



Introduction
A healthy and balanced diet during pregnancy is essential for foetal growth and development, and for maternal health throughout pregnancy. Behaviours during pregnancy can have long-term impacts on both mother and infant(Reference de Seymour, Beck and Conlon1,Reference Marshall, Abrams, Barbour, Catalano, Christian and Friedman2) . Poor quality diet during pregnancy has been associated with increased risk of inappropriate gestational weight gain(Reference Dolatian, Sharifi, Mahmoodi, Fathnezhad-kazemi, Bahrami-vazir and Rashidian3), pre-eclampsia(Reference Lokeswara, Hiksas, Irwinda and Wibowo4), and miscarriage(Reference Chung, Melo, Pickering, Dhillon-Smith, Coomarasamy and Devall5). Maternal undernutrition, micronutrient deficiencies, and overnutrition have been linked with poor infant outcomes, including preterm birth, intrauterine growth restriction, low birth weight, stillbirth, and macrosomia(Reference Lassi, Padhani, Salam, Bhutta, Saavedra and Dattilo6). Suboptimal maternal nutrition can have intergenerational implications, including the increased risk of chronic diseases such as coronary heart disease, hypertension, and type 2 diabetes(Reference Lassi, Padhani, Salam, Bhutta, Saavedra and Dattilo6,Reference Barker7) .
Pregnancy is often considered a ‘teachable moment’ when mothers may be more motivated to adopt positive behavioural changes, including improving their nutrition habits, than at other times across the lifecycle(Reference de Seymour, Beck and Conlon1,Reference Willcox, Campbell, McCarthy, Lappas, Ball and Crawford8) . This increased awareness is often attributed to their perception that good nutrition is important for the health and well-being of their child(Reference Grenier, Atkinson, Mottola, Wahoush, Thabane and Xie9). Pregnancy is thus an opportune time for health promotion as it is a period when a woman may focus on improving her own health and that of her foetus(Reference de Seymour, Beck and Conlon1).
Pregnancy nutrition education includes the provision of information and guidance on optimal nutritional practices to support a healthy pregnancy. Pregnancy nutrition education is a critical aspect of provision of nutrition and dietary support to optimise short- and long-term health outcomes for both the mother and baby. Key components of general nutritional health promotion in pregnancy include following a balanced diet as specified in pregnancy nutrition guidelines, appropriate energy and macronutrient intake, micronutrient intake and supplementation, hydration, and food safety (for example, avoiding listeria risks)(10,Reference Forbes, Graham, Berglund and Bell11) . General nutrition education can be provided to pregnant women by a variety of health care professionals, including midwives, obstetricians, and general practitioners. More specialised nutrition advice, such as medical nutrition therapy for conditions such as gestational diabetes mellitus, should be provided by accredited practising dietitians or registered dietitians, where available, to outline specific guidelines for both diet adequacy as well as management of the condition(Reference Andersen, Baird, Bates, Chapel, Cline and Ganesh12,Reference Weenen, Commandeur and Claassen13) . Overall, nutrition education aims to help women make informed choices about their diet to improve diet quality and overall well-being(Reference Marshall, Abrams, Barbour, Catalano, Christian and Friedman2,Reference Girard and Olude14) .
Providing nutrition education during pregnancy can generate awareness that may affect women’s nutritional behaviour in the longer term, influencing the overall health of the family unit(Reference Szwajcer, Hiddink, Koelen and van Woerkum15,Reference Arrish, Yeatman and Williamson16) . However, there is evidence suggesting that a women’s intention to improve nutrition during pregnancy does not always come with a commensurate increase in nutrition education from maternal health care providers(Reference Lucas, Charlton and Yeatman17). Studies have found that even when women are provided with education materials during pregnancy, they may not understand the intent of the nutrition messages if a health professional does not emphasise the importance or does not deliver it in a way that is meaningful, tailored, or accessible for the person(Reference Szwajcer, Hiddink, Koelen and van Woerkum18). Ensuring adequate nutrition education provision by health care providers during pregnancy is crucial, as such practices can influence improved pregnancy outcomes(Reference Ibikunle, Okafor and Adejimi19).
Despite the importance of nutrition education in supporting maternal health, the content and timing of this education varies. There is also considerable variation in the term ‘pregnancy outcomes’, which can include both maternal and neonatal outcomes(Reference Hong, Hwang, Han, Chae, Choi and Jeong20). Although some reviews have explored the effects of nutrition education on specific maternal outcomes, such as gestational diabetes mellitus(Reference Helm, Izuora and Basu21) and gestational weight gain(Reference Girard and Olude14), to our knowledge no review to date has included a combined summary of most commonly reported maternal pregnancy outcomes that have been considered outcomes targeted via delivery of nutrition education. This review addresses this gap and aims to comprehensively summarise the types of maternal outcomes that have been addressed through nutrition education programmes and interventions and the most useful approaches to positively impacting maternal health.
Method
A scoping review is considered the most suitable approach for addressing comprehensive research questions, identifying literature gaps, and facilitating the initiation of future studies(Reference Tricco, Lillie, Zarin, O’brien, Colquhoun and Kastner22). The selection, analysis, and reporting of study results were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines(Reference McInnes, Moher, Thombs, McGrath, Bossuyt and Clifford23). The search strategy was prospectively registered online with PROSPERO in July 2022 (CRD42022345130).
Eligibility criteria
Eligible publications in this review were selected based on the following PICOS criteria: (1) participation (P): pregnant women without any pregnancy complications or pre-pregnancy comorbidities; (2) intervention (I): nutrition education, which may include practical approaches (for example, cooking classes, demonstrations) or theoretical approaches (for example, dietary counselling, advice). Nutrition education could be provided as a standalone intervention or combined with other interventions, such as physical activity programmes. There were no limitations on the time of the programme or intervention; (3) comparison (C): standard prenatal/antenatal care or non-intervention groups; (4) outcomes (O): maternal outcomes, including those related to maternal health and well-being, such as gestational diabetes mellitus, or those related to behaviour, such as nutritional knowledge; study design (S): all study designs were included. A time limit was not imposed on this search to ensure all relevant studies were considered.
Publications were excluded if they only focused on neonatal or infant health outcomes. Non-English language papers, conference abstracts, and non-empirical studies, including editorials, theses, and reviews were excluded.
Search strategy
Key thematic areas searched were pregnancy, nutrition education, and interventions or programmes. Search terms were program* OR intervention* OR behavior* OR behaviour* OR education* AND pregnan* AND nutrition* OR diet*. Boolean search operators were adjusted for each database searched, as required. The search strategy was allied to the following electronic databases: Medline, Embase, CINAHL, Global Health, Scopus, PsycARTICLES, SocINDEX, Academic Search Complete. The initial search was undertaken in July 2022 and was updated in September 2024.
Following the systematic search, all identified citations were uploaded into Covidence(24), a web-based software platform designed to support the research review process. Duplicate search results were then removed. All titles and abstracts were screened by the first author (F.H.M.) and by a second author. Full texts were screened by the first author (F.H.M.) and additionally by a second author. Disagreement between authors regarding study inclusion was resolved through discussion to meet consensus. See Figure 1 for steps taken in the screening process.
PRISMA flowchart of the screening process and identification of eligible publications.

Figure 1. Long description
The flowchart illustrates the process of screening and identifying eligible publications for a study on maternal diet during pregnancy. It begins with 34,395 studies imported for screening. After removing 14,887 duplicates, 19,508 studies are screened, of which 18,932 are deemed irrelevant. This leaves 560 full-text studies assessed for eligibility. Out of these, 391 studies are excluded for various reasons, including being conference abstracts, lacking maternal outcomes, not being in English, having wrong outcomes, lacking an educational component, having a wrong study design, lacking a nutritional component, having unavailable full text, targeting the wrong patient population, or being a thesis/dissertation. Ultimately, 169 studies are included in the final analysis.
Data extraction and analysis
Data were extracted by the research team. Consistent with the scoping review methodology(Reference Tricco, Lillie, Zarin, O’brien, Colquhoun and Kastner22) aim of exploring the breath and depth of the evidence, rather than providing a detailed or meta-analysis, the data that enabled a characterisation of the landscape of evidence were extracted. Extracted data were reported in a table for analysis that included key characteristics of the study or report, research and data collection method, maternal outcomes under study, and intervention (if available). Given the variety of data present, data were also thematically analysed according to the type of maternal outcome. This allowed authors to draw common themes from the data. Thematic analysis considered the main themes identified within each of the included papers, which were then compared across the data set, resulting in a discussion of the main thematic areas across all included papers(Reference Neuendorf25).
Results
Publication selection
The search generated 34,395 articles from the following databases: Medline (11,567), Embase (6,211), CINAHL (4,152), Global Health (6,693), Scopus, PsycARTICLES (4), SocINDEX (284), Academic Search Complete (5,484); of these, 14,886 were duplicates. The titles and abstracts of 19,509 articles were read; 18,932 articles were excluded because they did not refer to a programme or intervention that sought to provide nutrition education during pregnancy. This left 560 articles for full-text review. The full text of 560 articles were reviewed; 391 articles were excluded as they did not meet the inclusion criteria. The remaining 169 studies were included in this review (see supplementary file 1 for a list of all included studies). The PRISMA(Reference Page, McKenzie, Bossuyt, Boutron, Hoffman and Mulrow26) flow diagram (Figure 1) presents the flowchart of the screening process and identification of the eligible publications.
Characteristics of included studies
The final selection of eligible publications included 102 randomised control trials (RCTs), 40 quasi-experimental studies, 11 cohort studies, seven retrospective cohort studies, two prospective cohort studies, and four cross-sectional studies. Across the whole sample, more than half of the studies were conducted from 2018 (n = 96, 57%). All but three RCTs were conducted after 2006, and most quasi-experimental studies (n = 27, 67%) were conducted after 2015. The remaining studies are more evenly spread across the period, as shown in Figure 2.
Bubble plot showing number of publications for different study designs by year.

Figure 2. Long description
A bubble plot displays the number of publications for different study designs by year. The x-axis represents the years from 1965 to 2025, while the y-axis is not explicitly labeled but implies different study designs. The plot includes various colored bubbles representing different study designs: green for RCT, dark blue for Retrospective cohort, light blue for Quasi experimental, yellow for Prospective cohort, orange for Cross sectional, and blue for Cohort. The size of the bubbles indicates the number of publications, with larger bubbles representing more publications. Notable clusters of larger bubbles appear around the years 2005 to 2025, particularly for the RCT and Quasi experimental study designs. The plot shows a significant increase in the number of publications over time, especially in the last two decades. All values are approximated.
Studies addressed a range of maternal outcomes through nutrition education. Primary maternal outcomes that were the focus of studies included were: gestational weight gain (GWG) (n = 63); prevention of gestational diabetes mellitus (GDM) (n = 21), gestational hypertension and/or preeclampsia (n = 13) and anaemia (n = 5); dietary outcomes (n = 52); nutritional status (n = 5); and nutritional knowledge, attitudes and/or behaviours (n = 27). A proportion of studies (n = 42) addressed multiple primary maternal outcomes. Most studies explored gestational weight gain, prevention of gestational diabetes mellitus, dietary outcomes, and nutritional knowledge, attitudes and/or behaviours were conducted from 2016, as shown in Figure 3.
Bubble plot showing number of publications for different maternal outcomes by year.

Figure 3. Long description
A bubble plot showing the number of publications for different maternal outcomes by year. The x-axis represents the years from 1965 to 2025, and the y-axis represents different maternal outcomes. The bubbles are color-coded to represent various outcomes: grey for Gestational Weight Gain, orange for Gestational Diabetes Mellitus, blue for Dietary outcomes, yellow for Nutritional knowledge, attitudes and behaviours, green for Hypertension, dark blue for Anaemia, and light blue for Nutritional status. The size of the bubbles indicates the number of publications. Larger bubbles represent more publications, and smaller bubbles represent fewer publications. The plot shows an increasing trend in the number of publications over time, with a significant rise in the number of publications from the 2000s onwards. The largest bubbles are seen in the years close to 2025, indicating a high number of publications in recent years. The plot highlights the growing research interest in maternal health outcomes over the years. All values are approximated.
Most studies (45%) were conducted in the USA (n = 21), Iran (n = 16), China (n = 15), Canada (n = 11), Finland (n = 11), and Australia (n = 10). In total, 156 individual research studies were included in the analysis. Studies with the largest number of publications included five resulting from the UPBEAT(Reference Poston, Briley, Barr, Bell, Croker and Coxon27–Reference Flynn, Seed, Patel, Barr, Bell and Briley31) trial from the UK, four from the Finnish Gestational Diabetes Prevention Study (RADIEL)(Reference Huvinen, Koivusalo, Meinilä, Valkama, Tiitinen and Rönö32–Reference Sahrakorpi, Rönö, Koivusalo, Stach-Lempinen, Eriksson and Roine35), and three each from the Lifestyle and Pregnancy (LIP)(Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jorgensen36–Reference Tanvig, Jensen, Andersen, Ovesen, Jørgensen and Vinter38) study from Denmark and the ROLO(Reference McGowan, Walsh, Byrne, Curran and McAuliffe39–Reference Conway, Cawley, Geraghty, Walsh, O’Brien and McAuliffe41) study from Ireland. Table 1 presents an overview of the number and type of study conducted for each maternal outcome (see supplementary table for the characteristics of the sample).
Overview of number and type of study conducted for each maternal outcome

Table 1. Long description
The table presents data on the number and type of studies conducted for various maternal outcomes. It includes columns for different study types such as RCT, Quasi-experimental, Cohort, Retrospective cohort, Cross-sectional, Prospective cohort, Intervention, and Total. The rows are categorized by maternal outcomes such as GWG, GDM, Anaemia, Dietary outcomes, Nutritional status, Nutritional knowledge, attitudes/behaviours, and Other. Each cell contains the count of studies conducted for each outcome and study type. Notable trends include a high number of RCTs for GWG and Dietary outcomes, and a significant number of Quasi-experimental studies for Nutritional knowledge, attitudes/behaviours.
GWG, gestational weight gain; GDM, gestational diabetes mellitus; Other: lignan concentrations, vitamin D status, induced abortion, health-related quality of life, and self-rated health.
