


Frailty is a complex evolutionary process that influences multiple dimensions of an individual’s life. It is associated with generalised chronic inflammation and protein degeneration(Reference Xue1,Reference Baechle, Chen and Makhijani2) . This syndrome predominantly affects the older population, whose physiological degenerative processes are accompanied by losses in physical capacity, functional skills and independence in daily life. Functional and cognitive decline results in disability and dependence on basic activities of daily living and instrumental activities of daily living. Thus, ageing is the greatest risk factor for many chronic diseases that contribute to morbidity and mortality(Reference Clegg, Young and Iliffe3). Furthermore, sarcopenia is a potentially reversible musculoskeletal condition/syndrome that encompasses muscle mass, and specific muscle strength, which is the relationship between muscle strength and muscle size. Consequently, sarcopenia contributes to a range of adverse health outcomes, including impaired functional capacity, mobility limitations, inability to perform activities of daily living and instrumental activities of daily living and poor quality of life (QoL)(Reference Baechle, Chen and Makhijani2). Age-related cognitive decline exacerbates these problems, reducing physical activity levels and increasing disabilities. The combination of frailty and dependence creates a state of high morbidity, leading to long-term disability, falls, hospitalisation and death(Reference Fried, Tangen and Walston4). Several meta-analyses have highlighted the negative impact of frailty on healthcare costs, emphasising the need for interventions to improve frailty and reduce associated costs(Reference Chi, Chen and Zhang5–Reference Pradana, Bai and Hidayat7). Interventions in this population should focus on reversing or slowing the progression of physiological and pathological states. It is well established that physical exercise, particularly strength training, has the most significant positive impact on older adults(Reference Casas Herrero, Cadore and Martínez Velilla8).
Nutritional supplements are frequently combined with resistance training to enhance an individual’s health. A wide range of supplements has been evaluated, patented and implemented in the sports domain to improve performance. Creatine is the most extensively studied supplement and has the strongest evidence base(Reference Kerksick, Wilborn and Roberts9–Reference Xu, Bi and Zhang23), included for sarcopenia management(Reference Liu, Zhang and Li24). Creatine is an endogenously generated molecule that is primarily synthesised in the liver from the amino acids L-arginine, glycine and methionine. However, this endogenous production supplies less than half of the physiological requirements(Reference Jäger, Purpura and Shao25). Although creatine can be obtained from dietary sources such as meat and fish, the amounts provided by these sources are insufficient to saturate the stores. Normal creatine requirements for an individual range between 2 and 3 g per day, whereas the typical intake for omnivorous individuals is between 0,75 and 1,5 g per day(Reference Kreider, Kalman and Antonio10). Approximately 95 % of this molecule is stored in the skeletal muscle, although it is also found in other tissues, such as the brain, where its concentration is up to six times lower(Reference Forbes, Cordingley and Cornish26).
Exogenous creatine supplementation is an effective nutritional intervention for increasing creatine levels in the body. Although multiple formulations such as creatine hydrochloride, citrate, malate, kre-alkalyn and ethyl ester are commercially available, creatine monohydrate CrM is the most supported in terms of efficacy and safety(Reference Jäger, Purpura and Shao25,Reference Kreider, Gonzalez and Hines27,Reference Kreider, Jagim and Antonio28) .
Supplementation protocols include two primary methods to elevate creatine levels: a loading phase involving four doses of 5 g each for 5–7 days or a daily intake of 0.3 g/kg body weight for 30 days(Reference Kreider, Kalman and Antonio10,Reference Candow, Chilibeck and Forbes29) . Creatine is primarily stored in the skeletal muscle and brain, making these organs the main beneficiaries of supplementation. Creatine exists in a minor proportion in its free form and predominantly as phosphocreatine (PCr), an energy-charged form. Both creatine and phosphocreatine, along with ATP, are part of the phosphate energy system, which is responsible for ATP synthesis and energy production(Reference Wallimann, Schlösser and Eppenberger30,Reference Wallimann, Dolder and Schlattner31) . Thus, higher intramuscular creatine levels correspond to greater energy production capacity. This increase in energy can manifest as greater work capacity and recovery, indirectly improving strength and power capabilities. Among the reviewed evidence, creatine was the only nutritional supplement that affected muscle mass in older patients. Improvements in function, strength and muscle mass have been observed in individuals aged 65–75 years and even in those aged >85 years(Reference Stares and Bains32).
Cognition encompasses a range of cognitive domains. These include attention, executive function, decision-making, memory, reasoning, perception, language, creativity and knowledge. As mentioned above, the brain is a storage site for creatine. Evidence suggests that Creatine supplementation increases cerebral creatine levels(Reference Pan and Takahashi33,Reference Dechent, Pouwels and Wilken34) . Studies in older patients using a loading protocol of 20 g/d of creatine for 7 days, compared with placebo showed significant improvements in memory(Reference McMorris, Mielcarz and Harris35). In addition, studies have shown a reduction in mental fatigue and improved cognitive function under stressful conditions, such as sleep deprivation or when cerebral energy demands are high(Reference Forbes, Cordingley and Cornish26,Reference Wallimann, Dolder and Schlattner31,Reference Gordji-Nejad, Matusch and Kleedörfer36–Reference Roschel, Gualano and Ostojic39) . CrM supplementation has also been proposed for the treatment of depression(Reference Sherpa, De Giorgi and Ostinelli40,Reference Fabiano and Stubbs41) .
