


Introduction
Approximately 30 per cent of all older adults (≥65 years) fall every year (Muir et al., Reference Muir, Berg, Chesworth, Klar and Speechley2010; Salari et al., Reference Salari, Darvishi, Ahmadipanah, Shohaimi and Mohammadi2022; Tinetti et al., Reference Tinetti, Speechley and Ginter1988), resulting in impaired mobility, fractures, and hospitalization (Tinetti et al., Reference Tinetti, Speechley and Ginter1988). To prevent falls, exercise programs that incorporate balance and functional movement reduce fall rates by 23 per cent (Bennie et al., Reference Bennie, De Cocker, Teychenne, Brown and Biddle2019; Sherrington et al., Reference Sherrington, Fairhall, Wallbank, Tiedemann, Michaleff, Howard, Clemson, Hopewell, Lamb and Sherrington2019, Reference Sherrington, Fairhall, Kwok, Wallbank, Tiedemann, Michaleff, Ng and Bauman2020). Yet despite the evidence that exercise can prevent falls, many persons in Canada are insufficiently active and do not meet the Canadian guidelines for physical activity (Government of Canada, 2021). To help explain physical inactivity and the factors that influence participation from the perspective of older adults, research suggests that a lack of tailored programming, limited supervision, insufficient education, low enjoyment, difficulty integrating exercise into daily life, limited social and professional support, low self-efficacy, absence of goal setting, and minimal participant involvement in planning are major barriers (Collado-Mateo et al., Reference Collado-Mateo, Lavín-Pérez, Peñacoba, Del Coso, Leyton-Román, Luque-Casado, Gasque, Fernández-Del-Olmo and Amado-Alonso2021).
To overcome the barriers to participation, it may be important to enable older adults to participate in community-based exercise services, especially considering that supervised exercise programs delivered by qualified professionals have been associated with improved physical functioning outcomes when implemented effectively (Gómez-Redondo et al., Reference Gómez-Redondo, Valenzuela, Morales, Ara and Mañas2024). Community exercise programs are not only preventive but complement rehabilitation by extending functional gains beyond the clinical setting. Rehabilitation typically focuses on restoring mobility, strength, and confidence following injury or illness; however, without ongoing opportunities to practice and reinforce these skills, improvements may plateau or decline (Sherrington et al., Reference Sherrington, Fairhall, Wallbank, Tiedemann, Michaleff, Howard, Clemson, Hopewell, Lamb and Sherrington2019; World Health Organization, 2017). Community programs provide structured environments where individuals can continue to build physical capacity, reduce the risk of recurrent falls, and sustain participation in meaningful activities (Sherrington et al., Reference Sherrington, Fairhall, Wallbank, Tiedemann, Michaleff, Howard, Clemson, Hopewell, Lamb and Sherrington2019; World Health Organization, 2017).
Despite the preventive and rehabilitative benefits of community-based exercise programs, providers have reported challenges modifying exercise for individuals with chronic conditions (McArthur et al., Reference McArthur, Ziebart, Papaioannou, Cheung, Laprade, Lee, Jain and Giangregorio2018) and therefore may need additional resources and system-level support. Furthermore, program delivery varies widely, as some services are led by qualified health professionals (e.g. kinesiologists and physiotherapists), while others rely on internally trained exercise providers or volunteers. While any increase in physical activity can contribute to better health and may support fall risk reduction, fall prevention exercise programs typically have an explicit aim of reducing falls and provide progressive balance and functional training in line with evidence-based recommendations. These recommendations specify that programs should provide a high challenge to balance, be offered for at least three hours per week, and be provided on an ongoing basis. For example, programs such as the Falls Management Exercise (FaME) and the Otago Exercise Programme have been shown to improve balance and reduce falls among community-dwelling older adults (Gawler et al., Reference Gawler, Skelton, Dinan-Young, Masud, Morris, Griffin, Kendrick and Iliffe2016; Iliffe et al., Reference Iliffe, Kendrick, Morris, Masud, Gage, Skelton, Dinan, Bowling, Griffin, Haworth, Swanwick, Carpenter, Kumar, Stevens, Gawler, Barlow, Cook and Belcher2014). However, a national survey of fall prevention community exercise programs for older adults in Canada reported that only 6 per cent of programs incorporated all three recommendations (Touchette et al., Reference Touchette, Oates, Menec and Sibley2021). This gap suggests that many existing community and clinical models may only partially align with evidence-based fall prevention exercise recommendations in real-world practice.
To ensure that implementation strategies are both effective and feasible, we must better understand how fall prevention exercise services are delivered in real-world contexts and the barriers and facilitators that influence their delivery. To do so, we conducted interviews with exercise providers operating in a range of community-based contexts to address the following questions:
-
• What are the barriers and facilitators that influence the delivery of fall prevention exercise services from the perspective of exercise providers?
-
• What contextual factors influence exercise delivery from the providers’ perspective?
By identifying barriers, facilitators, and contextual factors that influence program delivery, we aim to tailor implementation strategies that strengthen the delivery of the best practice fall prevention interventions.
Methodology
Positionality
In qualitative research, it is important to reflect on personal assumptions and perspectives to ensure transparency, credibility, and ethical integrity (Humphreys et al., Reference Humphreys, Lewis, Sender and Won2021). The researcher that led interviews and analyses, NT, is a young, white, male, English-speaking exercise physiologist who acknowledged his assumption that resistance, functional, and balance training were efficacious for improving physical functioning, well-being, and improved quality of life. When performing the interviews, NT aimed to be predictable, consistent, and accountable for his actions (Alessi & Kahn, Reference Alessi and Kahn2023) by explaining the interview questions and process before-hand and adhering to the described process. To ensure reflexivity, NT took notes to describe the tone and context of the conversations where needed and wrote an entry into a reflective journal before and after each interview.
