


In recent years, the field of eating disorders has become increasingly concerned with how long-standing and severe presentations of illnesses are defined and treated. For example, debate has arisen around the classification of certain eating disorder presentations as ‘severe and enduring’, and the construct of ‘terminal anorexia’ has been proposed alongside discussions about whether treatment withdrawal, palliative care or assisted dying should ever be regarded as appropriate responses to illness. Reference Guarda, Hanson, Mehler and Westmoreland1,Reference Sharpe, Adams, Smith, Urban and Silverstein2,Reference Downs, Ayton, Collins, Baker, Missen and Ibrahim3
In the case of terminality, there remains no established evidence base demonstrating the conceptual coherence or clinical utility of defining eating disorders as terminal. Reference Crow4 Despite this, a recent review documented international cases in which assisted dying was provided for 60 patients with eating disorders over 12 years. Reference Roff and Cook-Cottone5 Notably, references to terminality, treatment resistance and futility are found among the rationales used by clinicians to justify providing assisted dying in these cases.
Irrespective of policy considerations around assisted dying, and its significant ethical and practical concerns, this research evidence highlights the entanglement of language, clinical decision-making and treatment provision as a pressing difficulty for the field. The way in which clinicians, researchers and policy-makers talk about eating disorders, and the terminology they use, have profound consequences for care trajectories – shaping clinician engagement, patient expectations and treatment outcomes.
The multi-layered impact of clinical language
Drawing on insights from medical anthropology and critical discourse approaches, we recognise that the terms used within eating disorder care are not neutral. Rather, words are used within structures of power relations, are shaped by historical and cultural contexts and carry significant implications at every level of interaction. Foucault argues that language is instrumental in constructing discursive regimes that define what is considered normal or pathological, thereby shaping the boundaries of acceptable clinical practice. Reference Foucault6 Similarly, discourse both reflects and reproduces social structures and experience. Reference Fairclough7 This is illustrated in the context of eating disorders by ‘staged’ models of anorexia nervosa, which have been criticised for reinforcing hierarchies that privilege stereotypical presentations of anorexia as the ‘premier’ eating disorder and, in turn, contribute to the ongoing marginalisation of other experiences and identities. Reference Asaria8,Reference Kiely, Conti and Hay9,Reference Downs, Adams, Federici, Sharpe and Ayton10
In addition to shaping social structures, language also frames our understanding of our place within them, Reference Gee11 with clinical language playing a role in how patients are perceived and treated by others, and how they relate to themselves. Reference Downs12 In oncology and palliative care, for example, communicating empathetically and clearly, and responding to patient concerns have been shown to positively influence hope, understanding and adherence, with training in accommodating communication strategies improving both patient outcomes and clinician well-being. Reference Apostolovski, Look Hong, Wright and Gagliardi13 In long-term condition management, studies in diabetes and obesity care highlight how stigmatising or authoritarian language can undermine self-management, whereas person-first and collaborative communication fosters trust, empowerment and sustained engagement. Reference Albury, Strain, Le Brocq, Logue, Lloyd and Tahrani14 Recognising this, the Language Matters frameworks developed in the UK for diabetes and obesity care emphasises person-first terminology and partnership-oriented dialogue as practical strategies to improve engagement and reduce stigma. Reference Lloyd, Wilson, Holt, Whicher and Kar15
These findings remind us that language is not merely descriptive but also constitutive, actively shaping therapeutic relationships, treatment outcomes, professional culture and policy priorities. This paper takes this premise as its starting point, examining how language functions within eating disorder care to shape perceptions of recovery, responsibility and treatability, and the consequences for engagement, inclusion and equity.
Method
A critical discourse analytic framework was used to explore how clinical language both constructs and constrains treatment experiences in eating disorders. Reference Fairclough7,Reference Gee11 Our analysis drew on both experiential and textual sources. We examined a purposive corpus of 45 academic, policy and lived-experience publications cited in this paper, including debates on severe and long-standing eating disorders/severe and enduring anorexia nervosa (SEED/SE-AN) and terminality, harm-reduction approaches, service provision, lived-experience scholarship and recovery-oriented models, alongside national policy reports such as those from the UK’s Parliamentary and Health Service Ombudsman. These materials were analysed in parallel with our own reflective narratives as people with lived experience of long-standing and complex eating disorders.
