Through the development and industrialisation of countries, infectious diseases have been gradually replaced by chronic conditions such as cancer, diabetes and CVD known as an epidemiologic transition(Reference Adogu, Ubajaka and Emelumadu1). At the current stage, chronic diseases impose the largest economic and health-related burdens on societies(Reference Adogu, Ubajaka and Emelumadu1). Along with the importance of physical well-being in the occurrence of such conditions, psychological status has also been suggested as a matter of concern(Reference Machado, Veronese and Sanches2–Reference Wang, Li and Shi4). Anxiety, depression and psychological distress are among the top psychological disorders people are mostly affected by(Reference Baxter, Scott and Vos5,Reference Kessler6) . Global prevalence of psychological disorders is 22·1 % according to the latest report(Reference Charlson, van Ommeren and Flaxman7). Based on recent cross-sectional studies in Iran, over 30 %, 33 % and 38 % of adults have, respectively, experienced anxiety, depression and psychological distress(Reference Maroufizadeh, Pourshaikhian and Pourramzani8,Reference Ansari, Parsaei and Noorbala9) .
Diagnosing and treating psychological disorders are challenging due to their diverse clinical presentations, which make it crucial to explore preventive factors(Reference Malhi and Mann10). Environmental factors, family history and lifestyle behaviours, particularly dietary intakes, could be responsible for the prevalence of psychological disorders(Reference Saveanu and Nemeroff11). Although several dietary patterns and food groups have been studied in relation to them(Reference Gibson-Smith, Bot and Brouwer12–Reference Ventriglio, Sancassiani and Contu14), considering nutrients intake as potential predictors could broaden our knowledge towards the mechanistic pathways more efficiently. One-carbon cycle is among the recommended pathways by which nutrients could influence psychological health status(Reference Dahal and Devi15). This cycle contributes to the production of several neurotransmitters; some nutrients known as ‘methyl donor nutrients’ are involved in its regulation(Reference Anderson, Sant and Dolinoy16). Among methyl donor nutrients, B-vitamins (folate, B2, B6 and B12) have been mostly received research attention; however, choline and betaine have been less studied in relation to psychological disorders.
Current evidence for protective properties of choline and betaine against developing psychological disorders is mostly obtained from animal studies(Reference Glenn, Adams and McClurg17–Reference Jeyhoonabadi, Alimoahmmadi and Hassanpour19); human investigations are scarce in this regard. According to a recent cross-sectional study on American adults, individuals who consume the highest amounts of choline might have a lower possibility of developing depression signs compared with the lowest amounts consumers(Reference Li, Kang and Zhang20). Another study suggested that higher serum choline levels are negatively related to odds of anxiety, whereas no significant association was found with depression(Reference Bjelland, Tell and Vollset21). On the other hand, a cohort study on pregnant women found that plasma choline, but not betaine, may be a risk factor for antenatal anxiety and depression during pregnancy(Reference van Lee, Quah and Saw22).
To our knowledge, only one study has explored the relation between choline intake and depression(Reference Li, Kang and Zhang20), while there is no investigation regarding betaine intake as well as other psychological disorders. The pattern of psychological disorders in the Middle East differs from other regions due to its unique socio-economic challenges, highlighting it as a high-priority public health issue to address. Given the pivotal role of methyl donor nutrients in the synthesis of neurotransmitters and their importance in maintaining psychological health coupled with the paucity of evidence on choline and betaine intake as key methyl donors, this study aimed to investigate the association between dietary choline and betaine intake and common psychological disorders including depression, anxiety and psychological distress in a sample of Iranian adults. We hypothesised that a higher dietary intake of choline and betaine would be associated with a lower risk of depression, anxiety and psychological distress.
