


Introduction
The Welsh language expression Torri Y Llech, contracted to Torri’r Llech (TLl), is often translated as ‘breaking the rickets’ in English.Footnote 1 In Welsh folk terminology, curing disease was referred to as ‘Torri’r Clefyd’ [breaking the disease], possibly explaining the etymology of TLl. Footnote 2 TLl was fundamentally a folk medical practice that existed in various parts of Wales from at least the mid-nineteenth until well into the twentieth century, persisting around the south and west of the country.Footnote 3 The procedure involved cutting the ear (pinna) with a razor to induce bleeding, with the specific sites cut varying considerably over time. TLl was used as a treatment for a wide range of complaints (among these being rickets) and those undergoing the procedure would sometimes be cut multiple times if the problem being treated was considered particularly severe.Footnote 4 Over time there was significant variability in the age and sex of both the practitioners carrying out TLl as well as in those receiving the treatment. This dynamism gave rise to a diverse practice that occupies a unique place in the history of vernacular medical practices in Britain.
The wider Welsh medical landscape within which TLl existed underwent seismic changes over the documented timeline of the practice. These changes coincided with the rise of the biomedical establishment and were reflected across Europe as well as its expanding empires. As an ascendant biomedical culture permeated societies across the globe, driven by the forces of empire and with backing from official institutions of government its practitioners were invested with unrivalled capital and were able to increasingly define themselves as the global medical orthodoxy.Footnote 5 In Porter’s terms, ‘What began as the medicine of Europe is becoming the medicine of humanity’.Footnote 6 Tilley clarifies this historical trend by arguing that biomedical approaches have more specifically become the norm for governments the world over.Footnote 7 In turn, practitioners not sanctioned by state institutions have come to be seen as unorthodox by definition. Other terminological dualisms also exist such as modern/traditional, official/unofficial, and effective/non-effective, amongst others.Footnote 8 The term vernacular medicine is also used to denote unofficial modes of care.
Whilst much recent scholarship has considered the tensions between orthodox and unorthodox paradigms across the reaches of European empires, it is also useful to recall the ways in which these forces played out here in Europe and more specifically in Britain and Ireland.Footnote 9 In Wales particularly, a strong tradition of vernacular healing practices engendered a diverse medical marketplace consisting of actors such as bone-setters, urine casters, herbalists, ddynion and fenyw hysbus [wise men and women] and consurios [conjurers].Footnote 10 Due in part to the strength and diversity of unofficial approaches to care in Wales, it is this sector of the medical marketplace which has often dominated the early historiography of Welsh medical practices. Withey has noted that whilst a characterisation of Wales as a haven of exclusively folk medicine is indeed inaccurate, since Welsh people clearly also engaged with orthodox sources of care, folk healing practices have nonetheless long played a major role in the everyday sickness experience of Welsh people.Footnote 11 Though popular, unorthodox practices in Wales were not wholly insular as much of the epistemological basis of this sector from as early as the ninth century onward drew from wider European paradigms of disease.Footnote 12 This is further supported by Luft’s analysis of the constituent texts comprising the Meddygion Myddfai [The Physicians of Myddfai]. The texts which make up this corpus originate from the end of the fourteenth to the beginning of the fifteenth centuries and have in earlier accounts been held up as paradigmatic of Welsh folk medicine.Footnote 13 Luft points out in her analysis, however, that the conceptions of the human body and of disease contained therein are themselves redolent of contemporary European medical knowledge from the period in which they were written.Footnote 14 One particular practice that was popular in Wales since at least the fifteenth century which also shares a wider European heritage is bloodletting.Footnote 15
Bloodletting in accordance with the theory of the four humours has been practised in Europe and parts of Asia for millennia.Footnote 16 Likely originating in Ancient Greece, humoral bloodletting became especially popular through the practice and writings of Galen of Pergamon (129–216 AD).Footnote 17 Galen’s teachings and texts eventually came to form the bedrock of medical thought across medieval Europe.Footnote 18 In Wales, Withey discusses the process by which classical texts likely percolated down to Welsh practitioners between the ninth and twelfth centuries onward.Footnote 19 It is conceivable therefore that bloodletting as a humoral practice followed a similar course and certainly by the late fifteenth century was established in Wales, as exemplified by pictorial representations of sites for bloodletting by the Welsh poet Gutun Owain (Figure 1).Footnote 20 Bloodletting was widely practised during the early modern period across Britain and Ireland, though it came to be seen with increasing suspicion as the eighteenth century drew to a close.Footnote 21 Nonetheless, the practice remained popular throughout the nineteenth and in some instances into the early twentieth centuries.Footnote 22
Sites for bloodletting from the fifteenth century manuscript of Gutun Owain. The text is written in Middle Welsh. Copyright: Public Domain Licence. Source: Llyfrgell Genedlaethol Cymru – The National Library of Wales, Aberystwyth.

This article will aim to challenge this traditional narrative and make an original contribution to the literature by significantly extending the currently accepted timeline of humoral bloodletting and its practice both in Wales and Britain more widely. We will also aim to explore the origins, material practice, wider societal perception, and embodied experience of TLl as well as consider the ways in which it changed over time. By engaging with the literature in this way, we will additionally aim to explore the ways in which TLl could serve as a faultline for wider societal tensions between biomedical and unorthodox institutions of care from the mid-nineteenth through to the mid-twentieth centuries. Furthermore, we will attempt to establish TLl as a Welsh humoral bloodletting practice that persisted longer than any other documented bloodletting practice from across the British Isles. In doing so, this article will finally aim to convey a previously unrecognised resilience to the custom and to vernacular practice in Wales more generally.
To achieve these aims, we found it necessary to carefully scrutinise our methodology as there is undoubtedly a dearth of primary source material relating to TLl. Much of what exists takes the form of scattered accounts in contemporary newspapers as well as one brief autobiographical mention. There is additionally very limited secondary literature on the practice, with Thompson’s account forming the most authoritative to date.Footnote 23 Most of the newspaper accounts give adequate insight into the official view of the practice through the lens of local health and legal officials. This, however, omits the perception and experiences of those at the street-level, that is, of those administering and those having the practice performed upon themselves. This situation renders an inclusive and holistic account highly challenging and was a chief motivator for conducting a series of recorded interviews (undertaken by the primary author) with local people from the Upper Swansea Valley who either knew of TLl or who had it performed upon themselves.Footnote 24 Their timely accounts have enabled the story of TLl to be told from the bottom up, facilitating a more nuanced and balanced analysis of the practice. The interviews were conducted either in-person or remotely in English, and all were recorded to allow subsequent analysis. These recordings are now held at the Screen & Sound Archive at the National Library of Wales in Aberystwyth. All interviewees consented to being interviewed and to being named in subsequent works via recorded agreements prior to, or immediately following, the interviews proper.