To promote that our results aligned with the perspectives of the knowledge users, we convened a team of researchers, exercise providers, organizational representatives, and community members to provide input at all stages of the project. The study was reviewed by and received ethics clearance through the University of Waterloo Research Ethics Board (ORE 45977).
Methods
We conducted a study guided by qualitative description (Sandelowsk, Reference Sandelowsk2010) and performed interviews with exercise providers using a semi-structured interview guide and employed a thematic analysis from a post-positivist perspective.
Participants and recruitment
We used connections with municipal program providers, YMCAs, Victorian Order of Nurses, and Community Support Connections to purposefully recruit exercise providers in Ontario, Canada. We also purposefully sampled for providers by posting recruitment posters on social media and our lab website. Considering that the qualifications of an exercise provider can be variable (depending on the community and organization), we defined them as any individual who is currently teaching exercise at least twice per week (paid or unpaid) in programs that aim to prevent falls or improve balance, regardless of the provider’s educational status. While this included individuals who work for organizations, we also included exercise professionals who provide exercise services independently, such as kinesiologists, physiotherapists, clinical exercise physiologists, and certified personal trainers. To be included as an independent provider, we specified that providers must have experience delivering fall prevention exercise, either in person or virtually. All providers who were interviewed had to be able to perform the interview in English. To contextualize our findings, we collected information on age, sex, ethnicity, occupation, household income, education, and employment through a Qualtrics Survey (© 2024 Qualtrics) prior to the interview. All participants who consented completed their interviews; no repeat interviews were conducted, and transcripts were not returned for participant comment or correction.
Interview guide
Our interview guide was informed using the Consolidated Framework for Implementation Research (CFIR) (Damschroder et al., Reference Damschroder, Aron, Keith, Kirsh, Alexander and Lowery2009), which is an implementation framework that is designed to help researchers and practitioners systematically assess factors that influence the implementation and sustainability of initiatives (Featured Resource, n.d.). To identify barriers, facilitators, and contextual factors to exercise delivery, we drew on the CFIR inner setting domain and specifically adapted questions to the constructs of networks and communications, access to knowledge and information, relative priority, culture, and organizational incentives and rewards. The CFIR inner setting domain was used exclusively to guide question development; it was not applied as an analytic framework in coding or interpretation. Instead, we developed questions and prompts about the current barriers and facilitators to service delivery, and the support, training, and resources exercise professionals received. The completed guide was reviewed by our research team, with no major changes required.
Data collection
After we contacted potential participants and determined eligibility, we scheduled interview times and sent out a consent form and a Qualtrics Survey (© 2023 Qualtrics) to collect demographic information. When we conducted the interview, we asked whether they had any questions related to the consent form, verbalized that they were not responsible for appeasing the interviewer or researchers, provided a reminder that they could ask questions and skip questions regardless of the reason, and lastly, asked for verbal consent to record the conversation. Once the interview was completed, the interviewer thanked the participants for their engagement and let them know that their time and opinion were valuable. All interviews were audio-recorded over Zoom and transcribed verbatim by NT. We continued recruitment and analysis until data saturation was achieved, defined as the point at which no new themes or insights emerged from subsequent interviews (Guest et al., Reference Guest, Bunce and Johnson2006).
Thematic analysis
To understand the barriers, facilitators, and context, two researchers (NT and EM) conducted a reflexive thematic analysis (Braun & Clarke, Reference Braun and Clarke2006, Reference Braun and Clarke2019), embracing researcher subjectivity through collaborative interpretation rather than intercoder agreement, and applied NVIVO 14 (© QSR International 2024) for coding. Following Braun and Clarke’s six-phase approach with reflexive emphasis on iterative meaning-making, steps included: (a) transcription of the interviews verbatim; (b) familiarization with the interviews; (c) generating initial codes using the first two transcripts; (d) developing an initial coding template; (e) coding two subsequent transcripts to form the final coding template; (f) coding the remaining transcripts using the final coding template; and (g) interpretation of the data collected. In the beginning stages, NT and EM performed steps one, two, and three separately and met to discuss codes and construct the initial coding template through reflexive dialogue. NT and EM then coded an additional two transcripts before meeting to discuss and iteratively refine the final coding template, which NT used to finish steps 6 and 7. To determine themes, NT created a visual representation (thematic map) using the final coding template and compared it to the individual transcripts and among the codes. Once the initial thematic map was developed, it was presented to EM and the research group for feedback.
To improve the rigour and trustworthiness and address credibility, dependability, and confirmability (Forero et al., Reference Forero, Nahidi, De Costa, Mohsin, Fitzgerald, Gibson, McCarthy and Aboagye-Sarfo2018; Lincoln & Guba, Reference Lincoln and Guba1986), we: (a) held peer debriefing meetings with our research team; (b) established an audit trail during the data collection and analysis; and (c) recorded the interviewer’s perceptions and context in a reflective journal. To ensure transparency of our work, we followed the Standards for Reporting Qualitative Research (SRQR) (O’Brien et al., Reference O’Brien, Harris, Beckman, Reed and Cook2014) and included the consolidated criteria for reporting qualitative research (COREQ) (Tong et al., Reference Tong, Sainsbury and Craig2007) in our submission.
Demographic survey data were analysed descriptively in Microsoft Excel. Age was summarized with a mean and standard deviation, while categorical variables (ethnicity, sex, education level, household income, employment status, exercise habits, and professional background) were summarized with frequencies and percentages. Missing responses were excluded.
