


Vitamin D is mainly acquired by exposing the skin to sunlight’s UVB radiation, which converts cutaneous 7-dehydrocholesterol to pre-vitamin D3. To a lesser extent, vitamin D is also acquired from dietary sources (e.g. oily fish)(Reference DeLuca1). During winter at latitudes > 35° (e.g. Europe and North America), the availability of UVB reaches its nadir, resulting in vitamin D deficiency and insufficiency (serum 25-hydroxyvitamin D (25(OH)D) < 30 and 30–49·9 nmol·L–1(2))(Reference Cashman, Dowling and Skrabakova3). The best-understood function of vitamin D is its role in helping to maintain calcium and phosphate homeostasis(Reference DeLuca1,Reference Charoenngam, Shirvani and Holick4) . Vitamin D also promotes bone mineralisation and is necessary for the development and maintenance of skeletal health(2). Vitamin D deficiency and insufficiency are associated with rickets in children and osteomalacia and osteoporosis in adults(2,Reference Lips and van Schoor5) . Most observational and intervention studies examining vitamin D and skeletal health are among postmenopausal women and men aged over 60 years(2). A meta-analysis of randomised controlled trials concluded that combined vitamin D and calcium supplementation reduced the risk of fracture in older men and women (mean age 66 years)(Reference Yao, Bennett and Mafham6). With vitamin D receptors found in most human tissues(Reference Haussler, Whitfield and Kaneko7), evidence indicates that vitamin D also has beneficial effects outside of the skeleton, such as in promoting skeletal muscle repair and remodelling(Reference Owens, Allison and Close8,Reference Girgis and Brennan-Speranza9) and tendon healing(Reference Dougherty, Dilisio and Agrawal10). In young, physically active adults, the role of vitamin D in protecting against bone, muscle and connective tissue injuries remains unclear, with mixed findings from association studies(Reference Farrokhyar, Tabasinejad and Dao11–Reference Dao, Sodhi and Tabasinejad13). Daily supplementation with vitamin D and calcium for 8 weeks reduced the incidence of stress fractures by 20 % in female military recruits(Reference Lappe, Cullen and Haynatzki14). To the best of our knowledge, no randomised, placebo-controlled trials have assessed the effect of vitamin D supplementation alone on injury risk in young adults.
Whether it is synthesised endogenously or from dietary sources, vitamin D is hydroxylated by 25-hydroxylase to form the most abundant vitamin D metabolite, 25(OH)D(Reference DeLuca1). Controversy over whether 25(OH)D is the best biomarker of vitamin D status for skeletal health has arisen because alternative measures of vitamin D (e.g. ratio of vitamin D metabolites) were more strongly associated with bone density and fracture risk in some observational studies(Reference Allison, Farooq and Cherif15–Reference Ginsberg, Hoofnagle and Katz17). The clinical relevance and optimal concentrations of 25(OH)D remain a topic of ongoing debate(Reference Allison, Farooq and Cherif15,Reference Ginsberg, Katz and de Boer16,Reference Lawley, Syrop and Fredericson18,Reference Ginsberg, Hoofnagle and Katz19) . Serum 25(OH)D is mostly inactive and is converted by 1α-hydroxylase to form metabolically active 1,25-dihydroxyvitamin D (1,25(OH)2D), which circulates in picomolar concentrations. Serum 25(OH)D is also hydroxylated by 24-hydroxylase to form 24,25-dihydroxyvitamin D (24,25(OH)2D). Serum 24,25(OH)2D circulates in nanomolar concentrations and, despite being traditionally considered a waste product, may have roles in bone development, fracture healing and protection against cartilage damage(Reference St-Arnaud and Glorieux20–Reference St-Arnaud and Naja25). We have shown that greater conversion of 25(OH)D to 24,25(OH)2D relative to 1,25(OH)2D (i.e. low 1,25(OH)2D:24,25(OH)2D) and higher 24,25(OH)2D were associated with a lower incidence of overuse musculoskeletal and bone stress injury in young men and women undergoing arduous physical training(Reference Carswell, O’Leary and Swinton26).
The effect of vitamin D supplementation on the risk of musculoskeletal injury and vitamin D metabolites in young adults remains unclear. We used a randomised, placebo-controlled trial beginning in winter to examine the effect of 12 weeks of vitamin D supplementation on the risk of lower body (pelvic girdle, sacrum, coccyx and lower limb) overuse musculoskeletal injury in young healthy men commencing initial military training. Vitamin D supplementation was implemented during the first 12 weeks of training when the greatest training-induced musculoskeletal adaptations were expected to occur(Reference O’Leary, Izard and Walsh27). Injuries were recorded during training and subsequent 3 years of military service to examine if there were short- or long-term benefits of vitamin D restoration during training. Injuries sustained after the 12-week intervention were analysed as part of an exploratory observational follow-up. We hypothesised that vitamin D supplementation, by either simulated sunlight in accordance with recommendations on safe, casual sunlight exposure(28) or oral vitamin D3, would reduce the risk of overuse musculoskeletal injury.
