


Osteoporosis is characterised by a reduced bone mass and fragmentation of bone architecture, resulting in a higher risk of fracture, particularly of the wrist, spine and hip bones(Reference Sambrook and Cooper1). About half of all women and one-fifth of all men aged over 50 years will experience an osteoporotic fracture, chiefly due to osteoporosis(Reference van Staa, Dennison and Leufkens2,Reference Watts and Manson3) . Osteoporotic fractures are associated with significant morbidity, and about 30 % of affected individuals die within 1 year following a hip fracture(Reference Lund, Møller and Wetterslev4).
Low plasma levels of 25-hydroxy-vitamin D (25(OH)D), a biochemical marker of vitamin D status, have been associated with higher risks of osteoporosis(Reference Bischoff-Ferrari, Kiel and Dawson-Hughes5,Reference Kuchuk, van Schoor and Pluijm6) and osteoporotic fracture(Reference Gerdhem, Ringsberg and Obrant7,Reference Khaw, Luben and Wareham8) , but the results of randomised trials of vitamin D supplements for the prevention of fracture have been conflicting(Reference Yao, Bennett and Mafham9). The discrepant results of observational studies and randomised trials of vitamin D for the prevention of fracture may reflect limitations of the previous trials or residual confounding or other biases in the observational studies. Most of the previous trials of vitamin D evaluated relatively low doses of vitamin D, often administered intermittently (equivalent of 400 IU–800 IU daily) or included individuals at low risk of fracture or did not prioritise those with low plasma levels of 25(OH)D. The Biochemical Efficacy and Safety Trial of vitamin D (BEST-D) compared the effects of daily dietary supplementation with vitamin D3 using 2000 IU/d or 4000 IU/d or matching placebo for 12 months on plasma levels of 25(OH)D in 305 community-dwelling older people living in Oxfordshire in 2012, who were not taking drug treatment for osteoporosis. It aimed to assess what dose of vitamin D was required to achieve plasma levels of 25(OH)D > 90 nmol/l associated with the lowest risk of fracture in the observational studies. The BEST-D trial demonstrated that plasma 25(OH)D levels of 50 (18) nmol/l at baseline increased to 137 (39), 102 (25) and 53 (16) nmol/l after 12 months in those allocated vitamin D at 4000 IU or 2000 IU daily or placebo, respectively(Reference Hin, Tomson and Newman10).
The International Osteoporosis Society (IOS) and International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) and other expert groups advocated screening older people using blood levels procollagen type 1 N-propeptide (P1NP, a bone formation marker) and C-terminal telopeptide of type I collagen (CTX, a bone resorption marker) to predict bone mineral density (BMD), risk of fracture and response to treatment(Reference Delmas, Eastell and Garnero11–Reference Burnett-Bowie, Saag and Sebba16). An updated position statement by the IOS/IFCC Expert Group in 2025(Reference Bhattoa, Vasikaran and Trifonidi17) clarified terminology, pre-analytical variability and quantified the effects of these bone turnover markers (BTM) on risk of fracture. In a meta-analysis of the observational studies included in the recent IOS/IFCC report(Reference Bhattoa, Vasikaran and Trifonidi17), 1 sd higher plasma levels of P1NP or CTX were each associated with hazard ratios (95 % CI) of fracture of 1·30 (1·18, 1·43) and 1·21 (1·10, 1·33), respectively, with little attenuation after additional adjustment for a wide range of covariates. Short-term changes in plasma levels of BTM following bisphosphonate treatment also predicted long-term responses in BMD(Reference Burnett-Bowie, Saag and Sebba16). While vitamin D is a hormone that controls absorption of dietary Ca and mineralisation of bone, the effects of vitamin D on osteoblast or osteoclast activity in the bone microcellular unit have yet not been established. We hypothesised that if supplementation with vitamin D could reduce plasma levels of BTM, it could predict treatment responses to vitamin D that could be confirmed in further trials of vitamin D for the prevention of fracture in older people.
The present report used stored plasma samples from the BEST-D trial to measure plasma levels of BTM before and after supplementation with vitamin D or placebo(Reference Hin, Tomson and Newman10). In order to maximise the statistical power to detect effects of supplementation with vitamin D on BTM, we combined the results of the BEST-D trial with all previous trials of vitamin D in a meta-analysis assessing effects on plasma levels of BTM in community-dwelling older people. The aims of the present report were (i) to assess the effects of vitamin D on plasma levels of P1NP and CTX in stored blood samples in the BEST-D study population and (ii) to examine the effects of vitamin D on plasma levels of P1NP and CTX in a meta-analysis of all publicly available trials of vitamin D in community-dwelling older people.
