


Introduction
Azoospermia is characterized by the total lack of sperm in the ejaculate. It is diagnosed in up to 20% of infertile men and affects 1% of the overall male population (Esteves et al., Reference Esteves, Miyaoka and Agarwal2011). Azoospermia is classified into two types: obstructive azoospermia, which is due to a mechanical blockage in the reproductive tract such as in the vas deferens, epididymis, or ejaculatory duct, and nonobstructive azoospermia (NOA), which is caused by a failure in sperm production (Esteves et al., Reference Esteves2015). NOA can be linked to either intrinsic testicular defects (primary spermatogenic failure) or abnormalities in the hypothalamic-pituitary-adrenal axis (secondary spermatogenic failure), which together account for about 30% of NOA cases. In most patients, the causes of NOA are unclear and are termed idiopathic NOA (iNOA) (Wu et al., Reference Wu, Lin, Sun and Cheng2021). Histopathologically, non-obstructive azoospermia is commonly classified into three major subtypes: hypospermatogenesis, maturation arrest, and Sertoli Cell-Only syndrome. Hypospermatogenesis is characterized by reduced but complete spermatogenesis, whereas maturation arrest refers to interruption of germ cell development at a specific stage. In Sertoli Cell-Only syndrome, seminiferous tubules lack germ cells (GCs) and contain only Sertoli cells (SCs). These histopathological patterns may coexist focally within the same testicular tissue in patients with idiopathic NOA, contributing to the heterogeneous sperm retrieval outcomes observed during micro-TESE procedures. iNOA represents a distinct group of men characterized by eugonadism, primary infertility, reduced testicular volume, azoospermia, and elevated follicle-stimulating hormone (FSH) levels (Giannouli et al., Reference Giannouli, Goulis, Lambropoulos, Lissens, Tarlarzis, Bontis and Papadimas2004).
Despite significant spermatogenic dysfunction, direct examination of testis biopsy specimens identifies focal areas of spermatogenesis in 30–60% of affected men (Deruyver et al., Reference Deruyver, Vanderschueren and Van der Aa2014; Chen et al., Reference Chen, Ma, Zou, Wang, Qui, Xiao, Zhou and Ping2019; Corona et al., Reference Corona, Minhas, Giwercman, Bettocchi, Dinkelman-Smit, Dohle, Fusco, Kadioglou, Kliesch, Kopa, Krausz, Pelliccione, Pizzocaro, Rassweiler, Verze, Vignozzi, Weidner, Maggi and Sofikitis2019). For this patient group, the possibility of retrieving sperm via microdissection testicular sperm extraction (mTESE) depends on multiple factors. There is a need for detailed research and investigation to understand why sperm retrieval is successful in some groups (TESE+) but not in others (TESE-) during the procedure.
Galectins (Gals) are a family of ß-galactoside-binding lectins located in extracellular spaces and within cellular components, including the cell membrane, cytoplasm, and nucleus (Barondes et al., Reference Barondes, Cooper, Gitt and Leffler1994). Galectin-3 (Gal-3) is a protein with multiple functions, playing a significant role in various biologic processes across different tissues and being involved in numerous clinical conditions and diseases. Recent findings have shown that Gal-3 can recognize pathogen-associated molecular patterns and possesses pro-inflammatory properties that facilitate the infiltration of neutrophils and other immune cells to sites of infection. It can also be released as a damage-associated molecular pattern (Sato et al., Reference Sato, Bhaumik and Pelletier2014). Altered expressions and function of Gal-3 have been found in various diseases, highlighting its clinical importance. Higher levels of Gal-3 have been observed in several types of cancer, such as breast, colon, and lung cancer, where it contributes to tumour growth, angiogenesis, and metastasis (Song et al., Reference Song, Tang, Owusu, Sun, Wu and Zhang2014).
Studies have confirmed that Gal-3 is expressed within the human male reproductive system, notably in the testis and epididymis (Lima et al., Reference Lima, Perpétuo, Ret, Fardilha, Leita-Moeirra, Bastos and Vitorino2023). Additionally, it has been identified in ejaculated spermatozoa and extracellular vesicles within human semen (Deschilde et al., Reference Deschildre, Ji, Chater, Dacheux, Selva, Albert, Bailly, Hatey and Benahmed2007; Kim et al., Reference Kim, Ahn, Moon, Kim, Jee, Joo and Shin2008; Jones et al., Reference Jones, Saraswati, Block, Lichti, Mahadevan and Diekman2010). Nevertheless, the impact of Gal-3 on human testicular tissue remains incompletely understood, and there are no existing studies on Gal-3 in patients with iNOA. Given the unknown aetiology in patients with idiopathic non-obstructive azoospermia (iNOA), our study aimed to investigate the effect of Gal-3 in relation to the presence or absence of sperm in this cohort.
