


Introduction
Osteomyelitis variolosa is an osteological condition caused by the variola virus (the causative agent of smallpox) and is found in some individuals who have contracted smallpox in childhood but survived. There may be both short-term and long-term osteological effects, and some of these may appear only some years or decades after the initial smallpox infection. Here we present a case of osteomyelitis variolosa identified in a skeleton from the Western Cemetery at Cirencester (Corinium) in Britain, dated to the 3rd or 4th c. CE. Its significance is that it makes a contribution to the current debate over the antiquity of smallpox, as it shows that smallpox was present in late 3rd- or 4th-c. Britain. The findings have implications also for our understanding of the 2nd-c. Antonine Plague, whose identification as smallpox has been hotly contested in recent years.
Identification of osteomyelitis variolosa in osteology
Viral infections are typically acute, often leaving insufficient time for the development of macroscopically discernible changes in bone before the resolution of the disease by recovery or the death of the victim.Footnote 1 However, smallpox (variola) stands out as one of the few viral diseases recognizable in the archaeological record through skeletal remains. Despite the fact that smallpox was declared in 1980 by the World Health Organization to have been eradicated after a worldwide vaccination campaign in the 1970s, adults who survived a childhood infection of smallpox continue to present at clinics in India and China with skeletal abnormalities.Footnote 2 This kind of bone involvement is called osteomyelitis variolosa and occurs mainly in people who have had a smallpox infection in childhood – cases arising from a smallpox infection in adulthood are not unknown, but are very rare. The smallpox virus may directly infect bone marrow cells, disrupting the processes of bone growth and resorption (loss of bone cells that are absorbed back into the circulatory system) especially in its acute stage, or it may induce an autoimmune response that triggers inflammation, similar to the mechanisms observed in other viral arthritis.Footnote 3 During smallpox epidemics in the 20th c., approximately 2–5% of affected children, or 0.25–0.5% of all patients, exhibited osteoarticular manifestations, most frequently affecting the elbows, wrists, ankles, hands, and feet.Footnote 4 These osteoarticular complications typically appear between the first and fourth week of illness, initially presenting as gradual swelling around the joints and eventually affecting the adjacent long bones.Footnote 5 It is thought that the reason children are affected is that their bones have not stopped growing, and the virus attacks the skeleton particularly through the physeal growth plate, an area of cartilage towards the end of the long bones where longitudinal growth takes place.Footnote 6 This would explain why the joints are particularly affected, and why those who contract smallpox in adulthood rarely show osteological damage, since the cartilage growth plate has been replaced by an ossified plate once growth stops. The resulting deformities from the osteoarticular complications may arise from reparative ossification and distortion, including the cessation of longitudinal bone growth, possibly due to the destruction of the physeal growth plate.Footnote 7 In those who survive a childhood infection, further complications may arise in adult life, continuing to progress into old age.
In the archaeological record, 11 individuals with potential smallpox bone involvement have been identified thus far. They come from France, England, Canada, Portugal, Peru, and the United States, and date between the 10th and 19th c. CE (Table 1).Footnote 8 No individual before the 10th c. CE has previously been identified as having osteomyelitis variolosa.
Identified cases of osteomyelitis variolosa in medieval and early modern populations (after Crawford et al. Reference Crawford, Hodson and Errickson2024, 67, table 1, with additions and modifications).

Short-term and long-term sequelae of smallpox
Short-term consequences, or “sequelae”, of smallpox, such as skeletal involvement, typically manifest between one and six weeks following the onset of infection. During the incubation of smallpox, the virus may infect the bone marrow and cause inflammation and swelling of the soft tissue around joints, resulting in painful and restricted movement.Footnote 9 The skeletal effects are typically but not always bilateral (affecting both the left and the right limbs), and characterized by nonsuppurative osteomyelitis with necrosis, suppurative (pus-producing) arthritis as a result of a secondary infection, and multifocal nonsuppurative arthritis.Footnote 10 Five archaeologically identified individuals, all under the age of 13, exhibit bone alterations indicative of these short-term effects, suggesting they did not survive long enough for more prolonged impacts of the disease to develop (Table 1, nos. 1, 7, 8, 10, 11).
Long-term manifestations are seen in individuals who survived the original smallpox infection longer. They include joint instability, diminished function, and restricted mobility. Additionally, necrosis in fusing joints may lead to epiphyseal fusion, resulting in bone distortion, malformation, and ankylosis (joint stiffness and rigidity).Footnote 11 These late-stage conditions are typically observed in individuals more than a decade after the smallpox infection, and may continue to progress and deteriorate for many years, until the individual's death.Footnote 12
The primary distinction lies in the immediacy and type of skeletal involvement, with short-term effects being more reversible and less severe than the often irreversible, debilitating long-term conditions that emerge years after the initial disease episode. Skeletal evidence of short-term sequelae in adults is exceedingly rare, but smallpox should still be considered among the differential diagnoses when such lesions are observed.Footnote 13 This is particularly relevant in the archaeological record, especially for periods when smallpox was less likely to have been endemic, as its impact on adults may have been less rare than suggested in the clinical literature.Footnote 14 While later-stage lesions generally present bilaterally, some older clinical reports show that secondary pyogenic (suppurative or pus-producing) infections may occur unilaterally.Footnote 15 Where lesions do present bilaterally, they are not necessarily precisely symmetrical.
Lesion distribution
The most clearly diagnostic skeletal indicator of osteomyelitis variolosa is involvement of the arms, and particularly the bilateral involvement of the elbow joints.Footnote 16 As the key work on the archaeological identification of osteomyelitis variolosa, by Crawford et al., puts it: “Elbow involvement was documented in 80% of smallpox patients displaying bone involvement, and bilaterality was a key feature, which Cockshott and Macgregor (Reference Cockshott and MacGregor1958) stated was present on radiographs even when the condition was presenting unilaterally externally.”Footnote 17 In all published archaeological cases of osteomyelitis variolosa, lesions are recorded on both elbows unless only one has been preserved.Footnote 18 An additional characteristic feature of this condition is that it affects all three bones of the arm – the humerus, radius, and ulna – where the pathology often initially manifests in the proximal radius and ulna.Footnote 19
Lower limb involvement is also observed and may develop independently of the upper limb pathology.Footnote 20 In both acute and chronic stages, pathological alterations affect the joints, with chronic cases frequently exhibiting periosteal involucrum, a hallmark of persistent osteomyelitis. Osseous changes in the lower limbs include periosteal involucrum, a thickened layer of viable bone that forms in response to osteomyelitic inflammation, which has been recorded surrounding the epiphyses (the enlarged wide ends of long bones that articulate with the joints) of the tibia and fibula.Footnote 21 Skeletal lesions have also been identified in the tibiae, fibulae, and femora of individuals who died of smallpox.Footnote 22 Crawford et al. note: “The joints may also be affected, with ankle abnormalities seen in 18% of paediatric patients with bone involvement (Cockshott and MacGregor, Reference Cockshott and MacGregor1959) and 50% of adults with typical late smallpox manifestations (Tang et al., Reference Tang, Shao, Liu, Wen, Wang, Wang, Peng, Yao and Zuo2021). In adult individuals with osteomyelitis variolosa, distortion of the calcaneus (such as flattening and shortening) is a commonly reported symptom, potentially due to long-term changes in mobility and weight bearing.”Footnote 23
Pathological involvement is not confined to the long bones but also affects the small bones of the hands and feet, where destruction of the epiphyses and arrested growth can occur.Footnote 24 Initially, the involvement of these bones is characterized by inflammatory lytic lesions – areas of bone resorption that create pitted defects on the bone surface.Footnote 24 Chronic cases may result in stunted, shortened digits; these too are typically bilateral.Footnote 25
Despite the extensive skeletal manifestations of osteomyelitis variolosa, certain regions remain largely unaffected. The ribs, spine, and pelvis are not involved,Footnote 26 and cranial manifestations are rare – to date, only a single clinical case of skull involvement has been documented, occurring in an eight-year-old girl, and three cases in archaeology, including two 1.5-year-old infants from Peru, and one 12-year-old child from Alaska.Footnote 27
Individual sk847 from Cirencester
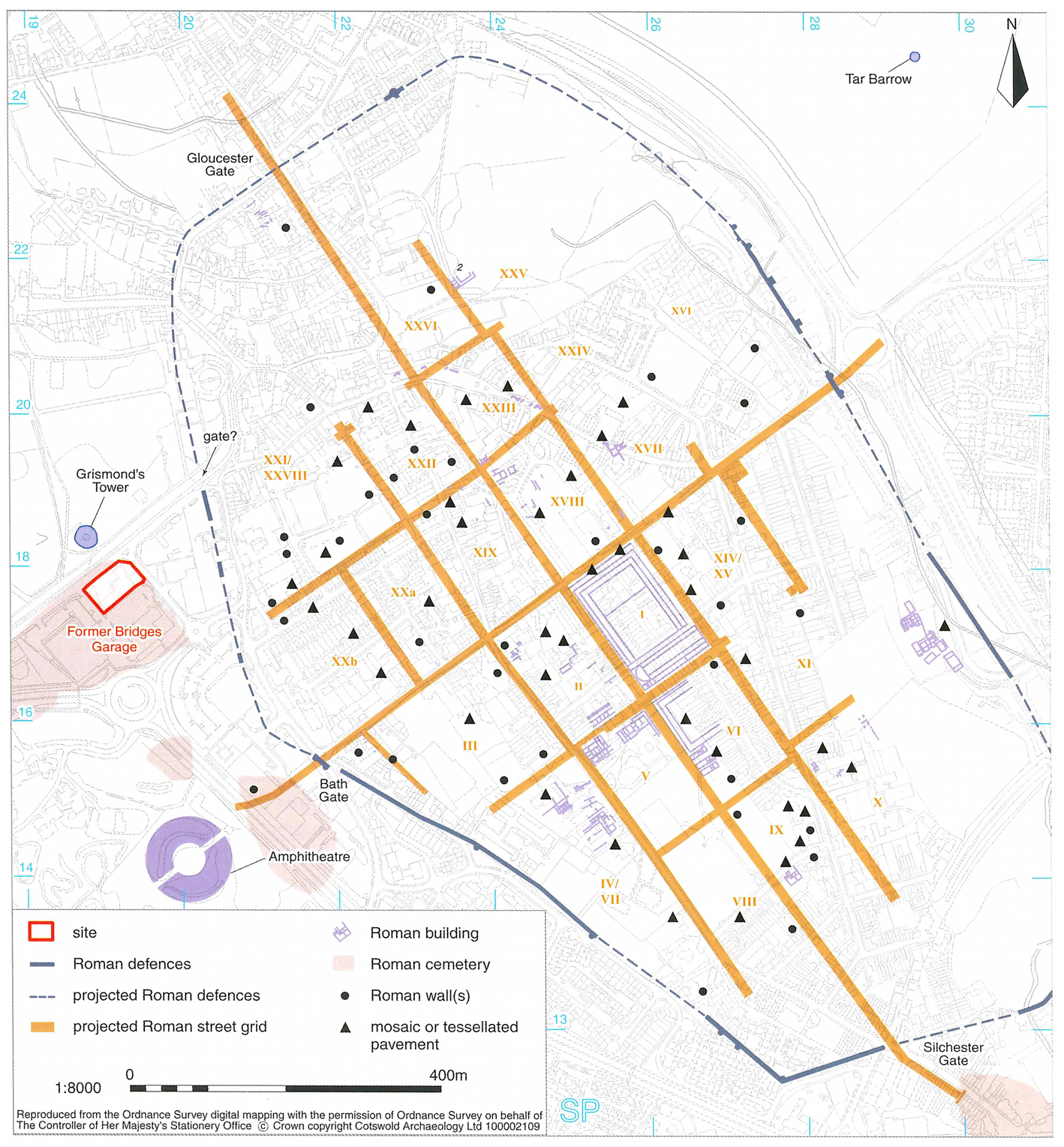
The Western Cemetery of Roman Cirencester is situated at the former site of Bridges Garage on the western edge of modern Cirencester, approximately 130 m outside the town walls of Roman Corinium (Fig. 1). Excavations conducted by Cotswold Archaeology from September 2011 to February 2015 revealed a total of 118 inhumations and 8 cremation burials. Stratigraphic analysis identified two principal phases of use: Period 1, from the late 1st to early 3rd c. CE, and Period 2, from the late 3rd to 4th c. CE, although some burials defy precise chronological assignment.Footnote 28
Plan of Roman Corinium, and the location of the Western Cemetery, at the site of the former Bridges Garage. (Holbrook et al. Reference Holbrook, Wright, McSloy and Geber2017, 2, fig. 1.1, courtesy of Cotswold Archaeology.)