Results
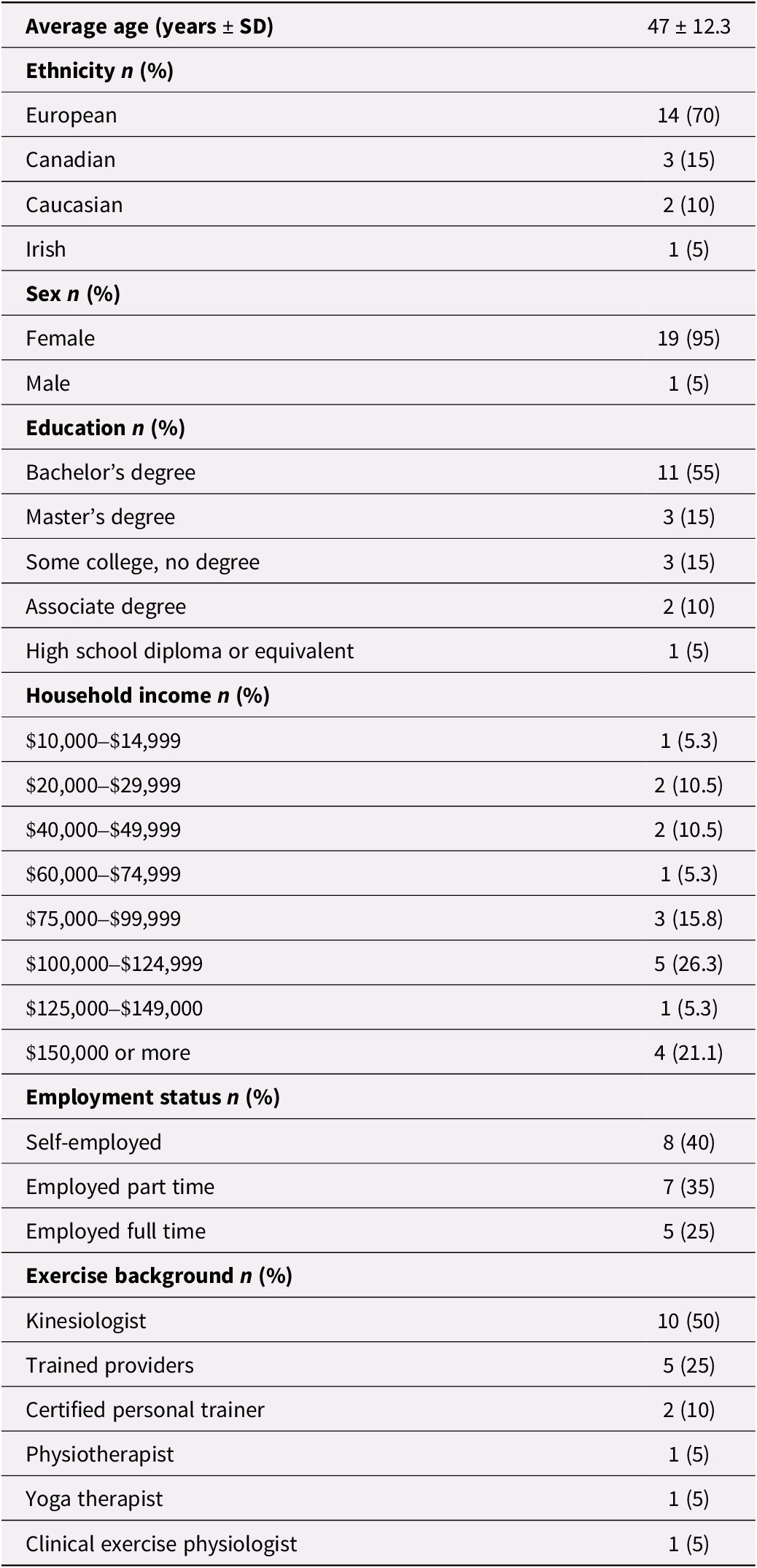
We conducted interviews with 20 exercise providers working in four distinct settings: Family Health Teams (n = 5), not-for-profit organizations (n = 4), municipal programs (n = 5), and independent practice (n = 6). Interviews were performed for an average (±SD) of 52 ± 8 minutes. Almost all the providers were female (95%) and of European ethnicity (70%). Most of the providers had a bachelor’s degree (55%), half were kinesiologists (50%), and while the remaining provider qualifications were variable, many were trained by the organization or asked to complete an accreditation elsewhere (25%). Income and employment status were variable (Table 1).
Results of the demographic survey sent to exercise providers
In our analysis, we identified two levels of barriers and facilitators. Some were consistent across all provider contexts, while others were specific to particular settings. The common barriers and facilitators are reflected in our first three themes: building trust among participants facilitated program success; creativity and fun were important for exercise delivery; and tailoring and progression of exercise quality depended on group size. To capture the context-specific influences (Family Health Teams, not-for-profit organizations, independent practice, and municipalities), we developed a final theme: networking and support were shaped by providers’ qualifications and work environment.