Most studies on older adults receiving creatine supplementation have included strength training protocols. Creatine plays a role in the energetic function of skeletal muscles, making it potentially ideal for enhancing the benefits of regular physical activity. Randomised clinical trials of creatine supplementation alongside resistance training involving participants of both sexes have examined muscle and bone density(Reference Candow, Chilibeck and Gordon42), muscle mass, strength, body composition(Reference Candow, Zello and Ling43–Reference Brose, Parise and Tarnopolsky45), oxidative stress emissions, defence mechanisms, QoL(Reference Amiri and Sheikholeslami-Vatani46) and effects on inflammation and insulin resistance(Reference Oliveira, Antunes and Gomes47). The results demonstrated maintenance and improvement of bone density, increased lean mass and muscle strength, reduced adipose tissue, decreased oxidative stress levels and improved QoL(Reference Candow, Ostojic and Forbes48).
In addition, as ageing progresses beyond the threshold of 65 years, an age often used as a clinical marker for increased vulnerability to sarcopenia, frailty and co-morbidity, the physiological context in which creatine may exert its effects shifts significantly. Creatine may have potential benefits for musculoskeletal wellbeing in the elderly(Reference Hong, Wang and Jin49). Older adults tend to have more pronounced anabolic resistance, neuromuscular decline and cognitive impairment, which may alter the efficacy and safety profile of creatine supplementation. Therefore, aggregating data from broader adult populations without age stratification may dilute the findings that are highly relevant to this vulnerable subgroup. In a meta-analysis that evaluated the effect of CrM supplementation, none of the studies included participants aged ≥ 75 years(Reference Wang, Qiu and Li16,Reference Candow, Prokopidis and Forbes21) .
While isolated strength training is an essential strategy to combat sarcopenia and age-related muscle loss, multicomponent training (MT) – incorporating strength, balance and aerobic exercises – is currently recognised as the clinical gold standard for older adults, particularly the oldest old (≥ 75 years). Previous robust evidence, including studies from our research group(Reference Martínez-Velilla, Casas-Herrero and Zambom-Ferraresi50), has demonstrated that multicomponent exercise programmes maximise improvements in activities of daily living, significantly reduce fall risk and help prevent cognitive decline more effectively than strength-only protocols. Building on this comprehensive approach, our study aims to evaluate the effects of CrM supplementation combined with MT on functional and cognitive capacities in older adults aged ≥ 75 years.
Methods
A randomised, double-blind, placebo-controlled, four-arm clinical trial will be conducted to assess whether a CrM supplementation intervention, with or without MT, improves functional and cognitive performance in community-dwelling older adults ≥ 75 years.
The participants will be divided into four groups: placebo supplementation (PL), placebo supplementation + multicomponent training (PL + MT), creatine monohydrate supplementation (CrM), and creatine monohydrate supplementation + multicomponent training (CrM + MT).
Participants will be randomly assigned to groups. At the initial assessment, participants will be informed only of their assignment to the exercise or non-exercise condition. The double-blind will be strictly maintained for the nutritional intervention (CRM/PL) for the study duration. All participants will receive supplements (CrM or PL). Half of the participants will perform eight supervised multicomponent physical training sessions in the gymnasium of the Geriatrics Unit of the hospital, together with the assigned supplementation. Participants not assigned to the supervised training sessions will receive the usual care provided to the other participants, both at their health centre and at the Geriatric Unit.
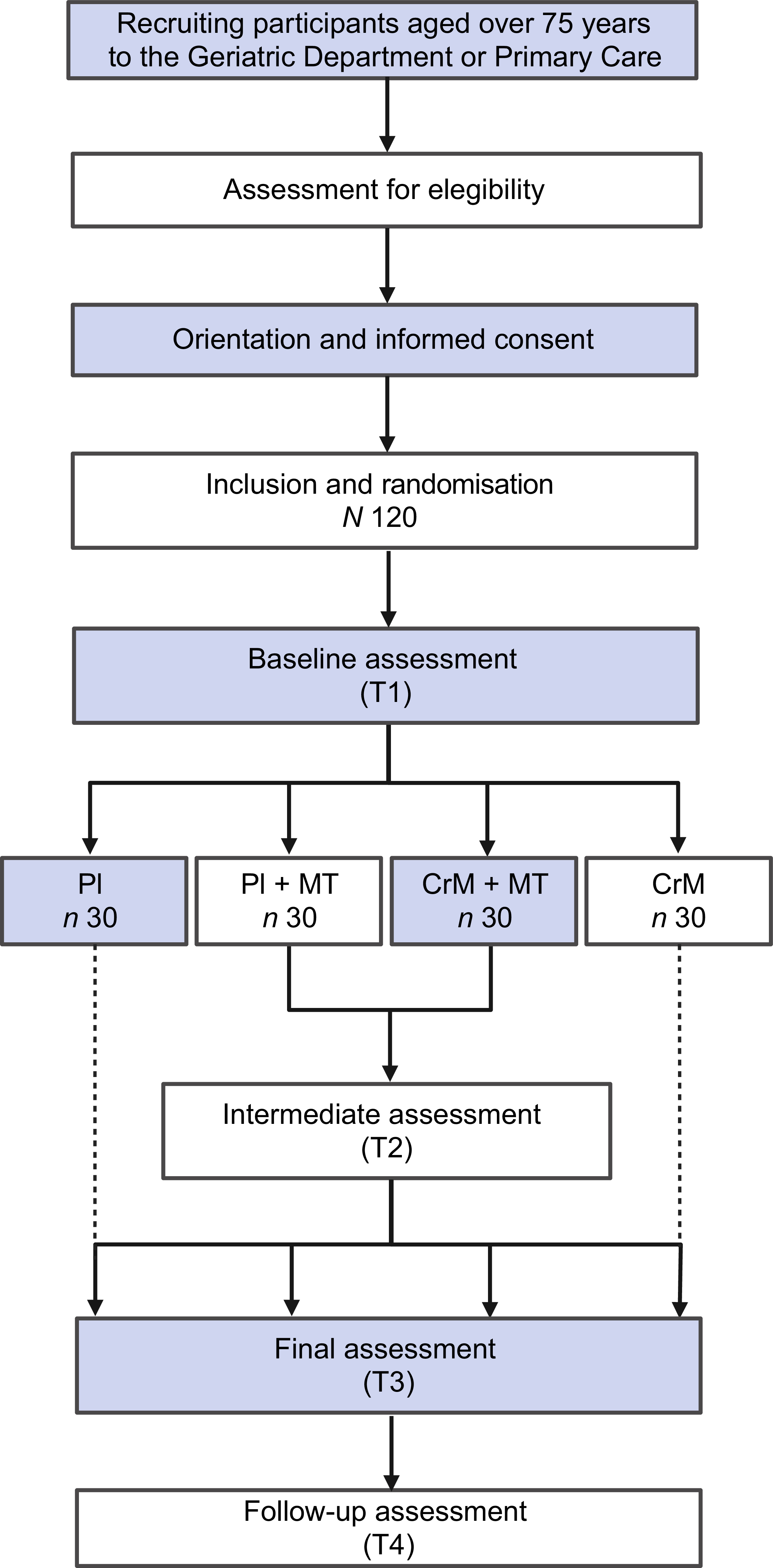
The study flow diagram is presented in Figure 1.
