


Metabolic dysfunction-associated steatotic liver disease (MASLD) is the most prevalent chronic liver disease worldwide(Reference Younossi, Golabi and Paik1). MASLD is defined as the presence of hepatic steatosis accompanied by one or more metabolic dysregulations(Reference Rinella, Lazarus and Ratziu2). Globally, nearly 38 % of the population has MASLD, and this is estimated to increase to almost half the adult population by 2040(Reference Le, Yeo and Zou3). MASLD is intricately linked with metabolic syndrome, type 2 diabetes and obesity, conditions that are associated with increased CVD risk and mortality(Reference Gami, Witt and Howard4). In fact, the risk for adverse liver outcomes, including advanced fibrosis, cirrhosis, hepatocellular carcinoma and mortality, is significantly increased in people who have hepatic steatosis with severe metabolic dysfunction(s)(Reference Elsaid, Bridges and Li5). MASLD has become the second leading cause of liver transplantation in America(Reference Cotter and Charlton6) and Europe(Reference Adam, Karam and Cailliez7). As per the global burden of disease data, MASLD-related deaths due to cirrhosis and hepatocellular carcinoma have increased by 76·7 % and 95·1 %, respectively, between 1990 and 2019(Reference Jiang, Mao and Liu8), contributing significantly to both clinical and economic burden(Reference Younossi, Blissett and Blissett9). Therefore, there is a critical need for intensified and sustainable interventions that can effectively mitigate both the risk of developing MASLD and its associated adverse outcomes(Reference Sualeheen, Tan and Georgousopoulou10).
In the context of limited effective pharmacotherapies, lifestyle interventions primarily focusing on weight loss through diet and physical activity remain the mainstay for MASLD prevention(Reference Rinella, Neuschwander-Tetri and Siddiqui11–Reference Keating, Chawla and De13). Growing evidence suggests that a region-specific Mediterranean Diet (MedDiet), characterised by a high intake of fruits, nuts, vegetables, whole grains, legumes and olive oil, along with moderate consumption of fish and poultry and limited intake of red and processed meats, is the cornerstone of therapeutic management of MASLD(Reference Kawaguchi, Charlton and Kawaguchi14,Reference Sangouni, Hassani Zadeh and Mozaffari-Khosravi15) and associated metabolic dysregulations(Reference Papadaki, Nolen-Doerr and Mantzoros16). The anti-inflammatory and antioxidative properties of the MedDiet may counteract key pathogenic pathways of MASLD, such as insulin resistance, inflammation and oxidative stress, thereby reducing hepatic steatosis and also addressing associated metabolic comorbidities(Reference Estruch17,Reference Abenavoli, Greco and Milic18) . Moreover, its emphasis on whole, seasonally available foods enhance sustainability and frugality, making it a practical choice for adaptation in non-Mediterranean regions(Reference Martínez-González, Hershey and Zazpe19,Reference George, Kucianski and Mayr20) . Despite the potential benefits of the MedDiet in mitigating liver-related complications, the association between adherence to the MedDiet, MASLD and long-term outcomes including incident hospitalisation and mortality remains underexplored, particularly in large, population-based Western cohorts. Furthermore, limited evidence exists regarding its long-term benefits for MASLD and its severity in non-Mediterranean populations(Reference Sualeheen, Tan and Georgousopoulou10). While some research indicates there are protective effects of the MedDiet for MASLD and its severity(Reference Sangouni, Hassani Zadeh and Mozaffari-Khosravi15,Reference Moosavian, Arab and Paknahad21) , most studies are based in Mediterranean regions where the diet is traditionally consumed. The UK Biobank, with over 500 000 adult participants, presents a unique opportunity to address this gap by examining if adherence to the MedDiet influences the risk of MASLD development and subsequent MASLD-related incident hospitalisation and mortality in a general Western population. This study, therefore, aimed to assess the association between adherence to the MedDiet and the risk of MASLD and its impact on the incident of hospitalisation and mortality related to MASLD and associated conditions. By elucidating the role of the MedDiet in MASLD progression and severity, the findings could aid in guiding public health strategies to enhance targeted preventive measures and reduce the burden of MASLD.
Methods
Study design and participants
This longitudinal study utilised data from UK Biobank, which is a large population-based cohort from over half a million (n 502 488) adults aged 40–69 years residing in the UK(Reference Allen, Lacey and Lawlor22). All participants were recruited from 1 of 22 assessment centres across England, Scotland and Wales from 2006 to 2011. Participants underwent comprehensive health assessment including collection of biological samples (blood, urine and saliva) and physical measurements (e.g. body composition and blood pressure)(Reference Allen, Lacey and Lawlor22). Demographic, lifestyle behaviours and general health-related information was collected through a touch screen questionnaire and brief verbal interview. In 2014, UK Biobank aimed to collect imaging data for 100 000 participants at imaging assessment centres and performed magnetic resonance imaging scans that included abdomen, heart and brain(Reference Allen, Lacey and Lawlor22). The UK Biobank study was approved by the North-West Multi-Centre Research Ethics Committee and obtained written informed consent from all study participants(Reference Allen, Lacey and Lawlor22).