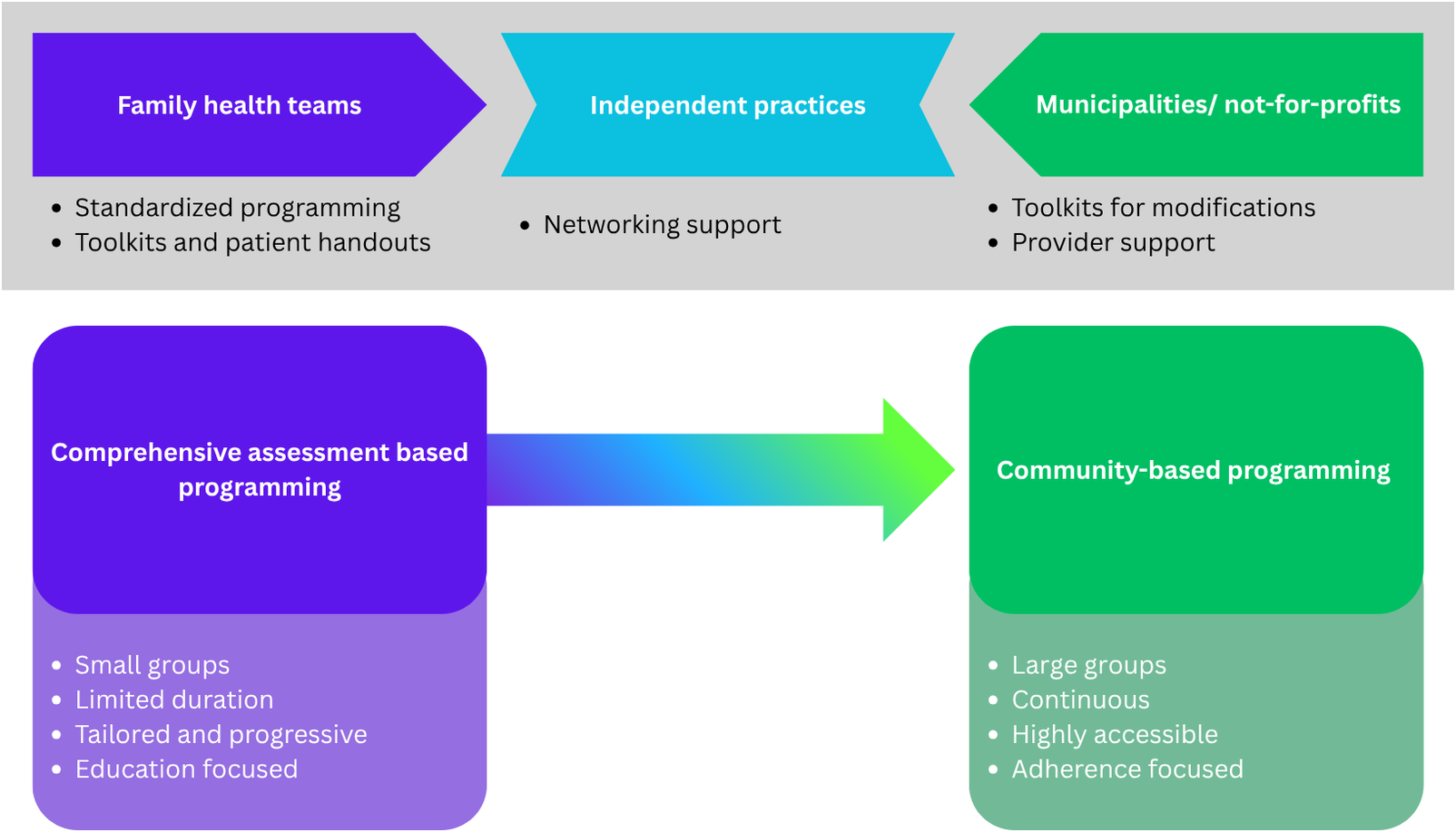
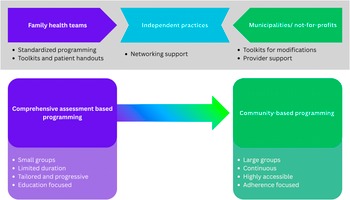
To illustrate the context of exercise services in Ontario, we created a figure that illustrates the types of services that were provided (comprehensive and community-based) and how each of the contexts generally fit within the types of services. We also provide some ideas for support based on the unique contextual barriers we identified in our themes (Figure 1).
Continuum of fall prevention exercise service delivery across organizational contexts. Notes: The horizontal arrow in the middle illustrates that program delivery is a spectrum from comprehensive clinical assessment programs (typically Family Health Teams) to larger community maintenance programs (typically municipal/non-profits), with independent services situated in the middle (highly variable). Organizational supports are suggested below each context (e.g. toolkits, networking, provider training) based on unique contextual barriers.
Common barriers and facilitators
Theme 1: Building trust among participants facilitated program success
While exercise services were variable depending on the context of delivery and the background or qualifications of the provider, it appeared that establishing trust among participants facilitated success. To create feelings of trust, providers believed that education on exercise and disease, tailoring to individual needs, performing exercise or functional testing, and providing follow-up were important.
In most cases, education was dependent on the expertise of the provider and usually included the rationale for exercise, information on specific diseases, advice on exercise principles (such as frequency and recovery), pain management, and how exercises translate to everyday activities. Education occurred during the demonstrations of the exercises, but also at the beginning and end of each session. For example, one provider described how they delivered education during the program:
…here’s why we’re going to be working on the shoulders or… this is why it’s important to maintain a nice chest where your chest is lifted and your chins away from your chest to maintain a beautiful curvature in the back of your body… So helping them understand the why. (P16)
Other than education, providers tried to meet the needs of participants by advocating for autonomy, monitoring the group visually, and providing positive reinforcement. Providers believed that these strategies were important to ensure participants completed exercises within their own capacity or ability, which helped improve confidence and adherence to exercise. One provider gave an example of how providing feedback can influence confidence and adherence:
…but say to them you’re doing this really well. That’s so much better… I think adherence to those exercises and that feedback… in terms of great job with this technique… They feel confident because they feel they’re being watched and have some confidence. (P8)
While education and a needs-first approach were the strategies mentioned most often, providers also talked about the importance of providing encouragement, giving proper demonstrations, being able to critically think and problem-solve, providing information and materials to facilitate learning, and being in contact with other health care professionals for support.
Therefore, it seemed that providers believed that creating safe and supportive environments helped participants feel more confident in their ability to perform exercise and adhere to the program. To create this environment, providers allowed for opportunities to ask questions, educated on exercise and self-monitoring, gave functional examples of exercises, and focused on positive feedback.
Theme 2: Creativity and fun were important for exercise delivery
On top of creating an environment where participants felt safe, many providers mentioned the importance of creativity and fun. Some of the main strategies that providers used to make programs enjoyable included facilitating socialization and having the freedom to adapt programs. To create an inclusive and fun environment, some providers mentioned that being themselves and sharing their own experiences outside of an exercise context was important. In some cases, providers mentioned that participants can develop emotional connections with the provider.