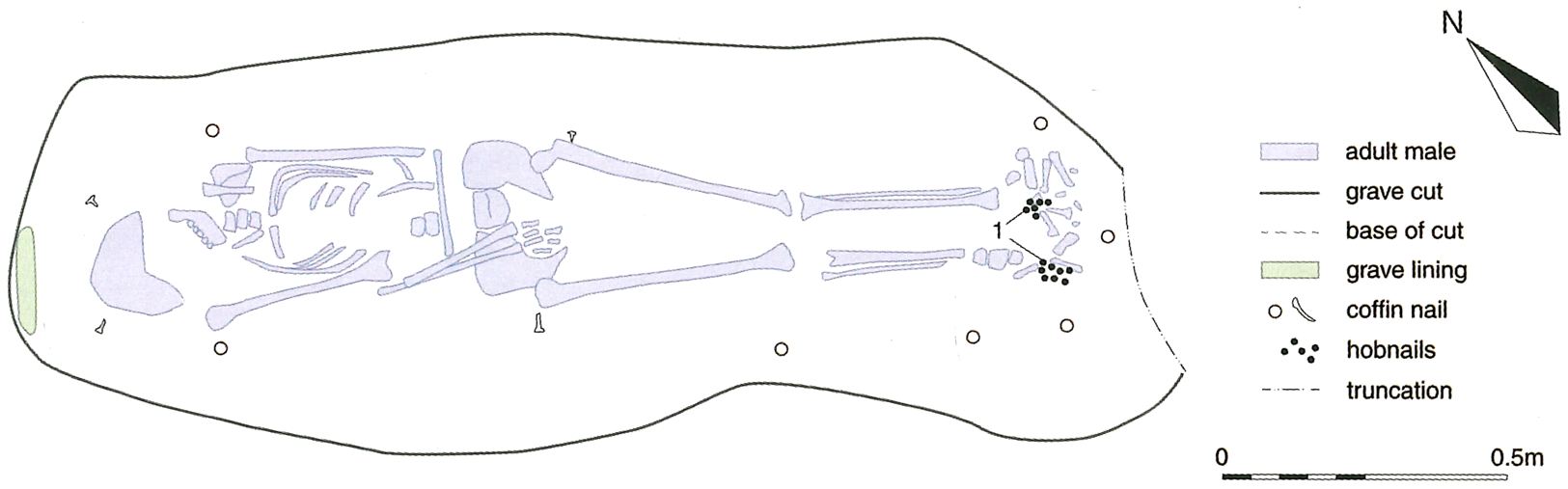
Individual B1187, catalogued as sk847 in the Corinium Museum collection, was interred in a grave designated as 848, assigned stratigraphically to Period 2. The grave is sub-rectangular, with vertical sides and a flat base. The deceased was laid supine, with the right arm draped over the pelvis and the left arm across the abdomen, the body oriented northwest to southeast (Fig. 2). Archaeological finds within the grave included 14 iron coffin nails and 85 iron hobnails, which from their position at the skeleton's feet must derive from footwear, suggesting that the deceased was buried with shoes or sandals on, and probably other clothes too.Footnote 29 Ten residual sherds of Dorset Black-burnished ware from the grave fill date from the mid-3rd to 4th c. CE.Footnote 30 The grave cut two earlier burials (B1192, whose fill contained late 3rd- to 4th-c. pottery, and B1194, undated), and its fill was cut by another burial, B1189, whose fill contained residual material from the 2nd to 4th c. CE.Footnote 31 Burial B1187 seems to date, therefore, to the later 3rd or to the 4th c. CE. Both the grave and associated finds were similar to other burials in the cemetery, and in the absence of isotopic studies, we cannot say whether this individual was born in Britain or migrated there later in life.
Plan of burial B1187 at Cirencester, showing position of the skeleton sk847 and associated artifacts. Note the flexed left arm laid across the abdomen. (Wright et al. Reference Wright, Weavill, Barber, McSloy, Geber, Holbrook, Wright, McSloy and Geber2017, 38, fig. 3.44, courtesy of Cotswold Archaeology.)

The skeleton is approximately 90% complete, with most elements at least partially preserved, and the bones are in very good condition. It is identified as a male aged between 41 and 50 years and displays a variety of lesions attributable to multiple etiologies.Footnote 32 Osteophytes (bone spurs) on the thoracic vertebrae, left-hand phalanx, right wrists, and the glenoid cavity of the right scapula probably result from advanced age and repetitive joint use throughout the individual's lifetime. The remaining lesions observed are, we argue, caused by osteomyelitis variolosa, as sequelae of a smallpox infection in childhood.
During a comprehensive survey, undertaken by the first author, of skeletal pathologies across 209 cemeteries from Roman Britain, this burial was identified as being of particular interest, given the suggestion in the excavation report by the osteologist, Jonny Geber, that the osteomyelitic infection of the left elbow joint might indicate smallpox, although he concluded that direct trauma was a more likely cause.Footnote 33 The most effective method of differentiating between the alternative hypotheses of osteomyelitis variolosa associated with smallpox and osteomyelitis as a result of direct trauma involves examining the distribution of the lesions across the skeleton, with particular emphasis on the presence of bilateral pathological changes in the elbows. Osteomyelitis variolosa frequently (but not always) presents bilaterally, especially in the elbows, while if osteomyelitic infection resulted from direct trauma one would expect it to be present in one elbow only. Permission was therefore sought and obtained from the Corinium Museum to study the bones at first hand, with the aim of resolving the question. A visit to the museum was undertaken on April 12, 2024, during which the pathology of the entire skeleton was thoroughly reassessed, with a particular emphasis on the right arm, for which less detail had been given in the excavation report.
Description of pathology
Multiple lesions and pathologies have been identified in individual sk847. Some pathologies present as degenerative changes, which are readily discernible, whereas others require more nuanced interpretation.
Lesions to be interpreted: elbows
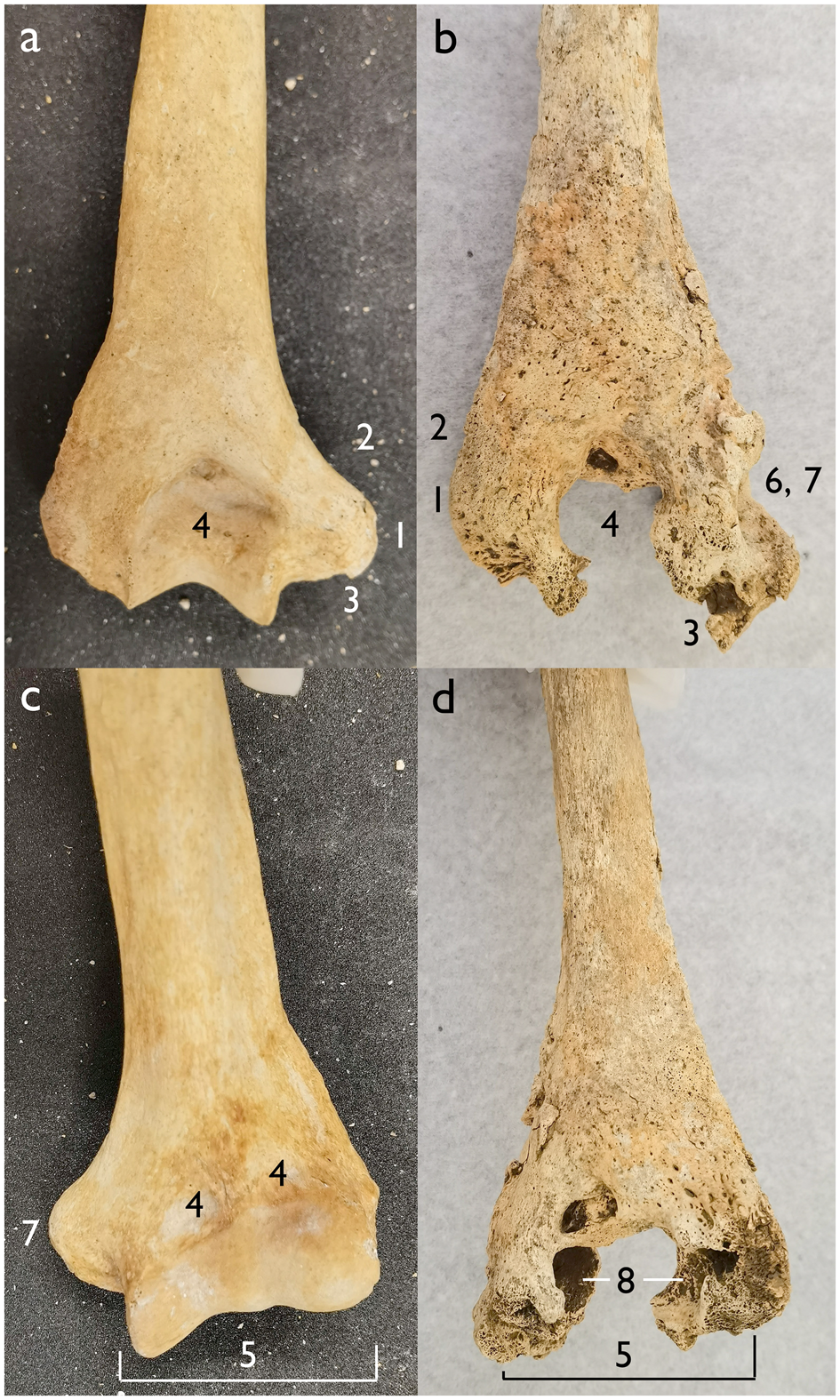
The most noticeable pathological change on this individual is the badly deformed left arm, which was carefully documented by Geber. His report is worth quoting here (we have added numbers in square brackets, referring to Figure 3 in order to illustrate the technical terminology used):Footnote 34
Severe osteomyelitic infection of the left elbow joint, resulting in a 90° flexed ankylosis. The distal humerus is displaying sclerotic porotic new bone across the entire anterior and posterior surface of the epiphysis [1] and metaphysis [2], with nodular new bone on the interosseus margin [3]. The entire fossa [4] and condyle [5] is destroyed, and a 14×11 mm large cloaca [6] is present on the medial surface of the original location of the tubercle [7], and an abscess [8] would have been present transverse across the interior of the bone onto the lateral portion of the epiphysis. Considerable damage and infection are also evident of the entire olecranonFootnote 35 of the ulna, where a more lytic appearance is observed superior of the radial head articulation and a continuation of the abscess into the olecranon. The head of the radius does also display this lytic abscess, at the medial aspect (10×14 mm) [Fig. 4d]. The full extent of the osteomyelitic abscess, positioned within the elbow joint, would have been approximately 35×35 mm. The infection may indicate smallpox.
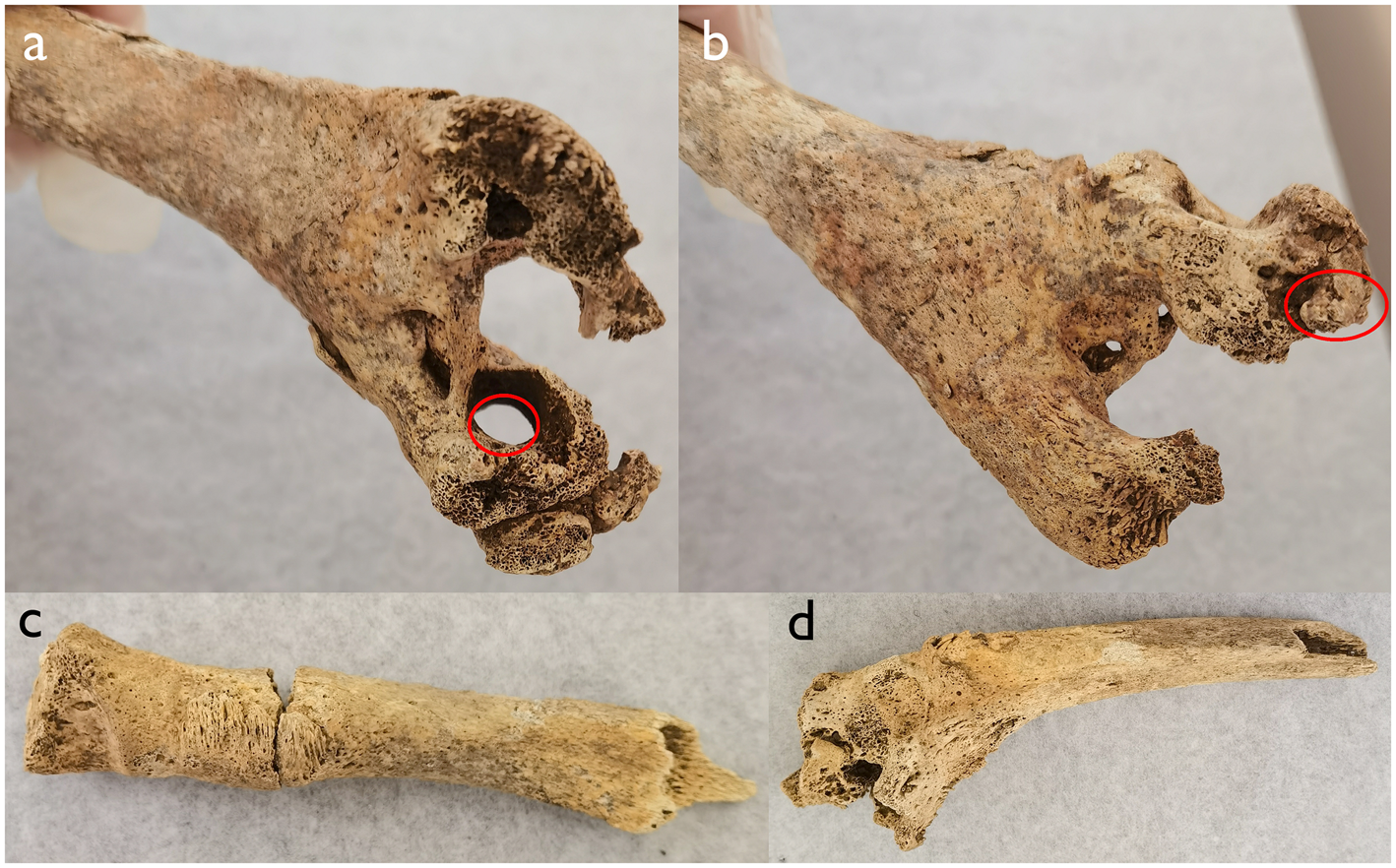
The left elbow joint thus exhibited complete destruction as a result of infection, with all three constituent bones – radius, ulna, and humerus – significantly affected (Figs. 3–4). The infection probably reached its most severe or acute stage within the marrow of the distal humerus, where the accumulation of pus started. As this accumulation of necrotic debris expanded, it compromised the structural integrity of the bone's cortex, leading to thinning of the cortex and the eventual formation of a cloaca – an opening through the cortex that facilitated the drainage of pus out of the bone (Fig. 3, no. 6; Fig. 4a). The bone damage here is also indicative of the effects typically associated with suppurative arthritis. In addition to these changes, bowing and bending of the radius and ulna are also evident (Fig. 4).
Comparison between a normal left humerus, from a male adult 1040 from the Late Roman cemetery at Little Keep, Dorchester, dated to the 4th c. CE, and the left humerus of sk847 from Cirencester. (a) Posterior view of a normal left humerus. (b) Posterior view of the left humerus of sk847. (c) Anterior view of a normal left humerus. (d) Anterior view of the left humerus of sk847. Features mentioned in Geber's description are numbered as follows: 1. Epiphysis; 2. Metaphysis; 3. Nodular new bone on the interosseus margin; 4. Fossa; 5. Condyle; 6. Cloaca; 7. Tubercle (of the medial epicondyle). 8. Bone eaten away by abscess. (Photos: H. Zhao; montage: A. Wilson.)

