


Highlights
-
Moyamoya disease (MMD) can present without the “puff-of-smoke” collaterals (smokeless), resembling moyamoya syndrome.
-
Genetic testing for RNF 213 assists in identifying the smokeless MMD variant and directs treatment.
-
Structural modeling shows variant-specific RNF213 disruptions that impair angiogenesis, highlighting its role in “smokeless” MMD expression.
Background
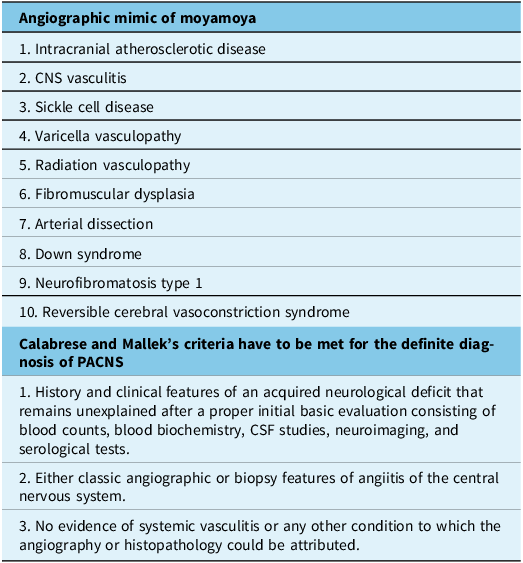
Moyamoya disease (MMD) is an idiopathic, sometimes familial condition characterized by progressive steno-occlusion of the distal internal carotid arteries (ICAs) and circle of Willis, often involving the carotid fork (distal to the anterior choroidal arteries). Reference Kuroda, Fujimura and Takahashi1 Its hallmark is a network of basal collaterals resembling a “puff-of-smoke” on angiography, as described by Suzuki and Takaku in 1969 based on 20 cases. The Suzuki staging system (I–VI), derived from serial angiograms of four young patients, remains a cornerstone of MMD classification. Reference Suzuki and Takaku2 Conditions mimicking MMD, collectively termed moyamoya syndrome (MMS) or quasi-moyamoya, include central nervous system vasculitis, intracranial atherosclerosis, sickle cell disease and varicella zoster vasculitis (Table 1). Reference Gonzalez, Amin-Hanjani and Bang3
Illustrates the angiographic mimics of moyamoya and demonstrates the diagnostic criteria of primary angiitis of the central nervous system (PACNS)

Table 1 Long description
A table listing angiographic mimics of moyamoya and diagnostic criteria for PACNS. The table has two sections. The first section lists ten angiographic mimics of moyamoya: intracranial atherosclerotic disease, CNS vasculitis, sickle cell disease, varicella vasculopathy, radiation vasculopathy, fibromuscular dysplasia, arterial dissection, Down syndrome, neurofibromatosis type 1, and reversible cerebral vasoconstriction syndrome. The second section outlines Calabrese and Mallek's criteria for the definite diagnosis of PACNS, which include a history and clinical features of an acquired neurological deficit that remains unexplained after a proper initial basic evaluation, either classic angiographic or biopsy features of angiitis of the central nervous system, and no evidence of systemic vasculitis or any other condition to which the angiography or histopathology could be attributed.
In patients presenting with steno-occlusive changes at the carotid fork but lacking the characteristic “puff-of-smoke” collaterals, there is a tendency to pursue extensive investigations and initiate empirical treatments for MMS. This approach may lead to unnecessary or even harmful interventions. Recognizing that such presentations can still represent MMD, particularly in the presence of RNF213 gene mutations, underscores the importance of incorporating genetic testing into the diagnostic process. Early identification through genetic studies can prevent misdiagnosis, reduce unwarranted treatments and facilitate appropriate management strategies.
We have identified a subset of patients exhibiting unilateral or bilateral, often asymmetric, steno-occlusive changes at the carotid fork without the hallmark “puff-of-smoke” angiographic collaterals. This absence frequently leads to diagnostic ambiguity, prompting extensive investigations and empirical treatments for MMS, which may be unnecessary or even detrimental. Notably, clinical exome sequencing targeting the RNF213 gene has clarified these diagnostic challenges, aligning with cases such as that reported by Morikawa et al., where a 40-year-old Chinese woman was initially misdiagnosed with primary angiitis of the central nervous system (PACNS) but was later correctly identified as having MMD with the p.R4810K variant and subsequently improved following revascularization. Reference Morikawa, Suzuki, Nakai, Takasu, Itoh and Ito4 To better characterize this distinct clinical entity, we propose the term “smokeless moyamoya,” acknowledging its divergence from classic MMD presentations. In this study, we detail the clinical, radiological and genetic profiles of these patients, assess their treatment outcomes and explore the structural implications of RNF213 variants to elucidate the molecular underpinnings of this phenotype.
Methods
Ethics statement
This study adhered to the Declaration of Helsinki principles. All participants, or a parent/guardian for minors, provided written informed consent. The Institutional Ethics Committee approved the study with reference number INK/COP/FM/05. Additionally, participants consented to genetic analysis per the Indian Council of Medical Research ethical guidelines (2017, section 10.4.5) .
