


Background and rationale
Multiple sclerosis (MS), which affects approximately 2·9 million people worldwide(1), is an autoimmune disease that causes central nervous system lesions, leading to physical, cognitive and various other neurological symptoms(Reference McGinley, Goldschmidt and Rae-Grant2). Although several types of the disease have been identified, approximately 85 % of cases are classified as relapsing-remitting MS (RRMS)(Reference Śladowska, Kawalec and Holko3).
It has been reported that symptoms commonly observed in individuals with MS – such as fatigue, cognitive impairment and depression – may negatively affect quality of life to a degree comparable to physical disability(Reference Bergmann, Becker and Watts4). Significant advances have been achieved in the treatment of the disease over the past two decades(Reference Cree, Oksenberg and Hauser5). Currently, treatment goals include preventing both the symptoms and the progression of the disease(Reference Śladowska, Kawalec and Holko3). Lifestyle modifications appear to be promising in this regard(Reference Stoiloudis, Kesidou and Bakirtzis6).
It is possible to improve the quality of life of patients with MS through lifestyle modifications(Reference Stoiloudis, Kesidou and Bakirtzis6–Reference Pivovarova-Ramich, Zimmermann and Paul9). In recent years, with the recognition of the positive effects of nutrition on the disease, patients have often tended to change their dietary habits after being diagnosed(Reference Armon-Omer, Waldman and Simaan10–Reference Esposito, Sparaco and Maniscalco12).
There are several dietary models recommended for patients with MS(Reference Simpson-Yap, Nag and Jakaria13,Reference Zielińska and Michońska14) . Based on the findings of previous studies, the recommendations primarily point to the Mediterranean diet(Reference Zielińska and Michońska14–Reference Ertaş Öztürk, Helvaci and Sökülmez Kaya19) and the MIND diet, which combines the Mediterranean and Dietary Approaches to Stop Hypertension diets(Reference Morris, Tangney and Wang20,Reference Noormohammadi, Ghorbani and Naser Moghadasi21) .
It has been suggested that the MIND diet may be effective in reducing the risk of developing neurodegenerative diseases and in improving cognitive functions and depression(22). Considering that cognitive impairment affects approximately 40–65 % of individuals with MS(Reference DeLuca, Chiaravalloti and Sandroff23) and has serious adverse effects on daily life functioning, it can be anticipated that the MIND diet may have beneficial effects for this patient group. However, studies investigating the implementation of the MIND diet in individuals with MS are quite limited(Reference Noormohammadi, Ghorbani and Naser Moghadasi21,Reference Kheirouri and Alizadeh24,Reference Navarrete-Pérez, Gómez-Melero and Escribano25) .
Based on these data, we present the protocol of a randomised controlled trial planned to investigate the effects of implementing a MIND or standard diet program in RRMS patients on disease-related symptoms.
Objectives
The primary objective of this study is to determine the effects of implementing a MIND diet v. a standard diet program in patients with RRMS on disease-related outcomes, including reduced quality of life increased fatigue, impaired cognitive function and brain fog.
The secondary objective is to evaluate the effects of implementing a MIND diet v. a standard diet program in patients with RRMS on anthropometric measures (weight, height, body fat percentage and neck, waist and hip circumferences) and blood parameters, including complete blood count, biochemical markers (fasting glucose, lipid profile, liver enzymes and albümin), C-reactive protein, thyroid hormones (T3, T4 and thyroid-stimulating hormone) and micronutrient status (folate, vitamin B12 and vitamin D).
Research hypotheses
H1a: The quality of life levels of the experimental group following the MIND diet and the control group following the standard diet program are not similar.
H1b: The fatigue levels of the experimental group following the MIND diet and the control group following the standard diet program are not similar.
H1c: The cognitive function levels of the experimental group following the MIND diet and the control group following the standard diet program are not similar.
H1d: The brain fog scale scores of the experimental group following the MIND diet and the control group following the standard diet program are not similar.
Method
The protocol was written in accordance with the updated Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidelines(Reference Chan, Boutron and Hopewell26). The SPIRIT 2025 checklist is presented in Appendix 1, the roles and responsibilities of the coordinating center and the individuals overseeing the study are presented in Appendix 2.
Patient and public involvement
Due to the study being planned as a single-centre study and the inability to establish a structure that would represent the population, patient and public involvement was not planned during the design, conduct and reporting stages of this study. However, after the study results are reported, they will be shared with patients and the public.
Trial design
The study is a single-centre, parallel-group (1:1), open-label, randomised controlled trial. Patients who are eligible and agree to participate will be randomly assigned to one of two groups for the 12-week intervention (I. MIND Diet and II. Standard Diet). The intervention duration is 12 weeks. Outcome measures will be assessed immediately before and after the 12-week intervention period.
Trial setting
The study will be conducted as a single-centre study at the Neurology Outpatient Clinic of Muğla Training and Research Hospital in Muğla Province, Türkiye. Participants will be determined among RRMS patients registered at the hospital and attending for routine follow-up visits, in accordance with the principle of voluntariness. The measurements and procedures to be performed during the patients’ initial and final visits (anthropometric measurements, administration of the MSQOL-54 questionnaire, the MFIS scale, the BICAMS battery and the brain fog scale) will be carried out in a room allocated by the institution. The patients’ blood tests are performed by the Neurology Outpatient Clinic of Muğla Training and Research Hospital during routine follow-up visits and are analysed in the hospital laboratory in accordance with standard clinical procedures. The preparation of the patients’ dietary interventions (I. MIND Diet, II. Standard Diet) will be explained via an online video call planned to last 30–45 min on the evening of the initial visit day, and the diet will be sent by e-mail to the patient or their relative (child, sibling, etc.).