The left elbow bones of sk847 from Cirencester. (a) Anterior view of humerus, showing the cloaca (circled). (b) Posterior view of humerus, showing the nodular new bone on the interosseus margin (circled). (c) Anterior view of radius. (d) Anterior view of left ulna. (Photos: H. Zhao; montage: A. Wilson.)

The left elbow joint also shows woven and lamellar bone formations, representing layers of new bone superimposed upon the original structure. These indicate a chronic alteration subsequent to the initial osteomyelitic infection, which resulted in the fusion of the humerus, radius, and ulna. Such skeletal changes categorically point to chronic osteomyelitis, a condition that probably beset the individual persistently throughout their lifetime. Chronic osteomyelitis commonly ensues from unresolved bone infections after attempts at intervention.Footnote 36 Particularly in pre-modern contexts, where pus may not have been thoroughly evacuated through a significant cloaca, the condition could be perpetuated by incompletely healed openings through the skin and the bone that facilitated subsequent secondary infections.Footnote 37 The pus drained out of the bone through the cloaca in the distal humerus mentioned above would have accumulated in the overlying tissue, causing inflammation and swelling; if this swelling either burst or was deliberately lanced, the site could easily have become infected. The multiple stages of bone destruction and new bone formation represented by the woven and lamellar bones and the destructive lesions suggest that this osteomyelitic transformation would probably have manifested in intermittently active phases, corresponding with any decline in immune function over the years – a phenomenon still observed in contemporary clinical practices.Footnote 38
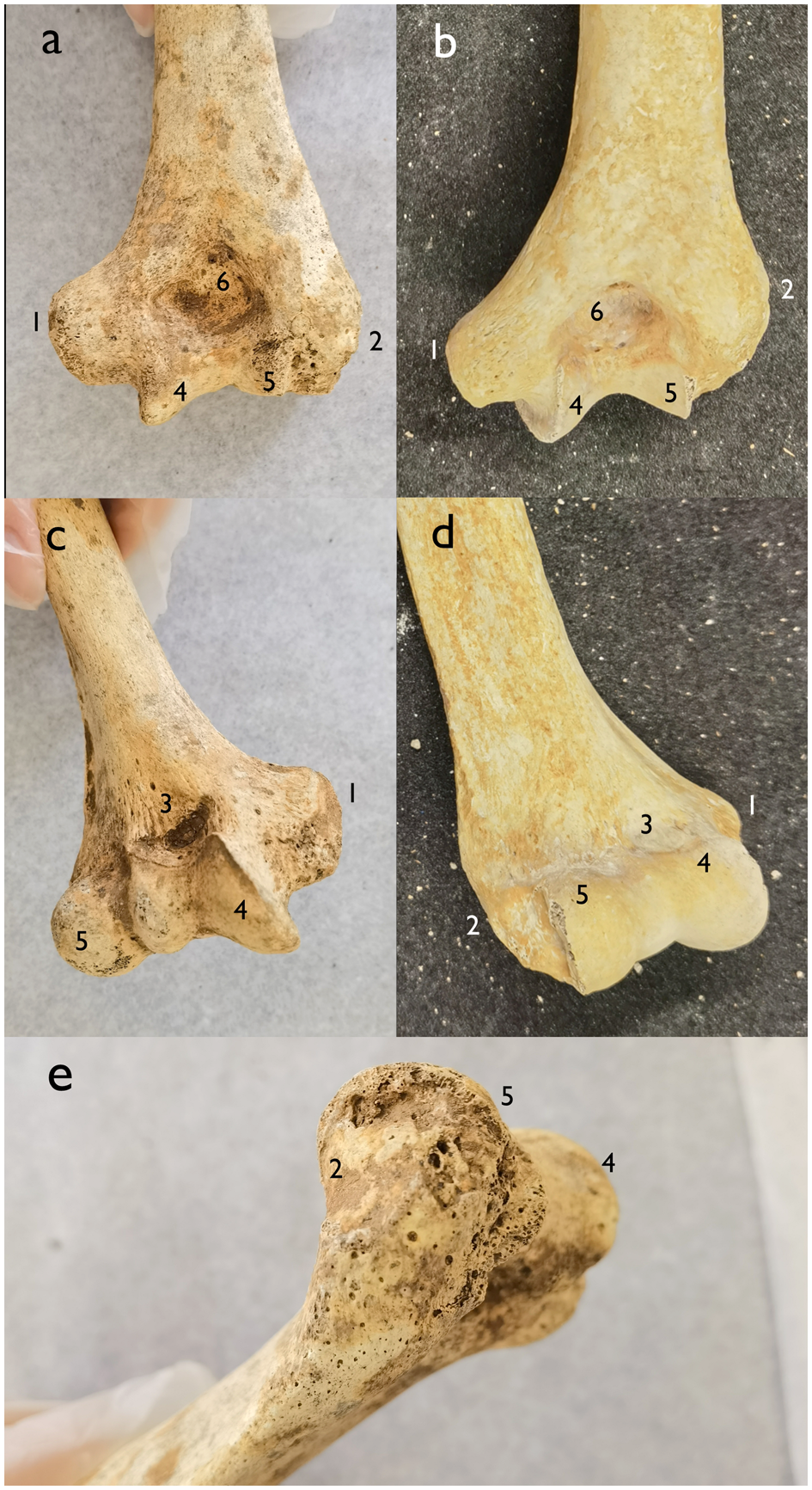
The pathology of the right elbow, which is not discussed in Geber's report, is detailed here for the first time (Figs. 5–8). Pitting and porosity are observed throughout the right distal humerus (Fig. 5), with the medial [1] and lateral [2] epicondyles being particularly affected. The distal humerus displays a bony outgrowth and thickening on the coronoid fossa [3]. The trochlea [4] is notably flattened, and the local surface of the bone appears uneven. In particular, the lateral part of the humerus, especially the lateral epicondyle, shows an area of lytic damage surrounded by porous reactive bone formation that extends approximately 32 mm towards the shaft's anterior surface near the capitulum [5]. The medial epicondyle exhibits bone growth and enlargement. The proximal side of the olecranon fossa [6] is uneven. Pathological changes on the coronoid fossa, the olecranon fossa, and the trochlea suggest degenerative changes, while the rest clearly indicate infections.
Comparison between the right humerus from sk847 and a normal humerus. (a) Posterior view of humerus of sk847. (b) Posterior view of humerus of male adult 1040 from Little Keep. (c) Anterior view of humerus of sk847. (d) Anterior view of humerus of male adult 1040 from Little Keep. (e) Lateral epicondyle of individual sk847 showing the pathological changes. Features mentioned in the text discussing the right humerus are numbered as follows: 1. Medial epicondyle; 2. Lateral epicondyle; 3. Coronoid fossa; 4. Trochlea; 5. Capitulum; 6. Olecranon fossa. (Photos: H. Zhao; montage: A. Wilson.)

