


Racial disparities in mental healthcare affecting Black and minority ethnic (BME) groups are well documented in the UK Reference Kapadia, Zhang, Salway, Nazroo, Booth and Villarroel-Williams1 and elsewhere. Reference Cook, Trinh, Li, Hou and Progovac2 Black individuals are disproportionately diagnosed with severe mental illness, experience coercive treatment and often encounter services via crisis or the criminal justice system. Reference Hennessy, Hunter and Grealish3,Reference Jeraj, Shoham and Islam-Barratt4 Systemic insensitivity and cultural misalignment exacerbate mistrust and create cycles of fear that hinder help-seeking. Reference Keating, Robertson, McCulloch and Francis5,Reference Lawrence, McCombie, Nikolakopoulos and Morgan6
Early intervention in psychosis services
Early intervention in psychosis (EIP) services are positioned to break these cycles during the critical period of psychosis onset. Reference Birchwood, Todd and Jackson7 Yet, despite valuing certain EIP aspects, BME individuals report mistrust and a lack of understanding as barriers to engagement. Reference Lawrence, McCombie, Nikolakopoulos and Morgan8
Mental health professionals may avoid discussions about race because of fear of being incorrect or causing offence. Reference Atewologun, Chilangwa Farmer, Kline, Nath, Somra and Warmington9,Reference Sue10 Services also fail to integrate cultural and spiritual contexts, perpetuating alienation. Reference Nwokoroku, Neil, Dlamini and Osuchukwu11 Tackling these disparities requires systemic change, cultural competence and collaboration with BME communities. Reference Robertson, Williams, Buck and Breckwoldt12,Reference Bignall, Jeraj, Helsby and Butt13
NHS England and Public Health England recommend involving BME individuals in intervention design and delivery. Although co-produced and culturally adapted interventions exist, Reference Edge, Degnan, Cotterill, Berry, Baker and Drake14,Reference Rathod, Kingdon, Phiri and Gobbi15 few have been evaluated or designed for service-level, anti-racist change. Reference Hassen, Lofters, Michael, Mall, Pinto and Rackal16 Additionally, training initiatives that include reflective practice are key to implementation success. Reference Hassen, Lofters, Michael, Mall, Pinto and Rackal16
SEE ME training
The SEE ME training, co-produced by Black experts by experience and National Health Service (NHS) mental health professionals, consists of a 20-min film featuring narratives from experts by experience, followed by reflective exercises. It aims to address unconscious bias, promote empathy, highlight systemic barriers and set change goals. Grounded in social identity theory, Reference Tajfel, Turner, Austin and Worchel17 it emphasises shared humanity to reduce prejudice and encourage inclusive care.
Current study
This study explores mental health professionals’ experiences of the SEE ME training, its impact and suggestions for future improvements.