Sample size
The study population consists of 327 RRMS patients registered at the hospital. Patients will be included in the study on a voluntary basis. A power analysis was conducted to determine the sample size, and calculations were performed using the G * Power program (version 3.1.9.2, Universität Düsseldorf, Düsseldorf, Germany). To support the sample size assumption, the mean (sd) values reported in the reference study(Reference Moravejolahkami, Paknahad and Chitsaz16) for the 3-month General Quality of Life subscale of the MSQOL-54 (intervention group: 63·2 (sd 5·0); control group: 52·7 (sd 12·8)) were taken as the basis, and the standardised effect size derived from these values was calculated as Cohen’s d = 1·05; this value corresponds to a large effect according to Cohen’s classification (d ≥ 0·80). However, adopting a more conservative assumption, an effect size of d = 0·80 was used for the sample size calculation(Reference Cohen27). Accordingly, for a two-arm parallel-group (1:1) design, assuming a two-sided significance level of α = 0·05 and statistical power of 1 − β = 0·80 for comparing the means of two independent groups using a two-sided independent-samples t test, the minimum required sample size was determined as n 1 = 26 and n 2 = 26 (total n 52). Considering the potential for data loss, an additional 20 % attrition rate (5 patients per group) was included, and the target sample size was planned as a total of 62 RRMS patients (n 1 = 31 and n 2 = 31)(Reference Cohen28).
Participant eligibility criteria
The eligibility of RRMS patients who apply to the Neurology Outpatient Clinic will first be assessed by the investigator physician (diagnostic criteria, medication use and Expanded Disability Status Scale score). Patients deemed eligible by the investigator physician will be referred to the principal investigator, and their eligibility for the study will be checked (BMI, adherence to a special diet, use of dietary supplements). The criteria for determining participants’ eligibility and the criteria for withdrawal from the study are as follows.
Inclusion criteria;
1. Adult RRMS patients aged between 18 and 64 years
2. Having been diagnosed with RRMS at least three months prior
3. No change in disease-modifying therapy within the past 6 months
4. Patients who use their medications regularly
5. An Expanded Disability Status Scale score ≤ 6
6. Patients with a BMI between 18·5 and 29·9 kg/m2
Exclusion criteria;
1. RRMS patients who are pregnant or in the lactation period
2. Presence of another chronic metabolic disease
3. Individuals with limb deficiency
4. Individuals following a specific diet
5. Individuals using antidepressants or mood stabilisers
6. Individuals using nutritional supplements or dietary support products
Criteria for withdrawal from the study;
1. In at least three (25 %) of the weekly interviews, inability to reach the patient, inability to obtain the dietary intake record and/or determination of low adherence to the MIND diet (≤ 5 points)
2. Experiencing a relapse during the intervention
3. Change in disease-modifying therapy during the intervention
4. Initiation of any form of medical nutrition therapy for any reason during the intervention
5. Diagnosis of any chronic metabolic disease or cancer during the intervention
6. Pregnancy occurring during the intervention period
Participant recruitment
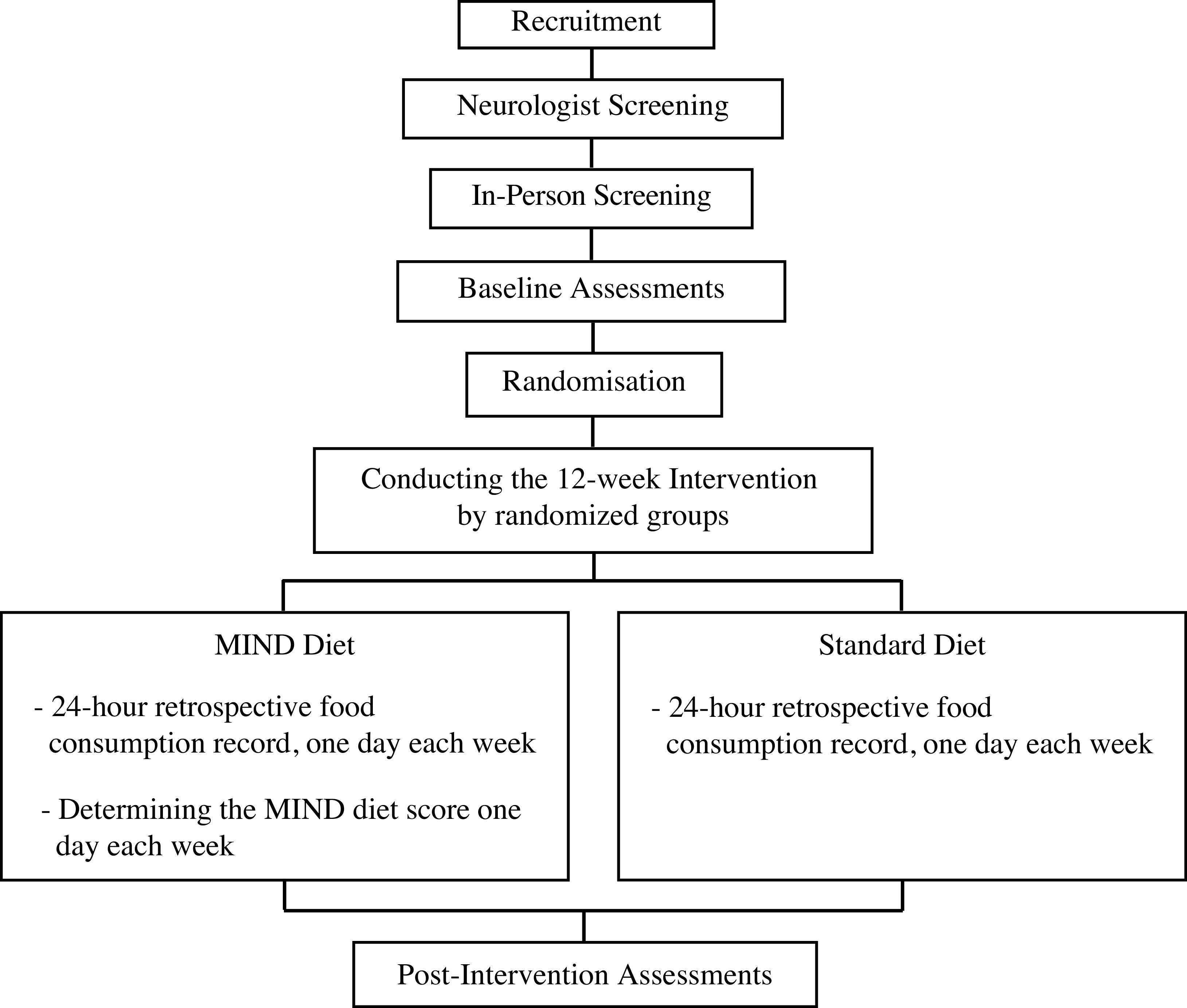
