


Background
Older adults represent one of the fastest growing demographic groups globally and in Canada (World Population Prospects 2019 Highlights, n.d.). As this population ages, increasing numbers of older adults require long-term residential care to support complex health, functional, cognitive, and social needs (Ng et al., Reference Ng, Lane, Tanuseputro, Mojaverian, Talarico, Wodchis, Bronskill and Hsu2020). Long-term care (LTC) homes are residential care settings for people who are unable to live independently and who require access to nursing, personal care, support, or supervision (Mitchell et al., Reference Mitchell, Teno, Kiely, Shaffer, Jones, Prigerson, Volicer, Givens and Hamel2009). In Canada, older adults admitted to LTC homes are increasingly functionally dependent and often require assistance with basic activities of daily living, including dressing, walking, transferring, eating, and drinking (Estabrooks et al., Reference Estabrooks, Ewa, Keefe and Straus2023; Ng et al., Reference Ng, Lane, Tanuseputro, Mojaverian, Talarico, Wodchis, Bronskill and Hsu2020). Cognitive impairment, particularly dementia, is a defining characteristic of Canada’s LTC population; about two thirds of residents have a diagnosis of dementia (Estabrooks et al., Reference Estabrooks, Ewa, Keefe and Straus2023; Long-Term Care Residents with Dementia | CIHI, n.d.).
Nutrition care is a particularly important component of daily care in LTC homes because eating and drinking are affected by residents’ physical, cognitive, social, and environmental circumstances (Blumberg et al., Reference Blumberg, Feldman, Murray, Burnes and Murawski2018; Shirai et al., Reference Shirai, Momosaki, Kato, Hori and Maeda2024). Although this study is not limited to residents with dementia, dementia can substantially affect food and fluid intake, mealtime participation, communication, and the level of support required from staff (Douglas et al., Reference Douglas, Jung, Noh, Ellis and Ferguson2021). Eating and drinking challenges are common and affect attention, motivation, recognition of food, motor coordination, swallowing, and ability to initiate or continue eating (Batchelor et al., Reference Batchelor, Smaoui, Passos and Liu2025; Jung et al., Reference Jung, Lee, De Gagne, Lee, Lee, Yoo, Won and Choi2021; Keller et al., Reference Keller, Carrier, Slaughter, Lengyel, Steele, Duizer, Morrison, Brown, Chaudhury, Yoon, Duncan, Boscart, Heckman and Villalon2017). Additionally, behavioural and psychological symptoms related to dementia such as distraction, resistance to assistance, or reduced engagement at meals, may further complicate nutrition care (Aselage & Amella, Reference Aselage and Amella2010).
These nutrition-related challenges often mean that residents require individualized support during meals (Liu et al., Reference Liu, Perkhounkova and Hein2023). In LTC homes, residents may require different levels of support, including verbal prompting, cueing, tray set-up, help opening packages, adaptive strategies, or direct eating assistance (Wu et al., 2017). Residents who require eating assistance are at increased risk of poor intake and malnutrition as compared with residents who eat independently (Jung et al., Reference Jung, Lee, De Gagne, Lee, Lee, Yoo, Won and Choi2021). Therefore, staff knowledge, confidence, and skill in supporting nutrition care are central to residents’ nutrition-related quality of life (Tucker et al., Reference Tucker, Luscombe-Marsh, Ambrosi and Lushington2022).
Nutrition care in LTC includes the provision of food and fluid, assessment and management of nutrition-related conditions, support for food and fluid intake, and educational systems that guide nutrition-related care practices (Cardenas et al., Reference Cardenas, Correia, Ochoa, Hardy, Rodriguez-Ventimilla, Bermúdez, Papapietro, Hankard, Briend, Ungpinitpong, Zakka, Pounds, Cuerda and Barazzoni2021; Volkert et al., Reference Volkert, Beck, Cederholm, Cruz-Jentoft, Goisser, Hooper, Kiesswetter, Maggio, Raynaud-Simon, Sieber, Sobotka, Van Asselt, Wirth and Bischoff2019). Nutrition care is a multidisciplinary responsibility involving registered nurses, personal support workers (PSWs), physicians, registered dietitians, recreation staff, food service staff, and other team members (Ball et al., Reference Ball, Crowley, Laur, Rajput-Ray, Gillam and Ray2014; Yinusa et al., Reference Yinusa, Scammell, Murphy, Ford and Baron2021; Ontario Long Term Care Action Group, 2019). Direct-care staff, including nurses and PSWs, are especially important because they provide day-to-day support with eating, drinking, mealtime routines, and resident engagement (Blumberg et al., Reference Blumberg, Feldman, Murray, Burnes and Murawski2018; Faraday et al., Reference Faraday, Salis and Barrett2019). Despite their central role in nutrition care, LTC staff may feel underprepared to address residents’ complex and individualized nutrition needs (Blumberg et al., Reference Blumberg, Feldman, Murray, Burnes and Murawski2018; Faraday et al., Reference Faraday, Salis and Barrett2019; Nasser et al., Reference Nasser, Cammer, Bandara and Bovee2021).
Education and training may therefore help staff connect nutrition-related knowledge with the realities of daily care in LTC homes. Existing reviews have examined staff training needs, mealtime difficulties, and interventions related to eating assistance (Abbott et al., Reference Abbott, Whear, Thompson-Coon, Ukoumunne, Rogers, Bethel, Hemsley and Stein2013; Chang et al., Reference Chang, Spencer, Ho, Kasa, Ataiza, Lambert and Chang2023; Keller et al., Reference Keller, Carrier, Duizer, Lengyel, Slaughter and Steele2014; Liu et al., Reference Liu, Galik, Boltz, Nahm, Lerner and Resnick2016). However, the literature remains heterogeneous with respect to educational content, delivery format, target staff groups, implementation context, and reported outcomes. In addition, less attention has been given to nutrition education across the full LTC care continuum, including palliative and end-of-life nutrition care (Morrison-Koechl et al., Reference Morrison-Koechl, Heckman, Banerjee and Keller2024).