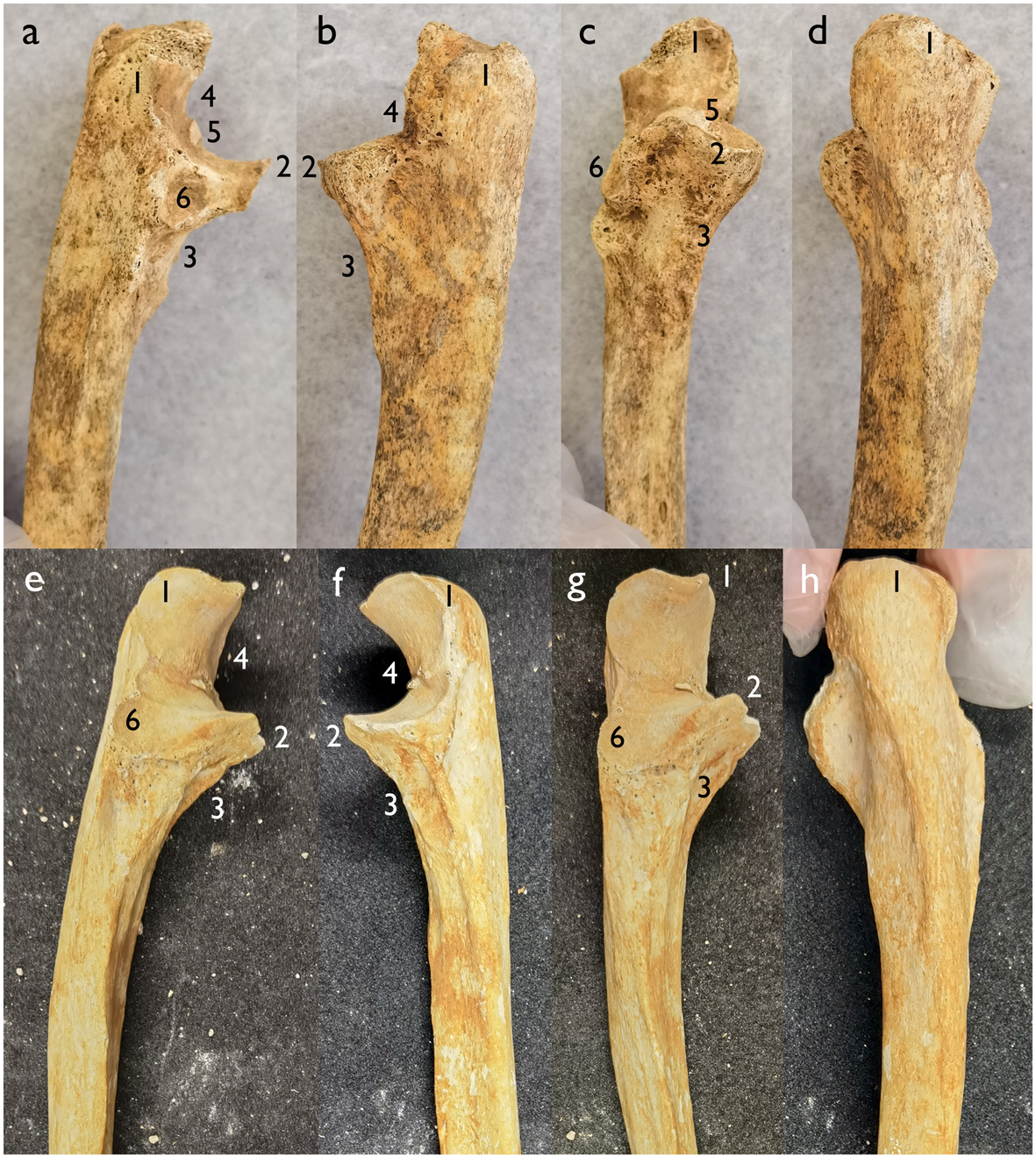
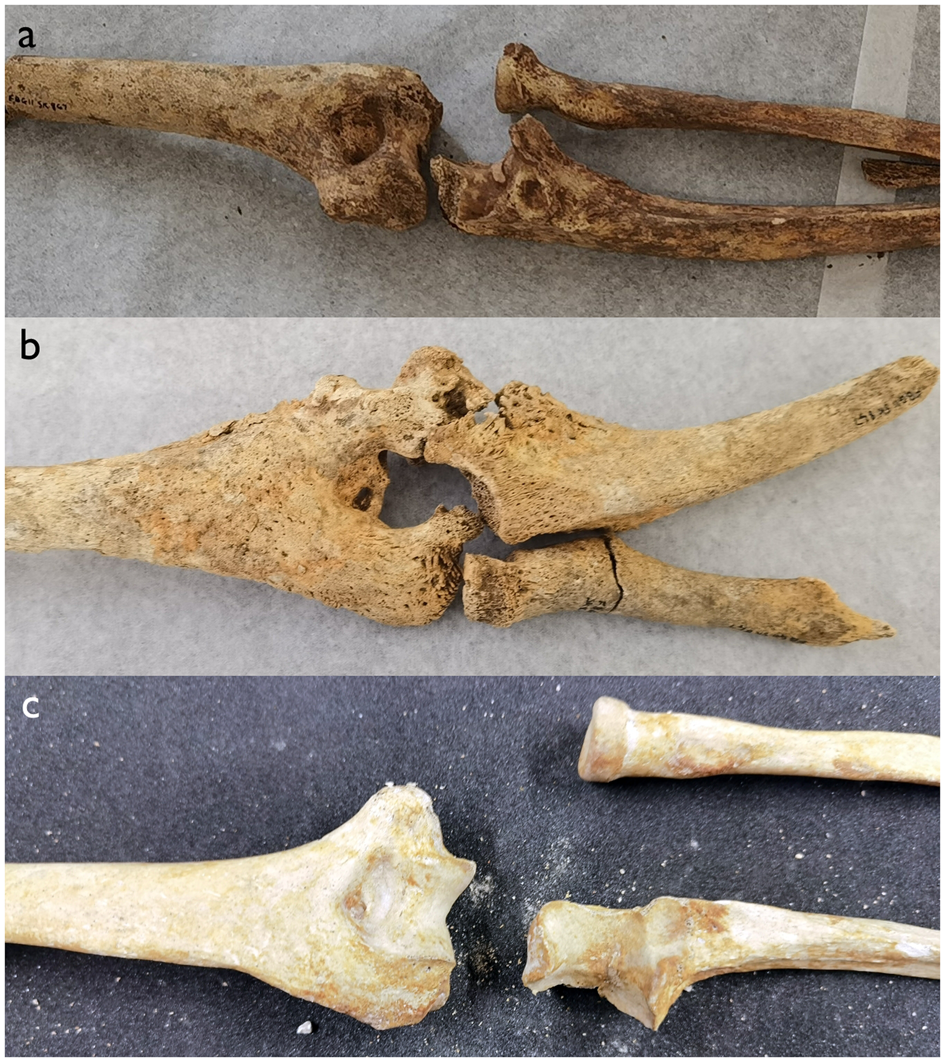
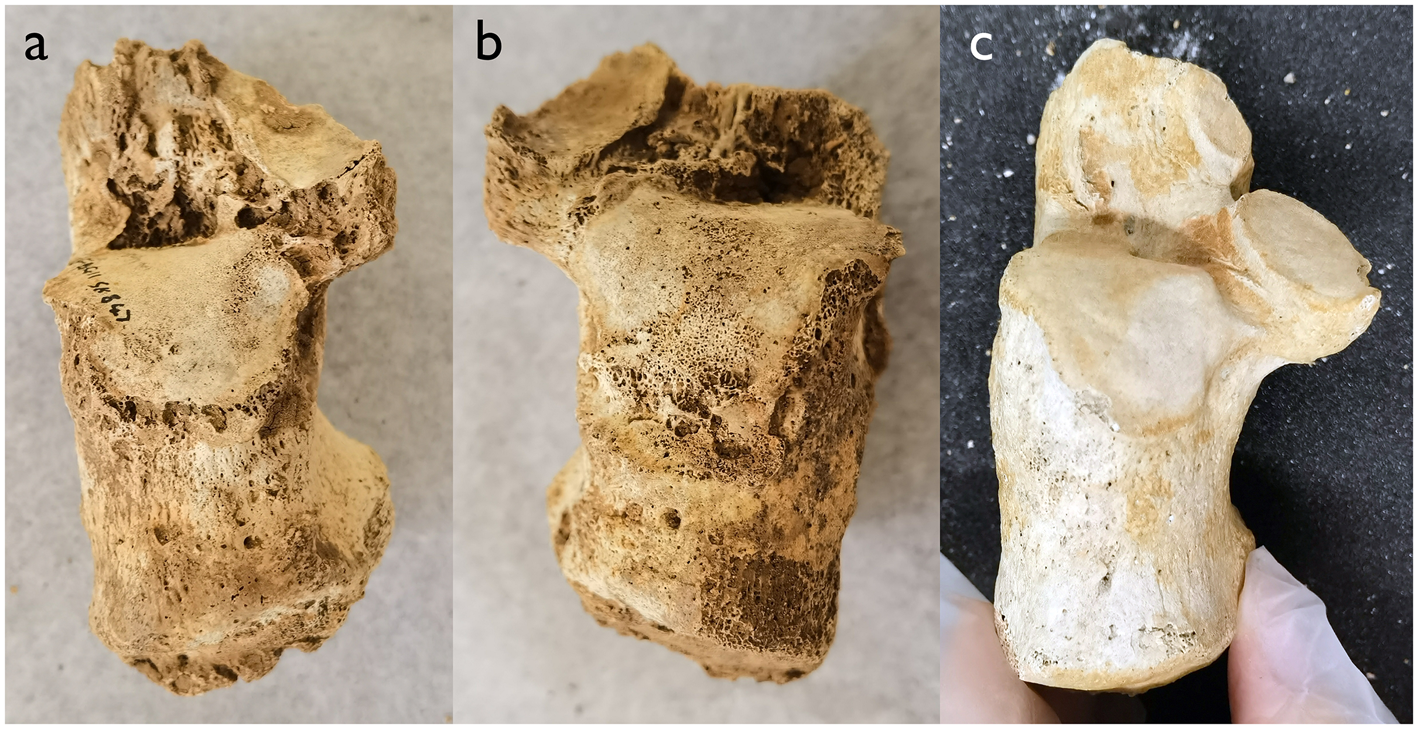
Comparison between the right ulna from sk847 and a normal right ulna. (a)–(d) Right ulna of sk847. (e)–(h) Right ulna of male adult 1040 from Little Keep. Features mentioned in the text discussing the right ulna are numbered as follows: 1. Olecranon; 2. Coronoid process; 3. Ulnar tuberosity; 4. Trochlear notch; 5. Enthesophytes; 6. Radial notch. (Photos: H. Zhao; montage: A. Wilson.)

