


Body composition estimation is an important component of assessing health and disease risks in a clinical setting. However, these estimates can be influenced by normal physiological variations that occur on a daily basis(Reference Rose, Farley and Slater1). A variety of laboratory-based methods have been utilised to assess body composition, with bioelectrical impedance analysis (BIA), dual-energy X-ray absorptiometry (DXA) and air displacement plethysmography (ADP) being among the most widely used. In the general population, the reliability (i.e. reproducibility) of these methods has been examined, typically through simple within-day test–retest assessments(Reference Siedler, Rodriguez and Stratton2–Reference Merrigan, Stute and Eckerle6). However, reliability is known to vary when based on within-day v. between-day assessments, and this variability may not be uniform across assessment technologies. This was observed by McLester et al. (Reference McLester, Nickerson and Kliszczewicz7), who examined the between-day reliability of three multi-frequency BIA (MFBIA) devices as compared with DXA in healthy young adults. While all methods in this study generally displayed strong reliability, the standard error of the measurement values were about 2 to 3 times larger for MFBIA as compared with DXA in males, while females displayed more similar reliability between these methods. Additional technical factors, such as manual v. automated regions of interest (ROI) selection for DXA assessments and electrode placement for bioimpedance devices, have also been shown to influence reproducibility(Reference Lohman, Tallroth and Kettunen8,Reference Vasold, Parks and Phelan9) .
Although the validity of individual methods like DXA, BIA and ADP has been examined in previous studies(Reference Tinsley10–Reference Brewer, Blue and Hirsch12), limited information about the within-day reliability and between-day reliability of these devices has been reported. When repeated measures are conducted immediately back-to-back within the same day (i.e. immediate test–retest), the observed within-day reliability primarily reflects technical error (i.e. error attributable to the device and the assessor), as detectable biological changes do not occur in the negligible time between assessments. Ideally, these measures are performed under standardised conditions (e.g. fasted state, refraining from recent exercise), further minimising biological variation relative to a person’s resting state. In contrast, when reliability is established from repeated assessments taken on different days (i.e. between-day reliability), the total error observed is a combination of technical and biological error (i.e. errors attributable to the device, assessor and biological variation in the body being assessed). Even when assessments are conducted in standardised conditions on the separate days, some degree of day-to-day biological variability is expected. Based on these considerations, the purpose of this study was to examine the test–retest reliability of body fat percentage (BF%), fat-free mass (FFM) and fat mass (FM) estimates from within-day and between-day comparisons utilising a variety of commonly employed laboratory-based methods of body composition assessment.
Methods
Participants and design
A convenience sample of generally healthy adults (defined as having no known disease or other condition that could be negatively affected by participating in the study) were recruited for participation in Lubbock, Texas, USA. Prospective participants were excluded from the study if they were taller than 193 cm or were heavier than 159 kg (due to the limitations of one DXA scanner), were missing any limbs or parts of limbs, had implanted metal due to previous medical procedure, had a pacemaker or electrical implant, had undergone a body-altering surgery (i.e. breast augmentation, liposuction, etc.) or were currently pregnant or trying to become pregnant. Eighteen adults, including eleven females (mean (sd); age = 25·7 (sd 7·5) years; body mass = 63·1 (sd 7·0) kg; height = 167·9 (sd 6·0) cm; BMI = 22·4 (sd 2·3) kg/m2; eight non-Hispanic Caucasian, two Hispanic Caucasian and one Asian) and seven males (age = 30·3 (sd 9·0) years; body mass = 74·2 (sd 12·7) kg; height = 176·4 (sd 9·4) cm; BMI = 23·7 (sd 2·5) kg/m2; four non-Hispanic Caucasian, two Hispanic Caucasian and one Hispanic Black) reported to the laboratory two times, separated by 24–48 h. Within-day reliability was established at the first laboratory visit utilising immediate test–retest assessments for each method under the standardised conditions. Based on the immediate test–retest nature of these assessments, within-day reliability was considered indicative of technical error only. Between-day reliability was established by repeating all the assessments under standardised conditions at the second laboratory visit, conducted on a separate day from the first visit. Between-day reliability was considered indicative of technical plus biological error due to day-to-day biological variation in addition to technical errors of separate assessments. For both visits, participants arrived after following overnight (≥ 8 h) abstention from eating, drinking, exercising and ingesting any alcohol or caffeine. Upon arrival, urine specific gravity was assessed using a digital refractometer (PA201X-093, Misco). Mean (sd) urine specific gravity values were 1·019 (sd 0·004) for visit 1 and 1·019 (sd 0·005) for visit 2. This study was reviewed and approved by the Texas Tech University Institutional Review Board (protocol no: IRB2019-730), and all participants provided written informed consent prior to participation.
Dual-Energy X-ray absorptiometry
DXA scans were performed on GE Lunar iDXA and Lunar Prodigy scanners (GE Healthcare). Nine participants were assessed with each DXA scanner to limit cumulative radiation exposure, with participants randomly assigned to either the iDXA or Prodigy scanner. Both scanners were calibrated daily prior to scanning using the manufacturer-supplied calibration block. Custom-made foam blocks were used to position the participants and ensure consistency for all measures(Reference Nana, Slater and Hopkins13). Foam blocks were placed bilaterally between the hands and the hips, while a strapped block at the feet maintained consistent foot positioning with a perpendicular orientation to the table. At the first visit, participants moved completely off the scanning table between duplicate scans. For each scan, a copy of DXA reports with automated ROI was saved. Thereafter, the same trained operator manually adjusted ROI lines within the software to indicate body segments (i.e. arms, trunk and legs). The automated and manual versions were analysed separately. DXA has previously been validated against a criterion four-compartment model for body composition, demonstrating strong group-level agreement(Reference Williams, Wells and Wilson14).