Methods
The Biochemical Efficacy and Safety Trial of vitamin D trial
Details of the design and methods used in the BEST-D trial have been previously reported(Reference Watts and Manson3,Reference Hin, Tomson and Newman10) . Briefly, BEST-D was a double-blind, randomised, placebo-controlled parallel group trial comparing the effects of daily supplementation with 4000 IU daily or 2000 IU daily of cholecalciferol (vitamin D3) or placebo administered over a 12-month period between 24 September 2012 and 14 March 2013. The two co-primary outcomes were plasma levels of biochemical markers of vitamin D status and the proportion of individuals with plasma levels of 25(OH)D greater than 90 nmol/l at 12 months. Other outcomes included cardiovascular risk factors and clinical tests of physical function. The study recruited 305 community-dwelling men and women aged 65 years or older from a single general practice in Banbury, Oxfordshire, UK. Participants were required to be ambulatory and not to consume greater than 400 IU vitamin D daily prior to enrolment in the trial and were not taking medication for osteoporosis, but no baseline measures of BMD were sought. Randomisation used minimisation to ensure balance of age and sex in each allocated treatment groups. Vitamin D3 or matching placebo was administered as soft gel capsules provided by Tishcon Corporation. Volunteers were to take 4000 IU/d or 2000 IU/d of vitamin D3 or matching placebo and were followed up for 1 year. Overall, 93 %, 93 % and 85 % reported doing so at 12 months. The BEST-D trial received approval from the National Research Ethics Service (NRES) Committee South Central Oxford B (REC reference: 12/SC/0243), the Thames Valley Primary Care Research Partnership and a Clinical Trial Authorisation from Medicines and Healthcare products Regulatory Agency (MHRA) and is included in the National Institute for Health Research (NIHR) Trial portfolio. The protocol for BEST-D was also registered with the European Union Drug Regulating Authorities Clinical Trials Database (EudraCT: 2011-005763-24). All participants provided written informed consent.
Biochemical markers of osteoporosis
A 10-ml non-fasting EDTA blood sample was collected for central laboratory analysis at the randomisation and 12-month visit in 101 placebo-allocated participants and 102 participants per group allocated 2000 IU or 4000 IU vitamin D3 daily in 2012. Blood samples were collected at whatever time participants attended for their study visit and centrifuged (2100 g) within 4 h of blood collection at a local centre. Aliquots of 1 ml of EDTA plasma were stored frozen at −80℃ prior to shipment on dry ice to the NDPH Wolfson laboratory where they were stored in liquid N2 until analysis in 2022. Plasma levels of P1NP and CTX were measured at the Wolfson laboratory in the EDTA plasma using electrochemiluminescence immunoassays on a Roche Cobas C601 analyser (Roche Diagnostics) using manufacturers’ reagents, calibrators and settings. Previously published studies (supported by additional unpublished studies conducted in our laboratory) confirmed long-term stability of plasma lipids and other clinical chemistry biomarkers that have been stored at −80℃ up to 13 years, but no data are available on long-term stability of CTX and P1NP(Reference Muzakova, Beekhof and Jansen18).
Statistical analyses
Assessments were conducted according to the intention-to-treat principle as outlined in the pre-specified analysis plan for primary and secondary outcomes in the original statistical analysis plan for BEST-D(Reference Hin, Tomson and Newman10). Comparisons of mean follow-up plasma levels of P1NP and CTX between treatment arms in BEST-D (either dose v. placebo) involved ANCOVA adjusted for the baseline levels (with multiple imputation used to impute missing data, with ten replicate sets and combination across sets using Rubin’s methods(Reference Rubin19). Due to their positively skewed distributions, analyses were conducted on a natural logarithmic scale for both biomarkers, with the baseline-adjusted mean follow-up levels subsequently transformed and presented as geometric means with approximate standard errors (where the approximate standard error of each geometric mean was estimated as the width of the 95 % CI for the geometric mean divided by 3·92). All p-values were two-sided. The sample size for BEST-D was selected to detect an 11 nmol/l difference in mean plasma 25(OH)D levels after 12 months between 100 µg/daily and 50 µg/daily vitamin D3 doses as co-primary outcomes, and the pre-specified secondary outcomes assessed effects of the combined two active doses of vitamin D3 v. placebo on plasma levels of 25(OH)D. With 204 participants allocated either dose of vitamin D3 and 101 allocated placebo, the trial had 80 % power at 2p = 0·05 to detect a 0·34 sd difference in PINP and CTX.
To assess the results of vitamin D on BTM in BEST-D in the context of all previously reported trials, we performed a systematic review and meta-analysis (with the protocol registered on PROSPERO CRD42022360277). Briefly, we searched PubMed and the Cochrane Central Register of Controlled Trials for relevant English-language reports published before 1 August 2022. Search terms included BTM, vitamin D and randomised controlled trials (online Supplementary Table S1). The study findings were reported according to the Preferred Reporting Items for Systematic Reviews (PRISMA)(Reference Moher, Liberati and Tetzlaff20). Randomised trials were eligible for inclusion if they met the following criteria: (i) comparisons of effects of vitamin D (+/– Ca) with placebo; (ii) treatment duration greater than 8 weeks; and (iii) measurement of mean blood levels of either P1NP or CTX or both before and after allocation to treatment with vitamin D or placebo. All randomised placebo-controlled trials were included, regardless of number of participants or dose of vitamin D, but trials using foods fortified with vitamin D were excluded. In addition, trials were excluded if participants were aged < 18 years or reported using additional treatments for osteoporosis or vitamin D supplements or commencing new treatments as part of the study (e.g. HIV treatment or steroids). Studies of selected patient groups were also excluded to minimise effects of other diseases on BTM(Reference Delmas, Eastell and Garnero11), including participants with chronic kidney disease or end-stage renal failure, pregnancy or a recent fracture (< 1 year). The results were recorded using a PRISMA flow diagram (online Supplementary Figure S2).