Method
Participants
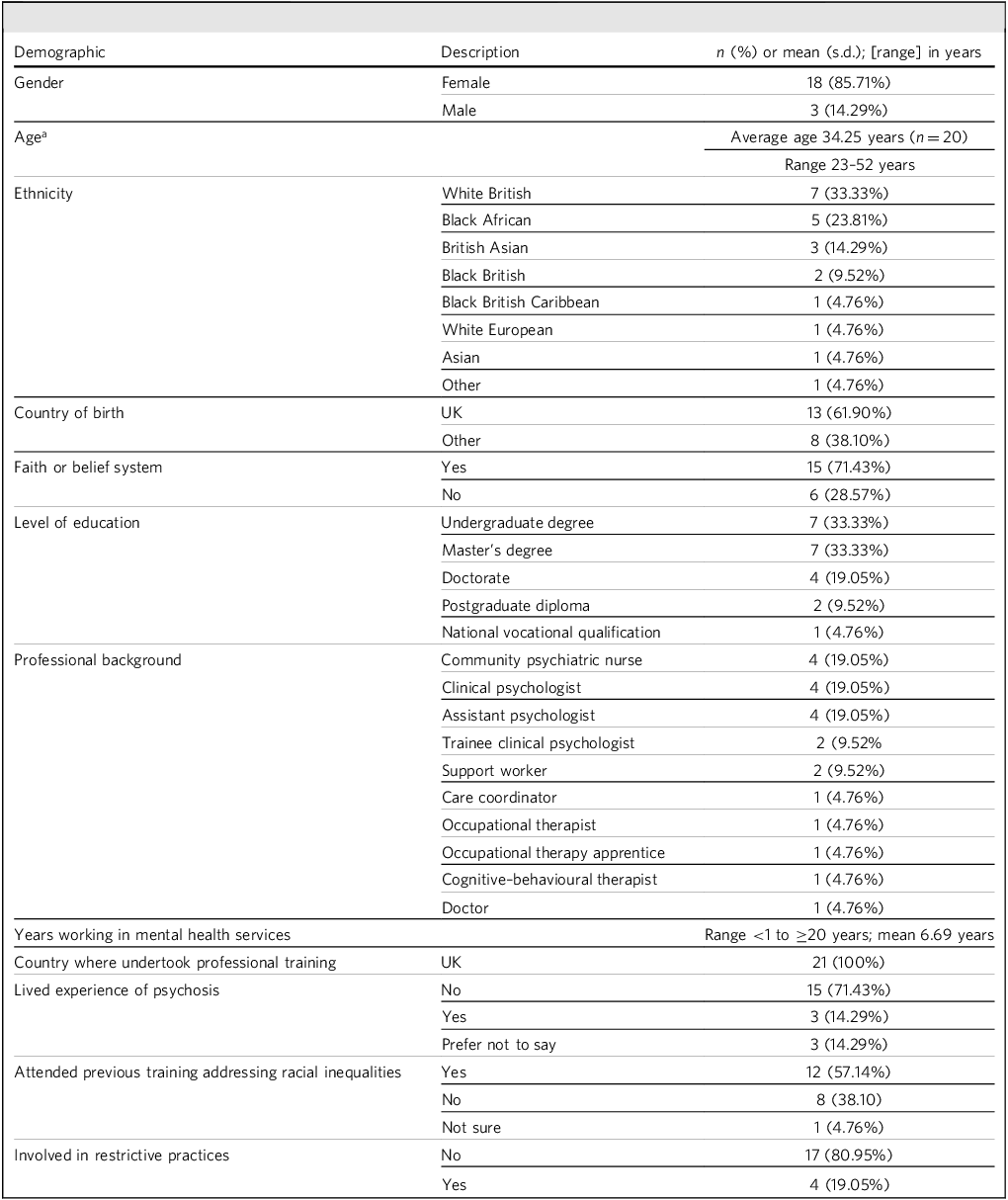
Twenty-one clinicians from North East London NHS Foundation Trust EIP services participated. Inclusion required recent attendance at the SEE ME training and employment in a clinical role. Co-producers of the training were excluded.
A range of demographic information was gathered, detailed in Table 1 below (n = 21). The sample was predominantly female, which is higher than the NHS average of 76%. 18
Participant demographics

a. One participant did not disclose their age.
SEE ME training
The SEE ME training consists of a 20-min film featuring four experts by experience sharing their personal narratives and mental health service experiences, including supportive moments, challenges, and experiences of stigma and misunderstanding. It concludes with a scene in which the experts by experience speak with three mental health professionals, reflecting together on what contributed to good care and what requires improvement. These narratives aim to counter simplistic racial stereotypes and promote understanding among clinicians. Following the film, participants engage in three reflective tasks designed to move from personal reflection to team-based action planning. Task 1 (individual) invites participants to consider what stood out to them in the film and why; for example, by asking ‘What stood out to you?’ and ‘Which aspects of your identity may have shaped your response?’. This encourages awareness of personal assumptions and unconscious biases. Task 2 (small groups of two to three people) focuses on perspective-taking. Participants discuss questions such as ‘Which parts of the clients’ stories did you pay most or least attention to?’ and ‘What might the client have wanted you to hold in mind about them?’. They also identify what additional information would help move work forward and what learning from the film could support this. Task 3 (larger groups of four to six people) shifts toward committed action. Groups identify one key takeaway, generate specific examples of how client stories can be brought into everyday practice and agree on first steps. They also consider how to keep the conversation active within teams.