Multi-Frequency bioelectrical impedance analysis
Two MFBIA analysers were used (mBCA 515/514, Seca® GmbH & Co.; InBody 770, Biospace Co.). The Seca® analyser utilised a 19-frequency, eight-point design, with contact electrodes for the hands and bare feet, and was conducted in the standing position. The frequencies utilised for this device ranged from 1 to 1000 kHz, along with a measuring current of 100 µa. This analyser has been validated against a four-compartment model for body composition(Reference Bosy-Westphal, Schautz and Later15). For the InBody analyser, participants stood barefoot with their feet positioned on the contact electrodes, while subjects held the designated handles with additional contact electrodes in both hands. Thirty impedance measurements with frequencies ranging from 1 to 1000 kHz were employed. The InBody 770 has previously demonstrated good test–retest reliability for BF%, FFM and FM in healthy men and women(Reference McLester, Nickerson and Kliszczewicz7). At the initial visit, the Seca MBFIA analyser was first performed twice in a row, without moving the participant, to determine the error derived from the device itself. The participant was then repositioned (i.e. stepped off and then stepped back on the device), and the test was repeated to determine the additional error of repositioning. This procedure was not possible for the InBody analyser due to the requirement to clear the scale before each test.
Bioimpedance spectroscopy
Bioimpedance spectroscopy (BIS; SFB7, ImpediMed) was utilised in conjunction with the manufacturer-specified hand-to-foot electrode arrangement and was calibrated daily using a manufacturer-supplied testing cell. Each participant remained supine for approximately three minutes immediately prior to BIS assessment. Before placing the electrodes, the electrode sites on the hands, wrist, foot and ankle were cleaned with alcohol pads. In accordance with the manufacturer guidelines, the BIS electrodes were placed unilaterally on the right side of the body. Before beginning the assessment, the participants’ limbs were spread apart to ensure there was no contact with other parts of the body. During the assessment, participants remained motionless in the supine position. Bioelectrical output was processed using manufacturer-provided software, and Cole-Cole plots were reviewed for quality assurance. The coefficients utilised for males (ρe = 273·9, ρi = 927·2) and females (ρe = 235·5, ρi = 894·2), as well as body density, body proportion and hydration values (1·05, 4·30 and 0·732, respectively), were the same utilised in previous investigations(Reference Moon, Smith and Tobkin16–Reference Tinsley, Moore and Benavides18). At the first visit, duplicate assessments were performed with the same set of adhesive electrodes, without removing the electrodes, to establish the technical error of the analyser itself. Then, the first set of electrodes was discarded and replaced with a new set, and the test was repeated to determine the additional error derived from a second set of adhesive electrodes (i.e. a new set of electrodes plus positioning by the researchers). Studies(Reference Moon, Smith and Tobkin16,Reference Moon, Tobkin and Roberts17) utilising the same analyser have demonstrated the validity of BIS, which estimates total body water through Cole modelling(Reference Cole19) and mixture theories(Reference Hanai and Sherman20), as compared with deuterium dilution.
Single-Frequency bioelectrical impedance analysis
The single-frequency BIA (SFBIA) analyser (Quantam V, RJL Systems) was tested daily before any measurement using a manufacturer-supplied testing cell. The total body water estimates from this SFBIA analyser, which are subsequently used to estimate body composition, have been validated against a deuterium oxide criterion(Reference Tinsley, Park and Saenz21). Participants rested in the supine position for approximately 5 min prior to the assessment. The SFBIA analyser used an eight-point bilateral, hand-to-foot electrode configuration. Prior to placing the electrodes, the electrode sites on the hands, wrist, foot and ankle were cleaned with alcohol pads. In accordance with the manufacturer guidelines, the electrodes were placed on the dorsal surface of both hands and feet. Before beginning the assessment, the participants’ limbs were spread apart to ensure there was no contact with other parts of the body. During the assessment, participants remained motionless in the supine position and bioelectrical output was processed using manufacturer-provided software. At the first visit, duplicate assessments were performed with the same set of adhesive electrodes, without removing the electrodes, to establish the technical error of the analyser itself. Then, the first set of electrodes was discarded and replaced with a new set, and the test was repeated to determine the additional error derived from a second set of adhesive electrodes (i.e. a new set of electrodes plus positioning by the researchers).
Air displacement plethysmography
ADP (BOD POD Cosmed USA) was performed in accordance with manufacturer recommendations and default software. ADP has previously demonstrated similar body density values to that of hydrostatic weighing and is generally considered a valid technique when compared with a four-compartment model(Reference Fields, Wilson and Gladden22–Reference Millard-Stafford, Collins and Evans24). To ensure that values were consistent, two to three volume measurements were obtained and used for analysis. Thoracic gas volume (TGV) was measured using the manufacturer’s procedures. Versions of the results with measured and predicted TGV were used for analysis. The Siri(Reference Siri25) equation was used to estimate body composition through the manufacturer’s software. Due to technical problems or missing data for some assessments, the sample size for the ADP analysis was 14.
