


Introduction
Patient death has a profound impact on healthcare professionals. Far from being absorbed as a routine aspect of clinical practice, the death of a patient, especially when by suicide, often exerts lasting effects on clinicians’ emotional well-being, clinical confidence and career trajectories, with consequences that may persist for years. Reference Linke, Wojciak and Day1–Reference McAnee, Norwood and Leavey3 Deaths of patients, whether expected or not, can leave clinicians with enduring grief, helplessness and anxiety that may affect both their personal well-being and professional practice. Reference Kostka, Borodzicz and Krzemińska4,Reference Akyol, Celik, Koc, Bayindir, Gocer and Karakurt5
Within this broader picture, patient suicide has emerged in research as a qualitatively different experience that carries a particularly significant toll for clinicians. Beyond grief, clinicians often describe guilt, incompetence, shame, anger and post-traumatic symptoms following patient suicides, Reference Leaune, Allali, Rotgé, Simon, Vieux and Fossati6,Reference Rajagopalan, Teck and Sng7 to the point that clinicians have been called ‘suicide survivors’ Reference Farberow8 or ‘second victims’. Reference Wu9 Surveys consistently show that around two-thirds of the clinical workforce will experience a patient suicide during their career, with many reporting moderate to severe psychological distress. Reference Sandford, Kirtley, Thwaites and OConnor2,Reference Gibbons, Brand, Carbonnier, Croft, Lascelles and Wolfart10 Organisational responses, including formal investigations and attending coroner’s court, can amplify clinicians’ emotional strain. Reference Campbell and Hale11 These experiences are not isolated: they ripple outwards, influencing clinical practice through defensive decision-making, increased risk aversion and even career change. Reference Sandford, Kirtley, Thwaites and OConnor2,Reference Croft, Lascelles, Brand, Carbonnier, Gibbons and Wolfart12 Such defensive responses are often shaped by a wider culture of blame and fear of litigation. Reference Sandford, Kirtley, Thwaites and OConnor13
Despite clinicians’ substantial need for support following patient death, especially suicide, supportive interventions often face persistent challenges at both the development and implementation levels. A key barrier in developing postvention support is the wide variation in how clinicians define adequate support, Reference Jupina, Mercer, Weleff, Hackett, Nunes and Sebastian14 making it hard to design interventions that work for everyone. Organisational barriers may further hinder the effective delivery of support and, even when resources are available, these are often underutilised. Reference Erlich, Rolin, Dixon, Adler, Oslin and Levine15–Reference Tsai, Moran, Shoemaker and Bradley17 This highlights ongoing gaps in both the design and delivery of postvention support.
Although all patient deaths can have profound effects on clinicians, it remains unclear how the impact of suicides differs from that of other deaths. Is the trauma of suicide fundamentally distinct, with a stronger impact, or are the emotional, professional and organisational consequences of suicidal and non-suicidal deaths more similar than assumed? In this mixed-methods study, integrating both quantitative and qualitative approaches, we aimed to investigate the impact of patient suicide compared with patient death on clinicians’ psychological well-being, clinical practice and career. Additionally, we sought to explore clinicians’ perspectives on how the current systems of support do, or do not, meet their needs.
Method
Design
A web-based survey was developed using Qualtrics and adapted from previous research. Reference Gibbons, Brand, Carbonnier, Croft, Lascelles and Wolfart10,Reference Wolfart18 Participants were presented with full study information as part of the digital informed consent process. The informed consent stated that participation was entirely voluntary. Digital consent was obtained via a checkbox prior to beginning the survey. In line with the Health Research Authority (HRA) tool, HRA approval was not required. The project was approved in accordance with the local Trust guidelines for staff surveys, and was reviewed by the medical director and internal communication team prior to distribution.
The survey consisted of two sections with a similar structure: one focused on suicidal patient deaths and the other on non-suicidal patient deaths. Each section began with a screening question asking whether the clinician had experienced a patient death of the specified type. If the respondent answered ‘yes’, they were directed to a corresponding set of questions. In both sections, participants were asked to focus on the incident that had the most significant impact on them. They responded to questions regarding the effect of the incident on their psychological well-being and clinical practice, what they found helpful or unhelpful in the aftermath and suggestions for potentially helpful support strategies and interventions. In addition, the suicide-related section included questions exploring clinicians’ views on (a) the predictability of suicides in secondary care, (b) experiences of external pressure to prevent suicides and (c) their perceived role in suicide prevention. For the layout of the questions, see Appendix 1 (found in the Supplementary material available at https://doi.org/10.1192/bjo.2026.12032). A mixed-methods design was used. Quantitative and qualitative data were collected simultaneously and integrated at the interpretation stage, allowing qualitative themes to contextualise and explain quantitative findings from a personal experiential perspective, consistent with Good Reporting of a Mixed Methods Study reporting guidelines. Reference Ocathain, Murphy and Nicholl19
Participants
The survey was distributed via the medical directors to clinicians working within South London and Maudsley NHS Foundation Trust (SLaM), including psychiatrists, nurses, psychologists, occupational therapists, social workers and support workers. SLaM provides a wide range of mental health services serving a local population of 1.3 million people in south London, as well as delivering national specialist services for adults and children. Responses were collected between July and August 2024 (1 month), with follow-up email reminders sent weekly. All data were collected anonymously, with no identifiable information collected. Information on support resources was provided to participants in the invitation email.