The medical landscape of nineteenth to mid-twentieth century Wales
The nineteenth to mid-twentieth centuries were a period of flux in Wales, as nodes of industrialisation drew rural dwellers from western, central, and northern Wales to work in the burgeoning coalfields and metalworks of the south.Footnote 25 Migrants also came from other parts of the British Isles as well as overseas.Footnote 26 By 1801 Wales’ total population sat at around 587,000, increasing by 1911 to approximately 2,421,000.Footnote 27 This growth was asymmetric and concentrated almost exclusively in the rapidly industrialising regions of South Wales such as Glamorganshire.Footnote 28 More rural counties tended to demonstrate either stagnant or decreasing population trends across this same time period.Footnote 29 These population upheavals inevitably had far-ranging social effects, one of which was to engender a dual sickness experience for Welsh people living either in the rural parts of the country or in the rapidly expanding industrial centres.
Waddington’s focus on rurality in nineteenth and early twentieth-century Wales helps to elucidate the unique health-seeking challenges faced in these areas. His work reveals the difficulty that Welsh rural sanitary authorities faced in policing geographically large areas, often with part-time staff who tended to be more poorly paid than their municipal counterparts.Footnote 30 Rural depopulation to more industrial areas then only served to compound these issues by shrinking ratepayer bases (i.e. local taxes) and exacerbating rural poverty. In addition central authority in the form of the Local Government Board in London was distant at best, derogatory at worst, with the board frequently using terms like ‘primitive’ and ‘stupid’ to describe rural Welsh populations and local officials.Footnote 31 Remote Welsh counties also suffered from a relative lack of general practitioners.Footnote 32 Suffice to say, rural Wales during this period was woefully underserved by official sources of medical care at a time when the particular challenges faced by local communities included water insecurity, dilapidated housing, lack of sanitary infrastructure as well as localised outbreaks of infectious diseases.Footnote 33 Contrary to the contemporary image of remote Welsh communities as healthier than their urban counterparts, rural mortality rates for regions such as Caernarvonshire periodically exceeded those of Wales’ urban areas in the 1880s and 1890s.Footnote 34
Given the clear health challenges faced by rural Welsh communities, it may not be surprising that people in rural Wales frequently turned to unofficial sources of medical provision. Folk practices already had a long tradition in Wales with many being rooted in Galeno-Hippocratic humoral belief systems. Withey further clarifies this position by describing the way in which these humoral belief systems tended to amalgamate with astrological and lay theories of health to form what he termed a ‘popular humoralism’.Footnote 35 Withey posits several possible reasons why such ideas remained popular for so long in Wales, including the country’s geographical remoteness, its unique language, and even its relative resistance to the influences of the Reformation, which in England had a more erosive effect on folk belief systems.Footnote 36 Writing about the early modern period, he describes how the strong oral tradition in Wales helped to propagate these ideas. Therefore by the nineteenth century it is likely that they were deeply embedded in the local medical marketplace of rural Welsh communities.Footnote 37 The popularity of unorthodox practices in Wales is evidenced by a 1910 government report which revealed that approximately 72.7% of Welsh towns reported practice by ‘unqualified persons’ to be prevalent or increasing as compared to 36.1% for England.Footnote 38 It is not surprising therefore that rural Welsh people had a range of unorthodox actors and practices to choose from, including the use of holy wells as well as the utilisation of charms. Tallis’ and Tulfer’s recent works have also helped to highlight the undeniably Christian influence on these practices with biblical references frequently being written onto charms and etched into cursing wells.Footnote 39 Bonesetters were also especially popular in Wales; some better-known examples of which include the Thomas family of Anglesey.Footnote 40 In fact, some commentators have described the plethora of folk practitioners in Wales as a ‘free-for-all’ and there is evidence that this situation continued even into the early twentieth century.Footnote 41 Whilst there were undoubtedly many influences on how rural Welsh people understood their bodies and in how they elicited health services, they were certainly never dogmatic in doing so. Withey makes the argument that early modern Welsh people across the class spectrum were themselves sovereign in deciding which sources of care to utilise, and for what ailments.Footnote 42 This article will aim to argue that this agency continued to be demonstrated by Welsh patients across the nineteenth as well as into the mid-twentieth centuries.
Those living in the more industrialised areas of Wales encountered their own health challenges, shaped mostly by the perilous nature of work in heavy industries as well as by higher population densities. The South Wales coalfields were particularly injurious and accident-prone, entailing higher levels of mortality and morbidity than other coal-mining regions.Footnote 43 In addition, the area saw higher levels of occupational diseases such as pneumoconiosis and silicosis.Footnote 44 Recurrent outbreaks of infectious diseases such as typhoid, smallpox, scarlet fever, and diarrhoeal illnesses were also central to the sickness experience of industrial communities during this period.Footnote 45 Taken together, the health challenges facing these populations were significant at a time which saw far less state involvement in health care provision. Coupled with the gross disparity in the quality of health services, this may explain some of the more pragmatic and community-based strategies these areas adopted, like medical aid societies. These schemes were funded by wage deductions and provided sick benefits and medical attendance for workmen and, crucially, for their dependents. They existed across Britain, but it was in South Wales that they were most comprehensive in scope. For example, from its foundation in 1874 up to the 1920s, the Tredegar Medical Aid Society had grown to cover 95% of the town’s population for medical aid (including dependents).Footnote 46 They offered the services of medical doctors, surgeons, pharmacists, physiotherapists, and possibly even bonesetters. Other sources of care outside the remit of the societies were also popular to include herbalism and spiritualism.Footnote 47 Pamela Michael even makes mention of herbalists offering their products and services in Neath market as late as the 1930s.Footnote 48 It is certainly possible that unorthodox and folk practices found their way into the urban medical markets of Wales via the process of internal migration which occurred with industrialisation. In his work studying the emigration of Welsh people to urban centres in England, Pooley found that many retained their rural Welsh customs and traditions.Footnote 49 It is therefore conceivable that this process also played out within Wales with rural dwellers helping to popularise their healing practices in urban Welsh settings.
Referring to the interwar period, Thompson points out that ‘patients made their choice of action based on their conception of their illness and its causation, and their estimation of the skill of various practitioners’.Footnote 50 Therefore, whether they were rural or city dwellers, patients in Wales clearly demonstrated a common agency in relation to whom they entrusted their care and for what ailments.