The patient recruitment strategy for the study will be that the neurologist investigator refers patients who are eligible in terms of diagnosis, medication and disability to the principalinvestigator. The BMI values of the patients referred to the investigator will be calculated, and their use of dietary supplements and whether they follow a special diet will be questioned. Patients who are eligible in terms of these conditions will be informed about the study. Interested individuals will be given the informed consent form (Appendix 3). A summary of the schedule of activities for participants is provided in Figure 1, and the full schedule is provided in Appendix 4.
Timing of screening, intervention and assessments. Primary and secondary outcomes will be assessed at baseline and week 13.

Randomisation
Block randomisation will be applied for allocating individuals who meet the inclusion and exclusion criteria and who consent to participate in the study to the study groups. ‘The Permuted Block Randomisation’ stage will be performed using a computer program by an independent researcher who does not have access to participants’ personal information. As the program randomly determines the order of participants using different block sizes (4 and 6), the principle of unpredictability will be achieved more strongly than in randomisation performed with fixed block sizes. The risk of selection bias with this method is minimal.
In accordance with the principle of voluntariness, each participant who meets the inclusion and exclusion criteria will be numbered in the order of enrollment and allocated to the intervention and control groups at a 1:1 ratio. Allocation information will be kept by another researcher who is not part of the study team. The principal investigator who will deliver the dietary intervention will remain unaware of the allocation until anthropometric measurements and the pre-test are completed. Allocation information – limited to the numbers of participants enrolled that day – will be disclosed at the end of each day by the researcher who holds the randomisation information to the researcher who will deliver the dietary intervention, immediately before the initiation of the dietary intervention. With this procedure, it is aimed to minimise potential allocation bias.
In order to preserve the between-group balance and the integrity ensured by randomisation, no additional participant recruitment is planned to replace participants who withdraw from or are excluded from the study during the post-randomisation intervention period. The loss-to-follow-up (missing data) rate was set at 20 % to maintain the statistical power of the study.
Blinding
Blinding” will not be performed due to the distinguishable nature of the dietary intervention for both participants and researchers, and the study will be conducted as an open-label randomised controlled trial. Statistical analyses will be carried out by a researcher independent of the research team. During the analysis process, groups will be coded in the dataset as ‘Group 1’ and ‘Group 2’, thereby blinding the researcher conducting the statistical analyses with respect to group allocation. After the analyses of the primary outcome measures are completed and reported, the group labels will be unblinded and blinding will be lifted.
Interventions and comparator
The intervention of this study is the MIND diet program for the intervention group and the standard diet program for the control group. Any occurrence of the situations listed in the withdrawal criteria section will affect the outcome outputs. In addition, for the same reason, initiating a new exercise program or starting nutritional or herbal supplements will not be recommended, and maintaining the current status will be requested.