Flow diagram of the study protocol. PL, placebo; MT, multicomponent training; CrM, creatine monohydrate.

Figure 1. Long description
The flowchart begins with recruiting participants aged over 75 years to the Geriatric Department or Primary Care. This is followed by an assessment for eligibility, orientation, and informed consent. After inclusion and randomization of 120 participants, a baseline assessment (T1) is conducted. Participants are then divided into four groups: PI with 30 participants, PI plus MT with 30 participants, CrM plus MT with 30 participants, and CrM with 30 participants. An intermediate assessment (T2) follows, leading to a final assessment (T3) and a follow-up assessment (T4). The flowchart uses rectangles to denote steps and includes labels such as PI, MT, and CrM to indicate different intervention groups.
The geriatric research team will be divided into two groups to maintain double blinding. One group will be responsible for performing the assessments, and the other group will be responsible for delivering the supplementation according to randomisation. In the case of the MT groups (PL + MT and CrM + MT), the schedules of the two weekly training sessions will be agreed upon.
Study participants and eligibility criteria
Participants will be recruited through referrals from the hospital’s geriatrics specialist practice and through dissemination and promotion in the community and health centres. Participants will meet the following inclusion criteria: (1) age ≥ 75 years, (2) ability to ambulate with or without personal/technical assistance, (3) life expectancy ≥ 6 months, (4) Barthel Index score ≥ 60 and (5) informed consent from participants or legal representatives.
The exclusion criteria will be as follows: (1) Global Deterioration Scale (GDS 6–7), (2) intolerance or allergy to foods or drugs, (3) deglutition problems (Dx: dysphagia), (4) any pathological or metabolic condition incompatible with physical exercise, (5) consumption of any creatine supplement during the last 6 weeks, (6) consumption of more than 200 mg of caffeine daily, (7) supervised physical training, (8) diagnosis of acute renal failure and (9) glomerular filtration rate less than 45 ml/min/1,73 m2 in a blood test in the last 12 months.
Sample size
Assuming a pre-post correlation of 0,7 in the Short Physical Performance Battery (SPPB) value and an expected change of 1 point in the exercise group and in the supplementation group, 2 points in the exercise and supplementation group, and no change in the control group, an effect size of 0,35 was expected for an ANOVA test of overall significance. For a significance level of α = 0,05 and a power of 80 %, twenty-four participants per group will be necessary to detect this effect size as statistically significant. Assuming a 20 % loss rate, this means a sample size of thirty participants per group, which totals 120 participants(Reference Martínez-Velilla, Casas-Herrero and Zambom-Ferraresi50).
Randomisation and blinding
The sample will be randomised using Randomizer® software to ensure the impartiality and scientific validity of the study. This programme guarantees a rigorously random distribution, minimises any possible bias and ensures an equitable distribution of participants among the different study groups. Thus, the integrity and reliability of the results obtained will be preserved.
After providing informed consent, 120 participants will be randomised into one of four arms: PL, CrM, PL + MT or CrM + MT. To maintain blinding throughout the study, participants, instructors delivering the MT and outcome assessors will remain unaware of group allocation.