Each author contributed first-person accounts, which were discussed collaboratively, enabling us to identify points of convergence and divergence between and within our own experiences and the discourses present in the literature. Through this iterative process, discursive patterns emerged that informed the tripartite intrapersonal, interpersonal and systemic framework used to structure our analysis. The approach aimed to integrate theoretical rigour with experiential knowledge, positioning lived experience as a valid and generative analytic resource. Reference Downs, Adams, Federici, Sharpe and Ayton10,Reference Downs16
Our personal experiences span different healthcare systems, with two authors based in the UK (J.D. and A.C.) and one in the USA (M.A.). Although service structures and funding models differ across these contexts, the role of language in shaping clinical engagement and perceptions of treatability were sufficiently comparable across settings to enhance the analysis. We therefore view this diversity as a strength, illuminating how systemic factors such as resourcing, commissioning and access arrangements interact with language to shape treatment experiences internationally.
Results
Intrapersonal impact: language shapes internalised narratives and self-perception
At the intrapersonal level, our lived experiences demonstrate how the language used to describe eating disorders can have a profound effect on how patients see themselves. When individuals are labelled as having a ‘severe and enduring eating disorder/anorexia’ (i.e. SEED or SE-AN), they may internalise a sense of hopelessness, and a suboptimal illness trajectory may become self-fulfilling. Reference Downs17 Author J.D. describes their experience:
‘Being told I had a “severe and enduring” eating disorder felt like a verdict. It wasn’t just a description of my past struggles – it felt like a prediction of my future. I began to believe that no matter what I did, I would always be ill, that I was incapable of recovery. The more I absorbed this, the harder it became to challenge the behaviours keeping me trapped in the illness. I stopped imagining a future where I could be free from the disorder because the language used around me suggested that future didn’t exist.’
Examples such as this bring to life how the narratives associated with labels such as SEED – often suggesting chronicity and resistance to treatment – can erode self-esteem and create a sense of inevitable decline when internalised. This, in turn, may reduce willingness to engage with treatment and create a self-reinforcing cycle, which we suggest could represent a form of learned helplessness. Reference Morgan, Gellman and Turner18
Importantly, clinicians are not immune to the intrapersonal impacts of clinical language used in eating disorder care, either, and may share their patients’ sense of helplessness when trying to treat complex conditions with limited resources. When notions of futility are internalised, clinicians may engage in exclusionary practices – such as denying care or attributing treatment failure to features of illness – as a way of protecting themselves from the moral injury of being unable to deliver high-quality treatment. Reference Beale19 This, in turn, can contribute to a self-reinforcing cycle of poor outcomes, pessimistic narratives and unaddressed structural shortcomings.
Interpersonal and clinical impact: language influences therapeutic engagement and decision-making
On the interpersonal level, clinical language shapes interactions between healthcare providers and patients. Roff and Cooke-Cottone’s 2024 study, documenting cases of assisted dying for patients with eating disorders, highlights how clinicians often applied ‘pseudo-diagnostic’ labels such as SE-AN and ‘terminal anorexia’ as if these were established categories, even though standardised criteria for these are lacking within diagnostic manuals. Reference Roff and Cook-Cottone5 Similarly, a recent review of 11 studies of patient cohorts defined as SEED found that, in addition to many of these patients never having received evidence-based treatment, the criteria for duration of illness varied considerably, and no clear definition of severity was provided across studies. Reference Birch, Downs and Ayton20
This imprecise use of language nevertheless shapes interactions between patients and clinicians in ways that influence treatment trajectories. Often operating within the context of specialist services where resources are constrained and treatment pathways are limited, eating disorder professionals may use labels that imply certain patients are unlikely to respond to care in general, rather than attending to the specific limitations of the care that is on offer and how this may shape treatment failure. Reference Guarda, Hanson, Mehler and Westmoreland1 Patients, in turn, may internalise these narratives, believing that their difficulties are inherent and intractible rather than shaped by contextual factors. Over time, this can contribute to disengagement on both sides, limiting opportunities for therapeutic collaboration, as author J.D.’s experience demonstrates:
‘Despite having to push for treatment for years, I was told repeatedly by clinicians that my illness was too entrenched, that I lacked motivation or that I was not engaging enough with the care being offered. Rather than considering whether the treatment could be improved to take into account my neurodivergence and co-occurring physical, psychiatric and neurodivergent conditions, I was left believing that my difficulties were my fault, that my suffering was inevitable and that I was wasting professionals’ time. It has taken me years to unlearn this and to trust in seeking help from others again.