Drawing from the Hassen et al Reference Hassen, Lofters, Michael, Mall, Pinto and Rackal16 review and relevant literature, the intervention focuses on four key areas: acknowledging unconscious bias, fostering empathy, addressing systemic determinants of health and setting clear goals. It is rooted in social identity theory, which highlights the role of group dynamics in shaping attitudes and behaviours. Reference Tajfel, Turner, Austin and Worchel17 The intervention seeks to reduce prejudice by emphasising shared humanity and individual distinctions, rather than stereotypes. Reference Bigler and Liben19 It also promotes positive intergroup contact between staff and experts by experience, to diminish prejudice and improve understanding. Reference Tajfel, Turner, Austin and Worchel17
Procedure
Recruitment occurred via study presentations and email invitations, as part of a researcher’s postgraduate degree in clinical psychology. Reference Lori20 Interested participants contacted the researcher and provided informed consent. Written consent was obtained via a signed participant consent form before the interview. At the start of each interview, verbal consent was also confirmed after participants had the opportunity to ask questions and the study details were explained again. Given the context of the training across the EIP teams, emphasis was placed on profession and ethnicity representation. Eighty-six individuals attended the training, and 24 individuals expressed interest in being interviewed, with 21 participating after drop-out. This comprises 24.42% of the total sampling pool. Written and verbal consent was obtained from all participants. Interviews were conducted via Microsoft Teams (Microsoft Corporation, Redmond, Washington, USA; https://www.microsoft.com/en-us/microsoft-teams/download-app?msockid=0a0fd3e1568569b028c6c64f57d06876) between April and May 2023, and lasted 33–60 min. Participants were compensated and debriefed in line with the British Psychological Society guidelines. 21
Data collection
Interviews were semi-structured and were developed with input from Black experts by experience and qualitative researchers. The first section explored professionals’ experiences of attending the SEE ME training, using questions such as ‘What was your experience attending the training’ and ‘What was it like for you to watch the video testimonials?’. The second section examined how the training influenced their understanding and practice, with questions such as ‘When watching the ‘SEE ME’ film, what did you take away about the experience of Black service users in NHS mental health services?’ and ‘What impact do you think the training has had on you in your role and practice as a (INSERT ROLE) working in early intervention in psychosis?’. The final section focused on future delivery, asking ‘How, if at all, do you think “SEE ME” training should be used in the future?’ and ‘What do you think could be done to improve the training to reduce racial inequalities and improve practice in the future?’.
Ethical approval
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human participants were approved by University College London Research Ethics Committee (identifier: 24629/001).
Analysis
Thematic analysis followed Braun and Clarke’s six-step process. Reference Braun and Clarke22 A critical realist stance informed the interpretation of subjective experiences.
Researcher reflexivity
The lead author, a biracial trainee psychologist, co-produced the training, but was not involved in delivery. Reflexivity was maintained through supervision, journaling and credibility checks.
Credibility
Bias was managed via bracketing interviews, dual coding and member checks with participants. Dual coding involved the research supervisor reviewing the coding of two transcripts and the initial theme structure proposed by the researcher, allowing any discrepancies in the analysis to be identified and refined until consensus was reached. Additionally, one interview transcript was independently coded by a co-researcher, who assessed how well the themes reflected the raw data and whether any important information had been overlooked.
Results
Initial analysis yielded 116 codes, which were refined to 68 and organised into 17 subordinate themes grouped under six superordinate themes. These are as follows: Stepping into the Shoes of Experts by Experience, Engaging in Personal Reflections, Considering Systemic and Structural Influences, Changes and Direction for Work, Process of the Training and Delivery of the Training. Illustrative quotes for each theme are presented in Table 2.
