


What nutrition challenges do Deaf communities face?
Hearing loss is a growing global public health challenge. Current estimates suggest that over 1·5 billion people globally, representing nearly one-fifth of the world’s population, live with some level of hearing loss(1). Among these individuals, approximately 430 million experience disabling hearing loss, and this number is estimated to exceed 700 million by 2050(1).
Access to ear and hearing care services is still limited due to a global shortage of trained professionals and specialists(1). This gap is more evident in low-and middle-income countries, where the need for healthcare services is highest. Consequently, fewer than one in five people who need hearing care services are able to receive them. Unaddressed hearing loss carries a substantial economic impact, with global costs estimated at nearly US$1 trillion annually(1).
Nutrition plays an essential role in maintaining health and preventing disease. Although hearing loss is one of the most prevalent sensory impairments worldwide, nutrition-related challenges among individuals with hearing impairment are often neglected(Reference V, Pasha and Fatima2). Despite the well-known and widely promoted importance of health literacy, many Deaf individuals face significant barriers to understanding medical terms and treatments, often due to a lack of sign language proficiency among healthcare professionals(Reference Naseribooriabadi, Sadoughi and Sheikhtaheri3).
Food insecurity is also a common concern among Deaf adults, which is associated with low income, depression and reduced quality of life(Reference Engelman and Kushalnagar4). According to the U.S. Household Food Security Survey screener, many adults with hearing impairment reported difficulty making food supplies last and lacked the financial means to purchase more within the past year(Reference Kushalnagar, Moreland and Simons5). Moreover, adults with hearing loss may experience a reduced ability to shop for and prepare food, alongside financial strain due to poorer physical health, consequently increasing the risk of food insecurity(Reference Gopinath, Tang and Tran6).
Evidence also indicates that Deaf adults experience a higher burden of obesity, type 2 diabetes risk and CVD risk factors compared with hearing populations(Reference Emond, Ridd and Sutherland7). In a UK-based study of 298 Deaf British Sign Language users, obesity prevalence was high, particularly among older adults(Reference Emond, Ridd and Sutherland7). Rates of high blood pressure were higher than those reported in the Health Survey for England (37 % v. 21 %), with 29 % of participants unaware of their condition and 42 % having poorly controlled blood pressure despite having initiated treatment. In addition, one-third of participants had elevated total cholesterol levels. Although self-reported CVD was less prevalent than in the general population, treatment rates were substantially lower(Reference Emond, Ridd and Sutherland7).
According to another study in the USA, adults with hearing loss were more likely to report chronic diseases such as CVD, compared with adults with good hearing, and disparities increased as the severity of hearing loss worsened(Reference Glassman, Jordan and Sheu8). Adults with hearing loss reported lower alcohol consumption but were substantially more likely to be unable to engage in regular moderate or vigorous physical activity(Reference Glassman, Jordan and Sheu8). Moreover, a systematic review reported consistent evidence of health inequalities among Deaf signing populations compared with the general population, including a higher prevalence of obesity, hypertension and mental health problems such as depression and anxiety, as well as poorer quality of life and overall health status in this population(Reference Rogers, Rowlandson and Harkness9).
Beyond physical health, these challenges diminish the overall quality of life. The US Department of Agriculture has reported an association between disability, poverty and food insecurity, noting that disability substantially increases the risk of living in poverty, which in turn increases the chances of experiencing food insecurity, considering that individuals with disabilities also face higher healthcare costs(Reference V, Pasha and Fatima2). In addition, those living with food insecurity are more susceptible to developing major depression or anxiety disorders(Reference Engelman and Kushalnagar4). Evidence shows that Deaf children also witness higher rates of undernutrition, stunting and dental problems in comparison with other children(Reference V, Pasha and Fatima2).
How can we prevent nutrition inequities in Deaf communities?
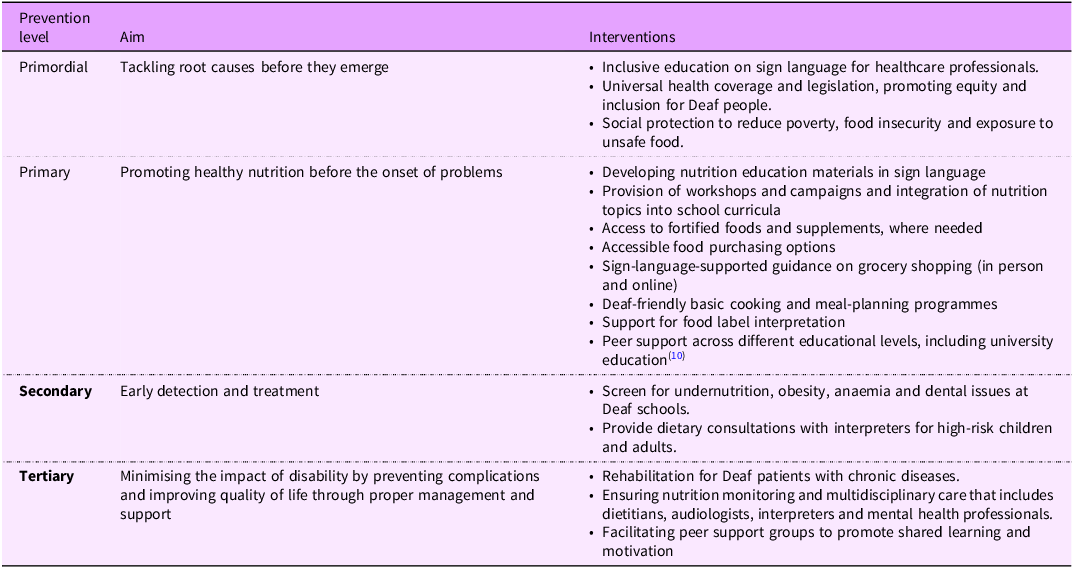
Closing the nutrition gap in Deaf communities requires a comprehensive, life-course approach. Many policies use one-size-fits-all approaches, lack disability-disaggregated data and exclude Deaf voices from decision-making. Primordial, primary, secondary and tertiary preventive strategies may mitigate the influence of the threat within the Deaf community. Examples are provided in Table 1.
Prevention strategies to diminish nutritional inequalities in Deaf communities