Looking back, I can see how I absorbed – or introjected – the narratives I was given: that I was resistant, difficult and incapable of change. I lost faith in the idea that treatment could help me and, as a result, I stopped engaging. I became withdrawn, dismissive and even hostile towards clinicians who were really trying to help me, because I truly believed there was no point in trying. It became self-fulfilling: the less I engaged, the more clinicians saw me as beyond help. The more they saw me this way, the more often they suggested I stop treatment. And so the cycle of illness continued.’
This example suggests that when clinicians adopt discourses of enduringness and futility, their interactions may reinforce the very sense of hopelessness that treatment needs to respond to. This can undermine the potential for therapeutic alliance and curtail recovery efforts. The language used in these encounters does not simply describe reality; it actively shapes it, influencing both the patient’s expectations of recovery and the clinician’s willingness to continue offering care.
Organisational and systemic impact: language is context-bound and context-reinforcing
At the organisational level, the pervasive use of labels such as SE-AN and SEED can exert influence at the level of policy-making and may shape service priorities, eligibility criteria and resource allocation in ways that risk pre-emptively limiting access to care. The systemic and structural features of services themselves – such as the availability and continuity of care, multidisciplinary input, resource levels and commissioning arrangements – may also be obscured by narratives of chronicity and treatment resistance. Reference Downs, Ayton, Collins, Baker, Missen and Ibrahim3 This is despite evidence that these underlying determinants play a critical role in shaping treatment outcomes.
For example, studies have shown that access to sustained and specialised intervention can significantly alter the trajectory of severe eating disorders. Approaches such as integrated and enhanced cognitive–behavioural therapy and intensive multidisciplinary programmes demonstrate that recovery-oriented, collaborative language and practice are already embedded in parts of the field. Reference Ibrahim, Ryan, Viljoen, Tutisani, Gardner and Collins21,Reference Federici and Wisniewski22 These models emphasise joint formulation, shared decision-making and autonomy-supportive communication, showing that, when structural and relational conditions are optimised, markedly better outcomes are possible. However, when evidence-based interventions are unavailable or difficult to access, the likelihood of poor outcomes increases, not necessarily because of the severity of illness itself, but because of the inadequacy of the treatment environment. Reference Ayton, Ibrahim, Downs, Baker, Kumar and Virgo23,Reference Viljoen, King, Harris, Hollyman, Costello and Galvin24 This is particularly the case for patients with co-occurring physical, psychiatric and neurodevelopmental conditions Reference Hambleton, Pepin, Le, Maloney, Touyz and Maguire25 and those with histories of trauma. Reference Day, Hay, Tannous, Fatt and Mitchison26
Policy analyses reflect these systemic shortcomings. In the UK, the Parliamentary and Health Service Ombudsman report ‘Ignoring the Alarms: How NHS Eating Disorder Services are Failing Patients’ (2017) documents the fatal consequences of delayed or denied care, exposing how gaps in service provision contribute to preventable deaths. 27 Similar structural failings are evident in other healthcare systems, where gaps in service provision (such as long waiting lists, inconsistent step-down care and limited availability of multidisciplinary approaches) fundamentally impair the way in which treatment is delivered and experienced, causing poor long-term outcomes and what has been described by Kaye and Bulik (2021) as a ‘crisis in care’. Reference Kaye and Bulik28
Author M.A. reflects on the context-bound nature of language, and how terms used in eating disorder treatment are both shaped by and reinforce structural insufficiencies in care:
‘There is a misconception that eating disorder treatment is readily available for anyone who is “ready” to recover. For years, I lacked access to competent outpatient care due to geographic and insurance barriers. Each time I left inpatient treatment, I returned home to a setting with no continuity of care, leading to repeated relapses. Characterising a significant subset of patients as “severe and enduring” obscures these systemic failures by shifting the focus onto presumed patient deficits rather than gaps in service provision.’