MIND diet
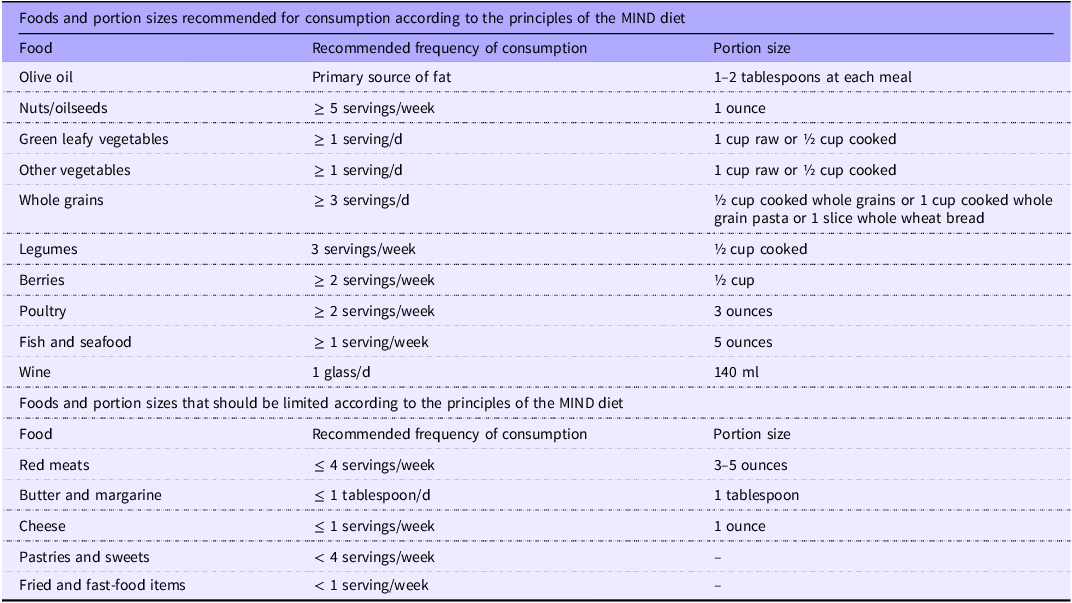
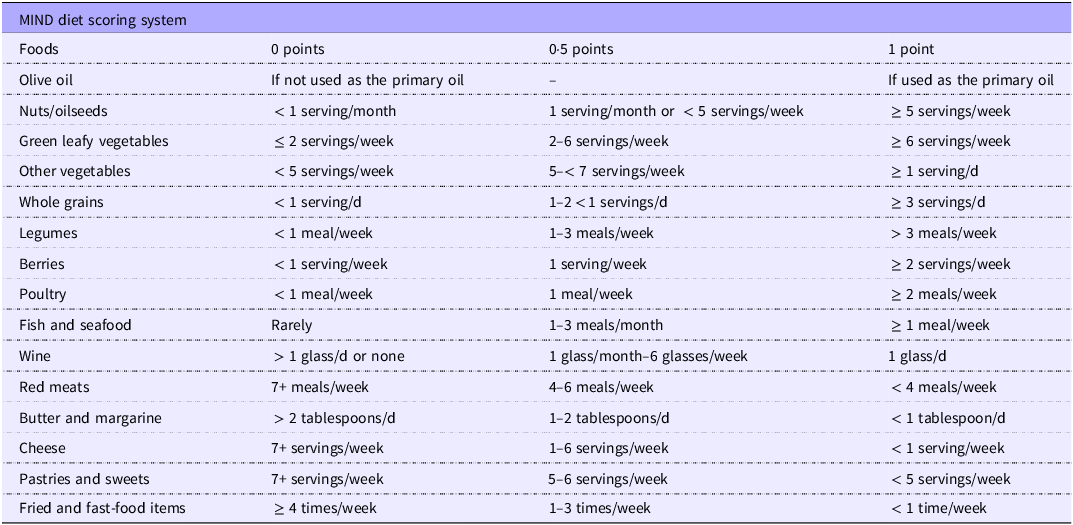
The MIND diet was developed in 2015 by nutritional epidemiologist Martha Clare Morris with the aim of preserving and enhancing cognitive function. It combines the principles of the Mediterranean diet and the Dietary Approaches to Stop Hypertension guidelines and has been suggested to be effective in reducing the risk of developing neurodegenerative diseases(22). Unlike the Mediterranean diet, the MIND diet emphasises increased consumption of fruits and green leafy vegetables while limiting cheese intake. The MIND diet consists of fifteen components, ten of which are considered brain-healthy and five of which are considered unhealthy(22). The principles and portion sizes of the MIND diet are presented in Table 1 (Reference Morris, Tangney and Wang20).
Principles and portion sizes of the MIND diet

Each patient’s diet will be individually prepared, and their energy requirements will be calculated using the Harris–Benedict Equation and the appropriate activity factor(Reference Mousavi-Shirazi-Fard, Mazloom and Izadi29). Of the total daily energy intake, 55 % will be obtained from carbohydrates, 15 % from proteins and 30 % from fats. The distribution of the diet throughout the day will be planned in accordance with the principles of the MIND diet to achieve the prescribed portion amounts. The diet plans will consist of three main meals and one snack.
Standard diet
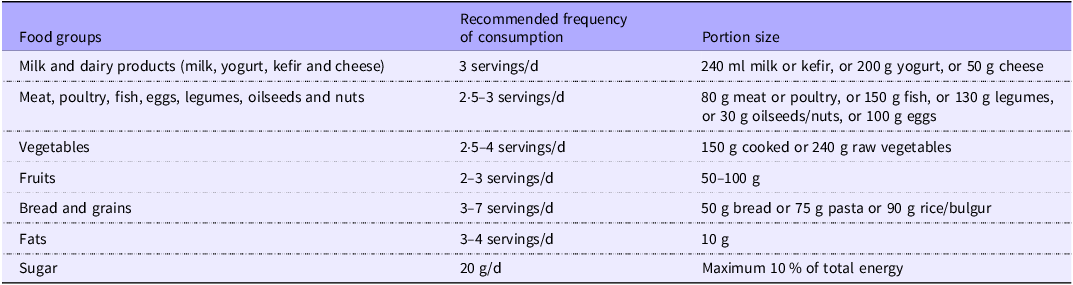
The standard diet program to be applied to the control group was planned in accordance with the Türkiye Dietary Guidelines (TÜBER)(30). The patients’ energy requirements will be calculated using the Harris–Benedict Equation with the addition of an activity factor(Reference Mousavi-Shirazi-Fard, Mazloom and Izadi29), and an isocaloric diet containing 55 % carbohydrates, 15 % protein and 30 % fat will be provided. The distribution of daily nutritional requirements across meals will be arranged in accordance with the principles outlined in TÜBER and tailored to individuals’ requirements (Table 2). Diet plans will be structured as three main meals and one snack. Participants will be asked to adhere to the planned diet for 12 weeks.