Quantitative data analysis
Mixed-effects regression models were used to examine the association between incident type (suicidal versus non-suicidal patient death) and various clinician outcomes. Mixed models were used because these enable the use of all available data and can handle missing data more appropriately. Reference Gueorguieva and Krystal20 Incident type was included as a fixed effect, and respondent identity was specified as a random intercept to account for individual-level variability through repeated measures. Respondents were asked to rate the effect of the incident on their emotional well-being, on a Likert scale, as either ‘0, no effect’, ‘1, mild’, ‘2, moderate’ or ‘3, severe effect’. They also rated their perceived responsibility at the time of the incident on a scale from 0 (‘not responsible’) to 4 (‘very responsible’). For outcomes measured on an ordinal scale, such as emotional impact and perceived responsibility, cumulative-link mixed-effects models (CLMMs) were fitted using the Laplace approximation. Separate models were conducted to examine the association of gender with the emotional impact of each incident type. A similar CLMM was applied to examine clinicians’ familiarity with procedures following the two types of patient death. For binary outcomes, such as whether the incident had influenced career choices or whether the clinician felt the need for support following the incident, binomial generalised linear mixed-effects models (GLMMs) with a logit link were used, with incident type as a fixed effect and respondent identity as a random intercept. All statistical analyses were conducted in R version 4.5.0 for Windows (R Foundation for Statistical Computing, Vienna, Austria; see https://www.r-project.org/). CLMMs were fitted using the clmm() function from the ordinal package (https://CRAN.R-project.org/package=ordinal), and GLMMs were fitted using the lme4 package (https://doi.org/10.18637/jss.v067.i01).
Thematic analysis
Text responses were analysed using thematic analysis following Braun and Clarke’s six-phase framework. Reference Braun and Clarke21 Codes were extracted from the whole corpus of free-text responses for both suicide and non-suicide free-text data-sets. Subthemes and themes were then built from patterns across the entirety of each data-set. Two overarching themes were identified across both data-sets: Individual Responses and Organisational Responses. Subthemes within Individual Responses included emotional responses, sense of responsibility and impact on work and career choices. Subthemes within Organisational Responses included blame, supervision, support and investigational processes.
Subthemes were generated separately for suicide and non-suicide data-sets, which enabled interpretive comparisons aiming to identify patterns of convergence and divergence between suicide and non-suicide death responses. This is consistent with Braun and Clarke’s recognition that thematic analysis can highlight similarities and differences across a data-set Reference Braun and Clarke21 . To ensure adherence to an inductive approach and minimise the influence of prior assumptions on the data, reflexivity was practised through peer debriefing sessions between the first and third authors, to examine prior assumptions and identify potential pre-existing biases. Equal attention was given to responses reflecting less severe experiences alongside more prominent accounts.
Results
The survey was distributed to approximately 500 clinicians, of whom 122 responded (≈25% response rate). Respondent characteristics are presented in Table 1. Of the 122 respondents, 83 (68%) reported having experienced at least 1 patient suicide and 71 (58%) had experienced at least 1 non-suicidal patient death. Notably, 53 clinicians (44%) had experienced both suicidal and non-suicidal patient death, enabling within-subject comparisons to account for individual-level differences. Of the 83 respondents who had experienced patient suicide, 59 (71%) had experienced more than one. Similarly, of the 71 respondents who had experienced non-suicidal patient death, 60 (85%) had experienced more than one. The majority (80%) of respondents who had experienced suicidal patient death and 59% of those who had experienced non-suicidal patient death reported that the incident occurred in general adult services, suggesting a potentially higher prevalence of both incident types in general adult services compared with other services.