Study inclusion and exclusion
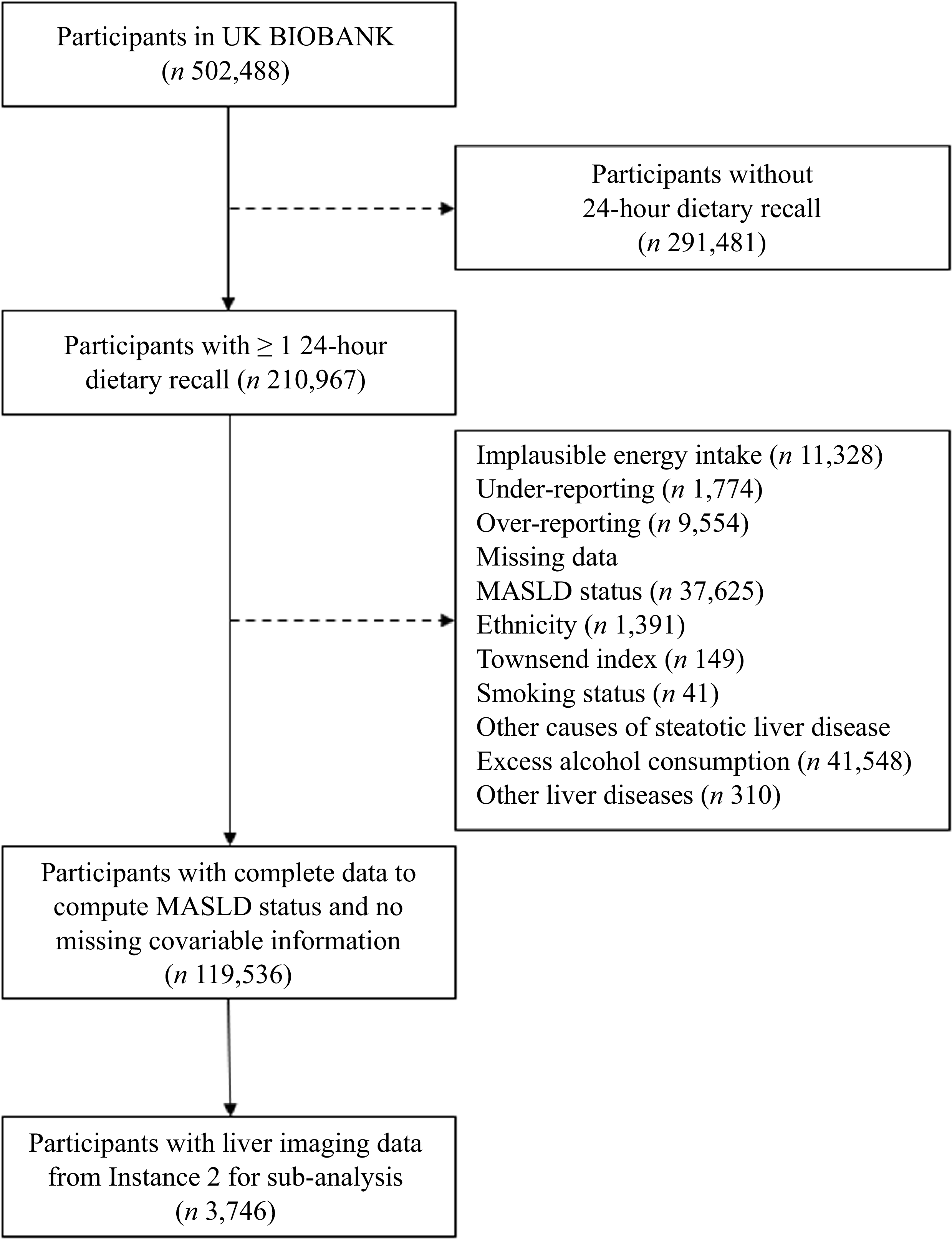
For this study, participants with at least one online 24-hour dietary recall, and who had available baseline data to predict MASLD and no missing covariate information, were included (n 119 536). Participants with energy intake levels deemed implausible, falling beyond the range of 500 kcal/d to 3500 kcal/d for females and 800 kcal/d to 4200 kcal/d for males, and were excluded(Reference Willett23). Participants who selected responses such as ‘don’t know’, ‘prefer not to answer’ or ‘prefer to abstain’ for covariates including ethnicity (n 401), qualification (n 575), annual household income (n 12 841) and smoking status (n 280) were coded as missing data. In addition, 19 080 participants had missing information for physical activity. Rather than excluding these individuals from the analysis, the missing data were handled using multiple imputation, as described below. Participants with excessive alcohol intake (> 30 g for males and > 20 g for females) were excluded. In accordance with the expert panel consensus statement on International Classification of Diseases, 10th Revision coding for steatogenic liver disease, individuals diagnosed with alcohol-related liver disease (K70), toxic liver disease (K71), viral hepatitis (B16-B19) or autoimmune hepatitis (K75·4) were further excluded from the analysis(Reference Hagström, Adams and Allen24). These conditions were collectively classified as ‘other liver diseases’ in the study flowchart (Figure 1). For the sub-analysis, participants with missing liver imaging data from Instance 2 were excluded, resulting in a sample of 3746 individuals for the sub-analysis (Figure 1).
Study flowchart for the UK Biobank Cohort. MASLD, Metabolic dysfunction-associated steatotic liver disease.

Sociodemographic and health-related information
Age, sex (males and females), education (college or university education, less than college or university education and vocational qualification), annual household income before tax (less than £18 000; £18 000 to £30 999; £31 000 to £51 999; £52 000 to £100 000; greater than £100 000) and Townsend deprivation index as indicators of socioeconomic status were acquired from baseline data. Smoking status was derived from participants’ responses to the baseline touchscreen questionnaire and categorised as ‘Never smoked’, ‘Former smoker’ or ‘Current smoker’. Physical activity was assessed using questions based on the short form of the International Physical Activity Questionnaire in the UK Biobank cohort(25,Reference Cassidy, Chau and Catt26) . Total physical activity was calculated as the sum of metabolic equivalent task minutes per week for walking, moderate and vigorous physical activity and was subsequently used in the analysis(Reference Cassidy, Chau and Catt26).
Dietary intake information
Dietary intake information was obtained from the web-based 24-hour dietary recall, the Oxford WebQ which was introduced at the end of recruitment between 2009–2010 and captured dietary intake information for about 70 000 participants at baseline. The Oxford WebQ was developed and validated against the interviewer administered 24-hour dietary recall for total energy and nutrient intake and recovery biomarkers to be utilised for UK Biobank(Reference Liu, Young and Crowe27,Reference Greenwood, Hardie and Frost28) . Participants provided dietary intake information during the initial visit at the assessment centre (baseline) and those who provided email-addresses to UK Biobank were invited via email to complete the diet questionnaire online on four separate occasions between February 2011 to April 2012 (cycle 1, February 2011 to April 2011; cycle 2, June 2011 to September 2011; cycle 3, October 2011 to December 2011; cycle 4, April 2012 to June 2012). The total period of available dietary data from the Oxford WebQ was 38 months (April 2009-June 2012). Email invitations were sent on different days of the week to capture variation in dietary intakes, and participants were given 3 days to complete the questionnaire for cycles 1 and 2 and 14 days for cycles 3 and 4. Information regarding the consumption of 200 typical foods and beverages consumed in the past 24-hours was collected. The quantity of each food and beverage consumed was calculated by multiplying the assigned portion size of each food or beverage by the amount consumed. The nutrient profile for each participant was generated by multiplying the quantity consumed by the nutrient composition of foods and beverages from UK food composition database(29). Participants with valid dietary data for ≥ 1 occasions were included for diet quality analysis(Reference Greenwood, Hardie and Frost28).