Foods and portion sizes recommended for consumption according to TÜBER
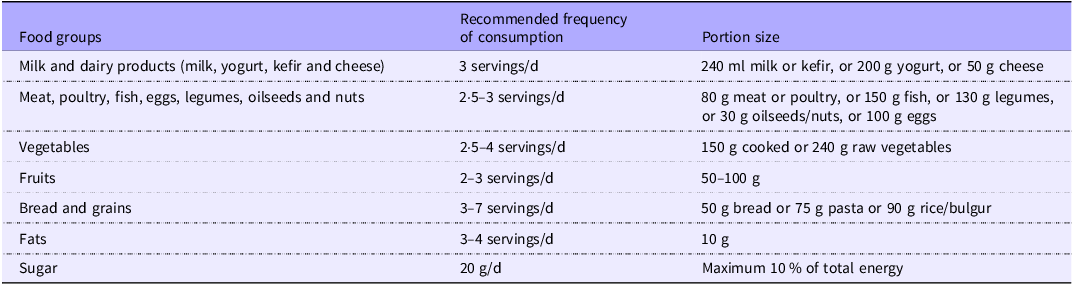
TÜBER, Türkiye Dietary Guidelines.
Delivery of dietary interventions and monitoring of compliance
The individually planned MIND diet and standard diet will be explained to the patients on the evening of the initial visit through an online video consultation lasting approximately 30–45 min, and the diet plan will be sent to the patient or their relative (child, sibling, etc.) via e-mail. Patients will be asked to adhere to their diets for 12 weeks. The primary goal is always to ensure optimal adherence to the diet. Therefore, participants will be regularly monitored through weekly online motivational interviews lasting approximately 30 min to assess their dietary compliance. Motivational interviewing is not merely a set of techniques but a communication method. Through motivational interviewing, it is possible to enhance an individual’s intrinsic motivation and focus on problem-solving(Reference Miller and Rose31). In this way, it also helps facilitate behavioural change(Reference Suire, Kavookjian and Feiss32). It is considered an important approach because it enables the adoption of desired nutritional behaviours and enhances adherence to the diet(Reference Pepe, Lottenberg and Fujiwara33).
During the weekly online motivational interviews, a retrospective 24-h dietary recall will be obtained from all participants. In addition, the MIND diet score will be applied to the patients in the MIND diet group to assess adherence to the diet(Reference Morris, Tangney and Wang20).
A list will be provided to each patient, listing alternative foods that are consistent with the dietary principles applied, physically accessible and economically affordable, together with their portion sizes. At this stage, patients will be encouraged to consume seasonal vegetables and fruits, which are more cost-effective within the framework of the dietary principles.
During the weekly online motivational interviews, all participants will be asked about the difficulties they experience regarding dietary adherence, and these difficulties will be recorded systematically. Personalised recommendations to increase dietary adherence will be provided for these difficulties (e.g. lists of physically and economically accessible foods, practical recipes, alternative suggestions for eating out, appropriate recipes for cravings for sweets, etc.).
Dietary intake record
Through the dietary intake record, the daily and meal-based energy and macronutrient intake of the patients will be determined. To accurately assess the quantity and content of foods, the visual portion sizes included in the TÜBER 2022 report will be used. The patients’ energy and macronutrient intake levels will be calculated by the researcher using the BeBIS computer program (Ebispro for Windows, Stuttgart, Germany; Turkish Version BeBIS, Nutrition Information System, Version 9). Any patient who cannot be contacted during at least three of the weekly sessions or whose dietary intake record cannot be obtained for any reason will be excluded from the study.
Assessment of adherence to the MIND diet
Adherence to the MIND diet will be determined based on the patient’s self-report using the MIND diet score. Each of the fifeen items is scored between 0 and 1 according to the degree of compliance with the principles of the MIND diet. The total score ranges from 0 to 15 points (Table 3). Higher scores are considered to indicate higher adherence. There are no definitive cut-off points for the MIND diet score. Tertile classifications (low, moderate and good adherence) based on participants’ MIND diet scores are performed at the analysis stage(Reference Morris, Tangney and Wang20). However, for the purpose of monitoring adherence in this study, participants with a MIND diet score ≤ 5 will be classified as having ‘low adherence’, and additional support procedures aimed at increasing adherence will be implemented.
MIND diet scoring

Data collection
Data will be collected through face-to-face interviews conducted twice: at the beginning of the implementation for the intervention and control groups (T0) and at the end of the 12-week intervention (T1). The data collection procedure consists of completion of the MSQOL-54(Reference Vickrey, Hays and Harooni34) Questionnaire, MFIS(Reference Ritvo, Fischer and Miller35), the BICAMS(Reference Benedict, Amato and Boringa36,Reference Langdon, Amato and Boringa37) battery and the Brain Fog scale(Reference Atik and İnel Manav38); performing anthropometric measurements and recording, from the patient file, the results of blood tests routinely requested by the Muğla Training and Research Hospital Neurology Outpatient Clinic.