Statistical analysis
Data analysis was performed using R (v. 4.5.1). Test–retest reliability was established using intraclass correlation coefficients (ICC; model 2,1 from the DescTools package (v. 0.99.60)), the absolute technical error of measurement (TEM; i.e. precision error) and the relative TEM (i.e. root-mean-square CV). The absolute TEM was calculated as
 $\sqrt {{{\sum {{D^2}} } \over {2n}}}$
where D is the difference between repeated measurements and n is the sample size. The relative TEM was calculated as the absolute TEM divided by the grand mean for the variable in question, multiplied by 100. To determine the within-day errors (i.e. technical error), the differences between consecutive tests at the first laboratory visit were used to calculate the aforementioned metrics. To determine the between-day errors (i.e. technical plus biological error), the differences between tests conducted at the first (i.e. the first measurement from the first visit) and second laboratory visits were used. All reliability metrics were calculated for BF%, FM and FFM, except that relative TEM values are not presented for BF% due to this variable already being presented in percentage units.
$\sqrt {{{\sum {{D^2}} } \over {2n}}}$
where D is the difference between repeated measurements and n is the sample size. The relative TEM was calculated as the absolute TEM divided by the grand mean for the variable in question, multiplied by 100. To determine the within-day errors (i.e. technical error), the differences between consecutive tests at the first laboratory visit were used to calculate the aforementioned metrics. To determine the between-day errors (i.e. technical plus biological error), the differences between tests conducted at the first (i.e. the first measurement from the first visit) and second laboratory visits were used. All reliability metrics were calculated for BF%, FM and FFM, except that relative TEM values are not presented for BF% due to this variable already being presented in percentage units.
Results
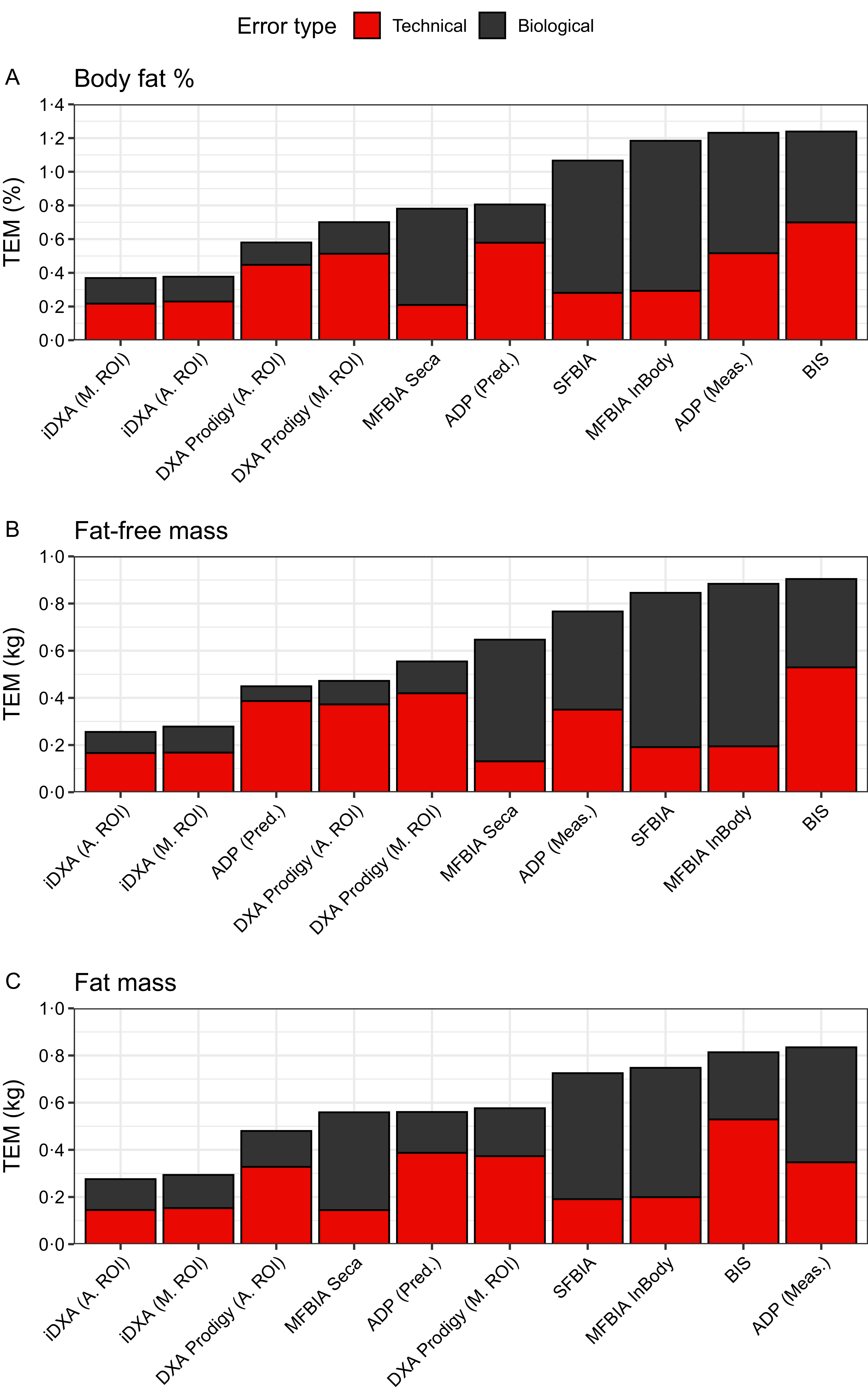
A combined visual summary of each method’s performance, including within-day (technical error) and between-day (technical plus biological error) measurement error, is displayed in Figure 1.