Data were extracted by two authors (CSA and JH) on trial author, year of publication, country and setting, number of participants (number enrolled and separately number completing treatment), sex, age, ethnicity, duration of treatment, use of placebo, blinding, details of whether samples were fasting/non-fasting, and pre- and post-treatment plasma levels of 25(OH)D, P1NP or CTX and vitamin D (+/– Ca) dose. If results of multiple follow-up periods were included, the results of the longest duration of follow-up were extracted. For trials that included multiple dosing regimens of vitamin D, the results for each dose were collected. Risk of bias (quality) assessment was carried out using a Cochrane Collaboration Risk of Bias tool (ROB2)(Reference Sterne, Savović and Page21) following data extraction. A risk of bias was conducted by one reviewer and then repeated on a random sample of trials by a second reviewer.
Data were converted so that all BTM markers were reported using the most frequently used units (ng/ml for both CTX and P1NP). For each trial, we extracted the mean (se) percentage change in levels of each BTM (comparing before v. after treatment) for each treatment group. The absolute differences between these two percentage changes (and their standard errors, and hence their 95 % CI) were then estimated for each trial. An inverse-variance-weighted meta-analysis of the estimates in the individual trials was then performed; such an analysis is valid irrespective of any true heterogeneity that may or may not exist between the effects in the different trials(Reference Bossuyt, Deeks and Leeflang22). Subgroup analyses were subsequently conducted to investigate possible sources of heterogeneity between results of individual trials. Subgroups included trials of treatment with vitamin D with or without additional Ca supplements, dose of vitamin D used (< 1500 IU and > 1500 IU) and trial duration (≤ 6 months and > 6 months). Sensitivity analyses were conducted by excluding trials in which study participants reported long-term use of steroids.
Results
Effects of vitamin D on procollagen type 1 N-propeptide and C-terminal telopeptide of type 1 collagen in the Biochemical Efficacy and Safety Trial of vitamin D trial
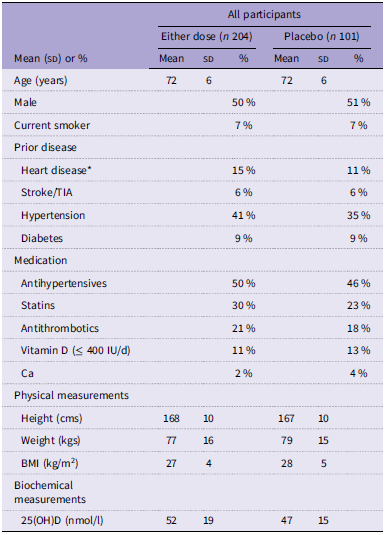
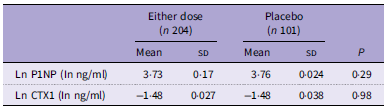
The baseline characteristics of the BEST-D study participants at randomisation by allocated treatment are shown in Table 1. The minimisation procedures used for randomisation ensured that the participants were well matched by allocated treatment. The mean age of study participants was 72 years, and about 50 % were women. A total of 102 participants were allocated to 4000 IU/d of vitamin D, 102–2000 IU/d, and 101 were allocated to placebo daily. Plasma levels of 25(OH)D increased from 53 nmol/l (se 2·41) to 100 nmol/l (se 1·73) or 135 (se 1·73) after 12 months for those allocated to 2000 IU/d and 4000 IU/d, respectively(Reference Watts and Manson3). The results for baseline-adjusted geometric mean plasma levels of P1NP and CTX at 12 months are provided in Table 2. Geometric mean (approximate se) levels at 12 months were similar for P1NP (41·7 (0·7) v. 42·9 (1·0) ng/ml; P = 0·29) and likewise for CTX (0·23 (0·01) v. 0·23 (0·01) ng/ml; P = 0·98) for either dose of vitamin D v. placebo, respectively.
Selected characteristics at randomisation in the BEST-D trial, by allocated treatment

BEST-D, Biochemical Efficacy and Safety Trial of vitamin D; 25(OH)D, 25-hydroxy-vitamin D.
Mean (sd) or % are shown.
*Defined as heart attack, angina or heart failure.
Effect of allocation to vitamin D3 v. placebo on plasma levels of P1NP CTX in the BEST-D trial

P1NP, procollagen type 1 N-propeptide; CTX, C-terminal telopeptide of type 1 collagen; BEST-D, Biochemical Efficacy and Safety Trial of vitamin D.
Values shown are the geometric mean (sd) levels after 12 months of treatment, by allocated treatment.