Given the diversity of existing education and training approaches, a scoping review was appropriate to map the extent, range, and nature of available evidence on nutrition education and training programs for LTC staff. This scoping review aimed to describe how these programs have been designed and delivered, identify the staff groups and LTC contexts represented, summarize the types of outcomes and feasibility-related data reported by included studies, and identify gaps to inform future research and practice.
Methods
This scoping review was conducted in accordance with the JBI methodology for scoping reviews and following the PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) (Peters et al., Reference Peters, Godfrey, McInerney, Munn, Tricco, Khalil, Aromataris, Lockwood, Porritt, Pilla and Jordan2024). The PRISMA-ScR checklist has been included in the Supplementary Materials. This scoping review is also registered with the Open Science Framework (Alizadehsaravi & Keller, Reference Alizadehsaravi and Keller2024). A scoping review design was selected as the literature on nutrition care education and training for LTC staff was expected to be heterogeneous. Outcomes reported in included studies were charted descriptively to show what has been measured and reported in the literature.
Search strategy
Licensed databases
The following databases were searched from May to October 2024: MEDLINE, CINAHL, Scopus, and PsycINFO; an updated search was conducted in September 2025. The search strategy used text and indexing terms to capture the key concepts: educational programs, staff in LTC homes, and nutrition care. Concepts were combined with the Boolean operator AND, and the search terms within each concept were combined with OR. Truncation and phrase symbols were used when appropriate to capture comprehensive results. The search strategy was developed with the assistance of a research librarian at the University of Waterloo. The search strategy with all identified keywords and index terms was adapted for each mentioned database. No date restrictions were applied when the searches were conducted (Supplementary Material – Sample Search).
Grey literature
Guided by the Canadian Agency for Drugs and Technologies in Health Grey Matters Tool, a grey literature search was conducted during May–October 2024 with an updated search conducted in September 2025. The Grey Matter Tool was used as a supplementary search guide to identify potentially relevant non-indexed sources, including reports, practice guidelines, organizational resources, and other publicly available materials related to nutrition care education or training in LTC homes. This approach provided an opportunity to search across both published and unpublished sources relevant to the review question. The search focused on websites and resources related to nutrition care, staff education, and resident engagement in nutrition or mealtime care. The following search terms were used alone and in combination: LTC, nutrition, food, mealtime, education, training, and staff.
Handsearching
The reference lists of the articles included in the review were also screened for additional relevant citations.
Inclusion and exclusion criteria
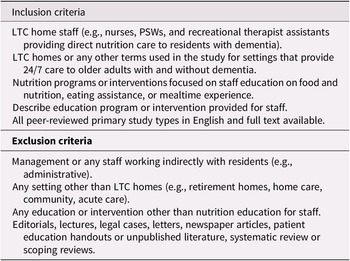
A priori eligibility criteria were set to determine the articles relevant in answering the review’s research questions. The inclusion and exclusion criteria are presented in Table 1 and based on the domains of participants, concept, context, and types of evidence sources, following the guidelines provided in the JBI Manual for Evidence Synthesis (Peters et al., Reference Peters, Godfrey, McInerney, Munn, Tricco, Khalil, Aromataris, Lockwood, Porritt, Pilla and Jordan2024).
Inclusion and exclusion criteria for screening sources of evidence

Table 1. Long description
The table is divided into two main sections.
Inclusion criteria include:
* L T C home staff such as nurses, P S Ws, and recreational therapist assistants providing direct nutrition care to residents with dementia.
* L T C homes or any other terms for settings providing 24/7 care to older adults with and without dementia.
* Nutrition programs or interventions focused on staff education on food and nutrition, eating assistance, or mealtime experience.
* Descriptions of education programs or interventions provided for staff.
* All peer-reviewed primary study types in English with full text available.
Exclusion criteria include:
* Management or any staff working indirectly with residents such as administrative staff.
* Any setting other than L T C homes such as retirement homes, home care, community, or acute care.
* Any education or intervention other than nutrition education for staff.
* Editorials, lectures, legal cases, letters, newspaper articles, patient education handouts, unpublished literature, systematic reviews, or scoping reviews.
Participants
This review included studies involving staff who worked in LTC homes and provided direct nutrition-related care to older adults. LTC staff were identified as individuals providing paid care or services to older adults in LTC homes (Lee et al., Reference Lee, Revelli, Dickson and Marier2022). Eligible staff groups included registered nurses, registered nurse practitioners or licensed practical nurses, registered nursing assistants, PSW, certified nursing assistants, registered dietitians, nutrition managers, food service staff, recreation staff, and other direct-care or mealtime support staff.
Education or training delivered during post-secondary, pre-licensure, or student education programs were not included. Nutrition education programs targeted to and often delivered in the LTC context were the focus as staffing roles, mealtime routines, resident complexity, organizational constraints, and implementation conditions differ from post-secondary classroom or clinical placement education.
Studies that included LTC residents but were not solely based on this area of practice were eligible if the LTC context and outcome measures were reported separately for this group. A specific diagnosis of dementia was not required for inclusion as the review aimed to capture nutrition education programs for LTC staff more broadly. However, studies involving residents living with dementia or cognitive impairment were included because these populations are highly represented in LTC homes and often require nutrition support.
Concept
This review included studies that developed, researched, or evaluated education or training programs related to nutrition care for staff working with older adults in LTC homes. Nutrition education and training programs included structured learning activities designed to support staff knowledge, awareness, confidence, skills, care practices, or implementation of nutrition care. Eligible programs included training sessions, workshops, huddles, coaching, hands-on mealtime support, audit-and-feedback activities, and e-learning. Nutrition education programs were eligible when they addressed one or more nutrition-related topics, including food and fluid intake, malnutrition risk, eating assistance, mealtime support, dining environments, or nutrition screening or assessment education.
Context
The context of this review is rooted in LTC settings, which are defined as residential homes for people who are unable to live independently and require access to nursing, personal care, support, and/or supervision (Canada, Reference Canada2003). The review considered education that was targeted at staff around the nutritional care of LTC residents.
Types of sources
This review considered all primary study designs, including qualitative studies, case studies, mixed methods, before- and after-intervention studies, prospective, longitudinal, retrospective case control, randomized controlled trials, and quasi-randomized clinical or controlled trials. Systematic reviews, rapid reviews, narrative reviews, and scoping reviews were not included in this review. In addition, editorials, clinical commentaries, lectures, legal cases, letters, newspaper articles, patient education handouts or unpublished literature, and articles that were not in English were not included in this review.
