

Vitamin D plays an important role in regulating cell proliferation/differentiation, the immune system, cardiovascular protection and bone metabolism(Reference Holick and Chen1,Reference Gil, Plaza-Diaz and Mesa2) . Consistent with this, low levels of vitamin D in the body (i.e. vitamin D deficiency) are considered detrimental to many aspects of health. When vitamin D deficiency is defined as blood 25-hydroxyvitamin D (25(OH)D) concentrations < 50 nmol/l, the prevalence of vitamin D deficiency is reported to be 24–40 % in European and North American countries, and the prevalence may be even higher in other populations(Reference Amrein, Scherkl and Hoffmann3).
Meta-analyses have found that vitamin D deficiency is associated with increased all-cause mortality, and this association is observed consistently across various general populations worldwide(Reference Zittermann, Iodice and Pilz4,Reference Schöttker, Jorde and Peasey5) . However, reports on the threshold of blood 25(OH)D concentrations, an appropriate biomarker of vitamin D status, at which all-cause mortality begins to increase are inconsistent. Two meta-analyses published in 2012(Reference Zittermann, Iodice and Pilz4) and 2014(Reference Garland, Kim and Mohr6) suggested < 75 nmol/l of blood 25(OH)D increases all-cause mortality risk. However, more recently published studies suggested lower thresholds, such as 35(Reference Sun, Langhammer and Skorpen7), 40(Reference Durazo-Arvizu, Dawson-Hughes and Kramer8), 50(Reference Dudenkov, Mara and Petterson9), 50(Reference Song, Lyu and Song10), 55(Reference Park, Han and Hwang11), 45–60(Reference Fan, Wang and Song12) and 65 nmol/l(Reference Zhu, Knuiman and Divitini13). These differences may be attributed to several factors, such as region, demographics, lifestyle, environmental factors and ethnicity(Reference Schöttker, Jorde and Peasey5,Reference Kritchevsky, Tooze and Neiberg14) .
The circannual change in sunlight exposure is a major factor influencing seasonal variation in blood 25(OH)D concentrations; concentrations are typically highest in summer and lowest in winter(Reference Holick15). Previous cohort studies have introduced season as a covariate when determining the threshold of blood 25(OH)D concentrations for mortality risk, but they rarely accounted for annual variation in 25(OH)D concentrations. Moreover, sex differences in blood 25(OH)D concentrations are considerable. According to a Japanese study, the prevalence of vitamin D deficiency in women is approximately twice that of men(Reference Nakamura, Kitamura and Takachi16), and thus sex differences may not be fully accounted for by statistical adjustments.
The Murakami cohort study of vitamin D (established in 2011, n 8498) is a population-based cohort study to determine the effect of vitamin D on age-related diseases in middle-aged and older people(Reference Nakamura, Kitamura and Takachi16,Reference Nakamura, Takachi and Kitamura17) . In the present study, plasma 25(OH)D concentrations were stratified by month (of blood collection) and sex to classify vitamin D level groups, allowing for season- and sex-stratified 25(OH)D groupings. We aimed to determine associations between vitamin D deficiency and mortality and identify risk thresholds in middle-aged and older individuals. Specifically, we examined risk thresholds of 25(OH)D concentrations for all-cause mortality by comparing season- and sex-stratified 25(OH)D groups with crude 25(OH)D groups.
Methods
Design and participants
This cohort study had an 11-year follow-up component. The Murakami cohort study targeted all 34 802 community-dwelling individuals aged 40–74 years residing in Murakami City, Sekikawa Village and Awashimaura Village in Japan, and 14 364 participated in the study. Of these, 8497 provided plasma samples. We excluded the following individuals: (1) 176 who had missing values for education, BMI or lifestyle information and 36 whose BMI values were outliers. The final population for statistical analysis included 8285 individuals. This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects/patients were approved by the Ethics Committee of Niigata University (Nos. 452 and 1324). Written informed consent was obtained from all participants.
Baseline survey
The baseline survey of the Murakami cohort study was conducted between 2011 and 2013. We used a self-administered questionnaire to obtain information on demographics, lifestyles, body size (height and weight) and disease history, including cancer, stroke, heart disease (myocardial infarction, angina, atrial fibrillation and/or heart failure), hypertension and diabetes. Codes for marital status, education level, occupation, smoking, alcohol consumption and disease histories are shown in online Supplementary Table 1. Total physical activity (PA) levels were assessed using the metabolic equivalent of task index (metabolic equivalent of task-h/d), which was calculated by multiplying the intensity of each activity by the number of hours per day using the Japan Public Health Center-based prospective study – physical activity questionnaire(Reference Kikuchi, Inoue and Odagiri18). Intensity of activities used in this calculation is also shown in online Supplementary Table 1. BMI was calculated as weight (kg) divided by the square of height (m2). Details of the baseline survey have been published elsewhere(Reference Nakamura, Takachi and Kitamura17).
Vitamin D measurements
Non-fasting blood specimens were collected, and plasma was obtained. Plasma specimens were stored at –80°C until biochemical analysis. Plasma 25(OH)D concentrations were measured by chemiluminescent immunoassay using the Liaison® 25OH Vitamin D Total Assay (DiaSorin Inc.; Stillwater, MN, USA). Intra- and inter-assay CV values were 3·2–8·1 % and 6·9–12·7 %, respectively. Details of collection and handling of blood specimens have been reported previously(Reference Nakamura, Kitamura and Takachi16,Reference Nakamura, Takachi and Kitamura17) .
Mortality during follow-up period
Information on dates of death and relocations up until 31 March 2024 were obtained from death and residency registration records in accordance with the Basic Residential Registry Law and the Family Registry Law. Information on causes of death was available up until 31 December 2022.