Diet quality analysis
For diet quality analysis, the reported food and beverage intake from Oxford WebQ, which was in portion and standard serving sizes, was first converted into gram weights. The Food Portion Sizes (third edition) by Food standard agency was used, and average portion of each food item and beverage was utilised as the reference for conversion(30). MedDiet score (MedDietScore) by Panagiotakos et al. (Reference Panagiotakos, Pitsavos and Arvaniti31) was modified and used to assess adherence towards a traditional Mediterranean dietary pattern.
MedDietScore
The MedDietScore assesses weekly consumption of 11 food components based on MedDiet pyramid recommendations(Reference Panagiotakos, Pitsavos and Arvaniti31). A monotonic function was used to assign scores from 0–5 based on weekly consumption of food components. For food groups that align closely with Mediterranean dietary pattern, i.e. non-refined cereals, fruits, vegetables, legumes, olive oil, fish and potatoes, a score of 0 was assigned for no consumption and scores 1 to 5 were assigned based on frequency of consumption, ranging from rare to daily intake. Due to unavailability of olive oil intake in the dataset, olive oil was replaced with MUFA:SFA ratio(Reference Trichopoulou, Costacou and Bamia32). Reverse scoring was applied for food groups to limit, which includes meat and meat products, poultry, and full fat dairy products. For alcohol, participants were assigned a score of 5 for < 300 ml/d, a score of 0 for either no consumption or consumption > 700 ml/d. Scores ranging from 1 to 4 were assigned for consumption levels between 600–700 ml, 500–600 ml, 400–500 ml and 300–400 ml/d, respectively. The original MedDietScore is a frequency-based index(Reference Panagiotakos, Pitsavos and Arvaniti31). However, in the present study, dietary intake was assessed using 24-hour recalls, and the average daily intake was multiplied by 7 to estimate weekly consumption, thereby approximating habitual intake. In addition, the olive oil component was replaced with the MUFA:SFA ratio. Given these methodological modifications, the score is referred to as the Modified-MedDietScore (M-MedDietScore). The total M-MedDietScore ranged from 0 to 55, with higher scores indicating greater adherence to the Mediterranean dietary pattern(Reference Panagiotakos, Pitsavos and Arvaniti31).
Metabolic dysfunction-associated steatotic liver disease definition
For this study, MASLD was confirmed by the presence of hepatic steatosis, as determined by the fatty liver index (FLI)(Reference Bedogni, Bellentani and Miglioli33) and liver imaging data from instance 2 (2014) for a subset of participants. The FLI was calculated using BMI, waist circumference, triglycerides and γ-glutamyl transferase from baseline. A FLI score of ≥ 60 was used to predict hepatic steatosis, in addition to the presence of at least one of the following five cardiometabolic risk factors: being overweight or obese, diabetes, hypertension, hypertriglyceridaemia or low HDL levels(Reference Rinella, Lazarus and Ratziu2,Reference Sualeheen, Tan and Daly34) . The metabolic risk factors criteria were confirmed from the baseline and described in detail below.
Cardiometabolic risk factor criteria for metabolic dysfunction-associated steatotic liver disease
The cardiometabolic risk factors assessed in this study were as follows: overweight was defined as BMI ≥ 25 kg/m2 (≥ 23 kg/m2 for Asians) and obesity as a BMI ≥ 30 kg/m2 (≥ 27·5 kg/m2 for Asians). Abdominal obesity was determined by waist circumference of ≥ 94 cm for males and ≥ 80 cm for females (≥ 90 cm for males and ≥ 80 cm for females in Asians). Type 2 diabetes status was established through self-reporting, supplemented by fasting glycated Hb (HbA1C) levels ≥ 6·5 % or the use of antidiabetic medications(35). Prediabetes was defined using a HbA1C level of 5·7 % based on MASLD criteria(Reference Rinella, Lazarus and Ratziu2). Hypertension was diagnosed with systolic blood pressure ≥ 130 mmHg and/or diastolic blood pressure ≥ 85 mmHg, or if the individual was taking antihypertensive medication. Hypertriglyceridaemia was identified with serum triglyceride levels ≥ 150 mg/dl or the use of lipid-lowering drugs, while low HDL was indicated by levels ≤ 40 mg/dl for males and ≤ 50 mg/dl for females, or if lipid-lowering medications were being taken(Reference Rinella, Lazarus and Ratziu2). Hypercholesterolaemia was defined as total cholesterol > 240 mg/dl or use of lipid-lowering medication(Reference Pasternak36).
Hospitalisation and mortality outcomes
Hospitalisation and mortality data were obtained from the linked electronic health records, with data available until April 2021 for hospitalisation and March 2021 for mortality. Incident hospitalisations and cause-specific mortality were identified using the International Classification of Diseases, 10th Revision coding, along with an expert panel consensus statement for MASLD(Reference Hagström, Adams and Allen24). MASLD events were identified by International Classification of Diseases, 10th Revision codes, including K74·0, K74·1, K74·2, K75·8, K76·0, K76·6, K76·7 and K76·9 as well as related conditions: cirrhosis (K74·6, I85·0, I85·9, I86·4, I98·2, I98·3, R18), and hepatic cancers (C22·0, C22·9). Additional events included CVD (I00-I09, I11-I13, I20-I51, I60-I69), diabetes mellitus (E10-E14), hypertensive disease (I10-I15), extrahepatic cancers (C00-C21, C23-C97), chronic lower respiratory disease (J40-J47), septicaemia (A40-A41) and renal disease (N00-N07, N18-N19, N25-N27, I120, I131, Z490, Z940, Z992). These causes were identified from existing literature as leading causes of death in individuals with steatogenic liver disease(Reference Golabi, Paik and Eberly37). Both primary and secondary contributory cause of mortality were screened and included in the analysis(Reference Hagström, Adams and Allen24). All-cause mortality was defined as mortality due to any cause. Detailed descriptions of these International Classification of Diseases, 10th Revision codes are provided in the online Supplementary Table S1.