Detailed description of intervention groups
Supplementation groups
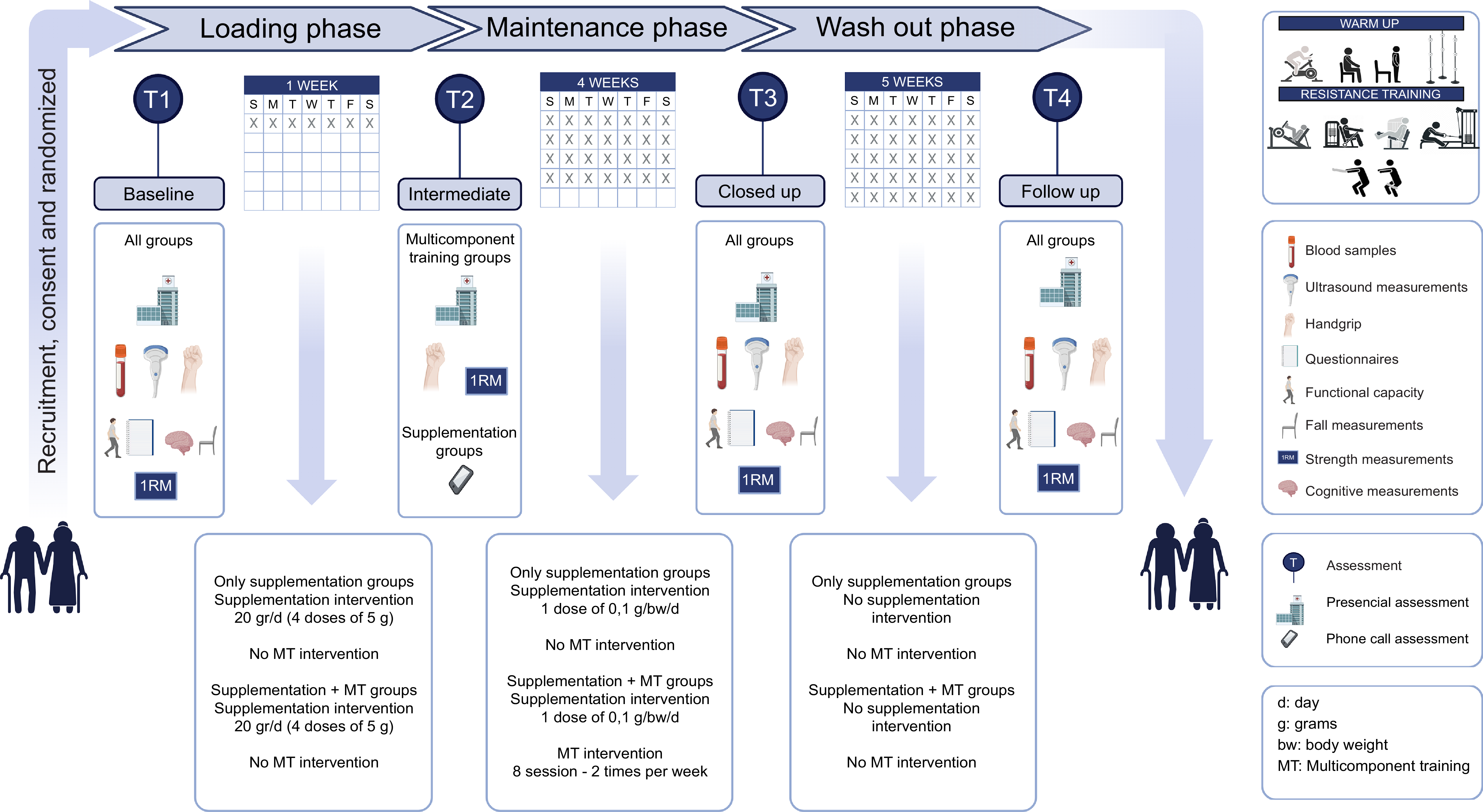
We will use micronised CrM (Creavitalis®; Alzchem Group). The placebo will be hydrolysed rice powder. All participants will receive oral and written instructions on how to take the supplements. Participants will receive the supplements in unsealed, opaque envelopes. All investigators will be blinded to the participants receiving CrM supplementation or placebo. The protocol consists of three interventions. The first phase, called the loading phase, will begin the day after the baseline. Participants will take 20 g of the powder placebo or CrM daily in four doses of 5 g for a week (7 d). In the maintenance phase, participants will receive a powder dose dependent on body weight (bw) (0,1 g × bw) daily for 4 weeks (28 d). Finally, in the 5-week (35 d) washout phase, participants will not take supplements or any exercise programme. Participants will be asked to maintain their usual physical activity and dietary routines throughout the intervention. To improve adherence and ensure correct supplementation, participants will complete and submit a registration form.
The timeline of the study protocol is detailed in Figure 2.
Timeline of the study protocol.

Figure 2. Long description
The diagram illustrates the timeline of a study protocol divided into four phases: recruitment, loading, maintenance, and washout. The recruitment phase involves consent and randomization. The loading phase lasts one week with daily supplementation and no exercise intervention. The maintenance phase spans four weeks with daily supplementation and exercise intervention, including multicomponent training sessions twice a week. The washout phase lasts five weeks with no supplementation or exercise intervention. The diagram includes various assessments such as blood samples, ultrasound measurements, functional capacity tests, strength measurements, cognitive measurements, and questionnaires. Different activities like warm-up exercises, resistance training, stationary bicycle, chair squats, leg press, seated bench press, leg extension, seated row, and core exercises are depicted. Assessments are conducted at four time points: baseline, intermediate, closed-up, and follow-up.
Multicomponent training groups
MT will begin after the loading phase. The intervention will consist of an exercise-training programme during the maintenance phase of supplementation. Professionals will guide and supervise MT sessions, either alone or in groups. Experienced physical trainers will carefully monitor and supervise all training sessions and provide instructions. Exercise intensity will be monitored using the modified Borg CR-10 scale. Participants will undergo a familiarisation session to ensure proper interpretation of perceived exertion. Given that many participants may be on chronotropic-blunting medications (e.g. β-blockers), heart rate is not a reliable intensity marker.