Study design and selection of participants
We conducted an ambispective observational study at our institute from March 2021 to January 2025, screening all stroke unit patients with ischemic stroke or atypical intracerebral hemorrhage (with or without intraventricular extension). Participants were selected based on (1) carotid fork narrowing or irregularities on CT/MR angiography, (2) negative systemic vasculitis screening, (3) no sickle cell anemia or infections (varicella zoster, HIV, hepatitis B/C, syphilis), (4) normal CSF analysis, (5) absence of “puff-of-smoke” collaterals on digital subtraction angiography (DSA) and (6) presence of RNF213 missense variants. Selected patients were prospectively followed for treatment and outcomes (Figure 1). Those with compound heterozygous RNF213 variants were excluded. The study’s reporting system followed the STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology) Reference von Elm, Altman, Egger, Pocock, Gøtzsche and Vandenbroucke5 (Supplementary file).
Flow chart of the study participants’ selection criteria. ICH = intracerebral hemorrhage; CTA = CT angiography; MRA = MR angiography; DSA = digital subtraction angiography; MMS = moyamoya syndrome; MMD = moyamoya disease; RNF213 = ring finger protein 213.

Baseline data collection
We collected demographic data, vascular risk factor history, clinical characteristics and laboratory parameters. Neurological status was assessed using the Glasgow Coma Scale (GCS), National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS). Peripheral blood samples were analyzed for biochemical, serological and immunological profiles using enzymatic methods.
Neuroradiological evaluation and assessment of angiographic landscape
Imaging protocol
Initial neuroimaging for all stroke patients followed institutional protocol, using non-contrast CT (NCCT) and CT angiography (CTA) or MRI and MR angiography (MRA). MRI was performed on 1.5- or 3.0-Tesla machines. In select cases, single-photon emission computed tomography with Technetium-99 m ethyl cysteinate dimer assessed regional blood flow and cerebrovascular reactivity before extracranial-intracranial (EC-IC) bypass surgery. Additional modalities included high-resolution vessel wall imaging (HR-VWI) and six-vessel cerebral DSA. Pre-DSA screening measured urea and creatinine levels. DSA, conducted on a flat-panel detector system (Artis Zee Floor, Siemens, Germany), involved bilateral super-selective catheterization of the common carotid, external carotid, internal carotid and vertebral arteries via femoral puncture, with contrast injection (5 mL/s) and multi-angle visualization (1024 × 1024 matrix, 22-cm field of view and 0.21 × 0.21-mm pixel size).
Post-neuroimaging data analysis
Post-imaging, 3D and 4D analyses generated virtual reality (VR) and maximum intensity projection (MIP) images. From DSA, 18 phases – including arterial, arteriovenous and venous – were selected for optimal segmentation, cutting and reconstruction quality. VR and MIP images depicted the siphon and bifurcation of the bilateral ICAs, anterior, middle and posterior cerebral arteries, vertebrobasilar system and circle of Willis. The arterial phase was further analyzed in anteroposterior, posteroanterior, left-lateral and right-lateral views for all patients.
Deoxyribonucleic acid sequencing and data analysis
Clinical exome sequencing by next-generation sequencing
Deoxyribonucleic acid (DNA) was extracted from peripheral blood using a Qiagen isolation kit. Libraries were prepared per the SureSelect XTHS2 protocol and sequenced on the Illumina NovaSeq 6000 platform. Demultiplexing generated FastQ files, and raw reads underwent quality control with FastQC v0.12.1. High-quality reads were mapped to the hg38 reference genome (GRCh38) using BWA-MEM. Variant calling, including single nucleotide variants and small insertions/deletions (InDels), was performed with GATK-v4.3 and the SMART-One™ Tech Platform, following best-practice workflows.
Multiple sequence alignment and pathogenicity score analysis
Conservation analysis of amino acid residues for RNF213 variants was performed using the UniProtKB/Swiss-Prot database and BLASTp, with hg38 as the reference genome. Variant pathogenicity and deleterious effects were assessed using bioinformatics tools, including Polyphen2, Reference Adzhubei, Schmidt and Peshkin6 PANTHER-PSEP, Reference Tang and Thomas7 ClinVar Reference Landrum, Lee and Benson8 and CADD. Reference Rentzsch, Witten, Cooper, Shendure and Kircher9
Methods of revascularization
Revascularization employed direct methods, such as EC-IC bypass (superficial temporal artery to middle cerebral artery [MCA]), and indirect methods, including encephalo-duro-arterio-myo-synangiosis (EDAMS) and/or encephalo-duro-arterio-synangiosis. The neurosurgical team determined the appropriate approach (direct, indirect or combined).
Follow-up
We recorded stroke recurrence and mRS scores at the longest post-surgical follow-up interval of 24 months.
Statistical analysis
Statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 26.0. A complete case analysis approach was employed. Categorical variables are presented as frequencies and percentages, while continuous variables are summarized using means and standard deviations (SD).