Intervention delivery methods
Most studies (n = 90, 53%) employed individual education as their main nutrition education activity. Most studies that employed individual education activities were RCTs (n = 69) and quasi-experimental studies (n = 15). Eleven studies used home visits to conduct individualised sessions or follow-up education interventions(Reference Kafatos, Vlachonikolis and Codrington42–Reference Ilboudo, Savadogo, Traoré, Meda, Kinda and Sombié52). Four studies utilised WeChat forums as a primary method of education(Reference Ding, Gou, Guan, Wang, Bi and Hong53,Reference Xu, Lin, Fang, Cui, Li and Yu54) or as a supplement to other education activities(Reference Lin, Yang, Zhang and Wei55,Reference Li, Piaseu, Phumonsakul and Thadakant56) . Six studies used a smartphone application that had been specifically designed for the study(Reference Robertson and Ladlow57–Reference Hao, Yang, Wang, Lan, Xu and Wang62) and four studies used a website(Reference Olson, Groth, Graham, Reschke, Strawderman and Fernandez63–Reference Wilkinson, Fjeldsoe and Willcox66) to assist in delivering nutrition education, allowing participants to track their dietary intake and receive feedback. Four studies used the telephone as the main method of counselling(Reference Sagedal, Øverby, Bere, Torstveit, Lohne-Seiler and Småstuen67–Reference Hillesund, Bere, Sagedal, Vistad and Øverby70) and 11 used telephone/text message follow-ups to support the education intervention by answering participants’ questions and reminding them of the recommendations(Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Mohsenzadeh-Ledari, Taghizadeh, Keramat, Moosazadeh, Yazdani and Najafi71–Reference Peiris, Wijesinghe, Gunawardana, Weerasinghe, Rajapaksha and Rathnayake80) . About one-third (n = 61, 35%) of studies incorporated physical resources (pamphlets, booklets, leaflets) as a complement to other education activities in individual or group education sessions, while two studies used a written information package as the main method of intervention(Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Muhamad, Mahmudiono, Abihail, Sahila, Wangi and Suyanto82) . In two studies, mothers received vouchers for foods, fruit, and vegetables in addition to nutrition education(Reference Girard, Grant, Watkinson, Okuku, Wanjala and Cole83,Reference Lacci-Reilly and Brunner Huber84) , and 11 studies used cooking demonstrations or classes to show mothers how to prepare healthy meals(Reference Tesfaye, Tamiru and Belachew44,Reference Kieffer, Welmerink, Sinco, Welch, Rees Clayton and Schumann46,Reference Katenga-Kaunda, Kamudoni, Holmboe-Ottesen, Fjeld, Mdala and Shi47,Reference Hillesund, Bere, Sagedal, Vistad and Øverby70,Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Jahan, Roy, Mihrshahi, Sultana, Khatoon and Roy85–Reference Subapriya and Chandrasekhar90) . See Table 2 for an overview of intervention activities by study type and maternal outcomes.
Intervention activities by study type and maternal outcomes

Table 2. Long description
The table presents a comprehensive comparison of intervention activities by study type and maternal outcomes. It includes data on individual education, group education, and other intervention activities such as home visits, WeChat forums, smartphone applications, websites, telephone counseling, physical resources, vouchers, and cooking demonstrations. The table is divided into several columns: Study type (RCT, Quasi-experimental, Cohort, Cross-sectional), Intervention activities (Individual education, Group education, Home visit, Restructuring, Intervention materials, Sessions), and Maternal outcomes (GWG, GDM, Anaemia, Dietary outcomes, Nutritional status, Nutritional knowledge/behaviours). Each row provides specific details on the number of studies and their focus areas. For instance, individual education is the most common activity, with 90 studies, predominantly RCTs and quasi-experimental studies. Home visits, WeChat forums, smartphone applications, and websites are also utilized for delivering nutrition education. Physical resources like pamphlets and booklets complement other education activities in about one-third of the studies. Vouchers for foods and cooking demonstrations are additional methods used to promote maternal health. The table highlights the diverse approaches and their effectiveness in different study types and maternal outcomes.
GWG, gestational weight gain; GDM, gestational diabetes mellitus.
Targeted maternal health outcomes
Five areas of maternal health were the key outcomes for the studies included. These outcomes included gestational weight gain (n = 77, 44%), gestational diabetes mellitus (n = 32, 19%), hypertensive disorders of pregnancy (n = 13, 5%), nutritional status (n = 5, 3%), and iron deficiency anaemia (n = 5, 3%).
Gestational weight gain
Over one-third (n = 74, 44%) of studies described a programme or intervention that sought to address gestational weight gain (GWG)(Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jorgensen36,Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jørgensen37,Reference O’Brien, Alberdi, Geraghty and McAuliffe40,Reference Okesene-Gafa, Li, McKinlay, Taylor, Rush and Wall50,Reference Li, Piaseu, Phumonsakul and Thadakant56–Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Olson, Groth, Graham, Reschke, Strawderman and Fernandez63,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Wilkinson, Fjeldsoe and Willcox66–Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Liu, Liu, Hua and Chen72–Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Bosaeus, Hussain, Karlsson, Andersson, Hulthén and Svelander78,Reference Phelan, Phipps, Abrams, Darroch, Schaffner and Wing79,Reference Lacci-Reilly and Brunner Huber84,Reference Jahan, Roy, Mihrshahi, Sultana, Khatoon and Roy85,Reference Watt, Appel, Lopez, Flores and Lawhon87,Reference Atkinson, Maran, Dempsey, Perreault, Vanniyasingam and Phillips91–Reference Halisah, Nur, Taslim, Chalid, Juliaty and Mappaware138) . In these studies, GWG was evaluated as total weight gain, weekly weight gain, and/or adherence to recommended weight gain during pregnancy. The Institute of Medicine (IOM) recommendations were used in most studies (n = 53, 72%) to categorise pre-pregnancy body mass index (BMI) and determine recommendations for weight gain during pregnancy(Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jorgensen36,Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jørgensen37,Reference O’Brien, Alberdi, Geraghty and McAuliffe40,Reference Li, Piaseu, Phumonsakul and Thadakant56–Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Olson, Groth, Graham, Reschke, Strawderman and Fernandez63,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Wilkinson, Fjeldsoe and Willcox66–Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Liu, Liu, Hua and Chen72–Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Phelan, Phipps, Abrams, Darroch, Schaffner and Wing79,Reference Lacci-Reilly and Brunner Huber84,Reference Watt, Appel, Lopez, Flores and Lawhon87,Reference Atkinson, Maran, Dempsey, Perreault, Vanniyasingam and Phillips91–Reference Opie, Neff and Tierney93,Reference Hajian, Aslani, Sarbakhsh and Fathnezhad-Kazemi95,Reference Malavolti, Petrella, Bertarini, Cicchetti, Neri and Facchinetti97–Reference Hui, Back, Ludwig, Gardiner, Sevenhuysen and Dean100,Reference Peccei, Blake-Lamb, Rahilly, Hatoum and Bryant102,Reference Buckingham-Schutt, Ellingson, Vazou and Campbell103,Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105,Reference Xu, Guo, Zhang and Lu106,Reference Nagpal, Prapavessis, Campbell, de Vrijer, Bgeginski and Hosein108,Reference Sartorelli, Crivellenti, Baroni, de Andrade Miranda, da Silva Santos and Carvalho110,Reference Garmendia, Corvalan, Araya, Casanello, Kusanovic and Uauy112–Reference Soltani, Duxbury, Arden, Dearden, Furness and Garland114,Reference Althuizen, Van Der Wijden, Van Mechelen, Seidell and Van Poppel116,Reference Kinnunen, Raitanen, Aittasalo and Luoto118,Reference Hui, Back, Ludwig, Gardiner, Sevenhuysen and Dean120–Reference Barquiel, Calvo, Moreno-Domínguez, Martínez-Sánchez, Muner and Bedate122,Reference Rauh, Gabriel, Kerschbaum, Schuster, von Kries and Amann-Gassner124–Reference Dorise, Byth, McGee, Wood and Blumenthal126,Reference Ghani and Khalaf129–Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131,Reference Vesco, Karanja, King, Gillman, Leo and Perrin133,Reference Guelinckx, Devlieger, Mullie and Vansant137,Reference Luo, Dong and Zhou139) . Almost one-third of the studies (n = 30, 40%) included participants who were living with overweight or obesity at the beginning of the study(Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jorgensen36,Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jørgensen37,Reference Okesene-Gafa, Li, McKinlay, Taylor, Rush and Wall50,Reference Robertson and Ladlow57,Reference Li, Aris, Han and Tan59,Reference Redman, Gilmore, Breaux, Thomas, Elkind-Hirsch and Stewart60,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Wilkinson, Fjeldsoe and Willcox66,Reference Liu, Wilcox, Wingard, Turner-McGrievy, Hutto and Burgis68,Reference Ferrara, Hedderson, Brown, Ehrlich, Tsai and Feng92,Reference Opie, Neff and Tierney93,Reference Hajian, Aslani, Sarbakhsh and Fathnezhad-Kazemi95,Reference Malavolti, Petrella, Bertarini, Cicchetti, Neri and Facchinetti97,Reference Peccei, Blake-Lamb, Rahilly, Hatoum and Bryant102,Reference Liu, Zhang, Zheng, Liang, Zhang and Tian104,Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105,Reference Mottola, Giroux, Gratton, Hammond, Hanley and Harris107,Reference Dodd, Kannieappan, Grivell, Deussen, Moran and Yelland109–Reference McGiveron, Foster, Pearce, Taylor, McMullen and Langley-Evans111,Reference Soltani, Duxbury, Arden, Dearden, Furness and Garland114,Reference Haby, Berg, Gyllensten, Hanas and Premberg115,Reference Kinnunen, Raitanen, Aittasalo and Luoto118,Reference Barquiel, Calvo, Moreno-Domínguez, Martínez-Sánchez, Muner and Bedate122,Reference Dorise, Byth, McGee, Wood and Blumenthal126,Reference Shirazian, Faris, Fox, Friedman and Rebarber130,Reference Lindholm, Norman, Kilander and Altman132,Reference Vesco, Karanja, King, Gillman, Leo and Perrin133,Reference Haby, Glantz, Hanas and Premberg135,Reference Guelinckx, Devlieger, Mullie and Vansant137) , while 13 studies included participants across all categories of BMI, from underweight to obesity(Reference Sandborg, Söderström, Henriksson, Bendtsen, Henström and Leppänen58,Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Abdel-Aziz, Hegazy, Mohamed, Kasem and Hagag73,Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Atkinson, Maran, Dempsey, Perreault, Vanniyasingam and Phillips91,Reference Hui, Ludwig, Gardiner, Sevenhuysen, Murray and Morris94,Reference Asbee, Jenkins, Butler, White, Elliot and Rutledge99,Reference Xu, Guo, Zhang and Lu106,Reference Krebs, Lorenz, Nawabi, Alayli and Stock113,Reference Althuizen, Van Der Wijden, Van Mechelen, Seidell and Van Poppel116,Reference Hui, Back, Ludwig, Gardiner, Sevenhuysen and Dean120,Reference Adam, Jarman, Barker, Manca, Lawrence and Bell121) . Five studies specifically focused on participants with pre-pregnancy BMI in the ‘healthy weight’ category(Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Liu, Liu, Hua and Chen72,Reference Bosaeus, Hussain, Karlsson, Andersson, Hulthén and Svelander78,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Ghani and Khalaf129) . In 28 studies (38%), pregnancy gestation on entry into the programme or intervention was less than 14 weeks of gestation (first trimester) (Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jorgensen36,Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jørgensen37,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Sandborg, Söderström, Henriksson, Bendtsen, Henström and Leppänen58,Reference Redman, Gilmore, Breaux, Thomas, Elkind-Hirsch and Stewart60,Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Abdel-Aziz, Hegazy, Mohamed, Kasem and Hagag73,Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Bosaeus, Hussain, Karlsson, Andersson, Hulthén and Svelander78,Reference Watt, Appel, Lopez, Flores and Lawhon87,Reference Malavolti, Petrella, Bertarini, Cicchetti, Neri and Facchinetti97,Reference Di Carlo, Iannotti, Sparice, Chiacchio, Greco and Tommaselli101,Reference Buckingham-Schutt, Ellingson, Vazou and Campbell103–Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105,Reference McGiveron, Foster, Pearce, Taylor, McMullen and Langley-Evans111,Reference Krebs, Lorenz, Nawabi, Alayli and Stock113–Reference Althuizen, Van Der Wijden, Van Mechelen, Seidell and Van Poppel116,Reference Kinnunen, Raitanen, Aittasalo and Luoto118,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Ghani and Khalaf129,Reference Shirazian, Faris, Fox, Friedman and Rebarber130,Reference Lindholm, Norman, Kilander and Altman132,Reference Gopalan, Haque, Ahmad, Gaur and Misra136,Reference Luo, Dong and Zhou139) , and three studies did not report on pregnancy gestation at the start of the programme or intervention(Reference Robertson and Ladlow57,Reference Lacci-Reilly and Brunner Huber84,Reference Li, Wang, Wang, Zhang and Sun96) .
