


Autism is a neurodevelopmental condition characterised by difficulties in social interaction and communication, along with repetitive and restricted behaviours, interests or activities. 1 Barriers to diagnosis include lack of awareness, limited services and funding. Approximately 1.1% of the UK population meets the criteria for autism spectrum disorder (ASD), with similar global estimates. Reference Micai, Fulceri, Salvitti, Romano, Poustka and Diehm2,Reference Zeidan, Fombonne, Scorah, Ibrahim, Durkin and Saxena3
Autistic individuals are at increased risk of mental health conditions, including obsessive–compulsive disorder, bipolar disorder, psychosis, anxiety, eating disorders and depression. Reference Eberhard, Billstedt and Gillberg4,Reference Lai, Kassee, Besney, Bonato, Hull and Mandy5 Suicidality is also elevated, with autistic people nearly three times as likely to die by suicide. Reference Hirvikoski, Mittendorfer-Rutz, Boman, Larsson, Lichtenstein and Bölte6 Factors such as social isolation, perceived burdensomeness and life stressors contribute to this risk. Reference Wood, Drahota, Sze, Har, Chiu and Langer7 High rates of anxiety (42%) and depression (37%) are common, Reference Gajwani and Minnis8 with anxiety amplifying core ASD symptoms and increasing the risk of self-harm. Reference Bennett, Jambon, Zaidman-Zait, Duku, Georgiades and Elsabbagh9
Autistic individuals also face higher exposure to abuse, victimisation and financial exploitation. 10 Early emotional dysregulation linked to family adversity is a strong predictor of later mental health difficulties, Reference Day, Simmons, Shade, Jennison, Allely and Mukherjee11 contributing to a ‘double jeopardy’ of neurological and environmental risks.
Males are more frequently diagnosed than females, with a shifting male-to-female ratio of 3:1. Reference Zeidan, Fombonne, Scorah, Ibrahim, Durkin and Saxena3,Reference Hsu, Chu, Tsai, Hsu, Huang and Cheng12 Some research suggests sex-based differences in co-occurring conditions and traits like camouflaging, although these are not unique to females. Reference Gaetano13,Reference Underwood14 Understanding such differences may support more tailored service provision.
Method
The current study was taken from a subset of analysis completed when exploring the phenotype of men and women presenting to a clinical service. The original study examined sex-specific phenotype of ASD in a random cohort of men and women, as part of a retrospective case-note audit. Reference Underwood14
The original study had been registered as a service evaluation piece with the internal Surrey and Borders Partnership NHS Foundation Trust (SABP) clinical governance procedures. Reference Underwood14 Full ethical approval was therefore not required.
The original study, looking at the ‘female phenotype’, was completed using a modified Delphi process to develop and create an audit checklist. To extract information around male and female phenotype presentations, a review of the literature was completed before a set of descriptors extracted. These were then presented and discussed with a small expert consensus group within the clinical team, and a further set of questions looking at wider factors was included. As part of this, additional information was sought. This was to create the overall audit checklist. Questions added included those around trauma, aetiological risk factors for neurodevelopmental conditions such as prenatal alcohol or prematurity, alongside an additional mental health diagnostic checklist. Although these variables are not necessarily independent as often trauma, comorbidity and prenatal alcohol are interlinked and contribute to childhood adversity, so the study analysed the factors independently. No specific tools were used in the final audit, but the questions were based on those found in the Patient Health Questionnaire-9 (PHQ-9). Overall, a total of 103 questions were included in the audit.
Participants were randomly selected from those seen in the SABP neurodevelopmental service historical record from 2013 to the point of audit completion in 2017. Assessments were conducted by two individuals, and every tenth assessment was quality checked by a third person. For any discrepancy in the quality check procedure, the wider supervisory team were consulted and a consensus reached. This allowed better reliability of the audit process. In total, 75 men and 75 women were included in the evaluation. All participants were aged ≥18 years and had been diagnosed with autism within the SABP specialist service. These were all clinical diagnoses and data extraction was obtained from the completed reports.
