


Traditional psychiatric undergraduate education often relies on didactic methods that may be inadequate to convey the complex emotional realities of clinical practice. Reference Sharma, Hewson, Mahalingappa, Fallon, Hyland and Abraham1 To bridge this gap, educators are increasingly turning to experiential pedagogies. Reference Pal, Taywade and Gopi2 Forum theatre, a cornerstone of Augusto Boal’s genre of theatre dubbed ‘theatre of the oppressed’, was developed as a radical pedagogical tool to catalyse social and political change. Reference Boal3 Boal’s methods dismantled the traditional divide between actor and spectator, empowering audiences to become ‘spect-actors’ – active participants who join the stage to rehearse real-world change through theatre.
In healthcare education, forum theatre has been adopted in recent years as a tool to improve communication and simulation skills. Reference Stevenson, Khan, Bharmal, Odejimi, Samnani and Wright4 Its pedagogical value is hypothesised to lie in its ability to create an environment for experiential learning by directly placing students in complex dilemmas, exposing them to sensitive issues such as racism that cannot be replicated in didactic lectures. Reference Manzi, Casapulla, Kropf, Baker, Biechler and Finch5 Although its effectiveness in enhancing the communication skills of psychiatric trainees has been demonstrated in a small study, Reference Stevenson, Khan, Bharmal, Odejimi, Samnani and Wright4 its application and utility in undergraduate medical education remains unexplored. Additionally, little is known about how this method could contribute to enhancing learners’ understanding of the lived experience of mental illness.
Aims of the current study
We conducted a study to: (a) explore the impact of a forum theatre-based educational intervention on medical students’ learning, emotional engagement, perceived clinical skill development and overall learning experience; and (b) explore what aspects of forum theatre contribute to its pedagogical value in medical education.
Method
Study design
This was a mixed-methods evaluation of a forum theatre-based educational intervention. Quantitative data were gathered via post-intervention surveys to measure self-reported changes across key domains. Qualitative insights were also elicited from this survey and from a focus group involving actors and clinical teaching fellow (CTF) facilitators to understand mechanisms underlying quantitative findings.
Participants
The population comprised fourth-year medical students undertaking their psychiatry rotation at the University of Birmingham, UK. Although participation in the intervention was integrated as a mandatory timetabled session, completion of the survey was voluntary.
The single focus group comprised seven participants: three professional actors and four CTFs.
Ethics statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. The study was reviewed and approved by the University of Birmingham’s Medical School Ethics Committee (ERN_3597-Dec2024). The project was discussed with the research governance manager at Birmingham and Solihull Mental Health NHS Foundation Trust, who confirmed that National Health Service (NHS) research ethics approval was not required as the project did not involve NHS data. Submission of the survey questionnaire was voluntary, with no academic penalty for non-completion. Informed consent was obtained from all focus group participants, with assurances of voluntary participation and anonymity.
Intervention
The Revolving Door intervention uses a stage play with the same name Reference Wright6 that has been adapted into a forum theatre-based intervention for delivery to medical students during their psychiatry rotation. The play begins with the story of Martin, a young man undergoing a first episode of psychosis, and his mother Audrey as they navigate the process of accessing timely and appropriate mental health support. The audience witness critical clinical interactions, from the first contact with a general practitioner until eventually a Mental Health Act (MHA) assessment, which illuminate the bureaucratic, interpersonal and emotional barriers often faced by patients. Despite the clinicians’ best intentions, the patient is terrified and they inadvertently increase his sense of alienation and emotional distress.
Facilitators then guide the audience through structured reflective discussion, encouraging learners to examine the decisions made by various clinicians. The scene is then re-staged, incorporating audience’s suggestions for alternative approaches and inviting students into the play. In doing so, the audience is not merely learning about psychosis – they are collectively experimenting with ways that they, as future clinicians, might directly improve patient care.