Selection of the sources
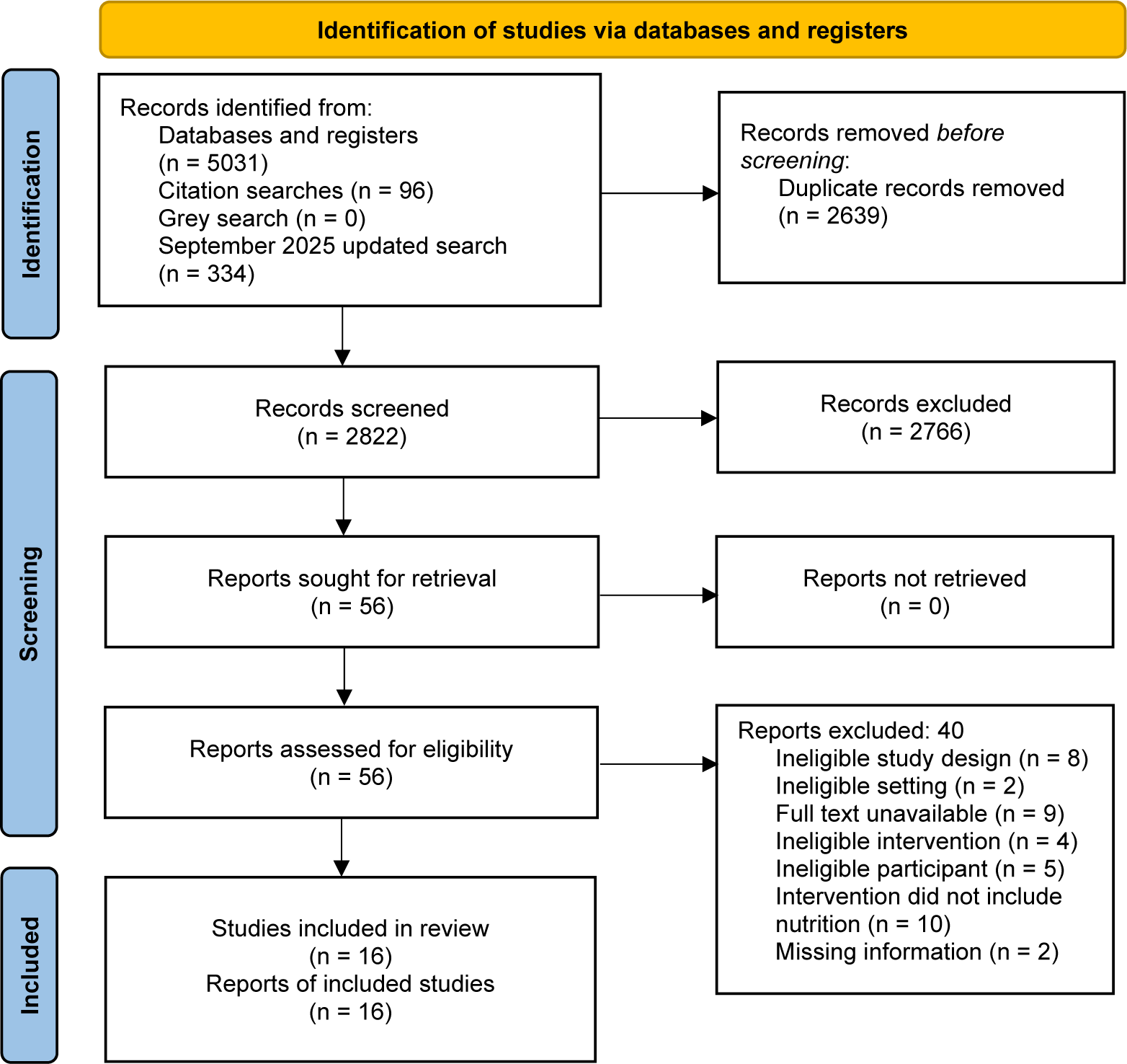
The search and article screening are presented in a chart of search results (Figure 1). After the search was conducted, all identified citations were compiled and uploaded into EndNote 21, where duplicates were removed. Citations were then transferred to Covidence (Veritas Health Innovation, Melbourne, Australia). Titles and abstracts and full-text screenings were completed by three independent reviewers (NA, SHL, and VK) with each article reviewed independently by two reviewers. Discrepancies were resolved in both stages of the screening by a third reviewer (NA). The reasons for excluding articles that did not meet the inclusion criteria were documented and reported (Figure 1).
A P R I S M A flowchart.

Figure 1. Long description
A vertical flowchart organized into three main phases: Identification, Screening, and Included.
1. Identification Phase:
- Top-left box: Records identified from Databases and registers (n = 5031), Citation searches (n = 96), Grey search (n = 0), and September 2025 updated search (n = 334).
- An arrow points right to: Records removed before screening: Duplicate records removed (n = 2639).
- A downward arrow leads to the next phase.
2. Screening Phase:
- Records screened (n = 2822). An arrow points right to: Records excluded (n = 2766).
- A downward arrow leads to: Reports sought for retrieval (n = 56). An arrow points right to: Reports not retrieved (n = 0).
- A downward arrow leads to: Reports assessed for eligibility (n = 56).
- An arrow points right to: Reports excluded: 40. Reasons include: Ineligible study design (n = 8), Ineligible setting (n = 2), Full text unavailable (n = 9), Ineligible intervention (n = 4), Ineligible participant (n = 5), Intervention did not include nutrition (n = 10), and Missing information (n = 2).
3. Included Phase:
- The final downward arrow leads to the bottom box: Studies included in review (n = 16) and Reports of included studies (n = 16).
Data charting
A data extraction form was developed from a template in Covidence and was pilot tested by the review team. Two reviewers independently extracted data from all included articles (NA and VK), with disagreements resolved through discussion. Extracted data included study characteristics (authors, years, country, aim, study design, sample size, and staff roles), nutrition education characteristics (purpose, focus and components, procedures and activities, mode of delivery, materials used, and duration), outcome measures, and main findings.