It is posited that apoptosis in human testes plays a role in regulating physiologic spermatogenesis and contributes to impaired sperm production in spermatogenetic failures (Lin et al., Reference Lin, Lamb, Wheeler, Abrams, Lipshultz and Kim1997). Caspases are integral to the process of apoptosis. Elevated caspase activation in human spermatozoa has been linked to decreased sperm concentration, abnormal morphology, reduced progressive motility (Almeida et al., Reference Almeida, Cardoso, Sousa, Viana, Gonçalves, Silva and Barros2005), diminished sperm penetration capacity (Grunewald et al., Reference Grunewald, Said, Paasch, Glander and Agarwal2007), and an impaired ability to undergo capacitation (Grunewald et al., Reference Grunewald, Sharma, Paasch, Glander and Agarwal2009). The significance of apoptosis in spermatogenic failure conditions remains poorly understood. The activation of caspase-3 marks the point of no return in the apoptotic cascade and is considered an important and reliable indicator of apoptosis. Active caspase-3 has been identified as a critical component in the apoptotic process associated with spermatogenetic arrest (Bozec et al., Reference Bozec, Amara, Guarmit, Selva, Albert, Rollet, El Sirkasi, Vialart, Bailly, Benahmed and Mauduid2008; Grunewald et al., Reference Grunewald, Sharma, Paasch, Glander and Agarwal2009).
Intracellular Gal-3 is significant for cell survival because it can inhibit the intrinsic apoptotic pathway (Davidson et al., Reference Alverez, Haswell, St. Clair, Perng, Shorebah, Pierce and Fregien2002, Hsu et al., Reference Hsu and Liu2004). Gal-3 interacts with Bcl-2 via its carbohydrate-recognition domain, thereby inhibiting the pro-apoptotic action of Bcl-2 molecules. It is hypothesized that pro-apoptotic proteins from the Bcl-2 family can promote the release of cytochrome-c into the cytosol, whereas anti-apoptotic proteins can inhibit this process. This release subsequently triggers the activation of caspase-3 and caspase-9, leading to apoptosis (Tsujimoto et al., Reference Tsujimoto and Shimizu2000). Khorsandi and Orazizadeh found that Gal-3 present in spermatogenic cell cytoplasm might play a role in inhibiting germ cell apoptosis, which can be affected by alterations in testosterone production and exposure to environmental toxins (Khorsandi et al., Reference Khorsandi and Orazizadeh2011). Building on this information, our study aimed to examine apoptosis through caspase-3 in TESE+ and TESE- patients with iNOA and investigate its correlation with Gal-3.
Material and method
Patient groups
This prospective study was conducted in the IVF Centre of Istanbul University, Istanbul Faculty of Medicine. All male patients were examined by a urology specialist and evaluated through at least two semen analyses, karyotyping, Y microdeletion tests, and serum FSH and testosterone levels. Patients who were diagnosed as having non-obstructive azoospermia and scheduled to undergo mTESE procedures between October 2023 and February 2024 were included in the study. Inclusion criteria were as follows: infertile patients who did not use antibiotics in the last year, did not take probiotics and similar supplements, had no infectious disease even at a mild level in the last 6 months, were screened for sexually transmitted diseases (hepatitis B and C, human immunodeficiency virus, cytomegalovirus, syphilis and chlamydia) and no infection was detected, had no chronic-immunologic disease, and those with no obstruction in the ejaculatory ducts were determined as eligible for the study. Patients with excess or deficiency in the number of chromosomes according to karyotype analysis (e.g. 47+XXY) and patients with Y chromosome microdeletion and loss of some genes (genes in Azoospermia Factor a and b regions) were not included in the study. Also, men with lower testosterone levels were excluded from the study. Those who received medical treatment for infertility, those with previous inguinal or scrotal surgery (orchiopexy, varicocelectomy…etc), and those with hormonal disorders were excluded from the study.