Most of these studies were RCTs (n = 51, 69%)(Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jorgensen36,Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jørgensen37,Reference O’Brien, Alberdi, Geraghty and McAuliffe40,Reference Okesene-Gafa, Li, McKinlay, Taylor, Rush and Wall50,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Sandborg, Söderström, Henriksson, Bendtsen, Henström and Leppänen58–Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Olson, Groth, Graham, Reschke, Strawderman and Fernandez63,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Sagedal, Øverby, Bere, Torstveit, Lohne-Seiler and Småstuen67,Reference Liu, Wilcox, Wingard, Turner-McGrievy, Hutto and Burgis68,Reference Abdel-Aziz, Hegazy, Mohamed, Kasem and Hagag73,Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Bosaeus, Hussain, Karlsson, Andersson, Hulthén and Svelander78,Reference Phelan, Phipps, Abrams, Darroch, Schaffner and Wing79,Reference Jahan, Roy, Mihrshahi, Sultana, Khatoon and Roy85,Reference Atkinson, Maran, Dempsey, Perreault, Vanniyasingam and Phillips91,Reference Ferrara, Hedderson, Brown, Ehrlich, Tsai and Feng92,Reference Hui, Ludwig, Gardiner, Sevenhuysen, Murray and Morris94–Reference Li, Wang, Wang, Zhang and Sun96,Reference Asbee, Jenkins, Butler, White, Elliot and Rutledge99–Reference Sartorelli, Crivellenti, Baroni, de Andrade Miranda, da Silva Santos and Carvalho110,Reference Garmendia, Corvalan, Araya, Casanello, Kusanovic and Uauy112,Reference Krebs, Lorenz, Nawabi, Alayli and Stock113,Reference Althuizen, Van Der Wijden, Van Mechelen, Seidell and Van Poppel116–Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Razzazi, Griffiths and Alimoradi127,Reference Vesco, Karanja, King, Gillman, Leo and Perrin133,Reference Guelinckx, Devlieger, Mullie and Vansant137) , with a smaller number being quasi-experimental (n = 11, 16%)(Reference Liu, Liu, Hua and Chen72,Reference Watt, Appel, Lopez, Flores and Lawhon87,Reference Opie, Neff and Tierney93,Reference McGiveron, Foster, Pearce, Taylor, McMullen and Langley-Evans111,Reference Soltani, Duxbury, Arden, Dearden, Furness and Garland114,Reference Haby, Berg, Gyllensten, Hanas and Premberg115,Reference Long, Martin and Janson-Sand128,Reference Ghani and Khalaf129,Reference Rajbir, Sukhvinder and Sangha134,Reference Haby, Glantz, Hanas and Premberg135,Reference Halisah, Nur, Taslim, Chalid, Juliaty and Mappaware138) , cohort (n = 6, 10%)(Reference Robertson and Ladlow57,Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Malavolti, Petrella, Bertarini, Cicchetti, Neri and Facchinetti97,Reference Shirazian, Faris, Fox, Friedman and Rebarber130–Reference Lindholm, Norman, Kilander and Altman132) , or cross-sectional (n = 3, 45) (Reference Wilkinson, Fjeldsoe and Willcox66,Reference Tajirika-Shirai, Takimoto, Yokoyama, Kaneko, Kubota and Miyasaka98,Reference Dorise, Byth, McGee, Wood and Blumenthal126) . About half of these studies were conducted in the USA (n = 15, 20%)(Reference Redman, Gilmore, Breaux, Thomas, Elkind-Hirsch and Stewart60,Reference Olson, Groth, Graham, Reschke, Strawderman and Fernandez63,Reference Liu, Wilcox, Wingard, Turner-McGrievy, Hutto and Burgis68,Reference Phelan, Phipps, Abrams, Darroch, Schaffner and Wing79,Reference Lacci-Reilly and Brunner Huber84,Reference Watt, Appel, Lopez, Flores and Lawhon87,Reference Ferrara, Hedderson, Brown, Ehrlich, Tsai and Feng92,Reference Asbee, Jenkins, Butler, White, Elliot and Rutledge99,Reference Peccei, Blake-Lamb, Rahilly, Hatoum and Bryant102,Reference Buckingham-Schutt, Ellingson, Vazou and Campbell103,Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105,Reference Dirige, McNutt, Hamatake, McGee and Manayan117,Reference Long, Martin and Janson-Sand128,Reference Shirazian, Faris, Fox, Friedman and Rebarber130,Reference Vesco, Karanja, King, Gillman, Leo and Perrin133) , Australia (n = 8, 10.5%)(Reference Robertson and Ladlow57,Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Wilkinson, Fjeldsoe and Willcox66,Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Opie, Neff and Tierney93,Reference Dodd, Kannieappan, Grivell, Deussen, Moran and Yelland109,Reference Dorise, Byth, McGee, Wood and Blumenthal126) , Canada (n = 8, 10.5%)(Reference Atkinson, Maran, Dempsey, Perreault, Vanniyasingam and Phillips91,Reference Hui, Ludwig, Gardiner, Sevenhuysen, Murray and Morris94,Reference Hui, Back, Ludwig, Gardiner, Sevenhuysen and Dean100,Reference Mottola, Giroux, Gratton, Hammond, Hanley and Harris107,Reference Nagpal, Prapavessis, Campbell, de Vrijer, Bgeginski and Hosein108,Reference Hui, Back, Ludwig, Gardiner, Sevenhuysen and Dean120,Reference Adam, Jarman, Barker, Manca, Lawrence and Bell121,Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131) , and China (n = 8,10.5%)(Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Liu, Liu, Hua and Chen72,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Li, Wang, Wang, Zhang and Sun96,Reference Liu, Zhang, Zheng, Liang, Zhang and Tian104,Reference Xu, Guo, Zhang and Lu106,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Luo, Dong and Zhou139) . Population sizes of studies exploring GWG ranged from 2,925(Reference Garmendia, Corvalan, Araya, Casanello, Kusanovic and Uauy112) to 12(Reference Li, Aris, Han and Tan59), with an average sample size of 241 (SD 473). Thirteen of the 74 studies (18%) employed a theoretical framework. Six studies employed the Social Cognitive Theory(Reference Sandborg, Söderström, Henriksson, Bendtsen, Henström and Leppänen58,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Liu, Wilcox, Wingard, Turner-McGrievy, Hutto and Burgis68,Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Ferrara, Hedderson, Brown, Ehrlich, Tsai and Feng92,Reference Xu, Guo, Zhang and Lu106) , two employed the Transtheoretical Model of Behaviour Change(Reference Liu, Liu, Hua and Chen72,Reference Ghani and Khalaf129) , and one study each employed the Health Belief Model(Reference Jing, Huang, Liu, Luo, Yang and Liao76), the Theory of Planned Behaviour(Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105), a Biopsychosocial Framework(Reference Watt, Appel, Lopez, Flores and Lawhon87), Health Action Process Approach(Reference Razzazi, Griffiths and Alimoradi127), and the Integrative Model of Behaviour Prediction and the Behaviour Model for Persuasive Design(Reference Olson, Groth, Graham, Reschke, Strawderman and Fernandez63).
Most studies (n = 47, 63.5%) employed individual counselling activities as the main nutritional education intervention, while seven (9.5%) studies provided group education sessions (see Table 2). Participants in 21 studies received personalised diet plans tailored to their age, weight, gestational age, activity level, and other factors(Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jorgensen36,Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Atkinson, Maran, Dempsey, Perreault, Vanniyasingam and Phillips91,Reference Opie, Neff and Tierney93–Reference Li, Wang, Wang, Zhang and Sun96,Reference Tajirika-Shirai, Takimoto, Yokoyama, Kaneko, Kubota and Miyasaka98,Reference Hui, Back, Ludwig, Gardiner, Sevenhuysen and Dean100–Reference Mottola, Giroux, Gratton, Hammond, Hanley and Harris107,Reference Haby, Berg, Gyllensten, Hanas and Premberg115,Reference Hui, Back, Ludwig, Gardiner, Sevenhuysen and Dean120,Reference Barquiel, Calvo, Moreno-Domínguez, Martínez-Sánchez, Muner and Bedate122,Reference Rauh, Gabriel, Kerschbaum, Schuster, von Kries and Amann-Gassner124,Reference Vesco, Karanja, King, Gillman, Leo and Perrin133) . The number of educational sessions in nearly half of the studies (n = 33, 45%) was three or more(Reference Vinter, Jensen, Ovesen, Beck-Nielsen and Jorgensen36,Reference O’Brien, Alberdi, Geraghty and McAuliffe40,Reference Okesene-Gafa, Li, McKinlay, Taylor, Rush and Wall50,Reference Liu, Wilcox, Wingard, Turner-McGrievy, Hutto and Burgis68,Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Abdel-Aziz, Hegazy, Mohamed, Kasem and Hagag73,Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Jahan, Roy, Mihrshahi, Sultana, Khatoon and Roy85,Reference Watt, Appel, Lopez, Flores and Lawhon87,Reference Atkinson, Maran, Dempsey, Perreault, Vanniyasingam and Phillips91–Reference Opie, Neff and Tierney93,Reference Hajian, Aslani, Sarbakhsh and Fathnezhad-Kazemi95,Reference Asbee, Jenkins, Butler, White, Elliot and Rutledge99,Reference Peccei, Blake-Lamb, Rahilly, Hatoum and Bryant102,Reference Buckingham-Schutt, Ellingson, Vazou and Campbell103,Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105,Reference Dodd, Kannieappan, Grivell, Deussen, Moran and Yelland109–Reference McGiveron, Foster, Pearce, Taylor, McMullen and Langley-Evans111,Reference Krebs, Lorenz, Nawabi, Alayli and Stock113,Reference Althuizen, Van Der Wijden, Van Mechelen, Seidell and Van Poppel116–Reference Huang, Yeh and Tsai119,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Razzazi, Griffiths and Alimoradi127,Reference Long, Martin and Janson-Sand128,Reference Shirazian, Faris, Fox, Friedman and Rebarber130,Reference Lindholm, Norman, Kilander and Altman132–Reference Haby, Glantz, Hanas and Premberg135) . Four studies included a mobile phone app(Reference Sandborg, Söderström, Henriksson, Bendtsen, Henström and Leppänen58–Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61) and three directed participants to a study website(Reference Olson, Groth, Graham, Reschke, Strawderman and Fernandez63,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Wilkinson, Fjeldsoe and Willcox66) . Six studies used text messaging to maintain contact with the sample(Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Wilkinson, Fjeldsoe and Willcox66,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Soltani, Duxbury, Arden, Dearden, Furness and Garland114,Reference Yang, Zhao, Tu, Chang and Xiao125) and 15 studies employed a form of telehealth or phone counselling(Reference Sagedal, Øverby, Bere, Torstveit, Lohne-Seiler and Småstuen67–Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Liu, Liu, Hua and Chen72–Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Bosaeus, Hussain, Karlsson, Andersson, Hulthén and Svelander78,Reference Phelan, Phipps, Abrams, Darroch, Schaffner and Wing79,Reference Ferrara, Hedderson, Brown, Ehrlich, Tsai and Feng92,Reference Opie, Neff and Tierney93,Reference Peccei, Blake-Lamb, Rahilly, Hatoum and Bryant102,Reference Dodd, Kannieappan, Grivell, Deussen, Moran and Yelland109,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Shirazian, Faris, Fox, Friedman and Rebarber130) . Nineteen studies provided women with a hard copy of information(Reference O’Brien, Alberdi, Geraghty and McAuliffe40,Reference Okesene-Gafa, Li, McKinlay, Taylor, Rush and Wall50,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Robertson and Ladlow57,Reference Liu, Liu, Hua and Chen72,Reference Khoigani, Nadjarzadeh, Mardanian, Riahi, Ardian and Salehi74,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Jahan, Roy, Mihrshahi, Sultana, Khatoon and Roy85,Reference Opie, Neff and Tierney93,Reference Hajian, Aslani, Sarbakhsh and Fathnezhad-Kazemi95,Reference Tajirika-Shirai, Takimoto, Yokoyama, Kaneko, Kubota and Miyasaka98,Reference Sartorelli, Crivellenti, Baroni, de Andrade Miranda, da Silva Santos and Carvalho110,Reference McGiveron, Foster, Pearce, Taylor, McMullen and Langley-Evans111,Reference Althuizen, Van Der Wijden, Van Mechelen, Seidell and Van Poppel116,Reference Dirige, McNutt, Hamatake, McGee and Manayan117,Reference Huang, Yeh and Tsai119,Reference Das Gecim and Ozturk123,Reference Razzazi, Griffiths and Alimoradi127,Reference Shirazian, Faris, Fox, Friedman and Rebarber130) . In most studies (n = 51, 69%), women in the intervention group had significantly lower total GWG and a lower rate of extreme or insufficient weight gain based on BMI compared to those in the control group, while in remaining studies (n = 19, 25.5%), there were no significant differences(Reference Okesene-Gafa, Li, McKinlay, Taylor, Rush and Wall50,Reference Sandborg, Söderström, Henriksson, Bendtsen, Henström and Leppänen58,Reference Li, Aris, Han and Tan59,Reference Olson, Groth, Graham, Reschke, Strawderman and Fernandez63,Reference Liu, Wilcox, Wingard, Turner-McGrievy, Hutto and Burgis68,Reference Bosaeus, Hussain, Karlsson, Andersson, Hulthén and Svelander78,Reference Watt, Appel, Lopez, Flores and Lawhon87,Reference Atkinson, Maran, Dempsey, Perreault, Vanniyasingam and Phillips91,Reference Hui, Ludwig, Gardiner, Sevenhuysen, Murray and Morris94,Reference Peccei, Blake-Lamb, Rahilly, Hatoum and Bryant102,Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105,Reference Nagpal, Prapavessis, Campbell, de Vrijer, Bgeginski and Hosein108,Reference Dodd, Kannieappan, Grivell, Deussen, Moran and Yelland109,Reference Althuizen, Van Der Wijden, Van Mechelen, Seidell and Van Poppel116–Reference Kinnunen, Raitanen, Aittasalo and Luoto118,Reference Adam, Jarman, Barker, Manca, Lawrence and Bell121,Reference Das Gecim and Ozturk123,Reference Razzazi, Griffiths and Alimoradi127) .