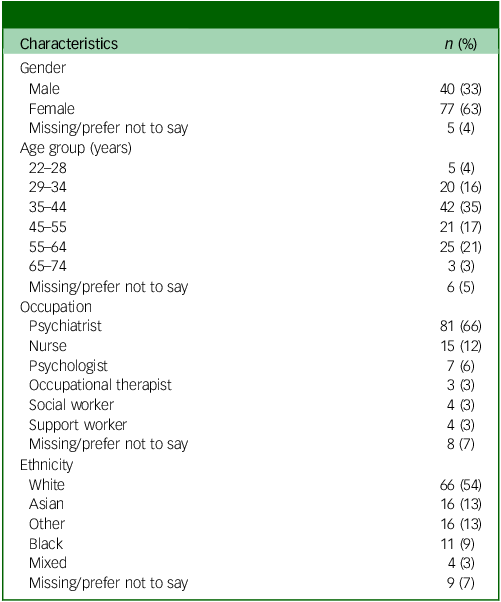
Characteristics of responding clinicians (N = 122)

Table 1 Long description
The table presents the characteristics of 122 responding clinicians. It includes data on gender, age group, occupation, and ethnicity. The gender distribution shows 40 males (33%), 77 females (63%), and 5 individuals who preferred not to say (4%). Age groups are categorized into 22-28 years (5%), 29-34 years (16%), 35-44 years (35%), 45-55 years (17%), 55-64 years (21%), 65-74 years (3%), and 6 who preferred not to say (5%). Occupations listed include psychiatrist (66%), nurse (12%), psychologist (6%), occupational therapist (3%), social worker (3%), support worker (3%), and 8 who preferred not to say (7%). Ethnicity data shows 66 white clinicians (54%), 16 Asian (13%), 16 other (13%), 11 black (9%), 4 mixed (3%), and 9 who preferred not to say (7%).
Effects on emotional well-being
Of the 83 respondents who had experienced patient suicide, 53% reported a moderate impact and 12% a severe impact. In contrast, of the 71 respondents who had experienced non-suicidal patient death, 36.6% reported a moderate impact and 4.2% a severe impact. Non-suicidal patient death was associated with significantly lower emotional impact compared with patient suicide (odds ratio 0.14, 95% CI [0.05, 0.41], z = −3.60, p < 0.001), indicating a stronger emotional effect of suicide on clinicians.
Following non-suicidal patient death, no clinicians thought their symptoms had met the clinical threshold for a psychiatric diagnosis, and none had taken sick or annual leave. In contrast, following patient suicide, six clinicians (7%) thought their symptoms had met the diagnostic threshold and five (6%) had taken leave. Gender was a significant predictor of emotional impact following both non-suicidal (odds ratio 0.23, 95% CI [0.08, 0.66], z = −2.73, p = 0.006) and suicidal patient death (odds ratio 0.31, 95% CI [0.11, 0.84], z = −2.27, p = 0.023) models, with males reporting lower emotional impact in both contexts. Additionally, participation in resuscitation following non-suicidal patient death was a significant predictor of emotional impact (odds ratio 2.32, 95% CI [1.10, 4.88], z = 2.20, p = 0.028), with those involved in resuscitation around twice as likely to report higher emotional impact.
Clinicians were asked to describe, in their own words, the emotional responses they had experienced (see Appendix 2 for word cloud visualisations of the codes). Following patient suicide, guilt and blame were particularly prominent in shaping the wide range of emotional responses, including sadness, fear/anxiety, shock, anger, feelings of incompetence, shame and post-traumatic stress symptoms:
‘Could I have done more? Should I have pushed harder for more restrictive options?’
Accounts frequently reflected a sense of failure and hopelessness, sometimes expressed as inevitability:
‘We knew he was going to kill himself. But there was nothing we could do to stop it. It was like watching a car crash in slow motion.’
Other clinicians noted the wider culture of blame:
‘Suicides are seen as failures… We don’t blame oncologists when their patients die of cancer – why do we blame psychiatrists when their treatment-resistant, severely ill patients take their lives?’
Additional emotions following suicide included irritability, distractibility, flashbacks, hypervigilance, resignation, isolation, regret, sleep disturbance and ongoing anxiety about future patients:
‘I feel like I need to try and be aware of things at all times if possible (which I know is unrealistic).’
In contrast, non-suicidal deaths were more often associated with sadness, shock, guilt, helplessness, numbness, confusion and internal self-questioning:
‘Have we done everything? Numbness, shock, sadness, am I in trouble?’
Although both types of death elicited distress, clinicians’ responses to suicide more consistently emphasised guilt and the experience of being blamed by others, whereas responses to non-suicidal deaths centred on grief and uncertainty about preventability. Notably, a subtheme of no or mild emotional impact emerged inductively from the non-suicide free-text responses; despite active searching, no comparable subtheme was identified within the suicide responses.
Perceived responsibility for the incident
Non-suicidal patient death was associated with significantly lower perceived responsibility at the time of the incident compared with patient suicide (odds ratio 0.31, 95% CI [0.15, 0.68], z = −2.95, p = 0.003).
