


Schizophrenia is a chronic and severe mental disorder involving marked disturbances in thought, perception, self-experience, affect, volition and behaviour. It affects roughly 24 million people worldwide – about 1 in 300 – and is associated with substantial social and occupational impairment. 1 Antipsychotic medication is the foundation of treatment, with clozapine recommended following inadequate response to two prior antipsychotics. Reference Keepers, Fochtmann, Anzia, Benjamin, Lyness and Mojtabai2 Psychosocial interventions, including cognitive–behavioural therapy and structured rehabilitation, further support recovery. Reference Vita and Barlati3 Nonetheless, around 20–30% of individuals experience enduring symptoms despite optimal treatment and are classified as having treatment-resistant schizophrenia (TRS).
Electroconvulsive therapy (ECT), introduced in 1938, was widely adopted for schizophrenia due to its observable effectiveness, particularly in catatonia, agitation and severe behavioural disturbance. Its use declined following the introduction of antipsychotics in the 1950s, Reference Fink and Sackeim4 although it has remained a useful adjunct in difficult-to-treat cases. Under-use has persisted, partly because of stigma, concerns about cognitive effects, limited service provision and a historical lack of robust evidence.
These factors have influenced clinical guidelines. National Institute for Health and Care Excellence (NICE) guidance discouraged routine ECT for schizophrenia, restricting its use to life-threatening or treatment-refractory catatonia. 5,6 However, these recommendations predate a growing body of evidence demonstrating improved outcomes when ECT is combined with antipsychotic therapy, including in patients not responding to clozapine and those presenting with catatonia, aggression or suicidality. Reference Chan, Abdin, Seow, Subramaniam, Liu and Peh7–Reference Sinclair, Zhao, Qi, Nyakyoma, Kwong and Adams10 More recent guidance, from the Royal College of Psychiatrists, Reference Ferrier and Waite11 the American Psychiatric Association, Reference Rasmussen12,13 the Royal Australian and New Zealand College of Psychiatrists Reference Weiss, Hussain, Ng, Sarma, Tiller and Waite14 and the World Federation of Societies of Biological Psychiatry, Reference Espinoza and Kellner15 endorses ECT as an effective augmentation strategy in TRS.
National Audit data offer an opportunity to evaluate the real-world effectiveness of ECT and identify which patients may benefit most.
Aims
Using 10 years of national Scottish ECT data collected by the Scottish ECT Accreditation Network (SEAN) for patients with a diagnosis of schizophrenia (n = 94) and schizoaffective disorder (n = 59), we investigated whether the evidence supported the use of ECT as an effective intervention. In addition, we examined whether there were significant group-level associations between post-ECT clinical outcomes and pre-ECT clinical variables that correlated with treatment response, and tested for predictors of individual patient outcomes.
Method
SEAN data 2009–2018
The Scottish National Audit Programme (SNAP) of Public Health Scotland provided anonymised SEAN Audit data for the period 2009–2018. 16 The SEAN Steering Group approved release of these data (SEAN reference: IR2022-00182) covering all ECT treatment episodes in Scotland for the period 2009–2018, totalling 4474 individual patient records. The National Audit data were anonymised before release to researchers, meaning that approval by the National Research Ethics Service was not required, confirmed by use of the National Health Service (NHS) Human Research Authority online decision tools (https://www.hra-decisiontools.org.uk/) and following discussion with the local senior Research and Development facilitator.
SEAN data stratification and coding (see Table 1)
The data-set was categorised based on primary diagnosis, which was carried out by the treating psychiatric team using coding from ICD-10. The majority of cases were diagnosed with either depressive disorder or recurrent depressive disorder (n = 3307). Other diagnostic categories included bipolar disorder (n = 605), postnatal depression (n = 51), schizophrenia and related primary psychoses (n = 270), neurotic and related disorders (n = 58), personality disorders (n = 10), organic disorders (n = 8) and cases with no specific diagnosis recorded (n = 165).