Prevention of gestational diabetes mellitus
Thirty-two studies (19%) described an education programme or intervention that sought to prevent GDM(Reference Poston, Bell, Croker, Flynn, Godfrey and Goff28,Reference Peacock, Seed, Dalrymple, White, Poston and Flynn29,Reference Huvinen, Koivusalo, Meinilä, Valkama, Tiitinen and Rönö32,Reference Koivusalo, Rönö, Klemetti, Roine, Lindström and Erkkola33,Reference McGowan, Walsh, Byrne, Curran and McAuliffe39,Reference Ding, Gou, Guan, Wang, Bi and Hong53–Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Hao, Yang, Wang, Lan, Xu and Wang62,Reference Sagedal, Øverby, Bere, Torstveit, Lohne-Seiler and Småstuen67,Reference Mohsenzadeh-Ledari, Taghizadeh, Keramat, Moosazadeh, Yazdani and Najafi71,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Gray-Donald, Robinson, Collier, David, Renaud and Rodrigues89,Reference Opie, Neff and Tierney93–Reference Li, Wang, Wang, Zhang and Sun96,Reference Liu, Zhang, Zheng, Liang, Zhang and Tian104,Reference Garmendia, Corvalan, Araya, Casanello, Kusanovic and Uauy112,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Razzazi, Griffiths and Alimoradi127,Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131,Reference Gopalan, Haque, Ahmad, Gaur and Misra136,Reference Luoto, Kinnunen, Aittasalo, Kolu, Raitanen and Ojala140–Reference Sadiya, Jakapure, Shaar, Adnan and Tesfa149) . Nine studies (27%) included participants who had one or two risk factors for GDM, including history of previous GDM(Reference Huvinen, Koivusalo, Meinilä, Valkama, Tiitinen and Rönö32,Reference Koivusalo, Rönö, Klemetti, Roine, Lindström and Erkkola33,Reference Xu, Lin, Fang, Cui, Li and Yu54,Reference Lin, Yang, Zhang and Wei55,Reference Luoto, Kinnunen, Aittasalo, Kolu, Raitanen and Ojala140,Reference Korpi-Hyövälti, Schwab, Laaksonen, Linjama, Heinonen and Niskanen143,Reference Chan, Tam, Ho, Kwan, Li and Sea144,Reference Deng, Hou, Wu, Liu, Ma and Yao147,Reference Sadiya, Jakapure, Shaar, Adnan and Tesfa149) . One-third of the studies (n = 11, 34%) included participants who were living with overweight or obesity(Reference Poston, Bell, Croker, Flynn, Godfrey and Goff28,Reference Peacock, Seed, Dalrymple, White, Poston and Flynn29,Reference Huvinen, Koivusalo, Meinilä, Valkama, Tiitinen and Rönö32,Reference Koivusalo, Rönö, Klemetti, Roine, Lindström and Erkkola33,Reference Ding, Gou, Guan, Wang, Bi and Hong53,Reference Opie, Neff and Tierney93,Reference Hajian, Aslani, Sarbakhsh and Fathnezhad-Kazemi95,Reference Liu, Zhang, Zheng, Liang, Zhang and Tian104,Reference Sun and Zhao141,Reference Korpi-Hyövälti, Schwab, Laaksonen, Linjama, Heinonen and Niskanen143,Reference Zhang, Wang, Yang, Niu, Li and Wang145) , while three studies included participants who were in the ‘healthy weight’ category of BMI(Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Karimipour, Sharifi, Seydkhani, Sayadi and Jalilian146) . Three studies did not report the mean age of their sample(Reference Gopalan, Haque, Ahmad, Gaur and Misra136,Reference Charkamyani, Khedmat and Hosseinkhani142,Reference Korpi-Hyövälti, Schwab, Laaksonen, Linjama, Heinonen and Niskanen143) ; the remainder of the studies were conducted with women aged between 24.3(Reference Gray-Donald, Robinson, Collier, David, Renaud and Rodrigues89) and 37.5 years(Reference Li, Wang, Wang, Zhang and Sun96) (average 30.5, SD 3.05). Half of studies (n = 16, 50%) included nutrition education programmes which were conducted in the first trimester of pregnancy (under 14 weeks of gestation) (Reference McGowan, Walsh, Byrne, Curran and McAuliffe39,Reference Ding, Gou, Guan, Wang, Bi and Hong53,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Mohsenzadeh-Ledari, Taghizadeh, Keramat, Moosazadeh, Yazdani and Najafi71,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Liu, Zhang, Zheng, Liang, Zhang and Tian104,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Gopalan, Haque, Ahmad, Gaur and Misra136,Reference Luoto, Kinnunen, Aittasalo, Kolu, Raitanen and Ojala140,Reference Sun and Zhao141,Reference Korpi-Hyövälti, Schwab, Laaksonen, Linjama, Heinonen and Niskanen143,Reference Chan, Tam, Ho, Kwan, Li and Sea144,Reference Karimipour, Sharifi, Seydkhani, Sayadi and Jalilian146–Reference Sadiya, Jakapure, Shaar, Adnan and Tesfa149) , and three studies did not specify the pregnancy gestation of participants at the start of the programme or intervention(Reference Lin, Yang, Zhang and Wei55,Reference Hao, Yang, Wang, Lan, Xu and Wang62,Reference Li, Wang, Wang, Zhang and Sun96) .
Most studies were RCTs (n = 24, 75%)(Reference Poston, Bell, Croker, Flynn, Godfrey and Goff28,Reference Peacock, Seed, Dalrymple, White, Poston and Flynn29,Reference Koivusalo, Rönö, Klemetti, Roine, Lindström and Erkkola33,Reference McGowan, Walsh, Byrne, Curran and McAuliffe39,Reference Ding, Gou, Guan, Wang, Bi and Hong53–Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Sagedal, Øverby, Bere, Torstveit, Lohne-Seiler and Småstuen67,Reference Mohsenzadeh-Ledari, Taghizadeh, Keramat, Moosazadeh, Yazdani and Najafi71,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Hui, Ludwig, Gardiner, Sevenhuysen, Murray and Morris94–Reference Li, Wang, Wang, Zhang and Sun96,Reference Liu, Zhang, Zheng, Liang, Zhang and Tian104,Reference Garmendia, Corvalan, Araya, Casanello, Kusanovic and Uauy112,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Razzazi, Griffiths and Alimoradi127,Reference Luoto, Kinnunen, Aittasalo, Kolu, Raitanen and Ojala140,Reference Korpi-Hyövälti, Schwab, Laaksonen, Linjama, Heinonen and Niskanen143–Reference Sadiya, Jakapure, Shaar, Adnan and Tesfa149) , with a smaller number being quasi-experimental (n = 5, 14%)(Reference Huvinen, Koivusalo, Meinilä, Valkama, Tiitinen and Rönö32,Reference Gray-Donald, Robinson, Collier, David, Renaud and Rodrigues89,Reference Opie, Neff and Tierney93,Reference Sun and Zhao141,Reference Charkamyani, Khedmat and Hosseinkhani142) , cohort (n = 3, 8.5%)(Reference Hao, Yang, Wang, Lan, Xu and Wang62,Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131) , or cross-sectional (n = 1, 3%)(Reference Gopalan, Haque, Ahmad, Gaur and Misra136). Population sizes of studies that focused on GDM ranged from 2,925(Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131) to 24(Reference Hui, Ludwig, Gardiner, Sevenhuysen, Murray and Morris94), with an average sample size of 405 (SD 710). Only four studies addressing GDM reported using a theoretical framework: one study employed the Health Belief Model(Reference Jing, Huang, Liu, Luo, Yang and Liao76), one employed the Control Theory with elements of Social Cognitive Theory(Reference Poston, Bell, Croker, Flynn, Godfrey and Goff28), one employed the Social Learning Theory(Reference Gray-Donald, Robinson, Collier, David, Renaud and Rodrigues89), and one employed the Health Action Process Approach(Reference Razzazi, Griffiths and Alimoradi127).
Most studies (n = 23, 70%) employed individual counselling activities as the main nutritional education intervention, while seven (21%) studies provided group education sessions (see Table 2). Participants in only nine studies received personalised diet plans tailored to their age, weight, gestational week, activity level, and other factors(Reference Opie, Neff and Tierney93–Reference Li, Wang, Wang, Zhang and Sun96,Reference Liu, Zhang, Zheng, Liang, Zhang and Tian104,Reference Sun and Zhao141,Reference Chan, Tam, Ho, Kwan, Li and Sea144,Reference Zhang, Wang, Yang, Niu, Li and Wang145,Reference Deng, Hou, Wu, Liu, Ma and Yao147) . More than half of the studies (n = 18, 55%) had three or more educational sessions(Reference Poston, Bell, Croker, Flynn, Godfrey and Goff28,Reference Huvinen, Koivusalo, Meinilä, Valkama, Tiitinen and Rönö32,Reference Koivusalo, Rönö, Klemetti, Roine, Lindström and Erkkola33,Reference Opie, Neff and Tierney93,Reference Hajian, Aslani, Sarbakhsh and Fathnezhad-Kazemi95,Reference Liu, Zhang, Zheng, Liang, Zhang and Tian104,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Razzazi, Griffiths and Alimoradi127,Reference Luoto, Kinnunen, Aittasalo, Kolu, Raitanen and Ojala140–Reference Sadiya, Jakapure, Shaar, Adnan and Tesfa149) . One study included a mobile smartphone application(Reference Hao, Yang, Wang, Lan, Xu and Wang62), seven used text messaging to maintain contact with the sample(Reference Ding, Gou, Guan, Wang, Bi and Hong53,Reference Lin, Yang, Zhang and Wei55,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Sun and Zhao141,Reference Deng, Hou, Wu, Liu, Ma and Yao147) , and ten used phone calls for follow-up or counselling(Reference Poston, Bell, Croker, Flynn, Godfrey and Goff28,Reference Sagedal, Øverby, Bere, Torstveit, Lohne-Seiler and Småstuen67,Reference Mohsenzadeh-Ledari, Taghizadeh, Keramat, Moosazadeh, Yazdani and Najafi71,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Opie, Neff and Tierney93,Reference Yang, Zhao, Tu, Chang and Xiao125,Reference Sun and Zhao141,Reference Chan, Tam, Ho, Kwan, Li and Sea144,Reference Karimipour, Sharifi, Seydkhani, Sayadi and Jalilian146,Reference Sadiya, Jakapure, Shaar, Adnan and Tesfa149) . Eleven studies reported providing participants with printed material(Reference Poston, Bell, Croker, Flynn, Godfrey and Goff28,Reference McGowan, Walsh, Byrne, Curran and McAuliffe39,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Mohsenzadeh-Ledari, Taghizadeh, Keramat, Moosazadeh, Yazdani and Najafi71,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Gray-Donald, Robinson, Collier, David, Renaud and Rodrigues89,Reference Opie, Neff and Tierney93,Reference Hajian, Aslani, Sarbakhsh and Fathnezhad-Kazemi95,Reference Razzazi, Griffiths and Alimoradi127,Reference Deng, Hou, Wu, Liu, Ma and Yao147,Reference Goodarzi-Khoigani, Mahmoodabad, Moghadam, Nadjarzadeh, Mardanian and Fallahzadeh148) . Of the 33 studies, only 14(Reference Koivusalo, Rönö, Klemetti, Roine, Lindström and Erkkola33,Reference Ding, Gou, Guan, Wang, Bi and Hong53,Reference Lin, Yang, Zhang and Wei55,Reference Mohsenzadeh-Ledari, Taghizadeh, Keramat, Moosazadeh, Yazdani and Najafi71,Reference Li, Wang, Wang, Zhang and Sun96,Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131,Reference Sun and Zhao141,Reference Zhang, Wang, Yang, Niu, Li and Wang145–Reference Deng, Hou, Wu, Liu, Ma and Yao147,Reference Allehdan, Basha, Hyassat, Nabhan, Qasrawi and Tayyem150–Reference Zhou, Wang, Chen, Liu and Wu153) reported a statistically significant result, with the programme or intervention demonstrating decreased incidence of GDM.
Mid-upper arm circumference (nutritional status)
Five studies measured mid-upper arm circumference (MUAC) to estimate the nutritional status of the women(Reference Tesfaye, Tamiru and Belachew44,Reference Beressa, Whiting and Belachew45,Reference Tsegaye, Tamiru and Belachew51,Reference Habtu, Agena, Umugwaneza, Mochama and Munyanshongore154,Reference Sisay and Tesfaye155) . Three studies were RCTs(Reference Tesfaye, Tamiru and Belachew44,Reference Beressa, Whiting and Belachew45,Reference Sisay and Tesfaye155) , and two were quasi-experimental studies(Reference Tsegaye, Tamiru and Belachew51,Reference Habtu, Agena, Umugwaneza, Mochama and Munyanshongore154) ; all were conducted after 2021. Four of the five studies were conducted in Ethiopia(Reference Tesfaye, Tamiru and Belachew44,Reference Beressa, Whiting and Belachew45,Reference Tsegaye, Tamiru and Belachew51,Reference Sisay and Tesfaye155) . Three of the five studies reported the use of the Health Belief Model and the Theory of Planned Behaviour(Reference Tesfaye, Tamiru and Belachew44,Reference Beressa, Whiting and Belachew45,Reference Tsegaye, Tamiru and Belachew51) .
Four studies used individual counselling as the main form of nutritional education intervention(Reference Tesfaye, Tamiru and Belachew44,Reference Beressa, Whiting and Belachew45,Reference Habtu, Agena, Umugwaneza, Mochama and Munyanshongore154,Reference Sisay and Tesfaye155) , while three involved home visits by a health professional(Reference Tesfaye, Tamiru and Belachew44,Reference Beressa, Whiting and Belachew45,Reference Tsegaye, Tamiru and Belachew51) . In most studies (n = 4, 80%), the number of sessions was more than three(Reference Tesfaye, Tamiru and Belachew44,Reference Beressa, Whiting and Belachew45,Reference Tsegaye, Tamiru and Belachew51,Reference Sisay and Tesfaye155) . All studies reported statistically significant improvements in average MUAC among the intervention group, with the proportion of MAUC < 23 cm (undernutrition status) significantly higher in the control group compared to the intervention group.
Iron deficiency anaemia prevention
Only five studies (3%) described an education programme or intervention that sought to prevent maternal anaemia(Reference Ilboudo, Savadogo, Traoré, Meda, Kinda and Sombié52,Reference Razzazi, Griffiths and Alimoradi127,Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131,Reference Wakwoya, Belachew and Girma156,Reference Kuma, Tamiru and Belachew157) . Most studies (n = 3, 60%) conducted nutrition education before 16 weeks gestation(Reference Razzazi, Griffiths and Alimoradi127,Reference Wakwoya, Belachew and Girma156,Reference Kuma, Tamiru and Belachew157) . Four studies were RCTs(Reference Ilboudo, Savadogo, Traoré, Meda, Kinda and Sombié52,Reference Razzazi, Griffiths and Alimoradi127,Reference Wakwoya, Belachew and Girma156,Reference Kuma, Tamiru and Belachew157) and one was a cohort study(Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131); all were conducted after 2020. Two of the five studies reported the use of the Health Belief Model(Reference Tesfaye, Tamiru and Belachew44) and the Health Action Process Approach(Reference Razzazi, Griffiths and Alimoradi127). Two studies used individual counselling as the main form of nutritional education intervention(Reference Ilboudo, Savadogo, Traoré, Meda, Kinda and Sombié52,Reference Wakwoya, Belachew and Girma156) , while one involved home visits by a health professional(Reference Ilboudo, Savadogo, Traoré, Meda, Kinda and Sombié52). In one study, the number of education sessions was fewer than three(Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131). Of the five studies, four reported statistically significant improvements in haemoglobin levels or reductions in the prevalence of anaemia(Reference Ilboudo, Savadogo, Traoré, Meda, Kinda and Sombié52,Reference Carbonneau, Dumas, Brodeur-Doucet and Fontaine-Bisson131,Reference Wakwoya, Belachew and Girma156,Reference Kuma, Tamiru and Belachew157) .