Bloodletting in Britain and Ireland
Bloodletting remained one of the most popular interventions utilised by a wide range of practitioners across Europe and the Arab world for millennia. The history of the practice across Britain and Ireland reflects this wider narrative but is key in understanding TLl’s place within the rich tapestry of the ‘ancient practice’.Footnote 51
Evidence for pre-humoral bloodletting in Britain and Ireland is scant at best. In a ninth-century Irish text there is evidence that bleeding was significant in diagnosing certain complaints, but whether this represents the existence of humoral ideas in Ireland before the arrival of the Anglo-Normans or whether it was part of a native paradigm of disease is less clear.Footnote 52 In Britain the earliest that humoral bloodletting can be definitively placed is around the seventh century AD.Footnote 53 During the early and much of the later medieval period bloodletting as an intended healing practice would most commonly have taken place in monastic settings, where bloodletting was often indulged by monks as part of a health maintenance regime (regimen sanitatis).Footnote 54 However, an 1163 papal edict discouraged monks from performing physick and more specifically forbade the letting of blood.Footnote 55 From then on bloodletting began to fall more squarely into the working jurisdictions of physicians, barber-surgeons (then later surgeons) and apothecaries across England, Scotland, Wales, and Ireland.Footnote 56 This situation likely persisted throughout the medieval and much of the early modern period, though during the seventeenth century sources start to emerge which also detail the practising of bloodletting by lay people and folk practitioners.Footnote 57 It was not only the nature of practitioners which were subject to change, but also the procedures themselves with a notable shift in preference to bleeding from the arm by the early modern period as opposed to the myriad sites used in the medieval period.Footnote 58
The popular perception of bloodletting in Western Europe underwent numerous changes during the nineteenth century. The early decades saw a huge increase in popularity for bleeding via the application of leeches, a practice promoted most notably by Francois-Joseph-Victor Broussais (1772–1838).Footnote 59 Despite the so-called ‘leech craze’, questions were starting to be asked of the practice using the nascent language of medical statistics. The work of Pierre Charles Alexandre Louis (1787–1872) utilised mathematical methods to more objectively question the value of bloodletting in pneumonia.Footnote 60 Whilst Louis himself remained a supporter of bloodletting, others would soon utilise and develop similar methods in challenging bloodletting more broadly. This culminated in the publication of John Bennett’s (1812–1875) ‘The Restorative Treatment of Pneumonia’ which demonstrated that patients not treated by bloodletting generally did better than those who were bled.Footnote 61 Bennett’s work cannot be viewed in isolation, however, as it occurred within the milieu of an evolving biomedical approach to disease. Bloodletting increasingly began to fall afoul of this new paradigm as germ theory offered new explanations for the causation of infectious diseases. In this new reality venesection in the cases of fever and infection became increasingly difficult to countenance, and so the practice was steadily abandoned to an ever-shrinking cluster of indications.Footnote 62 Despite this, advocacy for bloodletting survived in some surprising corners as late as the mid-1930s, as exemplified by the 12th edition of Sir William Osler’s (1849-1919) ‘The Principles and Practice of Medicine’ where it was still recommended in the case of pneumonia with right heart failure.Footnote 63 However, by the Second World War humoral bloodletting appears to have been largely abandoned by physicians and surgeons in Britain and Ireland.
Amongst unorthodox practitioners, it appears that bloodletting enjoyed variable patronage throughout the British Isles across the nineteenth and into the early twentieth centuries. In England and Scotland, there appears to be little evidence that the practice was taken up by lay practitioners in significant numbers. In fact, rural Scots often appeared to resist bloodletting with a country surgeon from Angus commenting in 1819 that ‘The old people [declared] that in their time no such thing [bloodletting] was ever allowed or thought of’.Footnote 64 In Wales and Ireland, the situation seems somewhat different with folk practitioners often resorting to bloodletting to tackle a range of ailments such as pleurisy, fever, perceived mental ‘slowness’ as well as locally defined diseases.Footnote 65 Wales was, however, unique amongst the four regions for possessing neither medical guilds nor companies of barber-surgeons.Footnote 66 It is of note that formalised medical institutions arrived relatively late in Wales. As a result, there was likely no formal civic structure within which to regulate bloodletting, which may have led to its democratisation amongst larger segments of the population. In effect almost anyone with the skills or resources could lay claim to the practice. Indeed, within Wales there is evidence that folk practitioners continued bloodletting into the early decades of the twentieth century, and possibly even later.Footnote 67
Torri’r Llech – Its origins and practice
As a practice, bleeding from the ear was not entirely unique to TLl. Roberts Johnson’s 1684 ‘manual of physick’ advised the ‘incision or scarification of the ears’ for the treatment of rickets.Footnote 68 Clearly bloodletting from the ears was at least in the ether in the centuries prior to TLl first entering the historical record. This first entry then occurs in the form of an interview in the Western Mail in 1921 where an ‘old lady’ recalls a man named ‘Jack from Llanfair’ carrying out the practice in the early 1860s near Lampeter.Footnote 69 The article also mentions that the practice had ‘been in vogue for generations’ implying it may have been practised even earlier than the 1860s.Footnote 70 This would not necessarily be surprising given the popularity of other bloodletting practices across Wales during this time period.Footnote 71 Jack would reportedly treat ailing children but was also stated to have attended a ‘young woman’ with an apparently successful outcome, suggesting it was not just children who underwent TLl at this early stage.Footnote 72
The death of 14-month-old John Jones after being treated with TLl serves as a poignant reminder that, far from being a benign procedure, it was in fact a form of minor surgery that could entail significant risk.Footnote 73 The subsequent inquest took place in Llanelli in 1875 after the boy’s mother took him to see ‘Richard of the Mill’, a local practitioner of TLl. Footnote 74 The boy reportedly suffered from vomiting and was generally unwell, with the boy’s mother stating he was ill in his ‘sides’, which she believed constituted llech. Footnote 75 After making local inquiries, she was apparently advised to consult Richard, who confirmed that ‘llech was on the child’ before cutting a fold of cartilage on the inside of the boy’s ear, instructing his mother to use warm water to wash the ears.Footnote 76 Sadly, by the next day the child was dead. Shortly before the boy died, his parents sent for the local assistant-surgeon who found the boy to be pale, clammy, and pulseless with cold skin.Footnote 77 Harrowingly he also described matting of the hair and clothing due to the blood. The assistant-surgeon goes on to say that he ‘ascertained that the child’s nature had a haemorrhagic tendency’, raising the possibility that the boy suffered from a clotting disorder.Footnote 78 On examining the ears, he found cuts on both of about a quarter inch in length penetrating through the cartilage. Interestingly, the boy’s mother said that she initially sent for a doctor before consulting the folk practitioner, but none attended.Footnote 79 This helps to illustrate Waddington’s observation of limited medical provision and coverage in rural nineteenth-century Wales.Footnote 80 The inquest hears evidence from Richard himself, who maintains his belief in the llech and in TLl as the requisite treatment. He also mentions how he has ‘cut a child so young as the deceased before now and younger too’.Footnote 81 The coroner ultimately declares his amazement at the existence of the practice and goes on to compare it to witchcraft, suggesting a clear friction between official establishments and the practice of TLl even at this relatively early stage.Footnote 82
An article in the same newspaper a week later documents the court’s final session and verdict. It describes how prior to the final session a ‘great crowd of people occupied the body of the hall not a few of the respectable inhabitants of our town being amongst them… a great deal of interest and public feeling and not a little indignation had been manifested in the case’.Footnote 83 Waddington has previously written of the popularity of unofficial sources of care among the working classes of nineteenth-century Britain.Footnote 84 However, the assemblage of so-called ‘respectable inhabitants’ among the crowd at the 1875 inquest suggests that local support for the practice was strong across a wider range of social strata than has previously been noted for other folk practices in Wales.Footnote 85 This sense of social approbation with regard to TLl may further be reflected in the final verdict as Richard of the Mill was ultimately acquitted, with the Bench ruling that ‘there is a general opinion (in the local community) that the treatment…is beneficial’ and that the case therefore could not constitute manslaughter.Footnote 86 In this same article, the nebulous meaning of llech is also demonstrated as the Bench state that amongst the local populace ‘nearly everything is put down as the llech’.Footnote 87 In the same session a local doctor then describes llech as when a ‘child has difficulty breathing and feels tight in the sides’.Footnote 88 It appears that at this time there was no clear definition of llech with it perhaps being considered akin to a generalised state of critical illness.