The technical and biological errors of each body composition estimation method, as indicated by the technical error of measurement (TEM), for body fat percentage (a), fat-free mass (b) and fat mass (c). The technical plus biological error, indicated by the total height of each bar, was established from between-day comparisons, while the technical error was established from within-day comparisons. DXA, dual-energy X-ray absorptiometry; A.ROI, automated regions of interest; M.ROI, manual regions of interest; MFBIA, multi-frequency bioelectrical impedance analysis; S.P., same placement; R., repositioned; BIS, bioelectrical impedance spectroscopy; S.E., same electrode; D.E., different electrode; SFBIA, single-frequency bioelectrical impedance analysis; ADP, air displacement plethysmography; Meas., measured; Pred., predicted.

Body fat percentage
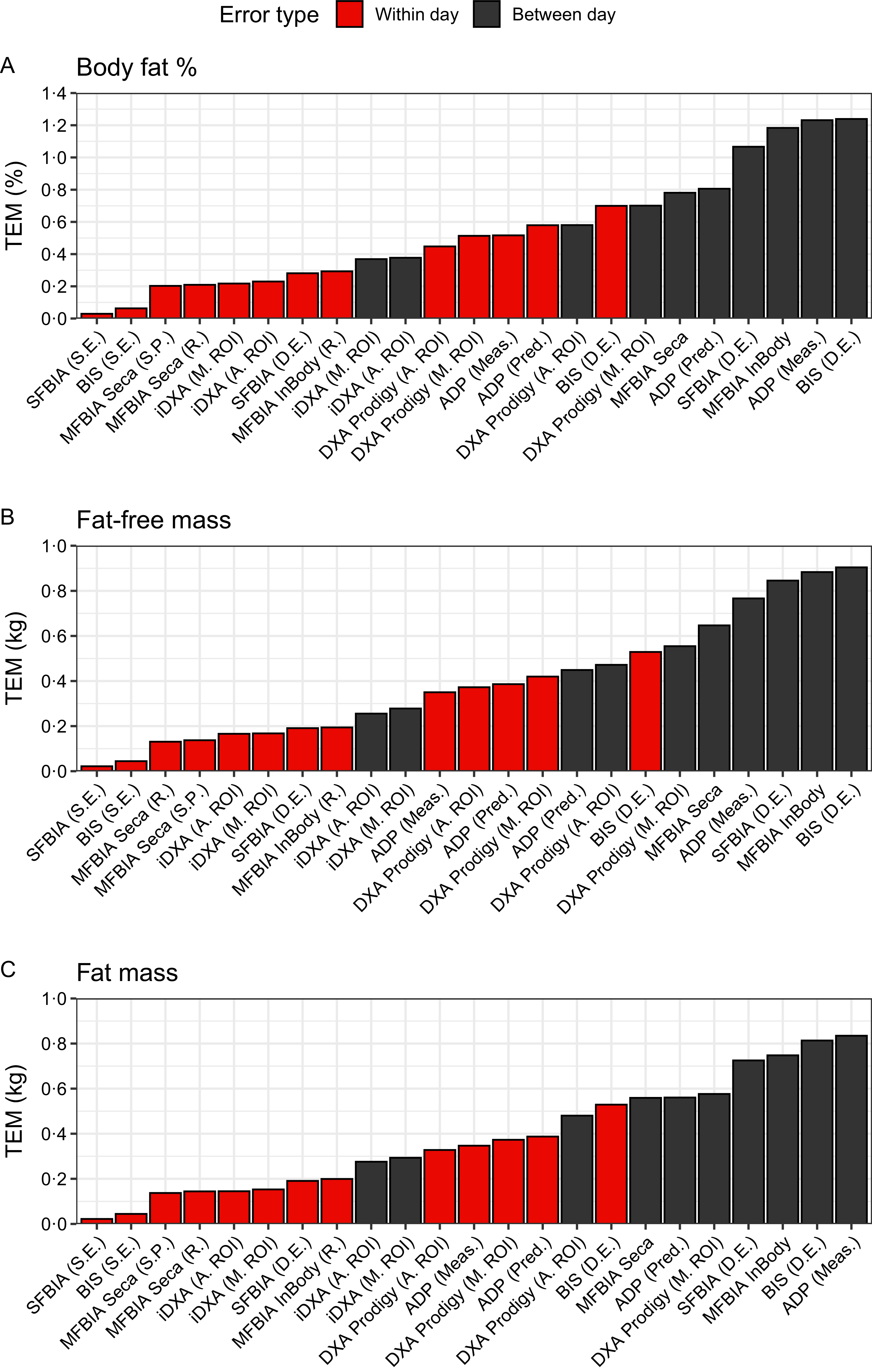
Across all within-day results for BF%, the SFBIA and BIS analysers with the same electrodes for duplicate assessments exhibited the lowest absolute TEM of 0·03–0·06 % (Table 1). Absolute TEM for within-day BF% errors ranged from 0·03 to 0·70 % across methods (Figure 2(a)). All within-day BF% measures demonstrated high reliability based on their ICC (ICC = 0·993–1·000). Moreover, for between-day errors in BF%, the iDXA with manual or automatic ROI exhibited the lowest absolute TEM of 0·37–0·38 %, while BIS displayed the greatest absolute TEM of 1·24 % (Table 1; Figure 2(a)). Between-day ICC for BF% ranged from 0·980 to 0·998 (Table 1).