Data analysis and presentation
Data were summarized using descriptive and narrative approaches. Extracted data were organized into tables describing study characteristics, education and training program characteristics, delivery approaches, outcome measures, reported findings, and feasibility-related data where available. The narrative summary was developed by grouping charted data according to the review questions and JBI scoping review domains, including participants, concept, context, program focus, delivery characteristics, outcome measures, and implementation-related information. No formal thematic analysis was conducted. Feasibility was not a primary outcome of this review. However, feasibility-related data, such as program acceptability, attendance, adherence, delivery mode, resources, duration, and implementation procedures, was extracted when reported by the included studies.
Statistical information, p values, and confidence intervals are included where reported in the articles to describe how outcomes were presented. Clinical significance is reported only when explicitly described by the original authors. This review mapped the extent, range, and nature of available evidence. No formal critical appraisal or risk-of-bias assessment was conducted; therefore, outcome findings are presented descriptively as reported by the included sources.
Results
A total of 5,031 articles were identified during the initial search conducted between May and October 2024. After removing duplicates, 2,639 articles were screened by title and abstract. Following full-text screening, 56 articles remained, with 14 meeting the criteria for inclusion and proceeding to data extraction. Screening the reference lists of the included articles yielded one additional study. The grey literature search did not identify any additional records that met the eligibility criteria.
An updated search conducted in September 2025 identified an additional 334 records. After duplicate removal and screening, one further article met the eligibility criteria and was added to the review. In total, 16 studies were included in this review. The main reasons for exclusion were ineligible study design, participants were not LTC staff, articles were not available as full texts, and the program did not include nutrition education, or it was not implemented in LTC homes. Articles with substantial missing information were excluded if authors did not receive details upon request and the data were not sufficient to confirm whether the educational program included a nutrition component for LTC staff, and whether LTC staff were the target participants, or whether the education was implemented in an LTC home.
Selected characteristics of the included studies are presented in Table 2. Review study references are cited in the Supplementary Material. The 16 included studies were conducted in nine countries: the United States of America (n = 4), Canada (n = 4), Sweden (n = 2), Taiwan (n = 1), Australia (n = 1), Korea (n = 1), Portugal (n = 1), Finland (n = 1), and the United Kingdom (n = 1). The studies were published between 2002 and 2025. Randomized or cluster randomized controlled trial designs were the most frequently reported study designs (n = 6), followed by pre- and post-intervention evaluations (n = 4), mixed methods studies (n = 2), repeated measures studies (n = 2), one stepped-wedge study, and one qualitative feasibility study.
Selected characteristics of included studies

Table 2. Long description
The table contains five columns: Author, year, country; Aim; Method; Sample size; and Staff/participant roles.
* Altus et al., 2002, USA: Explored family-style dining effects on dementia residents. Pre- and post-intervention evaluation. Sample: 5 residents, 1 staff. Roles: C N As.
* Batchelor-Murphy et al., 2015, USA: Enhanced staff knowledge and feeding practices. R C T feasibility study. Sample: 35. Roles: C N As, L P Ns, and R Ns.
* Chang et al., 2006, Taiwan: Developed training for nursing assistants. R C T. Sample: 67. Roles: R N As.
* Chang et al., 2007, USA: Assessed staff knowledge on nutrition. Pre- and post-intervention evaluation. Sample: 39. Roles: N R.
* Christensson et al., 2003, Sweden: Examined education impact on staff attitudes. Pre- and post-intervention evaluation. Sample: 151. Roles: R Ns and R N As.
* Gaskill et al., 2009, Australia: Investigated train-the-trainer program impact. Cluster R C T, 8 sites. Sample: 279 residents, 4 staff. Roles: R Ns.
* Jung et al., 2020, Korea: Assessed mobile app for meal assistance training. Mixed methods. Sample: 23. Roles: C N As.
* Keller et al., 2021, Canada: Evaluated 12-month CHOICE plus program. Stepped-Wedge, 3 sites. Sample: 121 residents. Roles: L P Ns, C N As, R Ds, and nutrition manager.
* Mamhidir et al., 2007, Sweden: Examined integrity-promoting care impact. R C T. Sample: 33. Roles: R Ns and R N As.
* Passos et al., 2025, Portugal: Determined effectiveness of educational intervention. Cluster R C T, 4 sites. Sample: 51 staff, 35 residents. Roles: C N As.
* Perivolaris et al., 2006, Canada: Evaluated dining program training. Repeated measures. Sample: 11 residents, 7 staff. Roles: L P Ns, R Ns, activity aid, and recreation therapist assistant.
* Simmons et al., 2013, USA: Implemented staff training for feeding assistance. R C T. Sample: 130 residents, 57 staff. Roles: R Ns and R N As.
* Suominen et al., 2007, Finland: Evaluated nutrition education in dementia wards. Repeated measures. Sample: 28. Roles: R Ns and food service personnel.
* Watkins et al., 2019, UK: Developed training for social interaction and autonomy. Qualitative feasibility study. Sample: 13. Roles: R N As, activity coordinators, mealtime assistants, chef, and L T C managers.
* Wu et al., 2018, Canada: Evaluated CHOICE mealtime program. Mixed methods. Sample: 64 residents, 16 staff. Roles: Personal support workers, dietary aids, L P Ns, and recreational therapist.
* Wu et al., 2021, Canada: Assessed 1-day Champion Training session. Pre- and post-intervention evaluation. Sample: 34. Roles: R D and nutrition managers.
CNA = certified nursing assistant, LPN = licenced practical nurse, RN = registered nurse, RNA = registered nurse assistant, RD = registered dietitian, NR = not reported.
Description of nutrition education
Participants
Participants included a range of LTC staff involved in nutrition, mealtime, or eating assistance care. Certified nursing assistants, nursing assistants, or personal support workers were included in seven studies. Registered nurses or licensed practical nurses were included in eight studies. Registered dietitians, nutrition managers, or food service personnel were included in four studies. Recreation, activity, or mealtime support staff were included in three studies. LTC managers or administrators were included in two studies. One study did not report the specific staff role of participants.
