

Child malnutrition remains a persistent global challenge(1,2) , driving increased mortality(Reference Kassaw, Amare and Birhanu3) and compromising lifelong economic(Reference Akseer, Tasic and Nnachebe Onah4), physical(Reference Soni, Fahey and Bhutta5) and mental health outcomes(Reference Roger, Vannasing and Tremblay6). Globally, stunting (height or length-for-age z-score (HAZ/LAZ) < −2 sd) and wasting (weight-for-height/length (WHZ/WLZ) < −2 sd) affect approximately 22 % (150·2 million) and 6 % (42·8 million) children under 5 years, respectively(1). While Kenya’s national undernutrition rates are lower than the global average (18·4 % stunting and 4·9 % wasting), they still fall above global targets(2), with stunting prevalence likely higher among HIV-exposed uninfected (HEU) infants(Reference Neary, Langat and Singa7).
Multiple factors drive undernutrition among children under 5 years in East Africa, including food insecurity(8), water insecurity(Reference Krumdieck, Collins and Wekesa9) and household poverty(Reference Kalichman10). These vulnerabilities are compounded by maternal human HIV status, which exists in a syndemic relationship with deprivation and resource insecurity(Reference Kalichman10–Reference Workman and Ureksoy13). While the overall prevalence of HIV in Kenya decreased from 5·6 % in 2010 to 3·2 % in 2023, the number of women of reproductive age living with HIV has risen, increasing the risk of HIV exposure for paediatric populations(14).
Early-life nutrition is a critical determinant of growth that is influenced by birth weight, breast-feeding practices and complementary feeding(Reference Adair and Guilkey15). HEU infants often have lower birth weights and poorer growth trajectories than HIV-unexposed uninfected (HUU) counterparts(Reference Alvarez, Miller and Santoso16,Reference Tiwari, Singa and Lihanda17) . Strikingly, our prior studies from Kenya suggest that breast-feeding rates may be higher among HEU infants than HUU infants, indicating the efficacy of breast-feeding promotion(Reference Rickman, Lane and Collins18). Other evidence has also shown that HIV-infected women are more likely to receive intensive counselling on exclusive breast-feeding(Reference Okanda, Otieno and Kinuthia19,Reference Nabakwe, Egesah and Kiverenge-Ettyang20) . However, less is known about complementary feeding, the introduction of solid foods alongside breastmilk or formula, in this context(Reference Grote, Theurich and Luque21).
In low- and middle-income settings, the adequacy of complementary feeding is often suboptimal due to inadequate access to nutritious foods(Reference Sokhela, Govender and Siwela22). Cross-sectional studies have shown that low consumption of animal-source foods (ASF) – which provide essential protein, Fe and Zn – is associated with greater risk of stunting and wasting between 6 and 24 months of age(Reference Tadele, Gebremedhin and Markos23). Meeting minimum dietary diversity (MDD) (consumption of at least five of eight specific food groups) is a common indicator of complementary feeding adequacy(Reference Heidkamp, Kang and Chimanya24,25) . Cross-sectional and longitudinal studies have linked higher MDD to reduced risks of malnutrition, yet many of these analyses use earlier definitions of dietary diversity that excluded breastmilk(Reference Aboagye, Seidu and Ahinkorah26–Reference Kamenju, Liu and Hertzmark29) or failed to account for the unique growth trajectories of HEU infants, who may have an elevated risk of malnutrition(Reference Lane, Widen and Collins30).
Therefore, the objective of this study was to evaluate the association between infant dietary diversity assessed at 9 months with subsequent growth and anthropometric measures of body composition, including risk of stunting and wasting, from 9 to 23 months of age among a cohort of HEU and HUU in Western Kenya. We also evaluated whether the consumption of ASF beginning at 9 months influenced later child growth and body composition outcomes. We hypothesized that infants with higher dietary diversity scores (DDS) and ASF consumption will have a lower likelihood of future stunting or wasting, as well as higher growth and body composition z-scores, compared to those with lower DDS and no ASF intake.
Methods
Study sample
Data were from the Pith Moromo 2 study, a longitudinal cohort designed to study the health consequences of food insecurity and HIV infection during pregnancy and lactation. From 2014 to 2017, 371 pregnant women were recruited from seven Family AIDS Care and Educational Services clinics in rural and urban Nyanza, Kenya, using non-probability, stratified sampling procedures based on HIV status (known, positive and newly diagnosed) and food insecurity (low, medium and high). The study has been described in detail previously(Reference Rickman, Lane and Collins18,Reference Widen, Tsai and Collins31) . Briefly, pregnant women were eligible if they were ≥ 18 years of age, gestational age ≤ 30 weeks, had known HIV status and had no plans to move from the study area. Prenatal in-person visits were conducted at 6 and 8 months’ gestation.
Study design
Postpartum telephone surveys for the maternal–child dyads were collected at 1 week and 6 months. Postpartum in-person dyad visits were held at approximately infant/child age 6 weeks and 3, 9, 12, 15, 18, and 23 months. This secondary analysis focuses on child visits from 9 to 23 months, as 9 months is the first visit where complementary feeding had been established. Similar to other research(Reference Andrade, Rebouças and Filho32,Reference Owais, Schwartz and Kleinbaum33) , the 9-month visit was chosen as the time frame to base dietary analysis as it was the first visit following the start of complementary feeding and is late enough in the complementary feeding period where a larger variety of foods should have been introduced and accepted. The 6-month visit was a telephone visit that did not include anthropometric measurements.