Statistical analysis
Median and interquartile range and numbers (and percentages) were used to characterise continuous variables and dummy variables, respectively. P for trend values for linear associations between 25(OH)D quintiles and participant characteristics were calculated using ordinal logistic regression analysis. Seasons were classified into five categories based on mean monthly plasma 25(OH)D concentrations at baseline(Reference Nakamura, Takachi and Kitamura17), as follows: (1) March and April (mean 25(OH)D, 42·6–42·8 nmol/l); (2) February and May (45·7–47·3 nmol/l); (3) June (49·0 nmol/l); (4) July, October, November, December and January (51·9–53·3 nmol/l) and (5) August and September (58·3–58·8 nmol/l). These categories were assigned numerical values and referred to as the ‘season score’. To account for seasonal- and sex-related variations in 25(OH)D concentrations, plasma 25(OH)D concentrations were divided into quintiles within each of the ten subgroups defined by season (five groups) and sex (two groups). These quintiles are referred to as ‘season- and sex-stratified quintiles’ herein. Hazard ratios (HR) for mortality according to quintiles were calculated using a Cox proportional hazards model. Covariates for the multivariate model were age, marital status (dummy variable), education, occupation (dummy variable), BMI, total PA, smoking, alcohol consumption and disease history for the season- and sex-stratified quintile model and season score, sex, age, marital status, education, occupation, BMI, total PA, smoking, alcohol consumption and disease history for the crude quintile model. Cubic spline curves with five knots were drawn to illustrate the multivariable-adjusted association between (a) season- and sex-stratified quintiles and (b) crude quintiles of plasma 25(OH)D concentrations and mortality hazard. Statistical analysis was performed using SAS statistical software (release 9.4, SAS Institute Inc.). P < 0·05 was considered statistically significant.
Results
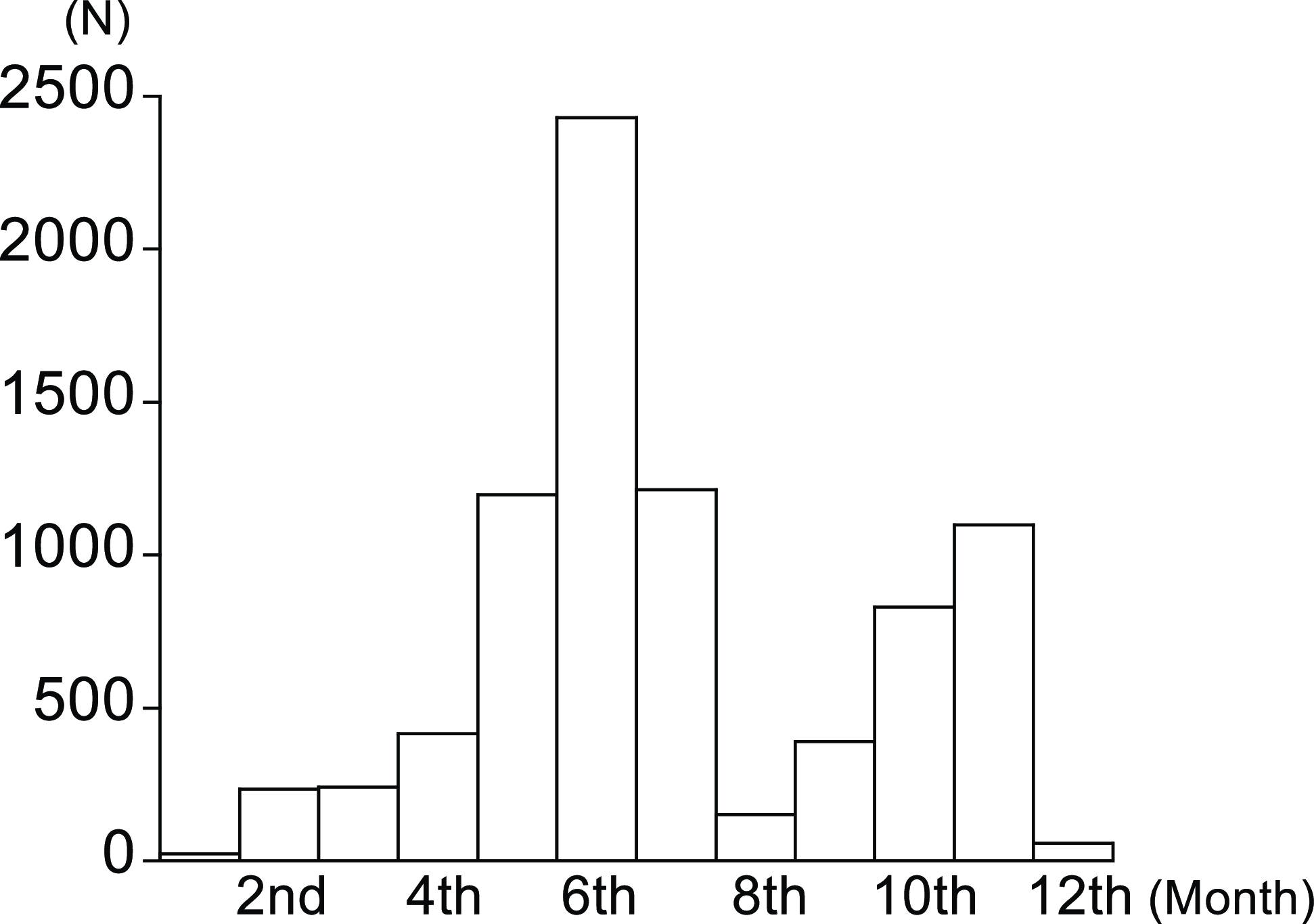
Mean age, 25(OH)D concentration and follow-up period of participants were 59·9 years (sd, 9·1), 50·1 nmol/l (sd, 18·1) and 11·4 years (sd, 1·5), respectively. The number of participants by month of blood collection is shown in Figure 1, which shows that fewer samples were collected during the winter months. The prevalence of low plasma 25(OH)D concentrations (defined as < 50 nmol/l) according to season score and sex at baseline is shown in online Supplementary Table 2. Agreement between the season- and sex-stratified and crude quintiles of 25(OH)D concentrations is shown in online Supplementary Table 3. The weighted κ coefficient was 0·72 (95 % CI: 0·71, 0·73). The number of deaths during the follow-up period was 641, including twenty participants in their 40s, 75 in their 50s, 258 in their 60s and 288 in their 70s. Cumulative all-cause mortality rates as determined by the Kaplan–Meier method stratified by crude quintiles of 25(OH)D concentrations are shown in online Supplementary Figure 1.
Monthly distribution of blood collection.