In the text responses, feelings of responsibility emerged in both types of death but were expressed differently. Following non-suicidal deaths, clinicians occasionally described direct responsibility, questioning whether clinical decisions such as prescribing may have contributed to the outcome:
‘Was it the medication I prescribed? Should I have done anything different?’
By contrast, following patient suicide, clinicians described a broader and heavier sense of responsibility. This included direct responsibility, fears that something they had said or done might have precipitated the act, as well as indirect responsibility, involving concerns that their actions or omissions had influenced the overall quality of care and, in turn, contributed to the suicide. As one clinician reflected:
‘I wondered if my review had somehow triggered him to do it because I had expressed concern about his mental state and referred him to HTT, I thought this might have made him feel hopeless. We had also discussed admission and again I worried this might have made him feel worse.’
Another wrote:
‘That I could (and should) have done more and that if I had done my job properly things would have been different.’
Effect on career choices
Of the 83 respondents who had experienced patient suicide, 12 reported that it had influenced their career choices compared with 8 out of 71 respondents who had experienced a non-suicidal patient death. There was a trend towards clinicians being less likely to report an impact on their career choices following non-suicidal patient death compared with suicide, although this effect did not reach conventional significance (odds ratio 0.03, 95% CI [0.0006, 1.07], z = −1.92, p = 0.055). This suggests a potential influence of the type of patient death on clinicians’ career trajectories.
In text responses, clinicians described avoiding high-risk clinical settings, such as acute or crisis care, in-patient units and general adult posts, and expressed a preference for roles within older adult services. In contrast, following non-suicidal patient death, some clinicians reported avoiding in-patient posts.
Effect on clinical practice
Clinicians were asked to describe how each type of incident had influenced their clinical practice, and reported that both patient suicide and non-suicidal death had led to doubt about clinical decisions, feelings of incompetence, greater risk aversion, avoidance of high-risk cases and consideration of leaving clinical work. Following suicide, these effects were more pronounced and often included persistent rumination, shame, heightened anxiety in clinical settings and a shift from therapeutic engagement towards risk management:
‘I focus too much on risk as the system won’t support me if I get it “wrong” – and not enough in being therapeutic for the patient.’
‘I would rather not work in a speciality where we are expected to take responsibility for others’ decisions.’
‘I will stop NHS practice – I fear the system will throw me under the bus if this happens again – again, even though I know it isn’t my fault. Life is too short to live under this cloud.’
The need for post-incident support
Clinicians were less likely to report needing support following non-suicidal patient death compared with patient suicide (odds ratio 0.35, 95% CI [0.13, 0.91], z = −2.51, p = 0.012). The odds of reporting a need for support were approximately 65% lower following non-suicidal deaths compared with suicides, suggesting greater perceived support needs in response to suicide-related incidents.
Factors that influenced clinicians’ experiences following the deaths
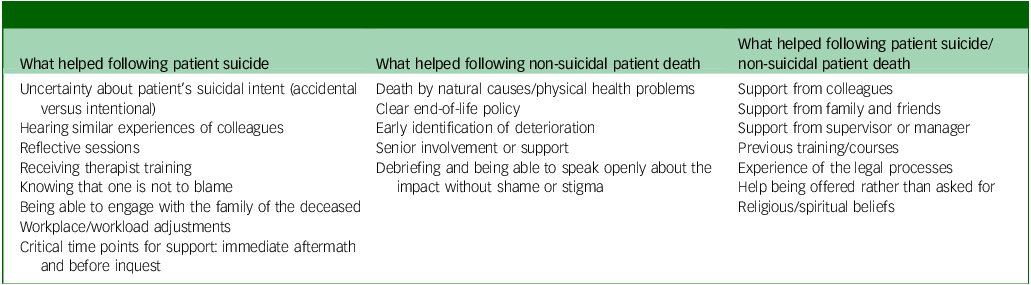
Clinicians were asked to give a free-text response about the people, interventions and experiences that either helped or did not help them in the aftermath of the death. The themes identified are shown in Tables 2 and 3, and the free-text responses that followed. Peer support, family and friends were most often valued in both contexts. Following suicide, medical defence organisations were also cited, whereas morbidity and mortality meetings were cited following non-suicidal deaths:
What helped following suicidal and non-suicidal patient death

Table 2 Long description
The table presents a comparison of factors that helped clinicians following either suicidal or non-suicidal patient deaths. It consists of two columns and multiple rows. The first column lists factors that helped after a patient suicide, including support from colleagues, family and friends, supervisors or managers, previous training, legal process experience, religious or spiritual beliefs, uncertainty about the patient’s suicidal intent, hearing similar experiences from colleagues, reflective sessions, therapist training, knowing one is not to blame, engaging with the family of the deceased, and workplace adjustments. The second column lists factors that helped after a non-suicidal patient death, including death by natural causes, clear end-of-life policies, early identification of deterioration, senior involvement or support, and debriefing without shame or stigma. Critical time points for support are also noted, such as immediate aftermath and before inquest for suicides.