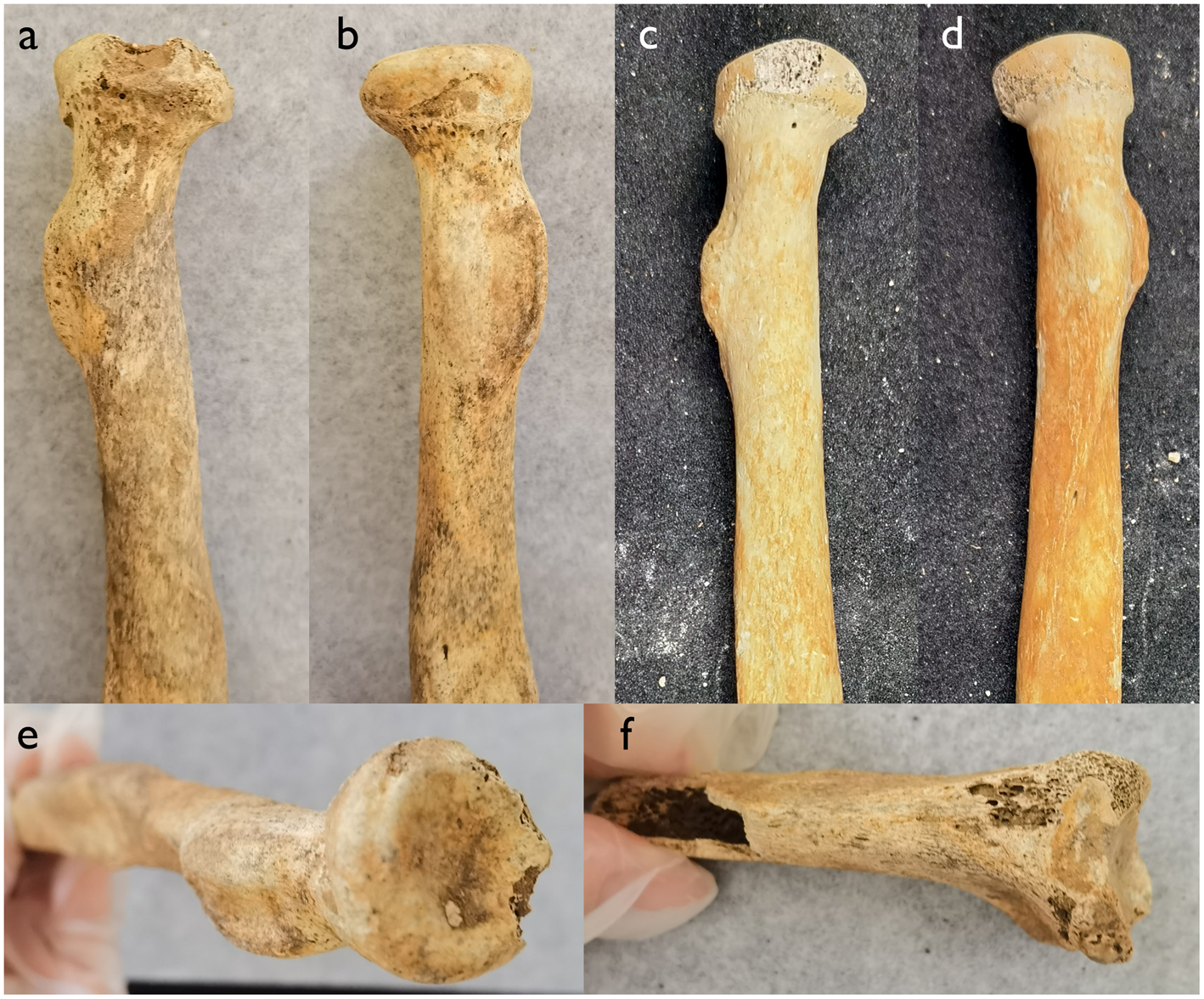
Comparison between the right radius from sk847 and a normal right radius. (a), (b) Proximal right radius of sk847. (c), (d) Proximal right radius of male adult 1040 from Little Keep. (e) Proximal right radius of sk847; (f) Distal right radius of sk847. (Photos: H. Zhao; montage: A. Wilson.)

The elbows of sk847 compared to a normal elbow. (a) Right elbow of sk847. (b) Left elbow of sk847; c) Right elbow of male adult 1040 from Little Keep. The photos aim to show pathologies on the bones, not their original positions in human bodies. (Photos: H. Zhao; montage: A. Wilson.)

The right proximal ulna exhibits notable deformation and slight bending (Fig. 6a–d). The shaft displays flecks of darker coloration attributable to periostitis, that is, non-specific infection on bones. Both the olecranon [1] and coronoid process [2] are abnormally widened and thickened. Below the coronoid process, sclerotic porotic new bone growth extends beyond the original ulnar tuberosity [3], which has been destroyed by lesions. The trochlear notch [4] is rendered shallow and uneven, with bony growths or enthesophytes [5] measuring 9 × 2 mm in the center. Around and below the radial notch [6], pronounced bone thickening is evident.
The proximal section of the right radius also shows slight bending, with pitting and porosity along the remaining radius (Fig. 7). Periostitis resulting from infection is widespread along the shaft, particularly on the lateral side. The radial head features a bony outgrowth or enthesophyte centered on the surface, approximately 1 mm in diameter. The distal end of the radius is slightly enlarged with an uneven articular surface, suggestive of degenerative changes.
The enthesophytes on the radial head and trochlear notch may be attributed to repeated use.Footnote 39 The flexed ankylosis of the left elbow, locking the joint at a 90° angle, meant that the individual would probably have become increasingly unable to use his left arm and relied heavily on the right arm, resulting in greater labor stress on the bones of that arm. The general changes in the shape of the right radius and ulna, along with the bony growth below the radial notch, may suggest a dislocation of the radius and ulna. Although dislocations are challenging to observe directly in osteology due to the disturbance of bones, similar pathological changes indicative of dislocations have been noted in other case studies.Footnote 40
In summary, the right elbow and its associated structures show significant damage and indications of infection. Following the initial infection, the individual experienced difficulties adapting to the deformed arms. Ongoing secondary alterations – attributable either to chronic osteomyelitis, as observed in the left arm, or to repetitive biomechanical stress, as noted in the right arm – persisted throughout the individual's life. Consequently, the normal architecture of the bilateral elbow joints was supplanted by deformities as time progressed, more severe on the left side than on the right (Fig. 8).
Lesions to be interpreted: feet and maxilla
Pathologies on the feet have been thoroughly documented by Geber although the distal tibiae and fibulae are badly preserved.Footnote 41 Arthropathies (joint diseases) affecting both feet exhibit degenerative changes and the formation of bony lumps, or osteophytes, on multiple articular surfaces (the calcanei are shown in Figs. 9 and 10). The left foot shows irregular marginal osteophytes along joints near the ankle and the heel, including the calcaneo-talar facets, cuboid articulation, and navicular bone.Footnote 42 Erosive lesions are found on the first metatarsal and its proximal phalanx (Fig. 11 [1, 4]).Footnote 43 The right foot displays marginal osteophytes on the talar and medial articulations of the calcaneus (the surface between two heel bones), and degenerative lesions along the articular surfaces in front of the heel, including the first cuneiform and navicular bones.Footnote 44 Additionally, erosive arthropathies affect the joint surface of the proximal phalanx of the right foot (Fig. 11 [2]).Footnote 45 An erosive lesion on the proximal side of the right first metatarsal is also evident (Fig. 11 [3]).Footnote 46
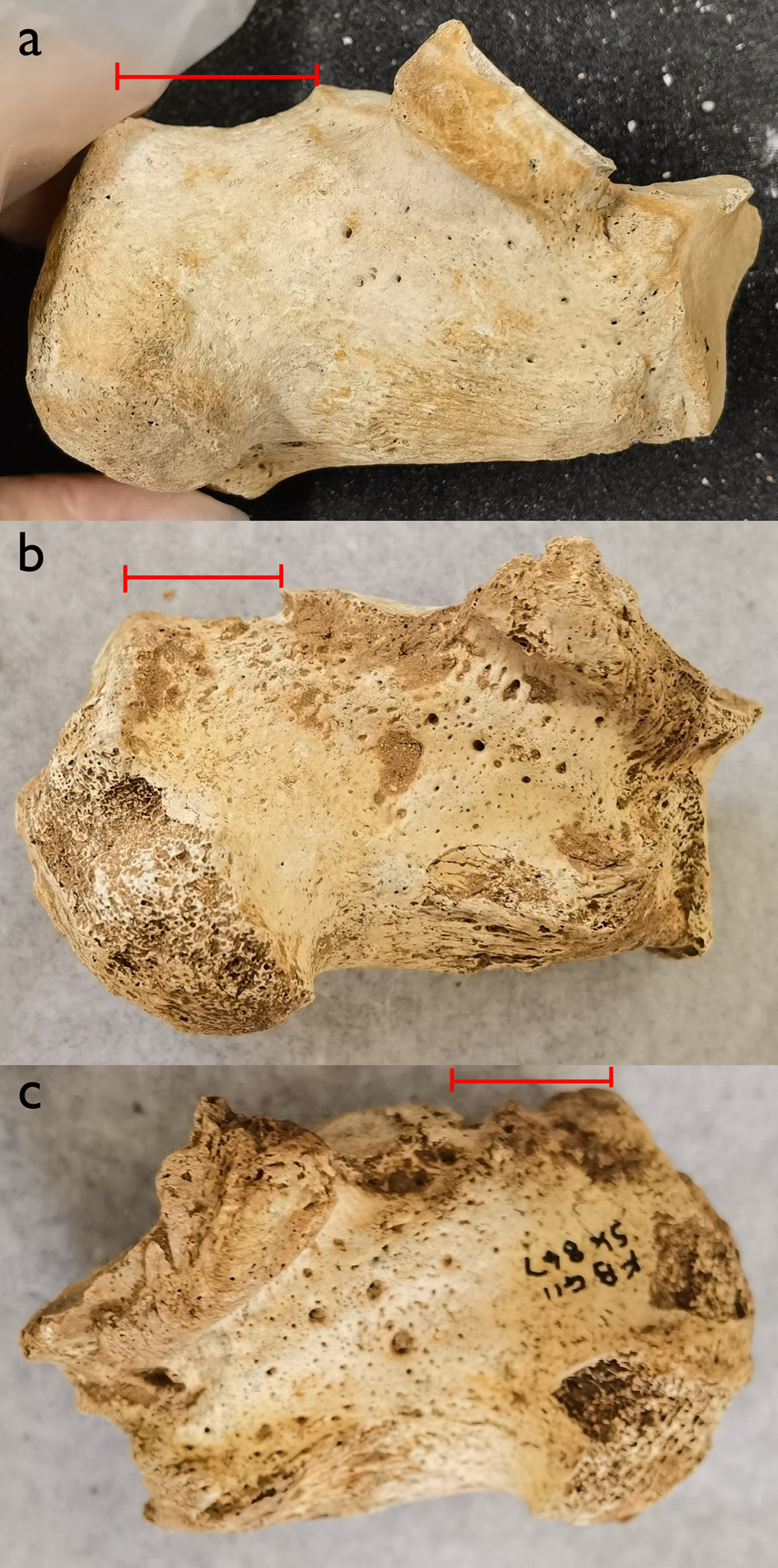
Calcanei of sk847 and a normal calcaneus. (a) Left calcaneus of sk847. (b) Right calcaneus of sk847. (c) Left calcaneus of male adult 1040 from Little Keep. (Photos: H. Zhao; montage: A. Wilson.)

Calcanei of sk847 and a normal calcaneus; the red line shows the shortening of the calcanei of individual sk847 compared to individual 1040 from Little Keep. (a) Medial view of left calcaneus of 1040 from Little Keep. (b) Medial view of left calcaneus of individual sk847. (c) Medial view of right calcaneus of individual sk847. (Photos: H. Zhao; montage: A. Wilson.)

First proximal phalanges and first metatarsals of individual sk847. (a) Left first proximal phalanx. (b) Right first proximal phalanx. (c) Left first metatarsal (top view). (d) Right first metatarsal (top view). (e) Left first metatarsal (bottom view). (f) Right first metatarsal (bottom view). Features mentioned in the text discussing the feet are numbered as follows: 1. Erosive lesion on left first proximal phalanx; 2. Erosive lesion on right first proximal phalanx; 3. Erosive lesion on right first metatarsal; 4. Possible erosive lesion on left first metatarsal. (Photos: H. Zhao; montage: A. Wilson.)