Methods
Study design and population
This study used data from Diet in relation to Metabolic, sleep and psychological health Status project, which is a population-based cross-sectional investigation performed on a sample of Iranian adults in 2021. Detailed methodology and key insights into Diet in relation to Metabolic, sleep and psychological health Status have been reported elsewhere(Reference Poursalehi, Shahdadian and Hajhashemy23). In brief, a total of 600 Iranian adults residing in Isfahan, Iran were invited to participate in this study, considering a multistage cluster random sampling method. Participants were recruited from twenty schools in different educational districts. All staffs aged 20–65 years including employees, assistants, managers, teachers and crews were eligible for this study, supporting a relatively representative sample. Individuals who (1) were on a special diet (e.g., weightloss or weightgain diet); (2) were pregnant or in a lactating period; (3) had missing data; (4) reported implausible energy intakes (< 3347.2 or > 17572.8 kJ/d)(Reference Willett and Hu24) and (5) had a history of stroke, CVD, type 1 diabetes and cancer were not considered for the current analyses. Considering the mentioned criteria, a total of 533 individuals were included in the final analyses. All participants signed written informed consent. This study was conducted according to the guidelines laid down in the Declaration of Helsinki and the local Ethics Committee of Isfahan University of Medical Sciences approved the study’s protocol (no. IR.MUI.RESEARCH.REC.1399.612).
Assessment of dietary intakes
A semi-quantitative 168-item FFQ, developed and validated for Iranian adults, was used to evaluate dietary intakes(Reference Mirmiran, Esfahani and Mehrabi25). An expert dietitian guided participants on how to fill out the FFQ. Participants were requested to report the frequency and quantity of each food item during the preceding year. Then, the reported frequencies and portion sizes of foods were converted to g/d using household measurement guidelines(Reference Ghaffarpour, Houshiar-Rad and Kianfar26). Converted values were then imputed to Nutritionist IV software modified for Iranian foods to extract intakes of total energy and key nutrients. Furthermore, daily choline and betaine intakes were obtained according to the US Department of Agriculture food content database(Reference Patterson, Bhagwat and Williams27).
Assessment of psychological disorders
The validated Iranian version of the Hospital Anxiety and Depression Scale was used to assess anxiety and depression(Reference Montazeri, Vahdaninia and Ebrahimi28). This questionnaire encompasses fourteen questions in two subscales of depression and anxiety. Each question is rated on a four-point scale, with higher scores reflecting greater levels of anxiety and depressive symptoms. The total score for each subscale ranges from 0 to 21; a score of 7 or below indicates a normal status, while a score of 8 or higher suggests the presence of anxiety or depression.
Moreover, the validated twelve-item Persian version of the General Health Questionnaire was used to measure psychological distress status(Reference Montazeri, Harirchi and Shariati29). A four-response option was applied to each item: less than usual, usual, more than usual and much more than usual. The current study used the bimodal approach to determine each person’s psychological distress score (0–0–1–1). Using this approach, the General Health Questionnaire scores range from 0 to 12; higher values indicate greater psychological distress. In this study, a score of 4 or more was considered as high level of psychological distress.
Assessment of other variables
Anthropometric values were evaluated by two trained dietitians. Weight was measured using a body composition analyzer (Tanita MC-780MA, Tokyo, Japan) with a precision of 0·1 kg, while participants were dressed in light clothing and barefoot. A tape measure fixed to the wall was used to assess height with a precision of 0·5 cm, with participants standing barefoot. Weight (kg) was divided by height squared (m2) to determine BMI. The validated International Physical Activity Questionnaire was used for evaluating physical activity(Reference Moghaddam, Aghdam and Jafarabadi30). Further information on demographic variables including gender, age, medical history, education, smoking, marital status and antidepressant medications (fluoxetine, amitriptyline, fluvoxamine, nortriptyline, citalopram and imipramine) was gathered by a self-administered questionnaire.
Statistical analysis
Kolmogorov–Smirnov test and Q–Q plots were employed to examine the normal distribution of study variables. First, dietary intakes of choline and betaine were adjusted for total energy intake by the residual method(Reference Willett, Howe and Kushi31). Participants were then classified into tertiles of energy-adjusted intake of choline and betaine. Demographic data is presented as mean (sd) for continuous and percentage for categorical variables. Differences of continuous and categorical variables across tertiles of dietary choline and betaine were compared using one-way ANOVA and chi-square test, respectively. Dietary intakes of selected nutrients and food groups are presented as mean (sd) and were compared across tertiles of choline and betaine intake by ANCOVA. Total energy and macronutrients intakes were adjusted for age and gender, while other dietary factors were adjusted for age, gender and total energy. Binary logistic regression was used to calculate OR and 95 %CI for psychological disorders across tertiles of dietary choline and betaine in crude and multivariable-adjusted models. Gender (male/female), age (continuous) and total energy intake (continuous) were taken into account in the first model. The second model has also included adjustments for physical activity (inactive/minimally active/active), education (≤ diploma/ > diploma), marital status (single/married/divorced or widow), smoking status (non-smoker/ex-smoker/current smoker), anti-depressant medication usage (no/yes), saturated fat (continuous) and Fe (continuous) intakes. In order to evaluate an overweight/obesity-independent association, further adjustment for BMI (continuous) was done in the last model. All OR (95 % CI) were calculated using the first tertile of choline and betaine as the reference group. Tertiles of choline and betaine were considered as an ordinal variable for trend estimation of OR across these tertiles. All statistical analyses were performed using the SPSS software (SPSS Inc., version 26.0). P values less than 0·05 were considered statistically significant.