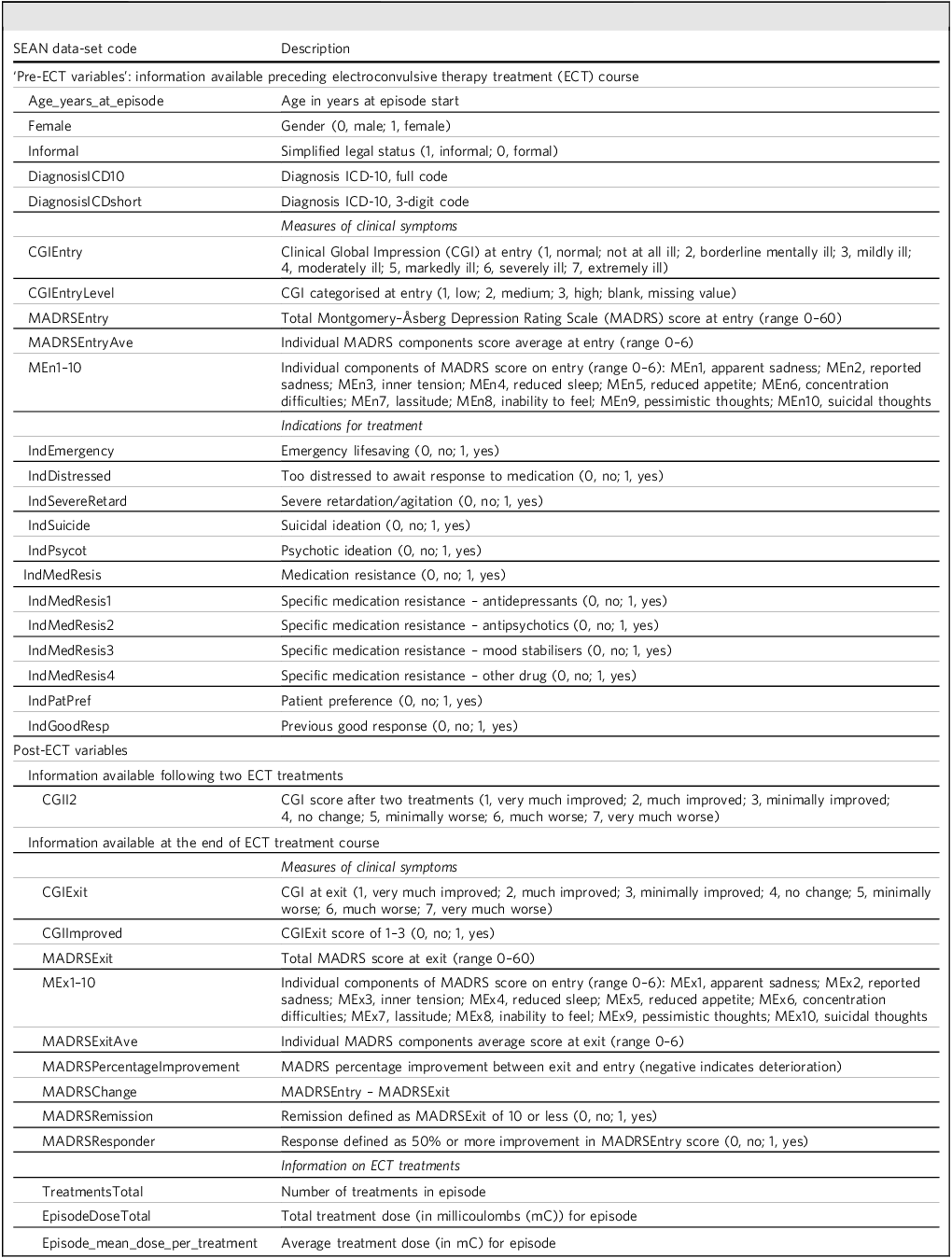
Scottish ECT Accreditation Network (SEAN) data-set codes and descriptions

Table 1 Long description
A table with 38 rows and 2 columns comparing Scottish ECT Accreditation Network data-set codes and descriptions. The first column lists the SEAN data-set codes, and the second column provides the corresponding descriptions. The table is divided into sections for pre-ECT variables, measures of clinical symptoms, indications for treatment, post-ECT variables, and information on ECT treatments. Pre-ECT variables include age, gender, legal status, diagnosis, and clinical symptoms measured by CGI and MADRS scores. Post-ECT variables include CGI and MADRS scores after two treatments and at the end of the ECT course, as well as information on the number and dose of treatments. The table provides a comprehensive overview of the data collected and measured in the context of electroconvulsive therapy treatment.
Because the primary focus of our analysis was the efficacy of ECT in schizophrenia, we filtered the SEAN data-set to include only those cases with a diagnosis of schizophrenia (n = 177) for which both entry Clinical Global Impression–Severity (CGIEntry) and exit Clinical Global Impression–Improvement (CGIExit) scores were available (n = 94). Baseline characteristics of patients with complete CGI data (n = 94) were compared with those without (n = 83), with no material differences observed in key demographic or clinical variables (Montgomery–Åsberg Depression Rating Scale–Entry (MADRSEntry), t = 1.57, p = 0.121; female, χ Reference Keepers, Fochtmann, Anzia, Benjamin, Lyness and Mojtabai2 = 0.35, p = 0.555; age_(years)_at_episode, t = 0.27, p = 0.788; CGIEntry, t = 0.23, p = 0.818). Entry MADRS scores were available for 57 patients and exit scores for 63 patients. For comparative purposes, we also examined outcomes in patients diagnosed with schizoaffective disorder (total n = 85) who had complete CGI scores (n = 59). MADRSEntry scores were available for 61 patients, and final MADRS scores (MADRSExit) for 56 patients. Although schizophrenia is primarily characterised by psychosis, the reduction of co-occurring affective symptoms could be a component of recovery, and MADRS scores may help predict those who are more likely to respond to ECT in both the schizophrenia and schizoaffective groups. It may be difficult clinically to differentiate schizophrenia from schizoaffective disorder, and so we also included an analysis of the two groups combined for additional comparison.