Structural modeling and variant generation of E3 ubiquitin-protein ligase RNF213
The E3 ubiquitin-protein ligase RNF213 (Isoform 3, UniProt ID: Q63HN8), a 5,207-amino-acid protein, was modeled using homology modeling. Its sequence was sourced from UniProt, and a BLAST search identified the cryo-EM structure (PDB ID: 8S24) as the optimal template based on structural and functional similarity. Reference Altschul, Gish, Miller, Myers and Lipman10–Reference Crespillo-Casado, Pothukuchi and Naydenova11 Template gaps, corresponding to missing residues (Supplementary file ), were reconstructed via loop modeling in Modeler 9.2. The structure was refined with SWISS-MODEL, followed by energy minimization in GROMACS (50,000 steepest descent steps) and a 300-ps molecular dynamics simulation to ensure stability. Reference Webb and Sali12–Reference Van Der Spoel, Lindahl, Hess, Groenhof, Mark and Berendsen14 Model validation used Ramachandran plot analysis in PDBSUM to confirm phi-psi angle conformity. Reference Laskowski15 Three variants – Val1529Met, Arg4708Cys and Arg4810Lys – were generated using COOT for refinement and PyMOL for visualization and mutagenesis. Reference Emsley and Cowtan16 Evolutionary conservation was assessed with ConSurf, highlighting critical structure-function regions. Reference Ashkenazy, Abadi and Martz17 This workflow produced a robust RNF213 model and its variants, offering insights into its structural and functional roles.
Results
Demographic and clinical characteristics (Table 2)
The cohort comprised 12 patients with a mean age of 44.3 years (SD ± 11.1). The majority were female (83.3%, n = 10), with males representing 16.7% (n = 2). Prevalent vascular risk factors included arterial hypertension (66.7%, n = 8), diabetes mellitus (58.3%, n = 7), hypothyroidism (50.0%, n = 6), obesity (33.3%, n = 4) and dyslipidemia (8.3%, n = 1). These risk factors were more commonly observed among females aged 31–60 years. Additionally, elevated serum homocysteine levels were identified in 16.7% of patients (n = 2).
Baseline demographic characteristics, clinical presentation and biochemical analysis

Table 2 Long description
A table comparing baseline demographic characteristics, clinical presentation, and biochemical analysis across patients. The table has 12 columns and 13 rows, including headers. The columns are labeled as Parameters, Patient ID 001, Patient ID 002, Patient ID 003, Patient ID 004, Patient ID 005, Patient ID 006, Patient ID 007, Patient ID 008, Patient ID 009, Patient ID 010, Patient ID 011, and Patient ID 012. The rows include Age, Age at onset, Sex, Vascular risk factors, Baseline neurological presentation, Stroke pattern on evaluation, Platelet count (L), Prothrombin time (PT) (sec), Bleeding time (sec), Clotting time (sec), Activated partial thromboplastin time (aPTT) (sec), International Normalized Ratio, WBC (cells/L), ESR (mm/h), CRP (mg/dL), Na+ (mEq/L), K+ (mEq/L), Creatinine (mg/dL), LDL (mg/dL), HDL (mg/dL), LDL/HDL, Homocysteine (mol/L), and CSF vasculitis panel. Each row provides specific data for each patient ID. Notable trends include variations in age, vascular risk factors, and biochemical analysis results across different patients.
TIA = transient ischemic attack; HX = History; B/L = bilateral; GCS = Glasgow Coma Scale; mRS = modified Rankin Scale; NIHSS = National Institutes of Health Stroke Scale; MCA = middle cerebral artery; ICA = distal internal carotid artery; PCA = posterior cerebral artery; NCCT = contrast CT; CRP = C-reactive protein; LDL = low-density lipoprotein; HDL = high-density lipoprotein; T2 DM = Type 2 diabetes mellitus; UL= upper limb; LL= lower Limb; UMN = upper motor neuron; DTR = deep tendon reflex; ESR= erythrocyte sedimentation rate; CVA = cerebrovascular attack; FTP= frontotemporoparietal; GTCS = generalized tonic clonic seizure; LOC = loss of consciousness.
Neurological presentation and stroke characteristics (Table 2)
Among the 12 patients in the cohort, 33.3% (n = 4) presented with a baseline NIHSS score ≥6, indicating moderate to severe stroke severity, and 83.3% (n = 10) had an mRS score ≥2, reflecting at least slight disability.
Common clinical presentations included facial palsy or weakness in 50% of patients (n = 6), hemiparesis in 41.7% (n = 5) – predominantly left-sided – and dysarthria in 41.7% (n = 5). Other symptoms comprised seizures (33.3%, n = 4), increased deep tendon reflexes (33.3%, n = 4), decreased plantar reflexes (25.0%, n = 3), gait disturbances (25.0%, n = 3), headache (25.0%, n = 3) and sensory deficits (25.0%, n = 3). Vision loss was reported in one patient.
All patients experienced ischemic symptoms. Two patients had transient ischemic attacks, including one with recurrent left hemispheric events. Notably, one patient (ID-07) experienced more than six stroke recurrences.
Infarcts predominantly involved the MCA territory, observed in 91.7% of patients (n = 11). Among these, right-sided infarcts were most common (63.6%, n = 7), followed by left-sided (27.3%, n = 3) and bilateral involvement (9.1%, n = 1). One patient exhibited an infarct in the posterior cerebral artery territory.