Results
Out of 600 invited individuals, 543 participants agreed to participate in the Diet in relation to Metabolic, sleep and psychological health Status study. An additional ten participants were excluded due to having incomplete data on the psychological disorders questionnaire (n 3), having more than seventy blank items on FFQ (n 4) and reporting energy intake outside the range of 3347.2–17572.8 kJ/d (n 3). Thus, the present analysis included a total of 533 participants, of whom 53·8 % were males. Participants had an average age of 42·6 (11·14) years; and mean BMI was 26·9 (4·41) kg/m2. Total prevalence of depression, anxiety and psychological distress was 18·9 % (n 101), 5·1 % (n 27) and 33·4 % (n 178), respectively. Average intake of betaine and choline in the total population was 99·25 (±47·28) mg/d and 424·11 (±198·52) mg/d, respectively.
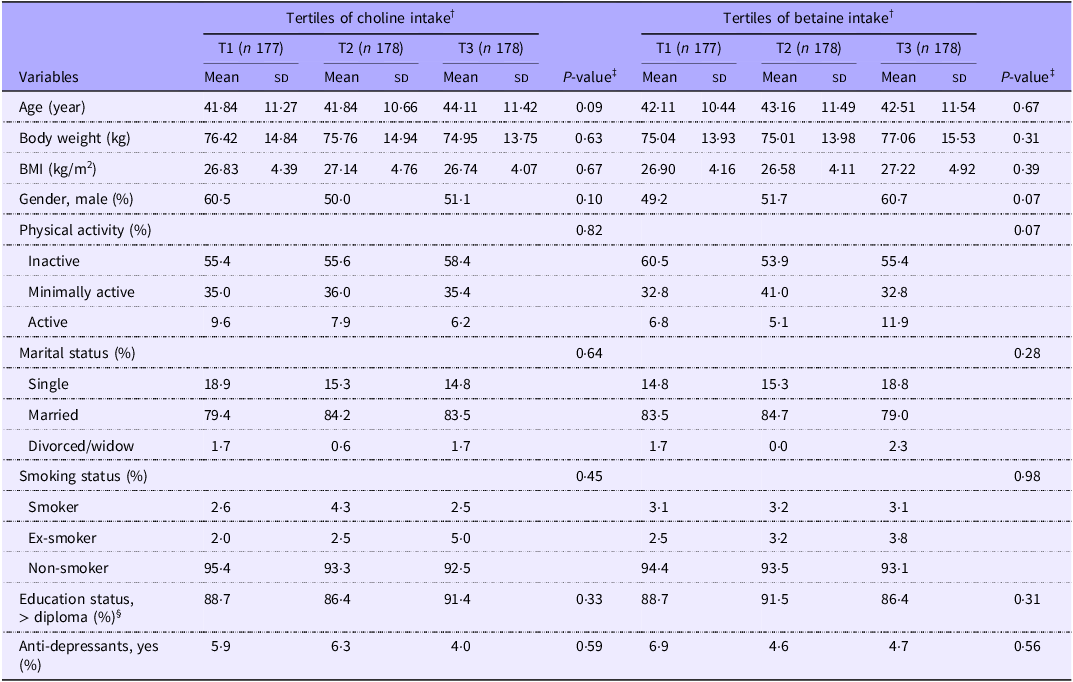
General characteristics of participants across tertiles of choline and betaine intake are presented in Table 1. There were no significant differences in terms of gender, age, BMI, weight, physical activity, education level, smoking status, marital status and use of antidepressant medications across tertiles of choline and betaine.