Eight studies included both staff and resident, while the remaining studies focused primarily on staff and implementation data regarding the nutrition education program. Staff sample sizes ranged from 1 to 151 participants. Resident sample sizes ranged from 5 to 279 residents. All included studies were conducted in LTC homes and involved staff providing care to residents with dementia or cognitive impairment.
Types of nutrition education
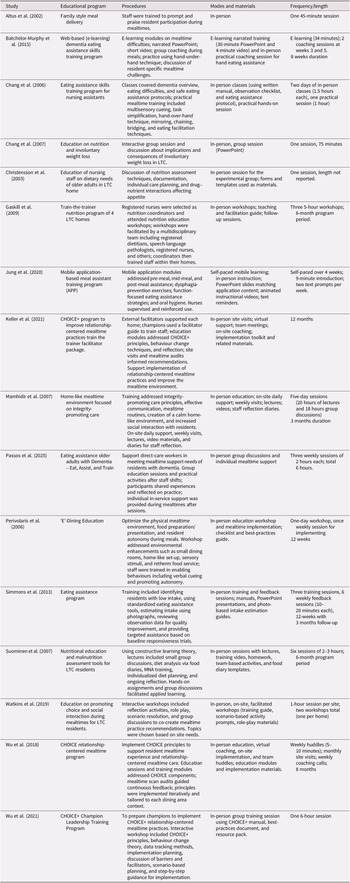
The focus of the nutrition educational program varied across the studies and presented in Table 3. Six studies focused primarily on improving staff knowledge, attitudes, or awareness related to nutrition care delivery (Batchelor-Murphy et al., 2015; Chang et al., 2007a; Christensson et al., 2003a; Gaskill et al., 2009a; Passos et al., 2025; Suominen et al., 2007a). Five studies focused on eating assistance or mealtime support strategies for residents requiring eating assistance (Batchelor-Murphy et al., 2015; Chang et al., 2006a; Jung et al., 2020b; Passos et al., 2025; Simmons et al., 2013a). Five studies focused on enhancing dining environments, mealtime routines, or residents’ mealtime experiences through education or training (Altus et al., 2002; Mamhidir et al., 2007; Perivolaris et al., 2006; Watkins et al., 2019a; Wu et al., 2018). Three studies explicitly incorporated relationship-centered principles into mealtime approaches (Keller et al., 2021a; Wu et al., 2018b; Wu et al., 2021).
Description of study education programs and implementation process

Table 3. Long description
The table contains five columns: Study, Educational program, Procedures, Modes and materials, and Frequency/length.
* Altus et al. 2002: Family style meal delivery. Staff trained to prompt and praise residents. In-person. One 45-minute session.
* Batchelor-Murphy et al. 2015: Web-based dementia eating assistance. E-learning modules and group coaching. E-learning and in-person coaching. 8 weeks duration.
* Chang et al. 2006: Eating assistance skills for nursing assistants. Classes on dementia and practical mealtime training. In-person classes and hands-on sessions. Two 1.5-hour classes and one 1-hour practical session.
* Chang et al. 2007: Education on nutrition and weight loss. Interactive group sessions. In-person PowerPoint. One 75-minute session.
* Christensson et al. 2003: Education on dietary needs. Discussion of assessment and care planning. In-person. One session.
* Gaskill et al. 2009: Train-the-trainer nutrition program. Workshops for registered nurses as coordinators. In-person workshops. Three 5-hour workshops over 6 months.
* Jung et al. 2020: Mobile application-based training. Modules on meal assistance and dysphagia prevention. Self-paced mobile learning and in-person instruction. 4 weeks self-paced.
* Keller et al. 2021: C H O I C E plus program. External facilitators and champions using guides. In-person site visits and virtual support. 12 months.
* Mamhidir et al. 2007: Home-like mealtime environment. Training on integrity-promoting care and communication. In-person lectures and daily support. 5-day sessions over 3 months.
* Passos et al. 2025: Eat, Assist, and Train. Group education and practical activities. In-person group discussions. Three weekly 2-hour sessions.
* Perivolaris et al. 2006: E-Dining Education. Workshops on physical environment and resident autonomy. In-person workshop. One-day workshop and weekly sessions for 12 weeks.
* Simmons et al. 2013: Eating assistance program. Training on intake estimation and standardized tools. In-person training and feedback. 12 weeks with 3 months follow-up.
* Suominen et al. 2007: Nutritional education and malnutrition assessment. Lectures, food diaries, and M N A training. In-person sessions and video. Six sessions over 6 months.
* Watkins et al. 2019: Promoting choice and social interaction. Interactive workshops and role play. In-person facilitated workshops. Two 1-hour workshops.
* Wu et al. 2018: C H O I C E relationship-centered program. Implementation of C H O I C E principles and audits. In-person and virtual coaching. 8 months.
* Wu et al. 2021: C H O I C E plus Champion Leadership Training. Preparing champions for implementation. In-person group training. One 6-hour session.
MNA = mini nutritional assessment, CHOICE = connecting, honouring, offering support, identity, creating opportunities, enjoyment, MTS/MTS+ = mealtime scan.
Delivery of the educational programs
All studies included an in-person component or educational program facilitator implementation activity. Murphy et al. (2015) used web-based e-learning combined with in-person coaching, and Jung et al. (2020b) used a mobile application with text-message reminders and in-person instruction. Four studies used workshops as a main delivery strategy (Gaskill et al., 2009a; Perivolaris et al., 2006; Watkins et al., 2019b; Wu et al., 2021). Four studies included hands-on coaching, mealtime support, or practical application during meals (Batchelor-Murphy et al., 2015; Chang et al., 2006b; Keller et al., 2021a; Wu et al., 2018). Five studies included videos or audiovisual materials (Batchelor-Murphy et al., 2015; Gaskill et al., 2009b; Jung et al., 2020a; Mamhidir et al., 2007; Suominen et al., 2007b), and four studies included lectures or PowerPoint-based presentation lectures (Chang et al., 2007b; Jung et al., 2020b; Suominen et al., 2007b; Mamhidir et al., 2007). Three studies used staff huddles or team-based meetings as part of implementation (Christensson et al., 2003b; Keller et al., 2021a; Wu et al., 2018) and two studies included coaching by a facilitator (Keller et al., 2021a; Passos et al., 2025).