Baseline biochemical parameters (Table 2)
All 12 patients underwent comprehensive biochemical profiling, including assessments of coagulation, metabolic, vascular, electrolyte, inflammatory, hemoglobinopathy, thyroid function and markers pertinent to PACNS, in accordance with European Stroke Organisation guidelines. No single parameter definitively indicated PACNS. Routine laboratory tests – including complete blood count, electrolytes, coagulation profile, lipid panel, liver and renal function tests – were within normal limits. CSF analyses revealed normal leukocyte counts, protein and glucose levels, effectively excluding infectious or neoplastic etiologies. Mean C-reactive protein (CRP) levels were elevated (8.02 ± 2.2 mg/dL), and low-density lipoprotein cholesterol levels were slightly raised (105 ± 3.2 mg/dL). Hypothyroidism was identified in six female patients. PACNS-specific panels were negative across all patients, a critical finding given the initial clinical suspicions of MMS or central nervous system vasculitis and the subsequent ineffectiveness of immunosuppressive therapies. Electroencephalograms conducted in patients presenting with seizures did not reveal significant abnormalities beyond expected patterns.
Neuroimaging findings and angiographic landscape
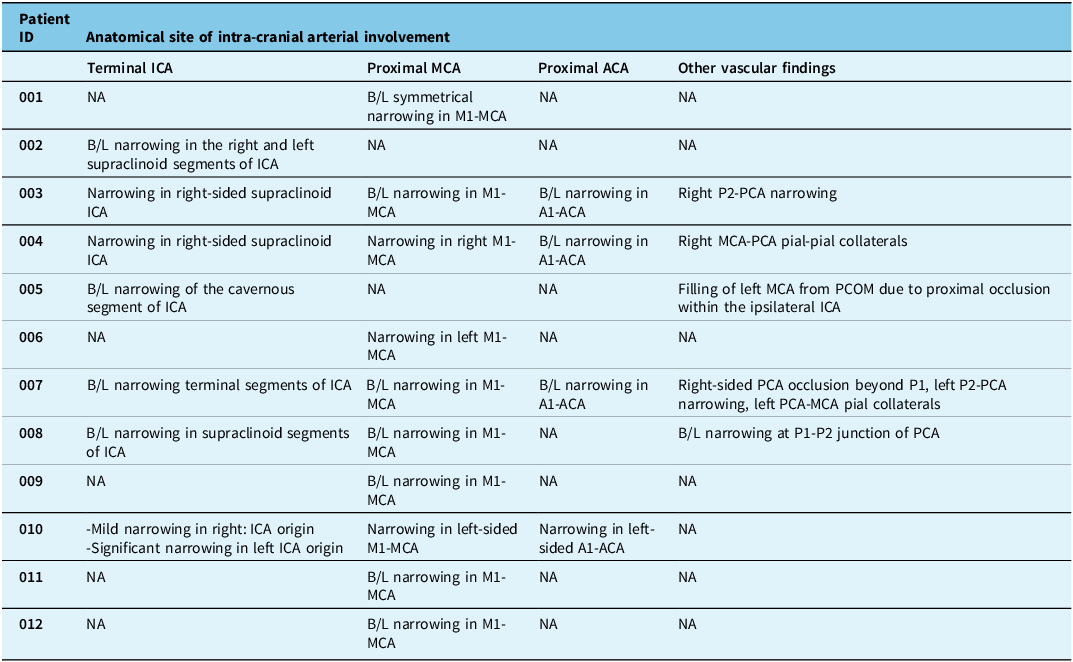
Initial MRI/MRA (TOF) and CT/CTA assessed brain involvement and carotid fork irregularities, followed by six-vessel DSA confirmation, optimizing efficiency. CT/MR perfusion aided hemodynamics assessment in some cases. DSA revealed bilateral carotid fork involvement in 91.7% (n = 11), with unilateral left M1 segment of the MCA narrowing in one (ID-006). Bilateral M1 segment of the MCA involvement occurred in nine cases, four of which had concurrent bilateral A1-ACA and terminal ICA stenosis. Isolated bilateral terminal ICA or supraclinoid ICA narrowing was seen in one each. No “puff-of-smoke” collaterals were observed, leading neuroradiologists to suggest the possibility of “central nervous system vasculitis” (Table 3, Figure 2A1–D6; Supplementary File).