Dietary outcomes
Fifty-two (31%) studies reported maternal dietary outcomes(Reference Poston, Briley, Barr, Bell, Croker and Coxon27,Reference Peacock, Seed, Dalrymple, White, Poston and Flynn29–Reference Flynn, Seed, Patel, Barr, Bell and Briley31,Reference Valkama, Koivusalo, Lindström, Meinilä, Kautiainen and Stach-Lempinen34,Reference McGowan, Walsh, Byrne, Curran and McAuliffe39–Reference Demilew, Alene and Belachew43,Reference Kieffer, Welmerink, Sinco, Welch, Rees Clayton and Schumann46,Reference Mendelson, Dollard, Hall, Zarrabi and Desjardin49,Reference Tsegaye, Tamiru and Belachew51,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Li, Aris, Han and Tan59,Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64–Reference Wilkinson, Fjeldsoe and Willcox66,Reference Hillesund, Bere, Sagedal, Vistad and Øverby70,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Katenga-Kaunda, Iversen, Holmboe-Ottesen, Fjeld, Mdala and Kamudoni86,Reference Sharma, Chuang, Byrd-Williams, Danho, Upadhyaya and Berens88,Reference Opie, Neff and Tierney93,Reference Nagpal, Prapavessis, Campbell, de Vrijer, Bgeginski and Hosein108,Reference Adam, Jarman, Barker, Manca, Lawrence and Bell121,Reference Rajbir, Sukhvinder and Sangha134,Reference Guelinckx, Devlieger, Mullie and Vansant137,Reference Halisah, Nur, Taslim, Chalid, Juliaty and Mappaware138,Reference Charkamyani, Khedmat and Hosseinkhani142,Reference Nguyen, Kim, Sanghvi, Mahmud, Tran and Shabnam158–Reference Fujimoto, Iida, Takeuchi, Shinohara, Kubota and Nakamura178) . The dietary outcomes in these studies included measures of dietary intake, specifically macronutrients, micronutrients, and energy intake (n = 33, 65%); consumption of various food groups (n = 15, 27%); dietary quality (n = 12, 34%); dietary diversity (n = 5, 9%); and/or adherence to recommendations based on different nutritional guidelines for pregnant mothers (n = 8, 15%). Almost one-third of the studies (n = 16, 32%) included participants who were classified as overweight or obese(Reference Poston, Briley, Barr, Bell, Croker and Coxon27,Reference Peacock, Seed, Dalrymple, White, Poston and Flynn29–Reference Flynn, Seed, Patel, Barr, Bell and Briley31,Reference Valkama, Koivusalo, Lindström, Meinilä, Kautiainen and Stach-Lempinen34,Reference Li, Aris, Han and Tan59,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Wilkinson, Fjeldsoe and Willcox66,Reference Opie, Neff and Tierney93,Reference Guelinckx, Devlieger, Mullie and Vansant137,Reference Moran, Flynn, Louise, Deussen and Dodd162,Reference Vander Wyst, Vercelli, O’Brien, Cooper, Pressman and Whisner165,Reference Kinnunen, Puhkala, Raitanen, Ahonen, Aittasalo and Virtanen169,Reference Eslami, Mohammad Alizadeh Charandabi, Farshbaf Khalili, Asghari Jafarabadi and Mirghafourvand173,Reference Hawkins, Hosker, Marcus, Rosal, Braun and Stanek III174,Reference Ainscough, O’Brien, Lindsay, Kennelly, O’Sullivan and O’Brien176) , while 12 studies included participants across the full spectrum of BMI, from underweight to obese(Reference Kieffer, Welmerink, Sinco, Welch, Rees Clayton and Schumann46,Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Sharma, Chuang, Byrd-Williams, Danho, Upadhyaya and Berens88,Reference Adam, Jarman, Barker, Manca, Lawrence and Bell121,Reference Rajbir, Sukhvinder and Sangha134,Reference Perreault, Mottola and Atkinson160,Reference Piirainen, Isolauri, Lagström and Laitinen163,Reference Malta, Gomes, Barros, Baraldi, Takito and Benício167,Reference Goodarzi-Khoigani, Moghadam, Nadjarzadeh, Mardanian, Fallahzadeh and Mazloomy-Mahmoodabad171,Reference Seo, Jeong, Koo, Yang and Park172,Reference Wilkinson and McIntyre177) . In 15 studies (29%) entry into the programme or intervention was in the first trimester (less than 14 weeks of gestation) (Reference McGowan, Walsh, Byrne, Curran and McAuliffe39,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Gootjes, Van Dijk, Koster, Willemsen, Steegers and Steegers-Theunissen65,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Guelinckx, Devlieger, Mullie and Vansant137,Reference Nguyen, Kim, Sanghvi, Mahmud, Tran and Shabnam158,Reference Günther, Hoffmann, Kunath, Spies, Meyer and Stecher161,Reference Piirainen, Isolauri, Lagström and Laitinen163,Reference Elmasri and Yonus166,Reference Malta, Gomes, Barros, Baraldi, Takito and Benício167,Reference Kinnunen, Puhkala, Raitanen, Ahonen, Aittasalo and Virtanen169–Reference Goodarzi-Khoigani, Moghadam, Nadjarzadeh, Mardanian, Fallahzadeh and Mazloomy-Mahmoodabad171,Reference Wilkinson and McIntyre177) , and nine studies did not report the pregnancy gestation of participants at the start of the programme or intervention(Reference Demilew, Alene and Belachew43,Reference Kieffer, Welmerink, Sinco, Welch, Rees Clayton and Schumann46,Reference Mendelson, Dollard, Hall, Zarrabi and Desjardin49,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Katenga-Kaunda, Iversen, Holmboe-Ottesen, Fjeld, Mdala and Kamudoni86,Reference Halisah, Nur, Taslim, Chalid, Juliaty and Mappaware138,Reference Frongillo, Nguyen, Sanghvi, Mahmud, Aktar and Alayon159) .
Most studies were RCTs (n = 36, 67%)(Reference Poston, Briley, Barr, Bell, Croker and Coxon27,Reference Peacock, Seed, Dalrymple, White, Poston and Flynn29–Reference Flynn, Seed, Patel, Barr, Bell and Briley31,Reference Valkama, Koivusalo, Lindström, Meinilä, Kautiainen and Stach-Lempinen34,Reference McGowan, Walsh, Byrne, Curran and McAuliffe39–Reference Demilew, Alene and Belachew43,Reference Kieffer, Welmerink, Sinco, Welch, Rees Clayton and Schumann46,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Li, Aris, Han and Tan59,Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Hillesund, Bere, Sagedal, Vistad and Øverby70,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Katenga-Kaunda, Iversen, Holmboe-Ottesen, Fjeld, Mdala and Kamudoni86,Reference Nagpal, Prapavessis, Campbell, de Vrijer, Bgeginski and Hosein108,Reference Adam, Jarman, Barker, Manca, Lawrence and Bell121,Reference Guelinckx, Devlieger, Mullie and Vansant137,Reference Nguyen, Kim, Sanghvi, Mahmud, Tran and Shabnam158–Reference Moran, Flynn, Louise, Deussen and Dodd162,Reference Hunt, Jacob, Ostergard, Masri, Clark and Coulson168–Reference Hawkins, Hosker, Marcus, Rosal, Braun and Stanek III174,Reference Ainscough, O’Brien, Lindsay, Kennelly, O’Sullivan and O’Brien176–Reference Fujimoto, Iida, Takeuchi, Shinohara, Kubota and Nakamura178) , with a smaller number of quasi-experimental studies (n = 13, 24%)(Reference Tsegaye, Tamiru and Belachew51,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Sharma, Chuang, Byrd-Williams, Danho, Upadhyaya and Berens88,Reference Opie, Neff and Tierney93,Reference Rajbir, Sukhvinder and Sangha134,Reference Halisah, Nur, Taslim, Chalid, Juliaty and Mappaware138,Reference Charkamyani, Khedmat and Hosseinkhani142,Reference Kaleem, Adnan, Nasir and Rahat164–Reference Malta, Gomes, Barros, Baraldi, Takito and Benício167) and cohort studies (n = 5, 9%)(Reference Mendelson, Dollard, Hall, Zarrabi and Desjardin49,Reference Gootjes, Van Dijk, Koster, Willemsen, Steegers and Steegers-Theunissen65,Reference Wilkinson, Fjeldsoe and Willcox66,Reference Piirainen, Isolauri, Lagström and Laitinen163,Reference Odiwuor, Kimiywe and Waudo175) . Population sizes of studies exploring dietary outcomes ranged from 2,554(Reference Gootjes, Van Dijk, Koster, Willemsen, Steegers and Steegers-Theunissen65) to 12(Reference Li, Aris, Han and Tan59), with an average sample size of 267 (SD 417). Fifteen of the 52 studies reported the use of a theoretical framework to support the design of the intervention or programme. Four studies employed the Social Cognitive Theory(Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Sharma, Chuang, Byrd-Williams, Danho, Upadhyaya and Berens88,Reference Vander Wyst, Vercelli, O’Brien, Cooper, Pressman and Whisner165,Reference Hawkins, Hosker, Marcus, Rosal, Braun and Stanek III174) , with two additional studies employing the Social Cognitive Theory and the Control Theory(Reference Poston, Briley, Barr, Bell, Croker and Coxon27,Reference Ainscough, O’Brien, Lindsay, Kennelly, O’Sullivan and O’Brien176) . One study employed the Health Belief Model(Reference Jing, Huang, Liu, Luo, Yang and Liao76) and two employed the Theory of Planned Behaviour(Reference Tsegaye, Tamiru and Belachew51,Reference Katenga-Kaunda, Iversen, Holmboe-Ottesen, Fjeld, Mdala and Kamudoni86) , while two studies employed the Health Belief Model in addition to the Theory of Planned Behaviour(Reference Demilew, Alene and Belachew43,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81) . Other studies employed the Transtheoretical Model of Behavioural Change(Reference Gootjes, Van Dijk, Koster, Willemsen, Steegers and Steegers-Theunissen65,Reference Hawkins, Hosker, Marcus, Rosal, Braun and Stanek III174) , the Ecological Model(Reference Malta, Gomes, Barros, Baraldi, Takito and Benício167), and Pender’s Health Promotion Model(Reference Goodarzi-Khoigani, Moghadam, Nadjarzadeh, Mardanian, Fallahzadeh and Mazloomy-Mahmoodabad171).
Twenty-two (41%) studies employed individual counselling activities as the main nutritional education intervention, while seven (13%) studies provided group education sessions (see Table 2). Only five studies provided personalised diet plans that were tailored to factors such as age, weight, gestational age, and physical activity level(Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Opie, Neff and Tierney93,Reference Perreault, Mottola and Atkinson160,Reference Piirainen, Isolauri, Lagström and Laitinen163,Reference Goodarzi-Khoigani, Moghadam, Nadjarzadeh, Mardanian, Fallahzadeh and Mazloomy-Mahmoodabad171) . Half of the studies (n = 26, 50%) included three or more educational sessions(Reference Poston, Briley, Barr, Bell, Croker and Coxon27,Reference Flynn, Seed, Patel, Barr, Bell and Briley31,Reference O’Brien, Alberdi, Geraghty and McAuliffe40–Reference Demilew, Alene and Belachew43,Reference Kieffer, Welmerink, Sinco, Welch, Rees Clayton and Schumann46,Reference Hillesund, Bere, Sagedal, Vistad and Øverby70,Reference Katenga-Kaunda, Iversen, Holmboe-Ottesen, Fjeld, Mdala and Kamudoni86,Reference Sharma, Chuang, Byrd-Williams, Danho, Upadhyaya and Berens88,Reference Opie, Neff and Tierney93,Reference Asbee, Jenkins, Butler, White, Elliot and Rutledge99,Reference Rajbir, Sukhvinder and Sangha134,Reference Charkamyani, Khedmat and Hosseinkhani142,Reference Nguyen, Kim, Sanghvi, Mahmud, Tran and Shabnam158,Reference Perreault, Mottola and Atkinson160–Reference Piirainen, Isolauri, Lagström and Laitinen163,Reference Elmasri and Yonus166,Reference Hunt, Jacob, Ostergard, Masri, Clark and Coulson168–Reference Seo, Jeong, Koo, Yang and Park172,Reference Hawkins, Hosker, Marcus, Rosal, Braun and Stanek III174) . Two studies included a smartphone application(Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Ainscough, O’Brien, Lindsay, Kennelly, O’Sullivan and O’Brien176) and four interventions directed participants to a study website(Reference Li, Aris, Han and Tan59,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64–Reference Wilkinson, Fjeldsoe and Willcox66) . Six studies employed text messaging to maintain contact with participants(Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Wilkinson, Fjeldsoe and Willcox66,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Vander Wyst, Vercelli, O’Brien, Cooper, Pressman and Whisner165,Reference Eslami, Mohammad Alizadeh Charandabi, Farshbaf Khalili, Asghari Jafarabadi and Mirghafourvand173) , while another six used phone calls for follow-up or counselling(Reference Hillesund, Bere, Sagedal, Vistad and Øverby70,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Opie, Neff and Tierney93,Reference Moran, Flynn, Louise, Deussen and Dodd162,Reference Seo, Jeong, Koo, Yang and Park172,Reference Hawkins, Hosker, Marcus, Rosal, Braun and Stanek III174) . Most studies (n = 47, 90%) reported a statistically significant result, indicating that the programme or intervention improved dietary outcomes(Reference Poston, Briley, Barr, Bell, Croker and Coxon27,Reference Peacock, Seed, Dalrymple, White, Poston and Flynn29–Reference Flynn, Seed, Patel, Barr, Bell and Briley31,Reference Valkama, Koivusalo, Lindström, Meinilä, Kautiainen and Stach-Lempinen34,Reference McGowan, Walsh, Byrne, Curran and McAuliffe39–Reference Demilew, Alene and Belachew43,Reference Kieffer, Welmerink, Sinco, Welch, Rees Clayton and Schumann46,Reference Mendelson, Dollard, Hall, Zarrabi and Desjardin49,Reference Tsegaye, Tamiru and Belachew51,Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Henriksson, Migueles, Söderström, Sandborg, Maddison and Löf61,Reference Gootjes, Van Dijk, Koster, Willemsen, Steegers and Steegers-Theunissen65,Reference Wilkinson, Fjeldsoe and Willcox66,Reference Hillesund, Bere, Sagedal, Vistad and Øverby70,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Katenga-Kaunda, Iversen, Holmboe-Ottesen, Fjeld, Mdala and Kamudoni86,Reference Sharma, Chuang, Byrd-Williams, Danho, Upadhyaya and Berens88,Reference Opie, Neff and Tierney93,Reference Rajbir, Sukhvinder and Sangha134,Reference Guelinckx, Devlieger, Mullie and Vansant137,Reference Halisah, Nur, Taslim, Chalid, Juliaty and Mappaware138,Reference Charkamyani, Khedmat and Hosseinkhani142,Reference Nguyen, Kim, Sanghvi, Mahmud, Tran and Shabnam158–Reference Wilkinson and McIntyre177) .