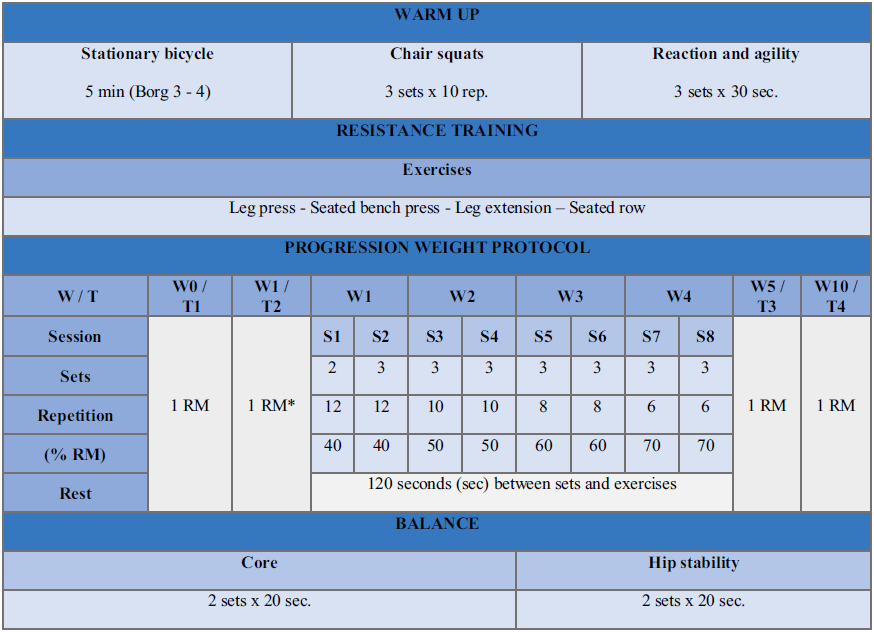
The sessions will be divided into three parts: warm-up, resistance training and cool-down. The warm-up will start on a stationary bicycle, sit-ups and reaction and agility exercises. Core and hip stability exercises will be performed at the end of each session. The resistance training protocol will include 2–3 sets of 8–12 repetitions at an intensity of 40–70 % of the one-repetition maximum (1RM). ‘1RM’ is the maximum resistance a person can move in one repetition of an exercise. Maximum dynamic strength will be estimated following the American College of Sports Medicine (ACSM) guidelines. To ensure safety in this advanced age group (≥ 75 years), a submaximal multiple-repetition test (e.g. 4–8 RM) will be performed to predict the 1RM, avoiding the risks associated with lifting a maximal load(Reference Liguori and Feito51). The 1RM will be measured at baseline and at the intermediate assessment to adapt to resistance training. The warm-up session will include chair squats (chair height 46 cm), reaction and agility (Lumminic 6 Pro). The resistance training machines will be leg press (Matrix Fitness Versa MD Leg Press), bench press (EGYM – Smart Strength Bench Press), leg extension (Versa MD Leg Extension Leg Curl) and seated row (EGYM – Smart Strength Seated Row).
The MT protocol is described in Table 1.
Multicomponent training protocol

Table 1. Long description
The table outlines a multicomponent training protocol, including warm-up exercises such as stationary bicycle, chair squats, and reaction and agility drills. The resistance training section lists exercises like leg press, seated bench press, leg extension, and seated row. The progression weight protocol details sessions, sets, repetitions, percentage of one-repetition maximum, and rest periods across multiple weeks. It specifies the number of sets and repetitions for each session, along with the percentage of one-repetition maximum to be used. Balance and core exercises, such as hip stability, are also included. The table provides a structured approach to resistance training over a period of weeks, with specific guidelines for each session.
T, assessment; S, session; RM, repetition maximums.
*Only training groups
The investigators and participants (e.g. acute illness, initiation of new medications and personal problems) will agree upon the criteria for discontinuing or modifying the interventions assigned to a particular trial participant.
Data collection
The assessments will be conducted at four different times. Baseline measurements (T1) will be taken at the time of inclusion in the study. After the loading phase, an intermediate assessment (T2) will be included in the training groups. Follow-up measurements will be taken 5 weeks after the baseline assessment (T3). In addition, a follow-up (T4) will be carried out 5 weeks after the end of the control or intervention periods to check whether the effects of supplementation last over time. The T4 assessment is scheduled exactly 5 weeks post-intervention to allow for a complete physiological washout of intramuscular PCr stores, which typically take 4–6 weeks to return to baseline(Reference Hultman, Söderlund and Timmons52).This timing will allow us to evaluate if the functional benefits are maintained after the ergogenic aid is eliminated. The times of measurement for the different outcomes are shown in Table 2.