Sometimes not so much a personal life, but just sharing… stories you have, and I think it’s very important that they know I’m a human being, not just going in, OK, we’re going to do exercises now, you know, and making it fun. (P46)
Because establishing a connection among participants was perceived as important, it appeared that successful programs were somewhat dependent on the personality of the provider and the environment they facilitated, especially considering that the programs themselves acted as a major outlet for many older adults, as mentioned by one of the providers:
I mean it is personality dependent. Some of the class participants, they want to just come do the workout and leave, they don’t want interactions. But in the reality these fitness classes for seniors… they’re not just about the exercise, they’re about getting them out of their home, allowing them to be in the community. And that’s important for them. (P52)
Similarly, many providers believed that focusing on socialization before, after, and during exercise was helpful. Socialization strategies included setting aside time before and after the exercise to chat with participants, advocating for participant interactions during exercise, utilizing engaging activities (such as trivia) during cooldowns, and providing snacks after sessions. Regardless of the strategies that were used, many providers mentioned how the social component was incredibly important in facilitating wellness, networking, and adherence, even when exercise was delivered virtually, as mentioned by one of our independent providers:
…but I usually log in 30 minutes before and I am always on after, because undoubtedly there’s questions, comments, curious people who just want to talk because a lot of these people are isolated and alone. (P17)
Another common strategy that was used to facilitate fun was music. Providers mentioned taking song requests from participants and tailoring the music to the exercise intensity. By including music that matched the tempo of the exercise, providers found that participants were more likely to increase the intensity. For example, one provider shared the type of music they used and how it impacted the class:
Music is a big one. Music makes people have fun. Right now I’ve been doing a lot of Cape Breton Scottish jigs because they get faster as they go on. It still starts pretty fast, but as it goes on it gets faster and encourages people to keep their energy up. (P24)
Therefore, it appeared that while education and safety were considered important, the ability to create a fun and interactive environment kept participants engaged and facilitated adherence. By creating a safe but fun environment, providers believed that participants not only improved their physical functioning but built meaningful relationships with others.
Theme 3: Quality exercise tailoring and progression was dependent on group size
To ensure that exercise services were effective, providers tailored exercises to the needs and abilities of the participants. One of the ways in which providers created tailored programs was by conducting individualized assessments during exercise, as mentioned by one of the providers working in a clinic:
I do a one-hour assessment with my patients and that includes like 10 minutes of their medical history and reviewing their bone density results with them. I do heart rate and blood pressure, height and weight. I do some postural assessments and then I do physical performance measures where I test their balance, their grip strength, their gate speed, chair stands… So by the end of that assessment the patients feel like I know them. (P8)
However, while assessments were important, they were mostly performed in a one-on-one or small group setting. For providers who worked with large groups, this was not possible, due to either time constraints or a lack of equipment. To overcome a lack of assessment-based tailoring, providers tried to educate participants on body awareness and adapted exercise selection based on participant feedback; however, these strategies did not provide the same level of individualization as assessment-informed tailoring. For example, one provider mentioned the focus on safety and how they tried to tailor exercise by educating the class while also providing modifications:
And so I put a lot of trust on people to kind of do what’s safe for them. We talk about that. Do what’s safe for you. I talk about amplifications and modifications to exercise, and I always try to present a modification, but getting the right level of activity I find very challenging… (P24)
Two of the main reasons why providers struggled to provide individualized tailoring in programs were group size and participant variability. In large groups, providers must demonstrate multiple variations of an exercise and keep the class on time, and while they may be able to make a few corrections, in most cases, it is not possible. For example, one provider mentioned the participant variability when delivering exercise and how it influenced exercise selection:
I’ve got clients who’ve had vertebrae fractures and can’t do anything. They can’t lie down or won’t… there’s quite a big [variation], like…we have to adapt the exercises. And then I’ve got clients who can do a push up, or do a wall push up… it’s quite a big range. (P12)
Large group settings also put pressure on the providers, as they constantly tried to challenge more physically able participants while also considering that some may not have the ability to understand or perform the exercise correctly. Ultimately, providers tended to tailor exercises to the general ability of the group and felt that this led to inadequate dosing of exercise for those more capable. One provider described the challenges with adapting exercise to a large group and their concerns with safety:
…it’s challenging for me as the instructor to show all the levels so that my people who have some dementia and get confused and try to do something they can’t. It’s really hard and I don’t have a good way to do it. So I feel like every time I run a group, I have a new list of exercises that are probably not safe for a group setting. (P24)
It is important to note that while most providers in large groups struggled with exercise dosing, providers who knew a large variety of exercises and modifications may have been better equipped to adapt to the context. For example, one provider talked about how their exercise background and experience influenced their ability to adapt to the needs of older adults:
…there’s always a challenge when you know, especially when you don’t know exactly who’s going to show up for the day. But I always kind of have a list of ongoing exercises in my head like OK, if that one doesn’t work, let’s try this one instead. And I think to an important part of like group fitness is always making sure that you have one or two or three exercises in there that you know everyone can do safely. (P42)
Ideally, once a program has been established, participants should progress over time to facilitate changes in physical functioning, whether that be changes in volume, intensity, or exercise selection. However, while progression over the course of a program was possible for those working in small groups, it was very challenging in the large group context, as mentioned by one of our providers:
It’s not as structured as you would do with personal training, that is for sure… like you have participants that maybe only come every other week or sometimes they’re off for a whole month. So you can’t really follow a completely structured program… because there’s so many variables. (P48)
To try and achieve some form of progression, providers in large groups educated participants on how to progress themselves and when it was safe to do so, such as encouraging people to increase the amount or repetitions, sets, or weight; however, this was dependent on the participant and may not have represented true progression. Another strategy that was used to overcome the large group context was splitting group programs into multiple levels of ability to facilitate progression, where participants graduated into a more challenging program after properly learning the exercises. For example, one of the providers working in a clinic setting talked about how they organized their service to overcome this challenge:
…at the end they’ve got good technique and they know what the exercise is, but they’re not at a progression level yet. So the level two is for people who’ve gone through all of those, and now they’re ready to do progressive resistance program…
(P8)Therefore, it appeared that group size was a significant barrier that limited the ability of providers to tailor and progress exercise programs; a possible solution was a tiered approach where participants who had learned enough in an introductory session ‘graduated’ to a program where exercises were progressed. In large groups, providers tried to tailor exercises through participant education on body awareness, appropriate exercise dosing, and progression. However, even though the strategies attempted to provide some level of progression, the effectiveness was unclear.