Nutritional knowledge, attitudes and/or behaviours
Twenty-seven (16%) studies reported on a programme or intervention that sought to improve nutritional knowledge, attitudes, and/or behaviours(Reference Katenga-Kaunda, Kamudoni, Holmboe-Ottesen, Fjeld, Mdala and Shi47,Reference Akeredolu, Osisanya, Okafor and Seriki-Mosadolorun48,Reference Soliman, Hassan, Fahmy, Abdelsalam and Salem75,Reference Amiri, Hamzavi Zarghani, Nazeri, Ghofranipour, Karimi and Amouzegar77,Reference Peiris, Wijesinghe, Gunawardana, Weerasinghe, Rajapaksha and Rathnayake80,Reference Muhamad, Mahmudiono, Abihail, Sahila, Wangi and Suyanto82,Reference Girard, Grant, Watkinson, Okuku, Wanjala and Cole83,Reference Subapriya and Chandrasekhar90,Reference Dirige, McNutt, Hamatake, McGee and Manayan117,Reference Long, Martin and Janson-Sand128,Reference Anderson, Campbell and Shepherd179–Reference Jahangiri, Shamsi, Khorsandi and Moradzade196) . Eight studies examined all three components: knowledge, attitude, and practice(Reference Soliman, Hassan, Fahmy, Abdelsalam and Salem75,Reference Amiri, Hamzavi Zarghani, Nazeri, Ghofranipour, Karimi and Amouzegar77,Reference Peiris, Wijesinghe, Gunawardana, Weerasinghe, Rajapaksha and Rathnayake80,Reference Anderson, Campbell and Shepherd179,Reference Rifayanto, Khomsan, Sinaga, Dewi and Ekawidyani189,Reference Permatasari, Rizqiya, Kusumaningati, Suryaalamsah and Hermiwahyoeni190,Reference Khani Jeihooni, Rakhshani, Harsini and Layeghiasl195,Reference Jahangiri, Shamsi, Khorsandi and Moradzade196) . One study evaluated nutritional knowledge along with nutritional attitudes(Reference Subapriya and Chandrasekhar90), while 12 studies assessed nutritional knowledge together with nutritional practices(Reference Katenga-Kaunda, Kamudoni, Holmboe-Ottesen, Fjeld, Mdala and Shi47,Reference Girard, Grant, Watkinson, Okuku, Wanjala and Cole83,Reference Dirige, McNutt, Hamatake, McGee and Manayan117,Reference Long, Martin and Janson-Sand128,Reference Hassoon and Zeidan180,Reference Zelalem, Endeshaw, Ayenew, Shiferaw and Yirgu181,Reference Teweldemedhin, Amanuel, Berhe, Gebreyohans, Tsige and Habte187,Reference Yani, Merbawani and Munfadlila188,Reference Abu-Baker, Abusbaitan, Al-Ashram and Alshraifeen191–Reference Baharzadeh, Marashi, Saki, Zare Javid and Araban194) . The knowledge components covered a wide range of essential topics; including nutritional requirements during pregnancy; benefits of supplements (iron and folic acid); food safety; and/or risks of undernutrition and inappropriate weight gain, relative to guidelines. Studies focusing on attitudes examined feelings toward healthier eating and/or the significance of supplements. Nutritional behaviours included adding an extra meal; diversifying food intake; reducing the consumption of substances like alcohol and caffeine; and/or using iodised salt and supplements. In only two studies, the gestational age of the mother on entry into the programme or intervention was less than 14 weeks of gestation(Reference Yani, Merbawani and Munfadlila188,Reference Arefi, Sadeghi, Shojaeizadeh, Yaseri and Sighaldeh193) , and almost half of the studies (n = 13, 48%) did not report the gestational age of the mother at the start of the programme or intervention(Reference Akeredolu, Osisanya, Okafor and Seriki-Mosadolorun48,Reference Soliman, Hassan, Fahmy, Abdelsalam and Salem75,Reference Peiris, Wijesinghe, Gunawardana, Weerasinghe, Rajapaksha and Rathnayake80,Reference Subapriya and Chandrasekhar90,Reference Long, Martin and Janson-Sand128,Reference Anderson, Campbell and Shepherd179–Reference Singh184,Reference Abu-Baker, Abusbaitan, Al-Ashram and Alshraifeen191,Reference Diddana, Kelkay, Dola and Sadore192) .
Most studies were quasi-experimental studies (n = 18, 66.5%)(Reference Soliman, Hassan, Fahmy, Abdelsalam and Salem75,Reference Muhamad, Mahmudiono, Abihail, Sahila, Wangi and Suyanto82,Reference Girard, Grant, Watkinson, Okuku, Wanjala and Cole83,Reference Subapriya and Chandrasekhar90,Reference Long, Martin and Janson-Sand128,Reference Anderson, Campbell and Shepherd179,Reference Shobeiri, Afshari, Nazari, Nazari and Farhadian182–Reference Abu-Baker, Abusbaitan, Al-Ashram and Alshraifeen191,Reference Baharzadeh, Marashi, Saki, Zare Javid and Araban194,Reference Khani Jeihooni, Rakhshani, Harsini and Layeghiasl195) , with a smaller number of RCTs (n = 6, 22%)(Reference Katenga-Kaunda, Kamudoni, Holmboe-Ottesen, Fjeld, Mdala and Shi47,Reference Amiri, Hamzavi Zarghani, Nazeri, Ghofranipour, Karimi and Amouzegar77,Reference Dirige, McNutt, Hamatake, McGee and Manayan117,Reference Diddana, Kelkay, Dola and Sadore192,Reference Arefi, Sadeghi, Shojaeizadeh, Yaseri and Sighaldeh193,Reference Jahangiri, Shamsi, Khorsandi and Moradzade196) , cohort (n = 1, 4%)(Reference Hassoon and Zeidan180), and cross-sectional studies (n = 2, 7.5%)(Reference Akeredolu, Osisanya, Okafor and Seriki-Mosadolorun48,Reference Zelalem, Endeshaw, Ayenew, Shiferaw and Yirgu181) . Population sizes of studies exploring knowledge, attitudes, and/or behaviours ranged from 743(Reference Aktaç, Sabuncular, Kargin and Gunes186) to 21(Reference Dirige, McNutt, Hamatake, McGee and Manayan117), with an average sample size of 131.8 (SD 148.8). Eight of the 27 studies employed a theoretical framework. Three studies employed the Health Belief Model(Reference Teweldemedhin, Amanuel, Berhe, Gebreyohans, Tsige and Habte187,Reference Diddana, Kelkay, Dola and Sadore192,Reference Baharzadeh, Marashi, Saki, Zare Javid and Araban194) , two studies employed the Theory of Planned Behaviour(Reference Khani Jeihooni, Rakhshani, Harsini and Layeghiasl195,Reference Jahangiri, Shamsi, Khorsandi and Moradzade196) , one employed Pender’s Health Promotion Model(Reference Shobeiri, Afshari, Nazari, Nazari and Farhadian182), and one study employed the Hierarchy of Effects Model(Reference Peiris, Wijesinghe, Gunawardana, Weerasinghe, Rajapaksha and Rathnayake80).
Seven (26%) studies employed individual counselling activities as the main nutritional education intervention, while ten (37%) studies including group education sessions (see Table 2). Only three studies (11%) conducted fewer than three educational sessions(Reference Amiri, Hamzavi Zarghani, Nazeri, Ghofranipour, Karimi and Amouzegar77,Reference Aktaç, Sabuncular, Kargin and Gunes186,Reference Teweldemedhin, Amanuel, Berhe, Gebreyohans, Tsige and Habte187) . Additionally, two studies included home visits from health professionals(Reference Katenga-Kaunda, Kamudoni, Holmboe-Ottesen, Fjeld, Mdala and Shi47,Reference Yani, Merbawani and Munfadlila188) , and two offered cooking classes(Reference Katenga-Kaunda, Kamudoni, Holmboe-Ottesen, Fjeld, Mdala and Shi47,Reference Subapriya and Chandrasekhar90) Three studies employed text messaging to maintain contact with participants(Reference Soliman, Hassan, Fahmy, Abdelsalam and Salem75,Reference Peiris, Wijesinghe, Gunawardana, Weerasinghe, Rajapaksha and Rathnayake80,Reference Khani Jeihooni, Rakhshani, Harsini and Layeghiasl195) , while two used phone calls for follow-up or counselling(Reference Amiri, Hamzavi Zarghani, Nazeri, Ghofranipour, Karimi and Amouzegar77,Reference Peiris, Wijesinghe, Gunawardana, Weerasinghe, Rajapaksha and Rathnayake80) . All studies except one(Reference Dirige, McNutt, Hamatake, McGee and Manayan117) reported a statistically significant improvement in nutritional knowledge, attitudes, and behaviours. These components were assessed using different validated questionnaires, and the results showed that the mean scores for knowledge, attitudes, and practices consistently improved across the studies.
Theoretical frameworks
Only 36 studies (21%) reported using a theoretical framework to guide their behavioural change interventions, with four studies employing two frameworks (see Table 3). The most common theoretical framework used was Social Cognitive Theory. This framework was employed in 14 studies (39%); most studies (n = 12,85%) were studies seeking to address gestational weight gain and dietary outcomes. Four of the six studies that employed Social Cognitive Theory to address gestational weight gain reported a statistically significant result(Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Ferrara, Hedderson, Brown, Ehrlich, Tsai and Feng92,Reference Xu, Guo, Zhang and Lu106) . Additionally, five of the six studies that employed Social Cognitive Theory to address dietary outcomes reported a statistically significant result(Reference Poston, Briley, Barr, Bell, Croker and Coxon27,Reference Sharma, Chuang, Byrd-Williams, Danho, Upadhyaya and Berens88,Reference Vander Wyst, Vercelli, O’Brien, Cooper, Pressman and Whisner165,Reference Hawkins, Hosker, Marcus, Rosal, Braun and Stanek III174,Reference Ainscough, O’Brien, Lindsay, Kennelly, O’Sullivan and O’Brien176) . The Health Belief Model was employed in nine studies. Three studies sought to increase nutrition knowledge and behaviours(Reference Teweldemedhin, Amanuel, Berhe, Gebreyohans, Tsige and Habte187,Reference Diddana, Kelkay, Dola and Sadore192,Reference Baharzadeh, Marashi, Saki, Zare Javid and Araban194) and another three studies addressed dietary outcomes(Reference Demilew, Alene and Belachew43,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81) . All six studies reported a statistically significant result(Reference Demilew, Alene and Belachew43,Reference Jing, Huang, Liu, Luo, Yang and Liao76,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Teweldemedhin, Amanuel, Berhe, Gebreyohans, Tsige and Habte187,Reference Diddana, Kelkay, Dola and Sadore192,Reference Baharzadeh, Marashi, Saki, Zare Javid and Araban194) . Eight studies employed the Theory of Planned Behaviour: four for dietary intake(Reference Demilew, Alene and Belachew43,Reference Tsegaye, Tamiru and Belachew51,Reference Haruna, Shiraishi, Matsuzaki, Yatsuki and Yeo81,Reference Katenga-Kaunda, Iversen, Holmboe-Ottesen, Fjeld, Mdala and Kamudoni86) , two for nutritional knowledge(Reference Khani Jeihooni, Rakhshani, Harsini and Layeghiasl195,Reference Jahangiri, Shamsi, Khorsandi and Moradzade196) , two for nutritional status(Reference Beressa, Whiting and Belachew45,Reference Tsegaye, Tamiru and Belachew51) , and one for gestational weight gain(Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105). Significant results were reported in all studies except one that addressed GWG(Reference Downs, Savage, Rivera, Pauley, Leonard and Hohman105).
Theoretical frameworks included in nutrition education interventions and programmes

Table 3. Long description
The table presents a comparison of various theoretical frameworks used in nutrition education interventions and programs. It includes 14 frameworks across six categories: GWG, GDM, hypertensive disorders of pregnancy, anemia, dietary outcomes, KBA, nutritional status, and total. The table has 14 rows and 8 columns. The columns are labeled with the categories, and the rows are labeled with the names of the theoretical frameworks. Notable trends include the frequent use of Social Cognitive Theory, Health Belief Model, and Theory of Planned Behaviour. Social Cognitive Theory is used in 14 studies, primarily for gestational weight gain and dietary outcomes. The Health Belief Model is used in nine studies, addressing nutrition knowledge, behaviors, and dietary outcomes. The Theory of Planned Behaviour is employed in eight studies, focusing on dietary intake, nutritional knowledge, nutritional status, and gestational weight gain.