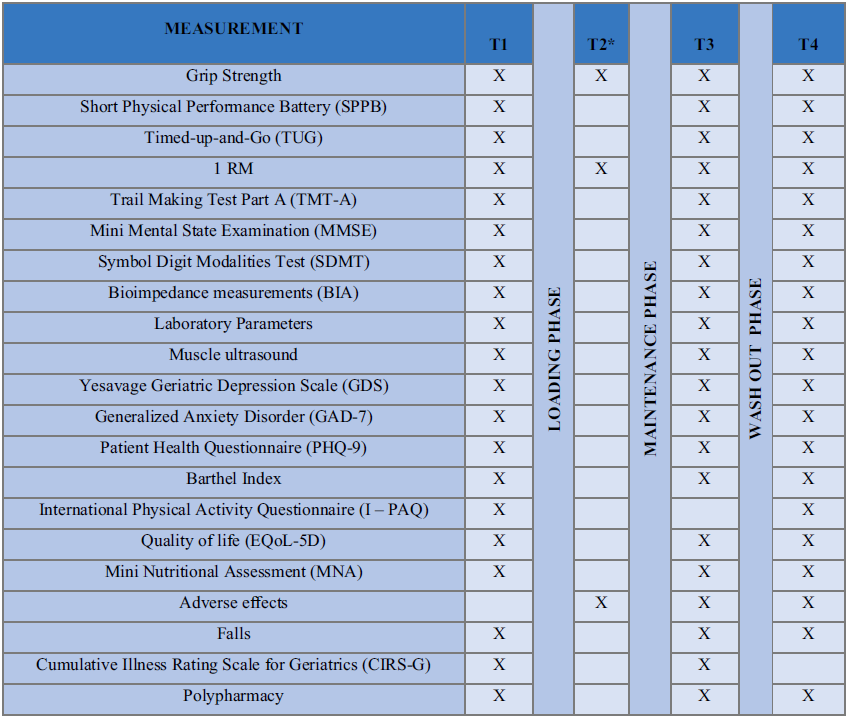
Time of measurement of different variables in the study subjects

Table 2. Long description
A table with four columns and sixteen rows. The columns are labeled Measurement, T1, T2, T3, and T4. The rows list various measurements such as Grip strength, Short Physical Performance Battery, 1 RM, Trail Making Test Part A, Mini Mental State Examination, Symbol Digit Modalities Test, Bioimpedance measurements, Laboratory parameters, Muscle ultrasound, Yesavage Geriatric Depression Scale, Generalized Anxiety Disorder, Patient Health Questionnaire, Barthel Index, International Physical Activity Questionnaire, Quality of life, Mini Nutritional Assessment, Adverse effects, Cumulative Illness Rating Scale for Geriatrics, and Polypharmacy. Each row indicates the timing of measurements during the study phases: Loading Phase, Maintenance Phase, and Washout phase.
*T2 only training groups.
Completed personal data or other documents containing protected personal health information will be kept in a locked file in the principal investigator’s office. Data will be entered into an electronic de-identified database by authorised study team members and checked for completeness and accuracy. Access to data with identifiers will be restricted to authorised study team members and the authorities. Electronic data will be stored on a secure server regulated by the local research institute. Identifiable data will be destroyed 10 years after the end of the study or 5 years after the last publication, whichever comes first.
Trial status
The trial commenced recruitment in December 2024 and is currently open for recruitment. Recruitment will cease when 120 participants are randomised. It is anticipated that this target will be achieved by June 2026.
Outcome measures
Primary outcome
-
- Functional capacity: SPPB to facilitate the early detection of frailty by evaluating the functionality of the lower extremities through three different tests, static balance, 4-m walking speed and time to perform five squats at a standard chair (46 cm in height approximately. Each parameter is scored from 0 to 4, with a maximum total score of 12 points. It allows us to quantify the physical frailty of participants according to their score: 0–3 disabled person, 4–6 frail person, 7–9 pre-frail person and 10–12 robust person(Reference Guralnik, Simonsick and Ferrucci53).
-
- Strength: One maximum repetition (1RM). This procedure will be carried out by performing multiple repetitions, with the objective of increasing the load until the repetition cannot be performed. The 1RM will be estimated as the last weight lifted(Reference Barbalho, Gentil and Raiol54,Reference Di Fabio55) .
-
- Cognitive status:
-
○ Trail Making Test – Part A (TMT-A). Participants will be required to put together a distribution of numbers from 1 to 25 on a sheet of paper(Reference Reitan56–Reference Iñesta, Oltra-Cucarella and Bonete-López59).
-
○ The Mini Mental State Examination (MMSE) assesses temporal orientation, spatial orientation, fixation memory, concentration and calculation, delayed memory, nomination, repetition, comprehension, reading, writing and drawing. The minimum and maximum scores are 0 and 30, respectively. A normal score is between 25 and 30 points, mild cognitive impairment is between 19 and 24 points, moderate impairment is between 14 and 18 points, and below that score it is classified as severe cognitive impairment or dementia(Reference Molloy and Standish60,Reference Folstein, Folstein and McHugh61) . The age and level of education of the test taker will be considered for the readjustment of the final score.
-
○ Symbol Digit Modalities Test (SDMT) measures sustained attention, processing speed, visual scanning speed and motor speed(Reference Iñesta, Oltra-Cucarella and Bonete-López59,Reference Smith62,Reference Smith63) .
-
- Laboratory parameters: The data obtained from the samples will be used for nutritional and safety assessments of the participants. Peripheral blood samples will be obtained from all participants at baseline, discharge and follow-up assessments. Serum and EDTA blood collection tubes (Vacuette®, Greiner Bio-One) will be used for samples collection. All peripheral blood samples will be centrifuged in a fixed-angle rotor at 3000 rpm for 15 min at room temperature. Serum, plasma and buffy coat will be collected, aliquoted into labelled cryovials and stored at −80°C. Laboratory parameters will include markers of renal safety (serum creatinine and estimated glomerular filtration rate), basal metabolic status (fasting glucose and lipid profile), nutritional status (total proteins and albumin) and basal inflammation.
-
Secondary outcome
-
- Muscle status: An ultrasound of the mid-thigh, using a Clarius® HD3 L7 probe (Clarius Mobile Health), will be performed to measure the total thigh thickness, quadriceps rectus femoris thickness, deep rectus thickness, subcutaneous adipose tissue thickness in cm, quadriceps rectus femoris area in cm2 and the angle of penetration of the each leg(Reference Saito, Ema and Inami64,Reference López Jiménez, Reinoso Párraga and González Ramírez65) .
-
- Anthropometric measurements: Body composition will be determined by conventional bioelectrical impedance analyser (BIA) and Bioelectrical Impedance Vector Analysis (BIVA) by a single investigator using a single-frequency 50 kHz bioelectrical impedance analyser (BIA 101 RJL, Akern Bioresearch) according to the standard tetrapolar technique, with the participant in the supine position and the electrodes placed on the dorsal surface of the right foot and ankle and right wrist and hand(Reference Goes, Santos and de Siqueira Oliveira66) to measure appendicular skeletal muscle mass index (ASM/BMI), RMR and phase angle. These variables will be assessed to evaluate the effect in body composition and nutritional status related to CrM supplementation and MT over the course of the intervention.