Data were compiled and analysed using SPSS version 26 for Windows (IBM Corp., Armonk, NY, USA; https://www.ibm.com/products/spss-statistics). All questionnaire items were analysed using a cross tabs procedure in SPSS to review frequency data, and chi-squared analysis was carried out to assess statistically significant differences. A Holm–Bonferroni correction was used to reduce the chance of type one error. Reference Gaetano13 The analysis presented here primarily focuses on the phenomenological outcomes, such as presence or absence of a particular diagnosis, e.g. depression or eating disorder. A full description of the process can be found in the original paper. Reference Day, Simmons, Shade, Jennison, Allely and Mukherjee11
Results
In total, 150 individuals were included within the study, 75 men and 75 women. Nearly 40% (n = 29) of the women were aged 25–44 years, and 30% of the males were aged 35–44 years or between the ages of 18 and 24 years. Regarding education, 42% of the women and 35% of the men had attended college as the highest level of education. Regarding employment, 7.9% of the women and 20% of the men were working in high-skilled jobs. Regarding relationships, 23% of the men had never been in a relationship, whereas this was 10% for the women; 29% of the men were married, whereas this was 21% for the women. Only 4% of the men and 1% of the women were in supported living, with the remaining either staying with family, living with a partner, living with friends or living alone. Table 1 demonstrates the demographics of the participants.
Demographics

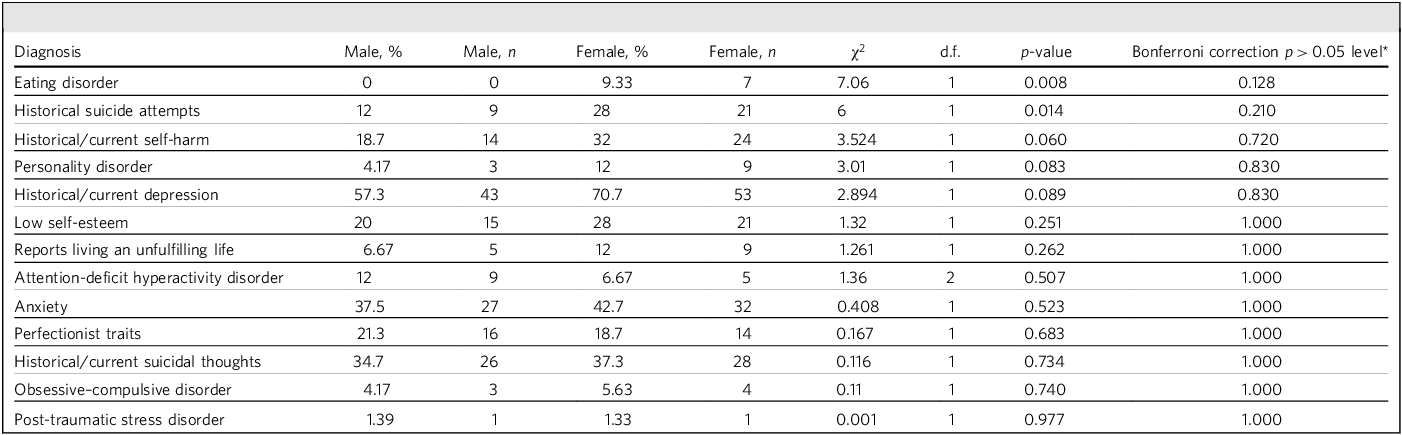
Mental health diagnoses were common among this cohort: 36% had current suicidal ideation, 20% had attempted suicide, 40% had a past or current diagnosis of anxiety and 62% had a past or current diagnosis of depression (Table 2).