First, participants’ anthropometric measurements will be taken by the researcher at the Muğla Training and Research Hospital Neurology Outpatient Clinic. Height will be measured in the Frankfort plane using a portable stadiometer.
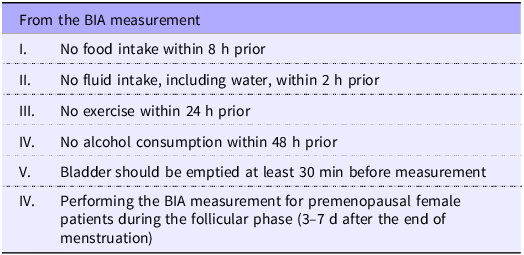
Patients’ body composition will be determined using a Tanita brand BC 418 model bioelectrical impedance analysis (BIA) device with a measurement precision of 0·1 kg. The Tanita BC 418 model BIA device is a non-invasive professional product with easy-to-use features that can perform total body analysis. However, to obtain a highly reliable measurement with BIA, certain conditions must be met (Table 4)(Reference Son, Han and Bennett39). For participants who accept to participate in the study but do not meet any of these conditions, an appointment will be scheduled for another date, and the BIA measurement will be performed on that day.
Requirements prior to BIA measurement

BIA, bioelectrical impedance analysis.
Circumference measurements will be taken from three regions – neck, waist and hip – using a non-stretchable tape measure with a width of 0·5 cm. Neck circumference will be measured horizontally just below the larynx. Waist circumference will be measured at the midpoint between the last rib and the iliac bone. Hip circumference will be measured, while the patient is standing, from the patient’s right side, horizontally at the widest part of the hips when viewed from the side. All circumference measurements will be repeated twice.
Following completion of the anthropometric measurements, the MSQOL-54 questionnaire, MFIS, the BICAMS battery and the brain fog scale will be completed with the assistance of the researcher.
MS patients attend routine follow-up visits at the neurology outpatient clinic at 3-month intervals. During these visits, blood tests routinely requested by the Muğla Training and Research Hospital Neurology Outpatient Clinic are performed. These blood tests include hemogram; biochemical parameters (glucose, HDL-cholesterol, LDL-cholesterol, total cholesterol, aspartate aminotransferase, alanine aminotransferase, albumin); C-reactive protein; thyroid hormones including T3, T4, and thyroid-stimulating hormone; and folate, vitamin B12, and vitamin D levels. The results of these blood tests will be obtained from the patient file and recorded in the data collection form. Data collection for each patient is planned to be completed within approximately 45 min.
Study outcomes
The primary outcomes of the study are the assessment of quality of life using the MSQOL-54 questionnaire and perceived fatigue using the MFIS questionnaire, cognitive functioning level using the BICAMS battery and brain fog status using the Brain Fog Scale. The secondary outcomes of the study are the assessment of anthropometric measurements and the status of blood parameters. Both primary and secondary outcomes will be recorded and evaluated twice, at the beginning of the intervention and at the end of the intervention. For each outcome, the analysis will be conducted based on change from baseline.
Primary outcomes
Assessment of quality of life
The MSQOL-54 questionnaire was developed by Vickrey et al. (Reference Vickrey, Hays and Harooni34). The questionnaire consists of twelve subscales: I – Physical Health, II-Role Limitations Due to Physical Problems, III Role Limitations Due to Emotional Problems, IV – Emotional Well-Being, V-Energy/Fatigue, VI – Health Perceptions, VII – Social Function, VIII – Cognitive Function, IX – Health Distress, X – Sexual Function, XI – Change in Health and XII – Overall Quality of Life. As a result of calculating the subdimensions with a specific weighting coefficient, I – Physical Health Composite Score and II – Mental Health Composite Score are obtained. The scores of each subdimension and the main dimensions range between 0 and 100. Higher scores are associated with better quality of life.
Assessment of perceived fatigue
The MFIS, included within the MS Quality of Life Inventory(Reference Ritvo, Fischer and Miller35), consists of twenty-one questions and three subscales (I-Physical, II-Cognitive and III-Psychosocial). The total score obtained from the three subscales ranges from 0 to 84 and constitutes the MFIS score. Higher scores are associated with greater fatigue.
Assessment of cognitive function level
BICAMS was developed in 2012 with input from a committee of professionals specialised in neuropsychological testing to facilitate cognitive assessment in MS(Reference Benedict, Amato and Boringa36,Reference Langdon, Amato and Boringa37) . BICAMS evaluates cognition under three subtests: the Brief Visuospatial Memory Test, the Symbol Digit Modality Test and the California Verbal Learning Test-II.
Brief Visuospatial Memory Test
This test, which evaluates visuospatial learning capacity, visual-spatial memory and recall, consists of six geometric figures arranged in two columns and three rows. Patients are asked to study the figures for 10 s. Afterwards, the figures are removed, and the patient is asked to draw them from memory on a blank sheet of paper. Each geometric figure is scored between 0 and 2, taking into account its accuracy and position. For each trial, the patient can receive a score ranging from 0 to 12. The total score is obtained by summing the scores from the three trials.