-
- Psychological status:
-
○ The Geriatric Depression Scale (GDS-15) assesses the presence or absence of depressive symptoms using a fifteen-item closed-response questionnaire, in which one point is awarded depending on the question and answer. The results can be interpreted as follows: scores of 0–5 are normal. A score greater than 5 suggests depression(Reference Yesavage, Brink and Rose67–Reference Yesavage and Sheikh70).
-
○ The Patient Health Questionnaire (PHQ) is a self-administered version for common mental disorders. The PHQ-9 is the depression module, which scores each of the nine DSM-IV criteria as ‘0’ (not at all) to ‘3’ (nearly every day)(Reference Kroenke, Spitzer and Williams71).
-
○ Generalised Anxiety Disorder (GAD-7) scale consists of seven items measuring worry and anxiety symptoms. Each item is scored on a four-point Likert scale (0–3), with total scores ranging from 0 to 21, with higher scores reflecting greater anxiety severity(Reference Spitzer, Kroenke and Williams72).
-
-
- Grip strength will be measured using a Takei Hand Grip Dynamometer. Grip strength will be assessed using a digital hand dynamometer. Participants will perform two maximum voluntary contractions with their dominant hand, separated by a 30-s rest interval. The highest value will be recorded for analysis(Reference Bohannon73,Reference Ramírez-Vélez, Sáez de Asteasu and Martínez-Velilla74) .
-
- Mini Nutritional Assessment (MNA) is a questionnaire used to screen the nutritional status of older adults, with questions in which the answers are scored from 0 to 2 or 3. The sum of the points ranges from 0 to 7, malnutrition; 8 to 11, risk of malnutrition; and 12 to 14, normal nutritional status(Reference Cereda75–Reference Vellas, Villars and Abellan78).
-
- Risk of falls: The Timed Up and Go Test (TUG) is a sensitive and specific test that measures the probability of falls in older adults. A standard chair (approximately 46 cm in height) and a cone will be placed 3 m away. The participant in a seated position will have to get up from the chair, move towards the cone, go around it and return to the chair to sit down. Less than 10 s is normal, 11–13 s indicates low disability and more than 13 s indicates a high risk of failure(Reference Pereiro, Campos-Magdaleno and Navarro-Pardo79–Reference Shumway-Cook, Brauer and Woollacott81).
-
- QoL: EuroQol Scale-5D (EQoL-5D). This instrument measures five dimensions of health status: mobility, self-care, usual activities, pain/discomfort and anxiety/depression(82,Reference Rabin and de Charro83) . In addition, the visual analog scale will be used to quantify perceived health (from 0, worst health state imaginable, to 100, best health state imaginable).
-
- Fatigue of the session with rating of perceived exertion: We will use the Borg Scale, which assesses the subjective effort perceived by a person performing an activity(Reference Borg84–Reference Borg86).
-
- Other end points: Geriatric syndromes, the Cumulative Illness Rating Scale for Geriatrics (CIRS-G), polypharmacy and the International Classification of Diseases (ICD-10), adverse events and falls.
-
- Sociodemographic variables: Level of education, marital status, residence, falls, hospitalisations, AE and deaths will be collected during the intervention.
Data analysis
First, a comprehensive descriptive analysis will be conducted on the entire sample and within individual groups. For continuous variables, measures of central tendency and dispersion will be calculated based on their distribution, utilising either the mean and standard deviation or the median and interquartile range. Qualitative variables will be summarised as frequencies and percentages, with corresponding CI to estimate overall prevalence. Baseline characteristics between the treatment and control groups will be compared using the Student’s t test or the Mann–Whitney U test for quantitative variables, and the χ 2 or Fisher’s exact test for qualitative variables.
The impact of the intervention on various outcome measures will be assessed using ANCOVA or linear mixed-effects models for continuous variables. Logistic regression models and analyses of rate or proportion differences will be applied to outcomes such as falls, mortality and institutionalisation. In the event of significant baseline imbalances in any independent variable, sensitivity analyses will be conducted to adjust for these differences in the final analysis. No imputation of missing data will be performed.
The analysis will adhere to the intention-to-treat principle, with additional per-protocol analyses performed as a secondary sensitivity measure. Statistical significance will be determined at a threshold of 0·05. Data analysis will be conducted using SPSS version 25.0 and R software (version 4.0).
Discussion
This randomised, double-blind, placebo-controlled, four-arm clinical trial will investigate the potential benefits of creatine supplementation in combination with MT on cognitive and functional capacities in individuals aged ≥ 75 years. Although previous studies have extensively documented the effects of creatine on muscle strength and physical performance, this study examined its impact on cognitive domains. The hypothesis to be tested is that creatine supplementation could specifically enhance cognitive capacity, particularly in memory, attention and executive function, in a population that is highly susceptible to age-related cognitive decline.
Cognitive improvements
Cognition encompasses a range of functions, including memory, attention and executive abilities. Emerging evidence suggests that creatine supplementation increases the cerebral creatine concentration, potentially enhancing energy availability for neuronal processes, particularly under conditions of heightened cerebral energy demand. Studies have demonstrated improvements in memory performance following short-term creatine loading protocols (20 g/d for 7 d) in older adults. This finding suggests an acute effect on tasks that require substantial mental effort(Reference Lobo, Tritto and Da Silva87,Reference Devries and Phillips88) . Moreover, creatine has been shown to mitigate mental fatigue and enhance cognitive function under stressful conditions, such as sleep deprivation(Reference Lobo, Tritto and Da Silva87,Reference Rae, Digney and McEwan89,Reference Todorovic, Nedeljkovic and Panic90) . While this study focuses on a population aged ≥ 75 years, the majority of prior research has excluded this demographic, thus highlighting a gap that this trial seeks to address(Reference Candow, Chilibeck and Forbes91).