Patients who underwent mTESE procedures for intracytoplasmic sperm injection and tissue sampling formed the study population. The patients were divided into two groups according to the presence of sperm in the sampled testicular tissue. The sperm-detected group in TESE was considered as TESE+ (n = 7), and the undetected sperm group in TESE was considered as TESE- (n = 8). The demographic and clinical characteristics of all participants were recorded, including age, body mass index (BMI), and hormone levels (luteinizing hormone (LH), FSH, prolactin (PRL), and testosterone).
Collection of samples
The patients underwent mTESE procedures by the same experienced urologist. In the m-TESE technique, first, a long longitudinal incision was made in the tunica albuginea. After the tunica albuginea was pushed upwards and the parenchyma was turned inside out, maximum surface area was provided with transverse slicing incisions on the parenchyma (Ichioka et al., Reference Ichioka, Matsui, Terada, Negoro, Goto and Ogava2020). A microscope was then brought to the field. The procedure was performed using a microscope with 15x magnification to enhance visualization and ensure precise tissue extraction from seminiferous tubules. Samples taken from the testicular tissue approximately 2–3 mm in size were placed in sterile tubes containing washing medium. The procedure took approximately 80–120 minutes for each patient and the biopsy material was examined within 10–15 minutes. Testicular tissue was dissected with the help of insulin injectors to milk the seminiferous tubules and the presence of sperm cells was evaluated under inverted microscope (Olympus Eppendorf Transfer Man NK2). The tissues were grouped according to the presence of spermatozoa and placed in suitable fixative for light microscopy.
Light microscope preparation
TESE tissues were followed up for morphologic evaluation and immunohistochemical staining in the Department of Histology and Embryology laboratory, Istanbul University. Testicular tissues of all groups were dehydrated by passing through a rising alcohol series after 10% Bouin fixation. The tissues, which were made transparent using toluene, were embedded in paraffin and blocked. Sections taken from the paraffin blocks with 3-µm thickness using a microtome were transferred onto positively charged slides and prepared for haematoxylin-eosin (H&E) staining and immunohistochemical staining.
Histomorphologic investigations
Tissue sections were kept in xylol for 1 hour for deparaffinization. After deparaffinization, paraffin sections were H&E stained for histomorphologic evaluation. The sections were examined under a light microscope (Zeiss Primostar 3 photomicroscope, Carl Zeiss Microscopy GmbH, Jena, Germany) at X10, X20, and X40 magnifications. Comparison between the groups was made according to the Johnsen score to evaluate the development of spermatoganial cells (Johnsen et al., Reference Johnsen1970). At least 10 fields were selected in each section and 50 seminiferous tubules were evaluated according to the Johnsen scoring at X20 magnification. For each patient, three serial histological sections were analysed, and all histological evaluations were independently performed by two blinded histologists to ensure the consistency and reliability of the analyses.
The Masson-trichrome stain was applied for fibrosis assessment. In Masson-stained preparations, seminiferous tubule wall thickness was measured by modifying literature data (Mohammadi et al., Reference Mohammadi, Behnam-Rassouli, Momeni and Mahdavi-Shahri2016; Faraji et al., Reference Faraji, Momeni and Malmir2019; Jensen et al., Reference Jensen, Wang, Mamsen, Giwercman, Jørgensen, Fode, Ohl, Dong, Hildorf, Pors, Fedder, Ntemou, Andersen and Sønksen2022). In each testicular tissue sample, measurements were made at three different points in 10 randomly selected seminiferous tubules. Comparison between groups was based on the mean of the measurements in each sample.
Immunohistochemical evaluations
For immunohistochemical evaluations, sections were deparaffinized and then treated with 3% endogenous peroxidase. Then tissue sections were rinsed in phosphate-buffered saline. Citrate buffer (pH:6.0) was used for antigen retrieval. After rinsing, short-term blocking was performed and then primary antibody was applied. For the detection and distribution of Gal-3 antibodies in the tissue, Gal-3 antibody (NB300-538, Novus Biologicals, Colorado, USA) was applied at a dilution of 12 µg/mL overnight. For apoptosis detection, pro- and active caspase-3 antibody (NB100-56708, Novus Biologicals, Colorado, USA) was applied at 14 µg/mL overnight. Secondary antibody and streptavidin-peroxidase were applied according to the procedure (TP-125-HL, UltraVision, Thermo Fisher Scientific, Waltham, Massachusetts, USA). DAB (DAB Chromogen & Substrate system, Thermo Scientific, Massachusetts, USA) as chromogen and haematoxylin was used for counterstaining. Staining intensity (0 = negative, 1 = weak, 2 = moderate positive, and 3 = strongly positive) and staining percentage (0–100%) were analysed in each of the previously listed components of the analysed testicular tissue separately. All evaluations were performed by two histologists in a double-blind manner. For immunohistochemical evaluation, three serial sections belonging to the same patient were analysed. In each preparation, at least 10 randomly selected microscopic fields were evaluated at X20 magnification, and a minimum of 50 seminiferous tubules were assessed for immunohistochemical analysis. All evaluations were independently performed by two blinded histologists to ensure the consistency and reliability of the immunohistochemical quantification.