Delivery context and unique barriers and facilitators
Theme 4: Networking and support are dependent on qualifications and work environment
While providers mentioned similar barriers and facilitators across contexts, we also found that the supports and work environments were different based on the context of delivery, and the qualifications or expertise of the provider. We describe the different contexts and their unique barriers and facilitators below.
Family health teams
Kinesiologists reported that starting a position in a Family Health Team was challenging. In this context, most kinesiologists were hired and given freedom to create an appropriate service or were asked to run an already existing program. While providers mentioned that they were very confident in their abilities, they felt overwhelmed when faced with creating new services or adapting to meet the expectations of an existing one. One provider talked about their challenges with support and their need to become more informed:
I’m working with the doctors and nurse practitioners. I don’t know other people doing this similar thing. Which was very challenging, you know, starting the role out. I think a lot of this stuff I just had to figure out on my own or take [a course]. I’ve taken every course that you can imagine to try to figure it out.
(P18)To overcome the challenge of developing a new service, kinesiologists reported connecting with other kinesiologists from other Family Health Teams. By connecting with others, kinesiologists felt more confident in how to design and implement new services. Connections were usually facilitated via online groups or forums where kinesiologists frequently asked questions and shared resources. For example, one provider reported their use of online resources to connect with another kinesiologist when creating a service:
I went to the website of every family health team and Community Health Centre in Ontario to see if they had a KIN and if they did, I emailed and called that KIN and said, hey, what do you do to figure it out? Because there was not a lot out there.
(P24)One explanation for a lack of guidance is the wide scope of practice of kinesiology. Several providers mentioned that each kinesiologist has their own background or expertise, which makes it difficult to find an appropriate resource or person for a particular question or concern:
…like we can address so many different aspects and especially as kinesiologists, we can talk about all the other factors that kind of fall into this category other than just like exercise like we can talk about nutrition and things like you know, mental health, we can talk about home environments. And so, there’s like a lot more things that we can touch on other than exercise.
(P11)Another challenge when starting the position was being able to feel confident delivering services to a variety of individuals living with unique chronic diseases or challenges. To overcome this, one kinesiologist mentioned the importance of continuing education: ‘…when it comes to like education. I think the more is better… The more education you can get in in this field. It’s definitely a benefit’ (P48).
In this regard, kinesiologists typically felt supported, as the Family Health Teams provided ample opportunity to attend educational webinars or workshops, as mentioned by one of our providers:
The Family Health team does do a great job of providing almost like a week’s worth of education days through our fiscal year, as well has an education budget. So, it’s strongly encouraged that we do our training. (P11)
Other than the challenges with onboarding, some providers mentioned that they spent a significant amount of time looking for resources or creating them for patients. To overcome the challenge of finding appropriate resources, providers would leverage their support networks, which included online groups and forums, as well as communicating with other health care professionals in their Family Health Team. However, one provider did mention that while being a part of a multidisciplinary Family Health Team was invaluable, the inclusion of kinesiologists on some multidisciplinary teams was novel, and the differences in perspective could pose a barrier.
There wasn’t that many resources. I think we were all kind of just figuring it out together because that was the first time that they had ever hired a kinesiologist. So they weren’t quite sure you know what the role would look like.
(P42)Therefore, it seemed kinesiologists working for Family Health Teams felt overwhelmed and in need of guidance from others (in the initial stages of the position), especially given the wide scope of kinesiology. It is important to note that the wide scope and freedom provided to create services also meant that the exercise services that were provided by Family Health Teams varied based on the kinesiologist’s expertise and access to standardized programming.
Not-for-profit organizations
In the not-for-profit context, exercise providers were most often trained for their role, which tended to be much narrower in scope. Providers in this context typically received specialized training directly from their organization or were referred to external accreditation programs, such as the Canadian Centre for Activity and Aging Seniors Fitness Instructor Course. In general, we found that providers who received training from their organization perceived it as very helpful, supportive, and informative.
Although the training varied depending on where it was obtained, it generally included access to informational materials, participation in online meetings (where exercises were demonstrated and activities encouraged), and opportunities to shadow experienced providers. Following the shadowing period, providers were required to deliver a standardized program under evaluation. Once the training requirements were met, providers were granted the autonomy to teach the program independently at their designated sites. One provider talked about the differences between providers and how they adapted their sessions after obtaining autonomy over their programs:
It’s been a year and a half. So now I mostly just make it up as I go, right? There are certain instructors. They have a routine… So for me I just had to find a pattern, like we do forward movement, side movements, back movements. So I just try to switch between each one… (P52)
Once teaching, providers were given other opportunities for support. Many mentioned having access to monthly meetings, education resources, and were encouraged to ask questions; however, regardless of supports available, providers reported that the volume of exercise delivery and perceived low pay were barriers:
Well… they don’t have is a very good pay grade, very low like you’re almost at minimum wage. Which is super sad because it’s such a beneficial program and I think the rate of pay deters people from applying for the role… (P46)
Despite their training, some providers felt overwhelmed when delivering exercise programs. At first, they reported challenges with delivering exercise and developing a routine with participants. Later, many felt pressured to continuously modify programs to meet participants’ needs and maintain engagement:
…it can be overwhelming at the beginning if you have to do an hour-long session and you think, well, how am I going to feel this hour… You need to deliver a variety of things and so that is probably what every exercise instructor realizes. Otherwise, I think they will see that their classes will drop considerably and they won’t have a lot of success if they stay at the same… (P48)
Therefore, in the context of community programs, it appeared that while the training of providers was perceived as comprehensive and prepared them to deliver programs, prior exposure to exercise and leadership may have facilitated confidence or self-efficacy in the early stages of delivery. Regardless of support, providers believed that the volume of exercise they performed when teaching classes and low pay were barriers.