The first identified reference to TLl in the twentieth century describes a ‘Cardiganshire man’ in the Rhondda Valley in 1902 carrying out the practice as a treatment for ‘Llechau’, then defined as rickets.Footnote 89 This again illustrates the plurality of the meaning of llech. The procedure is then described as ‘cutting a slit in the lobe’.Footnote 90 By the beginning of the twentieth century, despite the apparent publicity of fatal cases of TLl it seems this did little to deter patrons of the practice. In 1921, Dr D. Arthur Hughes, county medical officer of health for Carmarthenshire, made clear the orthodox establishment’s vehemence towards TLl by brandishing it a ‘pure fetish’ that ‘appeals only to the ignorant and superstitious’.Footnote 91 He describes how the procedure involves ‘making an incision into a certain part of the cartilage of a child’s ear for the cure of all cases of backwardness’.Footnote 92 This is relevant as this is the first reference to a cognitive indication for TLl and possibly represents a further mutation in the definition of llech. Hughes also adds that the cut was ‘usually performed by a woman’ and that the practice was handed down hereditarily.Footnote 93 In previous cases of TLl, it was men who often carried out the practice. Indeed, the prominent role played by ddynion hysbys [cunning men], in local Welsh communities during the nineteenth century, has previously been noted by both Tallis and Tulfer.Footnote 94 However, by the interwar years female practitioners appear to have become predominant in the practice. It may be possible that as the practice of male practitioners waned, the procedure was taken up by so-called fenyw hysbys [cunning women].
Astrological elements to TLl also became more clearly identified in the early decades of the twentieth century. Dr Hughes’ account that TLl had to be done during ‘the wax of the moon’ represents the first such reference, and clearly led to periods of acutely higher demand.Footnote 95 One female practitioner of TLl in Ammanford is even described as attracting ‘hundreds of mothers with babies in arms’, with a reported 250 visitors having their babies cut in a single day.Footnote 96 This is then fittingly described as a ‘pilgrimage’ with the valley train ‘on certain days full of whining children with bleeding ears’.Footnote 97 By the early 1920s, TLl clearly enjoyed huge popularity in and around Ammanford with people coming in spectacular numbers to be treated from all around Glamorganshire, Cardiganshire, and Pembrokeshire.Footnote 98 In this article the procedure is described as the ‘nicking with a sharp knife’ of the upper edge of the ear and that ‘even grown men’ suffering from ‘weakness and debility’ underwent TLl. Footnote 99 Further, the article also describes how parents would often take their children to both an orthodox and folk practitioner.Footnote 100 This account indicates that even by the early twentieth century, practitioners of TLl still existed as prominent members of the local medical marketplace and were likely perceived as just as efficacious as orthodox doctors by the lay populace of the region. This is consistent with Thompson’s observations that the folk medical sector was especially large in interwar South Wales, enjoying particular popularity in mining districts.Footnote 101
An article in the ‘Welsh Gazette’ again centres on Ammanford and lends further evidence to the pan-societal allure of TLl during this period, as ‘many apparently enlightened parents, and even public men’ were described as staunch believers in TLl and the ‘all-round improvement in health’ it was believed to induce.Footnote 102 This phenomenon whereby TLl enjoyed support across social classes was previously observed at the 1875 inquest but it may be possible that this popularity continued into the 1920s. Furthermore, reporting of TLl appeared to have reached audiences across the Anglosphere, with a broadsheet in New South Wales, Australia, even mentioning the practice in 1922.Footnote 103 Of note, the article characterises TLl as slitting a baby’s ear ‘to make it Bright and Lively’ and goes on to quote ‘A Welshman’ who reportedly remarked on how common the practice was in his boyhood, ‘particularly in the remote rural districts [of Wales]’.Footnote 104
Cases of infant death linked to TLl often appeared to serve as flashpoints for renewed hostilities between government establishments and proponents of TLl. In 1933 an inquest was held into the death of William Warboy at 18-weeks of age after having been cut in February of the same year.Footnote 105 He was reportedly cut by a ‘Mrs Rosser’ at no charge after being unwell with Influenza for the month previously.Footnote 106 The boy’s mother reportedly took him to see Rosser as he was crying and distressed, who then advised that he should be cut. The child was cut on a ‘portion of the upper part of the inside’ of both ears and bled ‘a few drops, not much’.Footnote 107 This small amount of bleeding may point towards a more superficial cut than in previous accounts. Luckily for Rosser, medical testimony ultimately concludes that Warboy died of ‘heart failure as a result of influenza’ and not from TLl. Footnote 108 Nonetheless, the presiding coroner lambasted the practice as ’illegal and dangerous’ and advised Rosser to cease practice immediately.Footnote 109 In line with previous sources, Rosser asserted that it was not only children that she had cut but also ‘grown-ups as well’. It is also of note that the coroner inquires with a Dr Harvey (assumedly a medical doctor) as to whether Warboy had rickets; to which Dr Harvey replied ‘No’.Footnote 110 This indicates that there may have been a discrepancy between the state and local population in their understanding of the term llech, with the former defining it as the discrete clinical entity of rickets involving bone disease and the latter as a more generalised state of poor health.Footnote 111
The Warboy story clearly caught the attention of the local readership as only a week later a cartoon was published on the front page (Figure 2) of the same newspaper depicting a suited man (assumedly a local official) holding his ear after having TLl performed on him by another ostensibly official character.Footnote 112 The man holding the razor stands ahead of a sign saying “Warning to councillors! In future any member with a “complaint” will be compelled to get his ears cut! We support an old Welsh custom!!’. The coroner stands between them, saying ‘this sort of thing must be stopped’.Footnote 113 The title of the cartoon is given as ‘coroner’s ban deplored – in municipal circles’ and is likely a comment on contemporary local politics within the municipal organisations.Footnote 114 It appears that TLl is being depicted as a mock disciplinary measure to silence dissent within municipal circles at the time. The description of TLl as an ‘old Welsh custom’ suggests a perception of TLl as a rustic, traditional, and quintessentially Welsh practice among the paper’s readership.Footnote 115 The depiction of an oversized, blood-stained razor and an axe on the table also hint at a perceived brutality of the practice and taken together it is possible that this image attempts to associate the taller, unidentified official with a sense of severity. The cartoon featuring on the front page also shows the degree of interest TLl clearly aroused among the readership.
Illustration referring to TLl featuring on page 1 of Llanelly Star’s issue of March 18th, 1933. Illustration by Harold Hodges and permissions granted by Reach PLC on behalf of Llanelli Star on May 4th 2023. Source: National Library of Wales, Aberystwyth.

Remembering TLl – What do the interviews reveal about the embodied experience and public perception of the practice in the post-war era?
The following section will now turn mostly to the interviews recorded over the course of 2023 by the primary author, in an attempt to highlight the personal experience of TLl for those undergoing, witnessing, or recollecting it. On a wider level, the following section will also consider how local communities came to understand TLl and the reasons for undergoing it.