Child anthropometric measures
At each in-person study visit, child body composition measurements were completed by trained staff. Weight (kg, Seca 874), length (cm, Seca 417), head circumference (cm, non-stretchable retractable tape measure) and mid-upper arm circumference (MUAC, cm; non-stretchable retractable tape measure) were obtained. Skinfold thickness was measured (mm) at the triceps, subscapular, iliac crest and mid-thigh using Harpenden calipers (Baty International). Child weight was measured by having the mother stand on the scale, zeroing out the scale and then handing the child to the mother. Child measures were completed at least twice each visit, using a pre-specified threshold for conducting a third measure, and the mean of the measure was calculated.
Z-score conversions
Growth measurements were converted to WHO z-scores for weight (WAZ), length (LAZ), weight-for-length (WLZ), MUAC (MUACZ), triceps (TSFZ) and subscapular (SSFZ) skinfold thickness using zanthro in Stata(Reference Vidmar, Cole and Pan34). Poor growth was defined according to the WHO guidelines: (1) wasting: weight-for-length (WLZ) < −2 sd; stunting: height-for-age z-score (LAZ) < −2 sd; underweight: weight-for-age (WAZ) < −2 sd (35). A cut-off of below −2 sd was also used for skinfold thicknesses and MUAC measurements.
Dietary measures
Maternal interviews assessing child dietary intake of certain foods in the prior 24 h were completed at all visits after 6 months. The interviewer asked mothers to answer yes or no if their child had eaten a food from twenty-six different food types. For example, one food type was ‘any meat, such as beef, pork, lamb, goat, chicken or duck’, while another was ‘baby cereal, porridge, bread, rice or other foods made from grains’. These twenty-six food types were grouped into the eight food categories recommended by the WHO and UNICEF(36). This information was used to calculate DDS (0–8) and meeting MDD – consuming at least five of the eight food categories during the previous day: breastmilk; grains, tubers, and plantains; beans, peas, lentils, nuts, and seeds; dairy products; flesh foods (e.g. fish, meat, poultry and offal); eggs; vitamin A-rich fruits and vegetables; and other fruits and vegetables. Dietary diversity is a global measure that quantifies the number of food groups out of 8 (listed above) in a diet during a specific period and is used as a potential indicator of nutritional adequacy(Reference Moursi, Arimond and Dewey37). In the 2021 guidance from the WHO and UNICEF, the minimal acceptable diet was included as an additional measure of diet adequacy and is comprised of MDD, minimum meal frequency and minimum milk feeding frequency(36). Minimum meal frequency is achieved by receiving solid, semi-solid or soft foods the minimum number of times or more the previous day and minimum milk feeding frequency by having at least two milk feeds the previous day. MAD is then calculated using an established formula(36).
The Institutional Review Boards at Northwestern University, Cornell University and The University of Texas at Austin approved the study procedures. All mothers provided written informed consent.
Statistical analysis
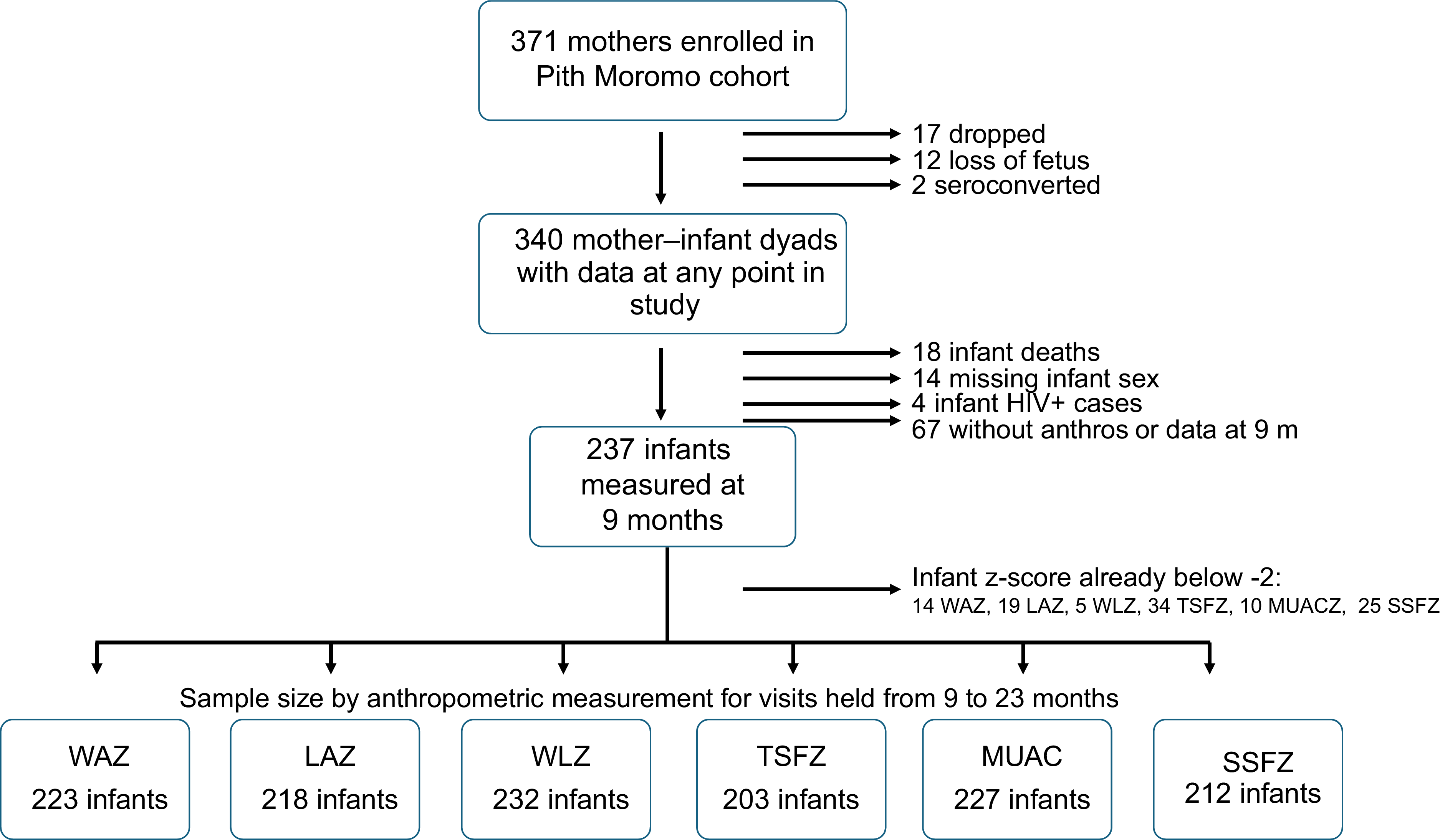
Statistical analyses were conducted in Stata 17 using an α level of < 0·05. To be included in the complete case analytic sample, infants had to be HIV-negative and have anthropometric measures and dietary data at 9 months as they were the outcome and predictor variables, respectively. Infants who seroconverted at any point during the study (n 2) were not included, as their growth would likely be affected by this change in HIV status. Additionally, those with missing sex (n 7) data were not included because their z-scores could not be calculated (Figure 1).