General characteristics of study participants across energy-adjusted tertiles of choline and betaine intake (n 533) * (Mean values and standard deviations)

Abbreviation: T: tertile.
* Continuous variables are expressed as mean (standard deviation (sd)) and categorical variables are displayed as percentage. Mean (sd) intake for choline in T1 was 282·02 (sd 55·37); in T2 was 405·96 (sd 29·24) and in T3 was 583·54 (sd 153·07) mg/d. For betaine, mean (sd) intake in T1 was 65·79 (sd 13·45); in T2 was 92·69 (sd 7·14) and in T3 was 139·08 (sd 41·32) mg/d.
† Choline and betaine intakes were adjusted for energy intake based on the residual method.
‡ Obtained by ANOVA for quantitative variables and chi-square test for categorical variables.
§ Education categorised as > diploma (post-secondary education, e.g., university) v. ≤ diploma or secondary level (completion of high school or lower).
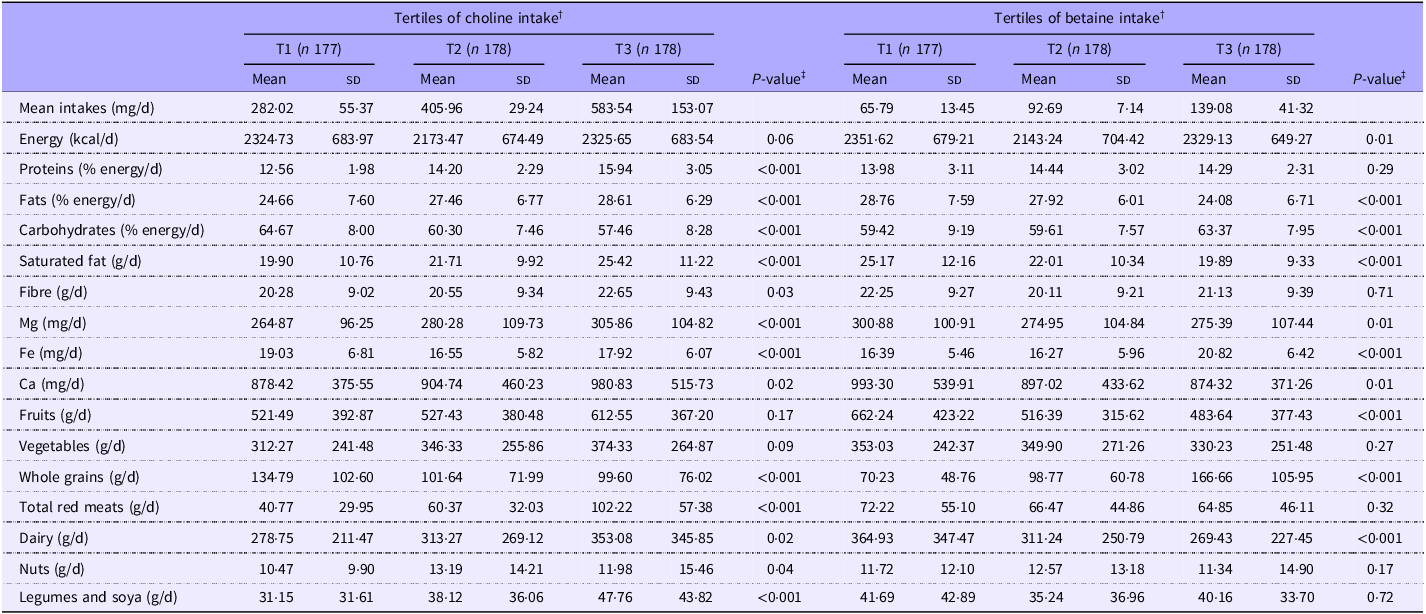
Dietary intakes of participants across tertiles of choline and betaine intake are demonstrated in Table 2. Individuals in the highest tertile of choline had significantly higher intakes of protein, fat, fibre, saturated fat, Ca, Mg, legumes and soya, nuts, red meats and dairy compared with those in the lowest tertile. Conversely, those in the highest tertile of choline intake had lower intakes of carbohydrates, Fe and whole grains compared with those in the lowest tertile. No significant differences were observed in terms of total energy, fruits and vegetables intake between dietary choline tertiles. Furthermore, participants in the third tertile of dietary betaine had higher intakes of carbohydrates, Fe and whole grains, as well as lower intakes of energy, fat, saturated fat, Ca, Mg, dairy and fruits compared with those in the first tertile. No significant differences were found in terms of protein, fibre, vegetables, red meats, nuts, legumes and soya intakes in tertiles of dietary betaine.