Symbol Digit Modality Test
This test assesses visual-motor information processing speed, sustained attention, and concentration capacity. It consists of symbols, each representing a number from 1 to 9. Patients are asked to study the symbols for 30 s and then, within 90 s, write the corresponding numbers beneath the symbols arranged in different sequences across various rows. The total number of correct responses is recorded, with one point awarded for each correct answer.
California Verbal Learning Test-II
This test, which evaluates verbal learning and recall, involves reading a list of sixteen words from four categories to the patients. They are asked to recall and repeat as many words as possible in the order they remember them. This procedure is repeated five times. One point is awarded for each correctly recalled word. The total number of words remembered across the trials constitutes the test score.
Assessment of brain fog
The Brain Fog Scale was developed by Atik and İnel Manavlı(Reference Atik and İnel Manav38). It consists of three subdimensions; I-Cognitive, II-Physical and III-Psychological and a total of thirty items. The total score ranges from 30 to 150. Higher scores on the subdimensions and the overall scale are interpreted as indicating a higher level of brain fog.
Secondary outcomes
Blood parameters
The blood parameters to be recorded have been defined as hemogram, fasting glucose, lipid profile (total cholesterol, HDL-cholesterol, LDL-cholesterol and TAG), the inflammatory marker (CRP), liver enzymes (alanine aminotransferase, ALT), albumin, thyroid function tests (T3, T4, thyroid-stimulating hormone) and folate, vitamin B12 and vitamin D levels. Through routinely performed blood tests, the effect of the implemented intervention on blood parameters will be determined, and the changes obtained will be evaluated as secondary outcomes.
Assessment of body composition
To determine body composition, height will be measured; weight, BMI, fat-free body mass, body fat mass and body fat percentage will be obtained as a result of body analysis performed using BIA (Tanita BC 418 model); and circumference measurements, including neck, waist and hip circumferences, will be taken and recorded in the data collection form. In this way, the effect of the intervention on body composition can be determined.
Adverse effects and harms
During the study, all adverse events reported by participants will be recorded and reported to the data monitoring committee and the ethics committee. The systematically conducted weekly interviews will facilitate the documentation of adverse effects and events. In the event of any harm related to the research, its treatment and associated costs will be covered by the investigators.
Data management and access
All data will be collected using participant identification numbers, with personal identifiers kept confidential and securely stored(Reference Regulation40). Printed documents, such as informed consent forms and questionnaires, will be stored in a locked cabinet accessible only to the research team. Data will be entered into an electronic database by the principal investigator through periodic follow-ups. To enhance data quality, the data will be checked using a double-check method by other researchers in the research team, independently of data entry and missing and outlier data will be monitored regularly. After the study is reported and published, anonymised data will be shared with other researchers upon ethically appropriate request.
Data monitoring and auditing
Data monitoring and oversight of the study will be conducted by the senior investigators and the supervisory team, D.T. and M.A.C., through meetings held every 6 months (Appendix 2). No interim analysis is planned for this study.
Statistical analysis method
Analyses will be conducted using IBM SPSS Statistics software. The significance level and type I error rate will be accepted as α = 0·05. In addition, effect sizes will be calculated and reported to determine the clinical significance of the observed effects.
After the data collection process is completed, the data will be checked and cleaned using descriptive statistics and data visualisation. Participants’ baseline demographic characteristics, lifestyle habits and clinical features will be summarised for each group using appropriate descriptive statistics (mean (sd) for normally distributed variables; median and interquartile range for non-normally distributed variables; frequency and percentage for categorical variables).
The homogeneity of demographic and baseline characteristics between the experimental and control groups will be assessed using χ 2 test or Fisher’s exact test for categorical variables and independent samples t test or Mann–Whitney U test for continuous variables.
The internal consistency reliability of the scales used in the study will be assessed using Cronbach’s alpha coefficient.
The normality of continuous variables will be assessed by examining skewness and kurtosis coefficients. Variables with skewness and kurtosis values within the range of ±2 will be considered normally distributed.
For between-group comparisons (experimental v. control), the independent samples t test will be used for normally distributed variables, while the Mann–Whitney U test will be applied for non-normally distributed variables. For within-group comparisons (pre-test v. post-test), the paired samples t test will be used for normally distributed variables, while the Wilcoxon signed-rank test will be applied for non-normally distributed variables.
When all parametric assumptions are met, a mixed-design repeated measures analysis of variance (mixed RM-ANOVA) will be performed to examine the main effects of group (experimental/control) and time (pre-test/post-test), as well as their interaction effect.
The primary analyses will be conducted according to the intention-to-treat approach, including all randomised participants regardless of protocol adherence or missing data. Missing data will be handled using appropriate methods such as Expectation-Maximisation algorithm or multiple imputation. Additionally, a per-protocol analysis will be performed including only participants who completed the study protocol without major deviations. Both analyses will be compared to assess the robustness and sensitivity of the intervention effects.
Data reporting and publication plan
The study will be reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines(Reference Moirangthem, Deshpande and Patil41). The results of the study will be disseminated to a wide range of stakeholders – including researchers, participating patients, other individuals with MS and healthcare providers – through websites, reports, presentations and peer-reviewed journal articles.