Experimental methods
British Army recruits volunteered to participate in this double-blind (participant, investigator), randomised, placebo-controlled trial and provided written informed consent. All participants were free from injury at the beginning of the study, having passed a physician-screened medical assessment during the first week of training. Initial military training followed a syllabus of basic military skills including physical training, weapon handling, map reading and fieldcraft. Recruits followed a progressive, structured physical training programme, consisting of endurance and circuit training, agility-based gymnasium work, assault course practice and marching whilst carrying a load. The physical demands of initial military training(Reference Wilkinson, Rayson and Bilzon29,Reference O’Leary, Saunders and McGuire30) and military service(Reference Nindl, Castellani and Warr31) have been reported previously, along with the incidence of lower body overuse injury during training(Reference Carswell, O’Leary and Swinton26,Reference Sharma, Greeves and Byers32) and military service(Reference Nindl, Castellani and Warr31,Reference Lovalekar, Hauret and Roy33) . Recruits ate at the same time in the same cookhouse whilst undertaking military training. The UK Ministry of Defence Research Ethics Committee approved the study (692/MODREC/15), and all procedures were conducted in accordance with the Declaration of Helsinki.
Participants
Participants were recruited at the beginning of their first week of initial military training at the Infantry Training Centre, Catterick, UK (latitude 54°N). Two hundred and fifty men met the study inclusion criteria and volunteered to participate (Figure 1). Infantry recruits were eligible to participate if they had Fitzpatrick sun-reactive skin types I–IV(Reference Fitzpatrick34), were not currently consuming supplements containing vitamin D and had not used a sun bed or travelled to a sunny climate in the preceding 3 months. Participants commenced their study participation in January or February of 2016 or 2017, when ambient UVB was negligible at UK latitudes.
Participant flow through the study. SSR, solar simulated UV radiation.

Experimental procedures
Participants were randomly allocated to one of four 12-week intervention groups: (1) solar simulated UV radiation (SSR); (2) placebo SSR; (3) oral vitamin D3; or (4) oral placebo (Figure 2). Participants were block randomised within their training platoons (using randomizer.org) to prevent any between-platoon differences in training conditions influencing the study outcomes. With the objective to restore and then maintain vitamin D sufficiency (serum 25(OH)D ≥ 50 nmol·L–1(2)), participants in the SSR and oral vitamin D3 groups underwent a 4-week restoration phase, necessary because 25(OH)D was at its winter nadir, followed by an 8-week maintenance phase. Compliance with the intervention was calculated by investigators counting any unconsumed oral capsules each week and using investigator records of SSR/placebo SSR exposures. On completion of the 12-week intervention, participants completed a questionnaire which asked them to guess which intervention (i.e. active or control) they thought they had received.
Schematic of study design, to investigate the effect of 12 weeks of vitamin D supplementation (solar simulated UV radiation (SSR) or oral vitamin D3) or placebo (placebo SSR or oral placebo) on the risk of lower body overuse musculoskeletal injury during 26 weeks of initial military training and subsequent 3 years of military service. Vitamin D supplementation during a 4-week restoration phase followed by an 8-week maintenance phase.

Participants’ medical records were accessed to obtain a record of clinician-diagnosed lower body overuse musculoskeletal injuries during their 6 months of military training and subsequent 3 years of military service. A venous blood sample was obtained during week 1 of initial military training (baseline) and at weeks 5 and 12 for the measurement of vitamin D metabolites (serum 25(OH)D, 1, 25(OH)2D and 24, 25(OH)2D), parathyroid hormone (PTH) and bone metabolism biomarkers carboxyl-terminal collagen crosslinks (CTX) and procollagen type I N-terminal propeptide (PINP). Baseline measurements of physical fitness, body mass and height were made. Physical fitness was assessed by a maximal effort 2·4 km run. Body mass and height (Seca) were measured in light clothing and without shoes. At baseline, participants self-reported their ethnicity, smoking and alcohol habits and bone injury history, using questionnaires. The sun-reactive skin type was determined through questionnaire assessment of sun-reactive history and phenotypic characteristics(Reference Fitzpatrick34).
Simulated sunlight
SSR was provided in accordance with guidelines on safe sunlight exposure for vitamin D synthesis(28), as described previously to achieve vitamin D sufficiency in most white-skinned individuals(Reference Rhodes, Webb and Fraser35). Participants assigned to the SSR intervention were exposed to 1·3 × standard erythemal dose using a whole body irradiation cabinet (Hapro Jade) fitted with Arimed B fluorescent tubes (Cosmedico), three times a week during the 4-week restoration phase and once a week during the subsequent 8-week maintenance phase, as described previously(Reference Carswell, Oliver and Wentz36). Approximately 40 % of the skin surface area was exposed by participants wearing a T-shirt and shorts. The exposures during each week of the restoration phase were equivalent to ∼15 min, unshaded midday summer sun exposure six times a week for a casually dressed individual in northern England (latitude 53·5°N)(Reference Rhodes, Webb and Fraser35). By accounting for pre-vitamin D3 irradiance at different latitudes(Reference Webb, Kift and Berry37), the equivalent exposure time would be ∼12 min in Philadelphia, Pennsylvania (40°N), and ∼18 min in Oslo, Norway (60°N). The once-a-week frequency of exposures during the maintenance phase was chosen based on pilot investigations that showed it maintained serum 25(OH)D ≥ 50 nmol·L–1. Identical-looking irradiation cabinets were used to expose placebo SSR participants to placebo SSR, with the transmission of 99·9 % of UV radiation prevented by covering the fluorescent tubes with a transparent UV radiation blocking film(Reference Carswell, Oliver and Wentz36). A constant SSR dose was maintained during the study, as described previously(Reference Carswell, Oliver and Wentz36). The duration of SSR and placebo SSR exposures (mean 222 (sd 23) s) was controlled by investigators and was the same for both groups.