Flow diagram from enrollment in Pith Moromo 2 to inclusion into analytic sample for each growth measure. WAZ, weight-for-age z-score; LAZ, length-for-age z-score; WLZ, Weight-for-length z-score; TSFZ, triceps skinfold z-score; SSFZ, subscapular skinfold z-score; MUACZ, middle-upper arm circumference z-score.

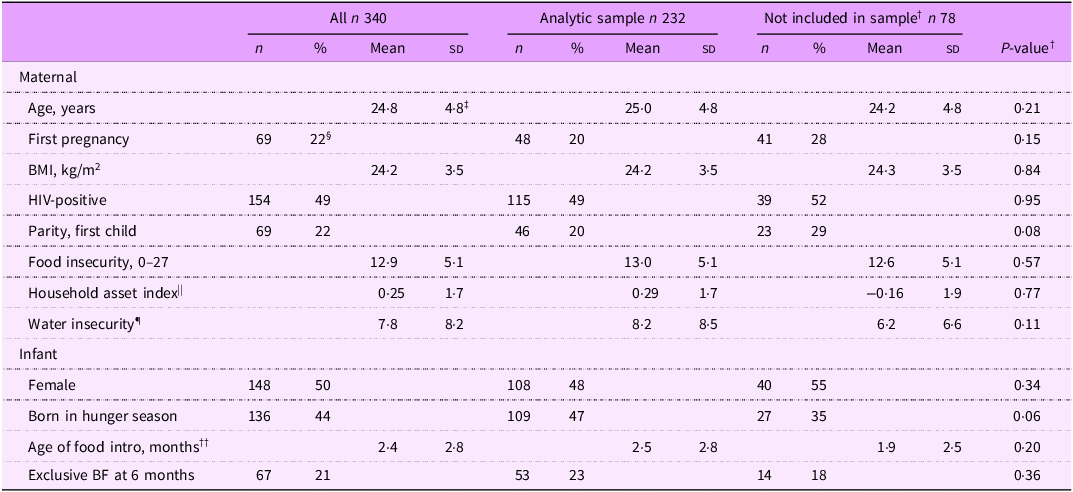
Sensitivity analysis of those included v. not included in the sample showed no notable differences (Table 1, although those not included in the sample had an earlier age of food introduction (1·61 months v. 2·6, P = 0·04), compared to those included in the analysis. Independent t tests were conducted to assess differences between maternal–infant dyads by MDD status (dichotomised yes/no) at 9 months. Dietary diversity was examined as two different exposures: MDD (dichotomised yes/no) and continuous DDS (scale 0–8); we also assessed the presence of specific ASF types, including flesh foods (meat, fish, poultry and organ meats) and eggs.
Characteristics of Pith Moromo 2 cohort of mother–infant dyads overall, and by inclusion in analytic sample

†Comparisons between those with 9-month data and those missing 9-month data were conducted using parametric tests for continuous, normally distributed variables and non-parametric tests for non-normally distributed variables.
‡Mean (sd) (all such values).
§ n (%) (all such values).
||Household asset index score –2·3–4·9; higher score equals more assets.
¶20 question scale; score 0–80; mean provided from last four visits.
††Data are available for only 274.
†Comparisons between those in and out of the analytic sample were conducted.
We conducted Cox proportional hazard analysis to identify the association between time to z-score −2 and the exposure – MDD and specific food intake. The proportional hazard assumptions were tested using estat phtest in Stata. To properly fit the Cox hazards model, the infants included could not have the presence of the growth condition (z-score already below −2 sd), as they were already below the endpoint and could not be included in the hazard model. The Cox models attempt to explain how an event in time, diet at 9 months, is associated with later changes in body composition z-score. Unadjusted and adjusted Cox proportional hazard regression models assessed associations between dietary exposures and child anthropometric measures that dropped below a −2 z-score threshold. Failure time was set as the first occurrence a child reached a z-score of −2 for the anthropometric outcome, including WAZ, LAZ, WLZ, triceps skinfold z-score (TSFZ), subscapular skinfold z-score (SSFZ), MUAC z-score and head circumference z-scores (HCAZ). Additional analyses were conducted to assess whether the same associations were observed for time-varying dietary diversity among the children included in the Cox models. For this analysis, adjusted and unadjusted longitudinal regression models assessed associations between lagged dietary diversity from the prior visit (9–23 months) with growth outcomes from 12 to 23 months. The Cox model allows for a dietary measure at a point in time to be associated with the risk of failure over time, while longitudinal regression allows dynamic dietary diversity to fluctuate and follow along as growth. Lagged growth is used, as diet at 9 months does not affect growth at 9 months. Diet at 9 months will affect growth at later time points.