(A1) and (A2) The right internal carotid artery angiogram in the anteroposterior and lateral projections shows abrupt narrowing involving the supraclinoid segment (black arrow) of the right internal carotid artery, with a thread-like appearance of the supraclinoid segment of the right internal carotid artery. Marked narrowing of the A1 segment of the right anterior cerebral artery (arrowhead) is also noted. The M1 segment of the right middle cerebral artery appears beaded (red arrow) with mild narrowing at places. However, the distal branches of the right middle cerebral artery show normal caliber and contrast opacification. (A3) and (A4) with left internal carotid artery injection in anteroposterior and lateral projection and (A5) and (A6) with right vertebral artery injection in anteroposterior and lateral projection show normal caliber and contrast opacification of the left internal carotid artery, left middle cerebral artery, left anterior cerebral artery, left vertebral artery, basilar artery and bilateral posterior cerebral arteries. Note the filling of the A2 segment of the right anterior cerebral artery and its branches through the anterior communicating artery on the left internal carotid artery injection. (B1) and (B2) Left internal carotid artery angiogram in the anteroposterior and lateral projections shows chronic complete total occlusion of the supraclinoid segment (black arrow) of the left internal carotid artery after the origin of the left ophthalmic artery. (B3) and (B4) Right internal carotid artery injection in anteroposterior and lateral projection showing normal caliber and contrast opacification of the right internal carotid artery, right anterior and right middle cerebral artery, and their branches. The A2 segment of the left anterior cerebral artery and the distal left anterior cerebral artery branches are normally opacified on the right internal carotid artery injection through the anterior communicating artery. (B5) and (B6) Right vertebral artery injection in anteroposterior and lateral projection shows near-complete reformation of the M1 segment of the left middle cerebral artery and its distal branches. However, no evidence of the typical “puff-of-smoke” appearance was seen. (C1) and (C2) Right internal carotid artery angiogram in the anteroposterior and lateral projections shows a moderate abrupt narrowing in the supraclinoid segment (black arrow) of the right internal carotid artery, with non-opacification of the M1 segment of the right middle cerebral artery (red arrow). (C3) and (C4) Left internal carotid artery injection in anteroposterior and lateral projection showing a moderate narrowing in the mid to distal M1 segment of the left middle cerebral artery (red arrow) without any obvious narrowing of the supraclinoid segment of the left internal carotid artery. (C5) and (C6) Left vertebral artery injection in anteroposterior and lateral projection shows partial reformation of the right hemi-anterior circulation via the posterior communicating artery and a few pial-pial collaterals from the right posterior cerebral artery branches. However, the typical “puff-of-smoke” appearance was not seen. (D1) and (D2) Right internal carotid artery angiogram in the anteroposterior and right anterior oblique projections showing a mild narrowing in the supraclinoid segment of the right internal carotid artery (black arrow). (D3) and (D4) Left internal carotid artery injection in anteroposterior and lateral projection showing moderate narrowing involving the supraclinoid segment of the left internal carotid artery with narrowing of the M1 segment of the left middle cerebral artery (red arrow). No evidence of abnormal collaterals or typical “puff-of-smoke” appearance was noted. (D5) and (D6) show serial DSA done after six months. (D5) shows a right internal carotid artery angiogram in anteroposterior projection with a mild increase in the narrowing in the supraclinoid segment of the right internal carotid artery (black arrow). (F) Left ICA angiogram on anteroposterior projection shows occluded M1 segment of the left middle cerebral artery, with accentuation of the narrowing in the supraclinoid segment of the left internal carotid artery (red arrow). However, even on the serial DSA, abnormal collaterals or typical “puff-of-smoke” appearances are not appreciated.

Anatomical site-specific involvement of the carotid fork in patients with “smokeless moyamoya”

Table 3 Long description
A table summarizing anatomical site-specific involvement of intra-cranial arterial involvement in patients with smokeless moyamoya. The table has 12 rows and 4 columns. The columns are labeled 'Patient ID', 'Terminal ICA', 'Proximal MCA', 'Proximal ACA', and 'Other vascular findings'. Row 1: Patient ID, 001; Terminal ICA, NA; Proximal MCA, B/L symmetrical narrowing in M1-MCA; Proximal ACA, NA; Other vascular findings, NA. Row 2: Patient ID, 002; Terminal ICA, B/L narrowing in the right and left supraclinoid segments of ICA; Proximal MCA, NA; Proximal ACA, NA; Other vascular findings, NA. Row 3: Patient ID, 003; Terminal ICA, Narrowing in right-sided supraclinoid ICA; Proximal MCA, B/L narrowing in M1-MCA; Proximal ACA, B/L narrowing in A1-ACA; Other vascular findings, Right P2-PCA narrowing. Row 4: Patient ID, 004; Terminal ICA, Narrowing in right-sided supraclinoid ICA; Proximal MCA, Narrowing in right M1-MCA; Proximal ACA, B/L narrowing in A1-ACA; Other vascular findings, Right MCA-PCA pial-pial collaterals. Row 5: Patient ID, 005; Terminal ICA, B/L narrowing of the cavernous segment of ICA; Proximal MCA, NA; Proximal ACA, NA; Other vascular findings, Filling of left MCA from PCOM due to proximal occlusion within the ipsilateral ICA. Row 6: Patient ID, 006; Terminal ICA, NA; Proximal MCA, Narrowing in left M1-MCA; Proximal ACA, NA; Other vascular findings, NA. Row 7: Patient ID, 007; Terminal ICA, B/L narrowing terminal segments of ICA; Proximal MCA, B/L narrowing in M1-MCA; Proximal ACA, B/L narrowing in A1-ACA; Other vascular findings, Right-sided PCA occlusion beyond P1, left P2-PCA narrowing, left PCA-MCA pial collaterals. Row 8: Patient ID, 008; Terminal ICA, B/L narrowing in supraclinoid segments of ICA; Proximal MCA, B/L narrowing in M1-MCA; Proximal ACA, NA; Other vascular findings, B/L narrowing at P1-P2 junction of PCA. Row 9: Patient ID, 009; Terminal ICA, NA; Proximal MCA, B/L narrowing in M1-MCA; Proximal ACA, NA; Other vascular findings, NA. Row 10: Patient ID, 010; Terminal ICA, Mild narrowing in right ICA origin, Significant narrowing in left ICA origin; Proximal MCA, Narrowing in left-sided M1-MCA; Proximal ACA, Narrowing in left-sided A1-ACA; Other vascular findings, NA. Row 11: Patient ID, 011; Terminal ICA, NA; Proximal MCA, B/L narrowing in M1-MCA; Proximal ACA, NA; Other vascular findings, NA. Row 12: Patient ID, 012; Terminal ICA, NA; Proximal MCA, B/L narrowing in M1-MCA; Proximal ACA, NA; Other vascular findings, NA.