Oral vitamin D3
An oral vitamin D3 capsule was consumed once a day for 12 weeks by participants allocated to the oral vitamin D3 intervention (Pure Encapsulations). A 1000 IU · d–1 dose was consumed during the 4-week restoration phase, and a 400 IU · d–1 dose was consumed during the subsequent 8-week maintenance phase, as described previously(Reference Carswell, Oliver and Wentz36). The restoration phase dose was chosen based on published predictive modelling for achieving vitamin D sufficiency(Reference Cashman, Hill and Lucey38), and pilot investigations showed it achieved similar serum 25(OH)D concentrations to SSR. The maintenance phase dose was chosen based on daily recommendations for vitamin D3 intake(2,39) and pilot investigations that showed it maintained serum 25(OH)D ≥ 50 nmol·l–1. An identical-looking cellulose placebo capsule was consumed once a day for 12 weeks by participants allocated to the oral placebo group (Almac Group). Independent analysis found that the 1000 and 400 IU capsules contained 1090 and 460 IU vitamin D3, respectively, and confirmed that the placebo capsules did not contain vitamin D (NSF International Laboratories).
Lower body overuse musculoskeletal injury
Injuries reported by participants to their military medical centre during 6 months of initial military training and subsequent 3 years of military service were diagnosed by clinicians and recorded in their medical records. Defence general practitioners and physiotherapists diagnosed injuries by taking detailed histories, conducting physical examinations and referring participants for imaging and further investigations, where necessary (e.g. MRI, X-ray). For all lower body overuse musculoskeletal injuries, the diagnosis, date of diagnosis and number of lost training or reduced duty days were retrieved from medical records by a physician independent of their clinical care and blinded to their allocated intervention group. Overuse musculoskeletal injuries were defined as pain, inflammation or a functional disorder that involved joints, muscles, tendons, ligaments and associated connective tissues, with the mechanism of injury a result of use over time, rather than a traumatic event(Reference Sharma, Greeves and Byers32) (e.g. plantar fasciitis, Achilles tendinopathy, patellar tendinitis, iliotibial band syndrome). Bone stress injuries were included as a type of overuse musculoskeletal injury. Bone stress injuries encompass the spectrum of overuse injuries caused by microdamage accumulation in bone, frequently referred to as stress reactions and stress fractures(Reference Hoenig, Ackerman and Beck40) (e.g. medial tibial stress syndrome, femoral, tibial, calcaneal and metatarsal stress fractures). Injuries sustained during the first 4 weeks of initial military training (vitamin D restoration phase) were excluded from analyses to control for latency.
During training, the number of lost training days due to each lower body overuse musculoskeletal injury was counted until a participant either returned to full training in their original platoon or was transferred to another platoon to complete missed training, physical rehabilitation or for discharge from the Army. The outcome of training was categorised as either a first-time pass, a pass following physical rehabilitation, medical discharge due to musculoskeletal injury, medical discharge not due to musculoskeletal injury or discharge for non-medical reasons. After training, the number of reduced duty days whilst serving in the military due to each lower body overuse musculoskeletal injury was counted. Three and a half years after commencing the study, participants were categorised as being either current serving infantry personnel, current serving non-infantry personnel, medically discharged from the Army due to musculoskeletal injury, medically discharged not due to musculoskeletal injury or discharged for non-medical reasons. Lost training days due to injuries sustained during the first 4 weeks of initial military training (vitamin D restoration phase) were excluded from analyses to control for latency.
Blood collection and handling
Whole blood samples were obtained by venipuncture from a prominent vein in the antecubital fossa into serum and EDTA vacutainers (Becton Dickinson). Whole blood in serum vacutainers was left to clot in a vacutainer rack for 1 h at room temperature. Blood samples were centrifuged at 1500 g for 10 min at 4°C, with serum and plasma aliquots immediately frozen at –80°C for later analysis.