Illustrative quotes for the themes

Stepping into the shoes of experts by experience
Participants described how the training facilitated a deep emotional connection with experts by experience, enabling a greater understanding of their lived experiences. Hearing first-hand testimonies evoked strong empathy and emotional resonance. Many expressed admiration for the courage of experts by experience in sharing their stories, which highlighted challenges such as trust issues and stigma within Black communities. The training prompted reflection on stereotypes and fostered an appreciation for the diversity and resilience within Black culture. Overall, this theme captured how the training empowered clinicians to engage more meaningfully with their clients’ perspectives and needs.
Engaging in personal reflections
This theme encompassed participants’ self-reflection, enhanced cultural awareness and a growing sense of responsibility in addressing racial inequality.
Self-evaluation
Participants valued the training for revealing unconscious biases and prompting critical introspection. Although some experienced discomfort, they acknowledged its importance in fostering culturally sensitive care. White participants reflected on limitations in their cultural understanding, whereas participants from BME backgrounds reported increased confidence in addressing culture within clinical practice.
Responsibility
The training highlighted the importance of both individual and collective responsibility in addressing racial disparities. Participants recognised that change requires coordinated effort at team and organisational levels.
Curiosity
Participants described a renewed curiosity about their clients’ identities and lives beyond the therapy room. This was accompanied by a desire to develop more authentic therapeutic relationships through understanding clients’ interests, backgrounds and experiences.
Together, these subthemes reflected a shift toward greater self-awareness, accountability and commitment to culturally attuned care.
Considering systemic and structural influences
This theme reflected participants’ growing awareness of broader structural and institutional contributors to racial inequality in mental healthcare.
Structural/systemic factors
Participants acknowledged that service frameworks, workforce homogeneity and societal stereotypes perpetuate disparities in care. They emphasised the need for systemic reform and regular anti-racism training to meaningfully address these embedded issues.
Power and privilege
The training encouraged participants to reflect on power dynamics in clinical relationships and the inherent privileges held by healthcare professionals. Many expressed a desire to use their influence to advocate for improved representation and more equitable systems of care.
This theme underscored participants’ recognition of not just the need for individual change, but also advocating for broader systemic transformation.
Changes and direction for work
Participants identified concrete changes they intended to make in both client-facing and team-facing domains, while also anticipating potential barriers.
Client-focused practice
Participants reported a renewed commitment to person-centred care. Key priorities included improving trust, transparency and shared decision-making, alongside greater cultural responsiveness in communication and engagement.
Staff-focused practice
Participants aimed to initiate more open conversations about race within their teams, adapt language use and embed cultural reflection into routine practice (i.e. through supervision, training and discussions in team meetings, etc.) Many highlighted the importance of continued learning and practical application of the training content.
Anticipated challenges
Participants acknowledged various barriers to implementation, including limited time, competing demands and staff burnout. Some also anticipated discomfort in addressing discriminatory behaviours among colleagues. Organisational support, sustained resources and follow-up learning opportunities were identified as essential to facilitate meaningful and lasting change.
Process of the training
This theme described participants’ experiences of the emotional, relational and psychological processes during the training.
Emotive responses
Participants reported a range of intense emotions, including anger, guilt, anxiety, shame and hope. Although emotionally challenging, many described this discomfort as necessary for personal and professional growth.
Shared humanity
Although related to the empathy described in the theme ‘Stepping into the shoes of experts by experience’, this subtheme reflects a broader interpersonal process that extends beyond understanding specific experiences of experts by experience. The first theme focused on perspective-taking, whereas shared humanity captures a more universal sense of connection in which participants recognised similarities in emotions, values and vulnerabilities. This included seeing experts by experience as individuals rather than representatives of a group, alongside noticing a parallel sense of closeness within their teams. The emotionally evocative film and reflective tasks encouraged openness about biases and uncertainties, allowing participants to share vulnerability and develop mutual respect. In this way, the subtheme highlights a shift from simply empathising with experts by experience to identifying with them – and with colleagues – through shared human qualities.