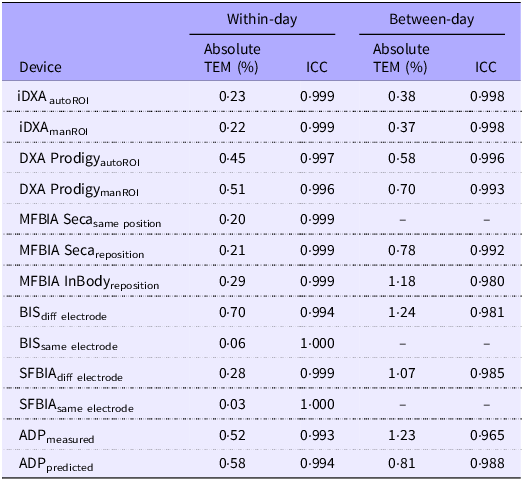
Reliability of body fat percentage estimates from laboratory-based body composition methods for within- and between-day measures

TEM, technical error of measurement; ICC, intraclass correlation; DXA, dual-energy X-ray absorptiometry; autoROI, automated regions of interest; manROI, manual regions of interest; MFBIA, multi-frequency bioelectrical impedance analysis; BIS, bioelectrical impedance spectroscopy; SFBIA, single-frequency bioelectrical impedance analysis; ADP, air displacement plethysmography.
Relative TEM values were not calculated since body fat percentage is already expressed in percentage units. Between-day assessments for select variables were not possible (i.e. duplicate assessments with the same pair of electrodes or without repositioning).
The within-day and between-day technical error of measurement (TEM) for body fat percentage (a), fat-free mass (b) and fat mass (c) for all body composition estimation techniques. DXA, dual-energy X-ray absorptiometry; A.ROI, automated regions of interest; M.ROI, manual regions of interest; MFBIA, multi-frequency bioelectrical impedance analysis; S.P., same placement; R., repositioned; BIS, bioelectrical impedance spectroscopy; S.E., same electrode; D.E., different electrode; SFBIA, single-frequency bioelectrical impedance analysis; ADP, air displacement plethysmography; Meas., measured; Pred., predicted.

Fat-Free mass
For FFM, absolute TEM for within-day measures ranged from 0·02 to 0·53 kg (Table 2), with the SFBIA and BIS analysers with the same electrodes for duplicate assessments exhibiting the smallest amount of error (0·02–0·04 kg) and BIS with different electrodes displaying the largest amount of error (0·53 kg). The within-day relative TEM for FFM ranged from 0·04 to –1·01 % (Table 2). All methods exhibited high within-day reliability (ICC = 0·992–1·000).
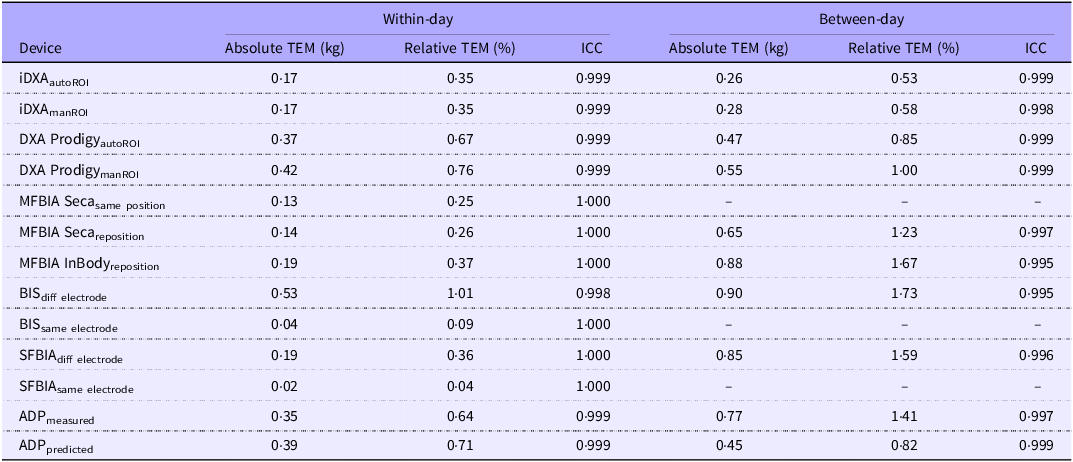
Reliability of fat-free mass estimates from laboratory-based body composition methods for within- and between-day measures

TEM, technical error of measurement; ICC, intraclass correlation; DXA, dual-energy X-ray absorptiometry; autoROI, automated regions of interest; manROI, manual regions of interest; MFBIA, multi-frequency bioelectrical impedance analysis; BIS, bioelectrical impedance spectroscopy; SFBIA, single-frequency bioelectrical impedance analysis; ADP, air displacement plethysmography.
The lowest absolute TEM for FFM between days was observed for iDXA with manual or automatic ROI (0·26–0·28 kg), and the largest error was observed for BIS (0·90 kg; Figure 2(b)). The relative TEM for FFM between days ranged from 0·53 to 1·73 % with ICC of 0·995–0·999.