Histologic score (H-score)
The assessments of the immunohistochemical expressions in TESE tissues were achieved by using H-scores. H-score = ∑Pi (i + 1). Here, i indicates the staining intensity (0 = negative, 1 = weak positive, 2 = moderate positive, and 3 = strongly positive) and Pi is the percentage of the cells stained for each intensity. Apoptosis and fibrosis indexes were calculated as the ratio of stained cells to all cells.
Statistical analyses
Images were photographed using a Zeiss Primostar 3 photomicroscope (Carl Zeiss Microscopy GmbH, Jena, Germany) at X4, X10, and X40 objectives. Measurements were made using the LabScopesoftware (Zeiss GmbH, Jena, Germany). After semiquantitative immunohistochemical evaluation, the distribution of the data was checked using the Shapiro–Wilk test. Welch’s t-test was applied as a parametric test. Values are shown as mean±standard deviation (SD). The Mann–Whitney U test was applied to non-parametric data. Statistical analysis was completed using the GraphPad Prism 10.0.2 software (GraphPad Software, San Diego, USA), and p < 0.05 was considered significant.
Results
Subject characteristics
Demographic and basic clinical features in the study population are shown in Table 1. Demographic and baseline characteristics showed no significant difference between the two groups in terms of age, size, weight, BMI, and LH and PRL levels (all p-values above 0.05). Serum FSH levels were higher in the TESE- group (36.7 ± 8.82) when compared with the TESE+ group (16.29 ± 3.69) (p = 0.031). By contrast, serum testosterone levels were lower in the TESE- group (3.884) compared with the TESE+ group (5.147) (p = 0.043). Testosterone levels were within the normal range in both groups.
Comparing demographic and basic clinical features

BMI, body mass index; LH, luteinizing hormone; FSH, follicle-stimulating hormone; PRL, Prolactin.
* indicates statistically significant values, defined as p < 0.05.
ǂ indicates the statistical test or comparison applied for the relevant variable.
Seminiferous tubule examination
In the TESE- group, where no spermatozoa were found, vacuolated, hollow areas and marked atrophy were observed. Consistent with hypo spermatogenesis, the number of mature cells was much reduced, and the germinal epithelium appeared loose with very few cells. Round spermatids were the most developed cells. The central lumen was enlarged and empty. There was germ cell aplasia and increased thickness of the seminiferous tubule wall, which might be compatible with tubular sclerosis (Figure 1).
Histopathological evaluation of TESE- and TESE+ groups. A, B and C represent the TESE- group; D, E and F represent the TESE+ group. A. Micrograph showing germ cell aplasia showing Sertoli cells (arrow). B. Atrophic areas (asterix) and vacuoles (arrowhead) are seen in all seminiferous tubules. C. Increased seminiferous tubule wall thickness consistent with tubular sclerosisis observed. D. Incomplete maturation arrest up to round-elongated spermatid (arrowhead) is observed. E. Inflammatory cells rich in lymphocytes (arrow) are increased in the interstitial area. Germ cell aplasia (asterix) is observed in the seminiferous tubule in the field of view. F. Cells of spermatagonial series a different stages of development such as elongated spermatids (arrowhead) and round spermatids (asterix) are observed. Haematoxylin & Eosin. The scale bar: 200 μm for 10X, 50 μm for 40X magnification.

Round spermatids and elongated spermatids were observed in the TESE+ group. Primary spermatocytes and a small number of more mature cells consistent with incomplete maturation arrest were focally observed. Germ cell aplasia was observed in some tubules, and there was focal spermatogenesis in others. There was lymphocytic inflammation in the interstitial area (Figure 1).
The histopathological findings in the TESE− group were predominantly compatible with severe hypospermatogenesis, focal Sertoli Cell-Only pattern, and tubular sclerosis. In contrast, the TESE+ group demonstrated focal spermatogenesis and incomplete maturation arrest in several seminiferous tubules. Due to the focal heterogeneity commonly observed in iNOA patients undergoing micro-TESE, some patients exhibited mixed histopathological features rather than a single uniform subtype.