Comparison of mental health outcomes seen in male and female sexes
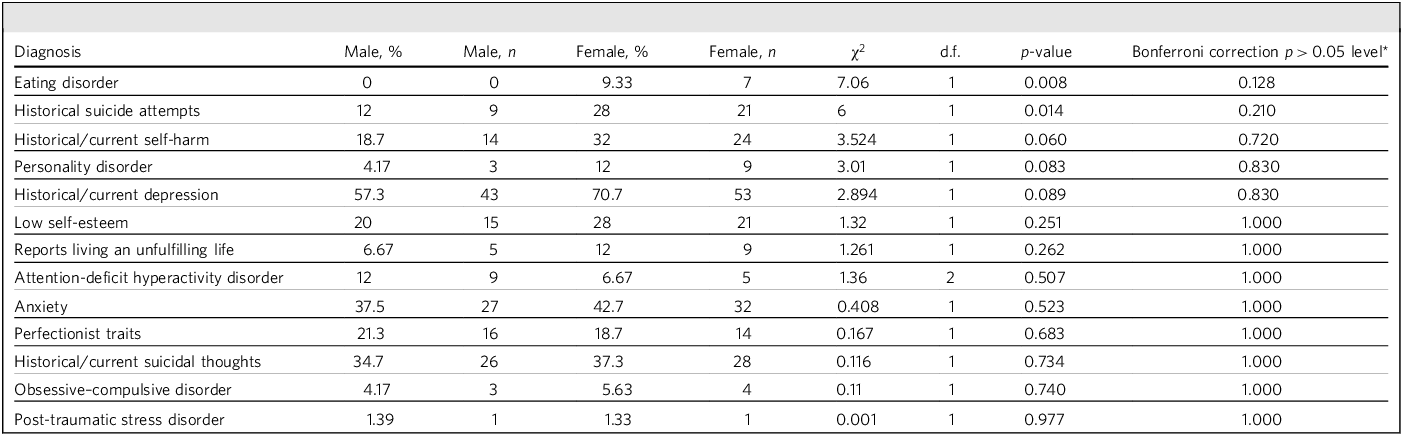
When using the unadjusted chi-squared model, more women had a diagnosis of an eating disorder (9.3% for women, 0% for men; p = 0.008), a past suicide attempt (21% for women, 9% for men; p = 0.014) and anxiety (53% for women, 40% for men; p = 0.029). However, once a Holm–Bonferroni correction was made, no significant statistical difference between men and women and the diagnosis of a comorbid mental health disorder was seen (all p > 0.05 Holm–Bonferroni correction). Reference Martini, Butwicka and Taylor15
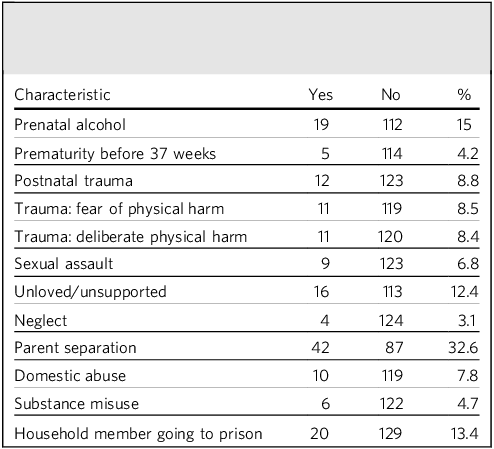
When considering factors that may have contributed to this outcome beyond the diagnosis alone, 32.6% of the cohort experienced parental separation and 15% had been exposed to prenatal alcohol. Nearly 10% had also experienced postnatal trauma, physical trauma, abuse, neglect or assault. It was unclear if these individuals were the same people or overlapping. It was not possible to correlate the characteristics in a multivariate model because of the numbers involved.
Table 3 demonstrates that prenatal exposure to substances, especially alcohol and postnatal trauma, is more common among autistic people, regardless of sex.