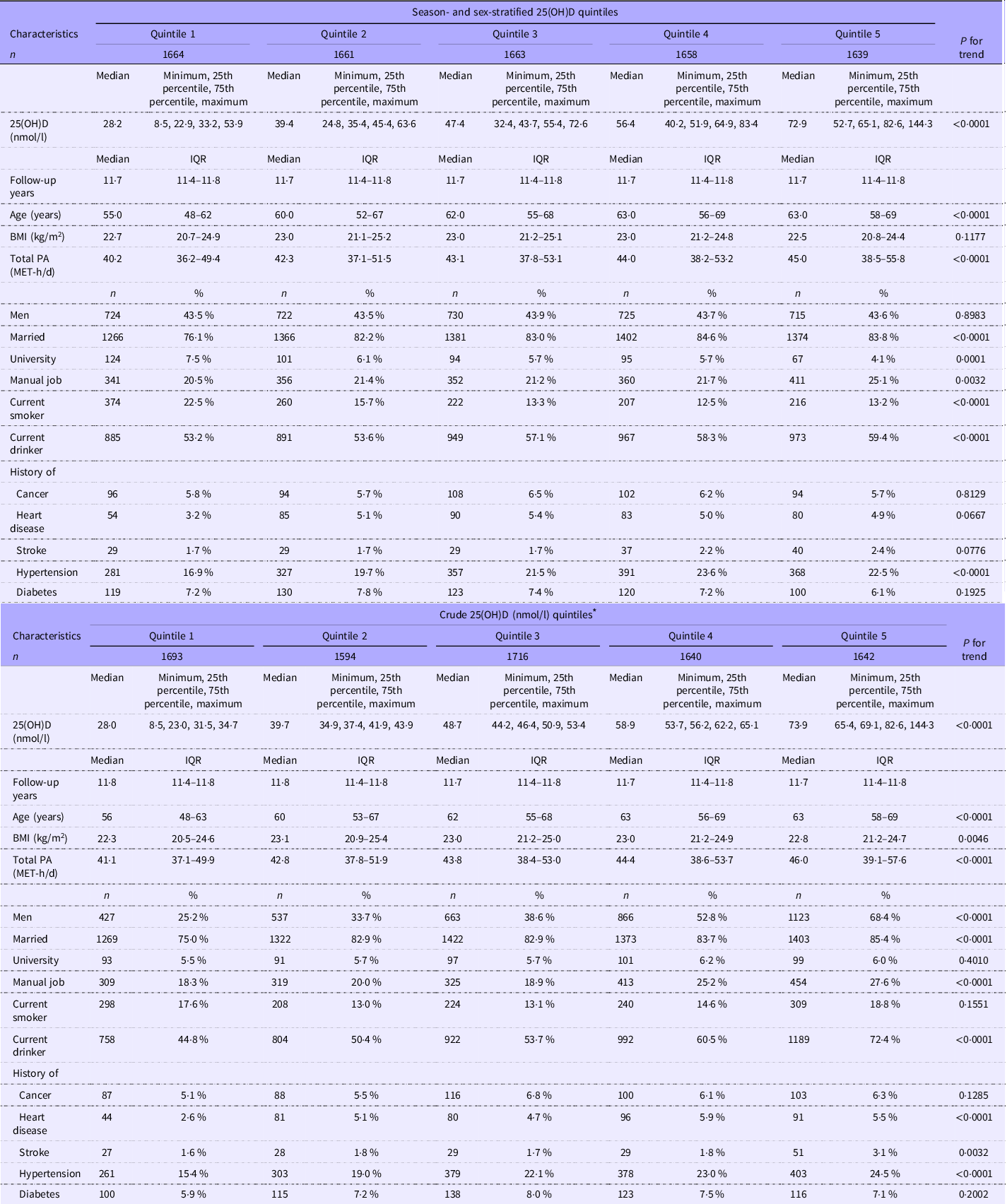
Participant characteristics according to season- and sex-stratified and crude quintiles of plasma 25(OH)D concentrations are shown in Table 1. Season- and sex-stratified quintiles were significantly, positively associated with age, total PA, being married, having a manual job, being a current drinker and having a history of hypertension and inversely associated with education level and being a current smoker. Crude quintiles were significantly, positively associated with age, BMI, total PA, being male, being married, having a manual job and having a history of heart disease, stroke or hypertension.
Participant characteristics according to season- and sex-stratified and crude quintiles of plasma 25-hydroxyvitamin D (25(OH)D) concentrations

PA, physical activity; MET; metabolic equivalent.