Biochemical analysis
Total serum 25(OH)D (25(OH)D2 and 25(OH)D3) and total 24,25(OH)2D (24,25(OH)2D2 and 24,25(OH)2D3) were measured with HPLC–MS/MS using a Micromass Quattro Ultima Pt electrospray ionisation mass spectrometer, as described previously(Reference Tang, Nicholls and Piec41). Serum 1,25(OH)2D was measured by a chemiluminescent immunoassay using a DiaSorin LIAISON® XL analyser (Stillwater). Plasma PTH, CTX and PINP were measured by electrochemiluminescence immunoassays using a Cobas c601 analyser (Roche Diagnostics). The measurement ranges of the assays were 0·1–200 nmol·L–1 for 25(OH)D2 and 25(OH)D3, 0·8–25·0 nmol·L–1 for 24,25(OH)2D2, 0·1–25·0 nmol·L–1 for 24,25(OH)2D3, 12–480 pmol·L–1 for 1,25(OH)2D, 0·1–530·0 pmol·L–1 for PTH, 0·20–1·50 µg·L–1 for CTX and 20·0–600·0 µg·L–1 for PINP. Results above the assay upper limit were repeated on dilution to produce a value within the working range of the assay. Values below the lower limit of quantification were not included in the calculation of total 25(OH)D or total 24,25(OH)2D. The mean CV for intra-assay imprecision across the measuring range of the assays was 4·9 % for 25(OH)D2, 8·3 % for 25(OH)D3, 7·7 % for 24,25(OH)2D2, 9·0 % for 24,25(OH)2D3, 7·4 % for 1,25(OH)2D, 2·6 % for PTH, 2·1 % for CTX and 3·3 % for PINP. The cumulative inter-assay CV were ≤ 7·4 % for 25(OH)D2, ≤ 9·6 % for 25(OH)D3, ≤ 10·6 % for 24,25(OH)2D2, ≤ 8·9 % for 24,25(OH)2D3, ≤ 9·3 % for 1,25(OH)2D, < 3·8 % for PTH, < 3 % for CTX and < 3 % for PINP. Our 25(OH)D and 24,25(OH)2D assays showed < 6 % accuracy bias against the Centers for Disease Control and Prevention’s reference method on the Vitamin D External Quality Assessment Scheme and < 9 % bias against the method-specific mean for 1,25(OH)2D. Certification performance standards set by the Vitamin D External Quality Assessment Scheme were met when the analyses were performed. All biochemical analyses were undertaken by the Good Clinical Laboratory Practice and Vitamin D External Quality Assessment Scheme certified Bioanalytical Facility at the University of East Anglia, Norwich, UK.
Statistical analysis
These data were secondary outcomes and analyses of a randomised placebo-controlled trial investigating the effects of vitamin D supplementation on exercise performance, respiratory infection and immune function for which an a priori minimum sample size was calculated(Reference Carswell, Oliver and Wentz36,Reference Harrison, Oliver and Kashi42,Reference Kashi, Oliver and Wentz43) . We have previously shown that both the SSR and oral vitamin D3 interventions increased serum 25(OH)D and 1,25(OH)2D to a similar extent(Reference Carswell, Oliver and Wentz36). Therefore, in this study, participants supplemented with vitamin D (SSR and oral vitamin D3) were collapsed into one vitamin D group, and those in the placebo groups (placebo SSR and oral placebo) were collapsed into one placebo group, resulting in one intervention group and one control group.
For the primary analysis of injury data, frailty models were employed, a class of survival models designed for recurrent-event data that account for unobserved heterogeneity among individuals. These models extend the Cox proportional hazard model by incorporating a gamma-distributed frailty term, representing individual-specific susceptibility to injury. Platoon was incorporated directly within the model as a stratification factor to account for the block-randomised platoon structure and shared training environment. An approximate detectable hazard ratio (HR) was derived from the achieved precision of each recurrent-event estimate. The standard error of the log HR was obtained from the model-derived 95 % CI and used under a conventional Wald approximation (two-sided α = 0·05; 80 % detection criterion) to estimate the magnitude of the between-group HR that the study was likely capable of distinguishing from the null.
Between-group differences in vitamin D metabolites and bone metabolism compounds over time were analysed using linear mixed-effects models, with adjustment for baseline values and inclusion of a random intercept for platoon to account for clustering arising from the block-randomised design. Model diagnostics were undertaken for all fitted models. For the frailty models, proportional hazards assumptions were assessed using scaled Schoenfeld residuals and inspection of log-minus-log survival plots. For the linear mixed-effects models, model assumptions were assessed by visual inspection of residual-v.-fitted plots and quantile–quantile plots of residuals to evaluate homoscedasticity and approximate normality. No substantial departures from model assumptions were identified. χ 2 tests were used to examine associations between categorical variables. Group differences in central tendency for skewed data, such as lost training days, were assessed using the Mann–Whitney U test. Analyses were intention-to-treat. Subsequent per-protocol analyses were performed to exclude participants with compliance to the intervention < 80 %. All analyses were conducted in R (version 4.4.3, R Core Team) with survival analyses conducted using the survival package(Reference Therneau, Lumley and Atkinson44). Statistical significance was accepted at P < 0·05.
Results
Baseline participant characteristics are shown in Table 1. Participants were sufficiently blinded to the intervention since 36 % correctly guessed their group, 30 % were incorrect and 34 % said they did not know whether they had received an active or placebo intervention.
Demographic, anthropometric, physical fitness, lifestyle behaviour and bone injury history at baseline, with participants randomised to vitamin D (solar simulated UV radiation (SSR) and oral vitamin D3) or placebo (placebo SSR and oral placebo)

Data are mean (sd) or percent.
Vitamin D status
At baseline, only 29 % of participants were vitamin D sufficient (serum 25(OH)D ≥ 50 nmol·L–1), 37 % were vitamin D insufficient (25(OH)D 30–49·9 nmol·L–1) and 34 % were vitamin D deficient (25(OH)D < 30 nmol·L–1). Both SSR and oral vitamin D3 supplementation were successful in achieving vitamin D sufficiency in 95 % of participants by week 5.