Meta-Analyses of trials of vitamin D on procollagen type 1 N-propeptide and C-terminal telopeptide of type 1 collagen
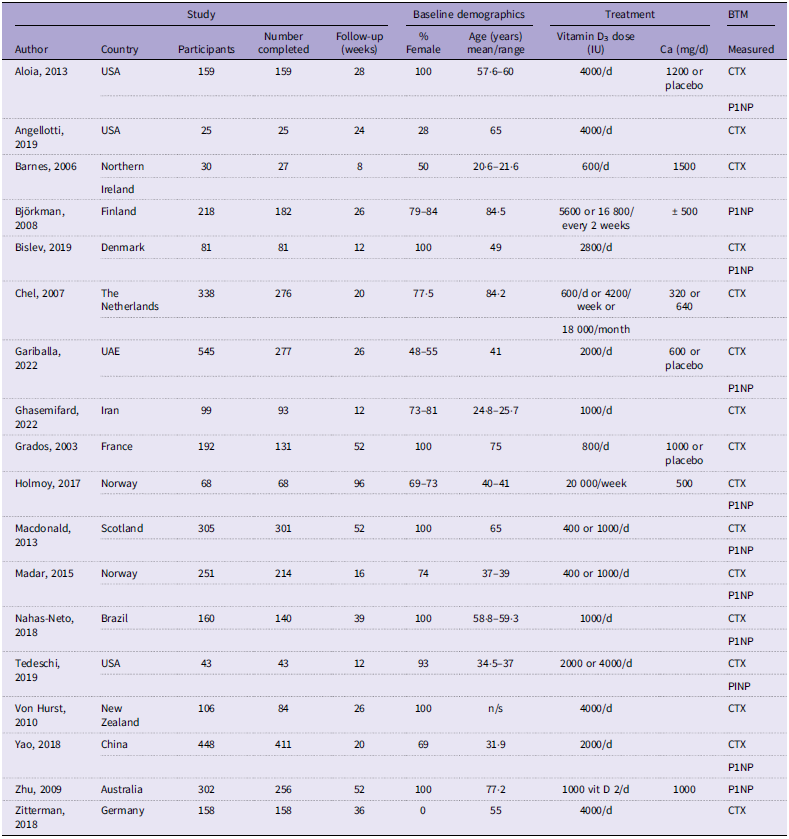
Details of the systematic review are provided using a PRISMA 2020 flow diagram(Reference Moher, Liberati and Tetzlaff20) (online Supplementary Figure S1). The initial search identified 1673 reports, which included 466 duplicates. After review of titles and abstracts, seventy-one reports were identified for retrieval. Overall, a total of eighteen trials, involving 2750 participants, assessed effects on plasma levels of CTX, and there was little heterogeneity between results of individual trials in these meta-analyses. Selected characteristics of the eighteen eligible trials are shown in Table 3. The sample sizes in the included trials assessing effects on CTX varied from 25 to 545. Overall, a total of thirteen trials involving 2735 assessed effects of vitamin D on plasma levels of P1NP. In assessments of trial quality for the eighteen trials, four trials were graded as having a high risk of bias, thirteen as having some concern of bias and one trial as having a low risk of bias (online Supplementary Figure S2).