According to the Johnsen score, there were more advanced spermatogonial series cells in the TESE+ group. The average TESE- group and TESE+ group scores were 2.889 and 6.577, respectively (p < 0.001) (Figure 2).
Johnsen scoring. A. Only Sertoli cell nuclei (arrow) are seen in the seminiferous tubule of the TESE- group. B. Spermatocytes (arrow) and spermatids (arrowhead) are seen in the TESE+ group. Johnsen score is higher in the TESE+ group (p < 0.05). Haematoxylin & Eosin. The scale bar: 50 μm for 40X magnification.

When analysing the connective tissue, an increase in seminiferous tubule wall thickness was found in the TESE- group. The seminiferous tubule wall was significantly thicker in the TESE- group (14.04 ± 2.7) compared with the TESE+ group (8.15 ± 1.57) (p < 0.001) (Figure 3).
Histomorphological evaluation of the seminiferous tubules. A, B represent the TESE- group; C, D represent the TESE+ group. A. The seminiferous tubule wall shows increased thickness with diffuse connective tissue (asterix). B, D. Representative measurements of seminiferous tubule wall thickness are indicated by the red measurement lines at high magnification. C. The seminiferous tubule wall appears normal. Statistical analysis showed increased thickness of the seminiferous tubule wall in the TESE- group (p < 0.05). Masson trichrome staining. Scale bar: 200 μm for X10 and 50 μm for X40 magnification.

Galectin-3 and caspase-3 expression profiles
The immunohistochemical results were analysed, and the differences between tissue staining and non-staining are shown in Figure 4. Gal-3 positivity was observed in both groups. In the TESE- group, SCs and cells in the interstitial area around the seminiferous tubules showed strong positivity. In the TESE+ group, a weak positive reaction was observed in SCs. In the statistical evaluation according to H-scores, Gal-3 intensity was higher in the TESE- group (p = 0.024) (Figure 4).
Immunohistochemical evaluation of galectin-3 and apoptosis. Galectin-3 showed strong positive reaction in Sertoli cells (arrow) and interstitial cells (asterisks) around the seminiferous tubules in the TESE- group, whereas it showed weak intensity in Sertoli cells (arrow) in the TESE+ group (p < 0.05). Apoptosis assessed by Caspase-3 showed strong immunopositive reaction in the cytoplasm of Sertoli cells (arrow) in TESE- group and weak positive reaction in spermatocytes (arrowhead) in TESE+ group. Apoptosis was higher in TESE- group (p < 0.05). DAB-Haematoxylin. The scale bar: 50 μm for 40X magnification.

Apoptotic marker caspase-3 expression levels showed significant differences when compared between the TESE- and TESE+ groups (p = 0.019). In the caspase-3 evaluation for apoptosis, caspase-3 immunopositivity was moderate in the TESE- group and mild in the TESE+ group. Staining was predominantly seen in SCs in the TESE- group, and in spermatogonial series cells in the TESE+ group. Caspase-3 immunopositivity was significantly higher in the TESE- group (Figure 4).
Correlation of galectin-3 and caspase-3 expression levels and clinical parameters
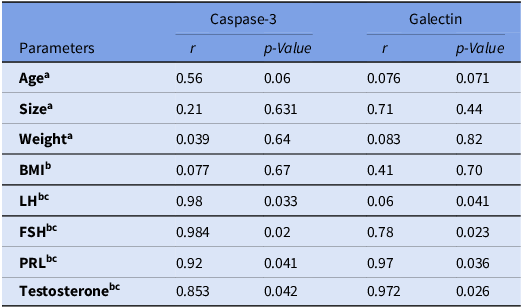
Correlation analyses were performed to verify the associations of clinical parameters and Gal-3 and caspase-3 expression levels. We found that serum FSH levels were positively correlated with caspase-3 (r = 0.64; p = 0.027) and Gal-3 (r = 0.052; p = 0.042) expressions in the TESE+ group. Also, when testosterone was investigated, we found a positive correlation with caspase-3 (r = 0.213; p = 0.032) and Gal-3 (r = 0. 563; p = 0. 018) expressions (Table 2). When the TESE- group was examined, a correlation was found between all hormone levels. Caspase-3and Gal-3 expressions showed a positive correlation with LH (p = 0.033 and p = 0.041, respectively), FSH (p = 0.02 and p = 0.023, respectively), PRL (p = 0.041 and p = 0.036, respectively), and testosterone (p = 0.042 and p = 0.026, respectively) (Table 3). The results showed that increased hormone levels were associated with elevated Gal-3 expression and increased caspase-3 activity, suggesting a relationship with inflammatory and apoptosis-related processes.