GWG, gestational weight gain; GDM, gestational diabetes mellitus; hypertensive disorders of pregnancy: gestational hypertension or pre-eclampsia.
Discussion
This scoping review is the first study to summarise the range and scope of nutrition education interventions that have targeted a range of key maternal outcomes as well as maternal diet and nutrition outcomes. Delivery of nutrition education showed positive impact on various maternal health and nutrition outcomes, including anthropometric outcomes (GWG and MUAC); health outcomes (prevention of GDM, and anaemia); dietary outcomes; and nutritional knowledge, attitudes, and behaviours.
Anthropometric outcomes
Nutrition education was found to be able to support pregnant women to achieve appropriate GWG. This finding is consistent with a previous systematic review of 13 studies showing that nutritional education was one of the most effective strategies for promoting appropriate GWG(Reference Girard and Olude14). The considerable variability in the timing and delivery of nutrition education makes it challenging to identify and synthesise the key components of successful interventions. While most studies found nutrition education effective for managing GWG, those that reported no significant findings incorporated similar components to those used in studies that demonstrated intervention effectiveness. This finding highlights the need to understand factors that influence the success of nutrition education interventions on GWG. By identifying and refining the key components of successful nutrition education on GWG, future programmes will be better able to assist pregnant women.
Pregnancy-related weight gain can result in women being identified as having high pregnancy BMI, a designation that is not necessarily reflective of overall nutritional status. As such, mid-upper arm circumference is often considered a more reliable and practical measure for evaluating nutritional status in pregnant women(Reference Beressa, Whiting and Belachew45). In the current review, all studies focusing on MUAC were published after 2021 and four of the five were conducted in Ethiopia. This indicates an emerging shift toward considering MUAC as a useful measure of maternal nutrition status during pregnancy, particularly in low-income countries where undernutrition and inadequate GWG may be more prevalent(Reference Beressa, Whiting and Belachew45). Although only five studies were identified that used MUAC, all reported consistently significant results, suggesting that the provision of individual counselling to women by health professionals before 20 weeks of gestation can improve nutritional status during pregnancy. This is consistent with previous research which suggests that individual nutrition education delivered by health professionals using a women-centred approach, whereby the unique circumstances of pregnant women is emphasised in the care, can be particularly effective in promoting positive outcomes(Reference Fujimoto, Iida, Takeuchi, Shinohara, Kubota and Nakamura178). While MUAC appears to be a practical and sensitive indicator of maternal nutritional status in low-resource and undernourished populations, its broader generalisability across diverse pregnancy populations, particularly in high-income settings, remains limited and warrants further investigation.
Maternal health outcomes
Nutrition education focused on maternal health outcomes had mixed results. Prevention of GDM, and iron deficiency anaemia, were the focus of 50 studies included in this review. Most of these studies were focused on GDM, although the majority of studies reported no significant differences as a result of the nutrition education intervention. Possible reasons for this could be the inclusion of heterogeneous participant groups across studies and that many studies did not appear to factor in the known risk factors of GDM, including pre-pregnancy BMI, maternal age, and a history of GDM(Reference Li, Hu, Zeng, Zheng, Ye and Wei197). Additionally, education commenced after 14 weeks of gestation in half of the studies. This potentially limits their impact on early pregnancy metabolic changes that contribute to GDM development(Reference Buchanan, Xiang and Page198). Future research that focuses specifically on expectant mothers with identified GDM risk factors, initiated in early pregnancy or even the preconception period, may have greater potential for a role of nutrition education in prevention of cardiometabolic health-related complications during pregnancy.
A small number of studies explored the role of nutrition education on iron deficiency anaemia. Iron deficient anaemia is the most prevalent micronutrient deficiency observed during pregnancy, and is known to significantly affect both foetal and maternal health(Reference Kuma, Tamiru and Belachew157). This review found that risk of anaemia may be reduced by providing education to pregnant women regarding the importance of iron supplementation and providing guidance on consuming an iron-rich diet. This finding highlights the importance of integrating women-centred nutrition-focused care, which accounts for socioeconomic and cultural factors, into standard prenatal practices as a way to improve both maternal and neonatal health outcomes through influencing a woman’s access to iron-rich foods and adherence to supplementation guidelines(Reference Purba and Sitepu199). Future research should explore the effectiveness of tailored interventions based on factors that impact women directly to enhance the impact of nutrition education on diverse populations.
Dietary outcomes
This scoping review found that maternal dietary outcomes are able to be improved through delivery of nutrition education during pregnancy. The World Health Organization (WHO) advises increasing energy intake and balancing nutrients in relation to energy expenditure during pregnancy(200) and encourages sufficient protein consumption while limiting fats, sugars, and sodium intake(200). Nutrition education during pregnancy is vital in encouraging adequate nutrient intake among pregnant women(Reference Fujimoto, Iida, Takeuchi, Shinohara, Kubota and Nakamura178). While previous research suggests that nutrition education is more effective when personalised according to age, weight, gestation, activity level, and level of nutrition knowledge(Reference Fujimoto, Iida, Takeuchi, Shinohara, Kubota and Nakamura178), only five studies included in this review included personalised diet plans. Much focus has been on women who are outside a ‘healthy weight’ range, yet research suggests that women in the ‘healthy weight’ range may have inadequate nutritional intake during pregnancy(Reference Kubota, Itoh, Tasaka, Naito, Fukuoka and Muramatsu Kato201,Reference Eshak, Okada, Kimura, Baba, Ikehara and Iso202) . Effective nutrition education programmes are essential, not only for women with obesity or underweight, but also for those considered in the healthy weight range. It should be noted that only two studies in this review focused on women with healthy weight BMI(Reference Li, Piaseu, Phumonsakul and Thadakant56,Reference Fujimoto, Iida, Takeuchi, Shinohara, Kubota and Nakamura178) . More research is needed to study women in all weight groups to better understand their nutritional needs during pregnancy.
Nutrition knowledge, attitudes, and behaviours
Our review indicated that nutrition education could improve nutritional knowledge, attitudes, and/or behaviours since all the studies included, except one(Reference Dirige, McNutt, Hamatake, McGee and Manayan117), reported a statistically significant result. While women may be aware of the importance of healthy eating during pregnancy, they often lack knowledge of the specific dietary recommendations or the necessary skills to improve their eating habits(Reference Hassoon and Zeidan180). A previous systematic review highlighted the interconnection of knowledge, attitude, and dietary practices, emphasising that knowledge and attitude influence each other and significantly impact dietary behaviours in pregnant women(Reference Bayked, Yimer, Gelaw, Mohammed and Mekonen203). These results, coupled with the findings of our scoping review, indicate the critical importance of nutrition education during pregnancy in shaping maternal behaviour, and underscore the need for evidence-based, widely accessible nutrition education to be included as part of antenatal care across health care settings. Interestingly, the use of theory to guide interventions and programmes has a positive role in the success of nutrition education programmes(Reference Murimi, Kanyi, Mupfudze, Amin, Mbogori and Aldubayan204). Although the use of theories was not dominant in this review, with only 21% of studies (n = 36) using at least one theory, studies that employed a theoretical framework were more likely to have significant findings. This supports the results of another systematic review showing that a well-applied theory may contribute to the success of nutrition education interventions(Reference Murimi, Kanyi, Mupfudze, Amin, Mbogori and Aldubayan204). The most common theoretical framework used in studies included in this review was Social Cognitive Theory(Reference Poston, Briley, Barr, Bell, Croker and Coxon27,Reference Poston, Bell, Croker, Flynn, Godfrey and Goff28,Reference Sandborg, Söderström, Henriksson, Bendtsen, Henström and Leppänen58,Reference Willcox, Wilkinson, Lappas, Ball, Crawford and McCarthy64,Reference Liu, Wilcox, Wingard, Turner-McGrievy, Hutto and Burgis68,Reference de Jersey, Meloncelli, Guthrie, Powlesland, Callaway and Chang69,Reference Sharma, Chuang, Byrd-Williams, Danho, Upadhyaya and Berens88,Reference Ferrara, Hedderson, Brown, Ehrlich, Tsai and Feng92,Reference Xu, Guo, Zhang and Lu106,Reference Vander Wyst, Vercelli, O’Brien, Cooper, Pressman and Whisner165,Reference Hawkins, Hosker, Marcus, Rosal, Braun and Stanek III174,Reference Ainscough, O’Brien, Lindsay, Kennelly, O’Sullivan and O’Brien176,Reference Arefi, Sadeghi, Shojaeizadeh, Yaseri and Sighaldeh193) . Social Cognitive Theory integrates concepts from cognitive, behavioural, and emotional approaches to behaviour change programmes. This makes this theory a practical choice for nutrition interventions(Reference Zheng, Mancino, Burke and Glanz205).
Finally, few of the interventions included in this review involved dietitians or other suitably trained health care professionals in the delivery of nutrition education, despite the overall positive effects observed across maternal, dietary, and behavioural outcomes. Integrating dietitians into routine antenatal care alongside midwives or public health nurses may strengthen the delivery of evidence-based nutrition education and improve the effectiveness of interventions aimed at optimising maternal health during pregnancy.
Future research exploring the role of nutrition education and pregnancy outcomes should consider a combination of the strengths identified in this scoping review. Specifically, future research should assess the user-friendliness of education materials across different delivery methods. It is important to consider the usability of different modes of delivery, including digital platforms, counselling, and physical forms of educational materials, for different population groups that include migrant women, women with low literacy (including low health literacy), and women with high-risk pregnancies. A human-centred design approach could optimise information delivery, ensuring alignment with how pregnant women seek and process nutritional guidance.
While there are clear findings of this scoping review, there are strengths and limitations that need to be taken into consideration. A key strength is its comprehensive overview of current evidence on the impact of nutrition education on maternal health and dietary outcomes, which highlights diverse intervention approaches and identifies gaps for future research. However, as a scoping review, this work does not seek to examine associations nor conduct a meta-analysis. A more targeted systematic review of specific components of this review could achieve these outcomes and may provide more concrete outcomes and areas for future research. The nature of this scoping review means the effectiveness of each mode of nutritional information could not be compared and contrasted. While a more targeted study may have enabled such an analysis, the value of this scoping review is its breadth in studies included. In addition, this review did not address nutrition advice received by women prior to conception or in previous pregnancies, an important target group. As participants were often volunteers who may have had a greater interest in nutrition than the general population, the reported practices probably overestimate the actual situation. A final limitation is the exclusion of non-English studies, which may have resulted in a publication bias toward studies located in high-income countries.
Conclusion
This review highlights the vast number of studies that have been conducted exploring the range of nutrition education methods and programmes seeking to improve maternal health and dietary outcomes. This review highlights considerable variability in the methods used to deliver nutrition education to women and identifies the need for refined delivery of nutrition education across diverse populations to positively impact maternal health during pregnancy. Future research should prioritise tailoring the duration or episodes of engagement, participant characteristics, and content of dietary interventions more consistently. Whilst the role of nutrition education is central in assisting the best maternal and child health and dietary outcomes, a consistent and best-practice approach to this is yet to be determined.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954422426100444
Acknowledgements
None.
Authorship
Conceptualisation, methodology: F.H.M., S.S.M., J.Z., J.W., P.V.D.P., and V.V.; screening, analysis, and interpretation of data: F.H.M., S.S.M., J.Z., J.W., P.V.D.P., and V.V.; writing original draft preparation: F.H.M., S.S.M., J.Z., P.V.D.P., and V.V.; writing review and editing: F.H.M., S.S.M., J.Z., J.W., P.V.D.P., and V.V. All authors have read and agreed to the published version of this manuscript.
Financial support
This research received no financial support.
Competing interests
All authors have worked in paid and unpaid roles with not-for-profit food security organisations or with organisations that focus on pregnancy and/or nutrition outcomes. No other competing interests to declare.