In the only extant first-person account of someone who underwent TLl, Clive Evans (CE) of Brynamman in the Upper Swansea Valley recalled how on a spring day in the late 1940s he was taken by his mother to Penygroes near Ammanford. Here, he had his left earlobe cut with a razor. He recalls being cut by a local woman because his mother thought he was ‘meddal’ [soft] and that his ‘mind was wandering’.Footnote 116 It may be possible to interpret this as another cognitive indication for TLl, perhaps a perceived learning difficulty and/or attention deficit since he later suggests that this issue was affecting his concentration at school. This is in line with previously reported cognitive indications for TLl such as ‘backwardness’.Footnote 117 Clive recalled the woman cutting ‘behind the lobe’ of his left ear with a ‘cut-throat’ razor and that he remembers no significant pain, characterising the brevity of the process as ‘a little slit and that was it’. Clive’s account establishes that even by the post-war era, the practice was still carried out in parts of South Wales. Clive also said he felt that the procedure ultimately had ‘no effect’ on him.Footnote 118 Another revealing statement was when Clive referred to the expression of ‘Torri’r Llech’ being more common than the procedure itself, since he could not recall hearing of anyone but himself undergoing it.Footnote 119 This suggests that by the post-war era TLl was increasingly occupying a more prominent place in the imagination and daily vernacular of the local community rather than in their day-to-day sickness experience as a physical procedure. Clive also discussed how the family most often utilised the local ‘family doctor’ when they required medical care.Footnote 120 This represents a continuation of the tendency for local people to utilise TLl alongside, and with equal regard to, other sources of care for specific complaints.
Raymond Davies (RD), also a native of Brynamman, recalled his brother being cut in 1948 by another female practitioner.Footnote 121 He recalled that she visited their home, cutting ‘a little snick’ behind the ear as his brother was perceived as being ‘slow’ or ‘backward’ at the time. He goes on to state his belief that TLl was akin to a ‘ritual’ and that the lady who performed it was herself ‘a fortune-teller’ living locally. Raymond recalled his then six-year-old brother crying whilst the procedure was done, demonstrating how TLl could be experienced as a distressing procedure, especially by children. He does not recall another visit from the woman and like CE’s account does not believe it had any tangible effect on his brother’s health or wellbeing.Footnote 122 Interestingly, he also recalled how TLl was practised by a chemist in Ammanford just at the beginning of the Second World War.Footnote 123 This is particularly revealing as it highlights the plurality of practice during this period, with a wide range of practitioners performing TLl across multiple domains. Withey’s study of probate inventories in early modern Wrexham reveals a similarly dynamic situation whereby practitioner titles were more fluid and where bloodletting appeared to be routinely carried out by multiple different characters (including surgeons, apothecaries, and barber-surgeons).Footnote 124 RD’s account suggests that this plurality of practice continued for much longer in parts of South Wales.
Whilst not one of the interview accounts, Roy Noble’s published autobiography sheds further light on the practice of TLl during this period. He mentions how TLl was used as a threat during his childhood in the mid-1950s to optimise his performance ahead of the eleven-plus examination.Footnote 125 He mentions how a woman in Gwaen-Cae-Gurwen in Glamorganshire carried out the practice and even describes the procedure in detail. He mentions how the procedure involved ‘a bowl of hot water, a towel and a sharp knife…She made a small cut in the lobe’.Footnote 126 These basic implements appear common to the material culture of the practice as far back as the case of John Jones in 1875. He also describes the indication for TLl as if a child ‘had promise’ but was not ‘firing on all cylinders in school’, implying a strong educational context to TLl by the 1950s.Footnote 127
Former Welsh rugby captain Sir Gareth Edwards (GE) recalled in his interview that around 1952 he was taken to a general practitioner as a child by his mother who inquired as to whether he should undergo TLl to attenuate his apparent hyperactivity. However, the doctor reportedly answered that TLl would be the wrong treatment for this complaint as they believed the purpose of TLl was to revitalise someone perceived as overtly languid, and so would not make the young Sir Gareth more sedate.Footnote 128 This suggests that by the early 1950s, the very word llech had become a contronym referring at once to states of hyperactivity as well as states of hypoactivity, or ‘slowness’ (the indication in CEs case). All the while, however, academic sub-attainment by either of these means seems to have been the driving force for consideration of TLl. GE’s interview also demonstrates that even local doctors in Gwan-Cae-Gurwen not only knew of the practice but did not overtly oppose it, as the doctor seemed to have objected merely on the basis of intended effect, and not efficacy or safety. Like RD’s account relating to the Ammanford chemist performing TLl, this too suggests a degree of interaction between official and lay practitioners with regard to TLl. Footnote 129 Sir Gareth’s testimony also sheds light on the wider community’s perception of TLl as he mentions how common the expression and its associated terms were in their everyday parlance. For example, he mentioned how a common expression was ‘Dere man chi’n fel llech’ [’Come on you’re like llech’], typically aimed at someone who was perceived as ‘slow’ or ‘subdued’, suggesting that in this context llech was taken to mean a lack of energy.Footnote 130 This correlates with CE’s account who recalled the everyday use of terminology associated with TLl, further highlighting the prominent role it played in the collective imagination of the local communities in which it existed. GE also recalled that there were people who practised TLl in Gwaen-Cae-Gurwen but that he had never seen the procedure done nor indeed had it performed upon himself, though understood it to involve cutting the earlobe.Footnote 131
Gethin Edwards’ (GnE’s) interview not only corroborated much of what was said in his brother’s interview but also offered further insight into the public perception of TLl. He mentioned how he believed TLl to have persisted in Gwaen-Cae-Gurwen into the 1960s and that it was ‘something that was talked about, wasn’t taboo and was a genuine concern to try and cure people’.Footnote 132 This reveals that even at this relatively late stage, TLl was still seen by many as a legitimate, curative practice within the local medical marketplace. Similar to Noble’s account, he also mentions how TLl was often used as a threat by parents to try and influence their children’s behaviour.Footnote 133 GnE’s description of the procedure as a ‘snip of the earlobe’ also reinforces the impression of an apparent transition away from deeper cuts of the cartilaginous parts of the ear and towards less severe cuts of the earlobe.Footnote 134 By the time Gethin started attending school in the more industrialised areas of the Swansea Valley, he mentions how he no longer recalls hearing of TLl, indicating a potential retreat of the practice towards the more rural areas of the region.Footnote 135
An idea of the astonishing longevity of TLl is revealed in Richard White’s (RW’s) account. RW, himself a native of Pontardawe in the Swansea Valley, mentions a recollection from his wife (Mair White, a teacher at the time in Cwmllynfell) regarding a child in her class.Footnote 136 He recalls how the child was doing ‘very badly’ academically and Mair apparently remembered the parents saying to each other ‘Mae eisiau Torri’r Llech’ [[the child] needs TLl]. This suggests that the parents believed the child may benefit academically from TLl. RW goes on to mention that TLl was ‘so rare even then’, hinting at a period where perhaps only isolated pockets of the practice still existed.Footnote 137 He also mentions how this was the first time that Mair, herself a Welsh speaker, had ever heard of it and incredibly goes on to mention that this event occurred ‘in the 70s or the 80s even’.Footnote 138 Whilst this account tells us less of what the individual experience of TLl may have been like at this late stage, it is still significant and could prove to be the most recent evidence of an active bloodletting practice in a humoral tradition native to Britain.