Correlation coefficients for caspase-3, galectin-3 expression levels and clinical parameters in the diminished TESE (+) group using Pearson’s correlation and Spearman’s rank correlation coefficient

BMI, body mass index; FSH, follicle-stimulating hormone; LH, luteinizing hormone.
a Pearson’s correlation coefficient was used.
b Spearman’s rank correlation coefficient was used.
c Day 3 of the cycle before stimulation.
Correlation coefficients for caspase-3, galectin-3 expression levels and clinical parameters in the diminished TESE (-) group using Pearson’s correlation and Spearman’s rank correlation coefficient

BMI, body mass index; FSH, follicle-stimulating hormone; LH, luteinizing hormone; PRL, prolactin.
a Pearson’s correlation coefficient was used.
b Spearman’s rank correlation coefficient was used.
c Day 3 of the cycle before stimulation.
Discussion
In this prospective study, we investigated the presence of apoptosis through caspase-3, an apoptosis marker, in TESE + and TESE- patients with iNOA, and evaluated its relationship with Gal-3. The results showed that patients with impaired spermatogenesis exhibited significantly higher expression of caspase-3 compared with those in whom sperm cells had been obtained with mTESE.
The seminiferous epithelium consists of Sertoli cells (SCs) and GCs at various developmental stages. SCs are the only somatic cells within the seminiferous epithelium and play essential roles in supporting spermatogenesis, maintaining the blood-testis barrier, and regulating testicular immune homeostasis (França et al., Reference França, Hess, Dufour, Hofmann and Griswold2016; Kaur et al., Reference Kaur, Wright, Greer, Mueller, Haynes, Dufour and Cheng2018). In addition, SCs secrete several immunoregulatory molecules, including galectins, transforming growth factor-β, and prostaglandins, which contribute to local immune regulation within the testis (Cupp et al., Reference Cupp, Kim and Skinner1999; Wollina et al., Reference Wollina, Schreiber, Gornig, Feldrappe, Burchert and Gabius1999; Dettin et al., Reference Dettin, Rubinstein, Aoki, Rabinovich and Maldonado2013; Luca et al., Reference Luca, Baroni, Arato, Hansen, Cameron and Calafiore2018). Gal-3, like Gal-1, is expressed during embryonic stages and may participate in early developmental processes. Gal-3 is produced by numerous cells, including those in both the innate and adaptive immune systems (Sehrawat et al., Reference Sehrawat and Kaur2020). Essential roles of galectins in the inflammatory response involve helping the ability of innate immune cells to detect and respond to chemotactic signals, migrating through the endothelium, and produce and release either pro-inflammatory or anti-inflammatory cytokines. Additionally, Gals facilitate the recognition, engulfment, and elimination of pathogens and damaged cells (Cerliani et al., Reference Cerliani, Stowell, Mascanfroni, Arthur, Cummings and Rabinovich2011).
Gal-3 has been identified in bulls, predominantly in the Leydig cells of the immature testis and in the peritubular myoid and interstitial cells of the mature testis (Kim et al., Reference Kim, Ahn, Moon, Kim, Jee, Joo and Shin2008). These findings indicate that Gal-3 expression may contribute to the maturation stage and activation of sperm cells. Researchers have identified Gal-3 in SCs, but it appears to be absent in GCs of both humans and rats. In healthy human testes, Gal-3 is specifically localized within the cytoplasm of SCs. However, an increase in Gal-3 immunostaining and/or a shift in its localization to the nucleus has been observed in infertile testes. Patients with azoospermia exhibited significantly higher serum and seminal levels of Gal-1 and Gal-3 compared with normal individuals (Gamalel Din et al., Reference GamalEl Din, Shaker, Fawzy Megawer, Abdel Salam, Abdelhalim and Adel2023). Gal-3 knockout (KO) transgenic mice demonstrated a delay in the initial wave of spermatogenesis. They also showed a reduced number of germ cells on postnatal days 5 (P5) and 15 (P15), along with defective maturation of SCs. These findings indicate that Gal-3 plays a role in regulating the initiation of spermatogenesis and the maturation of SCs, partly by preventing GC apoptosis and influencing testosterone biosynthesis (Lei et al., Reference Lei, Blois, Freitag, Ozdemir, Yuksel, Ozturk, Budak and Dogan2021). We observed significantly elevated Gal-3 expression in SCs from TESE- patients with iNOA. In this context, the up-regulation of Gal-3 may reflect an attempt to rectify impaired spermatogenesis. Moving forward, comprehending the role of Gal-3 in testicular physiology will provide valuable insights into the factors influencing GC development and steroidogenesis, and help identify novel biomarkers of testicular function.