Engagement
Most participants found the training positive, engaging and thought-provoking, with familiar content helping draw in even quieter staff. Emotional connection varied, often influenced by personal identity. Black staff, in particular, felt both pride and added responsibility to ensure respectful engagement, highlighting the risk of placing the burden of addressing inequalities on those most affected.
Resistance
Some participants described resistance to the training, often shown through defensiveness, minimising the service’s role in racial inequalities, or difficulty acknowledging areas for improvement. Some avoided engaging with race by shifting discussion to unrelated topics or struggled to reflect on how their identities shaped practice. Others expressed scepticism about the training’s value or the likelihood of meaningful change. Resistance also appeared in reframing inequalities as issues affecting all patients. These responses sometimes limited reflection and were understood as stemming from discomfort, anxiety or limited understanding of racism.
Psychological safety
Many participants felt the need to self-censor, with group dynamics – shaped by role, seniority and ethnicity – strongly affecting comfort levels. Junior BME staff worried about potential risks, whereas senior White staff were cautious about their influence. Being the only BME staff member in a group was especially uncomfortable. Although diversity sometimes challenged group comfort, it also offered valuable learning opportunities, underscoring the importance of thoughtful group arrangements in sensitive training.
Delivery of the training
This theme captured participant reflections on the format, positioning and potential enhancements for the training.
Positioning of the training
The training was widely regarded as relevant and valuable across roles. The tailored approach, protected time and leadership support were appreciated. Clear communication of its purpose helped to foster engagement. Many participants advocated for the training to be mandatory and recommended wider implementation across services, including leadership teams and in-patient settings.
Centring the patient voice and reflection
Participants valued the experiential nature of the training and the focus on the patient voice. This approach enriched learning and stimulated meaningful discussion. Some participants, however, felt that staff reflections in the film were less impactful, and occasionally perceived them as inauthentic or performative.
Practical considerations
Several suggestions for improvement were offered. These included extending the duration of the training to allow for deeper discussion, adding subtitles to the film to enhance accessibility and scheduling follow-up sessions for continued reflection and support. Ongoing supervision was also recommended to facilitate implementation and maintain momentum.
Discussion
This study explored mental health professionals’ experiences of the SEE ME training – an intervention developed for EIP services to address racial inequalities in care for Black individuals with psychosis. Thematic analysis of interviews with 21 participants identified six superordinate themes: Stepping into the Shoes of Experts by Experience, Engaging in Personal Reflection, Considering Systemic and Structural Influences, Changes and Direction for Work, Process of the Training and Delivery of the Training. These findings highlight the training’s impact on promoting empathy, self-awareness, awareness of structural inequality and motivation for positive change in clinical practice.
The journey of the training
The emotional and psychological trajectory of the SEE ME training reflected a range of responses among participants, particularly in relation to discussing race and systemic discrimination – topics often marked by apprehension. Reference Atewologun, Chilangwa Farmer, Kline, Nath, Somra and Warmington9 Some participants, especially those newer to the workforce, expressed anxiety before attending. In contrast, older staff appeared more at ease, possibly because of stronger workplace integration and experience navigating sensitive conversations. Reference Reina and Reina23
During the training, emotional responses diverged by ethnicity. BME staff described feelings of validation and hope, perceiving the training as a tangible commitment to equity. However, Black staff also reported an emotional burden – anticipating how their non-Black colleagues might react. White participants often experienced guilt or shame when reflecting on discrimination, responses commonly associated with anti-racism work. Reference Milazzo24 Although these emotions can lead to disengagement, most participants remained actively engaged.