ICA = distal internal carotid artery; MCA =middle cerebral artery; ACA = anterior cerebral artery; PCA = posterior cerebral artery; PCOM = posterior communicating artery; B/L = bilateral; NA = not applicable.
Results of next-generation sequencing and data analysis
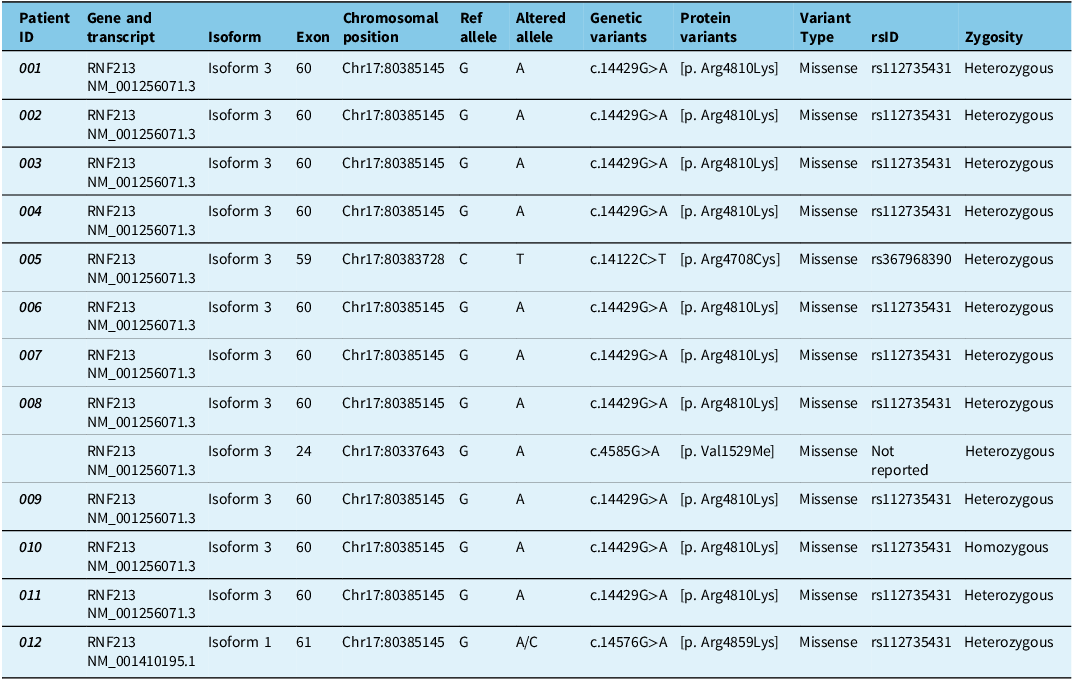
Of 12 patients, 9 had the p.R4810K (c.14576G > A) RNF213 variant (75%), 1 had p.R4708C (ID-005), 1 had p.R4810K plus p.V1529M (ID-008) and 1 had p.R4859K (Isoform 1) (Table 4). Variants with minor allele frequency <1 × 10−3 were rare, including novel p.R4708C (c.14122C > T) and p.V1529M (c.4585G > A) (Figure 3A–B, Supplementary File). Among p.R4810K cases, 88.9% (n = 8) were heterozygous, and one was homozygous. Variants spanned Isoform 1 (p.R4859K) and Isoform 3 (p.R4810K, novel), likely de novo. Pathogenicity scores (PANTHER, CADD, Polyphen2, ClinVar) are shown in Figure 3C.
(A) Variants identified in the study and their relative position across different domains of RNF213 (Isoform 3). (B) Conservation of the amino acid residues in RNF213 in correspondence to the above-reported variants. (C) Pathogenic characteristics of the identified RNF213 variants through different predicting software. ZF = zinc finger; AAA = ATPase associated with various cellular activities; PANTHER PSEP = protein analysis through evolutionary relationship - position-specific evolutionary preservation; Polyphen 2 = Polymorphism Phenotyping v2; CADD (PHRED) = Combination Annotated Dependent Depletion; ClinVar = clinical variant.