Overall, it appears that the embodied experience of TLl by the post-war era was highly variable, ranging from one of distress (as witnessed by RD) to one of apparent passivity (as described by CE). Less variable appears to be the wider societal perception of the practice within the communities where it was practised, since in all instances TLl appears to have been deployed as a sincere and well-meaning measure. In order to explain these later characteristics of the practice, it may be helpful to consider the ways in which it evolved over time.
Torri’r Llech – How did it change and what can we say of its wider significance?
Over time the procedure of TLl clearly underwent considerable change. In earlier instances, such as in the case of John Jones, cuts through the full depth of the ear’s cartilage are featured.Footnote 139 In later references, incisions over the cartilage of the ears are still mentioned; however, sources hint at more superficial wounds. For example, the Warboy case in 1933 mentions a cartilaginous cut but that the boy only bled slightly, raising the possibility of more superficial incisions by this point in time.Footnote 140 In 1921, the county medical officer for Carmarthenshire also referred to the procedure of TLl as ‘making an incision into a certain part of the cartilage’.Footnote 141 However, all references after the Second World War reference cuts of the ear lobes and this likely represents the final iteration of the practice over time.Footnote 142 As to why the methodology evolved in such a manner is more uncertain, though it is possible that the publicity generated by cases of alleged malpractice (inquests of 1875 and 1933) may have served to encourage practitioners of TLl to modify their procedures to become less injurious.
There also appears to have been a demographic change in the practitioners of TLl, with a shift from mostly men to almost exclusively women by the start of the First World War. A preponderance of male bloodletting practitioners has previously been noted by Paster in the early modern period as well as by Meek in the eighteenth century.Footnote 143 TLl does, however, raise the interesting possibility that within vernacular medical contexts, this pattern continued well into the nineteenth century before an apparent trend towards female bloodletters by the interwar period. Another possible explanation arises from the observation that this switch in practitioner sex occurred alongside a parallel change in the local population’s perception of those carrying out TLl. In 1875, John Jones’ mother referred to Richard of the Mill as a ‘doctor’ and paid him ‘three-pence’ for his services.Footnote 144 Contrast this with later cases such as Mrs Rosser who was neither paid for carrying out TLl nor referred to as ‘doctor’.Footnote 145 This suggests that earlier on, TLl was perceived more as a professional service demanding financial remuneration. Later, as biomedical institutions started to solidify their place as medical orthodoxy, it is possible that TLl was increasingly perceived in opposition as a folk or domestic remedy by its patrons. Whilst it does not appear that this impacted the perceived efficacy of the practice, as locals remained staunch supporters, it may have engendered a demographic change in those carrying out the procedure.Footnote 146
The indications for TLl also seem to have undergone several transformations over time, with the very meaning of llech undergoing parallel changes. In earlier sources, TLl was seemingly used to treat states of acute critical illness. This was the case in 1875, with John Jones presenting as acutely unwell and with the local doctor summoned to the inquest defining llech as ‘difficulty breathing’.Footnote 147 By 1921 the first cognitive indication for TLl is observed, as ‘backwardness’ in children is described as an indication.Footnote 148 At the same time, ‘weakness and debility’ is given as an indication in adults.Footnote 149 This may represent a trend towards cognitive indications of perceived mental ‘slowness’ in children, but a persistence of general poor health as an indication in adults. Contrary to this is the treatment of William Warboy in 1933, as the baby appeared to have presented with symptoms of heart failure and therefore likely presented as acutely unwell.Footnote 150 This illustrates how the indications for TLl should not be perceived as discrete or consistent with modern biomedical nosologies of disease. As TLl was an unregulated practice, indications for treatment are likely to have been locally defined and naturally more nebulous. This does not, however, preclude the existence of a general trend towards cognitive indications such as ‘backwardness’ in children.
By the early post-war era, indications for TLl seem to undergo a final change. Whilst RD cited ‘slowness’ as a reason his brother was cut in 1948, CE believed he himself was cut as his ‘mind was wandering’.Footnote 151 This suggests that a degree of attention deficit or difficulty concentrating could also be considered as indications for TLl. This is then supported by GE’s account where TLl was considered to counteract his perceived hyperactivity, with the local doctor then suggesting that TLl may well only worsen the issue.Footnote 152 This suggests that by the post-war era, the very word llech had become a contronym referring at once to states of hyperactivity as well as states of hypoactivity, or ‘slowness’. All the while, however, academic sub-attainment by either of these means seems to have been the driving factor for consideration of TLl (as observed in RW’s account).Footnote 153 The fact that this educational focus came into being just after the Second World War may not be a coincidence. The 1944 Education Act promised free secondary education to all children aged between 5 and 15 and introduced the tripartite system which established grammar, technical, and secondary modern schools.Footnote 154 A single examination determined which of these schools a pupil would go to, becoming known as the eleven-plus examination.Footnote 155 Parents would utilise all manner of methods to attain a competitive edge for their children including helping with early reading, home tutoring and residing in locations with more grammar school places.Footnote 156 Clearly middle-class families had a financial advantage in the deployment of such measures, and it was not long before the data reflected this. In 1953, Halsey and Gardner found that middle-class pupils were more likely to attain grammar school places and experience onward academic success than working-class children.Footnote 157 Therefore in overwhelmingly working-class South Wales, it may not be so surprising that parents turned to the tools placed before them by a strong and resilient vernacular medical paradigm which sustained an ongoing belief in the efficacy of TLl for the purpose of revitalisation. Similar uses for bloodletting are seen in other sources, for example, the 1915 account of John Haddon, a physician from Hawick in the Scottish Borders, who describes how in previous generations prior to being bled patients were ‘languid and lazy’ but after ‘felt as if their youth was renewed’.Footnote 158 Another important factor which possibly affected the demand for TLl is the development of the National Health Service. By widening access to orthodox sources of care for physical health complaints, it is possible that working-class families simply had less impetus to employ the practice in meeting any physical health needs. This may further explain its persistence for largely cognitive and intellectual indications.
This change in indication for TLl over time may also help to explain a demographic transition in those undergoing the procedure. Whilst adults are frequently referenced as patrons of TLl up until as late as 1933, by the post-war era only children appear to have been cut. As learning difficulties resulting in academic sub-attainment became the overarching indication for TLl, it is possible that only children were cut as the optimal time to intervene in order to improve academic performance is during childhood.
Whilst TLl was clearly a dynamic practice, one aspect in which it exhibited remarkable stability was in its status as a constant challenge to biomedical orthodoxy. As previously alluded to, many authors have helped to reveal the ways in which the nascent biomedical culture of Europe, through close affiliations with imperial institutions, interacted with pre-existing vernacular medical paradigms across the globe. These interactions were highly varied in nature and could range from co-option to attempts at supplantation. However, it is also useful to remind ourselves that this competition also took place here in Britain and the previously discussed accounts demonstrate that TLl was a practice situated at the faultlines of this wider struggle, with an increasingly assertive biomedical establishment frequently coming to head with an ever-resilient clientele. The inquest of John Jones in 1875 is a case in point with the coroner comparing the practice to witchcraft, yet with the local population making their sense of indignation known at the proceedings by occupying the hall.Footnote 159 What is particularly remarkable about TLl is the apparent failure by official institutions to constrain the custom, as manifested by renewed hostilities in 1921, 46 years after the case of John Jones. It was at this point that Dr Hughes brandished TLl as a ‘pure fetish’ that ‘appeals only to the ignorant and superstitious’ in his quarterly report.Footnote 160 At the same time, however, it appears that hundreds of children were still being cut in Ammanford, with valley trains reportedly ‘full of whining children with bleeding ears’.Footnote 161 The Warboy case reinforces this point, with the practitioner of TLl, Mrs Rosser, even mentioning how she would cut adults as well as children. In usual fashion, the presiding coroner lambasted the procedure as ‘illegal and dangerous’.Footnote 162 It is therefore apparent that despite half a century’s worth of institutional efforts to castigate and condemn TLl, this often did little to attenuate faith in the practice. The recognition that even in industrialised societies vernacular healing practices existed in competition with official ones is not novel; the existence of such pluralism is well recognised.Footnote 163 Rather, what TLl demonstrates is just how resilient this pluralism could be in certain parts of Britain, and further challenges narratives of ubiquitous dominance of biomedical institutions during the first half of the twentieth century.