Ethical approval of the study
This study will be conducted in accordance with the guidelines set forth in the Declaration of Helsinki. The conduct of the research at Muğla Training and Research Hospital was approved by the hospital administration, and institutional permission was granted on 8 January 2025. Ethical approval for the study was obtained from the Selçuk University Faculty of Health Sciences Non-Interventional Clinical Research Ethics Committee on 30 April 2025, with decision number 2025/643. During the conduct of this study, adverse events will be recorded and reported to the ethics committee. No major change is planned to the study protocol; however, any changes to the protocol will be reported and submitted as an amendment for ethical approval. Written informed consent will be obtained from all patients (Appendix 3). Participants will be informed that they may withdraw from the study at any time without providing any reason, and if they choose to provide a reason, it will be recorded. This research design was registered in the ClinicalTrials.gov database under the identifier NCT07057999 on 8 July 2025, prior to the commencement of data collection (https://clinicaltrials.gov/study/NCT07057999). This protocol was updated to Version 3 on 2 September 2025.
Study status
The data collection process began on 14 July 2025 and is planned to be completed in January 2026. The study results are expected to be reported and presented by July 2026.
Discussion
In light of the current evidence, evaluating the effectiveness of the MIND diet on fatigue, quality of life, cognitive function, and brain fog in patients with RRMS through a randomised controlled trial design will make a significant contribution to the literature. To our knowledge, no randomised controlled trial has yet been conducted on this topic, which makes this study original. To ensure the conduct of a high-quality study, a multidisciplinary team with expertise in MS and nutrition has been included in the study design.
In its clinical nutrition report on neurology, the European Society of Clinical Nutrition and Metabolism recommends a diet for MS patients that is limited in saturated fats and rich in MUFA and PUFA(Reference Burgos, Bretón and Cereda42). The MIND diet meets this recommendation.
The MIND diet offers potential benefits for improving fatigue, cognitive function and quality of life, which are common concerns among individuals with MS(Reference DeLuca, Chiaravalloti and Sandroff23,Reference Bhattarai, Patel and Dunn43) . Examining the effects of the MIND diet on quality of life and BICAMS components may help guide the existing evidence in the literature. Likewise, the results of this study regarding fatigue can be compared with the outcomes of similar research(Reference Navarrete-Pérez, Gómez-Melero and Escribano25). It has been reported that brain fog, which is associated with low quality of life and fatigue, is also observed in patients with MS(Reference Rosenberg, Thorpy and Doghramji44); however, no study on this specific topic has been conducted to date. With the study described in this protocol, we aim to contribute evidence to the literature in this area as well.
Studies conducted to determine the effects of MIND diet intervention on anthropometric measurements and biochemical parameters in MS patients make it possible to compare our secondary outcome measures, namely anthropometric measurements and biochemical results(Reference Atabılen, Tuncer and Polat45,Reference Eroğlu, Orhan and Arlı46) .
In summary, the data obtained from this study may indicate that the MIND diet has positive effects on improving fatigue, low quality of life, impaired cognitive function and brain fog resulting from MS and may contribute to the development of individualised nutritional therapies.
Strengths and limitations
Among the strengths of this study; to the best of our knowledge, it is the first randomised controlled trial planned to be conducted in the relevant field with valid and up-to-date outcome measures. For this reason, it is anticipated to fill an important gap in the literature. Including only RRMS patients in the study, preparing a nutrition program tailored to the needs of each participant, monitoring dietary adherence through regular follow-up, supporting adherence to the diet through motivational interviews and conducting the research by a multidisciplinary team are the strengths of the study.
This study has some limitations. The study being single-centred, the inability to blind patients due to the nature of the intervention, determining patients’ adherence to the diets based on self-report and collecting dietary intake records using the 24-h recall method are limitations of the study. Another limitation is that people are social beings, and dietary adherence can be influenced by many factors. Therefore, adherence to dietary interventions may vary, which may reduce the effect of the intervention. Post-intervention limitations of the study will be reported.
Supplementary material
For supplementary material/s referred to in this article, please visit https://doi.org/10.1017/S0007114526106850
Acknowledgements
The authors would like to thank all participants who agreed to take part in the study, those who assisted in participant recruitment and Professor Deniz Tanyer. Language editing and translation support for this study were provided by OpenAI’s ChatGPT (GPT-5, 2025 version). All scientific content and interpretations are the responsibility of the authors.
The study does not receive any external funding. The research will be conducted at Muğla Training and Research Hospital, and the host institution provides only in-kind support. The host institution has no role in the design, analysis and writing of the study.
Conceptualisation: B. Ü. Y., E. E. D. and N. A.; Data curation: B. Ü. Y., D. T. and E. E. D.; Investigation: B. Ü. Y., E. E. D., G. K. G. and N. A.; Methodology: B. Ü. Y., D. T., and N. A.; Project administration: B. Ü. Y., E. E. D. and G. K. G.; Supervision: N. A., Deniz Tanyer and Muhammed Ali Cebirbay; Writing – Original Draft: B. Ü. Y. and Writing – review and editing: all authors. All authors approved the final article.
The authors declare no conflicts of interest.
After the study is reported and published, anonymised data will be shared with other researchers upon ethically appropriate request.
This research design was registered in the ClinicalTrials.gov database on 8 July 2025, under the identifier NCT07057999. The protocol was updated to Version 3 on 2 September 2025 (https://clinicaltrials.gov/study/NCT07057999).
The full protocol and statistical analysis plan of the study are presented in the main text.
The results of the study will be disseminated to a wide range of stakeholders – including researchers, participating patients other individuals with MS and healthcare providers – through websites, reports, presentations and peer-reviewed journal articles.



 Open access
Open access