Dietary intakes of study participants across energy-adjusted tertiles of choline and betaine intake (n 533) * (Mean values and standard deviations)

* Values are means (standard deviation (sd)).
† Choline and betaine intakes were adjusted for energy intake based on the residual method.
‡ P-value obtained from ANCOVA. Energy intake and macronutrients were adjusted for age and gender; all other values were adjusted for age, gender and energy intake.
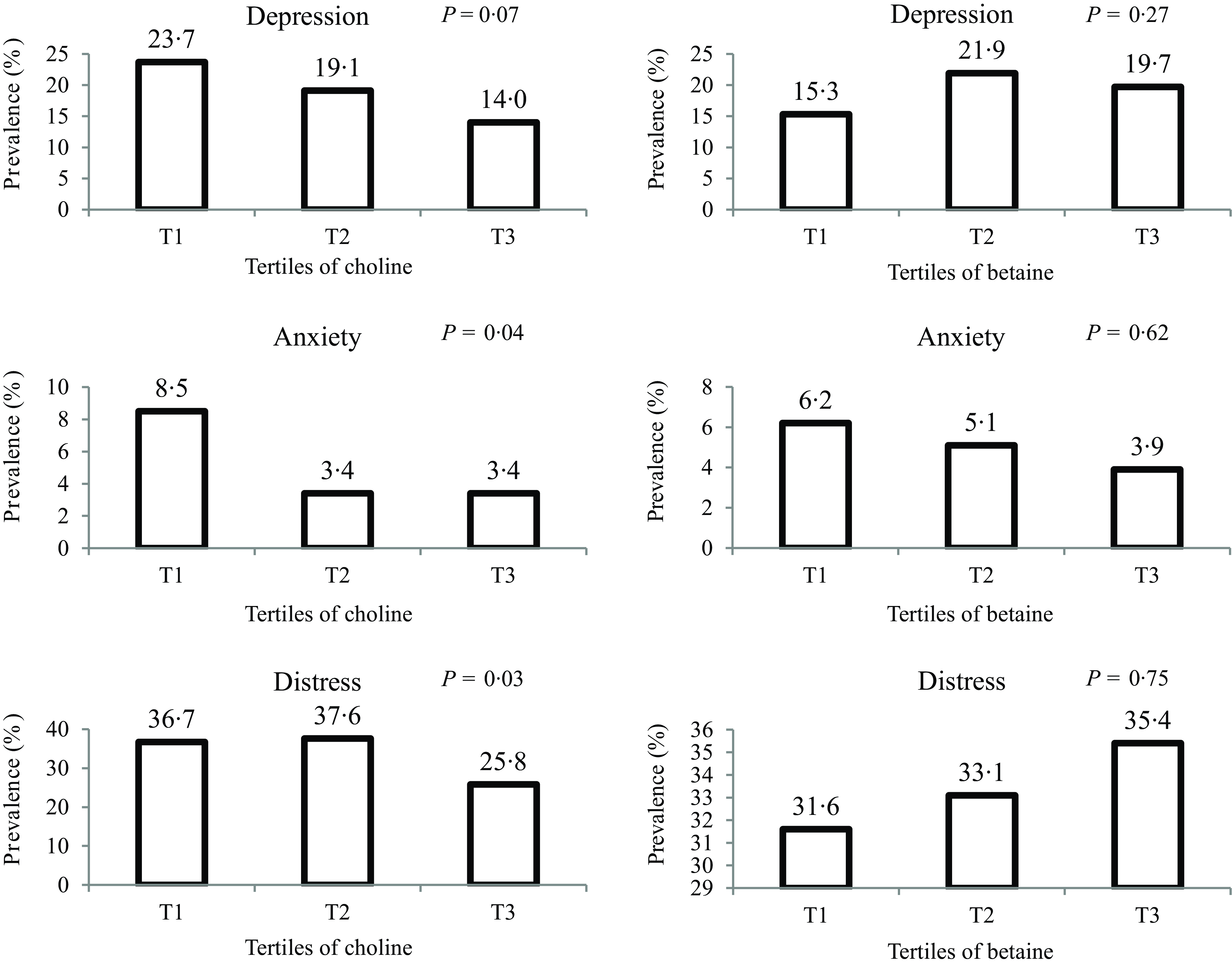
Figure 1 illustrates the prevalence of psychological disorders across energy-adjusted tertiles of choline and betaine intake. Participants in the highest tertile of choline intake, compared with the lowest tertile, exhibited a lower prevalence of anxiety (3·4 % v. 8·5 %; P = 0·04) and psychological distress (25·8 % v. 36·7 %; P = 0·03), while prevalence of depression did not differ significantly across choline tertiles (P = 0·07). There were no significant differences in the prevalence of depression, anxiety and psychological distress across tertiles of betaine intake.