Statistical analysis
Baseline characteristics of the overall cohort were compared using the t test or Mann–Whitney U test, depending on the normality of continuous variables, and the chi-square test for categorical variables. Continuous variables were reported as mean (sd) or median (interquartile range), and categorical variables as frequency (percentage), as appropriate. Binary logistic regression analysis was used to assess the relationship between M-MedDietScore (predictor variable) and MASLD (outcome variable). Two models were applied in the analysis: Model 1 adjusted for age, sex, ethnicity, qualification, household income, Townsend deprivation index, smoking status, physical activity and energy intake and Model 2 further adjusted for diabetes, hypertension, total cholesterol, HDL cholesterol, LDL cholesterol and CVD incidence occurred before the exposure variable, i.e. from the date of last dietary assessment. Covariates were selected based on previous literature and theoretical considerations, focusing on variables consistently linked with both the outcome and exposure variables(Reference Sualeheen, Tan and Daly38). A sensitivity analysis was also performed without the MUFA: SFA as a proxy to olive oil component in the M-MedDietScore, due to its absence in our dataset. This component, typically part of the adequacy criteria in the MedDietScore, was replaced by MUFA:SFA ratio in our study. The total M-MedDietScore was scaled in five-unit increments, with each increment representing a change in adherence equivalent to one component of the M-MedDietScore.
Multivariable Cox proportional hazard model with time-in-study as the timescale was used to estimate the association of M-MedDietScore with incident hospitalisation, cause-specific and all-cause mortality. Participants were followed from the date of their last dietary assessment (baseline) until the date of first in-patient hospitalisation, date of death or loss to follow-up – whichever came first. Separate analyses were conducted to assess the risk of incident hospitalisation (date of first in-patient hospitalisation) and mortality, with each outcome considered independently, using a censoring date of 31 December 2021. Two models were presented: Model 1 adjusted for age, sex, ethnicity, qualification, household income, Townsend deprivation index, smoking status, physical activity and energy intake and Model 2 further adjusted for diabetes, hypertension, total cholesterol, HDL cholesterol and LDL cholesterol. No significant sex interactions were observed; therefore, the pooled results are presented.
A subgroup analysis of incident hospitalisation and mortality was performed in participants with MASLD diagnosed at baseline, using both unadjusted and multivariable-adjusted models. To maximise the sample size and limit bias, multiple imputations was performed using the Nelson-Aalen estimator to account for missing covariates in survival analysis(Reference White and Royston39). The Nelson-Aalen estimator, which estimates the cumulative baseline hazard, was incorporated into the imputation models to ensure proper handling of the survival outcome(Reference White and Royston39). This approach allowed for robust imputation of missing values while preserving the association between covariates and survival, thereby minimising bias in the analysis. All statistical analysis was performed using STATA version 18.0, and a P-value < 0·05 was considered as statistically significant.
Results
Demographic characteristics
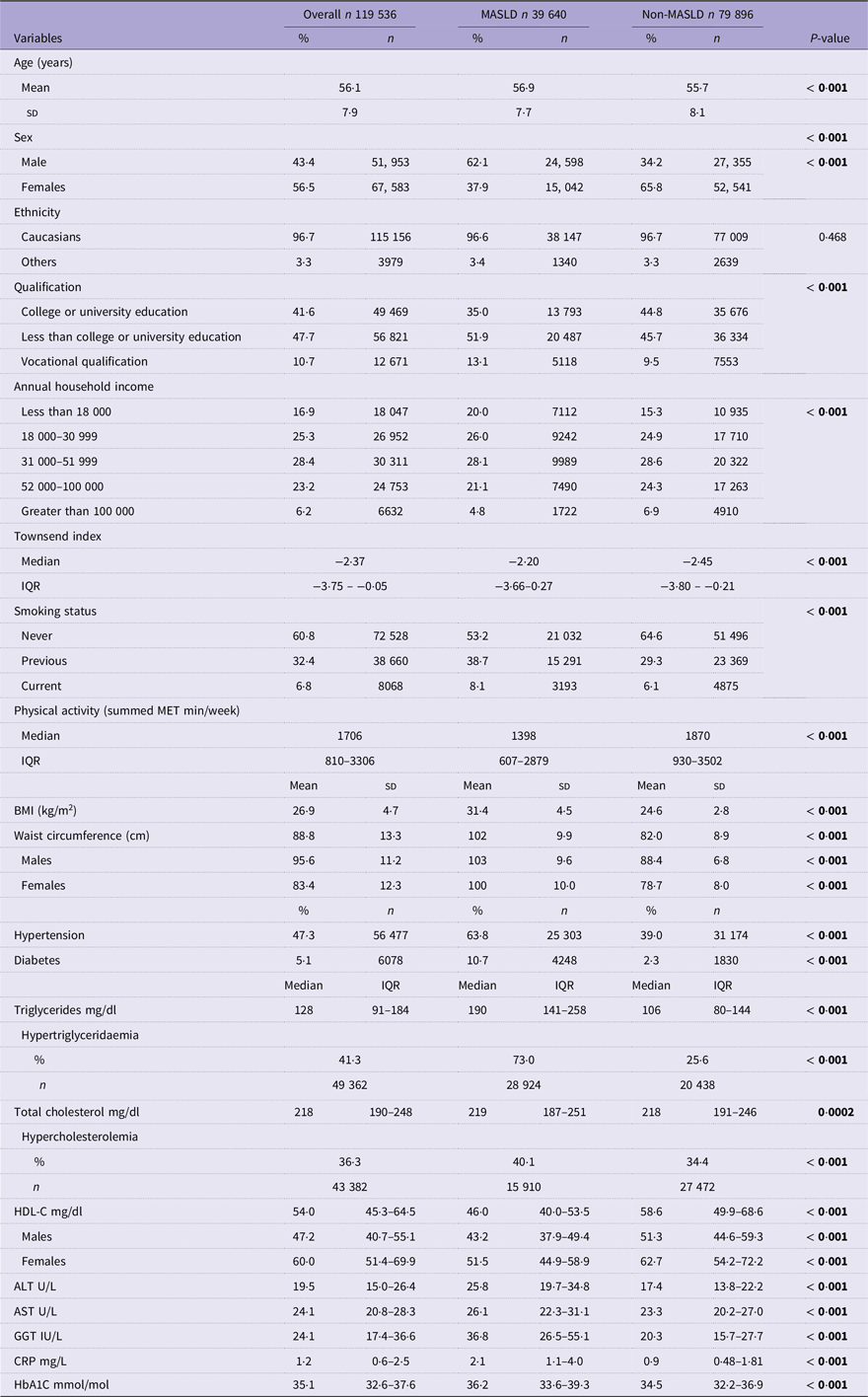
A total of 119 536 participants met the eligibility criteria and were included in the full analytical sample, with a mean age of 56·1 years and 43·4 % being males (Table 1). MASLD prevalence estimated with FLI from baseline and liver imaging from instance 2 were 33·1 % and 20·3 %, respectively. The prevalence of diabetes and hypertension estimated from baseline data was 5·1 % and 47·2 %, respectively, while 40·7 % were overweight and 21·5 % had obesity. The baseline characteristics of participants classified by MASLD status are reported in Table 1.