Genetic landscape of the 12 included patients with the “smokeless moyamoya phenotype”

Table 4 Long description
A table with 12 rows and 10 columns detailing genetic variants in patients with the smokeless moyamoya phenotype. The columns are labeled: Patient ID, Gene and transcript, Isoform, Exon, Chromosomal position, Ref allele, Altered allele, Genetic variants, Protein variants, Variant Type, rsID, and Zygosity. Each row provides specific data for each patient, including the gene and transcript involved, isoform, exon number, chromosomal position, reference allele, altered allele, genetic variants, protein variants, variant type, rsID, and zygosity. Notable patterns include the frequent occurrence of the p.R4810K variant and its heterozygous nature in most patients.
Clinical insights from treatment timeline
According to the AHA/ASA guidelines, Reference Guey, Tournier-Lasserve, Hervé and Kossorotoff21 all 12 received acute stroke care, transitioning to high-dependency units. Four received antiplatelets alone (2 with 1 recurrence, 2 with ≥3), while 8 received antiplatelets plus immunosuppression (5 with 1, 1 with 2, 2 with ≥3 recurrences) (Figure 4A–B, Figure 5), showing no benefit. Nine of 11 underwent EC-IC bypass (5 superficial temporal artery to MCA, 2 EDAMS, 2 combined), with no operated-side stroke recurrence and improved outcomes (Figure 4C, Figure 5). Two declined surgeries: ID-007 had six stroke recurrences, and ID-003 worsened to mRS 4 (Figure 5).
Treatment and follow-up: (A) Illustrates the two primary therapeutic regimens given to the patients after their baseline presentation. It also shows the recurrence of ischemic events related to each treatment group following discharge and during later follow-up visits. (B) Demonstrates the patients’ decisions and demographic summary in correspondence with revascularization surgical procedures. EC-IC = extracranial-intracranial; STA-MCA = superficial temporal artery-middle cerebral artery; EDAMS = encephalo-duro-arterio-myo-synangiosis; EDAS = encephalo-duro-arterio-synangiosis; U/L = unilateral; B/L = bilateral.

Illustrates the patient-wise treatment strategy and follow-up up to a maximum of 24 months.

Insights from structural modeling of RNF213
A homology model of RNF213 (Isoform 3, residues 421–5205) was constructed and refined using molecular dynamics simulations. Structural validation with PROCHECK revealed that 89.8% of residues resided within favored regions of the Ramachandran plot, indicating a reliable model. Secondary structure analysis showed that the protein comprised approximately 49% alpha-helices and 6.6% beta-strands (Figure 6A–F; Supplementary File).
(A) Cartoon representation of human RNF213 Isoform 3 (421-5205) and (B) Isoform 1 (427-5254). (C) and (D) demonstrate the Ramachandran plot statistics of human RNF213 Isoforms 3 and 1, respectively. (E) and (F) illustrate the electrostatic distribution of human RNF213 Isoforms 3 and 1, respectively.

Three RNF213 variants – Val1529Met, Arg4708Cys and Arg4810Lys – were analyzed for their impact on protein stability. ConSurf conservation analysis indicated that residues Val1529 and Arg4708 are highly conserved, suggesting that mutations at these positions may significantly affect protein function. In contrast, Arg4810 is less conserved, implying that the Arg4810Lys variant might have a subtler effect on protein stability (Figure 7A–F).
(A) Illustrates the mapping of different human RNF213 Isoform 3 variants. (B) and (C) demonstrate the surface representation of the evolutionary conservation of amino acid positions in human RNF213 Isoform 3 based on phylogenetic relations between homologous sequences. (D), (E) and (F) represent the residue interaction of wild-type (WT) and its variants in human RNF213 protein Isoform 3.

Discussion
MMD is a progressive cerebrovascular disorder characterized by steno-occlusive changes at the terminal portion of the ICAs and the development of abnormal vascular networks. The RNF213 gene, located on chromosome 17q25.3, has been identified as a major susceptibility gene for MMD, particularly the p.R4810K variant, which is prevalent in East Asian populations. Reference Kamada, Aoki and Narisawa18 This variant has been associated with increased risk of MMD and other steno-occlusive diseases, including intracranial atherosclerotic disease (ICAD), pulmonary arterial hypertension and coronary artery disease. Reference Yoshimoto, Tanaka and Koge19–Reference Suzuki, Kataoka and Hiraide20
In our study, we identified a cohort of patients exhibiting a unique “smokeless” phenotype of MMD, characterized by steno-occlusive changes at the carotid fork without the typical “puff-of-smoke” angiographic collaterals. All patients carried the RNF213 p.R4810K variant, with additional novel missense variants (p.V1529M, p.R4708C) identified in some cases. This phenotype challenges the conventional reliance on angiographic findings for MMD diagnosis and suggests that genetic testing for RNF213 variants can be instrumental in identifying such cases.