Note. Prevention levels are based on the public health prevention framework, including primordial, primary, secondary and tertiary preventions.
Examples of good practices
Governments and health organisations around the world have initiated implementing effective strategies to reduce health disparities and improve nutritional status among Deaf individuals. The WHO’s International Classification of Functioning, Disability, and Health provides a global framework for assessing health and disability at both individual and population levels(Reference V, Pasha and Fatima2). As another example, the government of India has supported Deaf children by promoting their inclusion in mainstream schools to build confidence and encourage their participation in social activities(Reference V, Pasha and Fatima2). The mid-day meal programme in India, which provides free nutritious lunches in public schools, has significantly reduced malnutrition and improved school attendance among children, especially in disadvantaged communities(Reference V, Pasha and Fatima2). Targeted education programmes have also shown positive results in improving the nutritional status of Deaf people. For instance, a school-based programme that was implemented for 6 months for Syrian refugee children in Lebanon resulted in improvements in dietary knowledge, attitudes and BMI scores(Reference Keogh, Kushalnagar and Engelman11).
What will it take to close the nutrition gap for Deaf individuals?
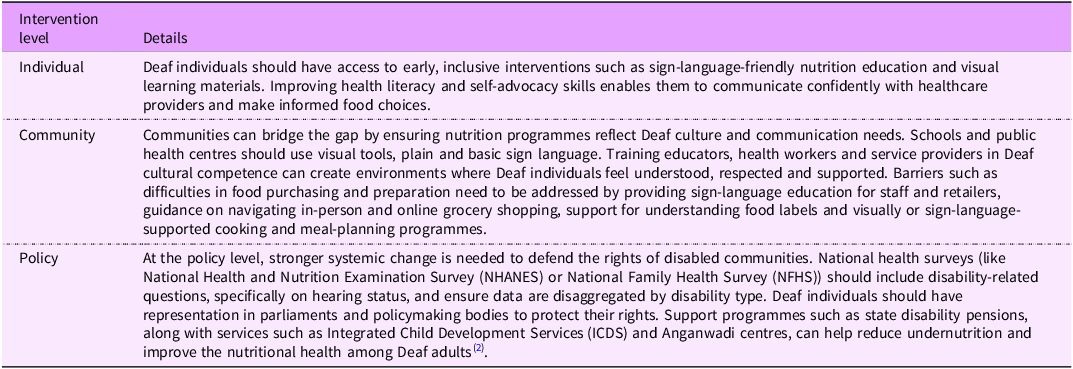
Addressing persistent nutrition-related disparities among Deaf individuals requires a comprehensive, multi-level approach that integrates actions at the individual, community and policy levels (Table 2).
A comprehensive approach for solving the problem

Note. This table outlines a conceptual, multi-level public health framework (individual, community and policy) for addressing nutrition inequities in Deaf communities.
Conclusion
Deaf communities face significant nutrition-related challenges that must be addressed. Closing this gap requires coordinated action across multiple levels. Ensuring accessible nutrition education, strengthening cultural and linguistic competence within health systems and integrating disability-disaggregated data into national surveys are some of the essential steps. Additionally, Deaf individuals should be actively involved in the development and evaluation of programmes and policies intended to support them. Implementing these strategies can help reduce the often ‘hidden’ burden of nutritional inequities experienced by Deaf individuals.
Data availability statement
This commentary does not contain original research data. No new datasets were generated or analysed for this work.
Acknowledgements
Not applicable.
Authorship
A.R. conducted the literature review and drafted the manuscript. D.A. provided supervision, contributed to the critical revision of the manuscript, revised and approved the final version.
Writing assistance: The authors received no third-party writing or editorial assistance for this commentary.
Financial support
The authors received no specific funding for this work.
Competing interests
The authors declare no conflicts of interest.
Ethics of human subject participation
This commentary did not involve human participants, animals or primary data collection requiring ethical approval.
Consent to participate: Not applicable.
Consent for publication: Not applicable.

 Open access
Open access