Characteristics of study population classified by MASLD status

MASLD, Metabolic dysfunction-associated steatotic liver disease; IQR, interquartile range; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CRP, C-reactive protein; GGT, gamma-glutamyl transferase; HbA1C, glycated Hb. Statistically significant p-vales are indicated in bold.
MASLD was determined by the presence of hepatic steatosis estimated by fatty liver index ≥ 60, plus the presence of at least one of five cardiometabolic risk factors including: being overweight or obese, presence of diabetes, hypertension, hypertriglyceridaemia- or low HDL levels.
t test, Mann–Whitney U test and χ 2 was used to test association between MASLD v. non-MASLD group. Values are reported as mean (sd) for continuous variables or median (interquartile range) for non-normally distributed variables, and as percentage (frequency) for categorical variables.
Dietary intake of participants with and without metabolic dysfunction-associated steatotic liver disease
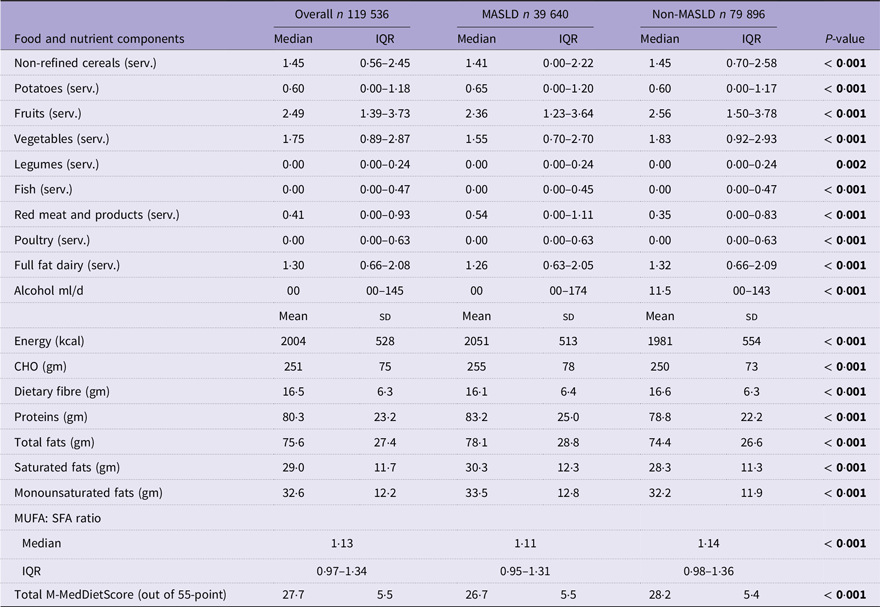
Notable differences were observed in food groups and nutrient intakes between those with and without MASLD. MASLD participants had significantly lower intake of non-refined cereals, fruits, vegetables and MUFA:SFA ratio compared with those without MASLD, indicating poor adherence to core dietary components of a traditional MedDiet (all P-values < 0·001). In contrast, individuals with MASLD reported significantly higher consumption of red meat, total energy, total fat and saturated fat (all P-values < 0·001). Collectively, these differences reflect an unhealthy dietary pattern in those with MASLD that may contribute to poorer metabolic health outcomes in this population. This ultimately resulted in a lower total M-MedDietScore (26·7 v. 28·2) in individuals with MASLD (P-value < 0·001) (Table 2).
Dietary profile of participants according to MASLD criteria for all Oxford Web Q cycles

CHO, carbohydrates; gm, grams; kcal, kilocalories; M-MedDietScore, Modified-Mediterranean Diet Score; ml, millilitre; MASLD, metabolic dysfunction-associated fatty liver disease; serv., servings. Values are presented as mean (sd) for normally distributed variables and as median (interquartile range) for non-normally distributed variables. Statistically significant p-vales are indicated in bold.
Independent t tests and Mann–Whitney U tests were used to compare differences between MASLD and non-MASLD groups. A P-value of < 0·05 was considered statistically significant.