Fat mass
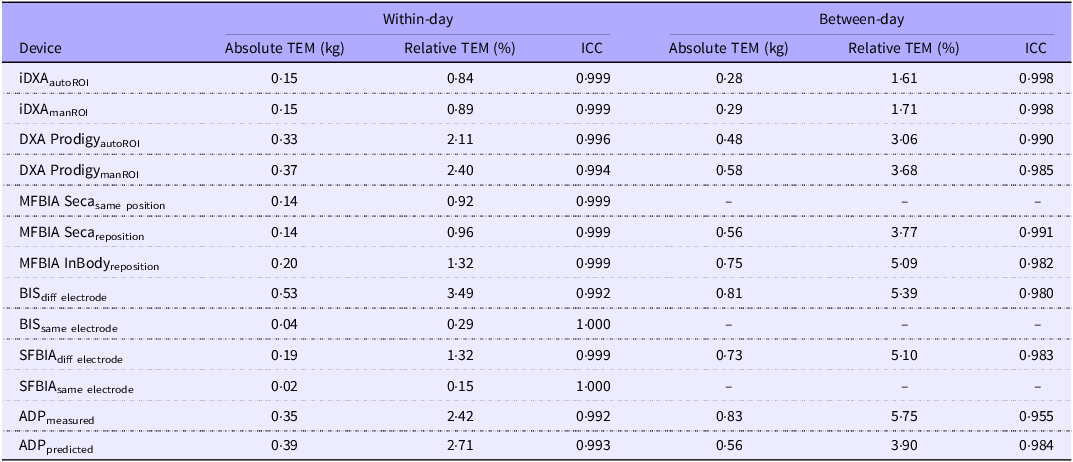
For within-day FM comparisons, absolute TEM ranged from 0·02 to 0·53 kg, while between-day values ranged from 0·28 to 0·83 kg (Table 3; Figure 2(c)). The relative TEM for within-day measurements ranged from 0·15 to 3·49 % and from 1·61 to 5·75 % for between-day measures (Table 3). Both between-day and within-day measures exhibited high ICC (0·992–1·000; 0·955–0·998) for all methods.
Reliability of fat mass estimates from laboratory-based body composition methods for within- and between-day measures

TEM, technical error of measurement; ICC, intraclass correlation; DXA, dual-energy X-ray absorptiometry; autoROI, automated regions of interest; manROI, manual regions of interest; MFBIA, multi-frequency bioelectrical impedance analysis; BIS, bioelectrical impedance spectroscopy; SFBIA, single-frequency bioelectrical impedance analysis; ADP, air displacement plethysmography.
Discussion
The purpose of this study was to examine the within-day and between-day test–retest reliability of body composition estimates using a variety of commonly employed laboratory-based methods. Prior studies have typically examined the reliability of laboratory-based body composition devices within a single day(Reference Fornetti, Pivarnik and Foley4–Reference Merrigan, Stute and Eckerle6) or between days(Reference McLester, Nickerson and Kliszczewicz7,Reference Vasold, Parks and Phelan9,Reference Schubert, Seay and Spain26) , but few studies have incorporated both, thereby allowing for the separation of technical error (variability attributable to the device and assessor) from biological errors (variability due to biological variation in the body being assessed). Distinguishing between these sources of measurement error allows for a clearer determination of whether body composition changes are likely due to true physiological changes or measurement error (i.e. data ‘noise’). In the present study, an overall comparison of between-day reliability reflective of technical plus biological errors indicated that reliability was highest for the iDXA scanner (TEM < 0·4 % for BF% and < 0·3 kg for FM and FFM), followed by the Prodigy DXA scanner, the Seca MFBIA analyser and ADP with predicted TGV (TEM ≤ 0·81 % for BF% and ≤ 0·65 kg for FM and FFM) – in varying order depending on the body composition variable. The InBody MFBIA analyser, ADP with measured TGV, SFBIA and BIS displayed the highest TEM values for all variables (< 1·25 % for BF% and ≤ 0·9 kg for FM and FFM), although these were still relatively low. Additional findings were as follows: (1) for DXA, ADP with predicted TGV and BIS, more of the overall error was classified as technical as opposed to biological; in contrast, more error was attributed to biological factors for both MFBIA analysers, SFBIA and ADP with measured TGV; (2) bioimpedance analysers with adhesive electrodes (SFBIA and BIS) displayed the smallest absolute and relative TEM for BF%, FFM and FM for within-day measurements when the electrodes were not replaced, indicating negligible error of the analysers themselves; (3) BIS with different electrodes displayed the highest TEM for within-day measurements, indicating that the adhesive electrodes and their placement may be an important source of technical error for this technique; (4) measured TGV for ADP slightly decreased TEM values for within-day measurements, but between-day TEM values were lower when using predicted TGV and (5) manual v. automated ROI segmentation for DXA minimally influenced reliability.