Statistical analyses
Descriptive and inferential statistical analyses were performed using JASP (version 0.15) 17 to compute measures of central tendency, dispersion and distributional properties for continuous variables, and to conduct correlation, t-test and analysis of variance procedures with effect sizes and confidence intervals. Complementary machine learning analyses were implemented in Python using the Scikit-learn library (version 1.6.1). Reference Pedregosa, Varoquaux, Gramfort, Michel, Thirion and Grisel18 A supervised algorithm (support vector regression) was applied following standard pre-processing (normalisation, feature selection) using tenfold nested cross-validation. Model performance was quantified using Pearson and Spearman correlations and mean absolute error.
Group-level association analyses (see Table 2)
Here the aim was to determine whether SEAN-recorded clinical indications for ECT and other clinical characteristics of patients (pre-ECT variables – for details see Table 1) were associated, at a group level, with measures of clinical improvement (post-ECT variables: CGIExit and MADRSExit). We tested for associations with each pre-ECT variable separately, because combinations of ‘independent’ pre-ECT variables can interact due to them being correlated. CGIExit and MADRSExit associations were tested using simple linear regression across the schizophrenia and schizoaffective groups. For comparison, CGI remission associations were also examined using simple logistic regression, with remission defined as a CGI score of either 1 (very much improved) or 2 (much improved) for comparison. Because individual MADRS items are highly correlated, we did not test these separately in our analyses.
CGIExit and MADRSExit associations using simple linear regression

Table 2 Long description
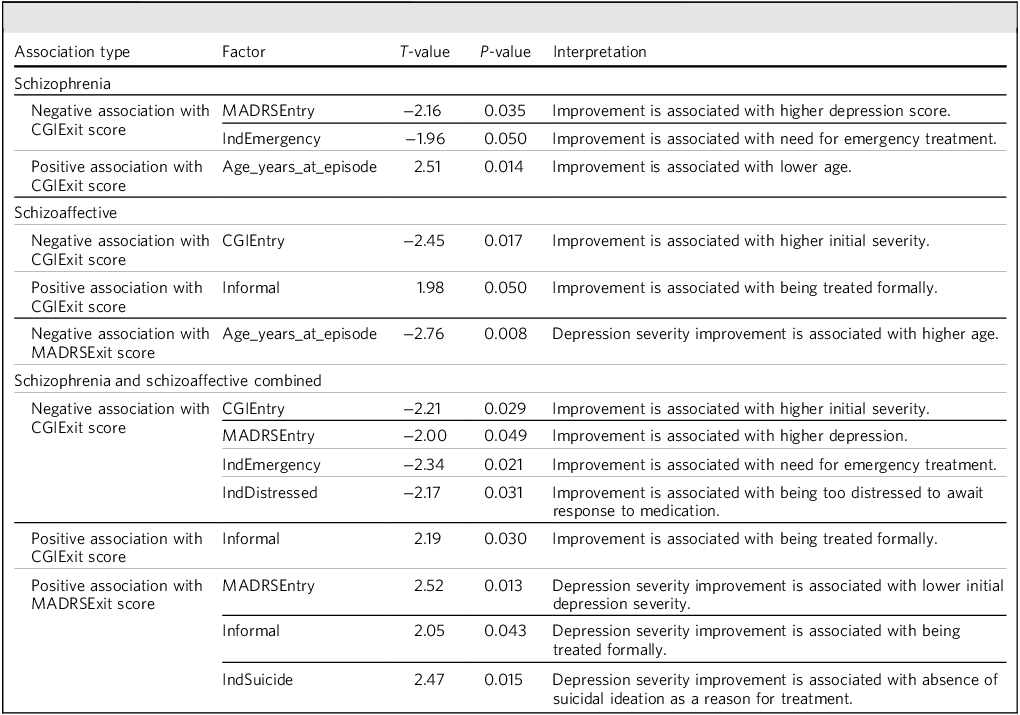
A table with five rows and five columns comparing CGIExit and MADRSExit associations using simple linear regression for schizophrenia and schizoaffective disorders. The columns are labeled Association type, Factor, T-value, P-value, and Interpretation. The table includes data on negative and positive associations with CGIExit and MADRSExit scores, factors such as MADRSEntry, IndEmergency, Age_years_at_episode, CGIEntry, Informal, and IndSuicide, and their corresponding T-values and P-values. Notable trends include improvement associated with higher depression scores, need for emergency treatment, lower age, higher initial severity, and formal treatment.
CGIEntry, Clinical Global Impression scores at the start of treatment; CGIExit, Clinical Global Impression scores at the end of treatment; MADRSEntry, Montgomery–Åsberg Depression Rating Scale scores at the start of treatment; MADRSExit, Montgomery–Åsberg Depression Rating Scale scores at the end of treatment; Informal, legel status; IndEmergency, treatment as an emergency; IndDistressed, treatment because of severe distress; IndSuicide, treatment due to active thoughts of suicide.