Physical function and muscle mass
The effects of creatine on muscle strength and mass have been extensively documented in both younger and older populations. Creatine in the phosphagen energy system facilitates ATP resynthesis during high-energy-demand activities. This process has the potential to enhance muscle performance and recovery(Reference Rawson and Venezia92,Reference Benton and Donohoe93) . Investigations in older adults combining creatine supplementation with resistance training have demonstrated significant increases in muscle strength, lean body mass and bone mineral density(Reference Sales, Pinto and Rodrigues94). However, these effects have not been thoroughly evaluated in individuals aged ≥ 75 years, rendering this study crucial for elucidating whether these benefits extend to the oldest segment of the population.
Combined effects of training and supplementation
MT, which encompasses strength, balance and aerobic exercises, forms the foundation for mitigating frailty and functional decline in older adults(Reference Liu and Latham95). The combination of creatine supplementation and structured physical training may yield synergistic effects, enhancing outcomes such as gait velocity, postural stability and overall QoL (Reference Chilibeck, Kaviani and Candow96,Reference Stefani and Galanti97) . Previous investigations have demonstrated greater improvements in physical and functional parameters among cohorts receiving both interventions compared with training alone, although the impact on cognitive outcomes remains insufficiently elucidated(Reference Forbes, Cordingley and Cornish26,Reference Candow, Vogt and Johannsmeyer44,Reference Chilibeck, Kaviani and Candow96,Reference Aguiar, Januário and Junior98,Reference Bonilla, Stout and Candow99) .
Safety considerations
Concerns regarding the potential renal toxicity of creatine supplementation have been refuted in healthy populations, including older adults, as no significant alterations in creatinine levels or glomerular filtration rate have been observed in controlled trials(Reference Tarnopolsky100,Reference Harmon, Stout and Fukuda101) . This investigation incorporates regular monitoring of renal function to ensure participant safety, reinforcing the established safety profile of creatine supplementation when administered appropriately(Reference Kreider, Kalman and Antonio10,Reference Poortmans and Francaux102) . Current evidence supports the safety and benefits of creatine supplementation throughout life, including in old age(Reference Kreider, Jagim and Antonio28).
Implications for clinical practice
The findings of this study may inform interventions that address functional and cognitive decline in older adults. If creatine supplementation proves efficacious, it could potentially serve as a cost-effective, scalable strategy to complement exercise programmes in the geriatric population of the community. Furthermore, this study addresses the critical need for evidence-based interventions in individuals aged ≥ 75 years, a demographic that is frequently under-represented in clinical trials(Reference Clegg, Young and Iliffe3,Reference Fried, Tangen and Walston4,Reference Cruz-Jentoft, Bahat and Bauer103,Reference Livingston, Huntley and Sommerlad104) .
Study limitations
This study protocol has several limitations. First, the 4-week (8 sessions) intervention is a relatively short period to observe significant structural changes in body composition, such as muscle hypertrophy, and may not capture long-term effects. However, previous studies indicate that early neural adaptations to resistance training in the oldest old occur within the first 2–4 weeks, leading to functional gains. This duration was chosen to robustly test the feasibility, safety and initial efficacy of the combined protocol. In a similar way, cognitive improvements might require a longer duration of supplementation to fully manifest, given the chronic nature of cognitive decline(Reference Lobo, Tritto and Da Silva87,Reference Devries and Phillips88,Reference Rawson and Venezia92) . Another potential limitation is the reliance on compliance with both the supplementation and exercise protocols. Second, while we aim to recruit both sexes equitably, the demographic reality of the ≥ 75 years age group and higher female volunteerism may result in a sex bias, making perfect sex stratification across the four intervention arms challenging.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107302
Acknowledgements
Open access funding provided by Universidad Pública de Navarra. M. F.-G. R. (main authorship) is supported by a predoctoral fellowship.
M. F.-G. R.: Conceptualisation, Investigation, Methodology, Project administration, Writing – original draft and Writing – review and editing. F. Z-F.: Conceptualisation, Methodology, Supervision, Writing – original draft and Writing – review and editing. F. Z-F.: Project administration and Resources. M. I-C.: Formal analysis, Investigation and Software Supervision. P. Á. R.: Conceptualisation, Investigation and Methodology. A. Z-M.: Conceptualisation and Methodology. I. E. B.: Project administration. B. C-V.: Investigation. D. M-P.: Formal analysis and Resources. A. C-S.: Investigation. D. M-C.: Investigation. N. S-R.: Conceptualisation, Investigation, Methodology, Project administration, Supervision, Writing – original draft and Writing – review and editing. N. M-V.: Conceptualisation, Investigation, Methodology, Supervision, Writing – original draft and Writing – review and editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest
The authors will disseminate the results of our study through presentations at international conferences and articles in peer-reviewed journals.
This study follows the principles of the Declaration of Helsinki (World Medical Association, 2013), and it has been approved by the Committee on the Ethics of Research on Medicines of the Autonomous Community in July 2024 (PI_2024/73). All participants will provide written informed consent to participate in this study.
The manuscript is adhered to SPIRIT guidelines for protocols.



 Open access
Open access