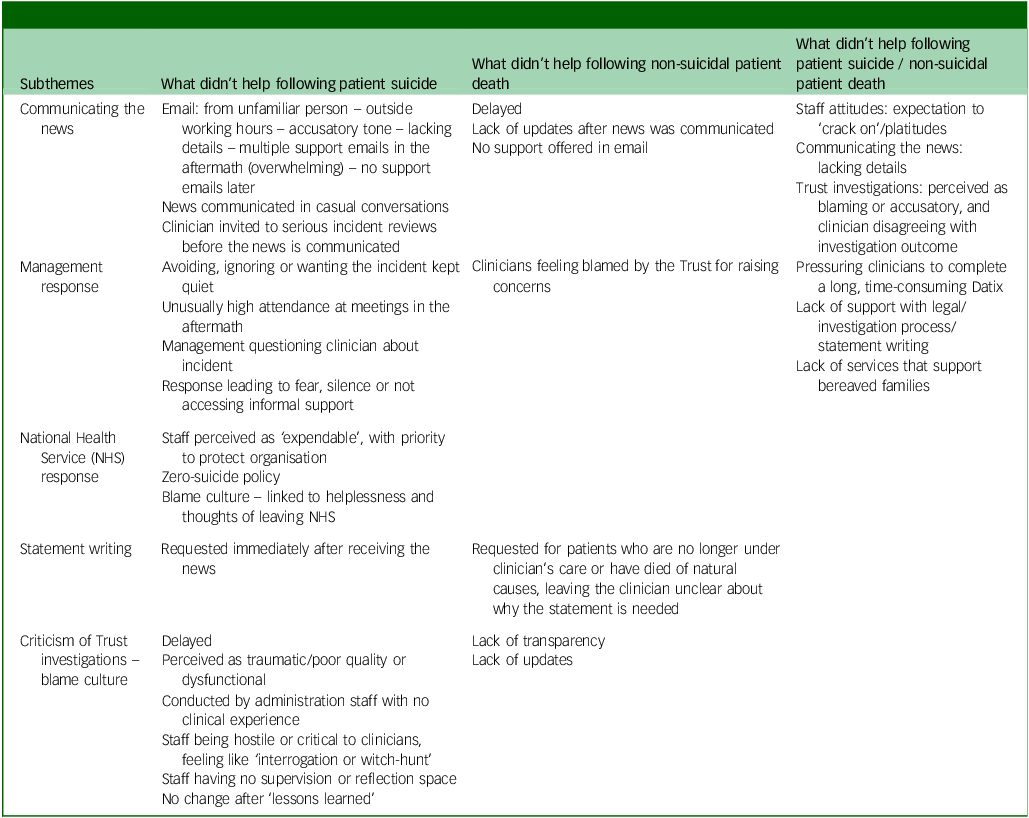
What didn’t help following suicidal and non-suicidal patient death

Table 3 Long description
The table presents a comparison of factors that did not help clinicians following suicidal and non-suicidal patient deaths. It is divided into three main columns: subthemes, what didn’t help following patient suicide, and what didn’t help following non-suicidal patient death. The table has multiple rows, each detailing specific issues such as staff attitudes, communicating the news, trust investigations, lack of support, management response, NHS response, statement writing, and criticism of trust. Each row lists the specific problems encountered in both suicidal and non-suicidal patient death scenarios. For example, staff attitudes included expectations to ‘crack on’ or platitudes, and communicating the news lacked details. Trust investigations were perceived as blaming or accusatory. The table highlights the lack of support with legal and investigation processes and the absence of services for bereaved families. Management responses included avoiding or ignoring the incident, and the NHS response often led to fear or silence. Statement writing was requested immediately after receiving the news, and criticism of trust was delayed and perceived as traumatic. The table provides a comprehensive overview of the challenges faced by clinicians in different contexts.
‘Talking to peers who had been through the process, honest discussion with supervisors/seniors, trusted seniors, about learning from event, talking through practicalities of what legal processes would be by someone with knowledge of it, step by step.’
‘Some support and underrating around the SI before I had to go through one. Feeling backed and reassured by perhaps someone who has been through it. To be honest I wanted an advocate of sorts, someone who reviewed the work outside the panel and said what I did was OK, perhaps my manager should have done this? The panel felt out for blood.’