Model covariates included infant sex, food insecurity score, household asset index, hunger season, water insecurity and maternal HIV status. Covariates were determined based on previous research demonstrating the impact of these factors on growth in similar populations(Reference Rickman, Lane and Collins18). Food insecurity was calculated using the 9-Item Individual Food Insecurity Access Scale (range 0–27) at 9 months in relation to diet(Reference Natamba, Kilama and Arbach38). Hunger season is a seasonal period when rainfall is minimal and thus fewer agricultural goods are produced with lower food availability. Hunger season was analysed as a time-varying binary variable aligned with study visits(Reference Widen, Tsai and Collins31). If a visit occurred from February to May, the visit was noted as ‘yes’, occurring during the hunger season. Visits from June through January were marked as not occurring during the hunger season. Household asset index included eighteen items commonly owned by households in the context and was created through item reduction via principal component analysis; higher scores indicated greater accumulated household wealth. Water insecurity was measured from a twenty-item scale previously validated in this population, evaluating water availability for drinking and other household activities as well as worry and missed opportunities due to lack of water in the prior 4 weeks(Reference Boateng, Collins and Mbullo39). Additional maternal indicators such as mother’s nutritional status and disease progression were not included as covariates as maternal determinants more strongly affect early infancy growth, while infant’s dietary behaviour, activity levels and motor development more strongly influence later growth.
Results
A total of 232 children were included in the analysis (Figure 1). There were no differences in baseline or complementary feeding data between those included and those excluded in the study, except that those excluded from this analysis had an earlier introduction to complementary foods (Table 1). The mean food insecurity score was 13·0, indicating mild food insecurity (FI, range 11–14), with 45 % of households experiencing mild FI. None of the covariates had statistically significant differences between those included v. not included in the sample or those who met compared to those who did not meet MDD.
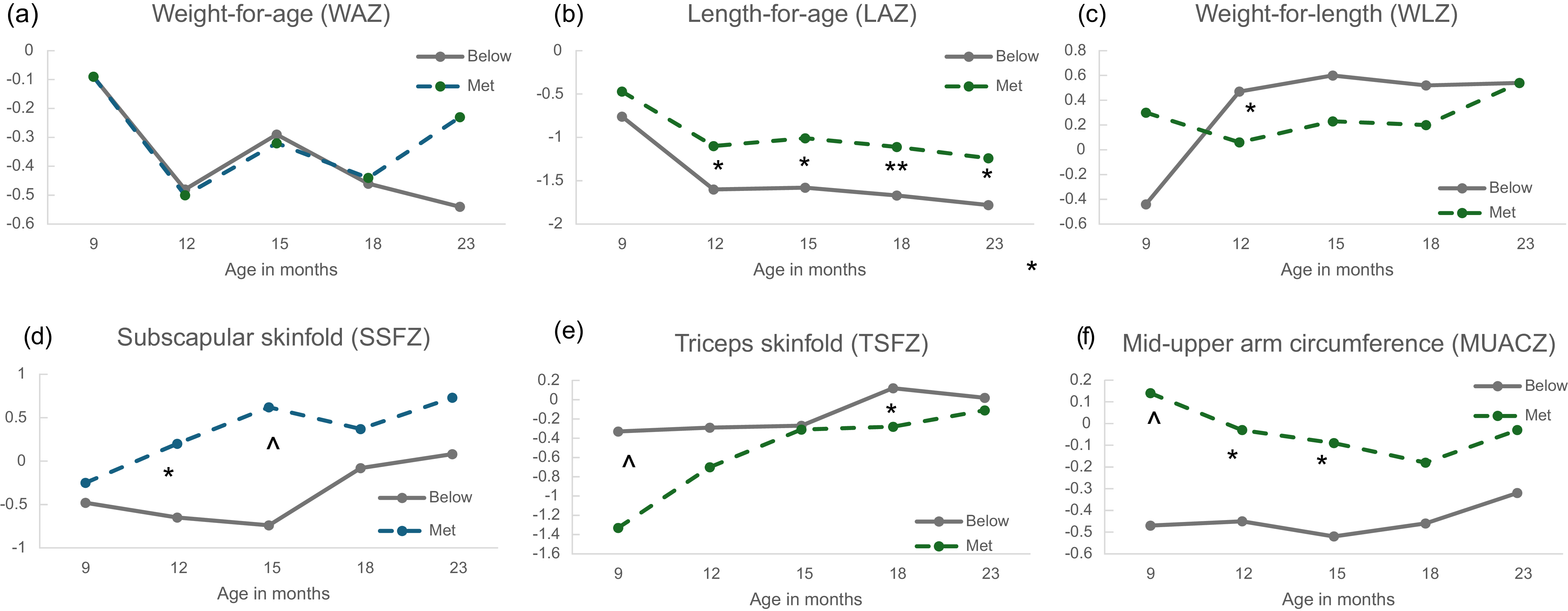
At the 9-month visit, 41 % of the infants met MDD. Infants who met MDD had an average DDS that was 3·3 points higher than those who did not meet (met 5·1 ± 1·0 v. unmet 1·8 + 1·0). Dyads in the analytic sample who met MDD (60 %) had birth parents who were younger (P < 0·05), experienced lower rates of depression (P < 0·05), had infants who were born during the hunger season (P < 0·01) and were longer by 23 months (P < 0·05) compared to those who did not meet MDD (Table 2, see online supplementary material, Supplemental Table 2). In the sample, both average LAZ and WAZ decreased over time from the 9-month to 23-month visit. For all infants, WLZ and HCAZ stayed relatively stable over time and above the median z-score. TSFZ, SSFZ and MUACZ increased from 9 months to 23 months (Figure 2, see online supplementary material, Supplemental Table 2). At 9 months, infants’ WAZ score in both those meeting MDD and those not meeting was just below the median (Figure 2). LAZ score in those not meeting MDD was modestly lower than in the group not meeting MDD, but not statistically different.