In a previous study conducted by Schubert et al. (Reference Schubert, Seay and Spain26) in predominantly normal-weight and overweight young adults, the authors examined the between-day reliability of laboratory-based body composition devices (i.e. DXA (Lunar Prodigy), ADP with predicted TGV and MFBIA (InBody 720)) compared with a four-compartment model of estimating body composition. This study displayed high between-day reliability for each device when estimating BF%, FFM and FM, with ICC ranging from 0·973 to 0·997. In our current investigation, DXA was the best-performing technology based on the absolute TEM for between-day reliability of all body composition estimates (absolute TEM of 0·26–0·58 kg for FM and FFM and 0·37–0·70 % for BF%), followed by ADP with predicted TGV (absolute TEM of 0·45–0·56 kg for FM and FFM and 0·81 % for BF%), with InBody MFBIA exhibiting the largest amount of error of these three methods (absolute TEM 0·75–0·88 kg for FM and FFM and 1·18 % for BF%). A similar pattern was also observed when examining ICC values for each method and body composition outcome. Previous studies that have examined the technical plus biological error (i.e. between-day error) of body composition techniques have reported DXA having a low amount of estimation error for FFM and FM in a variety of populations, including healthy young adults, resistance-trained individuals and individuals across the age span(Reference Rose, Farley and Slater1,Reference Schubert, Seay and Spain26–Reference Zemski, Hind and Keating28) . Similarly, in our current investigation, the iDXA scanner displayed the lowest errors for FFM and FM estimates, and both the iDXA and Prodigy scanners displayed a low amount of biological error for BF% estimates. For DXA, it has been hypothesised that the reliability may depend on the method of ROI analysis. Lohman et al. (Reference Lohman, Tallroth and Kettunen8) reported that manual ROI improved between-day reproducibility of appendicular values compared with automated ROI in healthy males. In our present analysis of the reliability of total body values, differences between manual and automated ROI were small. For FM and FFM, the automated ROI produced marginally lower between-day TEM values for both DXA scanners. For BF%, the TEM were virtually identical for the iDXA scanner, with the automated ROI demonstrating a slightly lower TEM for the Prodigy scanner. Collectively, these results indicate that the choice of automated v. manual ROI may not meaningfully influence the reliability of DXA total body composition estimates, although the additional consideration of the reliability of segmental estimates may be warranted for studies tracking changes in specific body regions.
In addition to DXA, two MFBIA devices – the InBody770 and Seca 515/514 – were included in the present investigation. A previous study directly comparing GE iDXA to an InBody analyser found that the InBody 770 demonstrated high between-day reliability for BF%, FFM and FM for both males and females with ICC ranging from 0·98 to 1·00, although the standard error of the measurement values were larger for the InBody 770 as compared with iDXA(Reference McLester, Nickerson and Kliszczewicz7). In the current analysis, the Seca 515/514 MFBIA displayed smaller errors across both within- and between-day measures, as compared with the InBody MFBIA analyser, with minimal differences when performing assessments without participant repositioning v. repositioning (for the within-day analysis). Moreover, a prior investigation using the Seca mBCA 515/514 reported that the device demonstrated good within-session reliability with a CV of 0·99 for BF%(Reference Merrigan, Stute and Eckerle6). Overall, the modern vertical bioimpedance analysers with contact electrodes evaluated in the present study generally demonstrated strong reliability, with some differences in performance between specific models.
Prior research has also examined the performance of traditional supine SFBIA devices, like the RJL Quantum analyser included in the present study. Based on the technical differences as compared with MFBIA (e.g. supine v. standing body position and adhesive v. contact electrodes), the reliability of such SFBIA analysers may be expected to differ. In a study performed by Vasold et al. (Reference Vasold, Parks and Phelan9), the authors reported that the RJL SFBIA displayed a high reliability for between-day measures of FFM estimates (ICC = 0·994), which was similar to the ICC in our current investigation for between-day measures (ICC = 0·996). However, we observed notably higher errors for between-day assessments compared with within-day assessments (within-day absolute TEM BF% = 0·28 %, FFM = 0·19 kg, FM = 0·19 kg; between-day absolute TEM BF% = 1·07 %, FFM = 0·85 kg, FM = 0·73), highlighting the contribution of biological errors when using this method. Interestingly, although the BIS analyser used in the present study exhibits similar characteristics to SFBIA (i.e. supine body position and adhesive electrodes), more of the cumulative error for BIS was categorised as technical rather than biological. From within-day evaluations, it was evident that the BIS analyser itself was responsible for very limited technical error, indicating the important contribution of the electrodes and their placement to the error of this method. Since longitudinal assessments will inherently require different electrodes, it is important to note the relatively large amount of technical error from this source, which will increase the magnitude of change in BF%, FFM and FM that must be observed to exceed the method’s error. Collectively, the SFBIA and BIS analysers themselves produced little error, but biological factors and the placement of new electrodes contributed varying amounts of error across these seemingly similar technologies.
Unlike SFBIA and BIS, where electrode placement can significantly affect the outcomes, ADP offers a non-contact alternative that has been evaluated for its within- and between-day reliability(Reference Schubert, Seay and Spain26). In a prior study, ADP demonstrated good within-day reliability for estimates of BF%, FFM and FM, with ICC of 0·973, 0·992 and 0·975, respectively. Similarly, another investigation that examined between- and within-day reliability of ADP demonstrated trivial typical error for FFM (relative TEM of 0·5–1·5 %) and moderate to substantial typical error for FM (relative TEM 3·4–3·6 %)(Reference Kerr, Slater and Byrne27) – values that are generally comparable to the present investigation. Moreover, Tucker et al. (Reference Tucker, Lecheminant and Bailey5) assessed the within-day test–retest reliability of BF% estimates from ADP in a large sample of middle-aged women, and the results indicated good test–retest reliability with an ICC of 0·998. Overall, the present results indicate that ADP demonstrates generally strong reliability, with superior between-day consistency observed when using predicted rather than measured TGV.