Association between MedDiet and risk of metabolic dysfunction-associated steatotic liver disease
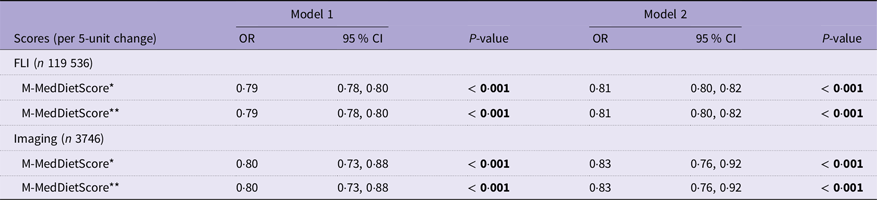
In all participants, each five-unit increase in the M-MedDietScore was associated with a significantly lower likelihood of MASLD, with 19 % lower odds when using the FLI as a surrogate marker of liver fat (OR: 0·81, 95 % CI: 0·80, 0·82), after adjustment for sociodemographic, lifestyle and clinical covariates in Model 2 (Table 3). Comparable associations were observed using imaging-derived liver fat data from instance 2, where each five-unit increase in the M-MedDietScore was associated with 17 % lower odds of MASLD (OR: 0·83, 95 % CI: 0·76, 0·92). In the sensitivity analysis excluding the MUFA:SFA ratio from the total M-MedDietScore, similar inverse association was observed in both participants diagnosed using FLI and those with imaging-based diagnosis following fully adjusted Model 2 (Table 3).
Association of MedDiet with MASLD

MASLD, metabolic dysfunction-associated fatty liver disease; FLI, fatty liver index; M-MedDietScore, Modified-Mediterranean Diet Score. Statistically significant p-vales are indicated in bold.
Model 1 adjusted for age, sex, ethnicity, qualification, annual household income, Townsend deprivation index, smoking status, physical activity and total energy intake.
Model 2 further adjusted for diabetes, hypertension, total cholesterol, HDL cholesterol, LDL cholesterol and CVD incidence occurred before the exposure variable.
Binary logistic regression analysis used to assess the association of MASLD assessed through FLI and imaging with 5-unit scaled M-MedDietScore.
* M-MedDietScore with MUFA:SFA ratio.
** M-MedDietScore without MUFA:SFA ratio.
Association between MedDiet and incident hospitalisation
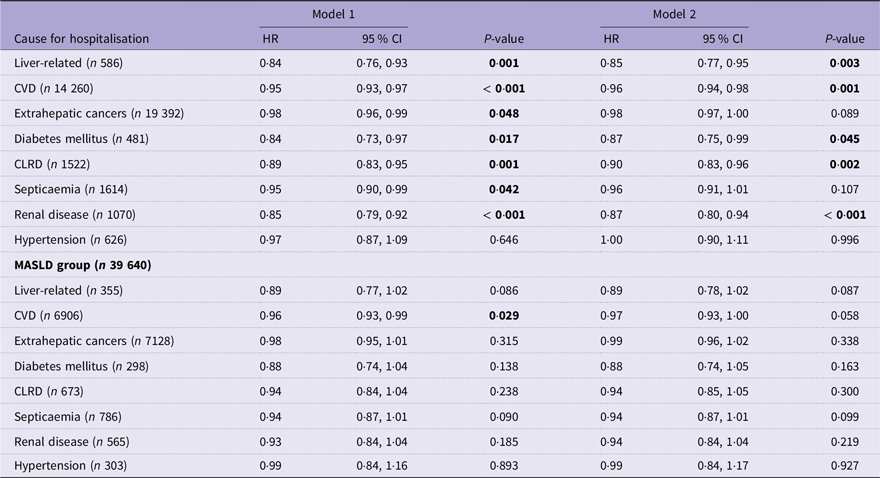
In the fully adjusted Cox proportional hazard model (Model 2), greater adherence to a MedDiet, reflected by a higher M-MedDietScore, was significantly associated with a reduced risk of hospitalisation for several conditions commonly linked to MASLD in the full analytical sample (Table 4). Each five-unit increase in the M-MedDietScore was associated with a 15 % lower risk of liver-related hospitalisation (hazard ratio (HR): 0·85, 95 % CI: 0·77, 0·95), a 4 % lower risk of CVD-related hospitalisation (HR: 0·96, 95 % CI: 0·94, 0·98), and a 10–13 % reduced risk of hospitalisation due to diabetes (HR: 0·87, 95 % CI: 0·75, 0·99), chronic lower respiratory disease (HR: 0·90, 95 % CI: 0·83, 0·96), and renal disease (HR: 0·87, 95 % CI: 0·80, 0·94). No significant associations were observed for hospitalisations due to extrahepatic cancers, septicaemia or hypertension.
Association between MedDiet and incident hospitalisation in overall cohort (n 119 536) and in the MASLD cohort (n 39 640) during a 10·1-year period

MASLD, metabolic dysfunction-associated fatty liver disease; CLRD, chronic lower respiratory disease; HR, hazard ratio. Statistically significant p-vales are indicated in bold.
Model 1 adjusted for age, sex, ethnicity, qualification, annual household income, Townsend deprivation index, smoking status, physical activity and total energy intake. Model 2 further adjusted for diabetes, hypertension, total cholesterol, HDL cholesterol and LDL cholesterol.
Cox proportional hazard analysis used to assess the relationship of incident hospitalisation with five-unit scaled M-MedDietScore.
In the MASLD subgroup (n 39 640), each five-unit increase in the M-MedDietScore was significantly associated with a reduced risk of CVD-related hospitalisation in the sociodemographic and lifestyle-adjusted model (Model 1: HR: 0·96, 95 % CI: 0·93, 0·99; P-value 0·029). However, this association was attenuated and became non-significant after further adjustment for CVD risk factors in Model 2 (HR: 0·97, 95 % CI: 0·93, 1·00; P-value 0·058). No other significant associations were observed for hospitalisation due to any cause in either model within MASLD subgroup (Table 4).
