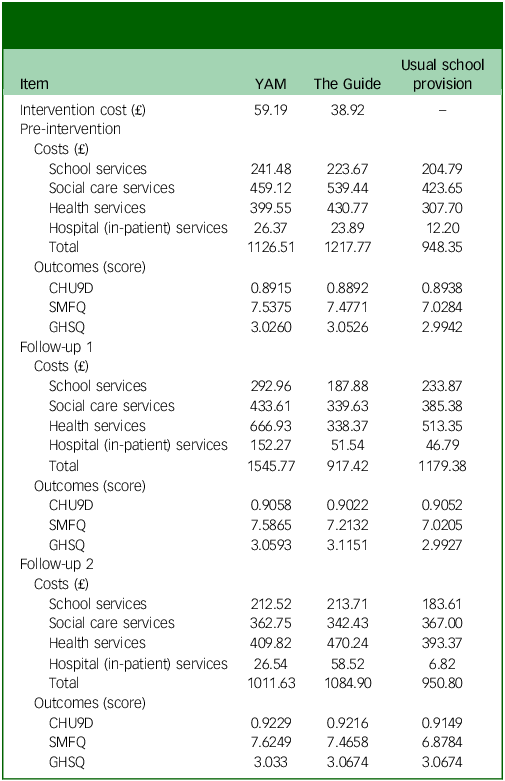
All costs are reported in 2021–2022 values. Total intervention delivery costs for YAM were estimated to be £238 408, with the per student cost at £59. Total cost for The Guide was estimated to be £155 582, which comes to approximately £39 per student. At baseline, health and social care costs were highest for students in schools randomised to The Guide (£1218 for the year before the intervention), and lowest for the usual school provision group (£948). At the first follow-up, the group with the greatest change in service use costs was YAM, with an average increase of £419 per student. This shift is largely attributed to the change in the use of health services, which increased by an average of £318 per student. At the second follow-up, incremental costs for The Guide, relative to usual school provision, was larger than that in the first follow-up, whereas incremental costs for YAM, relative to usual school provision, was smaller than that for the first follow-up. Detailed cost estimates are provided in Table 5.
Summary of student intervention costs, service use costs by sectors, and student outcomes

YAM, Youth Aware of Mental Health programme; The Guide, Mental Health and High School Curriculum Guide; CHU9D, Child Health Utility 9D Index; SMFQ, Short Mood and Feelings Questionnaire; GHSQ, General Help-Seeking Questionnaire.
Outcomes
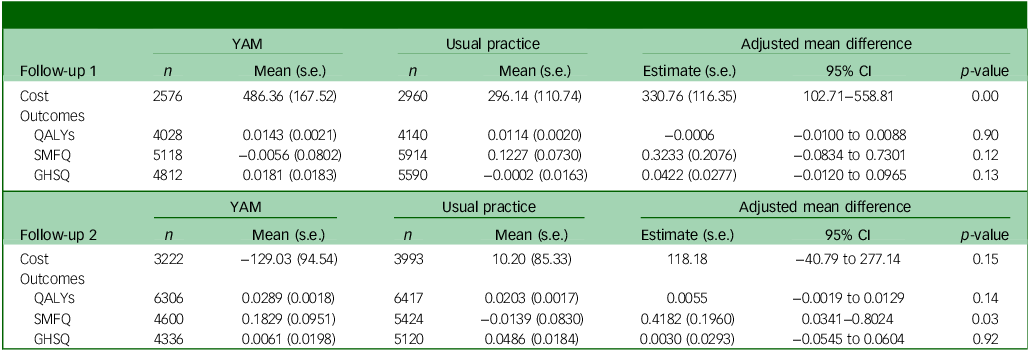
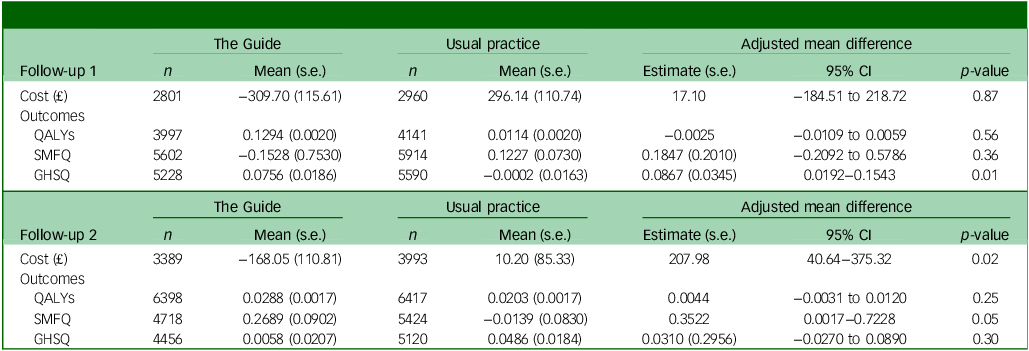
At the first follow-up, compared with students in schools randomised to usual school provision, students in schools randomised to The Guide experienced lower QALYs; however, the difference in average QALYs between the two groups was extremely small and not statistically significant. Students in schools randomised to YAM experienced similar outcomes, compared with those in schools randomised to usual school provision. Detailed results for primary outcomes for depressive symptoms and help-seeking behaviour are reported in Deighton et al. Reference Deighton, Hayes, Thompson, March, Thornton and Santos10 A summary of these results is presented in Tables 6 and 7. At second follow-up, students in schools randomised to either intervention group experienced an improvement in HRQoL outcomes, relative to those in usual school provision. Results of the cost-effectiveness analysis is presented in Table 8 and discussed below.
Changes in student costs and outcomes (YAM)