Characteristics of included trials in meta-analyses of vitamin D v. placebo on plasma levels of P1NP and CTX, respectively

Effects on plasma levels of procollagen type 1 N-propeptide and C-terminal telopeptide of type 1 collagen in meta-analyses of all trials
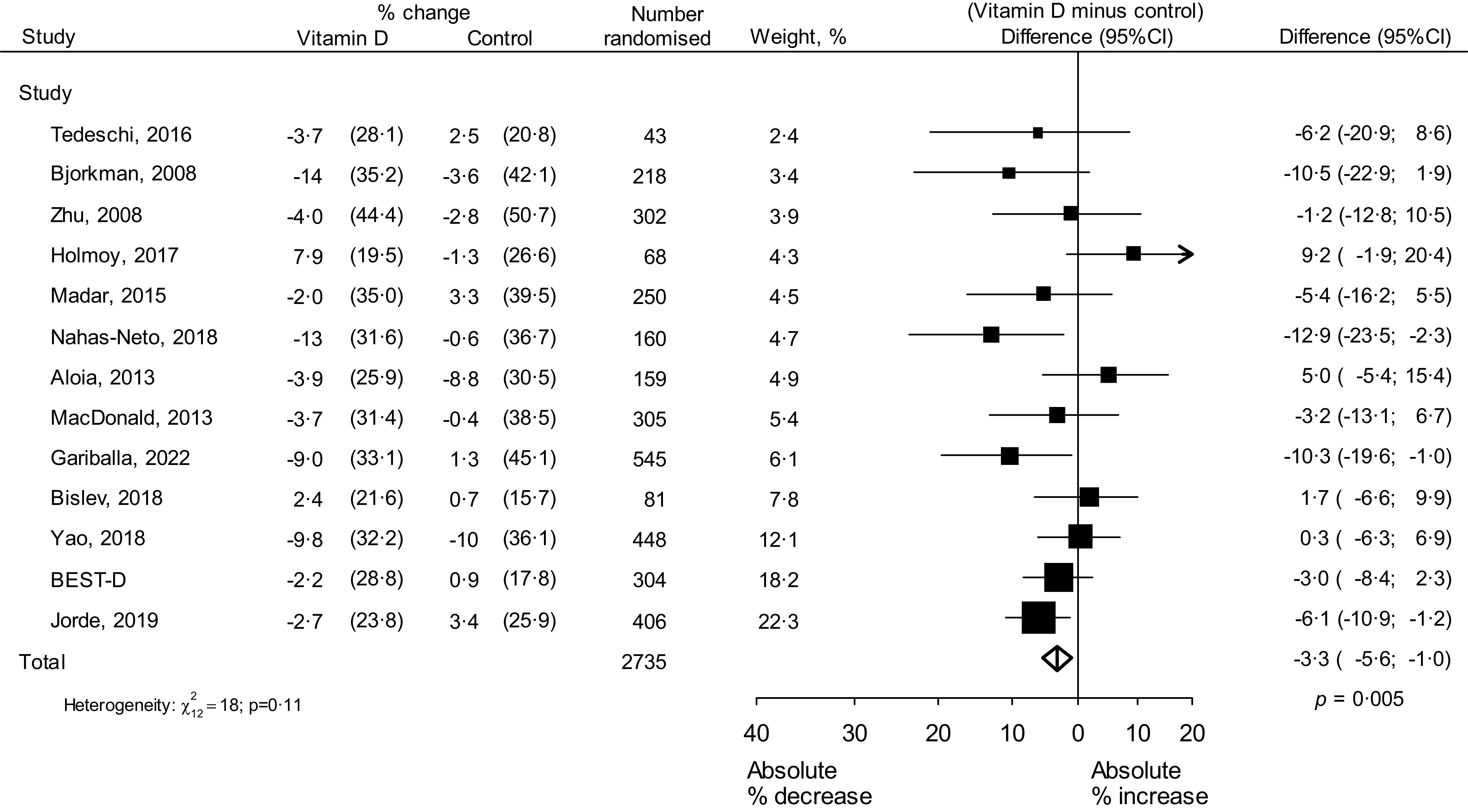
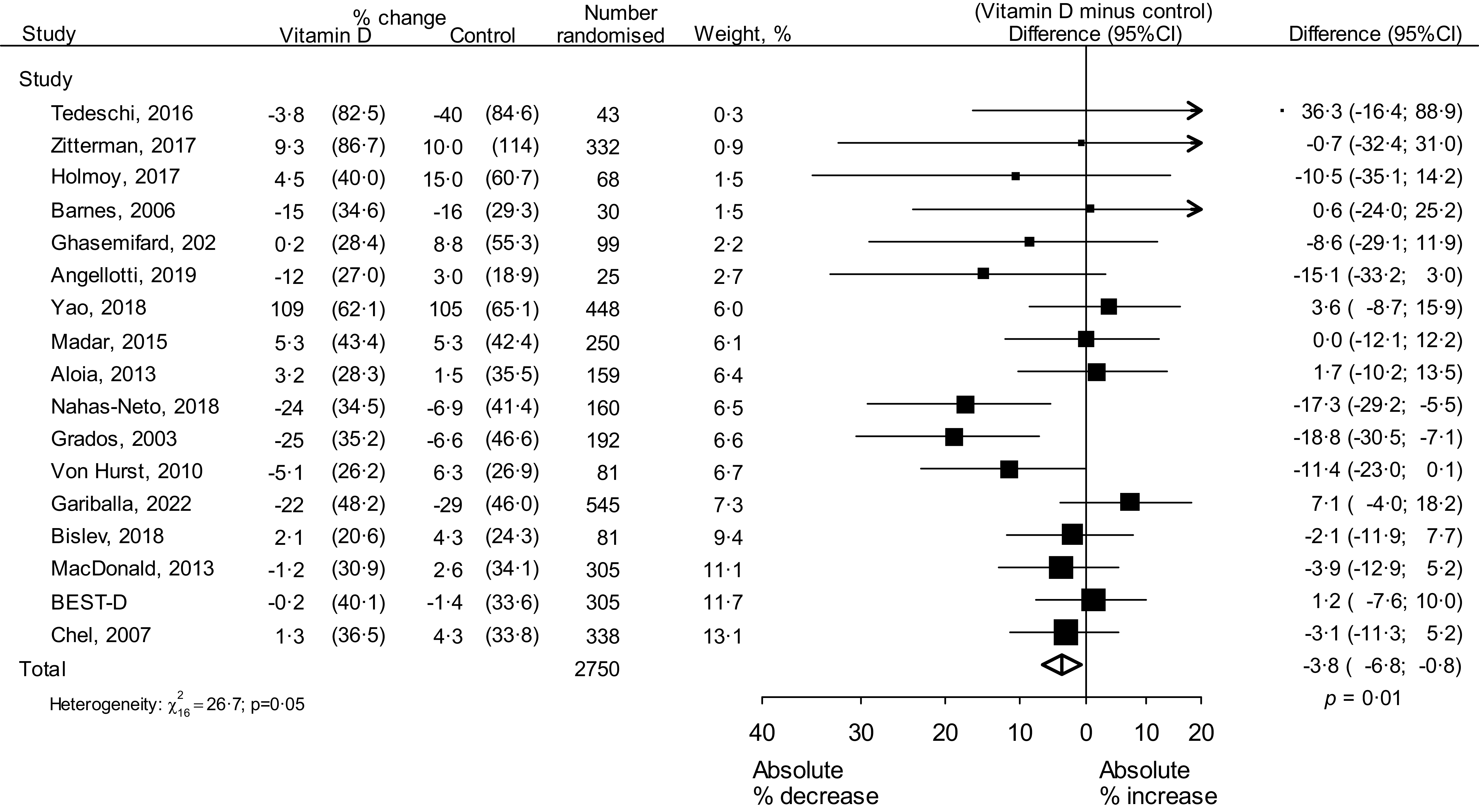
Among the thirteen trials, involving 2735 participants that assessed effects of vitamin D on plasma levels of P1NP, the average difference between the within-trial change in P1NP for patients allocated vitamin D and the within-trial change in P1NP for patients allocated control (i.e. vitamin D minus control) was −3·3 percentage points (95 % CI −5·6, −1·0, P < 0·005) (Figure 1). There was no significant heterogeneity between the results of the individual trials. Among the eighteen trials, involving 2750 participants with plasma levels of CTX, this average difference in CTX was slightly greater than for P1NP (average absolute difference −3·8 percentage points (95 % CI −6·8, −0·8); P = 0·01) (Figure 2), with some evidence of heterogeneity possibly reflecting residual uncontrolled bias in the individual trials.