Individual patient prediction analyses
The purpose of our individual patient prediction analysis was to test whether it was possible to train a machine learning model that can successfully predict CGIExit scores on an individual patient level. Consequently, all pre-ECT variables were entered as potentially useful predictors with the intention of identifying an accurate predictive model for CGIExit scores (see Table 1 for full definitions of variables). The first model (model 1) used all pre-ECT variables (CGIEntry, CGIEntryLevel, MADRSEntry, age_(years)_at_episode, female, informal, emergency indication for treatment (IndEmergency), being too distressed to await response to medication (IndDistressed), IndSevereRetard, absence of suicidal ideation as a stated reason for treatment (IndSuicide), IndPsycot, IndMedResis, IndMedResis1, IndMedResis2, IndMedResis3, IndMedResis4, IndPatPref, IndGoodResp, IndOther, MEn1, MEn2, MEn3, MEn4, MEn5, MEn6, MEn7, MEn8, MEn9, MEn10), with the second model (model 2) also including the clinical improvement measured after the first week of treatment (CGII2) score because this is collected shortly after starting ECT at the end of the first week.
To predict CGIExit scores, we used epsilon-support vector regression with radial basis function kernel implemented in Python (version 3.13.2) using the Scikit-learn package (code available at https://github.com/unky4/ECT-Schizophrenia-ML). The target variable was scaled to the range of 0 and 1, with missing features first individually imputed using the k-nearest neighbours algorithm with seven neighbours and the default ‘non-Euclidean’ distance metric, and then each feature was scaled separately between 0 and 1. Partial least-squares regression was used as a supervised feature reduction method because, when explored, it marginally outperformed the principal component analysis method. To gain an accurate representation of the evaluation metrics, we used tenfold nested cross-validation (ten inner and ten outer folds) with hyperparameter tuning and preprocessing steps carried out within the inner folds, with a fixed random seed value of 42. Feature importance was measured with SHAP (version 0.47.1). Reference Lundberg, Lee, Guyon, Luxburg, Bengio, Wallach, Fergus, Vishwanathan and Garnett19 Individual patient prediction was assessed with Pearson and Spearman correlations, as well as by comparison of the mean absolute error of the model to a baseline mean absolute error, which was calculated using the mean CGIExit score as the predictor.
Results
Descriptive statistics (see supplementary materials for summary table)
Schizophrenia
Data were available for 94 individual patients with a mean age of 44.62 years (s.d. 14.77) and a range of 16–71 years. The male:female ratio was 48:46 (1.04:1). Most patients were rated as severely ill or extremely ill on CGIEntry prior to ECT (see Fig. 1). The average MADRSEntry (pre-ECT baseline) score was 29.33, with s.d. 11.98 (median 30, range 5–53). The post-ECT MADRS mean score was 12.71, with s.d. 9.36 (median 10.0, mode 2). The difference between mean and median or mode indicates a strong right-skewed distribution to post-ECT MADRS scores.
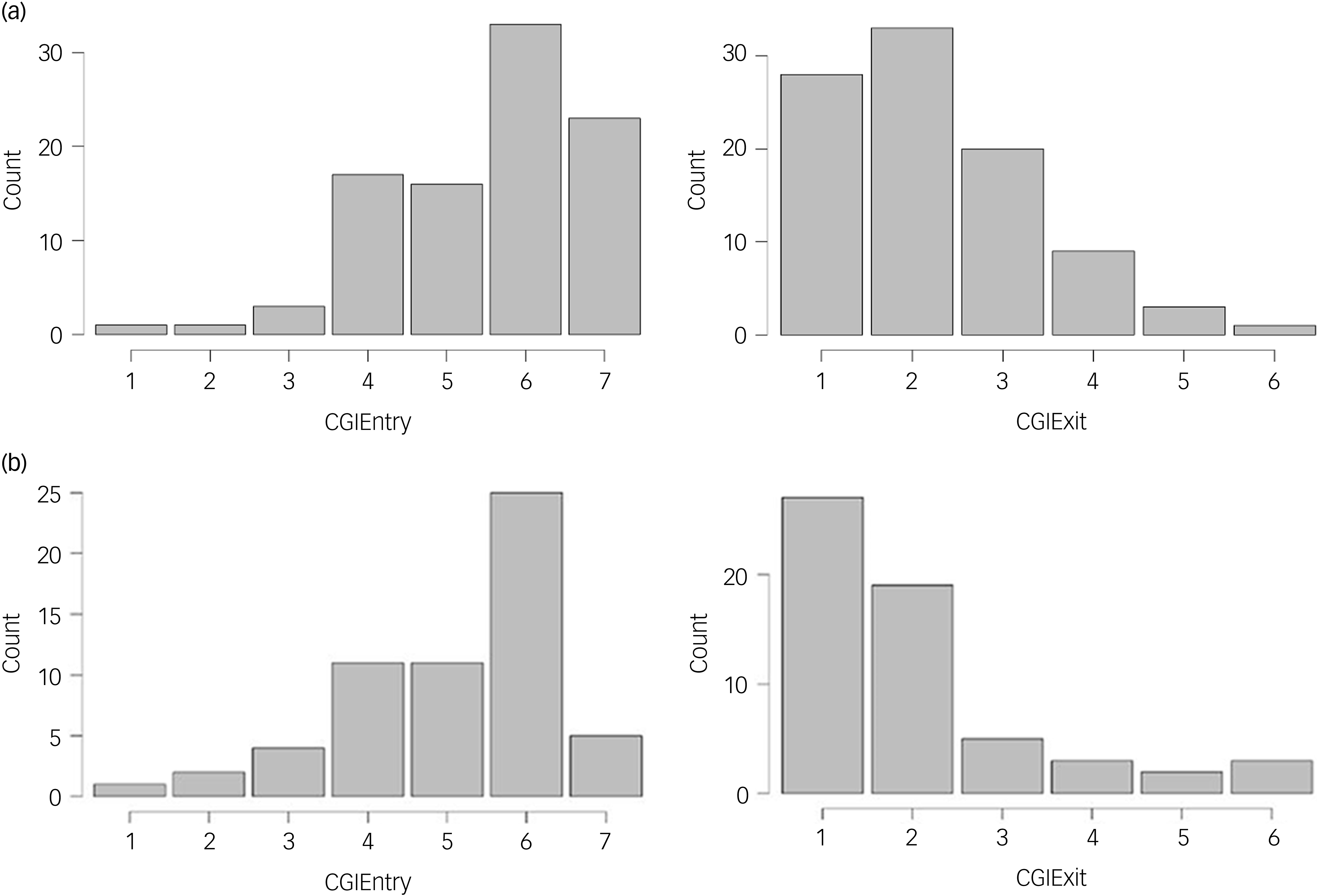
Clinical Global Impression (CGI) ratings at entry (CGIEntry) and exit (CGIExit) of electroconvulsive therapy episode. (a) Schizophrenia (n = 94). (b) Schizoaffective disorder (n = 59). CGIEntry 1, normal, not at all ill; 2, borderline mentally ill; 3, mildly ill; 4, moderately ill; 5, markedly ill; 6, severely ill; 7, extremely ill. CGIExit 1, very much improved; 2, much improved; 3, minimally improved; 4, no change; 5, minimally worse; 6, much worse; 7, very much worse.