YAM, Youth Aware of Mental Health programme; QALY, quality-adjusted life-years; SMFQ, Short Mood and Feelings Questionnaire; GHSQ, General Help-Seeking Questionnaire.
Changes in student costs and outcomes (The Guide)

The Guide, Mental Health and High School Curriculum Guide; QALY, quality-adjusted life-years; SMFQ, Short Mood and Feelings Questionnaire; GHSQ, General Help-Seeking Questionnaire.
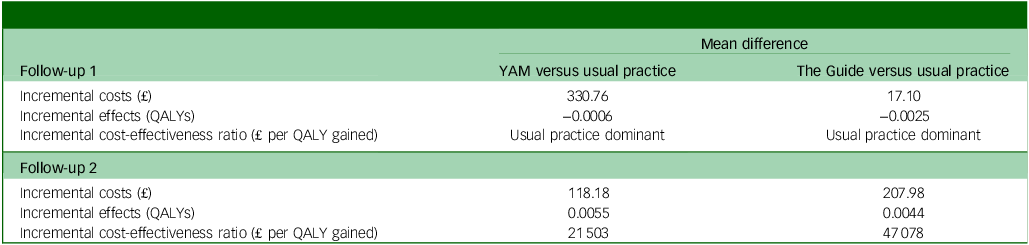
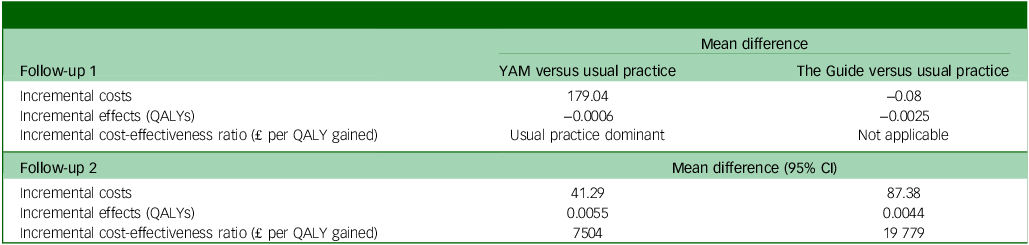
Cost-effectiveness of interventions, public health and social care perspective (with imputed Child Health Utility 9D Index data)

YAM, Youth Aware of Mental Health programme; The Guide, Mental Health and High School Curriculum Guide; QALY, quality-adjusted life-years.
Cost-effectiveness
Results from the first follow-up suggests that, relative to the students at schools randomised to usual school provision, those who attended sessions of YAM and The Guide experienced poorer outcomes in terms of QALY. However, it should be noted these differences are only marginal (−0.0006 QALYs and −0.0025 QALYs, respectively). Costs for both intervention arms were higher than that for usual school provision. Based on the cost-effectiveness thresholds set by the NICE of between £20 000 and £30 000 per QALY gained, neither intervention would be considered cost-effective. Results from bootstrapping indicate that at the £30 000 WTP threshold, YAM has a 4% probability of being considered cost-effective; for The Guide, this is 31%.
Results at the second follow-up show that, relative to students at schools randomised to usual school provision, students in schools randomised to YAM and The Guide experienced marginally higher HRQoL outcomes (0.0055 QALYs and 0.0044 QALYs, respectively). Costs for both intervention arms were still higher than that for usual school provision. For YAM, using results at second follow-up gives an ICER of £21 503 per QALY gained. For The Guide, the ICER at second follow-up was £47 078.
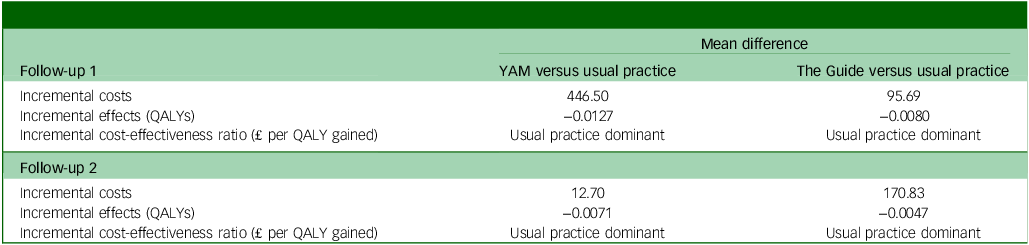
Results from the two sensitivity analyses are presented in Tables 9 and 10. We note that in the case of a strictly public health perspective, both interventions are potentially considered cost-effective at second follow-up. However, as this does not take into account costs incurred in school or social services, this is likely an underestimate of the overall costs. In all other scenarios, the interventions are not considered to be cost-effective.
Cost-effectiveness of interventions, public and social care perspective (with complete Child Health Utility 9D Index responses)