Vitamin D metabolites
Serum 25(OH)D increased from baseline in vitamin D participants (Figure 3(a)) and was higher than placebo at week 5 (36·5 (95 % CI 32·8, 40·2) nmol·L–1; P < 0·001) and week 12 (16·2 (95 % CI 12·3, 20·0) nmol·L–1; P < 0·001). Serum 1,25(OH)2D increased from baseline in vitamin D participants (Figure 3(b)) and was higher than placebo at week 5 (11·0 (95 % CI 5·4, 16·6) pmol·L–1; P < 0·001). There was no clear evidence of a between-group difference in 1,25(OH)2D at week 12 (5·2 (95 % CI –1·1, 11·5) pmol·L–1; P = 0·109), reflecting an increase in 1,25(OH)2D from week 5 to week 12 in placebo participants. Serum 24,25(OH)2D increased from baseline in vitamin D participants (Figure 3(c)) and was higher than placebo at week 5 (2·8 (95 % CI 2·5, 3·1) nmol·L–1; P < 0·001) and week 12 (1·9 (95 % CI 1·6, 2·3) nmol·L–1; P < 0·001). Serum 25(OH)D:24,25(OH)2D decreased from baseline in vitamin D participants (Figure 3(d)) and was lower than placebo at week 5 (–3·9 (95 % CI –5·0, –2·7); P < 0·001) and week 12 (–3·5 (95 % CI –4·3, –2·7); P < 0·001). Serum 1,25(OH)2D:24,25(OH)2D decreased from baseline in vitamin D participants (Figure 3(e)) and was lower than placebo at week 5 (–33·7 (95 % CI –40·0, –27·5); P < 0·001) and week 12 (–13·8 (95 % CI –17·4, –10·3); P < 0·001).
Vitamin D metabolites at baseline, week 5 and week 12 in participants randomised to vitamin D (solar simulated UV radiation (SSR) and oral vitamin D3) or placebo (placebo SSR and oral placebo). (a) 25-hydroxyvitamin D (25(OH)D); (b) 1,25-dihydroxyvitamin D (1,25(OH)2D); (c) 24,25-dihydroxyvitamin D (24,25(OH)2D; (d) 25(OH)D:24,25(OH)2D; (e) 1,25(OH)2D:24,25(OH)2D. *P < 0·05, v. baseline; †P < 0·05, v. week 5; # P < 0·05, v. placebo.

Parathyroid hormone and bone metabolism biomarkers
Plasma PTH decreased from baseline in vitamin D participants (Figure 4(a)) and was lower than placebo at week 5 (–0·5 (95 % CI −0·8, −0·3) pmol·L–1; P < 0·001) and week 12 (–0·6 (95 % CI −0·9, −0·3) pmol·L–1; P < 0·001). Plasma CTX decreased from baseline in vitamin D and placebo participants (Figure 4(b)) with no clear evidence of a between-group difference at week 5 (–0·01 (95 % CI −0·05, 0·02) μg·L–1; P = 0·501) or week 12 (–0·03 (95 % CI −0·06, 0·01) μg·L–1; P = 0·202). Plasma PINP increased from baseline to week 5 in vitamin D and placebo participants (Figure 4(c)) with no clear evidence of a between-group difference at week 5 (1·3 (95 % CI −4·1, 6·6) μg·L–1; P = 0·645) or week 12 (2·3 (95 % CI −4·0, 8·6) μg·L–1; P = 0·473).
Parathyroid hormone and bone metabolism biomarkers at baseline, week 5 and week 12 in participants randomised to vitamin D (solar simulated UV radiation (SSR) and oral vitamin D3) or placebo (placebo SSR and oral placebo). (a) parathyroid hormone (PTH); (b) carboxyl-terminal collagen crosslinks (CTX); (c) procollagen type I N-terminal propeptide (PINP). *P < 0·05, v. baseline; †P < 0·05, v. week 5; #P < 0·05, v. placebo.