‘Knowing I wasn’t to blame helps, and that it is the system and the “blame culture” of the NHS (and society as a whole) that is the issue. I can’t fight this, so I choose to do something else – leave NHS work and high-risk patients. I’ve done my bit – someone else can now live with the constant fear of adverse events.’
‘It felt it was all about what we could have done differently, and lessons learnt.’
‘The NHS response. Staff are expendable, cogs in a wheel. Protect the organisation is the number one concern. Denial of the reality – that very sick people die, and it isn’t your fault – and instead asking what went wrong.’
‘I found the trust’s internal serious incident process much less helpful, and felt in some way blamed by this (something which I was surprised not to be the case at the coroner’s court, even with the family present).’
‘Media interest which suggests you have been involved in some kind of crime.’
Support needed following a patient suicide
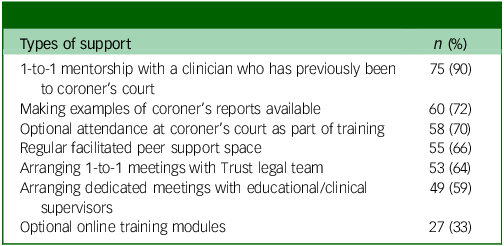
In this question, respondents were allowed to select multiple options. The seven most commonly chosen responses are presented in Table 4.
Support needed following a patient suicide (N = 83)

Table 4 Long description
A table titled ‘Support needed following a patient suicide’ with 7 rows and 2 columns. The table lists the most commonly chosen responses by respondents, who were allowed to select multiple options. The columns are labeled with the support options and the corresponding number and percentage of respondents who chose each option. The first row indicates that 75 respondents (90 percent) chose 1-to-1 mentorship with a clinician who has previously been to coroner’s court. The second row shows that 60 respondents (72 percent) chose making examples of coroner’s reports available. The third row indicates that 58 respondents (70 percent) chose optional attendance at coroner’s court as part of training. The fourth row shows that 55 respondents (66 percent) chose regular facilitated peer support space. The fifth row indicates that 53 respondents (64 percent) chose arranging 1-to-1 meetings with Trust legal team. The sixth row shows that 49 respondents (59 percent) chose arranging dedicated meetings with educational or clinical supervisors. The seventh row indicates that 27 respondents (33 percent) chose optional online training modules.
Familiarity with the post-incident process:
Clinicians were asked to rate their familiarity with the procedures following patient suicide or non-suicidal death. Among those who had experienced a patient suicide (N = 83), 27% reported being not at all familiar, 16% slightly familiar, 13% moderately familiar and 18% very familiar. In comparison, among those who had experienced a non-suicidal patient death (N = 71), 20% were not at all familiar, 18% slightly familiar, 23% moderately familiar and 25% very familiar. Clinicians were significantly (2.66 times) more familiar with procedures following non-suicidal deaths compared with patient suicides (odds ratio 2.66, 95% CI [1.08, 6.56], z = 2.14, p = 0.032).
Suicide-specific questions
We asked clinicians to rate the degree to which they felt that prevention of suicide was their role, on a Likert scale ranging from 0 (‘not at all’) to 5 (‘completely believe’). The majority (n = 57, 64%) selected a rating of 2 or 3, indicating a moderate sense of responsibility, with a mean score of 2.7 across 90 responses.
To assess perceived external pressure, clinicians were asked how much pressure they felt from external sources to prevent patient suicide, using a similar Likert scale ranging from 0 (‘no pressure’) to 5 (‘extreme pressure’). Almost two-thirds of respondents (n = 61, 69%) rated their response as 4 or 5, suggesting high levels of perceived external pressure, with a mean score of 3.7.
To explore clinicians’ views on the predictability and preventability of suicide, we asked them to rate how predictable they believed suicide is in secondary care, using a Likert scale from 0 (‘absolutely unpredictable’) to 5 (‘absolutely predictable’). Among 86 responses, the mean score for perceived predictability of suicide in secondary care was 1.9 out of 5. A total of 84 respondents (98%) rated predictability as 3 or below, and 58 respondents (68%) rated it as 2 or below, indicating a general perception of suicide as less than moderately predictable. To examine whether prior exposure to patient suicide had influenced clinicians’ views on its predictability, a Mann–Whitney U-test indicated no statistically significant difference in perceived predictability of suicide between those who had experienced a patient suicide and those who had not (U = 942.5, p = 0.159), suggesting a possibly broader view than one shaped by direct personal experience. In their text responses, clinicians identified several factors contributing to the unpredictability of suicide. These included patients masking their symptoms, being difficult to engage and the complexity and ambiguity of the diagnoses. Additionally, the threshold for detention under the Mental Health Act was noted as a challenge, because some patients may comply barely sufficiently to avoid crossing that threshold.