Prevalence of psychological disorders across energy-adjusted tertiles of dietary choline and betaine intake. Mean (sd) intake for choline in T1 was 282·02 (sd 55·37); in T2 was 405·96 (sd 29·24) and in T3 was 583·54 (sd 153·07) mg/d. For betaine, mean (sd) intake in T1 was 65·79 (sd 13·45); in T2 was 92·69 (sd 7·14) and in T3 was 139·08 (sd 41·32) mg/d.

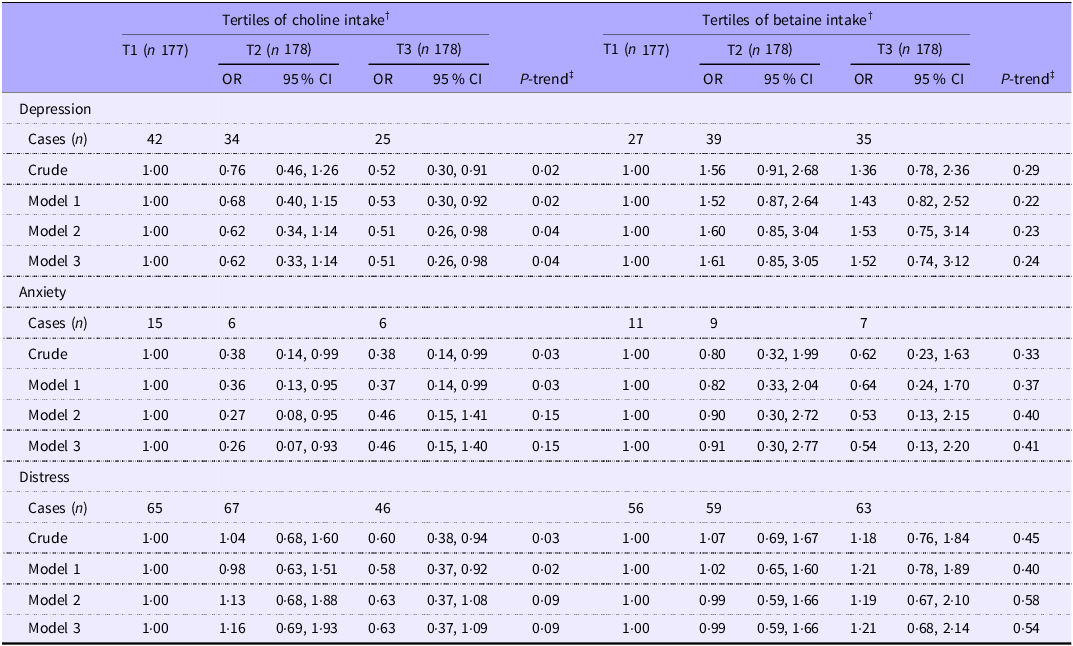
Crude and multivariable-adjusted OR for depression, anxiety and psychological distress across tertiles of choline and betaine intake are reported in Table 3. In the crude model, participants in the highest tertile of choline intake, compared with the lowest, had 48 %, 62 % and 40 % lower odds of depression (95 % CI: 0·30, 0·91), anxiety (95 % CI: 0·14, 0·99) and psychological distress (95 % CI: 0·38, 0·94), respectively. However, after adjusting for potential confounders in the final model, the associations remained significant for depression (OR T3 v. T1 = 0·51; 95 % CI: 0·26, 0·98) but not for psychological distress (OR T3 v. T1 = 0·63; 95 % CI: 0·37, 1·09) and anxiety (OR T3 v. T1 = 0·46; 95 % CI: 0·15, 1·40). Regarding betaine intake, there was no significant association with odds of depression, anxiety or psychological distress in the crude model. These associations did not change after adjusting for potential confounders (depression: ORT3 v. T1 = 1·52, 95 % CI: 0·74, 3·12; anxiety: ORT3 v. T1 = 0·54, 95 % CI: 0·13, 2·20; distress: ORT3 v. T1 = 1·21, 95 % CI: 0·68, 2·14).