Independent practice
While the focus of this project was to examine community programs delivered by organizations, we also interviewed people who delivered programs independently. In general, we found that independent providers focused on one-on-one services, small groups, or online sessions. While variable, many seemed to have had access to additional equipment to conduct comprehensive assessments. With a larger focus on assessment and tailoring, independent providers typically designed individualized programs for participants. Once the initial stage of the tailoring was completed, participants continued to see the provider (check-ups) until they were confident to exercise independently. At this point, some participants moved on to other programs or, if there was an option available, joined a group exercise service run by the same provider.
Providers delivering services independently also had variable levels of exercise training or education and may or may not have taken disease-specific courses, such as Bonefit™ or other online webinar courses. Those working in clinics were typically kinesiologists or physiotherapists and sometimes worked with other health care professionals within that setting. Those working from home tended to use their own connections for support, which were made at conferences, webinars, or previous positions. Supports made in this way were dependent on the provider, with many reporting that they worked alone. For example, one provider talked about their independent practice and how the transition influenced how they interacted with other professionals:
But I’ll be honest with you, a lot of what I do is in isolation now and since the pandemic I’ve went all online and I don’t have anybody that I’m working through. I’ve created my own like… no middleman anymore, so there’s not a lot of interaction. So it’s up to me to kind of go out there and… learn with courses and people that I trust in the industry. But as far as interconnectedness now over the last well… since 2020 has been kind of in isolation, so there’s not a lot of connection. (P17)
Therefore, independent providers seemed to focus mainly on assessments and creating individualized programs for participants. However, the type of services offered after the initial assessment depended on the qualifications of the provider, the equipment they had available, and the provider’s preference of exercise delivery. While some providers in this context were supported within clinics, there were also many who lacked support and delivered services in isolation.
Municipalities
Providers working for municipal programs were typically outsourced and mentioned applying for jobs after seeing an advertisement. In this case, providers found it helpful to understand the community, as it appeared to them that organizations were more interested in the provider’s ability to lead a class and facilitate socialization rather than their knowledge of exercise, as described by one of our providers who had several experiences delivering programs in the community:
I’m almost entirely interviewed by an administrative person who… they’re not sure what they’re looking for other than probably somebody that socially, is going to be able to interact with people… So, what I have found is they explore more about where my experience has been with different age groups of people. How am I going to interact with somebody who might be there to socialize… which in a lot of these community centres they put as much emphasis on the social component as they do on the Wellness component… (P16)
When a position was obtained, providers reported receiving little to no training and instead were given the freedom to create and implement their own programs. This meant that most of the characteristics of programs were based on the providers’ previous experience and background, as explained by two of our providers:
To this point… in any different situation I’ve been in, it’s been up to me to design it… It’s an hour long. Starts this time ends this time, it’s all yours. (P16)
So the city ones I have to plan whatever I’m going to do, whereas the [not-for-profit] ones I just kind of show up do the thing… (P53)
Similar to onboarding challenges, providers also mentioned inconsistencies with different positions and expectations, pressure to perform well, and feelings of competition among other providers, as reported below by one of our providers: ‘I found that hard when I first started, learning how to modify some of the exercises… but sometimes there can be…. Unfortunately, competition between classes or instructors…’ (P54).
Therefore, when delivering programs for cities or towns, it seemed that community providers felt similarly to kinesiologists, where they sometimes needed to design and create their own programs and resources. On the other hand, providers delivering exercise for cities and towns reported unique barriers, such as pressure to meet expectations and competition with other providers.
Discussion
This study identified four themes that shaped exercise providers’ experiences delivering fall prevention programs: building trust among participants was central to program success, creativity and fun facilitated engagement in exercise delivery, tailoring and progression of exercise quality was strongly influenced by group size, and networking and support were shaped by providers’ qualifications and work environments. Together, these findings highlight both common and context-specific barriers and facilitators that influence the delivery of fall prevention exercise services.
Tailoring and progression were generally only feasible when providers worked in small groups or one-on-one settings, sometimes with assessments to guide exercise prescription. This echoes findings from Malik et al., where providers reported group size as a major limitation to successful implementation and emphasized the benefits of small-group delivery (Malik et al., Reference Malik, Virag, Fick, Hunter, Kaasalainen and Dal Bello-Haas2020). Despite the challenge of tailoring in larger groups, providers in our study reported educating on body awareness, appropriate exercise dosing, and progression to overcome a lack of tailoring. While these strategies supported short-term engagement, it remains unclear whether the design and exercise selection of the programs align with established evidence for fall prevention, where the interventions in research studies are often tailored, delivered, and progressed by health care or exercise professionals. The issue of program design was also raised in a systematic review by Forsyth et al., where interventions often reflected provider experience or local practice rather than structured tailoring based on functional capacity or evidence (Forsyth et al., Reference Forsyth, Soh, Elks, Lin, Bailey, Rowbotham, Mant, Hartley and Deaton2024). Therefore, even though exercise tailoring and progression are important to ensure proper exercise dosing, group size, program design, and the expertise and experience of the provider are important factors that need to be considered when implementing exercise programs in the community.