Association between MedDiet and all-cause and cause-specific mortality
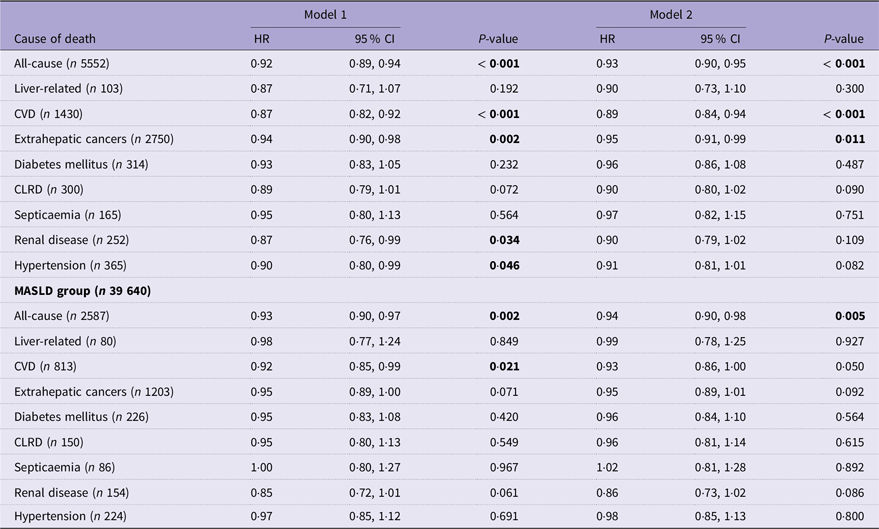
Of the 119 536 participants, a total of 5552 deaths occurred over a median follow-up of 9·7 years. In the fully adjusted model (Model 2), higher adherence to the MedDiet was significantly associated with a 7 % reduced risk for all-cause mortality (HR: 0·93, 95 % CI: 0·90, 0·95), an 11 % reduced risk for CVD mortality (HR: 0·89, 95 % CI: 0·84, 0·94) and a 5 % reduction in extrahepatic cancer mortality (HR: 0·95, 95 % CI: 0·91, 0·99) (Table 5). Although inverse associations were observed for renal-related and hypertension-related mortality in Model 1, these were no longer statistically significant in the fully adjusted Model 2 (all P-values > 0·05). No significant associations were found for mortality related to liver disease, diabetes, chronic lower respiratory disease or septicaemia (Table 5).
Association between MedDiet with all-cause and cause-specific mortality in the overall cohort (n 119 536) and in MASLD cohort (n 39 640) during a 9·7-year period

MASLD, metabolic dysfunction-associated fatty liver disease; CLRD, chronic lower respiratory disease; HR, hazard ratio. Statistically significant p-vales are indicated in bold.
Model 1 adjusted for age, sex, ethnicity, qualification, annual household income, Townsend deprivation index, smoking status, physical activity and total energy intake. Model 2 further adjusted for diabetes, hypertension, total cholesterol, HDL cholesterol and LDL cholesterol.
Cox proportional hazard analysis used to assess the relationship of all-cause and cause-specific mortality with five-unit scaled M-MedDietScore.
In MASLD subgroup (n 39 640), each five-unit increase in the M-MedDietScore was significantly associated with a 7 % reduction in all-cause mortality in Model 1 (HR: 0·93, 95 % CI: 0·90, 0·97) which remained significant in the fully adjusted (Model 2, HR: 0·94, 95 % CI: 0·90, 0·98) (Table 5). For CVD-related mortality, a significant 8 % reduction was observed in Model 1 (HR: 0·92, 95 % CI: 0·85, 0·99; P-value 0·021), but the association attenuated and became marginally significant (HR: 0·93, 95 % CI: 0·86, 1·00; P-value 0·050) after adjustment for CVD risk factors in Model 2. No statistically significant associations were observed for mortality related to any other cause in the MASLD subgroup (Table 5).
Discussion
This study conducted in the subsample of UK Biobank participants with complete dietary and clinical information showed that higher adherence to MedDiet was associated with a lower risk of prevalent MASLD. In the overall cohort, higher adherence to the MedDiet was linked to reduced risk of incident hospitalisation for liver-related, CVD, diabetes, chronic lower respiratory disease and renal disease. In the MASLD subgroup, the inverse association between higher MedDiet adherence and CVD-related hospitalisation was evident in the sociodemographic and lifestyle-adjusted model but attenuated after further adjustment for established CVD risk factors. Additionally, higher adherence to MedDiet was significantly associated with lower all-cause, CVD and extrahepatic cancer-related mortality in the full analytical sample. Higher MedDiet adherence was associated with lower all-cause and CVD-related mortality in those with MASLD after sociodemographic and lifestyle adjustment, and with lower all-cause mortality risk after further adjustment for clinical covariates. These findings underscore the potential benefits of the MedDiet in preventing MASLD prevalence and in reducing morbidity and mortality among individuals with established MASLD and associated comorbidities.
International guidelines support the provision of MedDiet as optimal for the prevention and management of MASLD(Reference Rinella, Neuschwander-Tetri and Siddiqui11,12) . To date, studies are lacking that assess the benefits of the MedDiet in Western countries where the MedDiet is not habitual, and there are limited studies that include longitudinal data exploring hospitalisation and mortality. The few studies conducted in Western countries indicate that MedDiet is associated with lower prevalence of MASLD(Reference Sualeheen, Tan and Georgousopoulou10) and optimises management(Reference Sualeheen, Tan and Georgousopoulou10). Despite overall adherence to the MedDiet being lower in Western populations compared with Mediterranean countries (Med population: MedDietScore 36/55 v. present study: 27·7/55)(Reference Foscolou, D’Cunha and Naumovski40), even this more modest adherence was associated with reduced all-cause and CVD-related mortality in individuals with MASLD in the present study. Findings from European non-Mediterranean regions including the general population from England (n 9645) and Switzerland (n 957) showed inverse associations between MASLD and higher adherence to the MedDiet(Reference Khalatbari-Soltani, Imamura and Brage41). A six week MedDiet intervention in an Australian biopsy MASLD cohort showed a significant reduction in hepatic steatosis and improved insulin sensitivity compared with low-fat high-carbohydrate diet (control)(Reference Ryan, Itsiopoulos and Thodis42). These protective associations of the MedDiet with MASLD, liver fibrosis and cardiometabolic outcomes have also been confirmed in several studies conducted in the general USA population(Reference Shah, Murthy and Allison43–Reference Konerman, Walden and Joseph46).