Multivariable-adjusted OR (95 % CI) for psychological disorders across energy-adjusted tertiles of choline and betaine intake (n 533) *

* All values are OR and 95 % CI. Mean (sd) intake for choline in T1 was 282·02 (sd 55·37); in T2 was 405·96 (sd 29·24) and in T3 was 583·54 (sd 153·07) mg/d. For betaine, mean (sd) intake in T1 was 65·79 (sd 13·45); in T2 was 92·69 (sd 7·14) and in T3 was 139·08 (sd 41·32) mg/d. Model 1: adjusted for age, gender and energy intake. Model 2: More adjustments for physical activity, education, marital status, smoking status, anti-depressant medication usage, saturated fat and Fe intake. Model 3: further adjustment for BMI.
† Choline and betaine intakes were adjusted for total energy intake based on the residual method.
‡ P trend was obtained by the use of tertiles of choline and betaine intake as an ordinal variable in the model.
Discussion
Findings from this study on Iranian adults indicate that higher intake of choline intake is associated with 49 % lower odds of depression after considering several potential confounders. Such an inverse association was significant in cases of anxiety and psychological distress in crude models; however, the relationship disappeared after controlling the confounders. No substantial relation was demonstrated between dietary betaine intake and these psychological disorders.
Psychological disorders are becoming more prevalent worldwide with a pronounced upward trend, affecting individuals’ quality of lives and increasing the risk of non-communicable diseases(Reference Stein, Benjet and Gureje32,Reference Blasco, García-Jiménez and Bodoano33) . Addressing these conditions can not only improve individuals’ well-being but also bring economic and social benefits to society. Diet has been known as a fundamental element in controlling psychological disorders and has captured significant interest in research(Reference Dash, O’Neil and Jacka34). Findings of the current study suggested that dietary choline intake may have clinical and public health implications for psychological disorders, particularly depression. This would provide an easily available dietary approach to support current treatments and people should be advised to consume more dietary sources of choline, such as dairy products, meat, poultry, fish, eggs, cruciferous vegetables and certain beans. Future research should primarily focus on prospective cohort and randomised controlled trials to examine dose–response correlations between depression and choline intake from diet and supplements and demonstrate causality.
Limited evidence is available regarding the association between choline and betaine consumption and common psychological disorders. A study involving 156 individuals with depression revealed a correlation between poorer depressive status and comparatively lower dietary choline consumption(Reference Wendołowicz, Stefańska and Jankowska35). Another recent cross-sectional study found an inverse relationship between dietary choline and depression in the National Health and Nutrition Examination Survey(Reference Li, Kang and Zhang20). Regarding serum concentrations, the Hordaland study, a large cross-sectional examination of a general adult population, revealed that higher choline concentrations were linked to 33 % higher risks of anxiety but not depression(Reference Bjelland, Tell and Vollset21). Moreover, a study of pregnant women found that while plasma betaine concentrations did not correlate with antenatal anxiety or depression during pregnancy, plasma choline might be a risk factor for these conditions(Reference van Lee, Quah and Saw22). Randomised controlled trials have shown that betaine plus S-adenosine-methionine is more beneficial than S-adenosine-methionine alone in treating depression(Reference Di Pierro, Orsi and Settembre36,Reference Di Pierro and Settembre37) . Differences in study populations, confounders included in the analyses, approaches for psychological status assessment and methods used to examine choline and betaine intakes can all account for these discrepancies among the findings of aforementioned studies.