Fig. 1 Long description
The bar graph compares Clinical Global Impression (CGI) entry ratings for schizophrenia and schizoaffective disorder patients. The x-axis represents CGIEntry ratings ranging from 1 to 7, where 1 indicates normal and 7 indicates extremely ill. The y-axis represents the counts of patients. For schizophrenia patients, the bars show counts for each CGIEntry rating, with notable peaks at ratings 4, 6, and 7. For schizoaffective disorder patients, the bars show counts for each CGIEntry rating, with notable peaks at ratings 1, 2, and 6. The bars are vertical and grouped by disorder type. All values are approximated.
Very few patients were capable of consenting, with only 15.96% treated informally. Where indications for ECT had been stated, 19.1% of treatment episodes were carried out as an emergency; 21.3% for severe distress; 26.6% for severe psychomotor retardation or agitation; 4.3% for clinically concerning suicidal ideation; 57.4% for psychotic symptoms; and 60.6% for medication resistance – mostly to antipsychotics (58.5%) but also to antidepressants (16%) and mood stabilisers (14.9%). These indications overlap, because some patients had more than one indication for treatment.
The average number of ECT treatments per patient was 9.62, with s.d. 4.65 (median 10, mode 12). The mean dose per treatment was 348.12 millicoulombs (mC), with s.d. 218.27 (median 297.2 mC, mode 200.0 mC). Again, the difference between mean and median and mode indicates a right-skewed distribution. The total treatment series cumulative dose was 3452.67 mC, with s.d. 3282.302 (median 2522.5 mC, mode 600 mC). This again reflects a right-skewed distribution.
Using CGIExit improvement scores, 86% of patients (81 of 94) showed improvement with ECT and 65% (61 of 94) were much or very much improved on CGI rating (CGIExit score 1 or 2), as illustrated in Fig. 1. The majority (63%) of patients achieved a clear response in relation to depressive symptoms (≥50% reduction in MADRS score from pre-ECT baseline), with a remission rate of 52.4% (final MADRS ≤10). Changes in scoring of individual MADRS items are summarised in the supplementary materials.
Schizoaffective disorder
Data were available for 59 individual patients with a mean age of 52.37 years (s.d. 16.56) and a range of 21–77 years. The male:female ratio was 22:37 (1:1.68). Most patients were rated as severely ill on CGIEntry prior to ECT (see Fig. 1). The average MADRS entry (pre-ECT baseline) score was 26.80, with s.d. 15.55 (median 30, mode 2, range 2–58). The post-ECT MADRS mean score was 11.22, with s.d. 11.26 (median 8, mode 2). The difference between the mean and median or mode indicates a strong right-skewed distribution to post-ECT MADRS scores.
The minority (30.5%) of patients were treated informally. Where indications for ECT had been stated, 13.6% of treatment episodes were carried out as an emergency; 30.5% for severe distress; 27.1% for severe psychomotor retardation or agitation; 6.8% for clinically concerning suicidal ideation; 44.1% for psychotic symptoms; and 61% for medication resistance, mostly to antipsychotics (55.9%) but also to antidepressants (30.5%) and mood stabilisers (28.8%). These indications overlap, because some patients had more than one indication for treatment.