Although Geber categorizes the pathologies observed on both feet mostly as “degenerative changes”,Footnote 47 the evidence suggests a more complex condition, particularly affecting the calcanei, tali, first metatarsals, and their proximal phalanges. The presence of erosive lesions and extensive bone destruction transcends typical degenerative changes. In particular, both calcanei exhibit significant deformation and shortening relative to normal specimens (Fig. 10). Moreover, the subtalar joint is an uncommon site for the development of osteoarthritis, probably because of the greater thickness of its articular cartilage and different metabolic activities compared to other joints.Footnote 48 Attributing the foot lesions solely to degenerative changes therefore seems inadequate.
The dense sclerosis observed in the right maxillary sinus of SK847, which Geber attributes to maxillary sinusitis,Footnote 49 may either be linked to the same pathological process affecting the elbows and feet or represent a co-morbidity (discussed below in the section in differential diagnosis).
Degenerative changes
Degenerative alterations are predominantly observed in the spine, wrist, shoulder, and thigh – details meticulously documented by Geber. Notably, osteophytes are present on the right shoulder (the glenoid cavity of the right scapula), the right wrist (along the articular surfaces of the scaphoid, lunate, and capitate), and at vertebrae T7–8 in the spine.Footnote 50 These are probably associated with repetitive movement and labor during the individual's lifetime. The ossification of the ligamentum flavum (ligament in spine) in vertebrae T4 to T10 may be explained by mechanical stress.Footnote 51 In particular, the abnormalities on the right scapula and right wrist may be explicable by the individual having had to rely increasingly on the right arm as the left elbow was inflamed and swollen and the joint ankylosed at a 90° angle. Possibly this asymmetrical reliance on the right arm, coupled with the effects on his gait of the degradation of his heel bones, may also have created stresses on his spine that could explain the pathology on the vertebrae too.
Additionally, an active patch of periosteal new bone formation was observed on the medial surface of the neck of the left femur, near the lesser trochanter, where the psoas major and iliacus muscles attach to the thighbone.Footnote 52 This strongly suggests that it resulted from atypical muscle use during the individual's lifetime, lameness caused by the observed damage to the feet, rather than directly from infectious disease.
Differential diagnosis
This individual exhibits alterations in multiple joints, with the most severe manifestations observed in the elbows, and the talo-calcaneal and metatarso-phalangeal joints in the feet. Although these lesions are not perfectly symmetrical, they tend to be bilateral. Evidence of infection is clear, particularly in the suppurative arthritis observed in the left elbow and the widespread periostitis in the right elbow. The erosive lesions on the feet may also have resulted from infection. Following these infections, secondary chronic changes are evident, including chronic osteomyelitis in the left elbow and enthesophytes in the right ulna and radius.
The systemic and bilateral nature of the joint afflictions across the body from elbows to feet makes the interpretation of the pathologies exhibited by individual sk847 challenging, as a few known diseases affect the joints in such a manner. Consequently, differential diagnosis is crucial to ascertain the most plausible explanation for these pathologies (Table 2).
Differential diagnosis of observed pathologies.

The hypothesis that trauma could account for the osteomyelitic changes observed in the left elbow joint of individual sk847 is now considered unlikely. The simultaneous occurrence of severe infections in both elbows and both feet without any accompanying fractures diminishes the plausibility of trauma-induced pathology. The lesions evident on individual sk847, including bilateral (though not symmetrical) lytic lesions on both elbows, more aptly correspond with typical smallpox sequelae, offering a comprehensive explanation for the observed abnormalities across the elbows and feet.
Potential alternative diagnoses include tuberculosis, leprosy, treponematosis (syphilis, yaws, bejel, and pinta), rheumatoid arthritis, mycosis, degenerative arthritis, and septic arthritis (Table 2).Footnote 53 Tuberculosis, mycosis, and septic arthritis represent infections that typically exhibit non-systemic characteristics. Tuberculosis manifests osteologically primarily through extensive bone destruction, as opposed to the bone growth or deformation observed in the case under examination. While mycosis and septic arthritis exhibit certain similarities with the presented case, their pathologies are not congruent with simultaneous afflictions of both the elbow and the feet.
Conversely, diseases such as treponematosis, leprosy, and rheumatoid arthritis are more frequently associated with the involvement of multiple joints. None of these conditions, however, can adequately account for the lesions observed in our case. Both treponematosis and leprosy typically commence with the cranium or facial bones, exhibiting destructive lesions such as caries sicca in treponematosis or extensive bone remodeling in leprosy. The sole pathology in the skull observed in our case is the dense sclerosis in the right maxillary sinus, which does not correspond with the typical manifestations of treponematosis or leprosy. Rheumatoid arthritis predominantly affects smaller joints such as those in the fingers, characterized by greater destruction and eburnation of the articulating surfaces rather than bone proliferation. Additionally, as an autoimmune disorder, rheumatoid arthritis fails to account for the infectious markers (periostitis) noted on the elbows.
Some traits possibly suggestive of degenerative joint disease are present in specific regions of the right elbow. These must be distinguished, however, from changes observed along the entirety of the affected area. The lesions extending along the shafts of the bones, distinct from the joint surfaces where degenerative changes typically manifest, cannot be reconciled with any known patterns of degenerative joint disease. Such extensive periostitis across all three bones, humerus, radius, and ulna, predominantly indicates an infectious etiology rather than degenerative alterations. Moreover, the extensive periostitis on all three bones is suggestive of infection, not degenerative changes.
Considering the locations of the lesions and their skeletal representations, osteomyelitis variolosa appears to be the most fitting diagnosis for all observed pathologies. The bilateral involvement of both elbows, including all three arm bones (humerus, radius, and ulna) with initial prominence in the proximal radius and ulna, aligns with known patterns of osteomyelitis variolosa.Footnote 54 Ankles and feet, which are also commonly affected sites, account for 18% of the diagnosed patients in the 19th–early 20th c.,Footnote 55 or 50% in clinical reports in the 21st c.Footnote 56 The distribution of lesions in cases of modern smallpox thus correlates with the lesions observed on the individual studied.
Given the rarity of osteomyelitis variolosa in both archaeological findings and modern clinical practice, it is important to compare the lesions of individual sk847 with other identified cases in the modern clinical literature to ensure the accuracy of the diagnosis.
Identification of osteomyelitis variolosa and lesion comparison
During 20th-c. smallpox epidemics, approximately 0.25–0.5% of all patients and 2–5% of affected children exhibited osteoarticular manifestations.Footnote 57 This suggests that osteomyelitis variolosa developed during the childhood of the individual in question. The majority of archaeologically identified cases of osteomyelitis variolosa in Table 1 involve children or juveniles, with only two older adults noted (Table 1, nos. 4 and 5), and just one report (Table 1, no. 4) providing photographic evidence of affected elbows. This underscores the importance of using modern medical records to enhance the diagnostic accuracy in archaeological cases where osteomyelitis variolosa is suspected in adult skeletons.
In contrast to juveniles and younger adults, older adults who have survived a smallpox attack often present with skeletal deformities and joint pain (arthralgia), attributable to superimposed degenerative changes.Footnote 58 Modern clinical reports corroborate this pattern; many patients experience severe pain and increasingly restricted movement in the joints affected by osteomyelitis variolosa decades after the initial infection. A notable case reported by Tang et al. involved a 70-year-old woman who, although infected in her childhood, began experiencing exacerbated limited movement and pain in her knees only a year prior to the report.Footnote 59 Another diagnosis of osteomyelitis variolosa also concerned a woman who was 70 years old at the time of presentation, who had experienced pain in her right knee for five years.Footnote 60 A case reported by Purandarnath and Douraiswami describes a 65-year-old woman who had endured pain and stiffness in both elbows and in joints of her feet for 30 years.Footnote 61 All three women had had smallpox in childhood. These clinical observations underscore the fact that while osteomyelitis variolosa is initially an acute infection of the bone, it continues to evolve into secondary arthritis and degenerative changes over decades. This progression is also evident in the case under discussion, where both infection and degenerative changes coexist. To refine the diagnosis of osteomyelitis variolosa, a comparative analysis with similarly diagnosed older adults is recommended, enhancing the accuracy of differential diagnoses and underscoring the chronic nature of the disease's impact on skeletal health.
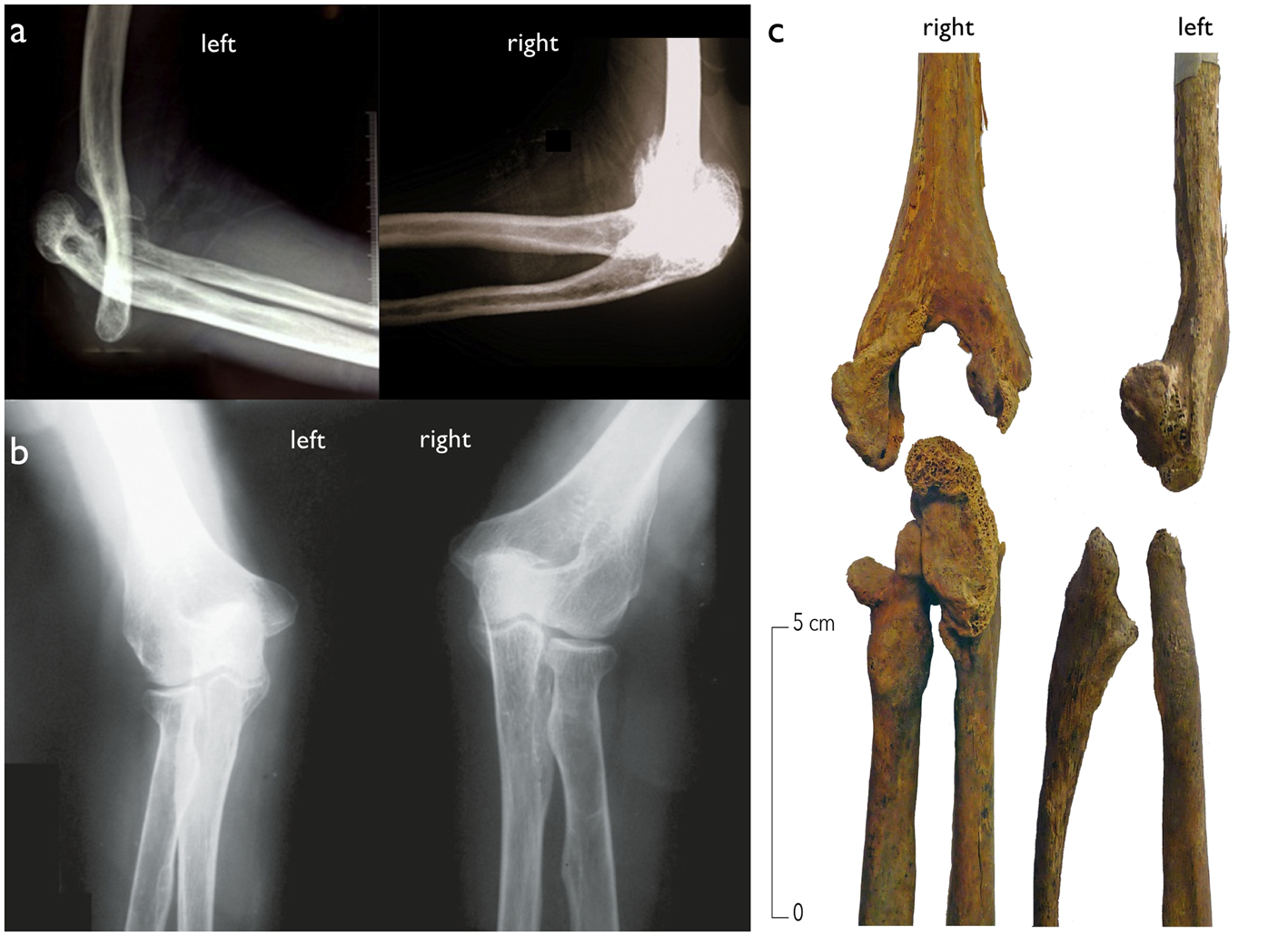
Comparative analysis of elbow and ankle lesions, as depicted in Figs. 12 and 13, provides further insight. Notably, bilateral changes in osteomyelitis variolosa do not always manifest symmetrically, and asymmetrical changes in the elbows have been documented in several cases identified in the 21st c. (Fig. 12).Footnote 62 This observation is particularly significant given that only 11 cases of osteomyelitis variolosa have been reported in the 21st c.Footnote 63 This asymmetry aligns with the unpredictable nature of infectious diseases; for example, periostitis caused by bacterial infection may vary in severity across affected sites in the body.Footnote 64 Historical data support this observation of asymmetry. According to Cockshott and MacGregor,Footnote 65 among 124 cases, 97 exhibited elbow involvement, with 19 exclusively unilateral, indicating a significant probability (approximately 20%) of asymmetrical manifestations among those affected. This variability in lesion symmetry is also evidenced by the skeletal findings illustrated in Figure 12.
Comparison of elbows affected bilaterally by osteomyelitis variolosa. (a) Radiograph of elbows of a 56-year-old man (Khurana et al. Reference Khurana, Vardhan and Negi2019, figs. 3 and 4, details). (b) Radiograph of elbows of a 65-year-old woman (Purandarnath and Douraiswami Reference Purandarnath and Douraiswami2011, fig. 4). (c) Photograph of the elbow bones of a medieval or early modern skeleton identified as of a woman aged between 20 and 49, from the convent of the Jacobins at Rennes, France (Colleter Reference Colleter2021, fig. 2, detail, courtesy of R. Colleter).