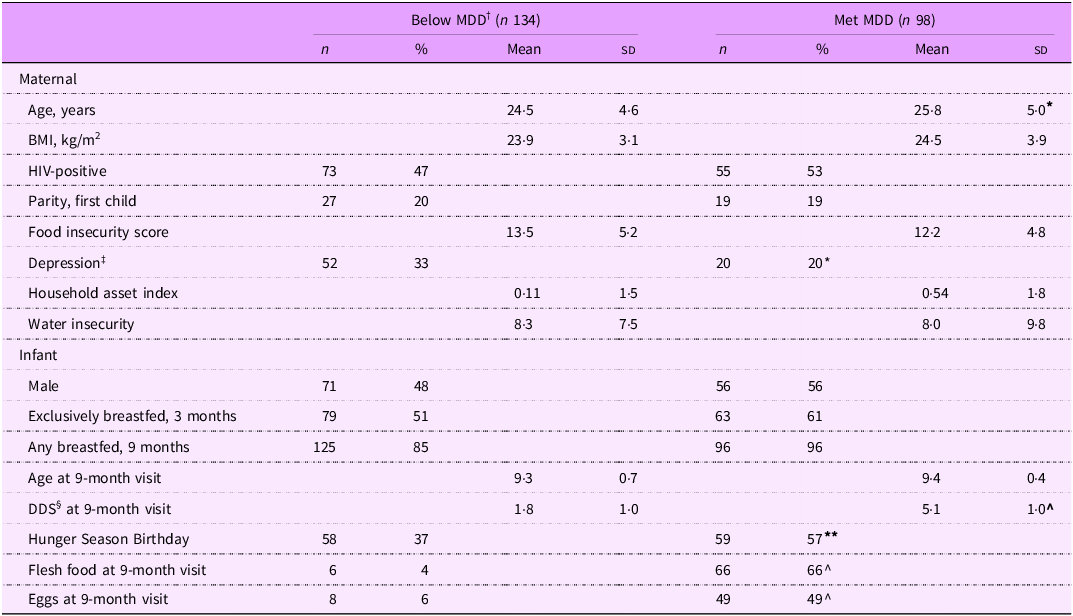
Characteristics of mother–infant dyads by MDD included in analytic sample, n 232
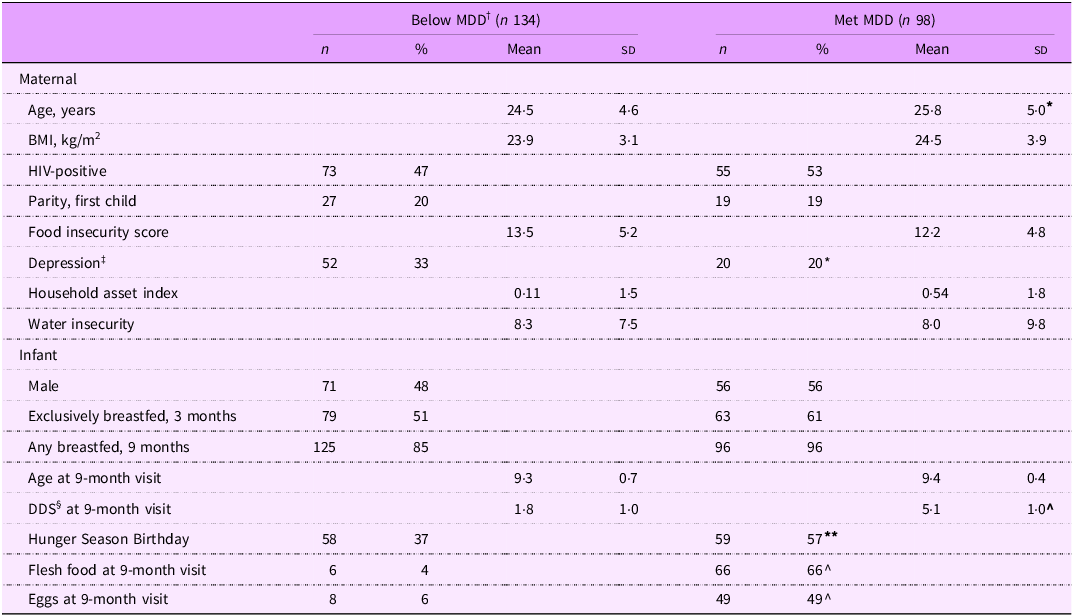
†MDD, minimum dietary diversity: below MDD (DDS ≤ 5); met MDD (DDS > 5).
‡Depression measured by CESD, scale 0–60.
§DDS, Dietary Diversity Score, range 0–8; z-scores: Testing for differences by MDD.
* P < 0·05, ** P < 0·01, ^ P < 0·001.
Mean z-scores of children at visits from 9 to 23 months of age in Pith Moromo 2, by minimum dietary diversity (MDD) status (met, MDD ≥ 5 or below, MDD < 5) for (a) weight-for-age z-score, (b) length-for-age z-score, (c) weight-for-length z-score, (d) subscapular skinfold thickness z-score, (e) triceps skinfold z-score and (f) mid-upper arm circumference z-score. Not shown head circumference z-score with no significant differences between the groups; *P < 0·05, **P < 0·01, ^P < 0·001.