Meta-analysis of randomised trials of vitamin D v. placebo on plasma levels of P1NP. The area of each box is proportional to the amount of statistical information (i.e. inversely proportional to the variance of the estimated difference) and the lines through the boxes denote 95 % CI. The arrow to the right-hand side means that the upper CI limit is beyond the range shown. The diamond reflects the overall summary of the effect of vitamin D on P1NP across all trials. P1NP, procollagen type 1 N-propeptide; BEST-D, Biochemical Efficacy and Safety Trial of vitamin D.

Meta-analysis of randomised trials of vitamin D v. placebo on plasma levels of CTX. The area of each box is proportional to the amount of statistical information (i.e. inversely proportional to the variance of the estimated difference), and the lines through the boxes denote 95 % CI. Arrows to the left- or right-hand side mean that the CI limits are beyond the range shown. The diamond reflects the overall summary of the effects of vitamin D on CTX across all trials. CTX, C-terminal telopeptide of type 1 collagen; BEST-D, Biochemical Efficacy and Safety Trial of vitamin D.

Subgroup analyses
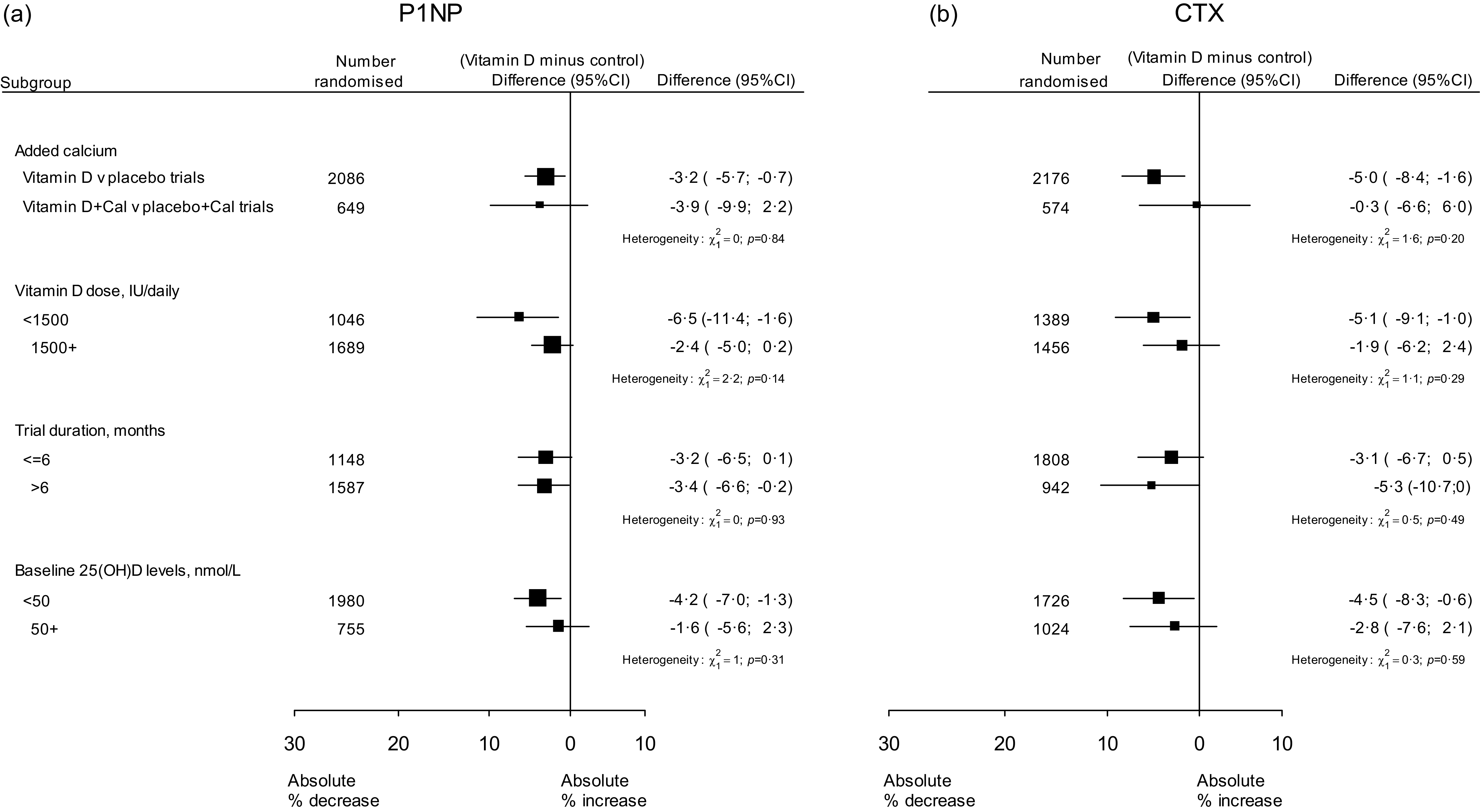
Stratifying trials of vitamin D by concomitant use of Ca supplements did not yield a greater reduction in plasma levels of P1NP among those with added Ca v. those with vitamin D alone (−3·6 % (−9·6, 2·4) v. −3·2 % (−5·7, −07); P for heterogeneity = 0·84), respectively (Figure 3, online Supplementary Figure S3). Conversely, stratifying trials of vitamin D only v. trials of vitamin D plus Ca did not suggest any greater reduction in plasma levels of CTX (P for heterogeneity = 0·01: online Supplementary Figure S4). Stratifying trials by dose of vitamin D (1500 IU v. ≥ 1500 IU daily) resulted in no heterogeneity in reduction in plasma levels of P1NP (P = 0·14) or on CTX (P = 0·29): Figure 3, online Supplementary Figures S5 and S6). Stratifying trials of vitamin D by trial duration did not indicate any differential effects on either plasma levels of P1NP or CTX (Figure 3, online Supplementary Figures S7 and S8). In addition, stratifying trials of vitamin D by trials after excluding trials of vitamin D in populations selected on the basis of a prior disease did not suggest any differential effects