* Cut-off values for crude 25(OH)D (nmol/l) quintiles were 34·7, 44·2, 53·4 and 65·1. Cut-off values for season- and sex-stratified analysis could not be calculated.
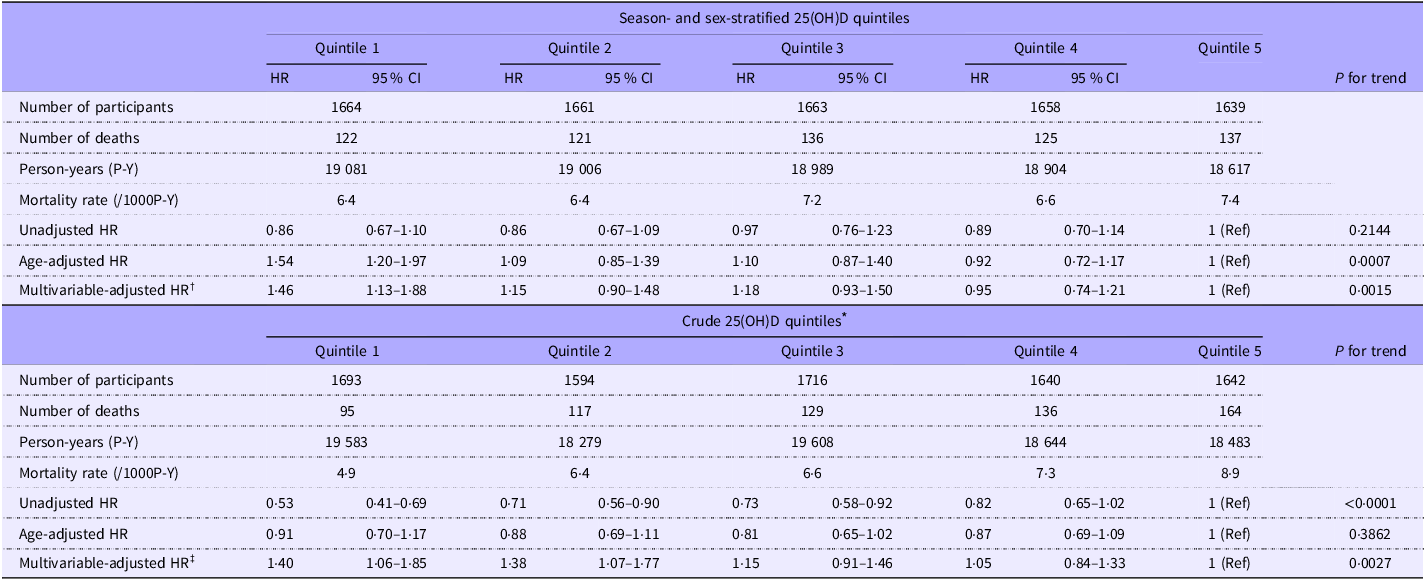
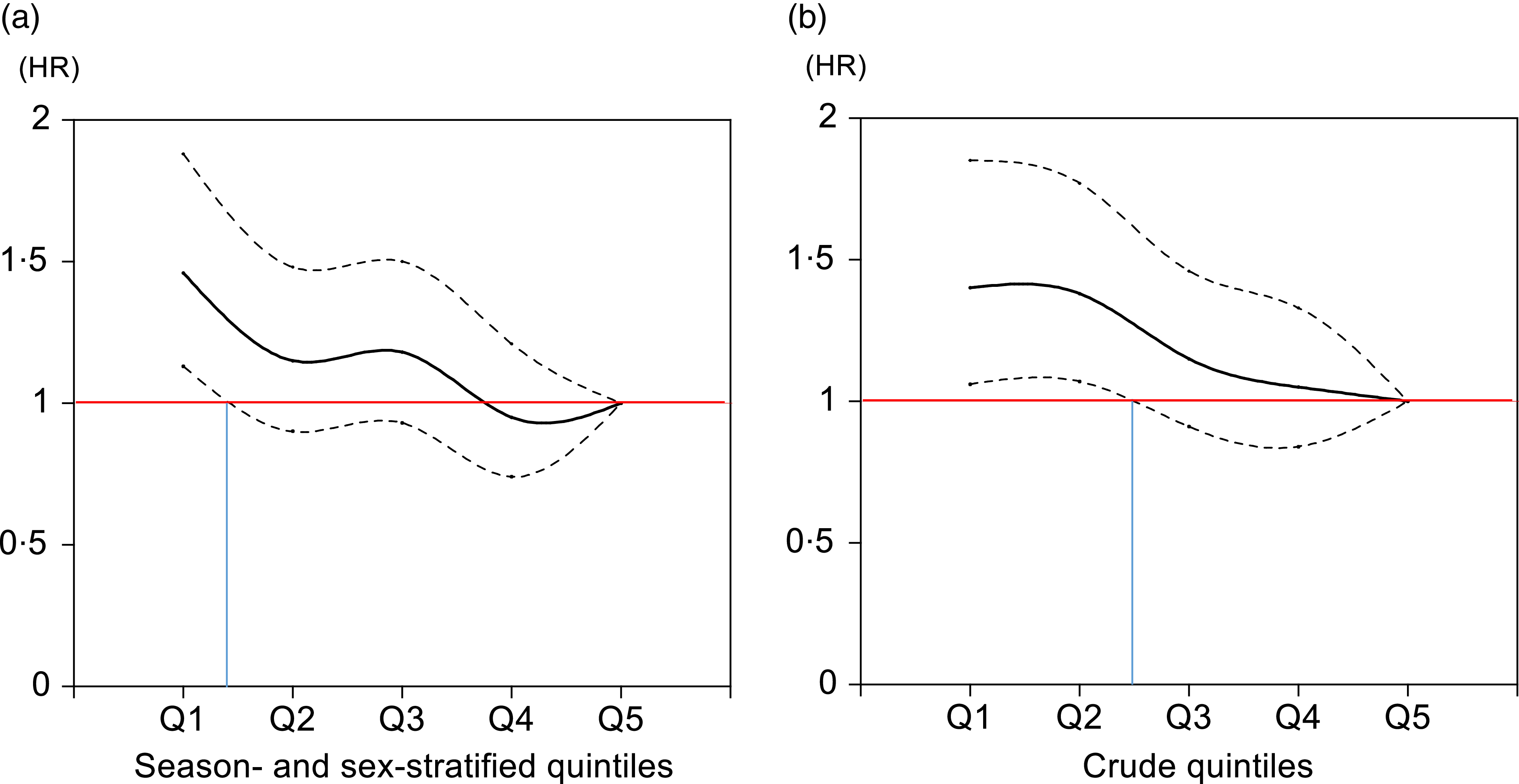
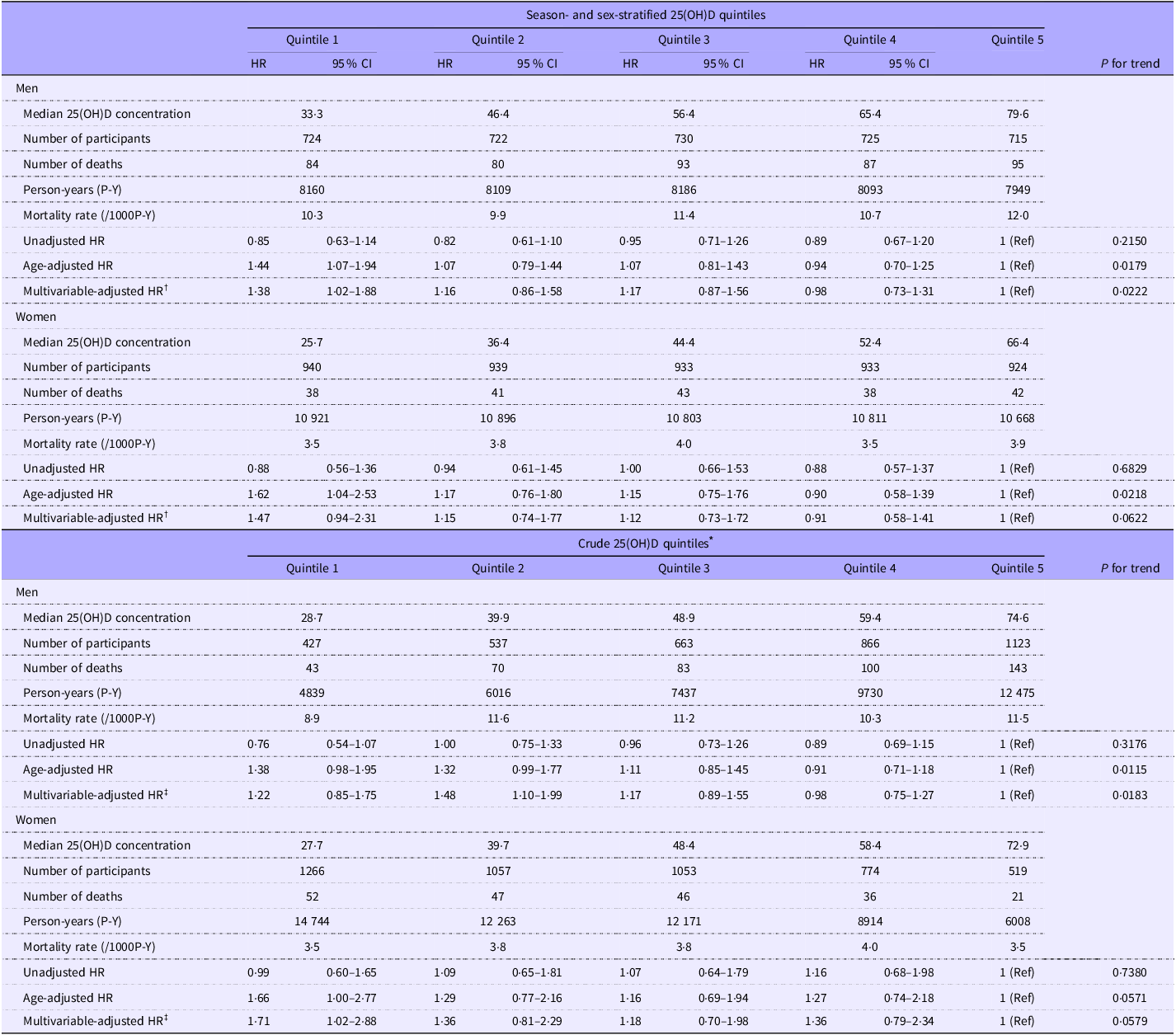
All-cause mortality and its HR according to season- and sex-stratified and crude quintiles of 25(OH)D concentrations are shown in Table 2. Lower season- and sex-stratified quintiles were associated with higher hazards of mortality (P for trend = 0·0015), with the first quintile having a higher HR (adjusted HR = 1·46, 95 % CI, 1·13, 1·88) than the highest quintile (reference). Lower crude quintiles were associated with higher hazards of mortality (adjusted P for trend = 0·0027), with the first and second quintiles having higher HR (adjusted HR = 1·40, 95 % CI, 1·06, 1·85 and 1·38, 95 % CI, 1·07, 1·77) than the reference. Cubic spline curves for these associations are shown in Figure 