Both TSFZ and MUACZ at 9 months were statistically significant between those meeting and those not meeting MDD at 9 months. Those meeting MDD had a lower TSFZ compared to those not meeting at 9 months. By 23 months, the difference was no longer statistically significant. There was no significant difference between average z-scores in any outcome for those meeting compared to not meeting MDD at 9 months.
Dietary diversity and animal-source foods with risk of adverse growth from 9 to 23 months
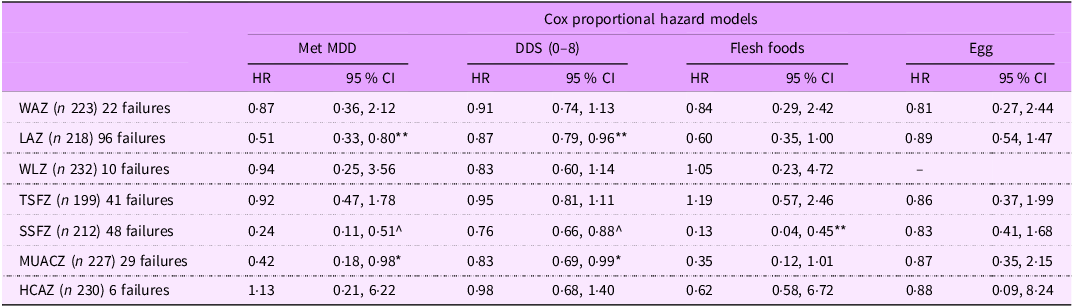
In Cox proportional hazard models, meeting MDD at 9 months was associated with a 51 % lower risk of stunting from 9 to 23 months and, further, 76 % and 58 % lower risk of z-scores falling below −2 sd for subscapular skinfolds z-score and MUAC z-score, respectively (Table 3, see online supplementary material, Supplemental Figure 1). In analyses using continuous DDS, each one-unit increase in DDS was associated with a 13 % reduced risk of stunting, a 24 % lower risk of low z-score for SSFZ and a 17 % lower risk for MUACZ (Table 3). Meeting MDD and continuous DDS were not associated with the risk of falling below −2 sd for WAZ, WLZ, TSF and HCAZ. No differences were noted between WAZ, WLZ, TSFZ and HCAZ in those meeting v. not meeting MDD at 9 months.
Associations between dietary diversity and dietary exposures with z-scores falling below –2 sd from 9–23 months, Pith Moromo 2

MDD, minimum dietary diversity; DDS, dietary diversity score; WAZ, weight-for-age z-score; LAZ, length-for-age z-score; WLZ, Weight-for-length z-score; TSFZ, triceps skinfold z-score; SSFZ, subscapular skinfold z-score; MUACZ, middle-upper arm circumference z-score; HCAZ, head circumference-for-age z-score.
Results are presented as hazard ratios, relative to 1 with values above 1 indicating increased hazard and values below 1 indicating lower hazard. Models adjusted for maternal HIV status, hunger season, food insecurity, infant sex, household asset index and water insecurity. Children excluded if 9-month data not available or already below cut-off. Analysis time: infant age in month.
P-value: *< 0·05, **< 0·01, ^< 0·001.
Following similar patterns for dietary diversity measures, intake of any flesh foods (i.e. meat, fish, poultry or organ meats) by 9 months was associated with an 85 % reduced risk of SSFZ falling below −2. Egg intake by 9 months was not associated with risk of stunting or z-scores falling below −2 for any anthropometric measure.
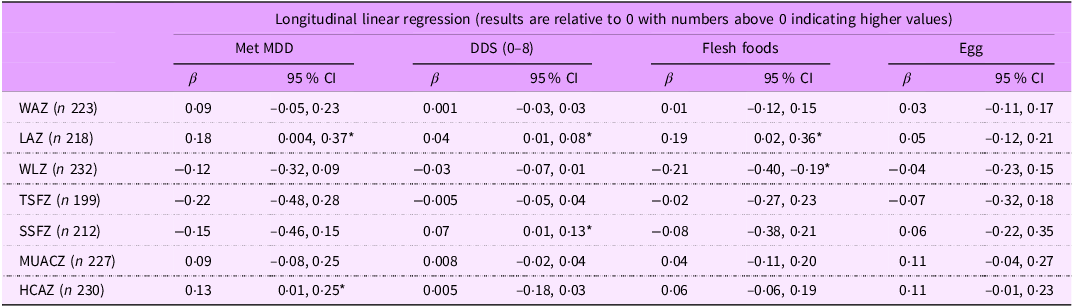
Similar to the hazard models, in our sensitivity analysis with the longitudinal regression models, a one-point increase in DDS across the study was associated with an average 0·04 higher LAZ score and meeting MDD was associated with an average 0·18 z-score (Table 4, see online supplementary material, Supplemental Figure 2). Unlike in the Cox models, intake of flesh foods during the 9–23 month period was associated with 0·19 higher LAZ from 12 to 23 months. A positive association was found between DDS and SSFZ, while a negative association was found between flesh food intake and WLZ (Table 4, see online supplementary material, Supplemental Figure 3). Finally meeting MDD was associated with 0·13 higher HCAZ score. In a sensitivity analysis including all infants with a 9-month visit, regardless of z-score, regression models demonstrated similar associations for all anthropometric outcomes as the primary models shown in the paper.