From a practical perspective, individuals performing body composition assessments should consider calculating and reporting the TEM, or a similar metric, for all devices within their own facility to better contextualise longitudinal changes in body composition. Establishing these facility-specific error thresholds can help determine whether observed changes in body composition reflect meaningful physiological adaptations or fall within the expected measurement variability. In this respect, the between-day error – including technical and biological errors – could be conceptualised as the magnitude of change that would need to be exceeded for a change to be considered meaningful. While the values presented in the current study provide some context for these values for several common assessment methods, the generally strong reliability displayed in the current investigation may not be reflective of performance in other settings, particularly when there is less control over pre-assessment standardisation of patients. Each method used within the current investigation is potentially susceptible to additional measurement error that may occur in a real-world environment. All methods are subject to greater technical error when inconsistent quality control (e.g. calibration), positioning and testing procedures are employed. All may also be subject to biological variability due to food and fluid ingestion and recent exercise, although the extent to which this impacts estimates can vary by method(Reference Tinsley, Harty and Stratton29,Reference Rodriguez, Florez and Prather30) . Some biological factors – such as skin temperature, clothing and body hair – may affect ADP in particular(Reference Higgins, Fields and Hunter31). BIA methods are particularly sensitive to hydration status, recent food or fluid intake when analysers include a built-in scale, and skin or environmental temperature, among other factors(Reference Kyle, Bosaeus and De Lorenzo32,Reference Tinsley, Stratton and Harty33) . For practitioners and clinicians, this information highlights the importance of patients adhering to pre-testing standardisation procedures whenever possible, including reporting for evaluation after an overnight fast or consistent time of day, refraining from physical activity and controlling fluid consumption to promote appropriate hydration status while avoiding errors from recent intake. Less consistent implementation of pre-testing guidelines, such as may occur in real-world testing environments, is expected to introduce more variability in each assessment, thereby worsening the between-day reliability of the techniques. Likewise, any individuals incorporating body composition methods (i.e. practitioners, clinicians and scientist), should be properly trained to ensure consistent device operation and reduce technical errors. Ultimately, facility-specific testing under realistic testing conditions, even when these conditions do not meet the typical best practices, is the best way to obtain reliability information to inform what constitutes a meaningful change in the specific testing context.
Some additional considerations should be taken into account when interpreting the results of the present study. The menstrual cycle was not controlled when scheduling study visits. However, a previous study(Reference Hicks, McLester and Esmat34) has noted the menstrual cycle having no significant influence on body composition results obtained by DXA, ADP and BIA. Additionally, the very short duration of the present study minimised the influence of potential changes for the between-day assessments. Nonetheless, the menstrual cycle may be a scheduling consideration for future longitudinal work. Additional research under less controlled field conditions and in populations with differing health status and clinical characteristics is warranted, as both considerations may further influence measurement error. These investigations should include an examination of the performance of methods across a diversity of body sizes and demographic characteristics due to the potential impact of these factors on method reliability. While the present sample included individuals with BMI values of 18·5–28·0 kg/m2, future work in those defined as having obesity based on BMI would further inform body composition assessment in this population. In general, some body composition methods demonstrate relative stability of performance across a wide range of body sizes, while others may be more susceptible to errors based on body size. These differences may be attributable to the different biophysical principles leveraged by each technique, as well as differences in manufacturer-specific algorithms. The present findings help establish the relevance of inter-device variability, but the findings should be further confirmed in individuals with obesity.
In conclusion, generally strong reliability of laboratory-based body composition methods was demonstrated for both within- and between-day estimates of BF%, FFM and FM. Differences in the amount of technical and biological error across broad technologies and specific devices were observed. Several methodological considerations and procedural variations were examined, and it was determined that some had measurable impacts on error (e.g. placement of adhesive electrodes for bioimpedance techniques and use of measured v. predicted TGV for ADP), while others exerted minimal impact (e.g. manual v. automated ROI for DXA). Importantly, the present results may represent a ‘best-case’ scenario, indicative of controlled research settings but not all real-world clinical environments. Investigators should employ appropriate caution when interpreting longitudinal body composition changes, considering the technical and biological errors of the specific technology being used. Ultimately, while some methods demonstrated superior between-day performance (e.g. iDXA and Prodigy DXA scanners, Seca MFBIA and ADP with predicted TGV), the choice of method should also be guided by the practicality of implementing these devices in the selected clinical or research setting.
Acknowledgements
The authors would like to acknowledge Jake Boykin, Dale Keith, Jacob Green, Sarah White, Abegale Betrus, Brielle Dehaven and Jacob Dellinger for their assistance with the original project yielding the data used in the present analysis. The authors would also like to thank the participants who volunteered their time to complete this study.
No specific funding support was received for this project. General laboratory funds were provided by Texas Tech University.
Conceptualisation: G. M. T.; Data curation: C. M. V., C. M. F., C. R., M. R. S., M. T. S. and P. S. H.; Formal analysis: G. M. T.; Investigation: C. R., M. R. S., M. T. S. and P. S. H.; Methodology: C. R., M. R. S., M. T. S., P. S. H. and G. M. T.; Project administration: C. M. V., M. R. S., M. T. S. and P. S. H.; Software: G. M. T.; Supervision: G. M. T.; Visualisation: G. M. T.; Writing – original draft: C. M. V. and G. M. T.; Writing – review and editing: C. M. V., C. M. F., C. R., M. R. S., M. T. S., P. S. H., A. E. W., M. H. S. and G. M. T.
G. M. T. has received support for his research laboratory, in the form of research grants or equipment loan or donation, from manufacturers of body composition assessment devices, including Size Stream, Naked Labs, Prism Labs, RJL Systems, MuscleSound, Biospace and Tanita. He is also a Scientific Advisor for Prism Labs, a smartphone 3D scanning company. None of these entities played a role in the present manuscript. The remaining authors report no conflicts of interest.

 Open access
Open access