2. In this graphical analysis, the threshold of 25(OH)D concentration at which the lower bound of the 95 % CI exceeded 1 was estimated to be 32·4 nmol/l when using season- and sex-stratified quintiles and 44·2 nmol/l when using crude quintiles. Similar analyses to those in Table 2 were conducted using sex-stratified and season-stratified quintiles for 25(OH)D groupings, with the results shown in online Supplementary Table 4.
All-Cause mortality and hazard ratios (HR) according to different quintiles of plasma 25-hydroxyvitamin D (25(OH)D) concentrations
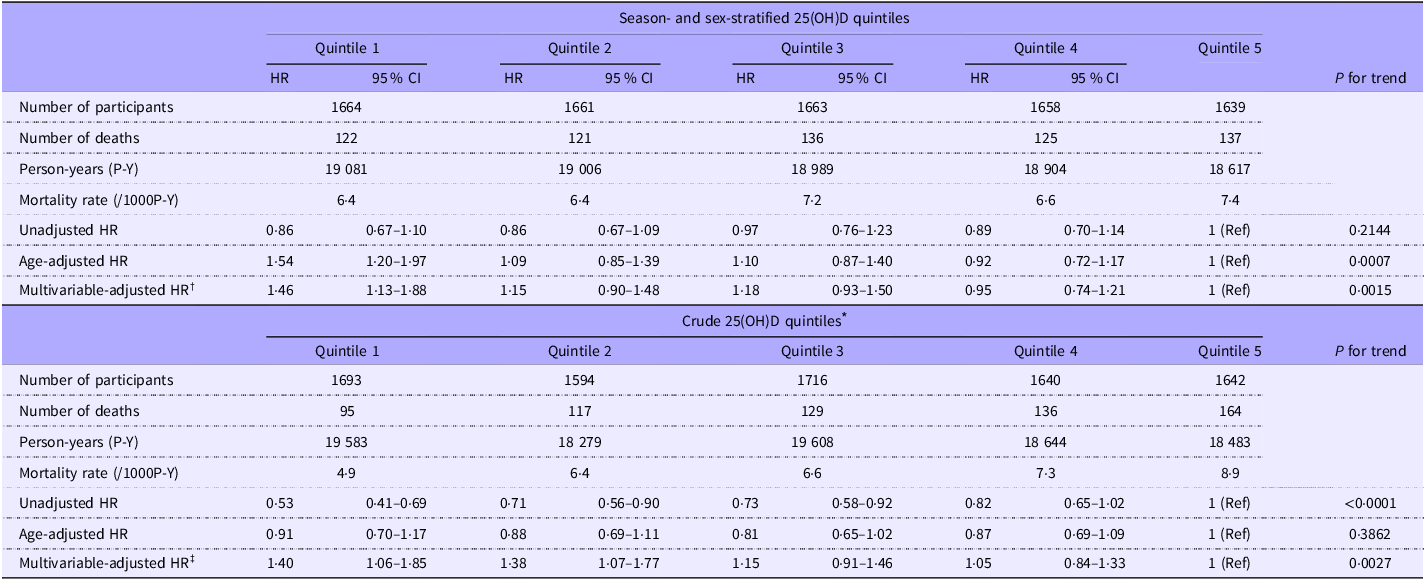
* Cut-off values for crude 25(OH)D (nmol/l) quintiles were 34·7, 44·2, 53·4 and 65·1. Cut-off values for season- and sex-stratified analysis could not be calculated.
† Adjusted for age, marital status, education, occupation, BMI, total physical activity, smoking, alcohol consumption and disease history.