Aetiological and risk factors linked to the neurodevelopmental and psychiatric presentations seen in the cohort

Discussion
The findings of this study align with existing literature highlighting the complex intersection between autism and co-occurring mental health conditions. Autism, defined as a neurodevelopmental condition characterised by difficulties in social interaction and communication, as well as restrictive and repetitive behaviours, 1 is often underdiagnosed or diagnosed late because of barriers such as limited public awareness, lack of service availability, and funding constraints. Reference Micai, Fulceri, Salvitti, Romano, Poustka and Diehm2 This is concerning, given estimates suggesting that 1.1% of the UK population meets criteria for ASD, with similar global prevalence rates. Reference Zeidan, Fombonne, Scorah, Ibrahim, Durkin and Saxena3
There is growing recognition that autistic individuals are at significantly higher risk for developing a range of mental health conditions, including obsessive–compulsive disorder, bipolar disorder, depression, psychosis, anxiety and eating disorders. Reference Eberhard, Billstedt and Gillberg4,Reference Lai, Kassee, Besney, Bonato, Hull and Mandy5,Reference Hirvikoski, Mittendorfer-Rutz, Boman, Larsson and Lichtenstein16 Alarmingly, research has found that autistic individuals are also at increased risk for suicidality, with suicide attempts and deaths occurring at roughly twice the rate of the general population. Reference Hossain, Khan, Sultana, Ma, McKyer and Ahmed17,Reference Hartley18 Life stressors, social isolation and perceived burdensomeness have been identified as contributing factors. Reference Hirvikoski, Mittendorfer-Rutz, Boman, Larsson, Lichtenstein and Bölte6 In addition, the high prevalence of anxiety (up to 42%) and depression (37%) in autistic individuals has been linked to exacerbation of core ASD traits and increased risk of self-harm. Reference Wood, Drahota, Sze, Har, Chiu and Langer7,Reference Gajwani and Minnis8
This cohort demonstrates no differences in the type or frequency of mental health diagnoses between autistic males and females. Despite the increased ratio of males/females, very few studies have explored the differences in mental health diagnoses between the two sexes. One study demonstrated autistic males were more likely to have a diagnosis of ADHD, but less likely to have bipolar disorder or schizophrenia. Reference Gaetano13 A previous large population-based cohort demonstrated that females are particularly more likely to develop anxiety, sleep or depressive disorders when compared with autistic males. Reference Hirvikoski, Mittendorfer-Rutz, Boman, Larsson and Lichtenstein16 However, although the women in our study had higher rates of an eating disorder, anxiety and self-harm, this was not statistically significant. This may be a result of the relatively small sample size in our cohort. This potentially has implication in service delivery and support needed for these groups.
This study highlights that autistic people have high rates of mental health conditions. This reiterates previous research that demonstrated increased rates of eating disorders, anxiety, psychosis and obsessive–compulsive disorder. For instance, a previous large population cohort found that both male and female autistic individuals were three times more likely to develop a mental health condition and were significantly more likely to be admitted to hospital. Reference Hirvikoski, Mittendorfer-Rutz, Boman, Larsson and Lichtenstein16 Furthermore, there is an increased risk of suicide, self-harm and suicidal thoughts. Potential explanations for this include the increased risk of traumatic life experiences such as isolation, victimisation and perceived burdensomeness. Not only do these experiences occur more frequently when someone is autistic, but they increase the risk of mental health conditions, which can also further perpetuate these experiences. Reference Douglas and Sedgewick19–Reference Cage, Di Monaco and Newell21 Mental health conditions can also amplify some of the behaviours associated with autism, such as social difficulties, repetitive behaviours and sensory challenges.
The present study also found that prenatal exposure to substances, especially alcohol and postnatal trauma, is more common among autistic people, in this sample. This double effect, where neurological vulnerability is compounded by external traumatic experiences such as victimisation, unemployment or abuse, Reference Martini, Butwicka and Taylor15 emphasises the need to consider both aspects in the presentation of autistic individuals when they present to mental health services.
Rates of trauma reported by this cohort seem surprisingly low and reasons for this are unclear. As data relied on retrospective examination of case notes it may be that incidents of previous trauma were not documented in full for all of the people in this sample. It may also be that memories of past traumatic events are subject to recall bias.