Data collection and analysis
Post-intervention survey
Following the session, students voluntarily completed an anonymous questionnaire comprising free-text responses and Likert-scale items using a 5-point scoring dimension, ranging from 1 (‘strongly disagree’) to 5 (‘strongly agree’). Survey domains included understanding of psychosis, confidence in clinical communication, emotional engagement and perceived educational value of the intervention. Feedback was collated for performances delivered between December 2023 and March 2025.
Focus group
A single focus group was conducted with the play’s facilitators and actors. Using a semi-structured format, the discussion explored their perceptions of the intervention’s effectiveness, emotional impact and observed student engagement (Box 1). The focus group was audio-recorded and transcribed.
Focus group questions
-
Q1 Please introduce your role in the play and previous experience with Revolving Door.
-
Q2 Why do you think this play is important?
-
Q3 Why did you get involved with the play?
-
Q4 What are the strengths of forum theatre as an approach for teaching?
-
Q5 What are the limitations of forum theatre as an approach for teaching?
-
Q6 Some may say that, in a busy medical school curriculum, dedicating time to a theatre experience may not be an efficient use of time. Any thoughts on this?
-
Q7 What are the obstacles to student engagement in forum theatre and how do you overcome this?
-
Q8 The play can be greatly emotional for students. What do you think about this?
-
Q9 Was there anything you found surprising about delivering the session?
-
Q10 Have there been any standout, memorable moments?
-
Q11 Any other comments?
Thematic analysis, as outlined by Braun & Clark, Reference Braun and Clarke7 was used to process the qualitative data. Two authors (R.B. and S.D.) familiarised themselves with the data, generated initial codes and collated these into potential themes. Themes were reviewed, defined and named through a collaborative and iterative process. Discrepancies were resolved through discussion with two additional authors (A.K.A.M. and A.Y.E.). The analysis was undertaken with the aid of version 1.4.1 of Taguette, the web-based, open-source qualitative research tool. Reference Rampin and Rampin8
The CTFs were positioned as both facilitators and researchers; the dual role provides contextualised insight into the intervention’s delivery. To mitigate bias, reflexive practice was employed through peer debriefing and a conscious effort to prioritise students’ and actors’ voices.
Results
Quantitative analysis
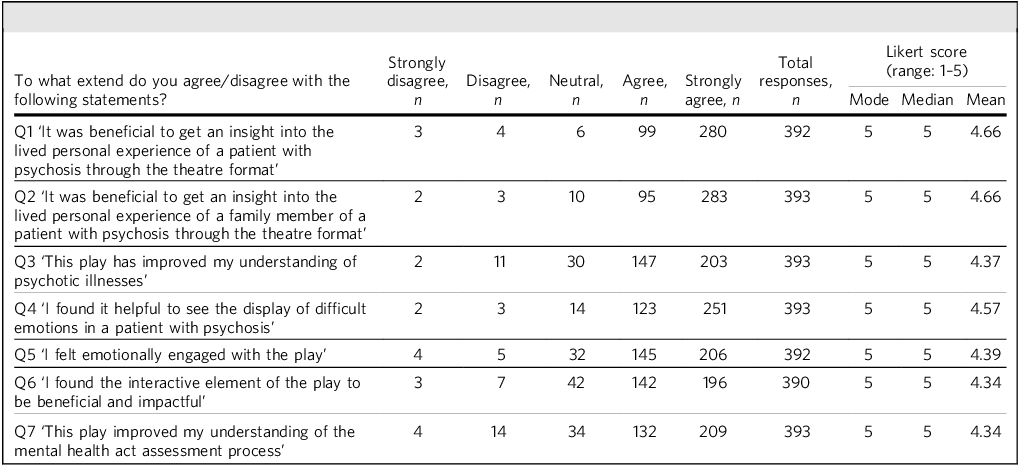
In total, 393 students completed the post-intervention survey (Table 1). The majority reported that the intervention had been helpful in gaining insight into the lived experience of both a patient (n = 280 ‘strongly agree’, n = 99 ‘agree’; mean score: 4.66) and their family member (n = 283 ‘strongly agree’, n = 95 ‘agree’; mean score: 4.66) through the medium of forum theatre.