YAM, Youth Aware of Mental Health programme; The Guide, Mental Health and High School Curriculum Guide; QALY, quality-adjusted life-years.
Cost-effectiveness of interventions, public health perspective (with imputed Child Health Utility 9D Index data)

YAM, Youth Aware of Mental Health programme; The Guide, Mental Health and High School Curriculum Guide; QALY, quality-adjusted life-years.
Discussion
This study contributes to the body of literature in terms of the health economic analysis of universal school-based interventions in addressing student emotional health and well-being. Our analysis found that neither the YAM programme nor The Guide demonstrated cost-effectiveness at the first follow-up, with marginal differences in both costs and outcomes compared with usual practice. At the second follow-up, the YAM intervention showed a higher probability of being cost-effective relative to usual practice, although this was based on small improvements in outcomes. These findings are consistent with previous research, which has similarly highlighted the challenges of demonstrating the economic value of universal mental health interventions in schools. Reference Schmidt, Werbrouck, Verhaeghe, Putman, Simoens and Annemans5 Although school-based approaches may have potential, our results suggest that the benefits of such interventions may be more pronounced in the medium to long term, with mechanisms such as increased mental health literacy and peer support networks contributing to cost-savings.
This is one of the largest trials on a range of school-based preventative interventions in England, providing robust data that reflects a wide range of school settings, increasing the external validity of the results. This study adds to the sparse literature on economic evaluations of school-based mental health interventions, assessing not only the costs of implementation, but also changes in service use costs associated with mental health and well-being resulting from the interventions. Detailed data on delivery costs and resources used were collected directly from participants by the research team, which improves understanding of the requirements for implementing such interventions.
Results from the health economic analysis of YAM and The Guide suggest that, based on responses from the first follow-up, there is a low probability that either intervention would be considered cost-effective. There was no evidence to suggest that students in schools randomised to either of the intervention arms had superior outcomes to those in the control arm. Therefore, there is a very low probability that either intervention would be considered cost-effective in the short run. These findings are consistent with those from existing studies of similar programmes, as found by reviews such as that of Mackenzie and Williams Reference Mackenzie and Williams4 – in that effectiveness of school-based universal interventions were neutral or small, with mixed results regarding efficacy – and trials such as MY Resilience In ADolescence. Reference Kuyken, Ball, Crane, Ganguli, Jones and Montero-Marin3 Results from the second follow-up, based on responses from 9 to 12 months after the end of intervention(s), indicate a higher probability (>50%) of YAM being considered cost-effective compared with usual practice. Although service use costs of the intervention group were still higher than that of the usual school provision group, this difference is notably smaller at the second follow-up (£118) compared with the first follow-up (£330).
The specific mechanisms underlying these changes are not entirely clear given the available data. Although cost-savings appear to result primarily from reduced use of health services, it remains uncertain whether this reduction is directly attributable to improved emotional wellbeing. Other potential mechanisms might include increased mental health literacy and awareness, which could lead to earlier self-management and reduced reliance on formal services, or enhanced problem-solving skills fostered by YAM, enabling students to cope more effectively with stressors without needing external support. Reference Kutcher, Wei, Costa, Gusmão, Skokauskas and Sourander21 Additionally, the group setting of the intervention may have contributed to peer support networks, further reducing the need for formal health services. Reference Lyons, Cooper and Lloyd-Evans22 This raises important questions regarding the general applicability of these programmes, particularly in diverse educational settings. It also raises the question of whether programmes of this design should be implemented, or whether alternative measures – such as targeted interventions for vulnerable populations, with associated screening processes – might be a better use of resources.
This study has its limitations. Self-reported data, particularly on service use and quality of life, may be subject to recall bias and/or social desirability bias, which may influence the precision of cost estimates. Studies have found that self-reported service use can be overestimated, when compared with administrative records. Reference Rhodes and Fung23 Additionally, we do not have certainty on whether students in this age group will reliably track and report their service use. However, any bias is likely to be consistent across both the intervention and control groups, suggesting that any impact on relative comparisons or cost-effectiveness estimates should be minimal.