The exact mechanisms for the protective role of choline and betaine in psychological disorders remain unclear; however, some potential pathways have been proposed. Prior studies introduced inflammation as a key element in developing depression(Reference Beurel, Toups and Nemeroff38–Reference Sorci and Faivre40). Choline acts as a precursor of acetylcholine, leading to a decrease in inflammation of neurons and an enhancement in cognitive function(Reference Fujii, Tsuchiya and Yamada41–Reference Sarter and Parikh43). Impaired cognition may make daily tasks challenging, which in turn can lead to anxiety symptoms(Reference Biringer, Mykletun and Dahl44). The different outcomes between betaine and choline in this study might be due to their different metabolic functions and their bioavailability. Choline might have a more direct impact on depression because of its role in neural signalling and membrane integrity(Reference Roy, Tomassoni and Nittari45). In contrast, betaine has primarily functioned as a methyl donor in the homocysteine–methionine cycle, which might have a less obvious or more indirect effect on psychological disorders(Reference Arumugam, Paal and Donohue46). The observed differences in their associations with depression might also be explained by the fact that dietary sources of choline could often provide higher accessible quantities than betaine. Despite the aforementioned mechanisms, the effects of choline and betaine on psychological health are still poorly understood. To elucidate the possible pathways by which they may impact psychological disorders, more human investigations with prospective designs are required.
The present study has several strengths. It is the first one that assessed the intake of choline and betaine in relation to common psychological disorders (depression, anxiety and distress) in a relatively representative sample of Iranian adults. Validated questionnaires were used to evaluate psychological disorders and dietary intakes, and several potential confounders were taken into account. Some limitations should be acknowledged when interpreting the results, as well. We should first acknowledge an inevitable phenomenon known as ‘reverse causality’ due to the cross-sectional nature of our study. Reverse causality refers to a situation in which the direction of the association is opposite to what is initially assumed. Individuals with anxiety, stress or depression may alter their dietary intakes as a result of their physiological disorders. Therefore, the association between dietary intakes and psychological disorders can be in both directions. Further studies with prospective designs, which could control the mentioned phenomenon more efficiently, are required to support our findings. Due to the limited sample size of the current study, we were not able to reconnoitre the relations in men v. women or normal-weight v. overweight/obese participants, separately. Furthermore, residual confounding might still remain even after controlling for numerous confounders. Although dietary intakes were evaluated using a validated FFQ, the results may be impacted by recall bias and in turn, lead to misclassification of participants. The applied FFQ also relied on the USDA database for choline and betaine due to the absence of a local equivalent, which might introduce some measurement errors, and its accuracy for choline and betaine in Iranian diets requires further validation. Additionally, supplement sources of choline and betaine were not assessed in this study, which may underestimate total intakes and limit our ability to account for their potential influence as confounders. In addition, although antidepressant usage was adjusted in the analyses, this confounder might still influence psychological disorders’ symptoms. Finally, despite covering a somewhat representative sample of Iranian adults, our study participants were school staff from Isfahan, which might not fully represent the general Iranian adult population, due to differences in occupation, education, socio-economic status and geographic location. The prevalence of depression, anxiety and psychological distress in this sample might also differ from national estimates, potentially reflecting occupational or regional factors. Future studies should include more diverse populations and a broader age range to enhance generalisability.
In conclusion, this study provides evidence for an inverse association between dietary choline intake and depression, while no significant relation was found in the case of anxiety and depression. Furthermore, findings failed to support a significant association between dietary betaine intake and odds of psychological disorders. These results imply that increasing consumption of dietary choline sources could be linked to lower odds of depression; however, as a cross-sectional study, causality cannot be inferred, and more prospective studies are required to confirm these findings and explore causality.
Acknowledgements
We wish to thank all participants who kindly participated in our study.
The financial support for conception, design, data analysis and manuscript drafting comes from Nutrition and Food Security Research Center, Isfahan University of Medical Sciences, Isfahan, Iran.
S. K., Z. M., F. S., Z. H., P. R. and P. S. contributed to conception, design, data collection, data interpretation, manuscript drafting, approval of the final version of the manuscript and agreed on all aspects of the work.
None of the authors had any financial or non-financial conflicts of interest.