Although many participants described the training environment as facilitating psychological safety, it is important to recognise that this coexisted with moments of apprehension, hesitancy and a sense of restriction in what could be said. Some discomfort and anxiety were expected and often viewed as part of meaningful reflection, with participants valuing the opportunity to work with challenging thoughts and emotions. Despite this, most experienced enough psychological safety to tolerate discomfort and engage openly. Protected time, structured reflective activities, locally relevant lived-experience narratives and familiarity with the format supported this process. Overall, effective anti-racism training must balance emotional safety with the productive discomfort needed for genuine self-examination.
Reconnecting with humanity in practice
A key outcome of the training was a renewed sense of shared humanity. Participants described a deeper emotional connection with the experts by experience, enabling them to see beyond diagnostic labels and engage more holistically with patients. The diversity of Black experiences portrayed in the training content sparked curiosity and disrupted monolithic assumptions. This empathetic curiosity – conceptually aligned with Desmond Tutu’s assertion that ‘we can only be human together’ – fostered greater interpersonal understanding and relational depth.
Participants reported enhanced capacity for mentalisation and empathy, particularly in navigating cultural differences and histories of systemic harm. The training also promoted vulnerability among colleagues, improving team cohesion and reflective dialogue, reflecting the shared humanity subtheme in which participants described connecting with one another through shared emotions, openness and recognition of mutual fallibility. These processes reflect principles within social identity and intergroup contact theories, which highlight the potential of shared experiences and personalisation to reduce prejudice and increase inclusive behaviour. Reference Phillips25,Reference Goar26
Collective and organisational responsibility
A notable enabler of engagement was leadership support, particularly the provision of protected time to attend the training. This top-down endorsement signalled that anti-racism work was an organisational priority, aligning with NHS England 27 guidance on reducing healthcare inequalities. However, bottom-up engagement was equally vital: the co-production of the intervention with North East London NHS Foundation Trust clinicians and patients ensured authenticity and contextual relevance. Reference Bennett and Keating28
Participants expressed a desire to take individual and collective action but emphasised the need for sustained structural support. Tackling systemic inequality requires interventions that empower staff to reflect on their own positionality while addressing broader service-level inequities. Reference Hassen, Lofters, Michael, Mall, Pinto and Rackal16 Equipping staff with the tools and confidence to identify and challenge institutional barriers is critical to transforming mental healthcare into a more equitable system.
Clinical recommendations
Future training should prioritise psychological safety, acknowledging the influence of known factors that influence psychological safety; age, Reference Buljac-Samardžić, Dekker-van Doorn and Van Wijngaarden29 ethnicity Reference Derickson, Fishman, Osatuke, Teclaw and Ramsel30 and profession. Reference Nembhard and Edmondson31 Anticipating emotional responses, such as defensiveness or distress, a training should include access to emotional support and structured debriefing.
Co-produced training, developed with input from patients, carers and clinicians, can enhance authenticity and engagement. Programmes should centre the client and carer voice, encouraging clinicians to adopt lived-experience perspectives and to involve clients in collaborative goal-setting.
To support practical application, training should include time for individual or team action planning. Concrete examples and simulated scenarios may assist clinicians in addressing racial inequalities more effectively. Incorporating principles from intergroup contact theory may also support positive engagement and reduce stereotyping.
The exclusion of carer perspectives was identified as a limitation, suggesting the value of their inclusion in future iterations. Finally, one-off training is insufficient for long-term change; sustained organisational support, including supervision and regular reflection, is essential. Ongoing evaluation of staff engagement with anti-racist practice should inform continuous improvement.
Future research
Longitudinal research is needed to explore the sustained impact of anti-racism training. Follow-up interviews at 6 and 12 months could assess behavioural changes and identify barriers to implementation. Quantitative evaluation of key mechanisms – such as empathy, reflexivity and intergroup attitudes – could provide further insight.
Importantly, future research should engage those who decline participation in anti-racism initiatives, to understand resistance, discomfort or disengagement. Understanding these barriers is crucial for inclusive training design and delivery.