Although this reflection refers specifically to the insurance-based healthcare context of the USA, comparable gaps in treatment continuity are seen within publicly funded systems such as the UK’s National Health Service. In both contexts, the framing of certain patients as ‘treatment resistant’ or ‘beyond help’ can obscure the structural factors which result in gaps in prevision, such as those related to commissioning, geography or capacity, potentially shifting responsibility for unmet need from systems to individuals.
Creating a shared therapeutic discourse and language of hope
Therapeutic optimism and holding hope
The potential of clinical language to be harmful is increasingly supported by theoretical and empirical research, including personal accounts from people with lived experience (PWLE). Reference Sharpe, Adams, Smith, Urban and Silverstein2,Reference Downs, Ayton, Collins, Baker, Missen and Ibrahim3,Reference Asaria8,Reference Downs16,Reference Downs17,Reference Elwyn29,Reference Collins30 However, just as the examples we have shared in this paper do not represent the whole picture of our own lived experiences, avoiding harm is not our only ambition for how the use of language can be reimagined in the context of eating disorders. We view it as equally important to consider how language can be used positively to create a shared discourse of therapeutic optimism that can be an active tool in promoting recovery, sustaining engagement and improving the effectiveness of treatment.
Our own experiences reflect this possibility, and have included instances where clinicians have used recovery-oriented, collaborative language in ways that have actively supported our sense of hope, trust and agency. In these contexts, even small shifts in wording – such as focusing on our goals, strengths and the possibility of change – have helped support engagement and a sense of partnership in our treatment. These moments demonstrate how hopeful and person-centred discourse is not an abstract ideal – it is a lived reality already present in pockets of good practice across eating disorder services. Indeed, the Academy for Eating Disorders’ ‘Nine Truths about Eating Disorders’ position statement provides clear, evidence-based messages that challenge stereotypes and convey hope, and can serve as a model for embedding positive framing within clinical discourse. Reference Schaumberg, Welch, Breithaupt, Hübel, Baker and Munn-Chernoff31
In our experiences, a crucial aspect of therapeutic optimism in eating disorder care is the principle of holding hope – the idea that clinicians, caregivers and the broader treatment culture must maintain belief in the possibility of recovery, even when the individual struggles to see it for themselves. For individuals who have been unwell for years and/or whose past treatment experiences may have led to a sense of futility, envisioning a future beyond their illness can be extremely difficult, despite there being no established criteria indicating that illness progression is inevitable. Reference Downs, Ayton, Collins, Baker, Missen and Ibrahim3,Reference Crow4 The importance of maintaining a stance of hope is also reflected more broadly in health communication research, where framing illness in ways that preserve agency and possibility is associated with better emotional well-being and therapeutic engagement. Reference Downs17,Reference Morgan, Gellman and Turner18,Reference Beale19 Within this context, language becomes not only a medium for care but an ethical practice that can open up the conditions for recovery.