Associations between lagged dietary diversity and dietary exposures with continuous growth measures from 9 to 23 months, Pith Moromo 2

MDD, minimum dietary diversity; DDS, dietary diversity score; WAZ, weight-for-age z-score; LAZ, length-for-age z-score; WLZ, Weight-for-length z-score; TSFZ, triceps skinfold z-score; SSFZ, subscapular skinfold z-score; MUACZ, middle-upper arm circumference z-score; HCAZ, head circumference-for-age z-score.
Results are presented as β coefficients, relative to 0 with values above 0 indicating higher scores. Each value is showing an estimate from an individual regression model. Models are adjusted for maternal HIV status, hunger season, food insecurity, infant sex, household asset index and water insecurity.
P-value: *< 0·05.
Discussion
In this cohort of Kenyan children who were HIV-exposed, uninfected or HIV-unexposed, we sought to examine the association between dietary diversity and ASF intake at 9 months with subsequent growth in the second year of life. Although most of the children in the study had inadequate growth during the first 2 years, those who met MDD had a lower risk of stunting, low trunk adiposity and low MUAC, reflecting a reduced risk of impaired linear growth, low central adiposity and smaller upper arm composition, compared to those who did not meet MDD. Using longitudinal regression models, we also examined whether dietary diversity over time was associated with growth and found that dietary diversity over time was positively associated with subsequent LAZ and SSFZ, suggesting higher dietary diversity may have persistent associations across the second year of life on linear growth and subcutaneous truncal adiposity. Together, these findings support some of our hypotheses that meeting MDD may support more optimal growth.
Minimum dietary diversity and anthropometric changes
Interestingly, in the Cox models, we found that MDD was not associated with HCAZ, WLZ, WAZ or TSFZ, but it was associated with lower risk of z-score falling below −2 for LAZ, SSFZ and MUACZ. While overall linear growth (LAZ) in the sample was faltering, relative size (WLZ), weight and upper arm skinfolds remained relatively stable within 1 sd, which may be why we observed no association between WLZ and WAZ with any of the dietary exposures. Our longitudinal regression models found an inverse association between lagged flesh food intake and WLZ, with intake of flesh foods being associated with lower weight relative to length z-scores. One reason could be children who had flesh food intake could potentially be longer in length but have similar weight to those without flesh food intake reported during the interview. These children may appear thinner but, as evidenced by our results in Table 3, still maintain a z-score within acceptable boundaries. Interestingly, both our Cox and longitudinal models show a positive association between flesh food intake and LAZ. Similar findings were also found by Duong et al. on associations with dietary diversity and linear growth but not ponderal (weight (kg)/height (m)) or relative size in children up to 25 months of age(Reference Duong, Young and Nguyen40).
Lower dietary diversity has been associated with stunting in both cross-sectional and prospective studies(Reference Kamenju, Liu and Hertzmark29,Reference Chalashika, Essex and Mellor41,Reference Park, Harari and Siden42) . Similar to this study, in a cohort study of Tanzanian infants by Kamenju et al., a higher DDS from 6 to 24 months protected against stunting and underweight at 24 months(Reference Kamenju, Liu and Hertzmark29); yet, body composition was not assessed, so body fat, another indicator of growth and nutritional risk, could not be evaluated. In our findings, meeting MDD at 9 months was associated with both a decreased risk of z-score −2 (indicative of malnutrition) for MUACZ and SSFZ, suggesting that both adiposity and muscle mass may be improved by the early introductions to a variety of foods.
Unlike our findings, others have found associations between dietary diversity with wasting and underweight in cross-sectional research, which is unable to disentangle temporality between associations(Reference Aboagye, Seidu and Ahinkorah26,Reference Motadi, Zuma and Freeland-Graves43) . Aboagye et al. used cross-sectional survey data in children aged 6–23 months in sub-Saharan Africa and found adequate MDD was associated with a 13 % lower likelihood of wasting and a 17 % lower likelihood of being underweight(Reference Aboagye, Seidu and Ahinkorah26). Motadi et al. found, in their cross-sectional study of 273 children aged 3–4 years from South Africa, that weight-for-age but not weight-for-length was associated with DDS(Reference Motadi, Zuma and Freeland-Graves43). However, a recent systematic review including both cross-sectional and longitudinal studies found that current evidence indicates possible associations between dietary diversity and stunting, which aligns with our findings; however, this association for wasting and underweight remained uncertain(Reference Molani Gol, Kheirouri and Alizadeh27).
Flesh food intake and anthropometric changes
Flesh foods were consumed by two-thirds of those meeting MDD but less than 10 % of those not meeting MDD. Flesh food consumption at 9 months was also associated with lower risk of SSFZ falling below −2 sd growth in our analysis, indicating that intake of flesh foods may also be associated with adiposity possibly by reducing fat wasting. Few studies have evaluated skinfold thickness measures with dietary diversity. However, these important measures can help identify how weight and subcutaneous adipose tissue are distributed and how they relate to health. Our study is likely the first to report outcomes on skinfold thickness associations with dietary diversity in children aged 9 to 23 months in a population of HEU and HUU children.
Egg intake and anthropometric changes
Our findings that egg consumption at 9 months was not associated with the risk of malnutrition up to 23 months are in contrast to Pasqualino et al., who found a difference in higher egg intake from infant age 6 to 12 months with increased WAZ at infant age 12 months in Bangladesh(Reference Pasqualino, Shaikh and Hossain44). A randomised control trial of 500 South African infants enrolled at age 6 to 9 months with the provision of one egg per day for 6 months v. no egg found no differences in LAZ, WAZ or WLZ between the two groups at child age 12–15 months(Reference Ricci, Faber and Ricci45). Our longitudinal regression models also found no association between lagged egg intake over time and anthropometric measurements across the 9–23 month period. Differences in outcomes from the previous research compared to ours could be related to portion size and frequency of intake, neither of which we were able to capture.