Torri’r Llech as a form of humoral bloodletting
The inclusion of TLl as a humoral bloodletting practice is supported both by the procedure itself as well as by its evolution over time. From the existing accounts it is clear that a variety of incisions were made, with more severe cartilaginous cuts featuring in earlier accounts eventually giving way to more superficial ones.Footnote 164 The location of incision also appeared to vary, from the upper portion of the inside of the ear eventually to the ear lobes.Footnote 165 This suggests that the physical location of the cuts was a less pertinent factor in achieving the desired effect, as the common aspect to all the documented methodologies is resultant bleeding. Indeed, bleeding is the only factor common to all the historical cutting methods of TLl suggesting it was this aspect of the practice that was central to its purpose. This is further supported in more detailed accounts of the practice, such as in the 1875 John Jones inquest. The man who cut the boy reportedly noted that he bled ‘very little’ on being cut, going on to advise that his mother use ‘warm water’ to clean the ears.Footnote 166 The fact that a deficiency of blood was consciously noted suggests that bleeding was the focal point of the procedure. Furthermore, the use of warm water would likely have encouraged further bleeding thus enhancing the haemorrhagic effect of TLl. This was not lost on the prosecution who stated that warm water would ‘increase haemorrhage rather than allay it’.Footnote 167 On cross-examination, the assistant-surgeon also describes how the cuts were everted and turned outwards at the margins, which may represent a further method to enhance bleeding.Footnote 168 It appears the coroner himself also believed TLl to be a form of bloodletting when he stated that ‘The stitch in the side is called llech, and bleeding is supposed to carry it off’.Footnote 169 The testimony of RD in relation to the cutting of his brother further supports this assessment, when he recollected ‘the nick was so small it was just [as] though they were pulling blood’.Footnote 170 Taken together, the commonality of bleeding as the final goal coupled with documented efforts to augment this process supports the conclusion that TLl was indeed a form of bloodletting.
The view that TLl represents a form of humoral bloodletting is shared by Thompson. He highlights how incidents of TLl reported in the press occurred chiefly during springtime, when blood was thought to be the dominant humour.Footnote 171 This is supported in primary sources, with CE also being cut in spring.Footnote 172 Seemingly instances where TLl was not performed in spring were in those cases where the indications for it could be considered emergencies, with John Jones suffering from an unknown acute illness in 1875 and William Warboy suffering from heart failure in 1933.Footnote 173 When TLl was done on an elective basis, it seems to have been done during spring. In Galenic belief systems, this season was traditionally associated with the qualities ‘hot’ and ‘wet’, corresponding with the humour of blood.Footnote 174
Numerous other historical examples illustrate this tradition. In fifteenth-century Wales, gwaedu’r gwanwyn [spring bleeding] was supposedly used to clear the body of amhurderau [impurities].Footnote 175 In medieval Ireland, bloodletting for the purposes of prophylaxis and health maintenance was also typically carried out during the spring or autumn, demonstrating that this was not a phenomenon unique to elective cases of TLl. Footnote 176 Furthermore, the accounts of Haddon in Scotland as well as that of an unnamed physician from Norfolk in 1915 and 1879, respectively, both cite bloodletting carried out in spring.Footnote 177 A final observation by Thompson arises from the understanding that in many humoral systems it is common to bleed veins that are distant from the affected site (and often on the opposite side of the body), to draw perceived excesses of morbid humours away from affected areas.Footnote 178 This practice, known as revulsive bleeding, was especially popular in the practice of Arabian physicians such as Avicenna.Footnote 179 In the case of TLl, Thompson then points out that to bleed a child with rickets from the ear therefore made perfect sense.Footnote 180 However, as has been observed the definition of llech did not appear to translate to the discrete clinical condition we know today as rickets but instead was likely a more nebulous term referring to generally poor states of health, mental ‘backwardness’, or extremes of energy levels. Despite the uncertain etymology of llech, the ears remain a peripheral site and in none of the documented cases were the ears the primary source of pathology. Therefore, it is still possible that bleeding from the ears was still influenced by a desire to draw morbid humours away from a principal site of concern. Furthermore, Noble describes the motive of TLl as ‘the belief being that, once the blood flowed, all the innate capabilities within you were released’, indicating again that the flow of blood was the central focus of the procedure and ultimately the effecting mechanism to bring about the desired effect.Footnote 181
Whilst TLl does appear to have been a form of bloodletting within a humoral conception of health and disease, it may well be more accurately described as a form of ‘popular humoralism’. As earlier described, this was characterised by Withey as a way in which people in Wales came to understand their bodies, where the body was understood in humoral terms alongside astrological, Christian, and vernacular theories of sickness and health.Footnote 182 The evidence discussed highlights that TLl was rooted in humoralism, and the persistence of astrological and indigenous Welsh influences has also been noted. Therefore, it does appear that TLl could most accurately be defined as a practice within the confines of ‘popular humoralism’.