We note also there is attrition in responses at both points of follow-up, relative to the baseline. Future studies on such interventions may benefit from more in-depth investigation as to whether the likelihood of being lost to follow-up is related to student characteristics (e.g. free school meal status). Similarly, subgroup analyses (e.g. by gender) may provide insight as to the type of students who are more likely to benefit from these interventions. In both intervention arms, more responses were received from female students than male students, whereas the opposite was true for the usual practice arm. The reason for this imbalance was outside the scope of the trial, and may be a potential topic for further investigation.
There is also a degree of uncertainty in the reports from staff involved in the delivery of interventions, and the categorical nature of response options (e.g. ‘preparation time’) may not fully capture the time spent, leading to potential inaccuracies. However, these types of responses are less cognitively taxing, Reference Bradburn, Sudman and Wansink24 and this limitation is difficult to avoid without time-tracking data, which would not be feasible. Furthermore, we utilised national average values when estimating resource use costs. Although this approach is standard practice in economic evaluations, it may not fully account for geographic or setting-specific cost variations. The exclusion of broader societal costs, such as productivity losses for parents, may have led to an underestimation of the full economic impact of these interventions.
As well as this, the follow-up period of up to a year following the end of the intervention may limit our ability to capture potential longer-term effects of the intervention. Although the two follow-ups provide early insights, they may not fully capture the long-term benefits of the interventions, particularly in terms of sustained mental health improvements and reduced service use. Longer-term outcomes, especially those related to educational attainment and adult mental health, remain uncertain. Although this trial has a relatively long time horizon compared with similar studies, Reference Hayes, Mansfield, Mason, Santos, Moore and Boehnke25 there is still a need for longer-term follow-ups on both costs and outcomes of participants, as evidence suggests that the full benefits of universal preventive mental health interventions may emerge over a longer time horizon, Reference Le, Esturas, Mihalopoulos, Chiotelis, Bucholc and Chatterton26 Longer-term follow-up would also provide a clearer understanding of how these interventions influence educational attainment and adult mental health outcomes, which are important for assessing the interventions’ full cost-effectiveness.
In conclusion, the AWARE trial provides important insights into the cost-effectiveness of school-based mental health interventions for year 9 students in England. Findings are in line with previous literature suggesting that school-based universal interventions have limited effects on students in terms of QALYs. Although there is some potential for YAM to be cost-effective in the medium term, these calculations are dependent on small changes in outcomes. Our findings are in line with previous analyses of interventions of similar design. Future efforts of improving student mental health and well-being may benefit from increased focus on individual-level, targeted interventions that address the needs of high-risk groups. Additionally, longer follow-up periods are necessary to fully capture the long-term impacts of these interventions, particularly regarding educational attainment and adult mental health outcomes.
Data availability
An anonymised data-set will be made publicly available in the future (planned for 2026).
Author contributions
K.Z. contributed to study methodology, formal analysis and data curation; wrote the original draft of the manuscript and reviewed and edited the manuscript. D.K. contributed to study methodology, formal analysis and manuscript review. J.B. contributed to study methodology, resources, manuscript review and funding acquisition. J.D. contributed to study conceptualisation, resources, manuscript review, project administration and funding acquisition. A.T. contributed to study resources, manuscript review and project administration. E.T. and E.A. contributed to data curation, manuscript review and project administration. C.K. contributed to data curation and manuscript review. D.H. contributed to manuscript review, project administration and funding acquisition. P.S. contributed to manuscript review and funding acquisition. J.S. contributed to manuscript review, resources and project administration. S.E.E.-L. contributed to study methodology, manuscript review, supervision, project administration and funding acquisition.
Funding
This research was commissioned and funded by the UK Department for Education. The commissioner and funder of the study had no role in data collection, data analysis, data interpretation or writing of the report.
Declaration of interest
S.E.E.-L. is a member of the BJPsych Open Editorial Board, but did not take part in the review or decision-making process of this paper. All other authors have no competing interests to declare.


 Open access
Open access
eLetters
No eLetters have been published for this article.