Limitations of this study include small sample size and clinical population, reducing the generalisation to the wider population and low statistical power. It is also possible that there may have been overcorrection by using a correction approach in some cases, suggesting a possible type two error because of the size of that sample. The cohort in this study were presenting for diagnostic assessment for autism as adults and had waited a long time to be seen, and this may have had implications for how they presented. Having to live as someone with unrecognised autism may also have contributed to poor mental health for some of these people. Reference Gellini and Marczak22,Reference Bitsika and Sharpley23 The study did not collect data on sex differences with trauma, although a recent study suggests that there may not be sex differences in the prevalence of traumatic stress in young people. Reference Tamilson, Eccles and Shaw24
Future research directions
Further research on sex differences in the presentation of individuals with co-occurring mental health conditions and autism are indicated, as this is an under-researched area and may have implications for service delivery. A recent study of autistic adults who had previously been diagnosed with borderline or emotionally unstable personality disorder included mostly female participants who felt that their previous mental health diagnosis had been erroneous and introduced diagnostic overshadowing. Reference Hollocks, Lerh, Magiati, Meiser-Stedman and Brugha25 This and the preponderance of females in this situation warrants further consideration.
In conclusion, mental health diagnoses are high among autistic people, in our sample. In this study, the results suggest there are no differences between the frequency and type of mental health condition in autistic individuals between males and females. Pre- and postnatal traumatic exposures are common among autistic people, resulting in a compound effect of neurological and external vulnerability toward developing mental health conditions.
About the authors
Charlotte Cliffe is a higher specialist trainee in Psychiatry with the Adult Neurodevelopmental Team, Surrey and Borders Partnership NHS Foundation Trust, Epsom, UK, and was a higher specialist trainee at Farnham Road Hospital, Surrey and Borders Partnership NHS Foundation Trust, Guildford, UK. Henrietta Rees is a higher specialist trainee in Psychiatry with the Adult Neurodevelopmental Team, Surrey and Borders Partnership NHS Foundation Trust, Epsom, UK, and was a higher specialist trainee at Farnham Road Hospital, Surrey and Borders Partnership NHS Foundation Trust, Guildford, UK. Howard Childs is a neurodevelopmental practitioner with the Adult Neurodevelopmental Team, Surrey and Borders Partnership NHS Foundation Trust, Epsom, UK. Rebecca Day is an assistant psychologist with the Adult Neurodevelopmental Team, Surrey and Borders Partnership NHS Foundation Trust, Epsom, UK. Elizabeth Shade is an assistant psychologist with the Adult Neurodevelopmental Team, Surrey and Borders Partnership NHS Foundation Trust, Epsom, UK. Luke Simmond is an autism specialist worker with the Adult Neurodevelopmental Team, Surrey and Borders Partnership NHS Foundation Trust, Epsom, UK. Jo Jennison is a clinical psychologist with the Adult Neurodevelopmental Team, Surrey and Borders Partnership NHS Foundation Trust, Epsom, UK. Clare Allely is a professor of forensic psychology at the University of Salford, Salford, UK. Raja Anindya Sekhar Mukherjee is a consultant psychiatrist with the Adult Neurodevelopmental Team, Surrey and Borders Partnership NHS Foundation Trust, Epsom, UK, a professor at University of Surrey Medical School, Guildford, UK, and an honorary professor at the University of Salford, Salford, UK.
Data availability
Data are available through the ethical approval process of the SABP NHS Trust Research Department.
Author contributions
C.C. and H.R. analysed the data and wrote the paper. R.A.S.M. supervised and created the project title. H.C. collected the data, contributed to the write-up and the final paper. R.D., E.S., L.S., J.J. and C.S.A. were involved in the project through either data collection or review of the final manuscript.
Funding
This study received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.


 Open access
Open access
eLetters
No eLetters have been published for this article.