Quantitative responses to the post-intervention survey

Respondents stated that the intervention improved their understanding of psychotic illnesses (n = 203 ‘strongly agree’, n = 123 ‘agree’; mean score: 4.37).
In addition they found it helpful to see the depiction of difficult emotions in a patient experiencing psychosis (n = 251 ‘strongly agree’, n = 123 ‘agree’; mean score: 4.57) and felt emotionally engaged throughout the intervention (n = 206 ‘strongly agree’, n = 145 ‘agree’; mean score: 4.39).
The students stated that the interactive element of the intervention was beneficial and impactful (n = 196 ‘strongly agree’, n = 142 ‘agree’; mean score: 4.34). Their understanding of the MHA assessment process also improved (n = 209 ‘strongly agree’, n = 132 ‘agree’; mean score: 4.34).
Qualitative analysis
Thematic analysis was undertaken on free-text questions in the post-intervention survey (Box 2) and the focus group transcript. Owing to recurrent themes identified across the survey and focus group, analysis was undertaken after pooling the data in order to give a succinct representation. Analysis yielded five overarching themes (Fig. 1).
Emerging themes from thematic analysis.

Free-text questions in the post-intervention survey
-
Q8 What have you found the most impactful and helpful aspect of the play?
-
Q9 Is there anything you would like to be done differently in the future?
-
Q10 What were your expectations of the play when you came in, and how did that resonate with what you have seen?
-
Q11 Any other comments?
Theme 1: immersive theatre as a catalyst for engagement and learning
The students consistently described the theatrical format as an engaging educational tool. Several commented on the realism of the scenarios and the way the performance simulated clinical reality without the abstraction of textbooks or traditional lectures. Interactive features, such as audience members being able to ‘rewind and replay’ scenes, were viewed as particularly impactful (student survey, SS):
‘It was helpful to see it live and be able to feel the emotion vs simply watching a YouTube video. It was very good to then make changes and rewrite the ending based on how we thought it could be improved.’ (SS)
The professional actors and facilitators (focus group, FG) agreed with this sentiment and acknowledged the power of theatre to engage students through many simultaneous means:
‘You know that people are learning on lots of different levels at the same time or absorbing it practically physically, emotionally, spiritually, intellectually. It’s all happening at the same time. Rather than those things being separate on a PowerPoint.’ (FG)
Although students acknowledged the merits of forum theatre, some had understandable concerns about having to perform in front of their peers in ‘rewind and replay’ scenes:
‘I found it stressful, the thought of being picked on to act in front of a large group of people and it held me back from answering questions.’ (SS)
The anxiety expressed by students was also recognised by the actors and facilitators in the focus group:
‘This kind of way of learning […] can feel really uncomfortable […] especially in the workshop bit where they’re called on to get involved.’ (FG)
Theme 2: change and transformation
The session provoked meaningful shifts in perception among participants – particularly regarding the complexity of psychiatric care, systemic barriers and their own developing professional identities. Many students described a growing awareness of the emotional and structural challenges faced by patients and families, and several cited the session as a pivotal moment in their psychiatry rotation:
‘I was genuinely moved by the play, so the emotional connection is guaranteed to have a lasting effect. The effects would be to keep empathy and understanding in the forefront of my consultations and realise that in every interaction with a [clinician] lies the potential to really make a difference in someone’s life.’ (SS)
Facilitators reflected on the difficulty of measuring such transformation in students. They remarked that their hope is that the students will reflect on what they have learnt and incorporate it into their future practice:
‘The spiritual changes that [happen] aren’t as easily quantifiable, the impact it will have cannot necessarily be measured today, [when] we do it next week or in 5 years. But you know, in 15 years’ time someone might be at a mental health assessment and go… ‘Oh, this is just like that play I saw’. It’s sort of like a gentle moulding rather than like an instructive thing, and gentle moulding takes time.’ (FG)
‘We wanted to stop at a moment of extreme dilemma […] when medical students stand in the shoes of the characters and [the management] is in their hands. That’s where the deepest learning takes place.’ (FG)
Theme 3: lived experience and authenticity
The authenticity of the characters and story, inspired by real people, was frequently cited as a key strength. Students responded strongly to the portrayal of both Martin and his mother Audrey, whose emotional labour and marginalisation were deeply felt:
‘I really loved that it helped us understand the patient’s perspective, the family’s perspective and also how to interact with a patient from the doctor’s perspective.’ (SS)
‘This play particularly resonated with me […] having experienced something very similar […] where a person close to me had acute psychosis. [The] process of getting them help can take a toll on family members and become very mentally draining, which again was portrayed very well in this play.’ (SS)
Theme 4: clinical skill development through performance
In addition to emotional engagement, students highlighted the session’s utility in developing concrete clinical skills. Scenarios involving mental state examinations, MHA assessments and formulation were embedded within the performance, offering students opportunities to observe and practise these skills in context:
‘Running through each section of the last scene with the changes implemented was really helpful and having the opportunity to observe peers taking part was very insightful.’ (SS)
‘Only 1% of medical students get [to watch an MHA assessment], the actual lived experience, whilst training. In this [play], many more medical students can get that direct experience.’ (FG)
Theme 5: humanity and empathy in psychiatric practice
The performance was widely perceived as a humanising force in psychiatric education. Students described developing a deeper emotional connection to both patients and carers, and many linked the session to broader professional values, such as compassion, humility and moral responsibility:
‘This play […] humanises patients so we move less as viewing them as symptoms and steps on a checklist but looking at patients more as humans with a life, family and ambitions.’ (SS)
‘Medical education kind of posits all disease processes as separate sterile things that occur to other people, when the messy human reality of it is that this is going to touch all of us in different ways.’ (FG)
‘It also raises questions […] that are really deep human questions about why am I a doctor in the first place […] or what is the purpose of medicine?’ (FG)
Discussion
This study evaluated the educational impact of Revolving Door, a forum theatre-based intervention for medical students. The results indicate that the majority of students strongly agreed that forum theatre is a highly effective pedagogical tool for gaining insight into the lived experience of psychosis (mean score: 4.66 out of 5) and the impact on family members (mean score: 4.67). Beyond general effectiveness, the findings suggest that the intervention operates through five distinct mechanisms: accelerating experiential learning, promoting transformative learning, leveraging productive anxiety, restoring epistemic justice and shaping professional identity.
Accelerating experiential learning mechanisms
The dismantling of the ‘fourth wall’, i.e. transforming the passive spectator into a ‘spect-actor’, is central to Boal’s theatre of the oppressed. Reference Boal3 Our respondents rated this interactive element highly (mean score: 4.34). When viewed through Kolb’s experiential learning theory, Reference Kolb9 the intervention appears to uniquely compress the learning cycle.
Kolb posits that learning takes place in a four-stage cycle:
-
(1) concrete experience: having an experience;
-
(2) reflective observation: reviewing/reflecting on the experience;
-
(3) abstract conceptualisation: concluding/learning from the experience;
-
(4) active experimentation: planning/trying out what you have learned.