on either plasma levels of P1NP or CTX (online Supplementary Figures S9 and S10). Likewise, stratifying trials of vitamin D by baseline plasma levels of 25(OH)D (< 50 nmol/l v. ≥ 50 nmol/l) demonstrated no greater reduction of vitamin D on plasma levels of P1NP (−4·2 % (−7·0, −1·3) v. −1·6 % (−5·6, 2·3), P = 0·31) and likewise for CTX (−4·5 (−8·31, −0·6) v. −2·8 (−7·6, 2·1) P = 0·59) (Figure 3, online Supplementary Figures S11 and S12).
Meta-analysis of trials of randomised vitamin D on plasma levels of P1NP and CTX, by relevant subgroups. The figure shows, for various subgroups of trials, the absolute differences between the mean percentage change in P1NP and CTX from baseline to follow-up among those allocated vitamin D and the mean percentage change in P1NP and CTX from baseline to follow-up among those allocated control. The heterogeneity tests assess if response to treatment differ by trial-level characteristics. P1NP, procollagen type 1 N-propeptide; CTX, C-terminal telopeptide of type 1 collagen.

Discussion
The results of the BEST-D trial, involving 305 healthy older adults, showed that daily dietary supplementation with high-dose vitamin D did not have any significant effects on plasma levels of P1NP or CTX compared with placebo over a 12-month period. However, a meta-analysis of thirteen randomised trials of vitamin D, involving a total of 2735 participants, demonstrated that allocation to vitamin D was associated with a 3·3 % (95 % CI 1·0, 5·6) reduction in plasma levels of P1NP. For CTX, a meta-analysis of eighteen trials, involving a total of 2695 participants, demonstrated that allocation to vitamin D was associated with a 3·8 % (0·8, 6·8) reduction in plasma levels of CTX. In subgroups of this meta-analysis, allocation to vitamin D was not associated with any differences in percent reductions in either plasma levels of P1NP or CTX in trials that used concomitant Ca supplements or used doses of vitamin D < 1500 IU of vitamin D daily than those with higher doses of vitamin D or had variable duration of treatment or in trial populations with plasma levels of 25(OH)D < 50 mol/l v. > 50 nmol/l, respectively. Unfortunately, it was not possible to assess the effects of vitamin D on plasma levels of BTM separately by sex or by fasting status due to lack of available data.