Additionally, we asked clinicians to rate how much they believed that the zero-suicide policy is achievable for patients under treatment, on a similar Likert scale from 0 (‘unachievable’) to 5 (‘achievable’). The mean score from 86 responses was 0.7 out of 5, with 59 (69%) selecting 0, reflecting a belief that the policy is unachievable.
Sensitivity analysis: subgroup analysis
To assess the robustness of the main model findings, direct paired comparisons were conducted in the subgroup of clinicians who had experienced both suicide and non-suicide patient deaths (n = 53). Wilcoxon signed-rank tests results were consistent with the main analysis: compared with non-suicide patient death, suicide was associated with significantly greater emotional well-being impact (W = 316.5, z = 3.581, p < 0.001, r = 0.803), greater sense of responsibility at the time of the incident (W = 284.0, z = 3.269, p < 0.001, r = 0.748), greater sense of responsibility with hindsight (W = 177.5, z = 2.707, p = 0.006, r = 0.690) and reduced familiarity with post-incident processes (W = 32.0, z = −2.330, p = 0.017, r = −0.626), confirming the main findings.
Discussion
Summary of the study and main findings
This mixed-methods study provides rare comparative evidence on the impact on clinicians of patient suicide versus non-suicidal patient death. Although both types of patient death were shown to affect clinicians’ well-being and practice, our findings demonstrate that suicide carries a heavier and more complex burden. Two-thirds of clinicians in our sample had experienced a patient suicide, with 65% reporting moderate to severe emotional effects compared with 41% for non-suicidal deaths. Integration of these findings with qualitative data revealed that suicide was prominently associated with heightened feelings of guilt and blame, greater disruption to clinical practice and increased consideration of career change. These findings align with a growing body of literature about the impact of patient suicide on clinicians, Reference Sandford, Kirtley, Thwaites and OConnor2,Reference Leaune, Allali, Rotgé, Simon, Vieux and Fossati6,Reference Rajagopalan, Teck and Sng7 and confirm that it represents not only a personal loss but also a distinct occupational trauma, shaped by both individual emotional responses and organisational cultures of blame.
Blame emerged as a key factor in shaping clinicians’ emotional and professional responses to patient death. Following suicide, clinicians often reported a powerful sense of external blame, by families, organisations and wider societal narratives of ‘blame culture’, combined with an internalised conviction that they themselves had failed. By contrast, non-suicidal deaths more commonly elicited self-questioning about clinical decisions or blame directed towards colleagues. This distinction resonates with recent psychodynamic accounts of suicide bereavement, which show how suicide unleashes intense guilt and delusional narratives of blame that place survivors, including clinicians, at the centre of responsibility for the death. Reference Gibbons22 Such narratives can become tormenting and obstruct the mourning process, while also permeating organisational and societal responses. Within healthcare, this manifests in a pervasive ‘blame and shame’ environment that heightens distress and obstructs learning. Reference Ng, Merry, Paterson and Merry23,Reference Ramsey, Sheard, Waring, McHugh, Simms-Ellis and Louch24 Many clinicians in our survey described feelings of personal failure and systemic abandonment. This burden is often intensified by organisational responses perceived as accusatory or lacking empathy, echoing findings from Sandford et al. Reference Sandford, Kirtley, Thwaites and OConnor13 This burden is compounded by the ideological weight of zero-suicide frameworks which, however well intentioned, frame every death as a preventable failure. As argued elsewhere, Reference Gibbons25 this constitutes a form of moral injury: clinicians are held to an impossibly certain standard in a domain defined by irreducible uncertainty. The implicit promise that suicide can be eliminated if professionals act correctly transforms grief into culpability, and uncertainty into negligence. Formal investigations are frequently experienced as punitive and protective of institutional interests, amplifying clinicians’ fear and reputational anxiety. Media coverage further entrenches these dynamics by assigning fault to individuals or services rather than addressing systemic issues. Reference Li, Morway, Velasquez, Weingart and Stuver26 Together, these forces contribute to defensive clinical practices that compromise therapeutic engagement and care quality. Reference Lorenc, Khouja, Harden, Fulbright and Thomas27
Notably, clinicians described a shift towards defensive practice, heightened anxiety and a diminished sense of therapeutic engagement. Our results support earlier research showing that patient suicide can lead to career changes and avoidance of high-risk clinical settings. Reference Croft, Lascelles, Brand, Carbonnier, Gibbons and Wolfart12,Reference Erlich, Rolin, Dixon, Adler, Oslin and Levine15 Defensive clinical practices, such as over-documentation, risk-averse decision-making and avoidance of high-risk patients, frequently arise in response to this culture of blame and fear of litigation. Reference Sandford, Kirtley, Thwaites and OConnor13,Reference Eftekhari, Parsapoor, Ahmadi, Yavari, Larijani and Gooshki28 A recent systematic review highlights that such practices are driven not only by legal concerns but also by clinicians’ feelings of mistrust and disempowerment within their organisations. Reference Lorenc, Khouja, Harden, Fulbright and Thomas27 These findings reinforce the need for a cultural shift towards supportive, learning-focused responses to patient death, particularly suicide, to reduce harm and support clinician well-being.