In traditional curricula, Kolb’s stages are often disjointed. Reference Yardley, Teunissen and Dornan10 A student might engage in abstract conceptualisation during a lecture on Monday, but not encounter the concrete experience of seeing a patient until a clinical placement weeks later. Furthermore, active experimentation is frequently curtailed by safety concerns; students rarely lead high-stakes assessments with patients, limiting them to observation. Reference Yardley, Teunissen and Dornan10
Revolving Door compresses this cycle into a rapid, iterative loop. The play provides the concrete experience; the facilitated discussion drives reflective observation and abstract conceptualisation; and the ‘rewind and replay’ mechanism allows for immediate active experimentation. Students valued the ability to ‘rewrite the ending’ and ‘make mistakes’, suggesting that testing communication strategies in real time is central to the method’s value. This aligns with literature suggesting that drama-based pedagogies allow learners to externalise decision-making, creating rich memory traces through embodied cognition. Reference Arveklev, Berg, Wigert, Morrison-Helme and Lepp11
Transformative learning as a vehicle for change
Whereas Kolb explains skill acquisition, Mezirow’s transformative learning theory best explains the shifts in perspective highlighted in the qualitative feedback. Reference Mezirow12 Mezirow argues that deep learning requires a ‘disorienting dilemma’ – an experience that challenges the learner’s existing frame of reference. Revolving Door creates this dilemma by presenting the medical system as a potential antagonist, challenging the students’ view of clinicians – and, by extension, of themselves – as purely benevolent healers.
Qualitative data from our study reveal that this cognitive dissonance forced students to grapple with the ‘messy human reality’ of practice. By altering the scenario’s outcome, students engaged in the rational discourse necessary to reintegrate this new perspective, viewing themselves not just as clinicians, but as agents of systemic change. Reference Mezirow and J13 Without the shaking of presuppositions, the experience would be distressing rather than transformative; the interactive nature of the forum ensures that the dilemma leads to growth rather than withdrawal. Reference Mezirow and J13
Productive anxiety and psychological safety
Respondents frequently highlighted the role of emotion, specifically anxiety, across all qualitative themes identified. Historically, medical education has viewed anxiety as an impediment to clinical reasoning. Reference Merkebu, Soh, Loncharich, Hawks, Costello and Shapiro14 However, our findings suggest a dichotomy: although some felt ‘daunted’, the majority found the emotional engagement (mean score: 4.40) and display of difficult emotions (mean score: 4.58) essential.
This supports the ‘pedagogy of discomfort’, which argues that leaving one’s comfort zone is necessary to recognise hegemonic norms. Reference Boler, Zembylas and P15 Unlike bedside teaching, where anxiety stems from the fear of causing actual patient harm, Reference Peters and ten Cate16 forum theatre shifts risk to the social domain. Here, the ‘patient’ cannot be injured; instead, the primary risk is the performance anxiety associated with acting in front of peers. This allows students to inhabit a space where collective failure is reframed as necessary. Facilitators balanced this by creating a ‘very supportive’ environment, transforming the anxiety of ‘taking the stage’ into productive vigilance.
Restoring epistemic justice
Revolving Door potentially addresses a critical ethical issue: the validation of patient knowledge. Fricker defines testimonial injustice as the downgrading of a speaker’s credibility owing to prejudice. Reference Fricker17 In psychiatry, patient narratives are often subordinated to the clinician’s ‘objective’ assessment. Reference Ballesteros18
By centring on an authentic narrative, the intervention attempts to restore epistemic agency. Students reported that the play ‘humanises patients’, preventing them from becoming ‘steps on a checklist’. Witnessing the social determinants leading to a crisis forces students to interpret resistance not as pathology, but as a rational response to a frightening system. This counters hermeneutical injustice, defined as the injustice endured by individuals when their experiences do not align with existing popular mental schemas, Reference Ballesteros18 and equips students with the resources to understand the clinical encounter from the patient’s epistemology via the abovementioned transformative learning theory strategies.
Professional identity
Finally, the emotional resonance of the play contributes to the formation of professional identity. Shapiro’s concept of the ‘feeling physician’ emphasises emotional engagement as a clinical skill. Reference Shapiro19 By embodying the psychiatrist during a crisis, students act out ‘becoming a doctor’, moving from passive information gatherers to compassionate practitioners.