Currently, there is a lack of longitudinal studies in people with MASLD assessing the impact of diet, including the MedDiet, on morbidity and mortality. Previous research has consistently demonstrated the detrimental effects of cardiometabolic risk factors on all-cause mortality in MASLD, with the risk of all-cause mortality increasing proportionally with each additional risk factor(Reference Li, Chen and Deng47). Our results indicate that modifiable lifestyle factors including diet that were assessed in relation to mortality in MASLD, demonstrated that adherence to a MedDiet reduced all-cause mortality, CVD and extrahepatic cancer-related mortality. These results are in line with findings from a Global Burden of Disease study highlighting that in addition to metabolic risk factors, diet independently drives the global burden and liver-related mortality(Reference Paik, Mir and Alqahtani48). This was further supported by an analysis of the USA NHANES database, which included 3548 participants with fatty liver as determined by the FLI(Reference Vilar-Gomez, Vuppalanchi and Gawrieh49). Higher diet quality, assessed using the Healthy Eating Index-2015, was associated with lower CVD, cancer-specific and all-cause mortality(Reference Vilar-Gomez, Vuppalanchi and Gawrieh49). Our results reinforce the importance of high-quality diets, particularly adherence to the MedDiet, for reducing morbidity and mortality, which supports current clinical recommendations that this diet is optimal for management of MASLD and risk reduction(Reference Rinella, Neuschwander-Tetri and Siddiqui11,Reference Eslam, Sarin and Wong50,51) .
Evidence suggests that CVD-related mortality (10·3 %) is the second leading cause of death after liver-related mortality (45·8 %) among all deaths in the USA. MASLD population(Reference Golabi, Paik and Eberly37) and people with MASLD have more than a two-fold increased likelihood of non-fatal CVD than those without MASLD(Reference Targher, Byrne and Lonardo52). Our findings indicate that adherence to the MedDiet was protective against incident hospitalisation due to liver-related conditions and CVD, as well as CVD-related mortality, both in the overall UK Biobank cohort and among individuals with established MASLD. These findings align with a meta-analysis of observational studies that examined the association between adherence to the MedDiet and the risk of CVD incidence and mortality(Reference Rosato, Temple and La Vecchia53). In this study, individuals with the highest adherence to the MedDiet had a significant 21–39 % lower relative risk of CVD compared with those with the lowest adherence, both in Mediterranean populations (relative risk: 0·61, 95 % CI: 0·46, 0·79) and in the non-Mediterranean populations (relative risk: 0·79, 95 % CI: 0·70, 0·89)(Reference Rosato, Temple and La Vecchia53). MASLD is closely linked to early atherosclerosis, as reflected by increased carotid intima-media thickness (IMT-CC) and one study in obese patients with MASLD reported that IMT-CC was predicted by eotaxin levels and the severity of hepatic steatosis(Reference Tarantino, Costantini and Finelli54). In parallel, the CORDIOPREV trial showed that a MedDiet, compared with a low-fat diet, reduced carotid IMT-CC and carotid plaque height over long-term follow-up, supporting the potential vascular benefit of the MedDiet(Reference Jimenez-Torres, Alcalá-Diaz and Torres-Peña55). Collectively, these findings underscore the robust and consistent cardiovascular benefits of MedDiet across diverse populations and highlight its critical role as a dietary strategy for reducing CVD burden including mortality particularly in those with established MASLD.
A major strength of this study is its large sample size of nearly 120 000 participants, along with the use of cause-specific hospitalisation and mortality data. Both primary and secondary contributory causes of mortality were screened and included in the analysis. To capture accurate dietary intake information, the UK Biobank study employed the Oxford WebQ, a validated web-based 24-hour dietary recall questionnaire designed to minimise respondent burden and reduce measurement error. Additionally, participants with implausible dietary energy intakes were excluded from the analysis. However, this study has several limitations that warrant consideration. First, due to the absence of liver imaging data at baseline, MASLD was identified using the FLI, a biochemical-based algorithm. While not definitive, FLI has demonstrated acceptable diagnostic accuracy for predicting MASLD in large national databases(Reference Sualeheen, Tan and Daly34). Second, some participants had only one 24-hour dietary recall, which may not accurately reflect habitual dietary intake. However, sensitivity analyses stratified by participants with 1 d v. ≥ 2 dietary recalls demonstrated consistent findings (online Supplementary Table S2), with the inverse association between M-MedDietScore and MASLD remaining unchanged, suggesting that the observed relationship is robust while allowing us to preserve the representativeness and statistical power of the sample. Third, a substantial proportion of participants had missing data on multiple covariates. To maximise sample size, minimise selection bias and to address missing data in the survival analysis, multiple imputation was conducted using the Nelson–Aalen estimator to account for missing covariates. Fourth, the frequency of olive oil consumption, a component of the MedDietScore, was unavailable in the UK Biobank dataset; thus, this component was substituted with the MUFA:SFA ratio, and a sensitivity analysis was conducted excluding the olive oil component from the score confirming it didn’t alter outcomes. Finally, the cohort was predominantly of Caucasian ancestry, which may limit the generalisability of findings to more ethnically diverse populations, especially given the known variability in MASLD susceptibility across various ethnic groups(Reference Rich, Oji and Mufti56). This sample may also not be generalisable to the general population given the potential of healthy volunteer selection bias.
Conclusion
Greater adherence to the MedDiet, as assessed by the M-MedDietScore, was associated with lower likelihood of MASLD in a subsample of UK Biobank participants with complete dietary and clinical information. In this full analytical sample, higher adherence to the MedDiet was associated with a reduced incidence of several MASLD-related hospitalisations and mortality. Among participants with MASLD, greater adherence was associated with lower CVD incidence and mortality after adjustment for sociodemographic and lifestyle factors. This study supports the recommendation of MedDiet for the prevention and management of MASLD in Western, non-Mediterranean populations. Thus, access to dietary intervention to support the adoption of MedDiet could serve as a management strategy for MASLD and preventative strategy that may help reduce the burden of hepatic and CVD in Western, non-Mediterranean populations.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107351
Acknowledgements
We thank Dr Gavin Abbott (Institute for Physical Activity and Nutrition, Deakin University) for his valuable biostatistical guidance and support.
E. S. G. was supported by a Deakin University Faculty of Health Dean’s Postdoctoral Fellowship while conducting this study.
E. S. G.: Conceptualisation (lead); writing and review (equal); formal analysis (A. S.) lead interpretation E. S, G and A. S. equal. A. S.: Data curation (lead); Investigation (equal); formal analysis (equal); writing (equal). All other authors contributed intellectually to the manuscript including reviewing and editing.
All authors declare no conflict of interest.



 Open access
Open access