‡ Adjusted for season score, sex, age, marital status, education, occupation, BMI, total physical activity, smoking, alcohol consumption and disease history.
Cubic spline curves showing the multivariable-adjusted association between (a) season- and sex-stratified quintiles and (b) crude quintiles of plasma 25(OH)D with the hazard of all-cause mortality. The threshold of 25(OH)D concentration at which the lower bound of the 95 % confidence interval exceeded 1 was calculated to be 32·4 nmol/l when using season- and sex-stratified quintiles and 44·2 nmol/l when using crude quintiles. 25(OH)D, 25-hydroxyvitamin D.

All-cause mortality and its HR according to season- and sex-stratified and crude quintiles of 25(OH)D concentrations by sex are shown in Table 3. Lower season- and sex-stratified quintiles were associated with higher hazards of mortality (adjusted P for trend = 0·0222) in men, with the first quintile having a higher HR (adjusted HR = 1·38, 95 % CI, 1·02, 1·88) than the reference. Associations in women were similar to those in men, but not significant. Lower crude quintiles were associated with higher hazards of mortality (adjusted P for trend = 0·0183) in men, with the second quintile having a higher HR (adjusted HR = 1·48, 95 % CI, 1·10, 1·99) than the reference. In women, lower crude quintiles were marginally associated with higher hazards of mortality (adjusted P for trend = 0·0579), with the first quintile having a higher HR (adjusted HR = 1·71, 95 % CI, 1·02, 2·88) than the reference. Cubic spline curves for these associations by sex are shown in online Supplementary Figure 2. Based on season- and sex-stratified quintiles, the 25(OH)D concentration threshold at which the lower bound of the 95 % CI exceeded 1 was estimated to be 30·1 nmol/l for men and 29·1 nmol/l for women. When using crude quintiles, the corresponding thresholds were estimated to be 35·2 nmol/l for men and 29·4 nmol/l for women.
All-Cause mortality and hazard ratios (HR) according to season- and sex-stratified quintiles of plasma 25-hydroxyvitamin D (25(OH)D) concentrations by sex

* Cut-off values for crude 25(OH)D (nmol/l) quintiles were 34·7, 44·2, 53·4 and 65·1. Cut-off values for season- and sex-stratified analysis could not be calculated.
† Adjusted for age, marital status, education, occupation, BMI, total physical activity, smoking, alcohol consumption and disease history.
‡ Adjusted for season score, age, marital status, education, occupation, BMI, total physical activity, smoking, alcohol consumption and disease history.
All-cause mortality and HR according to season- and sex-stratified quintiles of plasma 25(OH)D concentrations by age group (< 65 v. ≥ 65 years) in men and women are shown in online Supplementary Table 5. The inverse association between them tended to be more robust in the age ≥ 65 years group (P for trend = 0·0449) in men and age < 65 years group (P for trend = 0·0637) in women.
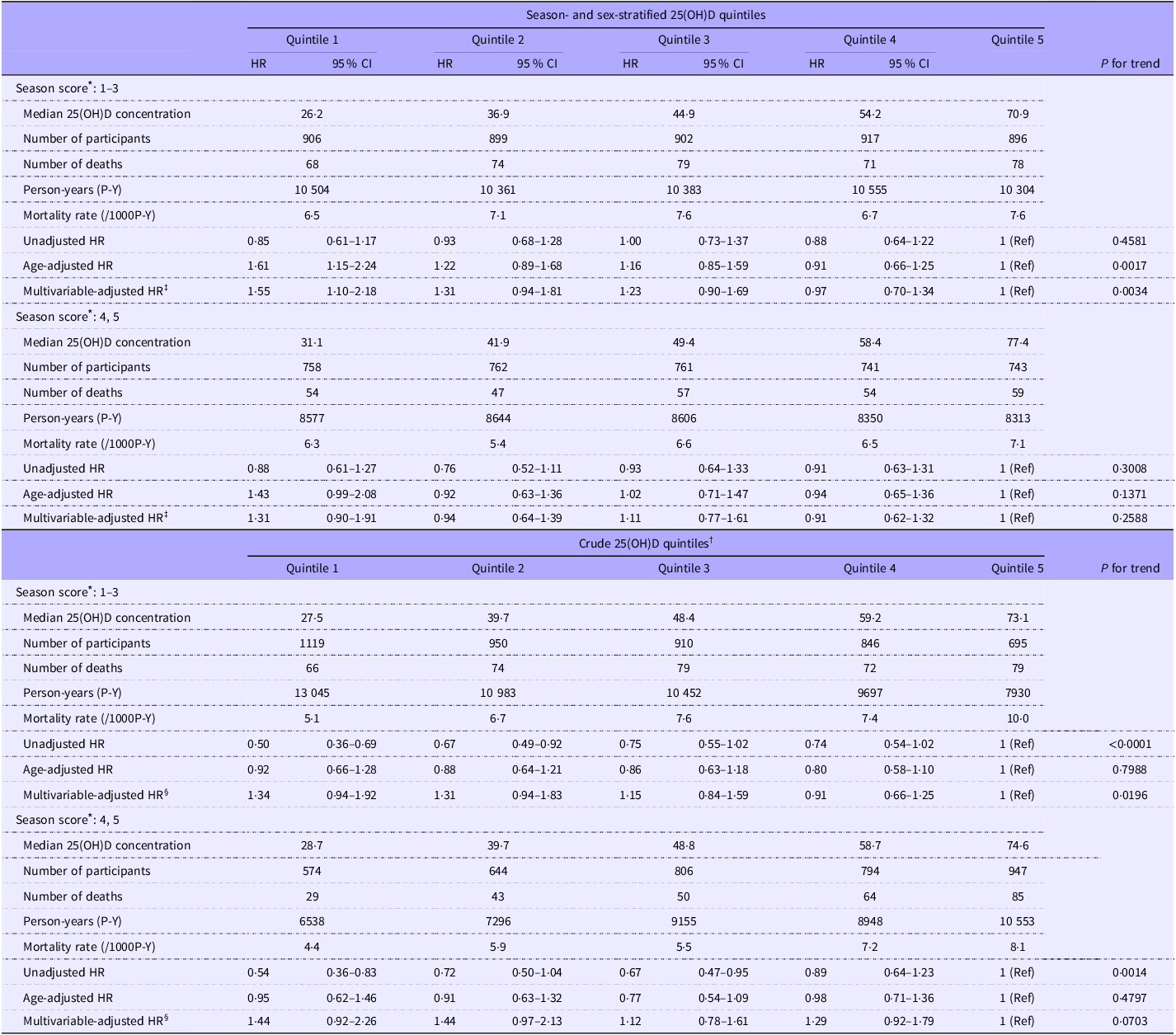
All-cause mortality and HR according to season- and sex-stratified quintiles of plasma 25(OH)D concentrations by season subgroup (season score 1–3 v. 4, 5) are shown in Table 4. Season- and sex-stratified 25(OH)D quintiles showed a dose-dependent association with mortality during seasons when plasma 25(OH)D concentrations were lower (adjusted HR = 1·55, 95 % CI: 1·10, 2·18, P for trend = 0·0034), but not during seasons when concentrations were higher (adjusted HR = 1·31, 95 % CI: 0·90, 1·91, P for trend = 0·2588).