The length of the sessions ranged from 30 minutes to 7 hours. Some studies included reminders, checklists, specific forms, or short summaries of the content that was provided to the participants to encourage their learning (Chang et al., 2006a; Christensson et al., 2003b; Jung et al., 2020b; Keller et al., 2021a; Perivolaris et al., 2006; Simmons et al., 2013a; Wu et al., 2018), whereas others provided extensive guidebooks or instructor manuals (Chang et al., 2005; Simmons et al., 2013; Watkins et al., 2019; Wu et al., 2021). The educational programs were developed and adapted from prior research or were developed solely by the authors. Participant attendance or adherence was measured or reported in some studies (Jung et al., 2020b; Simmons et al., 2013b; Watkins et al., 2019b).
Evaluation and outcome measures
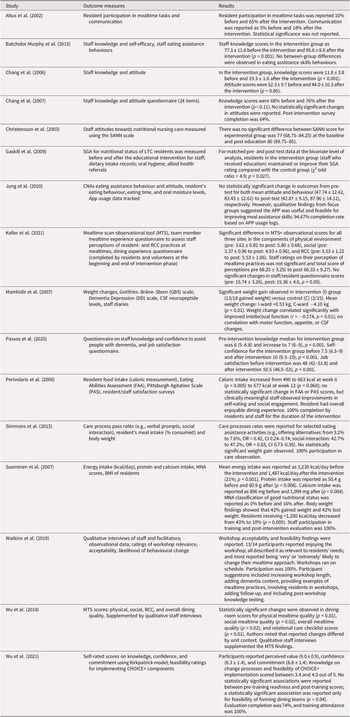
Nutrition education programs outcomes and findings of the studies are presented in Table 4. The included studies reported a range of staff-, resident-, and implementation-related outcomes. Staff-related outcomes included knowledge, attitudes, experience, confidence, self-efficacy, and nutrition or mealtime care practices. Resident-related outcomes included food intake, nutritional status, eating behaviours, meal duration, hydration, and participation during meals. Feasibility-related outcomes were reported less consistently, but some studies described program acceptability, attendance, adherence, perceived usefulness, or implementation considerations. Nine studies reported staff knowledge, attitudes, confidence, self-efficacy, experience, or perceived value as outcomes (Batchelor-Murphy et al., 2015; Chang et al., 2006b; Chang et al., 2007b; Christensson et al., 2003b; Jung et al., 2020a; Keller et al., 2021a; Passos et al., 2025; Suominen et al., 2007b; Watkins et al., 2019a). Five studies reported eating assistance or mealtime assistance practices (Batchelor-Murphy et al., 2015; Chang et al., 2006b; Jung et al., 2020a; Perivolaris et al., 2006; Simmons et al., 2013b). One study reported resident participation and communication during meals (Altus et al., 2002). Seven studies reported resident nutritional status, food intake, body weight, or related eating and hydration outcomes (Altus et al., 2002; Batchelor-Murphy et al., 2015; Gaskill et al., 2009a; Mamhidir et al., 2007; Perivolaris et al., 2006b; Simmons et al., 2013b; Suominen et al., 2007b).
Nutrition education programs outcomes and findings

Table 4. Long description
The table consists of three columns: Study, Outcome measures, and Results.
* Altus et al. 2002: Measured resident participation and communication. Participation increased from 10% to 65% and communication from 5% to 18% post-intervention.
* Batchelor-Murphy et al. 2015: Measured staff knowledge and self-efficacy. Knowledge scores improved from 77.1 plus or minus 11.6 to 95.6 plus or minus 8.6 (p = 0.001).
* Chang et al. 2006: Measured staff knowledge and attitude. Knowledge improved from 11.8 plus or minus 3.8 to 19.3 plus or minus 1.6 (p < 0.001).
* Chang et al. 2007: Measured staff knowledge and attitude via a 24-item questionnaire. Knowledge increased from 68% to 76%.
* Christensson et al. 2003: Measured staff attitudes using the S A N N scale. No significant difference was found (77 baseline to 80 post-education).
* Gaskill et al. 2009: Measured S G A for nutritional status. Intervention group maintained or improved S G A ratings compared to control (p = 0.027).
* Jung et al. 2020: Measured C N A eating assistance behavior and attitude. No significant quantitative changes, but qualitative findings suggested app feasibility.
* Keller et al. 2021: Measured M T S observational scores. Significant improvements in physical environment (3.62 to 5.80), social (3.37 to 4.93), and R C C (3.53 to 5.53).
* Mamhidir et al. 2007: Measured weight and G B S scale. Significant weight gain in intervention group (+0.53 kg) versus control (-4.10 kg, p < 0.01).
* Passos et al. 2025: Measured staff knowledge, confidence, and job satisfaction. All three measures showed statistically significant increases (p < 0.001).
* Perivolaris et al. 2006: Measured caloric intake. Intake increased from 490 to 663 kcal at week 6 (p = 0.005).
* Simmons et al. 2013: Measured care process pass rates. Social interaction increased from 42.7% to 47.2%.
* Suominen et al. 2007: Measured energy, protein, and calcium intake. Energy intake increased from 1,230 to 1,487 kcal/day (p < 0.001).
* Watkins et al. 2019: Qualitative interviews on workshop acceptability. 13 of 14 participants enjoyed the workshop and reported high likelihood of behavioral change.
* Wu et al. 2018: Measured M T S scores. Significant changes in physical, social, and overall mealtime quality (p < 0.02).
* Wu et al. 2021: Measured self-rated knowledge and confidence using the Kirkpatrick model. Participants reported high perceived value (9.0 plus or minus 0.9) and commitment (8.8 plus or minus 1.4).
SANN scale = staff attitudes to nutritional nursing care, SGA = subjective global assessment tool, RCC = relationship-centered care, CAN = certified nursing assistant.
Across the studies, educational programs were commonly reported to be associated with improvement in staff knowledge, skills, confidence, and mealtime assistance practices. Additionally some studies showed improved relationship-centered care (Keller et al., 2021a; Wu et al., 2018b).