Gal-3 may exert different biological functions depending on its intracellular or extracellular localization. Intracellular Gal-3 is primarily associated with anti-apoptotic and regulatory cellular activities, whereas extracellular Gal-3 is more closely linked to inflammatory responses (Stillman et al., Reference Stillman, Hsu, Pang, Brewer, Johnson, Liu and Baum2006; Haudek et al., Reference Haudek, Spronk, Voss, Patterson, Wang and Arnoys2010). Chronic tissue injury and persistent inflammation may further promote Gal-3-mediated fibrogenesis, leading to tissue remodelling and scar formation (Califice et al., Reference Califice, Castronovo, Bracke and van den Brûle2004; Henderson et al., Reference Henderson and Sethi2009). In our study, the increased seminiferous tubule wall thickness observed in the TESE− group supported the potential fibrogenic role of Gal-3. Moreover, Gal-3 positivity in the TESE− group was detected in both Sertoli and interstitial cells, whereas staining in the TESE+ group was predominantly limited to Sertoli cells. This distribution pattern may indicate increased inflammatory activity within the interstitial compartment of TESE− patients.
In addition to its role in inflammation and fibrosis, Gal-3 regulates several cellular processes, including angiogenesis, tumour progression, and apoptosis-related pathways (Califice et al., Reference Califice, Castronovo, Bracke and van den Brûle2004). Previous studies have suggested that Gal-3 participates in mitochondrial apoptosis pathways associated with cytochrome-c release and caspase-3 activation (Fukumori et al., Reference Fukumori, Takenaka, Yoshii, Kim, Hogan, Inohara, Kagawa and Raz2003; Fukumori et al., Reference Fukumori, Oka, Takenaka, Nangia-Makker, Elsamman, Kasai, Shono, Kanayama, Ellerhorst, Lotan and Raz2006). Gal-3 may also contribute to germ cell survival through modulation of apoptosis-related mechanisms (Kim et al., Reference Kim, Ahn, Moon, Kim, Jee, Joo and Shin2008). Consistent with these findings, increased caspase-3 positivity has previously been demonstrated in patients with impaired spermatogenesis, including hypospermatogenesis, maturation arrest, and Sertoli Cell-Only syndrome (Kilic et al., Reference Kilic, Lortlar and Bardakci2009; Singh et al., Reference Singh, Jaiswal, Singh, Trivedi, Agrawal, Gupta, Rajender and Singh2019). Similarly, our study showed that elevated caspase-3 expression in the TESE− group was associated with enhanced apoptotic activity. Taken together, the observed association between Gal-3 and caspase-3 suggests that inflammation-driven apoptotic and fibrotic processes may contribute to impaired spermatogenesis in patients with iNOA.
From a therapeutic perspective, Gal-3 may represent not only a diagnostic biomarker but also a potential therapeutic target in patients with iNOA. Previous experimental studies in inflammatory and fibrotic disorders have demonstrated that inhibition of Gal-3 signalling can attenuate fibrosis, suppress inflammatory responses, and modulate apoptosis-related pathways. Considering the increased Gal-3 expression observed in TESE− patients, together with enhanced caspase-3 activity, seminiferous tubule wall thickening, and impaired spermatogenesis, targeting Gal-3 may offer a novel therapeutic approach for improving the testicular microenvironment and preserving spermatogenic function. Modulation of Gal-3 activity may reduce chronic inflammation, limit fibrotic remodelling, and decrease germ cell apoptosis within seminiferous tubules. However, because Gal-3 also exerts intracellular anti-apoptotic and immunoregulatory effects, further mechanistic studies are needed to determine whether Gal-3 inhibition would produce beneficial or context-dependent effects in human testicular tissue. Future translational and experimental studies investigating selective Gal-3 inhibitors may further clarify their potential role in the treatment of male infertility.