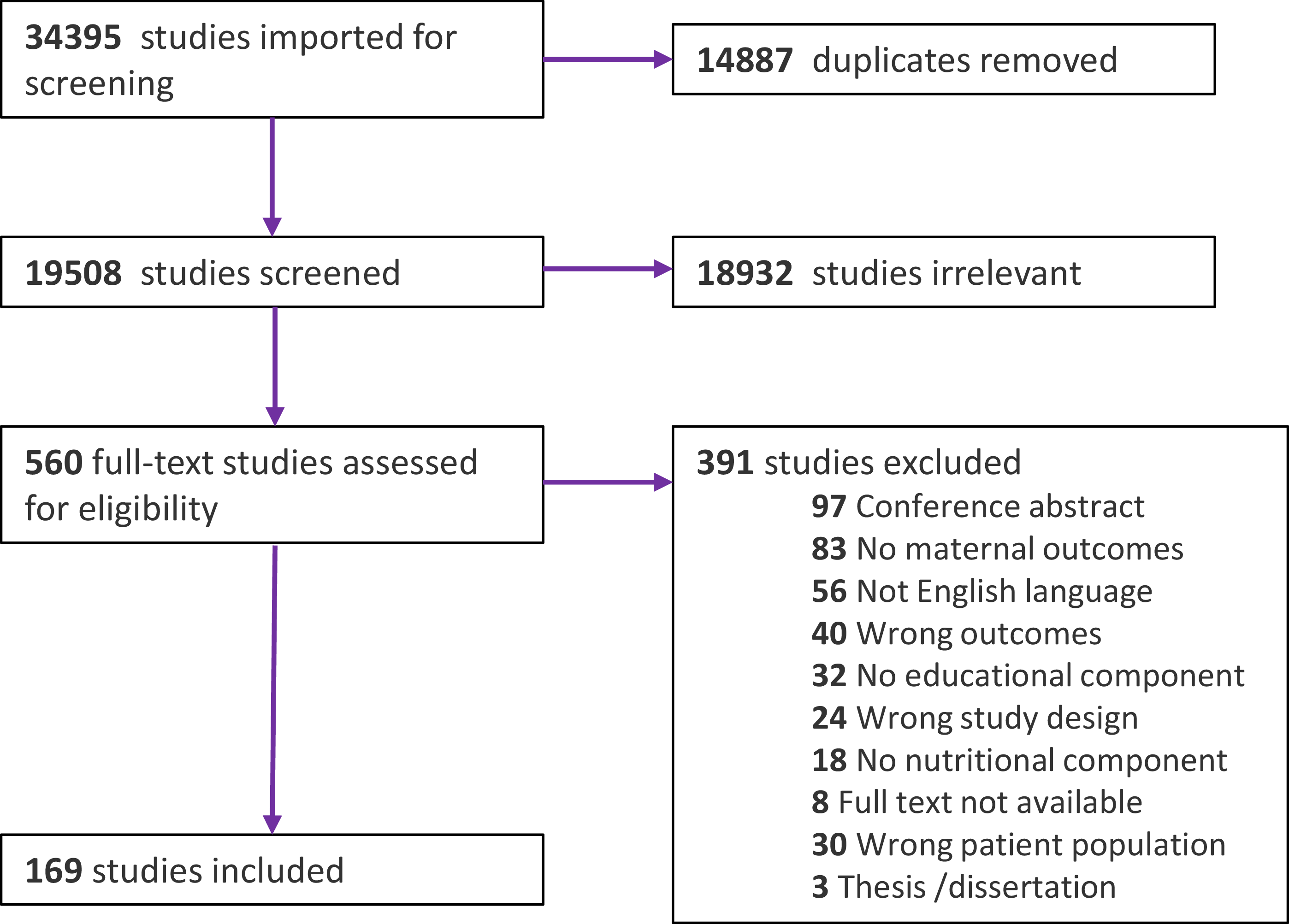
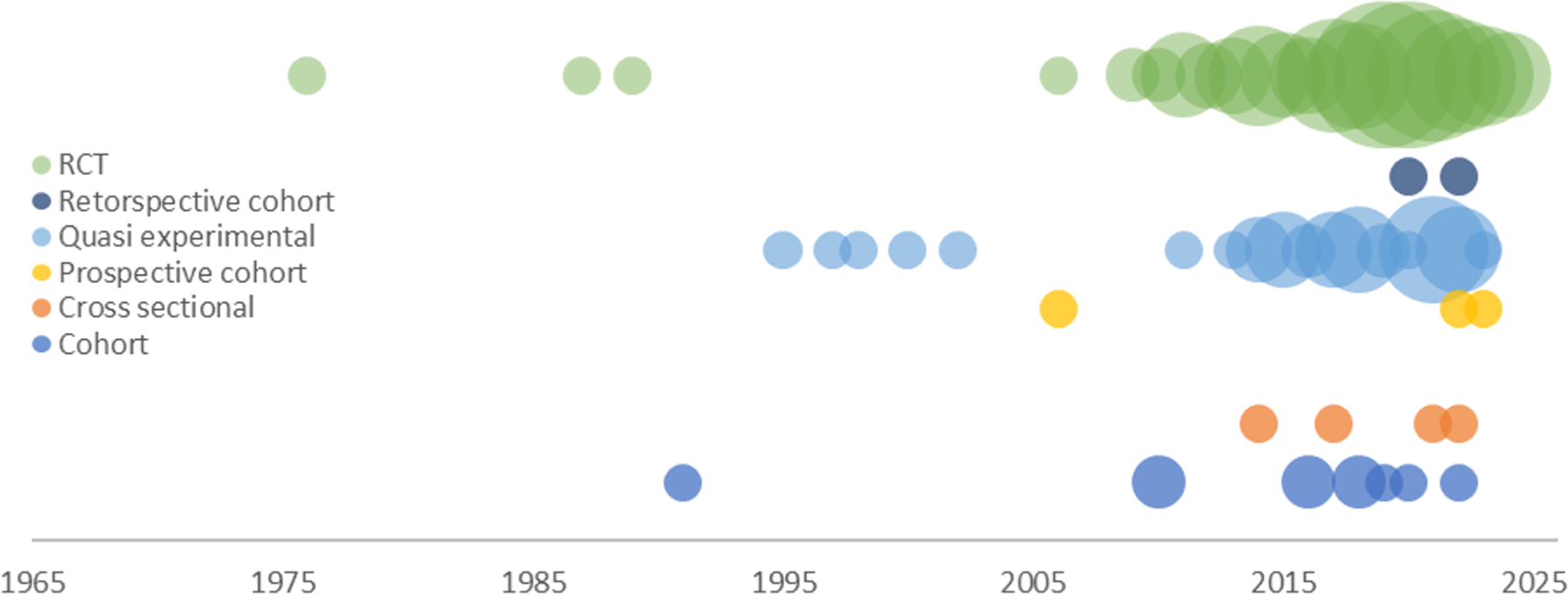
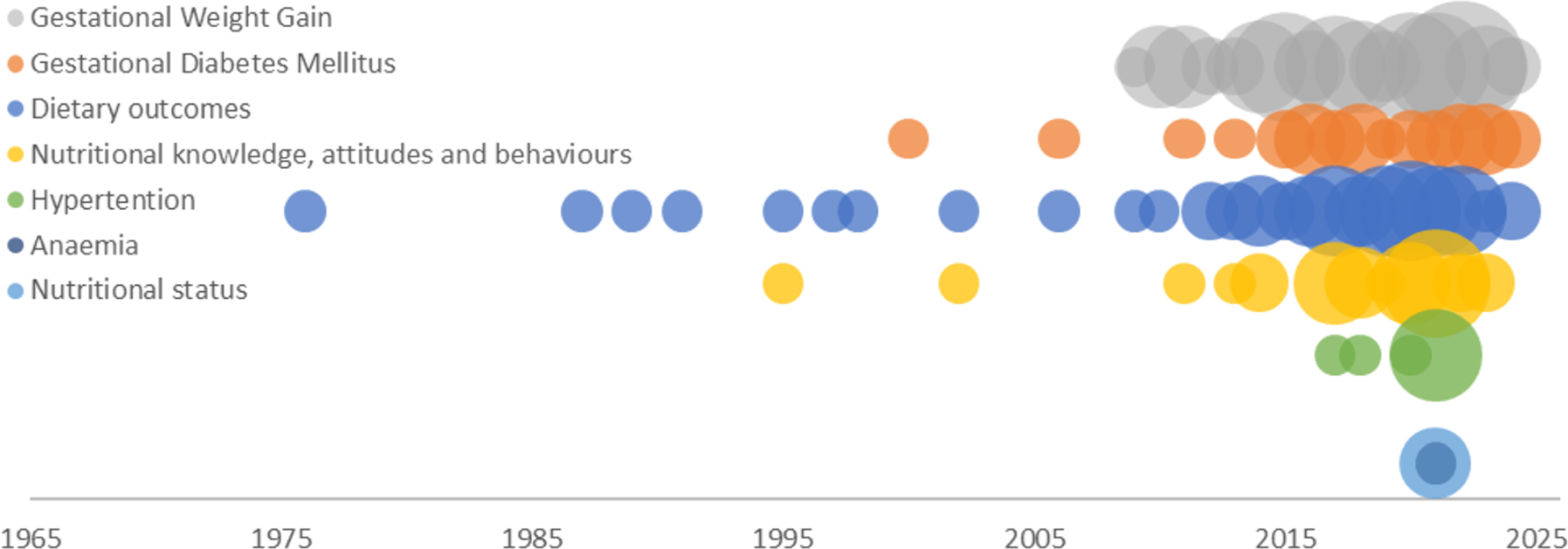
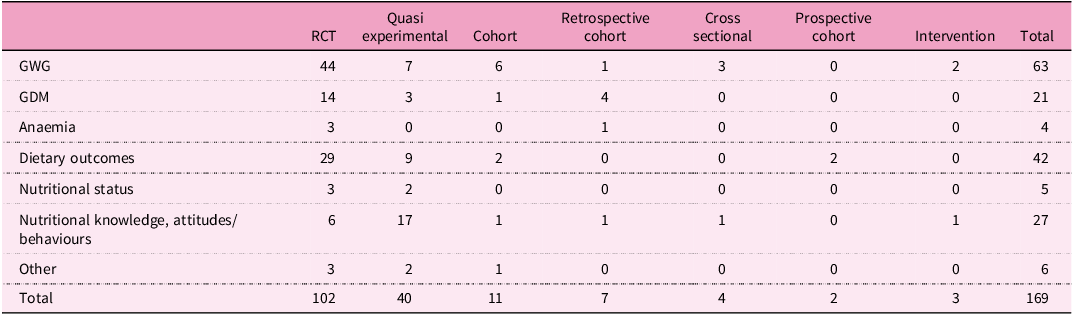
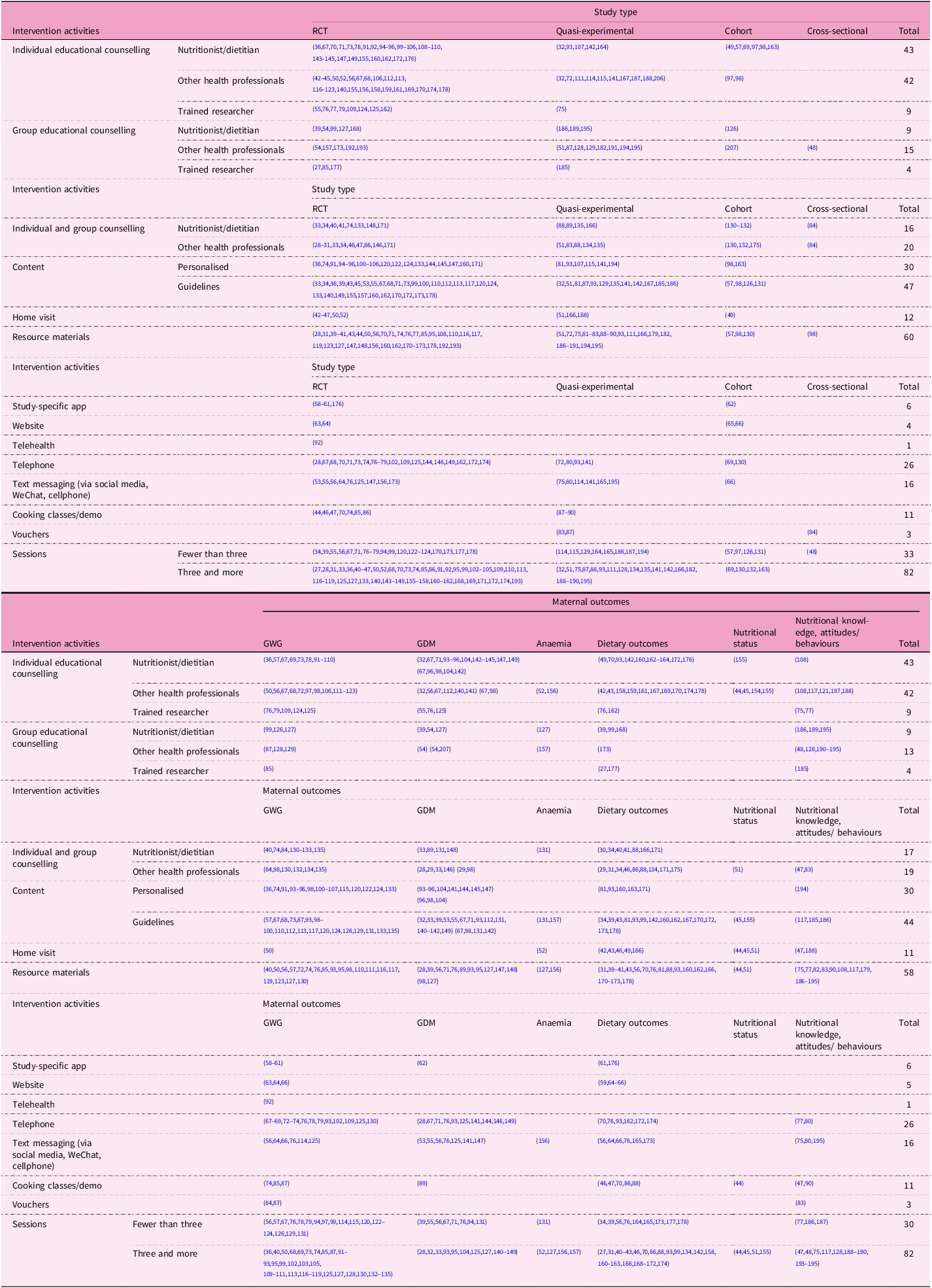
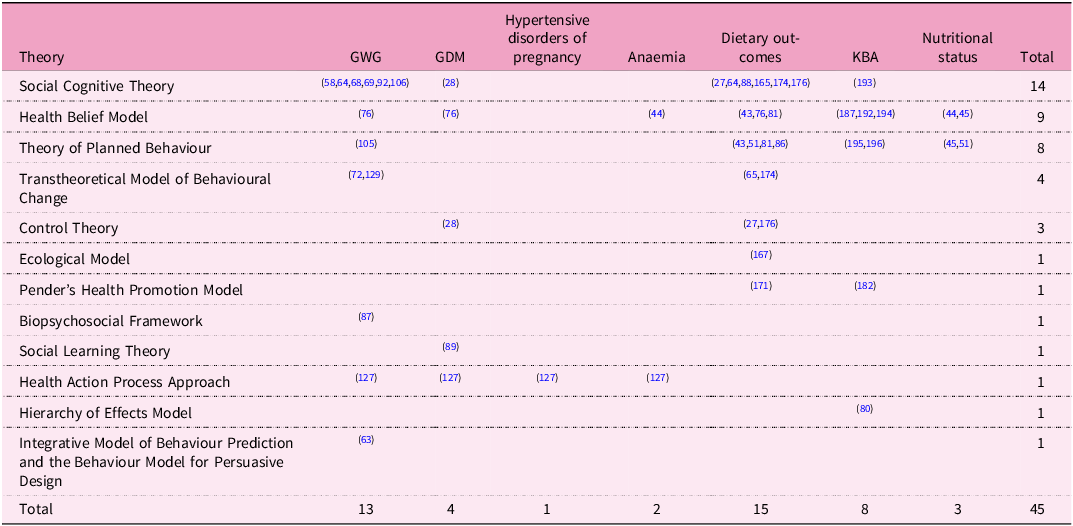



 Open access
Open access