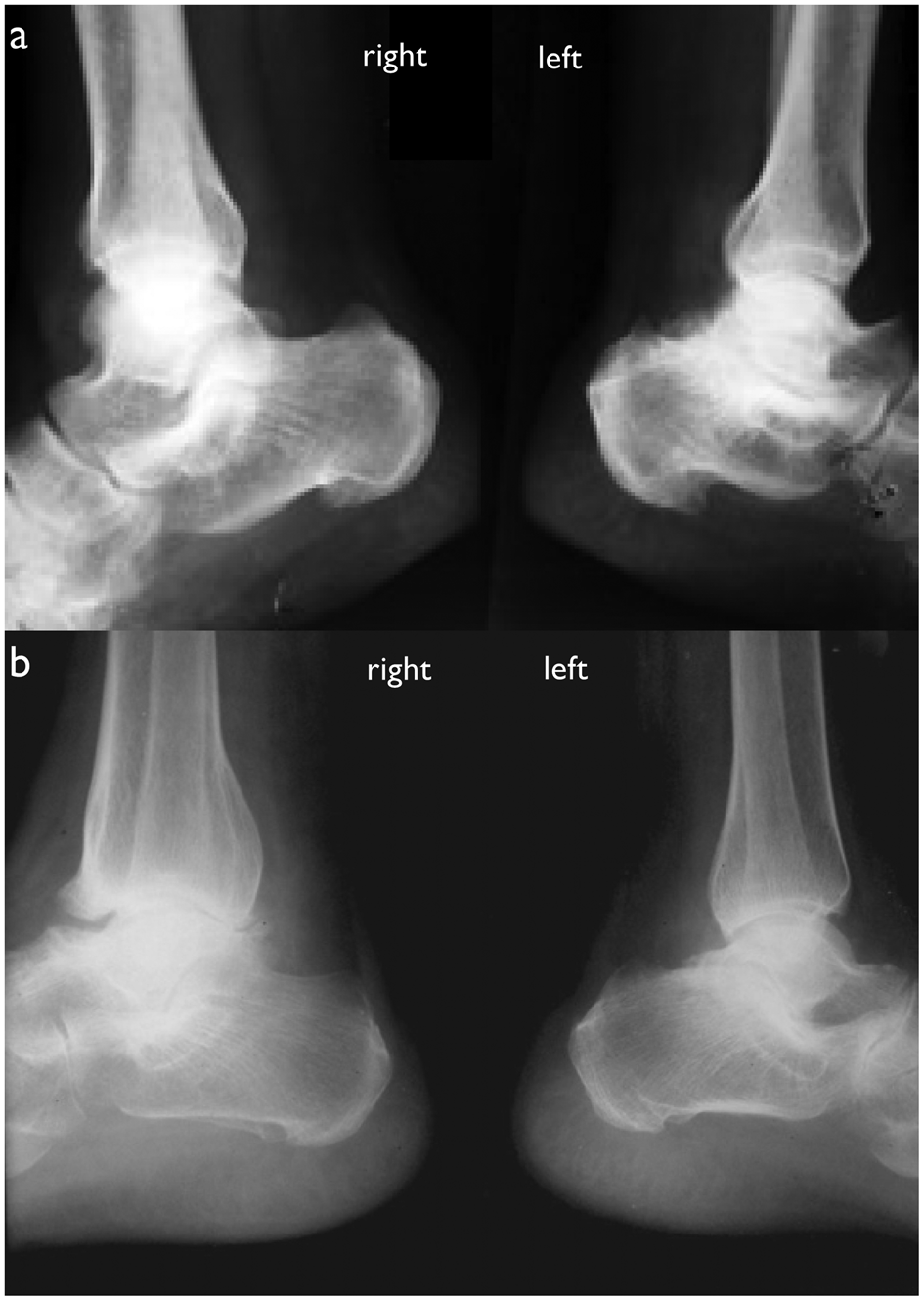
Comparison of ankles affected bilaterally by osteomyelitis variolosa. (a) Radiograph of feet of a 64-year-old man, with the left foot more severely affected, showing shortening of the left calcaneum (Arora et al. Reference Arora, Agarwal and Kumar2008). (b) Radiograph of feet of a 65-year-old woman (Purandarnath and Douraiswami Reference Purandarnath and Douraiswami2011, figs. 2 and 3, details).