Feasibility-related data
Feasibility was not consistently or explicitly evaluated across the studies. However, several studies reported feasibility-related data, including staff attendance, adherence to the activities, acceptability, perceived usefulness, duration, delivery mode, and resources required for implementation. Six studies addressed feasibility through the study design, study aim, or feasibility-related outcome measures (Jung et al., 2020a; Keller et al., 2021a; Simmons et al., 2013a; Watkins et al., 2019a; Wu et al., 2018b; Wu et al., 2021).
Staff knowledge, skills, confidence, and attitudes reported as outcomes
Nine studies reported staff knowledge, skills, confidence, self-efficacy, experience, perceived value, or attitudes as outcomes of nutrition education or training interventions (Batchelor-Murphy et al., 2015; Chang et al., 2006; Chang et al., 2007; Christensson et al., 2003b; Jung et al., 2020a; Keller et al., 2021a; Passos et al., 2025; Suominen et al., 2007b; Watkins et al., 2019a). These interventions addressed topics such as residents’ nutritional needs, malnutrition risk factors, mealtime support, eating assistance, relationship-centered care, and strategies for improving the mealtime environment.
Individual studies reported changes in staff outcomes using different measures. For example, Batchelor-Murphy et al. (2015) reported changes in staff knowledge and self-efficacy scores from pre- to post-intervention. Chang et al. (2006) reported changes in nutrition knowledge scores following staff training and practical coaching. Passos et al. (2025) reported changes in staff knowledge, self-confidence, and intrinsic job satisfaction. Wu et al. (2021) reported staff-rated perceived value, confidence, commitment, and feasibility ratings following CHOICE+ Champion training. Changes in staff attitudes were less consistently reported. Chang et al. (2006), Christensson et al. (2003), and Jung et al. (2020) reported attitude-related outcomes, but findings varied across studies.
Mealtime assistance practices
Five studies reported eating assistance or mealtime care practice outcomes. Reported practices included verbal prompting, offering food alternatives, social interaction during meals, individualized eating assistance, cueing, hand-over-hand or hand-under-hand techniques, and strategies to promote resident autonomy (Batchelor-Murphy et al., 2015; Chang et al., 2006a; Keller et al., 2021a; Wu et al., 2018b).
Nutritional status of the residents
Seven studies reported resident-level outcomes, including nutritional status, food intake, body weight, eating behaviours, meal duration, and hydration (Altus et al., 2002; Batchelor-Murphy et al., 2015; Gaskill et al., 2009a; Mamhidir et al., 2007; Perivolaris et al., 2006b; Simmons et al., 2013b; Suominen et al., 2007b). Resident-level outcomes were not measured consistently across studies. Some studies reported food intake or nutritional status indicators, while others reported weight, mealtime behaviours, hydration-related measures, or participation during meals. The timing of outcome measurement and the tools used also varied.
Relationship-centered mealtime care
Four studies addressed environmental, social, or relational aspects of mealtime care that affect relationship-centered care (Keller et al., 2021a; Perivolaris et al., 2006a; Watkins et al., 2019a; Wu et al., 2018b). Reported outcomes included mealtime environment, social interaction, relationship-centered care indicators, resident participation, staff perceptions, dining quality, and qualitative feedback from staff or facilitators of the educational sessions. The interventions included components such as huddles, coaching, audit-feedback, team-based meetings, reflective activities, and implementation planning. The reported outcomes suggest that studies in this area have examined both observable mealtime environments and staff or resident perceptions.
Discussion
This scoping review mapped the scope, characteristics, and reported outcomes of nutrition education programs delivered to staff working in LTC homes. The included studies varied in educational content, delivery format, duration, staff groups, study design, and outcome measures. Most reported outcomes related to staff knowledge, confidence, mealtime assistance practices, dining environments, and selected resident nutritional outcomes.
There was heterogeneity across the delivery, format, duration, focus, and content. Several nutrition education programs were delivered through brief 15- to 30-minute single-session formats (Altus et al., 2002; Batchelor-Murphy et al., 2015; Chang et al., 2005), whereas others extended over multiple sessions (Christensson et al., 2003; Keller et al., 2021a; Wu et al., 2018; Jung et al., 2020). This variation suggests that nutrition education for LTC staff has been approached in multiple ways, ranging from brief information-focused training to more practice-oriented and team-based models. The diversity of approaches also reflects the complexity of nutrition care in LTC homes, where staff are required to support residents with a wide range of cognitive, functional, behavioural, and nutritional needs.
Across the included studies, staff-related outcomes were commonly reported, including knowledge, skills, confidence, self-efficacy, attitudes, and feeding assistance practices (Altus et al., 2002; Batchelor-Murphy et al., 2015; Chang et al., 2005; Chang et al., 2007; Jung et al., 2020; Suominen et al., 2007; Watkins et al., 2019; Wu et al., 2021). Several studies reported changes in staff knowledge or confidence following educational programs, while others described changes in mealtime assistance behaviours, such as verbal prompting, cueing, offering food alternatives, and tailoring assistance to residents’ individual needs (Batchelor-Murphy et al., 2015; Simmons et al., 2013). The studies differed in the tools used to measure these outcomes, the timing of follow-up, and the extent to which changes were sustained over time. As this review did not include formal critical appraisal, these findings should be interpreted as a descriptive summary of reported outcomes rather than as evidence that particular program components were effective. A review by Mogre et al. (Reference Mogre, Scherpbier, Stevens, Aryee, Cherry and Dornan2016) revealed that nutrition training improved nutrition-related knowledge among healthcare professionals, yet it was insufficient to ensure effective nutrition care delivery (Mogre et al., Reference Mogre, Scherpbier, Stevens, Aryee, Cherry and Dornan2016).
Several studies reported resident-level outcomes, including dietary intake, body weight, malnutrition risk, eating behaviours, meal duration, hydration, and participation during meals (Gaskill et al., 2009; Simmons et al., 2013; Suominen et al., 2007). These outcomes were not consistently measured across studies, and the findings reported by individual studies varied. Some studies described maintained or improved nutritional indicators, while others reported no measurable changes in resident weight, food intake, eating behaviours, hydration, or meal duration. Similarly, in a review evaluating the impact of mealtime interventions for LTC residents, Abbott et al. (Reference Abbott, Whear, Thompson-Coon, Ukoumunne, Rogers, Bethel, Hemsley and Stein2013) reported that there were insufficient data for a meta-analysis of the impact of staff training on resident nutritional status or intake (Abbott et al., Reference Abbott, Whear, Thompson-Coon, Ukoumunne, Rogers, Bethel, Hemsley and Stein2013). Resident outcomes are therefore best understood as part of the range of outcomes reported in the literature, rather than as evidence of impact.