Guarding against futility
The cognitive rigidity and ambivalence that can arise with eating disorders make engaging with treatment challenging, particularly when weight restoration or behavioural change may trigger overwhelming distress. Reference van Elburg, Danner, Sternheim, Lammers and Elzakkers32 Likewise, the ability to make a well-reasoned decision to refuse treatment (or medical care altogether) can be congruent with the nature of an eating disorder, Reference van Elburg, Danner, Sternheim, Lammers and Elzakkers32,Reference Westmoreland, Johnson, Stafford, Martinez and Mehler33 and is exacerbated by the deleterious effects of malnutrition on the starving brain. Reference Tadayonnejad, Pizzagalli, Murray, Pauli, Conde and Bari34 It is therefore vital that clinicians do not overlook or ignore the reality of physical compromise when considering whether to engage a patient in treatment that conflicts with their stated wishes, Reference Westmoreland and Mehler35 especially when patients have reported valuing compulsory treatment following recovery. Reference Collins30
In these instances, it may be particularly important for clinicians, caregivers and broader treatment cultures to do more than provide interventions that safeguard against adverse outcomes, including death. Maintaining belief in the possibility of recovery is vital when patients and their loved ones may themselves feel ambivalent or hopeless. Reference Elwyn29,Reference Burman, Rhodes, Vatter and Miskovic-Wheatley36 Author A.C. reflects on the decisions taken by clinicians on their behalf which protected them from falling into hopelessness:
‘When extremely unwell with my eating disorder, my capacity to engage in any form of reasoned consideration of my condition was severely restricted. I was terrified of death – an inevitability that some part of me knew was imminent without intervention – but even more so of the equally active yet immediately threatening prospect of weight restoration. This cognitive dissonance was accompanied by a pervasive sense of futility, marred by negative past treatment experiences and an utter inability to envision recovery as a possibility.
My life was saved by decisions about my care being taken out of my hands by a treatment team actively invested in my recovery. My experience is one shared by others who, despite a poor prognosis, received appropriate and life-affirming care and went on to achieve active recovery.’
The power of futile narratives and past difficult treatment experiences to shape a patient’s orientation towards recovery is made clearly evident in this account, as is the extent to which a clinical team’s ability to adopt a therapeutic stance can help support engagement and lead to positive recovery outcomes despite severe illness. Although rejecting therapeutic nihilism in favour of hope does not guarantee recovery, we view it as a core condition of environments within which recovery is more likely to become a reality.
Supporting structural change
Beyond individual clinician–patient relationships, the language used within treatment teams, clinical training and policy frameworks needs to be oriented towards an optimistic conceptualisation of patients, treatment and the possibility of healing and health that can be achieved even in the most complex of cases. As part of this, providing training for clinicians to recognise the importance of illness narratives at both the intra- and interpersonal level could be widely beneficial, as there is evidence showing that greater clinician awareness of how language can shape patient experience may improve service accessibility and reduce drop-out rates. Reference Linardon, Hindle and Brennan37
Therapeutic pathways may also benefit from drawing upon narrative-focused practices, such as literary and audiovisual storytelling, which, although situated outside of traditional evidence-based treatments, have been demonstrably valuable for a number of individuals and groups experiencing eating disorders in re-conceptualising their experiences of illness and perspectives on recovery. Reference Daugelat, Gregg, Adam, Schag, Kimmerle and Giel38,Reference Habibagahi and Ferrari39 Policy-makers may also benefit from looking to guidelines from New Zealand and Australia as an example of how to explicitly embed the communication of hope and belief in recovery within future frameworks. Reference Hay, Chinn, Forbes, Madden, Newton and Sugenor40
Epistemic justice and the co-production of treatment