Differentiating “smokeless” MMD from ICAD is crucial, as their pathophysiological mechanisms and treatment responses differ. Reference Guey, Tournier-Lasserve, Hervé and Kossorotoff21 While ICAD is primarily managed with medical therapy, surgical revascularization remains the mainstay treatment for MMD. Reference Grubb, Powers, Clarke, Videen, Adams and Derdeyn22–Reference Komotar, Starke and Otten24 HR-VWI can aid in this differentiation; MMD typically presents with concentric, non-enhancing lesions and smaller outer diameters, whereas ICAD often shows eccentric plaques with wall enhancement and larger outer diameters. However, HR-VWI is not without limitations. There can be overlapping imaging features between MMD and ICAD, leading to potential misinterpretations. Reference Kathuveetil, Sylaja, Senthilvelan, Kesavadas, Banerjee and Jayanand Sudhir25 For instance, both conditions may exhibit vessel wall enhancement, and the presence of such findings alone may not conclusively distinguish between them. Given these challenges, incorporating genetic testing, particularly for RNF213 variants like p.R4810K, can enhance diagnostic accuracy. RNF213 mutations are strongly associated with MMD, especially in East Asian populations, and their presence can support the diagnosis in cases where imaging findings are inconclusive. Reference Kamada, Aoki and Narisawa18 Early genetic testing can prevent misdiagnosis, avoid unnecessary treatments and guide appropriate surgical interventions.
The absence of basal collaterals in “smokeless” MMD raises questions about the underlying molecular mechanisms. Classical moyamoya vessels arise from the remodeling and dilation of pre-existing penetrating arteries, a process involving both arteriogenesis and angiogenesis. Reference Liu, Wang and Akamatsu26 RNF213 is believed to play a role in angiogenesis, and mutations in this gene may disrupt normal vascular remodeling. Studies have shown that RNF213-mediated angiogenesis may be an intrinsic phenomenon, independent of hypoxia-driven mechanisms. Reference Ye, Niu and Liang27–Reference Chen, Tang, Li, Liu, Wang and Huang28
In our cohort, all patients who underwent revascularization surgery (n = 9) demonstrated favorable postoperative outcomes, including improved mRS scores and no stroke recurrence at the operated side. These findings underscore the efficacy of surgical intervention in “smokeless” MMD cases.
Our study has several limitations. First, it was conducted with a limited sample size, which may affect the generalizability of our findings. Second, all patients were enrolled from a single center, potentially introducing selection bias. Third, due to ethical constraints, we could not perform genomic, transcriptomic and proteomic analyses on intracranial vascular samples, which could have provided further insights into the molecular basis of this novel phenotype. Future studies should aim to overcome these limitations by incorporating larger, multicenter cohorts and comprehensive molecular investigations.
Our findings underscore the existence of a “smokeless” MMD phenotype associated with RNF213 variants, reinforcing the diagnostic value of genetic testing in patients with steno-occlusive changes lacking characteristic angiographic collaterals. As genetic testing transitions from research to routine clinical application, it is important to consider both turnaround time and cost. In our setting, concurrent moyamoya-targeted exome sequencing typically returns results within two weeks – well within the decision-making window for revascularization, particularly in adult cases. The cost, ranging from USD 110 to 130, is considered reasonable given the potential for genetic findings to inform diagnosis, avoid misclassification and prevent inappropriate therapies such as unwarranted immunosuppression. Early recognition of this phenotype may optimize patient management by guiding timely surgical intervention and improving long-term outcomes.
Conclusion
“Smokeless” MMD, marked by carotid fork steno-occlusion without classic basal collaterals, often mimics other vasculopathies, leading to diagnostic uncertainty. Incorporating RNF213 genetic testing alongside vessel wall imaging enhances diagnostic accuracy, distinguishing “smokeless” MMD from conditions like ICAD or PACNS. Early identification enables timely surgical revascularization, aligning treatment with classical MMD protocols and improving patient outcomes.
Supplementary material
The supplementary material for this article can be found at https://dx.doi.org/10.1017/cjn.2025.10371.
Data availability
Anonymized data supporting this study’s findings will be made available upon reasonable request to Dr Jayanta Roy (jroyneuro01@gmail.com) for researchers with appropriate qualifications.
Acknowledgments
The authors would like to acknowledge Professor Avik Roy Chowdhury from the Department of Laboratory Medicine for seamless efforts in managing all the lab reports and his views. We would also acknowledge the combined efforts of the medical records division, technicians of the MRI division and the CathLab team. Finally, we would like to express our gratitude toward our patients and their family members for the support they have given toward the fulfillment of this work.
Author contributions
J.R. contributed to (1) the conception organization of the study and (2) the writing of the first draft of the manuscript; S.D. contributed to (1) the conception organization of the study and (2) the writing of the first draft of the manuscript; R.M. contributed to (1) the conception organization of the study and (2) the writing of the first draft of the manuscript; G.S. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; B.M. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; M.T. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; N.R. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; A.S. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; S.P. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; P.S. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; S.B. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; A.M. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; J.B.-L. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; M.H. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript; S.H. contributed to collaborated on (1) the conception, organization and execution of the research project and (2) the review and critique of the manuscript. All authors have reviewed and approved the final manuscript.
Funding statement
This study has been supported by institutional intramural funding. Julián Benito-León is supported by the National Institutes of Health (NINDS #R01 NS39422 and R01 NS094607) and the Recovery, Transformation, and Resilience Plan of the Spanish Ministry of Science and Innovation (grant TED2021-130174B-C33 and NETremor and grant PID2022-138585OB-C33, Resonate).
Competing interests
The authors declare that they have no competing interests.











 Open access
Open access