While specific foods provide nutrients necessary for human growth and survival (such as the Fe and Zn in meats), other foods can also provide these nutrients. The ability of multiple foods to provide essential nutrients is likely one reason we observed associations between overall dietary diversity and the risk of stunting, subscapular skinfold thickness, and MUACz but not with specific food groups.
Our findings highlight that early DD is important for supporting linear growth. Yet, research has shown that improving access to foods does not always change dietary diversity(Reference Nicastro, Mocello and Weke46). The Supporting Healthy Mothers study, a feeding support programme with education and monetary support in Kenya for women with HIV, changed the nutrition behaviour of exclusive breast-feeding for 3 months(Reference Maltby, Odhiambo and Nyaura47). Community-based programmes and other policies and interventions should incorporate nutrition components addressing dietary diversity practices to not only improve access but also dietary diversity and growth.
This study has limitations that should be noted. One limitation is that we did not collect information on meal frequency, so we were unable to calculate minimal meal frequency and MAD. In addition, due to the nature of the dietary diversity questions, the amounts of each type of food eaten were unknown, so we could not calculate estimated energy intake and therefore cannot know if children with greater dietary diversity and more favourable eating profiles were eating more food or just higher-quality food. To address this limitation, we performed longitudinal regressions to evaluate the relationship of dietary diversity with growth from 9 to 23 months. Moreover, infant dietary diversity is validated as a tool for measuring nutritional exposures in this context, and it allowed us to contextualise how different dietary components were associated with growth(Reference Heidkamp, Kang and Chimanya24). While skinfolds are a proxy for adiposity in children, there are limitations to the measures such as difficulty in measuring squirming infants and the influence of hydration status or illness. Due to the small sample size, subgroup analysis comparing exposed v. unexposed infants was not conducted. Finally, we acknowledge that the missingness of data at 9 months and subsequent visits may underreport our low growth measures. Due to Cox model parameters, our analysis excluded infants who had suboptimal growth at 9 months; thus, our findings are generalisable to infants with similar growth parameters. Other limitations of Cox models are low event rates, although our sample had adequate events, and competing risks, which may bias results.
Nevertheless, this paper has several strengths, including the prospective longitudinal design and the frequency of repeated anthropometric measurements across the second year of life. Another strength is that almost half of the cohort was HEU infants, allowing us to evaluate growth in the first two years in this group of infants who are understudied at higher risk of poor growth(Reference Rickman, Lane and Collins18) and who are increasing part of Kenya’s infant population. Cox proportional hazards have not been a common method to evaluate diet in relation to growth in infant populations, and our paper is one of the first to examine associations between dietary diversity and time to event malnutrition, as a measure of nutritional health. Abebe et al. used Cox modelling in 476 Ethiopian infants and children to estimate the time to recovery from malnutrition (returning to a z-score > −2)(Reference Abebe, Simachew and Delbiso48). Tewoldie et al. used time to full enteral feeding in a low birth weight infant population(Reference Tewoldie, Girma and Seid49). Similar to our research, Ejigu et al. used Cox hazards to evaluate factors associated with stunting and underweight but did not assess sixteen dietary measures(Reference Ejigu, Magnus and Sundby50). In prospective, longitudinal studies like ours, Cox proportional hazard models should be considered as a way to understand early-life predictors of aberrant growth before they occur.
In conclusion, in our longitudinal cohort of HEU and HUU children, meeting MDD at 9 months was associated with reduced risk of stunting through 23 months, compared to those not meeting MDD. Improving complementary feeding by increasing dietary diversity and supporting the intake of flesh food throughout the first two years may help reduce the incidence of stunting and support optimal growth in HEU and HUU children. Our results highlight the need for early-life complementary feeding interventions to support children living in low- and middle-income countries. Policies that increase access to foods and other resources to increase dietary diversity are needed to mitigate the risk of stunting and support healthy growth. Our findings further suggest that we must continue to focus on improving the feeding environment in lower- and middle-income countries to improve infant and global health, especially in vulnerable populations exposed to HIV.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980026102912
Acknowledgements
The authors are thankful for the support and collaboration of the Kenya Medical Research Institute (KEMRI); the Director General of KEMI and the Deputy Director of the Centre for Microbiology Research (CMR); the Pith Moromo and Pii Ngima participants; the study nurses Joy China, Joyce Bonke and Tobias Odwar; the study trackers Benter Ogwana, Teresa Owade and Sarah Obaje and the anthropologist Patrick Mbullo.
Financial support
Research activities and SLY were supported by the National Institute of Mental Health (NIH/NIMH K01MH098902; R21MH108444). EMW was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development (K99/R00 HD086304 and P2CHD042849), the National Institute of Diabetes and Digestive and Kidney Diseases (NIH/NIDDK T32DK091227; T32DK007559) and an unrestricted fellowship to support research in maternal and child health from PepsiCo Global R + D. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflict of interest
The authors declare no conflicts of interest.
Authorship
E.M.W., M.O. and S.Y. designed the PM study; S.M.C., P.W. and J.D.M. conducted the research; S.F.F., S.Y. and E.M.W. designed the secondary analysis; S.F.F., R.R.R., D.P. and E.M.W. analysed the data; S.F.F., S.M.C., J.D.M., D.P., S.Y. and E.M.W. interpreted the findings; S.F.F., S.Y. and E.M.W. wrote the paper. E.M.W. has primary responsibility for final content. All authors read and approved the final manuscript.
Ethics of human subject participation
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Institutional Review Boards at Cornell University, Northwestern University, and the Kenya Medical Research Institute. Written informed consent was obtained from all mothers.



 Open access
Open access