In our study, providers frequently reported the importance of creating a safe and social environment. To create a safe environment, providers encouraged participants to ask questions, educated them on exercise and self-monitoring, gave functional examples of exercises, and focused on positive feedback. Creating a safe environment to encourage older adults to exercise is understandable, as qualitative evidence suggests that functional capacity and risk of injury influence perceived capability and reduce motivation (Meredith et al., Reference Meredith, Cox, Ibrahim, Higson, McNiff, Mitchell, Rutherford, Wijayendran, Shenkin, Kilgour and Lim2023). One potential reason providers emphasized safe environments is that adherence, alongside tailoring and progression, is critical for fall prevention, as evidence suggests that attending more than 80 per cent of sessions reduces fall risk (Osho et al., Reference Osho, Owoeye and Armijo-Olivo2018). At the same time, we also identified that social engagement and supervision were key factors that providers believed were important. To support the influence of socialization on exercise adherence among older adults, Park et al. found that the social environment is important when identifying physical activity levels among older adults (Park et al., Reference Park, Prochnow, Vigil and Smith2025), and while socialization is not important to all, it has been reported previously as an important motivator for older adults (Kilgour et al., Reference Kilgour, Rutherford, Higson, Meredith, McNiff, Mitchell, Wijayendran, Lim and Shenkin2024). Together, our findings suggest a central division: large groups may promote social engagement and adherence, whereas small groups enable tailored and progressive exercise. Ideally, programs would offer both, but resource limitations pose significant challenges, given that Canadian organizations report financial and staffing constraints that limit their capacity to promote physical activity (Ramanathan et al., Reference Ramanathan, Faulkner, Berry, Deshpande, Latimer-Cheung, Rhodes, Spence and Tremblay2018).
Beyond the shared barriers, providers also reported unique barriers in each context. For example, we found that kinesiologists working in Family Health Teams spent a significant amount of time finding resources for patients and struggled to develop programs (during the initial stages of their position); independent providers seemed to lack support or networking capacity; providers working for not-for-profit organizations struggled with the novelty of teaching exercise (volume of exercise and expertise) and receiving low pay; and providers working for municipal programs struggled with feelings of expectations and competition with other providers. Although it may be challenging to address the unique nuances of each context, others have suggested that having consistent fall prevention programs could help address provider barriers (Malik et al., Reference Malik, Virag, Fick, Hunter, Kaasalainen and Dal Bello-Haas2020).
Based on our results, it seems that certain settings may offer distinct advantages when leveraged strategically to support proper implementation. For example, Family Health Teams are often situated within clinical environments and may be better suited to support individual assessments, small-group formats, and progressive exercise dosing, addressing barriers related to tailoring and provider expertise. In contrast, programs delivered in the not-for-profit and municipal settings – often led by providers trained for their role – may prioritize accessibility and scale and therefore benefit from structured toolkits and training supports that enhance adherence, safety, and basic progression principles within large groups. Lastly, services offered in independent practices, while variable, offer adaptability and creativity when sufficient support is available, and may be optimized for hybrid or specialized services. Ultimately, implementation efforts should consider how each model aligns with its delivery context and whether a hybrid approach – combining features from multiple models – might balance access, adherence, and quality in community-based exercise programming for older adults.
There are limitations to our study. Although we recruited providers from several contexts (Family Health Teams, non-profit organizations, independent practice, and municipalities), our sample consisted primarily of females of European ethnicity. We also recognize that our sample does not represent all exercise services available in Ontario, and the variability in provider training, equipment, and organizational priorities within each context limits the transferability of our findings. For example, other important settings such as hospital-based rehabilitation, long-term care facilities, private fitness clubs, and rural or Indigenous community programs may face distinct barriers and facilitators related to medical oversight, resource availability, cultural tailoring, and geographic access. While participants worked across diverse Ontario settings (urban and rural), we did not systematically record specific regions or rural–urban status, further limiting our ability to examine geographic variation in implementation barriers. Future research should examine these contexts to provide a more comprehensive understanding of fall prevention exercise delivery.
Conclusion
Delivering exercise programming in large groups remains a major barrier to proper tailoring and progression. In response, many providers emphasized creating safe and socially engaging environments to support participation and adherence. Beyond group size, providers also face context-specific barriers, including resource constraints, lack of networking support, low pay, and organizational expectations. Designing effective fall prevention programs therefore requires attention to group size, provider experience, and delivery context. Future efforts should aim to balance exercise tailoring with additional strategies that facilitate adherence by leveraging the strengths of different models and exploring hybrid approaches that optimize both access and quality.
Data availability statement
The data sets generated and/or analysed during the current study are not publicly available due to confidentiality agreements with participants, but de-identified excerpts are available from the corresponding author on reasonable request.
Acknowledgements
We acknowledge the support of Natalie Hoshing & Jenn McDonald (Community Support Connections), Rhona McGlasson (Bone and Joint Canada), Tiffancy Smith (City of Waterloo), Danielle Todd (Victorian Order of Nurses), Joanna MacFadzean, and Crystal Hughes (YMCA of Three Rivers), who served as members of the research team informing the project.
Author contribution
Conceptualization: N.T., L.M.G.; Formal analysis: N.T.; Funding acquisition: N.T., L.M.G.; Investigation: N.T.; Methodology: N.T., L.M.G.; Project administration: N.T., L.M.G.; Supervision: J.T., A.-A.V., P.C., Z.W., J.S., J.W., L.M.G.; Validation: J.T., A.-A.V., P.C., Z.W., J.S., J.W.; Visualization: N.T.; Writing – original draft: N.T.; Writing – review and editing: J.T., A.-A.V., P.C., Z.W., J.S., J.W., L.M.G.
Financial support
We acknowledge the support of the Natural Sciences and Engineering Research Council of Canada (NSERC), CREATE 509950–2018 Training in Global Biomedical Technology Research and Innovation. The authors wish to acknowledge the CAN-TAP-TALENT for its role in supporting the completion of this CAN-TAP-TALENT Research Project. The CAN-TAP-TALENT is funded by the Canadian Institutes of Health Research (CIHR) – FRN 184898.
Competing interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical standard
The study was reviewed by and received ethics clearance through the University of Waterloo Research Ethics Board (ORE 45977). When we conducted the interview, we asked whether participants had any questions related to the consent form, verbalized that they were not responsible for appeasing the interviewer or researchers, provided a reminder that they could ask questions and skip questions regardless of the reason, and lastly, asked for verbal consent to record the conversation. All participants provided informed consent for publication of anonymized data. No identifying information is included in this manuscript.


 Open access
Open access