Musculoskeletal injury and outcome of training
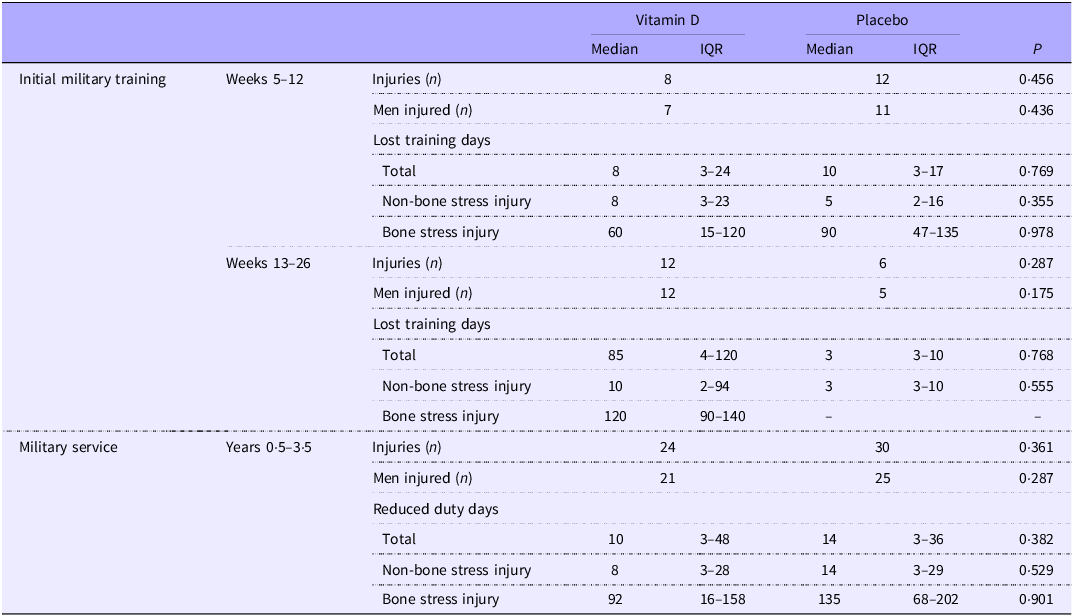
During initial military training and subsequent military service, 100 lower body overuse musculoskeletal injuries (including fourteen lower body bone stress injuries) were diagnosed by clinicians. During the first 4 weeks of military training (4-week restoration phase), eight lower body overuse musculoskeletal injuries (including two lower body bone stress injuries) were diagnosed. With injuries in the first 4 weeks excluded to control for latency, there was no clear evidence of a between-group difference in the incidence of lower body overuse musculoskeletal injury during weeks 5–12 (P = 0·436) or weeks 13–26 (P = 0·175) of initial military training or during subsequent military service (years 0·5–3·5, P = 0·287; Table 2). Frailty models accounting for recurrent injuries indicated no difference in the risk of lower body overuse musculoskeletal injury between vitamin D and placebo participants during initial military training (38 injuries: 20 vitamin D, 18 placebo; HRplacebo:vitamin D = 1·23 (95 % CI 0·57, 2·66), P = 0·597) or when including subsequent military service (92 injuries: 44 vitamin D, 48 placebo; HRplacebo:vitamin D = 0·94 (95 % CI 0·60, 1·46), P = 0·782). Given the number of injuries and the achieved precision of the recurrent-event models, the analysis during initial military training was likely only sensitive to very large between-group differences in hazard (approximate HR ≤ 0·33 or ≥ 3·00), whereas the analysis across the full follow-up period was likely sensitive to moderate-to-large differences (approximate HR ≤ 0·53 or ≥ 1·89). Excluding injuries in the first 4 weeks, there were no differences between vitamin D and placebo participants in the number of lost training days per injury during weeks 5–12 (P = 0·769) or weeks 13–26 (P = 0·768) of initial military training or reduced duty days per injury during subsequent military service (years 0·5–3·5, P = 0·382; Table 2). The outcome of initial military training (P = 0·471) and status three and a half years after commencing the study (P = 0·629) were not different between vitamin D and placebo participants (Table 3).
Lower body overuse musculoskeletal injury incidence during initial military training and subsequent military service, with participants randomised to vitamin D (solar simulated UV radiation (SSR) and oral vitamin D3) or placebo (placebo SSR and oral placebo). Injuries in the first 4 weeks excluded to control for latency

IQR, interquartile range.
Lost training days and reduced duty days are median (IQR) per injury.
Outcome of training and status three and a half years after commencing the study, with participants randomised to vitamin D (solar simulated UV radiation (SSR) and oral vitamin D3) or placebo (placebo SSR and oral placebo)

Data are n (%). P values are from χ 2 tests comparing the overall distribution of participants across the listed categories between the vitamin D and placebo groups; they do not refer to individual rows separately.
Compliance
Results were not substantially changed when participants with compliance to the intervention < 80 % were excluded from analyses (n 16 excluded during the 4-week restoration phase; n 17 excluded during the 8-week maintenance phase). One participant allocated to the vitamin D group and vitamin D insufficient after the 4-week restoration phase had < 80 % compliance with the intervention.
Discussion
Twelve weeks of either safe simulated sunlight or oral vitamin D3 supplementation were both effective in restoring and maintaining vitamin D sufficiency. We speculated that restoring vitamin D sufficiency from its winter nadir, at the beginning of 26 weeks of arduous military training, which increases military recruits’ risk of overuse musculoskeletal injury(Reference Carswell, O’Leary and Swinton26), would maximise the potential for vitamin D to reduce injury risk. Contrary to our hypothesis, we found no clear evidence for vitamin D supplementation to reduce the risk of lower body overuse musculoskeletal injury. However, the number of injuries observed was relatively low, meaning that the findings remain uncertain and smaller effects, whether beneficial or detrimental, cannot be ruled out. To the best of our knowledge, this study is the first randomised, placebo-controlled trial to include an examination of the effect of vitamin D supplementation without calcium on musculoskeletal injury risk in young adults.
Vitamin D metabolites
We achieved and maintained the Institute of Medicine and European Food Safety Authority–defined vitamin D sufficiency(2,45) in 95 % of supplemented participants. Vitamin D supplementation also increased the serum concentration of 1,25(OH)2D and 24,25(OH)2D (metabolites of 25(OH)D), compared with placebo, resulting in a decrease in the two vitamin D metabolite ratios. Serum 1,25(OH)2D concentrations are tightly regulated by PTH, calcium and phosphate(2); therefore, this small but statistically significant increase in 1,25(OH)2D was not expected. The mean 1,25(OH)2D:24,25(OH)2D in vitamin D–supplemented participants was less than 32, which was previously associated with a lower incidence of overuse musculoskeletal injury(Reference Carswell, O’Leary and Swinton26). However, the mean 24,25(OH)2D in vitamin D–supplemented participants was less than the 7·7 nmol·L–1 threshold previously associated with being protective against overuse musculoskeletal injury(Reference Carswell, O’Leary and Swinton26), and a greater increase in 24,25(OH)2D may be necessary for injury risk to be reduced. The mean 25(OH)D in the vitamin D–supplemented participants was more than 75 nmol·L–1, which was recommended by the Endocrine Society as a target 25(OH)D, although more recent guidelines do not endorse this threshold because of the lack of clinical trial evidence(Reference Demay, Pittas and Bikle46). Whether a reduction in risk of overuse musculoskeletal injury would have occurred if all supplemented participants achieved 25(OH)D > 75 nmol·L–1 is not known.