Previous studies investigating azoospermia reported significantly elevated FSH levels, whereas LH and testosterone levels generally showed no significant differences (Iftikhar et al., Reference Iftikhar and Muhammad Shakeel2002; Abdalrazig et al., Reference Abdalrazig and Ismail2017). In most patients with idiopathic azoospermia, serum testosterone levels remain within the normal range, although decreased levels may occasionally be observed (Hauptman et al., Reference Hauptman, Perić, Marić, Bojanac, Sinčić, Zimak, Kaštelan and Ježek2021). Consistent with these findings, serum FSH levels were significantly higher in the TESE− group in our study, whereas testosterone levels were lower compared with the TESE+ group. In addition, Gal-3 and caspase-3 expressions were positively correlated with serum testosterone levels, suggesting that testicular damage and impaired spermatogenesis may influence hormonal regulation and interstitial cell activity. FSH plays an important role in the regulation of spermatogenesis through its effects on SCs and germ cell survival (Sharpe et al., Reference Sharpe, McKinnell and Kivlin2003; Zimmermann et al., Reference Zimmermann, Stévant, Borel, Conne, Pitetti, Calvel, Kaessmann, Jégou, Chalmel and Nef2015). Previous studies have demonstrated significantly elevated FSH levels in patients with azoospermia (Abdalrazig et al., Reference Abdalrazig and Ismail2017). Consistent with these findings, serum FSH levels were significantly higher in the TESE− group in our study. Experimental studies have also suggested that FSH may influence Gal-3 expression and apoptosis-related pathways in Sertoli cells (Suomalainen et al., Reference Jiang, Savontaus, Simonsen, Williamson, Müllenbach, Gromoll, Terwort, Alevizaki and Huhtaniemi2004). In our study, Gal-3 and caspase-3 expressions were positively correlated with elevated FSH levels in the TESE− group, suggesting a possible association between impaired spermatogenesis, inflammation, and apoptosis-related activity.
Our study has several limitations. First, the relatively small sample size may limit the statistical power and generalizability of the findings. Second, the absence of obstructive azoospermia and fertile control groups restricts the ability to determine whether the observed alterations in Gal-3 and caspase-3 expression are specific to iNOA. Third, the immunohistochemical findings were not supported by additional molecular analyses such as Western blotting, quantitative PCR, or biochemical assays. In addition, tissue samples from different focal regions within the same testis were not evaluated separately, preventing assessment of regional heterogeneity in spermatogenesis and inflammatory activity. Therefore, larger multicenter studies incorporating molecular and functional analyses are needed to validate these findings and further clarify the clinical significance of Gal-3 in male infertility.
This study investigated the potential roles of caspase-3 and Gal-3 in patients with iNOA. Caspase-3 immunopositivity was significantly higher in the TESE− group, indicating increased apoptotic activity in patients without sperm retrieval. Although Gal-3 positivity was observed in both groups, its expression intensity was markedly higher in the TESE− group. Elevated Gal-3 expression together with increased caspase-3 positivity may reflect enhanced inflammation- and apoptosis-related processes contributing to fibrosis and impaired spermatogenesis. These findings suggest that Gal-3 may serve not only as a biomarker associated with unsuccessful sperm retrieval but also as a potential therapeutic target in male infertility.
Data availability statement
Raw data can be shared and will be available upon request.
Acknowledgements
The authors thank all individuals for their participation in our study.
Author contributions
AAA, MD, ESY, and KNU designed the research. AAA, MD, ESY, and KNU carried out the experiment. AAA,MD, BKB, ESY, KNU performed the analytic calculations and contributed to the interpretation of the results. AAA, MD, BKB, AK, CA wrote the manuscript. AK, CA supervised the project. ESY, KNU, AK, CA helped and jointly supervised the work.
Funding
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. No funding was received for conducting this study. The authors declare they have no financial interests. The authors have no conflicts of interest to declare that are relevant to the content of this article.
Competing interests
The authors have no conflicts of interest.
Ethical standards
Istanbul Medipol University Non-Interventional Clinical Research Ethics Committee Approved with the Decision dated 12.10.2023 and numbered E-10840098-772.02-6597.
Capsule
Elevated Galectin-3 expression may be associated with inflammation, fibrosis, and apoptosis-related processes contributing to impaired spermatogenesis.
Attestation statement
-
• The subjects in this trial have not concomitantly been involved in other randomized trials.
-
• Data regarding any of the subjects in the study has not been previously published.
-
• Data will be made available to the editors of the journal for review or query upon request.







 Open access
Open access