All-cause mortality and hazard ratios (HR) according to season- and sex-stratified and crude quintiles of plasma 25-hydroxyvitamin D (25(OH)D) concentrations by season group

* (1) March and April (mean 25(OH)D, 42·6–42·8 nmol/l); (2) February and May (45·7–47·3 nmol/l); (3) June (49·0 nmol/l); (4) July, October, November, December and January (51·9–53·3 nmol/l) and (5) August and September (58·3–58·8 nmol/l).
† Cut-off values for crude 25(OH)D (nmol/l) quintiles were 34·7, 44·2, 53·4 and 65·1. Cut-off values for season- and sex-stratified analysis could not be calculated.
‡ Adjusted for sex, age, marital status, education, occupation, BMI, total physical activity, smoking, alcohol consumption and disease history.
§ Adjusted for season score, sex, age, marital status, education, occupation, BMI, total physical activity, smoking, alcohol consumption and disease history.
Mortality from and HR for cause-specific death from cancer, cardiovascular and cerebrovascular diseases and other causes according to season- and sex-stratified quintiles of 25(OH)D concentrations are shown in online Supplementary Table 6. Season- and sex-stratified quintiles of 25(OH)D concentrations were inversely associated with mortality from cancer (adjusted P for trend = 0·0170) and other causes (adjusted P for trend = 0·0257), with the first quintile having a higher HR (1·67, 95 % CI, 1·11, 2·50) for cancer. There was no association between 25(OH)D quintiles and mortality from cardiovascular and cerebrovascular diseases (adjusted P for trend = 0·8891).
Discussion
The present study is the first to report an inverse association between blood 25(OH)D concentrations and mortality in population-based cohorts in Japan. We found that all-cause mortality began to significantly increase at the lowest quintile (median = 28·2 nmol/l) when using season- and sex-stratified 25(OH)D groupings and at the second quintile (median = 39·7 nmol/l) when using crude 25(OH)D quintiles. This suggests that the risk threshold for vitamin D deficiency in relation to all-cause mortality is overestimated by approximately 10 nmol/l when using the crude blood 25(OH)D concentrations, particularly in men. A potential explanation for this is the reclassification of individuals who should have been in the first quintile into the second quintile, thereby elevating the HR in the second quintile. This reclassification could have resulted from seasonal variations in blood collection, which occurred more frequently in non-winter than winter seasons. Consequently, individuals with relatively low vitamin D levels were less likely to be classified as deficient when assessed solely based on crude 25(OH)D concentrations. In addition, vitamin D levels in men were much higher than in women, which may also have contributed to this discrepancy.
Several cohort studies published in the last decade have reported the risk threshold of blood 25(OH)D for all-cause mortality using a season variable (i.e. a variable representing the four seasons) as a covariate in multivariate analysis. Durazo-Arvizu et al. (Reference Durazo-Arvizu, Dawson-Hughes and Kramer8) reported a threshold of 40 nmol/l when comparing 25(OH)D concentrations by dividing them into increments of 10 nmol/l in a study of 15 099 USA individuals aged ≥ 20 years (mean age: 45 years; mean 25(OH)D concentration, 64 nmol/l). Zhu et al. (Reference Zhu, Knuiman and Divitini13) reported a threshold of 60 nmol/l, determined by the lower bound of the 95 % CI which exceeded 1 on a cubic spline curve in a study of 3946 Australians aged 25–84 years (mean age: 52·5 years; mean 25(OH)D concentration: 60·6 nmol/l). In two studies that used quartile groupings, Sun et al. (Reference Sun, Langhammer and Skorpen7) reported a threshold of 35 nmol/l (upper bound of the lowest quartile) in a study of 6613 Norwegians aged ≥ 20 years (mean age: 47·3 years; mean 25(OH)D concentration: 47·3 nmol/l), and Park et al. (Reference Park, Han and Hwang11) reported a threshold of 55 nmol/l (upper bound of the third quartile) in 27 846 Koreans aged ≥ 20 years (mean age: 45·1 years; mean 25(OH)D concentration: 44·5 nmol/l). Two studies adopting the USA Institute of Medicine’s 25(OH)D classification (< 30, 30–49, 50–74, ≥ 75 nmol/l) reported a threshold of 50 nmol/l in a study of 11 022 NHANES III participants (mean age: 54·3 years; mean 25(OH)D concentration: 75 nmol/l)(Reference Dudenkov, Mara and Petterson9) and a threshold of 50 nmol/l in a study of 18 797 Koreans aged ≥ 40 years (mean age 58·2 years; mean 25(OH)D concentration: 55·8 nmol/l)(Reference Song, Lyu and Song10). Finally, a large UK Biobank cohort study reported thresholds of 45–60 nmol/l. Compared with the results of previous studies, the estimated threshold of between 28·2 and 39·4 (medians of Quintile 1 and Quintile 2 using season- and sex-stratified 25(OH)D groupings) or 44·2 nmol/l (upper boundary of Quintile 2 using crude 25(OH)D grouping) in the present study (mean age: 59·9 years; mean 25(OH)D concentration: 50·1 nmol/l) lies around the midpoint or lower. This lower threshold may at least in part be attributed to the null association between 25(OH)D groups and mortality from cardiovascular and cerebrovascular diseases (shown in online Supplementary Table 6), probably due to low mortality from cardiovascular disease in Japan(Reference Iso19).