The average number of ECT treatments per patient was 9.66, with s.d. 4.95 (median 11, mode 12). The mean dose per treatment was 368.62 mC, with s.d. 199.98 (median 362.5 mC, mode 400.0 mC). Again, the difference between mean and median and mode indicates a right-skewed distribution. The total treatment series cumulative dose was 3722.05 mC, with s.d. 2706.70 (median 3259 mC, mode 5400 mC). This again reflects a right-skewed distribution.
Using CGIExit improvement scores, 86.4% of patients (51 of 59) showed improvement with ECT and 78.0% (46 of 59) were much or very much improved on CGI rating (CGIExit scores 1 or 2), as illustrated in Fig. 1. The majority (66.7%) of patients achieved a clear response in relation to depressive symptoms (≥50% reduction in MADRS score from pre-ECT baseline), with a remission rate of 63.6% (final MADRS ≤10). Changes in scoring of individual MADRS items are summarised in supplementary materials.
Group-level association analyses (see Table 2)
Simple linear regression analyses identified several pre-treatment clinical variables that were significantly associated with ECT outcomes. The patterns of these associations differed notably between the diagnostic groups of schizophrenia and schizoaffective disorder.
Schizophrenia
For the schizophrenia cohort, several factors predicted a more robust overall clinical improvement, as indicated by a negative association with the CGIExit score. Specifically, better outcomes were associated with higher baseline depression severity (MADRSEntry, p = 0.035) and an emergency indication for treatment (p = 0.05). Conversely, a less favourable outcome, reflected by a positive association with the CGIExit score, was significantly associated with older age (p = 0.014). No associations were found with the severity of depressive symptoms post-treatment (MADRSExit).
Schizoaffective disorder
For the schizoaffective disorder group, a better overall clinical improvement (CGIExit) was associated with a higher initial illness severity (CGIEntry, p = 0.017). A less favourable outcome, however, was associated with being treated as an informal patient (p = 0.05). For depressive symptoms in this group, a better outcome (MADRSExit) was significantly associated with older age (p = 0.008).
Schizophrenia and schizoaffective disorder combined
Analysis of the entire data-set found predictors of clinical improvement negatively associated with CGIExit scores, including: higher initial illness severity (CGIEntry, p = 0.029); higher baseline depression severity (MADRSEntry, p = 0.049); emergency indication for treatment (IndEmergency, p = 0.021); and being too distressed to await response to medication (IndDistressed, p = 0.031). Being treated informally was positively associated with both CGIExit score (Informal, p = 0.03) and MADRSExit score (Informal, p = 0.043), suggesting that patients treated under the Mental Health Act showed greater improvement. Depression severity at exit (MADRExit) was associated with lower entry depression severity (MADRSEntry, p = 0.013), and with the absence of suicidal ideation as a stated reason for treatment (IndSuicide, p = 0.015).
Individual patient prediction analyses for CGII2 (see Fig. 2)
For schizophrenia patients, the individual patient predictive metrics for model 1 were r = 0.21 (p = 0.047), ρ = 0.22 (p = 0.032), mean absolute error 0.89 and baseline mean absolute error 0.91. The 6 most important variables for determining CGIExit scores were Age_years_at_episode, MADRSEntry, MEn9, MEn8, IndEmergency and MEn1 (see Fig. 2(a)). For model 2, with the addition of the CGII2 variable, the evaluation metrics were r = 0.22 (p = 0.037), ρ = 0.22 (p = 0.03), mean absolute error 0.89 and baseline mean absolute error 0.91. Here, the most important features were similar to model 1, but also included the variable Clinical Global Impression of Improvement after 2 treatments (CGII2) as the seventh most important feature (see Fig. 2(b)).
Individual patient predictive metrics for schizophrenia outcome. (a) Model 1 displays the predictive metrics and variable importance using only pre-treatment clinical variables (Pearson correlation r = 0.21, p = 0.047; Spearman correlation ρ = 0.22, p = 0.032). (b) Model 2 shows the impact of including the score for Clinical Global Impression of Improvement after 2 treatments (CGII2) alongside pre-treatment variables (Pearson correlation r = 0.22, p = 0.037; Spearman correlation ρ = 0.22, p = 0.03). For both models, the most influential variables for determining individual outcomes were age at episode (Age_years_at_episode), baseline depression severity (MADRSEntry) and specific symptoms including anhedonia (MEn8) and pessimistic thoughts (MEn9). Other significant variables were: being treated as an emergency (IndEmergency), for severe psychomotor retardation (IndSevereRetard), for severe distress (IndDistress), formally – under the Mental Health Act (Informal), the initial Clinical Global Impression score (CGIEntry) and other individual MADRS symptoms – apparent sadness (MEn1), reported sadness (MEn2), reduced appetite (MEn5), lassitude (MEn7) and suicidal thoughts (MEn10). Both models produced a mean absolute error (MAE) of 0.89, performing slightly better than the baseline MAE of 0.91.