Relationship-centered care in mealtime and nutrition education was also reported in some studies (Keller et al., 2021a; Wu et al., 2018). Relationship-centered care has been incorporated within broader culture change movements in LTC homes, which aim to shift the field towards supporting the multi-directional care of both residents, family, and staff (Dupuis et al., Reference Dupuis, McAiney, Fortune, Ploeg and Witt2016). Central features of this model include fostering a more ‘homelike’ physical environment, prioritizing interpersonal relationships as the basis of care, strengthening staff empowerment, and promoting supportive leadership. This approach is particularly relevant during mealtimes, which represent one of the most frequent and socially meaningful routines in LTC homes. Within LTC homes, this approach is particularly relevant as care is shaped by ongoing interactions, familiarity, trust, and responsiveness to residents’ preferences and needs (Dupuis et al., Reference Dupuis, Gillies, Carson, Whyte, Genoe, Loiselle and Sadler2012; Gurung & Chaudhury, Reference Gurung and Chaudhury2025). Several included studies applied these principles specifically to mealtime environments and nutrition-related care, including programs that incorporated team-based activities, huddles, reflective discussion, and structured feedback (Keller et al., 2021a; Wu et al., 2018; Wu et al., 2021).
Across the included studies, nutrition education programs were delivered using a range of educational approaches, including didactic lectures, printed materials, workshops, facilitated discussions, coaching, reflective activities, huddles, audit–feedback, and technology-enabled formats (Batchelor-Murphy et al., 2015; Chang et al., 2006; Chang et al., 2007; Christensson et al., 2003b; Jung et al., 2020a; Keller et al., 2021a; Passos et al., 2025; Suominen et al., 2007b; Watkins et al., 2019a). These strategies were commonly used to help staff connect nutrition-related knowledge with the practical realities of mealtime care in LTC homes. Some studies also described the importance of aligning training content with staff-identified needs or involving staff in the development or implementation of educational initiatives, which may support relevance and acceptability (Muller-Schoof et al., 2023; Tang et al., 2025). Educational programs that align content with staff-identified needs delivered in person promote deeper learning and more durable behaviour change (Surr et al., 2017).
A notable gap identified in this review was the limited attention to nutrition education related to palliative and end-of-life care in LTC homes. The nutrition education programs identified in this review were oriented towards supporting staff to maintain or improve residents’ nutritional intake, mealtime assistance, dining experience, or nutrition-related knowledge. However, none specifically addressed nutrition education for residents approaching the end of life. Residents, family members, and LTC staff may experience uncertainty around food, fluid, comfort feeding, swallowing changes, appetite decline, and decision making as residents approach end of life. Previous work has also highlighted unmet needs in end-of-life communication and care processes in LTC, including the need for clearer guidance on how and when to provide nutrition care (Banerjee & Rewegan, Reference Banerjee and Rewegan2017; Durepos et al., Reference Durepos, Kaasalainen, Sussman, Parker, Brazil, Mintzberg and Te2018). As such, future nutrition education initiatives should therefore consider how staff can be better supported to provide nutrition care across the full continuum of living and dying in LTC homes (Morrison-Koechl et al., Reference Morrison-Koechl, Heckman, Banerjee and Keller2024).
Strengths and limitations
A strength of this review is the use of a comprehensive search strategy across four licensed databases, grey literature searching, and reference list screening. The search was developed with support from a research librarian and was updated in September 2025, strengthening the currency of the review. The review was conducted using JBI methodology and reported following PRISMA-ScR guidance. Screening and data extraction were completed by independent reviewers, with disagreements resolved through discussion or by a third reviewer.
Several limitations should be acknowledged. The included studies demonstrated substantial heterogeneity in study designs, educational content, program duration, delivery formats, staff groups, resident populations, outcome measures, and reporting styles. This limited direct comparison across studies and supported the use of a descriptive scoping review approach.
No formal critical appraisal or risk-of-bias assessment was conducted. This is consistent with the purpose of this scoping review, which was to map available evidence rather than assess certainty of evidence or determine effectiveness. As a result, the findings should not be interpreted as conclusions about the effectiveness of nutrition education or training programs.
Although grey literature searching was conducted, web-based searches may not fully capture health education programs or quality improvement initiatives implemented in LTC homes. Many nutrition education programs are developed and evaluated internally by LTC organizations, health authorities, or professional groups but may not be written into formal reports, indexed in searchable databases, or made publicly available online. As a result, relevant practice-based education initiatives may have been missed.
Conclusion
This scoping review mapped the available studies on nutrition education and training programs for LTC staff. The studies described a range of program types including lectures, workshops, printed materials, huddles, coaching, e-learning, mobile application training, and reflective activities. Reported outcomes commonly included staff knowledge, confidence, attitudes, eating assistance practices, dining environments, resident-related nutritional status, and feasibility-related indicators. Many studies had short follow-up periods, limiting the ability to describe how long reported outcomes were maintained. Outcome measures varied across studies and sometimes relied on tools that were not clearly described or validated. Nevertheless, significant gaps remain: many studies lack long-term follow-up data to determine sustained change, and few address palliative and end-of-life nutritional care, a critical care context in LTC. Future work should prioritize the development and rigorous evaluation of sustainable, context-sensitive training that equips staff to deliver nutrition care rooted in relationship-centered practice and supported by organizational systems, leadership, and resource investment.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0714980826100786.
Acknowledgments
The authors acknowledge the contributions of the research librarian, Jackie Stapleton for assisting in developing the search strategy at the University of Waterloo.
Author contribution
NA led the development and writing of this scoping review, with critical input and revisions from HK, SL, and VK.
Financial support
This research was conducted without financial support.
Competing interest
The authors declare no competing interest.




 Open access
Open access