Further investigation is also needed to evaluate the training’s impact in other settings (e.g. in-patient, community, child and adolescent mental health services), and its influence on specific outcome disparities, such as access to psychological therapy or use of restrictive interventions.
Limitations
The sample was predominantly female, raising questions about gender representativeness and engagement among male staff. Moreover, participants self-selected into the study, likely introducing positive bias. The perspectives of those who did not engage – either with the training or the research – remain unknown. Additionally, although the interviewer was not involved in delivering the training, their involvement in co-production may have influenced participants’ responses. Social desirability bias cannot be ruled out, given the sensitive nature of the training content. These limitations highlight the importance of involving independent researchers in future evaluation work.
In conclusion, this study provides unique insights into mental health professionals’ experiences of the SEE ME training – an initiative designed to address racial inequalities for Black patients in NHS EIP services. The training fostered reflection, empathy and cultural humility, while encouraging individual and collective responsibility and action. Key strengths included its co-production with experts by experience and the embedding within the local context. Future training should focus on embedding anti-racist principles into the fabric of clinical care, supported by ongoing training, leadership endorsement and structural reform. These findings offer a foundation for the development of meaningful, sustainable interventions to reduce racial disparities in mental health services.
About the authors
Lori Bain is a trainee cinical psychologist at the Research Department of Clinical, Educational and Health Psychology, University College London, UK. Miriam Fornells-Ambrojo, PhD, DClinPsy, is an associate professor and academic director at the Research Department of Clinical, Educational and Health Psychology, University College London, UK; and a consultant clinical psychologist and Professional and Strategic Lead for Psychological Services for First Episode Psychosis, North East London NHS Foundation Trust, London, UK. Mishka Mahdi is a trainee clinical psychologist at the Research Department of Clinical, Educational and Health Psychology, University College London, UK. Alaina Husbands is a trainee clinical psychologist at the Research Department of Clinical, Educational and Health Psychology, University College London, UK. Michaela Eells is a trainee clinical psychologist at the Research Department of Clinical, Educational and Health Psychology, University College London, UK. Chelsea Gardener, DCliPsy, is a lecturer at the Research Department of Clinical, Educational and Health Psychology, University College London, UK.
Data availability
Due to the sensitive nature of the qualitative data and to protect participant confidentiality, the raw data from this study cannot be shared publicly.
Acknowledgements
We gratefully acknowledge the invaluable contributions of the experts by experience from the North East London NHS Foundation Trust, who generously shared their personal narratives and collaborated in the co-creation of the SEE ME training programme. Their insights and lived experiences significantly enriched the development and relevance of this work. All identities have been protected to ensure confidentiality and anonymity. This research was originally conducted as part of a doctoral thesis for the Doctorate in Clinical Psychology programme. Permission has been obtained to reuse and adapt this material for the purposes of the current publication. The original thesis is available as: Bain L. Addressing inequalities in the care of Black people with psychosis: a qualitative approach evaluating the impact of the ‘See Me’ film training on mental health professionals.Reference Lori20
Author contributions
L.B. contributed to study conceptualisation, methodology, validation, formal analysis, investigation and resources (contributed to the development of the SEE ME training programme), and wrote the original draft of the manuscript. M.F.-A. contributed to study conceptualisation, validation, resources (contributed to the development of the SEE ME training programme), supervision, project administration and funding acquisition, and reviewed and edited the manuscript. M.M. contributed to study conceptualisation, validation and resources (contributed to the development of the SEE ME training programme). A.H. and M.E. contributed to study conceptualisation and resources (contributed to the development of the SEE ME training programme). C.G. contributed to study conceptualisation, validation, resources (contributed to the development of the SEE ME training programme), supervision and project administration, and reviewed and edited the manuscript.
Funding
Funding was provided by the North East London NHS Foundation Trust Research and Development Department and University College London through the Doctorate in Clinical Psychology (DClinPsy) programme.
Declaration of interest
None.


 Open access
Open access
eLetters
No eLetters have been published for this article.