Fig. 2 Long description
The bar graph compares the mean SHAP values of various clinical variables for two models predicting schizophrenia outcomes. The x-axis represents the mean SHAP value, while the y-axis lists the clinical variables. There are two sets of horizontal bars, one for Model 1 and one for Model 2. Model 1 includes pre-treatment clinical variables, and Model 2 includes the score for clinical improvement measured after the first week of treatment (CGII2) alongside pre-treatment variables. The most influential variables for both models are age at episode, baseline depression severity (MADRSEntry), and specific symptoms including anhedonia (MEn8) and pessimistic thoughts (MEn9). The bars are colored in shades of gray, with each bar representing a different clinical variable. All values are approximated.
For schizoaffective patients, and for schizophrenia and schizoaffective patients combined, neither model 1 nor model 2 yielded any significant results.
Discussion
Using a decade-long national Scottish data-set (SEAN), we found strong evidence that ECT is an effective treatment option for schizophrenia and schizoaffective disorder. We observed an 86% improvement rate in both diagnostic groups, especially in treatment-resistant cases. We also identified different predictors of response. For patients with schizophrenia, younger age and higher baseline depression were associated with a more favourable response. Conversely, for the schizoaffective group, older age and lower baseline depression were associated with better outcomes.
Our results provide a real-world validation for the efficacy of ECT in the most treatment-refractory patients with schizophrenia. The 65% rate of ‘much’ or ‘very much improved’ in the Scottish cohort is consistent with the response rate of ∼54% reported in pivotal systematic reviews, and in a major meta-analysis of ECT for treatment-resistant, and clozapine-resistant, schizophrenia by Lally et al Reference Lally, Tully, Robertson, Stubbs, Gaughran and MacCabe8 and Wang et al, Reference Wang, Pu, Jiang, Cao, Wang and Zhao20 respectively. Additionally, a 2019 Cochrane review by Sinclair et al Reference Sinclair, Zhao, Qi, Nyakyoma, Kwong and Adams10 found that ECT more than doubled the likelihood of a clinical response (risk ratio 2.06).
For schizoaffective disorder, ECT demonstrated similarly high real-world effectiveness, with 86.4% of patients showing clinical improvement and 78% rated as ‘much’ or ‘very much improved’ on CGI scores. These response rates are notably higher than those observed in schizophrenia, consistent with prior evidence that affective illness is strongly associated with ECT responsiveness. The magnitude of improvement in our cohort underscores ECT’s therapeutic value in this diagnostic group, particularly where pharmacological strategies have failed. In addition, CGII2, a measure of early clinical improvement, was associated with response of moderate to severely ill schizoaffective patients but not for those with a diagnosis of schizophrenia, and hence significant clinical changes may be noticed sooner in schizoaffective patients compared with those with a diagnosis of schizophrenia.
We identified several key predictors for a robust ECT response in schizophrenia: young age, the clinical indication of emergency treatment and baseline depression severity (MADRS), with anhedonia and pessimistic thoughts being particularly influential. In schizoaffective disorder, greater baseline illness severity and impaired decision-making ability were associated with more marked improvement on CGI scores, whereas higher age predicted better depression outcomes on MADRS ratings. These findings suggest that clinical severity and certain functional impairments may be useful markers for identifying patients most likely to benefit from ECT in this population.
Our findings show both notable similarities and differences compared with ECT response predictors in major depressive disorder (MDD). Reference van Diermen, van den Ameele, Kamperman, Sabbe, Vermeulen and Schrijvers21 In schizophrenia, young age predicted better response whereas, in MDD, older age consistently predicted better ECT response. However, in depression the age effect may partly reflect the greater prevalence of psychomotor disturbance and psychotic features in older patients, both of which are themselves associated with favourable ECT response. The association of improved response with higher baseline depressive symptom severity in both our schizophrenia and combined cohorts is consistent with the MDD literature, where greater baseline severity is more strongly associated with response than with remission. Similarly, the association in schizophrenia between better outcome and emergency treatment indication or greater illness severity parallels findings in MDD, where psychotic features, severe distress, psychomotor agitation or retardation, urgency of treatment and impaired decision-making capacity are all linked to favourable ECT outcome. Reference Semple, Suveges and Steele22
A full evaluation of ECT’s clinical role in the treatment of schizophrenia extends beyond symptom change to broader health outcomes. Although mortality was not assessed in our data-set, several large observational studies have reported associations between ECT and substantially lower all-cause mortality. When considered alongside the high rates of clinical improvement observed here, these external findings suggest that ECT may have wider health benefits that warrant further investigation in prospective designs. Schizophrenia confers a marked reduction in average life expectancy (15–28 years), largely due to preventable medical illness. 23,Reference Olfson, Gerhard, Huang, Crystal and Stroup24 A recent meta-analysis of over 1 million individuals reported a 30% reduction in all-cause mortality associated with ECT, a finding echoed in multiple large-cohort studies. Reference Rhee, Shim, Nasir, McIntyre, Kaster and Wilkinson25 Together, these data indicate a favourable risk–benefit profile.