The persistence of Torri’r Llech in South Wales
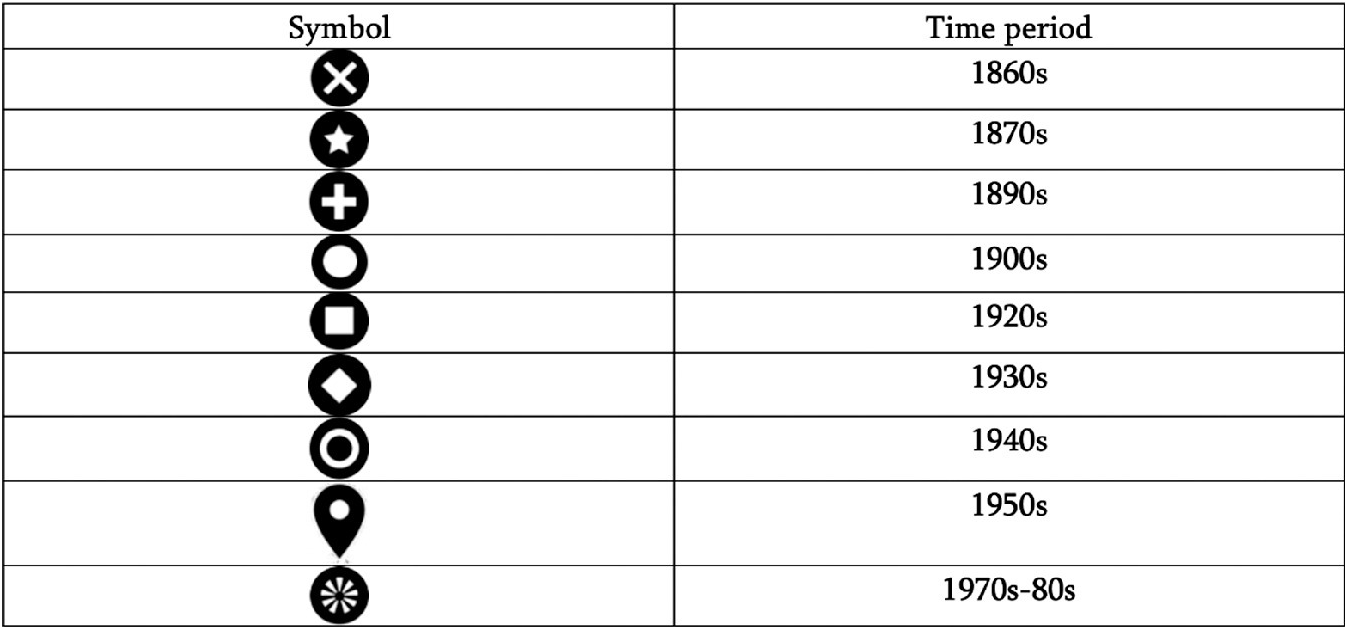
The existing accounts and secondary literature appear to support the assertion that TLl was a practice unique to Wales. Whilst bloodletting from the ears in cases of rickets appeared to be a wider approach promoted during the later seventeenth century, no other such practice has been identified in Britain or Ireland over a similar time scale, or for remotely the same constellation of indications, as TLl. Footnote 183 Whilst its use may have remained largely confined to Wales, it certainly was not static within the country itself and appears to have undergone a process of internal migration. Figure 3 illustrates this process, with a movement from largely rural areas of Mid and South Wales to mostly industrial areas of the south. By the 1940s, a final contraction then appears to have occurred in isolated pockets of the Upper Swansea Valley. Figure 3 was generated by mapping all known instances of TLl by location and decade, with Table 1 serving as a legend for interpretation. Part of this trend was also noted by Thompson, who described how TLl spread to urban areas of South Wales through the migration of people to the industrialised south.Footnote 184
A map of Mid and South Wales denoting the locations of documented references to TLl and the period in which they occurred. Table 1 serves as a legend to enable interpretation. Source: Map generated from Google My Maps and published under Google’s ‘fair use’ copyright policy.

Legend displaying the time periods referred to by various symbols used in figure 3. Source: Symbols obtained from Google My Maps and published under Google’s ‘fair use’ copyright policy.

The testimonies of CE and RD serve as the latest definitive accounts for the practice of TLl in the Upper Swansea Valley, placing it to the late 1940s.Footnote 185 Despite neither GE, RW, nor Noble physically witnessing the procedure, their accounts may still suggest a persistence of the practice through the 1950s, with the interview of RW hinting at the possible existence of TLl even as late as the 1980s.Footnote 186 This would appear to confer a longevity to TLl that is unique to bloodletting in a humoral context in Britain or Ireland. In England, where unorthodox practice was already less pervasive than it was in Wales, there is little evidence for bloodletting being carried out in line with a humoral paradigm by the mid-twentieth century.Footnote 187 Though bloodletting continued to be recommended in the later editions of Osler’s textbooks in the 1930s, it’s unlikely that these recommendations were drawing on humoralism but rather on more rational-empirical epistemologies.Footnote 188 This insight can more broadly be applied to instances of bloodletting carried out by physicians or surgeons in the twentieth century and so it is likely that the only instances where bloodletting was carried out in a humoral context would be in lay and unorthodox settings.Footnote 189 In Scotland, Hamilton has already alluded to the apparent unpopularity of bloodletting in such contexts.Footnote 190 In Ireland, Grace identifies a 1938 reference where an Agnes Boyle from Co. Mayo recalls bloodletting being carried out ‘in the olden times’ by two ‘quacks’.Footnote 191 Based on the current literature, it therefore seems likely that TLl does in fact represent the latest example of a bloodletting practice carried out in a humoral context native to the British Isles. Whilst the practice of Unani Tibb also draws on humoral traditions, and is indeed practised across the UK today, it did not originate in Europe and therefore lies beyond the scope of this work.
Conclusion
In this article we have endeavoured to situate TLl within the wider historiography of Welsh unorthodox medical practice, as well as of bloodletting more widely. We drew on a collection of existing as well as novel sources to describe some of the more widely publicised legal inquiries and notable accounts relating to TLl. In doing so we aimed to document the practice having delineated its origins, demarcated its practice and also having explored the ways in which it was understood by those around it. This then facilitated a consideration of TLl’s adaptability in the ways that it evolved over time, and how it could also serve as a useful litmus test for the wider perception of unorthodox practices among the burgeoning biomedical institutions of the late nineteenth to early twentieth centuries. The relative failure to stamp out what these same institutions perceived as a ‘pure fetish’ also challenges more teleological accounts of biomedical progress and dominance here in Britain.Footnote 192 TLl then found further significance through a consideration of its material culture, revulsive nature, and predominance to be carried out in spring which allowed us to situate it as a popular humoral practice. In doing so, this argument reinforces a lineage between Welsh folk practices and wider European medical paradigms. Moreover, by again drawing on the relevant literature and especially on the interview material TLl was identified as potentially the last bastion of humoral bloodletting across the span of the British Isles, with one reference alluding to its survival possibly as late as the 1970s to 1980s in the Upper Swansea Valley.Footnote 193
Whilst TLl undoubtedly reveals much about the longevity of humoralism, it is also important to recall the harm that the practice could inflict on those undergoing it. This is most clearly demonstrated in the case of John Jones.Footnote 194 Whilst TLl undoubtedly did little to allay the boy’s suffering, it is useful to recall that even orthodox practitioners at the time were unlikely to have been able to offer much more in the way of curative treatment. Rather what such cases exhibit is a wider trend seen across almost all reports of TLl, which is that patients, or their caregivers, were always sovereign in their utilisation of the practice for specific complaints. People would consult doctors, cunning folk, or even friends and family as part of a diverse local medical marketplace, with TLl representing just one of many available options. This may seem to confer a banality to the practice, but we would in fact argue that this insight could serve as TLl’s greatest legacy since it demonstrates the profoundly pluralistic nature of Welsh medical and health-seeking practices. Critically it also reminds us that even in parts of Britain, far from being secure in their authority, biomedical establishments were still firmly in competition with unofficial modes of care even as late as the mid-twentieth century.
Acknowledgement
With thanks to Roy Noble for helping to locate interviewees during the early stages of the project.
Contributions
TKW conducted literature review, undertook all interviews as well as drafting, revisions and submissions. MC read and commented upon drafts, providing critical guidance during the re-drafting process. The literature review and interviews were completed as part of TKW’s Diploma in the History of Medicine at the Worshipful Society of Apothecaries.
No ethical approval required.
No external funding received.
No conflict of interest for either TKW or MC.




 Open access
Open access