Study limitations
Although many found the interactive elements of the intervention empowering, some students reported anxiety around potentially being called on to perform in front of their peers. Such performance anxiety is a recognised challenge in formats such as simulation-based teaching and objective structured clinical examinations. Reference Yu, Chang, Kim, Park, Chung and Lee20 Furthermore, careful thought is required to ensure the psychological safety of the audience. Utilisation of CTFs who have had previous engagement with the students can cultivate safety through familiarity. A play such as this could be potentially anxiety triggering for students, particularly those with lived experience of mental illness. If uncontained, this risks significantly limiting learning. It is the responsibility of facilitators to strike a balance between emotional connection and clinical learning by framing the experience sensitively in the introduction and offering post-production debrief opportunities.
The play highlights how Martin and his family were let down by the healthcare system. This risks reinforcing a binary perception of ‘good’ versus ‘bad’ consultations and clinicians. With experienced facilitation, students can reflect on the systemic pressures and ethical dilemmas faced by clinicians in navigating nuanced perspectives.
Another notable limitation of the study is the lack of longitudinal evaluation to determine whether the use of students’ perceptions is a valid proxy measure for concrete improvement in clinical practice. In addition, to ensure participant anonymity, only the minimum necessary personal information was processed for the study’s specific aims. Without collection of data such as gender and ethnicity, a more granular analysis of how demographic backgrounds may have influenced perspectives on the session could not be undertaken.
Educational implications
This evaluation demonstrates that a forum theatre-based intervention is an effective pedagogical method that supports cognitive understanding, emotional insight and clinical skill development. Its immersive, participatory structure encourages students to practise empathy, navigate uncertainty and reflect on systemic barriers, providing the space to explore professional identity challenges and epistemic injustices. Students are given the opportunity to affirm their shared humanity with the characters in the play, stimulating mutual understanding, which Boal argues is ‘the most powerful weapon’ in catalysing change. Reference Boal3
The convergence between student feedback and facilitator intent suggests that this model has potential to expedite transformative learning in psychiatric education. As future iterations of medical education increasingly prioritise experiential approaches, forum theatre may offer a powerful template for humanising psychiatry.
About the authors
Sian Davies is a higher trainee (Specialty Trainee Year 4, ST4) in forensic psychiatry at the Tamarind Centre, Birmingham and Solihull Mental Health NHS Foundation Trust, Birmingham, UK. Ahmad Kamaleldeen Abdou Mohamed is a higher trainee (ST4) in general adult psychiatry at Church Hill House, Berkshire Healthcare NHS Foundation Trust, Bracknell, UK. Roshni Bahri is a Year 1 Core Trainee (CT1) in general adult psychiatry at Oleaster Hospital, Birmingham and Solihull Mental Health NHS Foundation Trust, Birmingham, UK. Azjad Yasmin Elmubarak is a Trust Grade Doctor at the Zinnia Centre, Birmingham and Solihull Mental Health NHS Foundation Trust, Birmingham, UK. Erin Turner is a consultant psychiatrist and Head of Academy at the Barberry Academy, Birmingham and Solihull Mental Health NHS Foundation Trust, Birmingham, UK. Polly Wright is a playwright and director of The Hearth Centre, Birmingham, UK.
Data availability
The data that support the findings of this study are available from the corresponding author S.D. on reasonable request.
Acknowledgements
We thank past, present and future casts of Revolving Door for their incredible performances and ongoing dedication to medical education.
Author contributions
S.D. was the main author of this paper, with support from R.B., A.K.A.M. and A.Y.E. in writing the manuscript and undertaking quantitative and qualitative analysis. E.T. and P.W. were the supervisors of this project. S.D., A.K.A.M., R.B. and A.Y.E. were Clinical Teaching Fellows involved in facilitating the play and discussion and were present for the focus group.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.


 Open access
Open access
eLetters
No eLetters have been published for this article.