Margolis et al. and Tang et al. have concluded that the pathological changes in residual osteoarticular lesions of smallpox are non-specific and that no diagnostic radiographic image exists for osteomyelitis variolosa.Footnote 66 This variability in pathological representation should therefore be considered a characteristic trait of osteomyelitis variolosa.
The comparative analysis of the elbow lesions in individual sk847 reveals that the right elbow aligns closely with the radiograph of a diagnosed case of osteomyelitis variolosa shown in Figure 12b, where the pathological changes on the elbows are nonsuppurative. The left elbow of sk847 is more severely destroyed than the examples in Figure 12, as a result of suppurative arthritis. It is widely recognized that smallpox can lead to pyogenic, or suppurative, arthritis, although this complication has become less frequent after the 20th c.Footnote 67 Given these observations, we can confidently assert that the lesions on both elbows in individual sk847 may be attributed to smallpox and its chronic sequelae.
Regarding the foot lesions, there is a close degree of congruence with known cases (Figs. 9, 10, and 13). Distortions of the calcaneus, such as flattening and shortening, are commonly reported symptoms in adults with osteomyelitis variolosa due to long-term changes in mobility and weight-bearing.Footnote 68 The case of individual sk847 exhibits bilateral shortening of the calcanei, resembling the findings reported in Arora et al., although in their report the alteration was unilateral.Footnote 69 Additionally, although not fully ankylosed, the tarsal bones, first metatarsals, and first proximal phalanges in individual sk847 show severe deformities. These findings closely parallel those reported in Nema et al.Footnote 70
The dense sclerosis observed in the right maxillary sinus of sk847, which Geber suggested was caused by maxillary sinusitis,Footnote 71 may also perhaps be attributable to smallpox, although other explanations are possible too. Cockshott and MacGregor described a case involving an 8-year-old girl where “the lateral wall and the floor of the right antrum showed much bony thickening in the radiograph.”Footnote 72 Although no radiograph was published, the description closely aligns with the pathology observed in sk847, which exhibits similar dense sclerosis across the entire floor and lateral wall of the right maxillary sinus (also called “maxillary antrum”). In the absence of preserved soft tissue, however, we cannot determine whether this lesion was a result of smallpox or an independent episode of maxillary sinusitis.
The collective findings from the differential diagnosis and comparison with known cases strongly support the hypothesis that osteomyelitis variolosa is the most probable cause for the observed lesions on individual sk847's elbows and feet. While it is possible to find separate explanations for each individual lesion, the holistic explanation provided by osteomyelitis variolosa, encompassing all observed symptoms, presents the most coherent and likely diagnosis.
The corollary is that individual sk847 was a survivor of an earlier smallpox infection. This person died in the late 3rd or the 4th c. CE at the age of between 40 and 50, having contracted smallpox almost certainly in childhood, some 25–50 years previously. The bone involvement began acutely as suppurative osteomyelitis in the tubular bones,Footnote 73 notably leading to the destruction of the left elbow through the formation of pus. The initial alteration in joint structures probably commenced at the elbows, with subsequent involvement of the feet and maxilla occurring within 1–2 days.Footnote 74 The progression to nonsuppurative arthritis, occurring within 1–4 weeks of the onset, then severely compromised both bone growth and joint function at these sites.Footnote 75 Throughout this pathological progression, individual sk847 would have experienced significant pain and swelling around the affected joints, endured prolonged periods of low fever, and suffered from increasingly restricted joint mobility.Footnote 76 The left arm became virtually unusable, with loss of movement and the joint locked in a 90° angle; there would probably also have been some loss of movement and function in the right arm. Later, in adulthood, the individual experienced chronic complications surrounding all the previously infected joints. The acute infection in the left elbow transitioned to a chronic state, marked by cycles of new bone formation and repair during periods when the individual was stronger and healthier, and exacerbations of the infection during times of weakened health. Concurrently, degenerative changes intensified in the right elbow and feet, exacerbated by the underlying deformities. The damage to both feet, including heels and toes, caused deformities and the individual would certainly have had difficulty walking. The immobility of his flexed left elbow meant that when he was laid out for burial in his coffin, the left forearm had to be laid over his abdomen.
Genetic evolution of smallpox and historical implications
Genetic evolution of smallpox
Osteomyelitis variolosa, a specific skeletal manifestation of smallpox, is directly linked to infection by the variola virus (VARV), the causative agent of smallpox. The antiquity of smallpox as a human-specific disease is a matter of current debate, and the Cirencester skeleton bears on this debate.
Variola virus is one of several related poxviridae which have evolved from a common ancestor, a more generalized orthopoxvirus, to target specific species: its closest relatives are camelpox, affecting camels, and taterapox, affecting gerbils. Cowpox, monkeypox, and vaccinia virus affect several host species with different degrees of severity.Footnote 77 There is no agreement about when an ancestral strain of VARV diverged from a more general orthopoxvirus, capable of infecting various species, to become a human-specific variola virus causing smallpox.
Ancient DNA studies have identified two extinct clades of variola virus. One is known as modern VARV (mVARV), which can be traced back at least to a 17th-c. CE ancestor of strains of the modern smallpox declared eradicated in 1980. The other clade is known as ancient VARV (aVARV), and has been found in Viking-age or earlier burials dating between the 7th and 11th c. CE, but seems to have become extinct thereafter; it is a sister clade, not a direct ancestor, of mVARV.Footnote 78 The modern smallpox of the mVARV clade that was eradicated in the 1970s existed in two strains – variola major, with case fatality rates of 20–30%, and variola minor or alastrim, with far lower case fatality rates, of 1–5%. The aVARV clade is more distantly related, and its symptoms and case fatality rates are unknown, leading Timothy Newfield et al. to deny that it was smallpox at all, and to argue that we only know that the mVARV clade is capable of instigating smallpox.Footnote 79 As Monica Green has put it, such “reductive nominalism” is unhelpful, and there are actually indications that the symptomatology of variola virus in the Middle Ages shared a number of key elements with modern smallpox. These indications include a discussion of judarī (the Arabic word for smallpox used up to the 1970s) by the Persian medical author Rhazes, writing in 10th-c. Baghdad, which mentions excruciating pain in the limbs (from the bone infection), and facial scarring caused by judarī mentioned in 11th-c. Arabic poetry from Sicily.Footnote 80 Given the trading connections between Viking Scandinavia and the medieval Arab world, the medieval smallpox these sources describe could well be closely related to the aVARV in Viking burials. Medieval skeletons exhibiting osteomyelitis variolosa, from 10th-c. Cambridgeshire and 11th-c. France (Table 1, nos. 1 and 2), also confirm that a version of VARV circulating at the time caused pathological sequelae like those of modern smallpox.
The interpretation of the VARV genetic data is contentious. Three separate issues are at stake, two chronological and one of disease identification. The first is that widely varying dates have been calculated by different research groups for the time to most recent common ancestor. These disparities were apparently caused by variations in methods of molecular clock calculation, or the parameters and modelling assumptions used. The most recent common ancestor of the ancient and modern VARV clades was calculated by Barbara Mühlemann et al. in Reference Mühlemann, Vinner, Margaryan, Wilhelmson, de la Fuente Castro, Allentoft, de Barros Damgaard, Hansen, Nielsen, Strand, Bill, Buzhilova, Pushkina, Falys, Khartanovich, Moiseyev, Jørkov, Sørensen, Magnusson, Gustin, Schroeder, Sutter, Smith, Drosten, Fouchier, Smith, Willerslev, Jones and Sikora2020 to have existed between 2,200 and 1,400 years ago (at 95% confidence), meaning that aVARV and mVARV diverged from each other after that; that is, sometime between around 200 BCE and 600 CE.Footnote 81 A more recent study, by Igor Babkin et al. in 2022, narrows that range somewhat to between ca. 160 CE and 500 CE.Footnote 82
Babkin et al. calculated that the emergence of VARV from a generalized orthopoxvirus occurred not very long before that, between 13 and 494 CE (95% highest priority density interval).Footnote 83 In 2023, however, Diego Forni et al. calculated a radically different and much older set of results. They factored into their molecular clock analyses a new model that posits a power-law decay in the rate of change over time, based on observations that the longer the period of observation, the slower the apparent overall rate of change in viral evolution – the so-called time-dependent rate phenomenon.Footnote 84 Forni et al. calculated that the VARV lineage diverged from an orthopoxvirus between about 8,000 and 4,000 years ago, and that aVARV and mVARV diverged from a common ancestor between 3,790 and 4,351 years ago (95% highest priority density interval), that is, 2329–1768 BCE,Footnote 85 suggesting the existence of human-infecting smallpox after this period. All three of these different studies use radiocarbon dates that fail to account for the marine reservoir effect, which makes radiocarbon dates appear older than they should be. The earliest date for an archaeological aVARV specimen is from a Sámi burial at Lødingen in Norway, radiocarbon dated to between 603 and 653 cal. CE at two standard deviations (95.4% confidence), but uncorrected for marine reservoir effects, which may mean that the burial could be several hundred years younger.Footnote 86
The studies of Mühlemann et al. and Babkin et al. allow for the emergence of smallpox in the Roman era (after 200 BCE or after 160 CE, on their different calculations), while Forni et al.'s study requires that it emerged well before the Roman period. Distinctive skin lesions, which may possibly be from smallpox, have been observed on Egyptian mummies dating from between 1580 BCE and 1100 BCE,Footnote 87 and this would be consistent with Forni et al.'s dating, but no aDNA studies have been undertaken on these mummies, and the suggestion that they might exhibit smallpox remains speculative. But Forni et al.'s method does not account for the likelihood that during a pandemic, or even during large epidemics, the mutation rate may increase because the viral population has grown by orders of magnitude, and so there is a statistical likelihood of more mutations. (We have seen this recently with the very rapid mutation rates of Covid-19 between 2020 and 2022.) If the early evolution of smallpox from a generalized orthopox virus infecting multiple host species to a human-obligate pathogen involved a zoonosis and subsequent pandemic as a new disease rampaged through immunologically naïve populations,Footnote 88 we might expect a very high initial rate of change, rather than a consistent power-law decay rate. The effect would be that the time to most recent common ancestor might be not nearly as long as Forni et al. estimate.
The second problem is the tendency of some authors to focus on the midpoint of the date range calculated for the emergence of a particular clade and to draw over-precise conclusions from that. Thus Mühlemann et al. reported their calculation of the time to most recent common ancestor for aVARV and mVARV as “1.7 thousand years ago (kya) [95% highest priority density interval (HPD95): 2.2 to 1.4 kya]”; this was interpreted by Newfield et al. as implying that a VARV strain capable of instigating smallpox did not materialize before the 4th c. CE.Footnote 89 Clearly, that is not a legitimate conclusion. Rather, we should be dealing with the 95% probability that the event could have occurred at any time in the range calculated, between ca. 200 BCE and 600 CE – or, according to Babkin et al.'s calculation, between ca. 160 CE and 500 CE.Footnote 90
Thirdly, there is the problem of the relationship between the different strains identified genomically, and the nature of the disease, in terms of its symptoms, pathology, infectivity, case fatality rates, etc. As noted above, some have denied that aVARV should be considered smallpox at all and have suggested we abandon the use of the term “smallpox” altogether when talking about the ancient world.Footnote 91 Until we can equate particular genes with specific disease effects, the symptoms and epidemiology of medieval and earlier smallpox must remain shadowy; but the cases of osteomyelitis variolosa identified in medieval skeletons (Table 1) do show the existence of a pre-modern disease that caused the same long-term sequelae as smallpox. The evidence of the Persian medical writer Rhazes and Sicilian Arabic poetry mentioned above also show that medieval smallpox shared features with modern smallpox. The diagnosis of osteomyelitis variolosa in individual sk847 from Cirencester is important in this context because it shows the presence of a disease active in Roman Britain in the 3rd or 4th c. CE that also caused the same osteological sequelae as smallpox. Because no aDNA analysis has been performed on the Roman or Viking-age skeletons with osteomyelitis variolosa (and in any case the virus might not persist in the bones of someone who had survived a smallpox infection), we do not know whether these cases were caused by the aVARV or the mVARV clade; either is possible, as we have seen from the discussion above of the date after which they split from their most recent common ancestor. The Cirencester skeleton represents the earliest evidence yet identified in Europe of smallpox, or of a disease so like smallpox that it was capable of causing the same sequelae.
Smallpox and the Antonine Plague
The question of the antiquity of smallpox is bound up with the current debate over the identification of the Antonine Plague of the later 2nd c. CE. The symptoms of the plague described by the ancient physician Galen have as their most distinguishing feature a rash or exanthema, which was black from putrefied blood within the blisters; this was accompanied by diarrhea, often with black excrement (resulting from internal bleeding), stomach upset and sometimes vomiting, a sensation of fever internally but little outward sign of it, and fetid breath.Footnote 92 The possible identification of the disease as smallpox was first suggested in 1845, and argued for strongly by Littman and Littman in 1973.Footnote 93 By the time of a conference on the impact of the Antonine Plague in 2012, the retrospective diagnosis of smallpox had become widely accepted and was being used to try to understand the demographic impact, based on the case fatality rates of modern smallpox.Footnote 94 Already in 2005, however, Danielle Gourevitch had pointed out that Galen does not mention the permanent scarring caused by smallpox, and had suggested, therefore, that the Antonine Plague was one of the poxviridae, an ancestor of smallpox, but sufficiently different not to leave scarring.Footnote 95 This argument was developed by Rebecca Flemming, and has recently been accepted also by Colin Elliott who, in his book on the Antonine Plague, rejects the diagnosis of smallpox.Footnote 96 The argument from silence, however, is not strong: we are at the mercy both of the haphazard survival of ancient sources (and there are many fewer from the late 2nd c., for example, than from the 1st c. CE), and of the conventions of their genres. Even ancient medical writings often do not mention the kinds of things a modern medical writer might be interested in, and as Littman and Littman already pointed out, the scarring often did not appear until some days or weeks after the disease had passed, while Galen's focus was on the disease in its critical stages.Footnote 97 Moreover, Galen was not trying to write a complete symptomatology of the Antonine Plague; he mentions the plague in passing when one or more of its symptoms are relevant to other phenomena he is discussing. Since, if scarring did occur, he would have been unable to cure or prevent it, he may have been disinclined to mention it at all. Little can be concluded from the absence of references to scarring in either Galen's work or other literature. Similarly, the lack of pockmarked portrait statues could be explained easily by the idealizing conventions of Roman art. A stronger challenge to the straightforward identification as smallpox seemed to be mounted by the aDNA research discussed above showing that a number of aVARV strains of variola virus were circulating in the Middle Ages that differed in several respects from modern VARV. Doubts about the congruence of ancient and modern variola variants have even led some to call for abandoning the term “smallpox” in reference to diseases of antiquity.Footnote 98
Certainly, we should not uncritically assume that the symptoms, transmission rates, case fatality rates, etc. of ancient smallpox or an ancestor of modern smallpox were necessarily the same as for modern smallpox – not least because modern smallpox itself could have very variable case fatality rates, depending on whether the variola major or the alastrim strains were involved. Several points, however, stand. First, even if the aVARV clade produced symptoms substantially different from modern smallpox (and we do not know this for certain), molecular clock calculations of the time to most recent common ancestor of the aVARV and mVARV clades put the divergence of those clades at some time between the third millennium BCE and 600 CE, depending on whose calculations one believes. Even on the later ranges calculated by different teams, 200 BCE–600 CE, or 160 CE–500 CE, an mVARV clade could have appeared as a result of this divergence before or around the time of the Antonine Plague in the 160s CE. Second, the common ancestor of aVARV and mVARV had already diverged from a more generalized orthopoxvirus to become a human-specific virus at some date before that, and certainly either by or during the Roman Imperial period on anybody's calculation. Third, Galen describes a disease with such strong resemblances to smallpox that even if it was genetically somewhat different, it produced most of the same symptoms as modern smallpox. Fourth, archaeologically attested cases of osteomyelitis variolosa show the antiquity of a form of variola virus capable of causing the same osteological sequelae in survivors as did modern smallpox.
It is in this context that the skeletal remains of individual sk847 from Cirencester have a bearing on the argument. Although they date more than a century later than the Antonine Plague, they show that the variola virus had been introduced into the Roman world by the late 3rd or the 4th c. CE at the very latest, and probably before that. Indeed, it may well have become endemic by then; individual sk847 from Cirencester survived a childhood infection of smallpox, and this would be entirely consistent with endemic disease. The Antonine Plague, a devastating pandemic, with symptoms comparable to smallpox and a high mortality rate compatible with the first exposure of a naïve population to variola virus, is the obvious context for that original introduction of the disease into the Roman world, probably by troops returning from Lucius Verus's Parthian campaign in 165 or 166 CE. (The Plague of Cyprian is not a likely contender here; no account of its symptoms includes the characteristic exanthema of smallpox, and a viral hemorrhagic fever is more likely.Footnote 99) Those who had caught the disease and survived would have gained lifelong immunity to further infection, and the repeated waves of the Antonine Plague between the mid 160s and the 180s may reflect the behavior of the disease before enough people had gained immunity for it to become endemic, thereafter typically infecting mainly children who had not yet been exposed to it. The apparent disappearance of the Antonine Plague from our classical sources in the late 2nd c. may well reflect the fact that it became endemic. Periodic epidemics might also have occurred through reintroduction to regions where the disease had not manifested for a while and a non-immune population had grown up. As Monica Green points out, Gregory of Tours may describe smallpox in the 6th c. CE,Footnote 100 and there are various mentions either explicitly of smallpox or of a disease behaving very like smallpox from the 4th c. onwards in China,Footnote 101 and from the 7th c. onwards in the Eastern Mediterranean and western Asia. These suggest a basic continuity in the main outlines of the symptoms of the disease, even if there were doubtless a number of genetic variations of different strains.Footnote 102
If we wished instead to believe that the Antonine Plague was not caused by variola virus, we would need to assume not only that it was a different disease, which may have since become extinct, but also that the variola virus that caused the osteomyelitis variolosa in the Cirencester skeleton arrived in the Roman world unheralded in our surviving sources before the end of the 3rd c. That is not entirely impossible, and certainty cannot be achieved without ancient DNA analyses of victims of the Antonine Plague, but Occam's razor would argue against it. Meanwhile, we hope that the identification of osteomyelitis variolosa presented here may assist recognition of other cases in the archaeological record.
Acknowledgments
We are deeply grateful to Caroline Morris from the Corinium Museum and Elizabeth Selby from the Dorset Museum for their gracious hospitality and continuous assistance during Haoyue Zhao's visits to their collections. Their generosity in allowing access to their resources and permission to use photographs from their collections enabled and significantly enriched this research. We thank Wadham College, Oxford, for a travel grant to Haoyue Zhao that facilitated these visits. We also thank Dr Qiang Shen (MD), Dr Tong Zhao (MD), and Dr Mengjun Wang (MD, PhD), consultant radiologists at Beijing Shijitan Hospital, Capital Medical University, for their advice. Comments by the journal's two anonymous reviewers have helped us strengthen our argument, and we are grateful to them, and also to Dr Rosie Crawford for comments and corrections.
Competing interests
The author(s) declare none.


 Open access
Open access