The potential for cognitive side-effects, particularly memory loss, is a significant concern with ECT and must be addressed during the consent process. Reference Tan, Lim, Martin and Tor26 There is robust evidence that schizophrenia as an illness is associated with severe cognitive impairments, and there is evidence that ECT does not worsen long-term cognition. Specifically, a 2024 systematic review of treatment-resistant patients Reference Vaccarino and Vaccarino27 found no long-term cognitive harm, with some domains, such as executive function, even showing improvement. This is further supported by a Singaporean study Reference Rajagopalan, Lim, Tan, Martin, Lee and Tor28 which found a 45.6% cognitive improvement following ECT, particularly in those with poorer baseline function. Ultimately, the risk of cognitive decline from untreated psychosis appears to be far greater than that posed by ECT.
The ultimate goal of treatment is to restore function and improve quality of life. The benefits of ECT extend beyond clinical scales, with studies demonstrating significant improvements in quality of life (e.g. utilising the EuroQol Five Dimension questionnaire (EQ-5D) or the World Health Organisation Quality of Life – Short Form questionnaire (QHO-QOL Brief)) Reference Tan, Lim, Martin and Tor26 and higher Global Assessment of Functioning (GAF) scores. Reference Sinclair, Zhao, Qi, Nyakyoma, Kwong and Adams29 Furthermore, ECT reduces psychiatric readmission to hospital in the year following treatment, Reference Lin, Liu, Hsieh, Chien, Chen and Liao30,Reference Joo, Kim, Jo, Ahn, Choi and Choi31 which suggests enhanced clinical stability and relapse prevention.
Our study, combined with a robust body of evidence, reveals a significant gap between current UK clinical guidelines and best practice for schizophrenia. The NICE guidelines (CG178 and TA59) 5,6 restrict ECT to rare, life-threatening cases, a stance based on outdated evidence. The current NICE recommendations were formulated using evidence available at the time, which pre-dated recent meta-analyses and large naturalistic data-sets. Our findings, together with accumulating external evidence of symptomatic, functional and mortality benefits, indicate that the evidence base has evolved substantially. These developments may be informative for future guideline reviews given the adverse effects of prolonged untreated psychosis. Reference Drake, Husain, Marshall, Lewis, Tomenson and Chaudhry32 With a number needed to treat of approximately three for clinical improvement, and external evidence of reduced all-cause mortality, delayed or absent access to ECT may have important adverse consequences. We recognise that mortality studies of ECT are observational and may be influenced by residual confounding; however, the consistency of findings across multiple populations strengthens confidence in the association.
Strengths and limitations
The primary strength of this study is its large, national, multicentre, longitudinal SEAN data-set, which provides high ecological validity and statistical power by capturing real-world ECT outcomes in a large number of patients with schizophrenia over a decade. However, its retrospective and observational design limits causal inference and makes it susceptible to unmeasured confounders. A further limitation is the absence of a psychosis-specific scale, such as the Positive and Negative Syndrome Scale (PANSS), although this is partly mitigated by the correlation observed between MADRS and CGI scores, and we suggest that PANSS should be added to standard ECT practice for patients presenting with psychosis.
Future directions
Our national cohort demonstrated ECT’s effectiveness for both schizophrenia and schizoaffective disorder, with 86% of patients across both diagnoses showing clinical improvement. Substantial improvement (‘much’ or ‘very much improved’) was observed in 65% of those with schizophrenia and in 78% with schizoaffective disorder. These findings challenge the perception of ECT as a last-resort treatment and highlight a significant gap between current NICE guidelines and robust evidence. A review may help ensure equitable patient access, particularly given that untreated psychosis is strongly associated with adverse long-term outcomes and premature mortality. To reduce high relapse rates, over 50% on medication alone, Reference Aoki, Tajika, Suwa, Kawashima, Yasuda and Shimizu33 services should prioritise continuation and maintenance ECT. Future research needs to adopt prospective designs, routinely collect patient-reported outcomes and trial novel electrode placements such as frontomedial Reference Steele, Farnan, Semple and Bai34 to further optimise efficacy and minimise side-effects.
About the authors
David M Semple, Division of Psychiatry, University of Edinburgh, UK; and University Hospital Hairmyres, NHS Lanarkshire, Glasgow, UK. Szabolcs Suveges, School of Medicine, University of Dundee, UK. J. Douglas Steele, School of Medicine, University of Dundee, UK.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjb.2026.10256
Data availability
The data that support the findings of this study are available on request from the corresponding author, D.M.S., following appropriate permissions being obtained from SNAP and SEAN.
Acknowledgements
The authors thank the SEAN Steering Group for approving our use of the SEAN data-set. In addition, we thank data analyst David Murphy at Public Health Scotland for his work in extracting anonymised data.
Author contributions
D.M.S. and J.D.S. formulated the research questions, designed the study, analysed the data and wrote the article. S.S. contributed to statistical analysis and machine learning prediction analyses.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.
Transparency declaration
The authors confirm that the manuscript is an honest, accurate and transparent account of the study being reported.
Analytic code availability
The analytic software utilised – JASP and Scikit – are available to other researchers at https://jasp-stats.org/ and https://pypi.org/project/scikit-learn/.
Research material availability
Materials supporting the findings in this study are available to other researchers following an access request from SNAP and the approval of SEAN.




 Open access
Open access
eLetters
No eLetters have been published for this article.