Parathyroid hormone and bone metabolism biomarkers
We found that plasma PTH was lower in vitamin D–supplemented participants at weeks 5 and 12, compared with placebo. This finding is consistent with a previous study, where PTH was lower in military trainees supplemented with vitamin D and calcium for 9 weeks, compared with placebo(Reference Gaffney-Stomberg, Lutz and Rood47). Gaffney-Stomberg and colleagues also reported that the ratio of osteoprotegerin to receptor activator of nuclear factor B ligand increased with vitamin D and calcium supplementation, indicating decreased bone resorption; however, neither we nor Gaffney-Stomberg et al. observed a between-group difference in CTX or PINP, markers of bone metabolism(Reference Gaffney-Stomberg, Lutz and Rood47). An increase in osteoclast activity typically occurs in response to high-impact physical activity(Reference Smith, Tacey and Mesinovic48); however, we observed a decrease in CTX, a marker of bone resorption released during type I collagen breakdown, in both groups. We observed an increase in PINP, a marker of bone formation released during type I collagen synthesis, in both groups, which, given the decrease in CTX, most likely reflects adaptive bone formation. Combined vitamin D and calcium supplementation has been shown to prevent increases in CTX during military training(Reference Gaffney-Stomberg, Hughes and Guerriere49). Increases, decreases and no changes in bone metabolism biomarkers have been reported during military training(Reference Greeves, Beck and Nindl50). These divergent findings are potentially due to variability in baseline bone density and the intensity of training. No relationship between markers of bone metabolism and bone stress injury risk has been observed in observational studies of military training, suggesting that these biomarkers are of limited use for monitoring injury risk or adaptive bone formation(Reference Greeves, Beck and Nindl50).
Overuse musculoskeletal injury
In agreement with the null effect on injury risk which we observed, vitamin D supplementation (2000 IU · d–1) did not affect musculoskeletal outcomes, including fracture risk and bone mineral density, in two large cohorts of generally healthy older men and women (n 28 028)(Reference LeBoff and Bischoff-Ferrari51). In contrast to our study, the participants in those studies were older adults and not vitamin D deficient or insufficient at baseline(Reference LeBoff and Bischoff-Ferrari51). We supplemented participants whilst they were undertaking initial military training, meaning they were exposed to a novel musculoskeletal stimulus at the same time as receiving vitamin D. Using observational study designs, serum 25(OH)D was not associated with bone health or musculoskeletal injury in several studies of athletic and military cohorts(Reference Allison, Farooq and Cherif15,Reference Allison, Farooq and Hamilton52–Reference Halliday, Peterson and Thomas55) . In contrast, athletes and military personnel who sustained a musculoskeletal injury(Reference Rebolledo, Bernard and Werner56,Reference Maroon, Mathyssek and Bost57) , including bone stress injury(Reference Dao, Sodhi and Tabasinejad13,Reference Davey, Lanham-New and Shaw58) , had lower serum 25(OH)D concentrations than their uninjured peers. Serum 25(OH)D and 1,25(OH)2D were not related to overuse musculoskeletal injury in military recruits when examined in isolation from 24,25(OH)2D(Reference Carswell, O’Leary and Swinton26). Whether supplementation with 24,25(OH)2D can decrease 1,25(OH)2D:24,25(OH)2D to ≤ 32, increase 24,25(OH)2D to ≥ 7·7 nmol·L–1 and reduce the risk of overuse musculoskeletal injury(Reference Carswell, O’Leary and Swinton26) remains to be determined. Supplementation with 24,25(OH)2D has been shown to promote fracture healing in mice(Reference Martineau, Naja and Husseini59), and 24,25(OH)2D improves skeletal mineralisation in individuals with X-linked hypophosphataemia(Reference Carpenter, Keller and Schwartz60) and renal insufficiency(Reference Birkenhager-Frenkel, Pols and Zeelenberg61), demonstrating a role of this metabolite in promoting skeletal health and thereby potentially reducing injury risk.
Lappe et al. reported that 8 weeks of vitamin D and calcium supplementation reduced the incidence of bone stress injury by 20 % in young women during military training(Reference Lappe, Cullen and Haynatzki14). The need for calcium supplementation in addition to vitamin D to reduce injury risk remains to be determined but is likely necessary if dietary calcium intake is insufficient. Prolonged exercise can cause a decrease in serum calcium and an increase in PTH and bone resorption(Reference Wherry, Swanson and Kohrt62). Calcium supplementation before exercise maintains circulating ionised calcium, suppresses PTH, decreases bone resorption and may improve bone calcium balance(Reference Coombs, Greeves and Young63); therefore, calcium intake before exercise is an important consideration for athletes and military personnel. Combined vitamin D and calcium has been demonstrated to prevent bone loss in postmenopausal women and men aged over 60 years, whereas vitamin D alone did not affect bone mineral density(Reference Cranney, Weiler and O’Donnell64), which supports the idea that vitamin D combined with calcium may be necessary for skeletal health benefits to occur.