The shift towards a recovery-oriented discourse also requires embracing epistemic justice – the recognition that individuals hold unique and indispensable insights into their own conditions, which have equal value alongside other, more conventional, ways of knowing. Reference Downs, Adams, Federici, Sharpe and Ayton10,Reference Gee11 As noted earlier, diverse lived experiences of eating disorders – especially those that do not fit narrowly defined demographic and symptomological stereotypes – have long been excluded from treatment narratives and research, resulting in models of care that can be experienced as harmful and exclusionary. As such, co-production methods that include the perspectives of a broad range of PWLE need to be embedded across research, policy and clinical practice in order to create treatment models that are more responsive to the needs of all patients, thus dismantling systemic barriers to care. Reference Downs16,Reference Bell, Lim, Williams, Girdler, Milbourn and Black41,Reference Lwembe, Green, Chigwende, Ojwang and Dennis42
Recent studies in the context of eating disorders show how incorporating the lived experiences of patients in service design can lead to more effective treatment models that achieve better outcomes. For example, autistic PWLE of eating disorders and clinicians have co-produced guidelines for including autistic patients within clinical research projects, showing how lesser/poorly understood lived experiences can be harnessed to create more inclusive interventions that are likely to help a more diverse range of people. Reference Nimbley, Maloney, Gillespie-Smith, Sharpe, Buchan and Kettley43
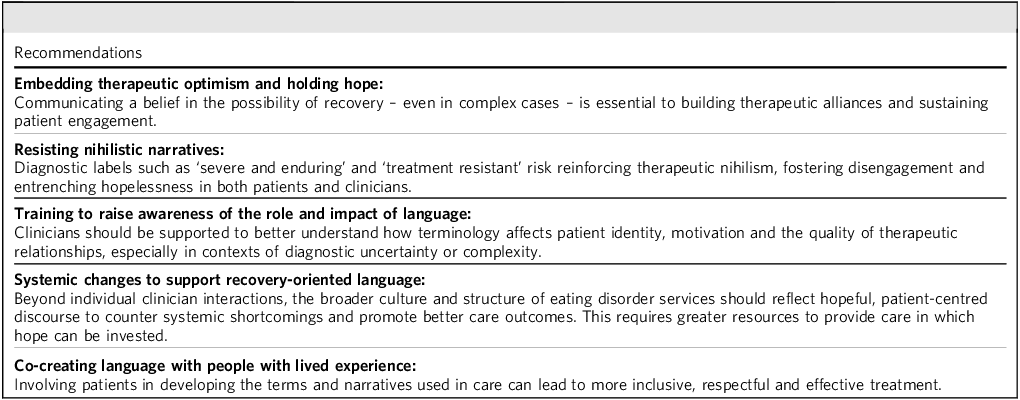
In terms of co-creating a shared language, we hope this paper adds meaningfully to arguments made elsewhere in favour of greater engagement with PWLE in discussions about how their conditions are described, defined and diagnosed. Reference Reay, Holliday, Stewart and Adams44,Reference Broomfield, Rhodes and Touyz45 When clinicians view patients as credible interpreters of their own experience, the therapeutic discourse may shift from one of uneven power dynamics to one of partnership and mutual respect. Our recommendations in Table 1 offer a starting point for creating clinical discourses rooted in partnership and compassion.
Recommendations for language use in eating disorder care

Discussion
Despite the complexity of the subjects and experiences we have discussed in this paper, we hope one thing is clear: the language used to describe eating disorders does not simply reflect reality, it actively shapes it. With some key – albeit limited – examples, we have shown how language influences how individuals understand their own illnesses and how clinicians and patients engage with one another as treatment progresses. The context-bound nature of discourse can also tell us something about how the structural and institutional limitations of existing systems of eating disorder care may be upheld, at least in part, by limiting narratives and narrow conceptualisations of illness. In turn, an awareness of the power of language provides opportunities for re-creating both the way we talk about eating disorders and the development of more inclusive, adaptive care models that better respond to the diverse needs of individuals like ourselves.
Co-creating a recovery-oriented discourse is not about offering false reassurance or downplaying the challenges and complexity of treatment. It is about recognising that the way we speak about illness can either open or close doors, and ensuring that language does not predefine someone’s trajectory but instead holds space for possibility. It is about adopting a stance of persistence, adaptability and an unwavering commitment to the potential for change. A patient-centred, collaborative approach to language has the power not only to alter individual treatment trajectories – it is a central part of transforming our treatment systems more broadly, for the benefit of all those involved in providing and receiving eating disorder care.
Importantly, there are already promising examples of this work in practice, both within specialist eating disorder services and wider health movements that model hopeful, compassionate and collaborative dialogue. Building on these developments offers a route towards creating systems and cultures of care that prioritise the possibility of recovery, rather than foreclose it.
About the authors
James Downs, Marissa Adams and Anna Carnegie are independent researchers with lived experience of eating disorders.
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Author contributions
J.D. conceptualised the manuscript. All authors contributed in writing, editing and reviewing all aspects of the work.
Funding
This paper received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.

 Open access
Open access
eLetters
No eLetters have been published for this article.