Given that the COVID-19 pandemic, which began in 2020, may have influenced mortality rates, we assessed all-cause mortality and HR according to season- and sex-stratified quintiles of plasma 25(OH)D concentrations based on follow-up through 2019 (mean follow-up period: 7·4 years) (online Supplementary Table 7). The trends were generally similar to those observed in the overall analysis (Table 2), but the HR for the lowest quintile was 1·27 (95 % CI: 0·86, 1·87), which tended to be lower than that in the overall analysis (HR = 1·46). Thus, there may have been a potential interaction effect of COVID-19 on the association between blood 25(OH)D concentrations and mortality.
The 25(OH)D concentrations observed in the present study population should be compared with those of other Japanese populations to determine if they are representative. Two population-based studies of the general Japanese population reported prevalence rates of blood 25(OH)D concentration < 75 nmol/l of 72 % in men and 88 % in women (n 1683; mean age, 70·3 years; October–January)(Reference Yoshimura, Muraki and Oka20) and 90 % in women (n 1211; mean age, 64·1 years; September–December)(Reference Tamaki, Iki, Sato and Oka21). In the present study, the corresponding prevalence rates were 85 % in men and 96 % in women (data not shown), suggesting that prevalence rates in the present study were slightly higher than those reported in previous studies. This could be explained by the slightly younger study population in the present study relative to those in previous studies, as younger Japanese adults tend to have lower blood 25(OH)D concentrations(Reference Nakamura, Kitamura and Takachi16).
Strengths of the present study include the large sample size and demonstration that relying solely on statistical adjustments for key confounding factors such as season and sex may not be appropriate when analysing the strength of associations between 25(OH)D concentrations and mortality risk. The present study also has some limitations. First, blood 25(OH)D concentration was measured once at baseline, and its changes during the follow-up period were not evaluated. This may have resulted in a discrepancy in the classification of 25(OH)D concentrations. Second, we did not account for all confounding factors affecting the association between 25(OH)D concentration and mortality. Accordingly, there may be unknown confounders that could have influenced the observed associations. Third, we used the chemiluminescent immunoassay method to measure blood 25(OH)D concentrations. However, the chemiluminescent immunoassay method has been reported to yield lower vitamin D values compared to LC–MS/MS (the gold standard, approximately 10 %(Reference Moon, Cho and Hur22,Reference Rahman, Al-Taiar and Shaban23) ), which may have led to an overestimation of vitamin D deficiency. Therefore, the cut-off value of blood 25(OH)D concentration for mortality may be slightly lower than that suggested in the present study. Finally, generalisation of our results should be approached with caution. Blood collection was conducted mostly in non-winter seasons, which may have led to false vitamin D sufficiency and introduced classification discrepancies. Given the marked sex difference in 25(OH)D concentrations, these types of discrepancies may be less likely in settings where blood collection occurs during seasons with low sunlight exposure and in populations with smaller sex differences.
The present study demonstrated that using season- and sex-stratified quintiles of blood 25(OH)D concentrations effectively removed the confounding effects of season of blood collection and sex, which are important factors influencing the relationship between 25(OH)D concentrations and disease occurrence. This approach enabled the identification of a 25(OH)D concentration associated with mortality that is less affected by these factors. However, the observed differences between season- and sex-stratified quintiles and crude quintiles suggest that the threshold may vary depending on season or sex. While no sex-specific differences in the threshold were observed, a dose-dependent increase in mortality risk was observed as 25(OH)D concentrations declined among participants whose vitamin D levels were measured during seasons when 25(OH)D concentrations tend to be lower, rather than the risk being elevated only in the lowest quintile. These findings suggest that the association between vitamin D levels and mortality may differ by season.
Conclusions
Blood 25(OH)D concentrations are inversely associated with all-cause mortality in middle-aged and older Japanese people, and the risk threshold for vitamin D deficiency associated with mortality based on season- and sex-stratified 25(H)D groupings ranged from 28·2 to 39·4, with no sex difference. Crude blood 25(OH)D concentration may modulate the estimated risk threshold for vitamin D deficiency associated with mortality. Further studies on whether the threshold of the association between blood 25(OH)D concentrations and mortality varies by season are warranted.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114525105308
Acknowledgements
We are indebted to DiaSorin Inc. for providing the plasma 25(OH)D assay. We also thank the following institutions for their help with blood collection: Murakami City Government, Sekikawa Village Government, Awashimaura Village Government, the Medical Association of Murakami City and Iwafune District, Murakami General Hospital, Niigata Prefectural Sakamachi Hospital, Sampoku Tokushukai Hospital, Murakami Memorial Hospital, Senami Hospital, Sakanamachi Hospital, Aoki Clinic, Arakawa Chuo Clinic, Anzai Clinic, Hatori Clinic, Homma Clinic, Iga Clinic, Otabe Clinic, Sakura Clinic of Internal Medicine, Sano Clinic, Sato Clinic, Sato Clinic of Internal Medicine, Sato Clinic of Internal Medicine and Pediatrics, Sawada Clinic, Sega Clinic, Sekikawa Medical Office, Suzuki Clinic (Murakami City), Suzuki Clinic (Tainai City), Shibata Comprehensive Health Care Service Center, Kenko-Igaku-Yobo-Kyokai, Niigata Association of Occupational Health, Niigata Health Care Association, BML, Inc. and Kotobiken Medical Laboratories, Inc.
This work was supported by JSPS KAKENHI Grants (JP23249035, JP40339958, JP15H04782 and JP19H03897), a National Cancer Center Research and Development Fund (23-A31[toku]) (since 2010) and the JGS Grant for Geriatric Nutrition Research (supported by Otsuka Pharmaceutical Factory, Inc.). The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
K. Kitamura: Conceptualisation, data curation, investigation, formal analysis, writing – original draft; Y. Watanabe: investigation, writing – review & editing; K. Kabasawa: writing – review & editing; T. Saito: investigation; A. Takahashi: investigation; R. Kobayashi: investigation; R. Oshiki; investigation; K. Watanabe: supervision; R. Takachi: investigation, data curation, writing – review & editing; S. Tsugane: supervision, funding acquisition; K. Nakamura: investigation, project administration, funding acquisition, writing – review & editing. All authors have read and approved the final manuscript.
The authors declare they have no conflict of interest with respect to this research study and paper.



 Open access
Open access