Vitamin D supplementation has been demonstrated to enhance the recovery of skeletal muscle following the damaging effects of eccentric exercise (4000 IU · d–1 for 6 weeks)(Reference Owens, Sharples and Polydorou65) and reduce proinflammatory cytokines production following eccentric contractions (2000 IU · d–1 for 3 weeks), which in theory could help to protect against musculoskeletal injuries(Reference Zebrowska, Sadowska-Krepa and Stanula66); however, empirical injury data to support this hypothesis are needed.
Strengths and limitations
Blinding was effective in this randomised placebo-controlled trial because less than half of the participants (36 %) correctly guessed their allocated intervention. Musculoskeletal injuries were diagnosed by clinicians, and lost training or reduced duty days were recorded to quantify the severity and burden of injury. We recognise this study has limitations. Participation was limited to men with sun-reactive skin types I–IV, because women were not allowed to undertake infantry training when the study was recruiting participants, and the SSR protocol(Reference Rhodes, Webb and Fraser35) would not achieve vitamin D sufficiency in individuals with sun-reactive skin types V and VI (brown or black skin)(Reference Farrar, Kift and Felton67). Whether vitamin D supplementation affects the risk of overuse musculoskeletal injury in women and those with darker skin remains to be determined; divergent results could emerge because bone density adaptations during initial military training differ between sexes and ethnicities(Reference Hughes, Taylor and Guerriere68). We reported previously that daily exposure to natural sunlight (ambient UVB) and dietary vitamin D intake were not different between groups during the 12-week intervention(Reference Harrison, Oliver and Kashi42); however, springtime ambient UVB caused serum vitamin D metabolites to increase in placebo participants at week 12. After the 12-week intervention, participants lived freely, that is, able to follow their own supplementation regime and use sun beds, for example. The impact of this freedom on the study outcomes measured after week 12 is not known; thus, the analysis of injuries that occurred after the end of the 12-week intervention should be considered an exploratory observational follow-up. Our study design enabled us to examine short- and long-term effects of vitamin D by implementing supplementation during the initial weeks of training when the greatest musculoskeletal adaptations were anticipated to occur before participants commenced their regular lifestyle as serving military personnel. More broadly, the number of injury events was modest, which means that the estimates were not highly precise and smaller effects of vitamin D, whether beneficial or detrimental, may not have been detected. The relatively small sample size may have prevented us from detecting any small effect of vitamin D on musculoskeletal injury risk. The total number of bone stress injuries was low (n 14); therefore, these data were not analysed separately. We have, however, shown that vitamin D supplementation had no impact on tibial adaptations to military training(Reference O’Leary, Izard and Jackson69), which may be relevant to bone stress injury risk. The relatively small sample size also prevented us from conducting any subgroup analyses based on the concentration of vitamin D metabolites at baseline, for example, only vitamin D–deficient participants or those with serum 1,25(OH)2D:24,25(OH)2D > 32(Reference Carswell, O’Leary and Swinton26).
Conclusion
In a randomised placebo-controlled trial, safe simulated sunlight and oral vitamin D3 supplementation were both effective in achieving and maintaining vitamin D sufficiency in almost all. We found no clear evidence that 12 weeks of vitamin D supplementation affects the risk of lower body overuse musculoskeletal injury during 6 months of military training or subsequent 3 years of military service, although the relatively low number of injury events limited precision and means smaller effects cannot be excluded.
Acknowledgements
The authors thank Dr Daniel Kashi, Xin Hui Aw Yong, Mark Ward, Claire Potter, Dr Anna Ferrusola-Pastrana and Dr Sophie Harrison for their assistance with data collection. LER acknowledges the support of the National Institute for Health and Care Research Manchester Biomedical Research Centre.
The study was funded by the UK Ministry of Defence (Army).
A. T. C.: investigation, methodology, visualisation, writing – original draft, writing – review and editing; P. S.: formal analysis, visualisation, writing – review and editing; T. J. O.: investigation, visualisation, writing – review and editing; S. J.: investigation, methodology, visualisation, writing – review and editing; J. C. Y. T.: investigation, methodology, visualisation, writing – review and editing; S. J. O.: investigation, methodology, supervision, writing – review and editing; L. M. W.: investigation, methodology, writing – review and editing; R. M. I.: methodology, writing – review and editing; N. T.: investigation, writing – review and editing; D. A.:investigation, methodology, writing – review and editing; L. E. R.: methodology, supervision, writing – review and editing; N. P. W.: investigation, methodology, supervision, writing – review and editing; W. D. F.: investigation, methodology, supervision, visualisation, writing – review and editing; J. P. G.: methodology, supervision, visualisation, writing – review and editing.
The authors have no conflicts of interest to declare.
The data that support the findings of the study are not publicly available but are available from the corresponding author pending approval from the UK Ministry of Defence.







 Open access
Open access