Furthermore, clinicians reported feeling less familiar with post-suicide procedures and expressed a stronger need for support, particularly in the form of legal guidance and peer mentorship. Support strategies face barriers at both the development and uptake levels, as noted in previous studies. Reference McAnee, Norwood and Leavey3,Reference Simms-Ellis, Harrison, Sattar, Sweeting, Hartley and Morys-Edge16,Reference Tsai, Moran, Shoemaker and Bradley17 Exploring the mismatch between clinicians’ support needs and the resources provided, many respondents called for more proactive, personalised and legally informed support systems. This underscores the need for more clinician-centred policies that foster supportive environments, improve postvention protocols and encourage and normalise open dialogue about the emotional impact of patient suicide.
The low-risk paradox and the challenge of predictability
A particularly salient theme emerging from this study is the ‘low-risk paradox’ of suicide. Despite rigorous risk assessments and clinical vigilance, suicide often occurs in patients deemed low risk. Reference Berman29–Reference Windfuhr and Kapur31 In our study, clinicians described how this unpredictability undermined their confidence in professional judgement and contributed to feelings of helplessness and guilt. Nearly all respondents (98%) rated suicide in secondary care as less than 60% predictable, reflecting widespread concern about the limitations of current risk assessment tools and highlighting the need for more nuanced approaches to suicide prevention.
This paradox also has significant policy implications, particularly for the zero-suicide policy. In our study, 69% of respondents rated the policy as unachievable, raising concerns that it sets unrealistic expectations and fosters a culture of blame when suicides inevitably occur. This disconnect between policy and clinical reality may contribute to burnout, defensive practice and attrition from high-risk roles.
Limitations
Although the study offers valuable insights, several limitations must be acknowledged. First, the use of an online survey introduces the possibility of response bias whereby the most severely affected clinicians may have been more motivated to respond. However, even with response bias considered, our findings still provide important insights into the experiences of clinicians most severely affected by patient death, and can inform the development of targeted support strategies for this group. An aim for future research could be to incorporate strategies to assess potential differences between respondents and non-respondents to further clarify the generalisability of findings. Although our response rate was ≈25%, low response rates are common in surveys of healthcare professionals, and previous studies indicate that even samples with <30% response rates can provide meaningful insights, particularly when exploring experiences of high-stress events. Reference Lang32,Reference Rimmer33 Second, the reliance on self-reported data introduces the possibility of recall bias and social desirability effects. Clinicians may have under- or over-reported their emotional responses due to stigma or professional expectations. Third, the sample was drawn from a single NHS trust, which may have limited the generalisability of the findings to other regions or healthcare systems. Fourth, due to practical constraints, the order of the survey blocks (suicide/non-suicide) could not be randomised across respondents, which may have introduced order effects. Additionally, the predominance of female clinicians (63%) limits the generalisability of gender difference analyses. Last, within our sample the reported emotional impact and sense of responsibility did not significantly differ between in-patient and community settings in which the death occurred, suggesting a similarity of impact regardless of care setting. However, these findings are considered exploratory given the small subgroup sizes and cannot be readily generalised.
To conclude, this study underscores the profound and multifaceted impact of patient suicide on healthcare professionals. The emotional toll, professional disruption and systemic challenges described by clinicians highlight the urgent need for more compassionate, informed and responsive support systems. The low-risk paradox and the perceived unachievability of zero-suicide policies call for a re-evaluation of current approaches to suicide prevention. By acknowledging the limits of predictability and focusing on clinician support, healthcare systems can better navigate the complex impact of patient suicide and foster a more resilient workforce.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.12032
Data availability
The data that support the findings of this study are available from the corresponding author, R.C., upon reasonable request and in accordance with local Trust guidelines.
Author contributions
K.M.M.: conceptualisation, survey design, data collection, data analysis (both quantitative and qualitative), writing of the first draft and revision of manuscript R.G.: survey design, qualitative analysis supervision, writing of the first draft and revision of manuscript R.C.: conceptualisation, survey design, qualitative analysis, writing of the first draft and revision of manuscript, project management and supervision.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.



 Open access
Open access
eLetters
No eLetters have been published for this article.