The recent IOS/IFCC position statement on BTM for prediction of fracture(Reference Bhattoa, Vasikaran and Trifonidi17) reported that plasma levels of P1NP predict fracture. It also reported that levels of P1NP are stable in whole blood for up to 72 h after centrifugation and that blood sampling can be collected at any time of the day regardless of fasting or hours since last meal. In contrast, the same report highlighted that higher plasma levels of CTX also predict higher risk of fracture but are constrained by a substantial circadian variation with the highest CTX levels on awakening in the morning that increase by 20 % after breakfast. While CTX levels should ideally be measured after an overnight fast in blood samples collected in the mornings, the trials were assessing randomised differences between the groups that were collected using the same procedures(Reference Bhattoa, Vasikaran and Trifonidi17).
The BEST-D study had several strengths including treatment of 305 older people with high-dose vitamin D for 12 months, but blood samples were collected in non-fasting blood samples between 09.00 and 17.00, which may be sub-optimal for the stability of CTX. The chief strength of the meta-analyses of vitamin D trials assessing effects on P1NP in 2654 participants and CTX in 2695 participants, respectively, included the large number of participants studied and wide range of relevant subgroups analysed. The randomisation should have avoided many of the issues resulting from different times of the day of blood sample collection. Taken together, the findings provided support for prediction of modest treatment responses to vitamin D for the prevention of fractures in high-risk populations. Unfortunately, it was not possible to stratify the tabular data results in the meta-analysis of the trials by sex, as the sex-specific results were not routinely provided in most individual trials. While plasma levels of CTX have a substantial circadian variability (with a 2-fold higher night-time compared with day-time plasma levels of CTX)(Reference Bischoff-Ferrari, Kiel and Dawson-Hughes5), variability in response to assay platforms and variability in response to hours since last meal, P1NP is unaltered by time of day or hours since last meal(Reference Bhattoa, Vasikaran and Trifonidi17). Among the included trials in the meta-analysis, five trials did not use fasting samples and most trials did not record information on whether samples were collected in the fasting state or indicate timing of blood collection.
Importantly, plasma levels of BTM are increasingly being used to assess responses to specific treatments for osteoporosis, with trials demonstrating that early changes in BTM predict a long-term response in BMD(Reference Eastell and Hannon23–Reference Ravn, Thompson and Ross26). However, the changes in plasma levels of BTM in response to other osteoporosis treatments are substantially greater than those observed for vitamin D, even at the high doses used in the BEST-D trial. It is suggested that to predict a positive BMD response, a (about 3 %) higher CTX level would need to reduce BMD by 35 % to –55 %(Reference Bischoff-Ferrari, Kiel and Dawson-Hughes5). Previous meta-analyses of studies of BTM and fracture risk demonstrated a moderate but significant positive associations of higher plasma levels of P1NP and CTX levels with incidence of fracture after adjusting for BMD and clinical risk factors(Reference Tian, Ma and Feng14,Reference Johansson, Odén and Kanis15) . However, it is not known if more modest changes in BTM could affect BMD or risk of fracture(Reference Eastell and Hannon23–Reference Christgau, Bitsch-Jensen and Hanover Bjarnason30). Likewise, given the small differences in the effects of vitamin D on P1NP and CTX observed in the present meta-analysis of all available trials, there are insufficient data to recommend vitamin D based on changes in BTM levels alone observed in the present meta-analyses. Our previous meta-analysis of eleven trials of vitamin D supplementation alone did not find a reduced risk of any fracture, but a meta-analysis of six trials of combined supplementation with vitamin D and Ca demonstrated a 6 % reduction in risk of any fracture (RR 0·94 (95 % CI 0·89, 0·99)) and a 16 % reduction in hip fracture (0·84 (0·72, 0·97))(Reference Yao, Bennett and Mafham9). The results of the present meta-analysis provide support for further trials of high doses of vitamin D in populations with low plasma levels of 25(OH)D. Further trials of vitamin D for the prevention of fracture are required in postmenopausal women or older people of either sex, nursing home residents or ethnic groups with low plasma 25(OH)D levels, to provide reliable evidence for the efficacy and safety of supplementation with vitamin D for the prevention of fracture and other health outcomes.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526107193
Acknowledgements
The authors would like to thank all staff in the BEST-D Trial Collaborative Group and participants in the trial.
Tishcon Corporation (Westbury, NY, USA) donated the active and placebo vitamin D capsules. The British Heart Foundation (PG/12/ 32/29544) and the British Heart Foundation Centre for Research Excellence provided partial funding for the study. The Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU) at the University of Oxford receives funding from the UK Medical Research Council, the British Heart Foundation and Cancer Research UK. The authors acknowledge funding from the University of Oxford Medical Sciences Pump-Priming scheme awarded to the Nuffield Department of Population Health.
J. A. and R. J. C. designed the BEST-D trial. J. A. and R. J. C were Co-PIs for the trial and conceived the study design and obtained funding to conduct the study. H. H. supervised the recruitment of study participants and data collection and was in charge of all contact with study participants. M. H. conducted measurements of plasma levels of P1NP and CTX and all other assays in the trial. R. J. C. and J. A. jointly supervised C. S. A. to conduct a meta-analysis of the randomised trials. J. H. and J. E. performed the statistical analyses. C. S. A. wrote the first draft of this report, and all other authors contributed revisions to the report.
None of the authors have any conflicts of interest in relation to this report.



 Open access
Open access