Visceral adiposity and abdominal obesity are related to increased cardiovascular risk(Reference Powell-Wiley, Poirier and Burke1). Excess body weight contributes to low-grade systemic inflammation, characterized by elevated inflammatory cytokines and metabolic dysregulation, further increasing the risk of cardiovascular comorbidities(Reference Zhou, Gizlenci and Xiao2,Reference Soták, Clark and Suur3) . The World Health Organization estimates that 17·9 million deaths each year are caused by cardiovascular diseases globally(4). In this sense, the literature has been dedicated to studying the mechanisms involved in developing cardiovascular diseases, mainly those caused by modifiable risk factors(Reference Fan and Watanabe5). The pathogenesis of atherosclerosis, one of the leading causes of acute myocardial infarction, is mainly explained by the process of aggression to the vascular endothelium, which begins with the accumulation of oxidized lipids in the wall of the endothelial intimal layer, forming an atheroma plaque that obstructs the passage of blood flow(Reference Libby6,Reference Jebari-Benslaiman, Galicia-García and Larrea-Sebal7) .
Endothelial dysfunction promotes impairments related to vascular tone, fluid exchange, and angiogenesis, and is characterized as one of the key processes in the pathophysiology of atherosclerosis(Reference Medina-Leyte, Zepeda-García and Domínguez-Pérez8). The vascular endothelium is formed by a single layer of endothelial cells that are in the endothelial intimal layer and perform activities such as vasodilation, inhibition of platelet aggregation, inflammation, and oxidative stress(Reference Poredos, Poredos and Gregoric9). In cases of endothelial instability, caused by aggression to the endothelium, the beginning of the cascade of events of atheroma plaque formation may occur, which involves the infiltration of leukocytes and recruitment of neutrophils mediated by vascular cell adhesion molecule-1 (VCAM) and by intracellular adhesion molecule-1 (ICAM)(Reference Yu, Liu and Peng10) and uptake of long-chain fatty acids, mediated by the scavenger receptor B2 (CD36)(Reference Shu, Peng and Hang11).
Oxidative stress, a result of increases in free radicals in relation to the content of antioxidants(Reference Khosravi, Poursaleh and Ghasempour12), promotes aggression to the vascular endothelium(Reference Li, Xin and Gu13). With increased oxidative stress, damage to molecules in cell membranes, such as proteins, nucleic acids, and lipids, can occur(Reference Forman and Zhang14). Furthermore, the hardening of arteries caused by endothelial dysfunction, or the reduction in the diameter of blood vessels caused by atheroma plaques, can result in increased blood pressure(Reference McClary and Massey15). Both upper and lower limb blood pressure, such as that assessed by the ankle-brachial index (ABI)(Reference Casey, Lanting and Oldmeadow16), are related to cardiovascular events, resulting in increased intima-media thickness of the carotid artery and carotid-femoral artery pulsation velocity(Reference Tatasciore, Di Nicola and Tommasi17).
To improve risk factors related to endothelial dysfunction, several studies have been dedicated to evaluating the effect of foods rich in antioxidant compounds on cardiovascular health, mainly in people with increased cardiometabolic risk, such as in individuals with excess body weight(Reference Reverri, LaSalle and Franke18–Reference Bardagjy, Hu and Giebler21). Dietary interventions involving herb-derived foods and beverages may benefit oxidative stress, especially in individuals with excess body weight, owing to their rich phenolic compound content(Reference Montazeri, Fatahi and Sohouli22–Reference Ghafouri, Hajiluian and Jafari Karegar26). In this sense, kombucha stands out as a fermented, lightly carbonated beverage rich in phenolic compounds such as epicatechin, epigallocatechin, epicatechin gallate, and epigallocatechin gallate, which are capable of neutralizing reactive oxygen and nitrogen species(Reference Musial, Kuban-Jankowska and Gorska-Ponikowska27). This beverage is produced with teas from Camellia sinensis leaves (black, green, white, or red tea), among which green tea stands out due to its high antioxidant potential(Reference Jakubczyk, Kałduńska and Kochman28).
Although kombucha has been produced for millennia, its popularity has increased only recently. Consequently, few studies have investigated its effects on human health(Reference Kapp and Sumner29,Reference Antolak, Piechota and Kucharska30) . To date, no clinical research has been dedicated to evaluating the effect of daily consumption of green tea kombucha on oxidative stress and endothelial health. Therefore, the present study aimed to investigate the effect of this beverage on health in individuals with excess body weight. The energy-restricted diet was adopted in both groups as it is a standard intervention to reduce cardiovascular risk in overweight individuals without apparent comorbidities.
Methods
This is a secondary analysis of a previously published study by our team, entitled ‘Green tea kombucha impacts inflammation and salivary microbiota in individuals with excess body weight: a randomized controlled trial’. Considering the previously demonstrated anti-inflammatory effects of green tea kombucha, this secondary analysis assessed whether these effects also extend to oxidative stress and endothelial function. More details on the methodology used can be found in Fraiz et al. (2024)(Reference Fraiz, Bonifácio and Lacerda31).
Study design
This randomized, controlled clinical trial was conducted with two parallel experimental groups without blinding. The control group followed an energy-restricted diet of 500 kcal/d, and the kombucha group, in addition to the diet, consumed 200 ml of green tea kombucha daily for 10 weeks.
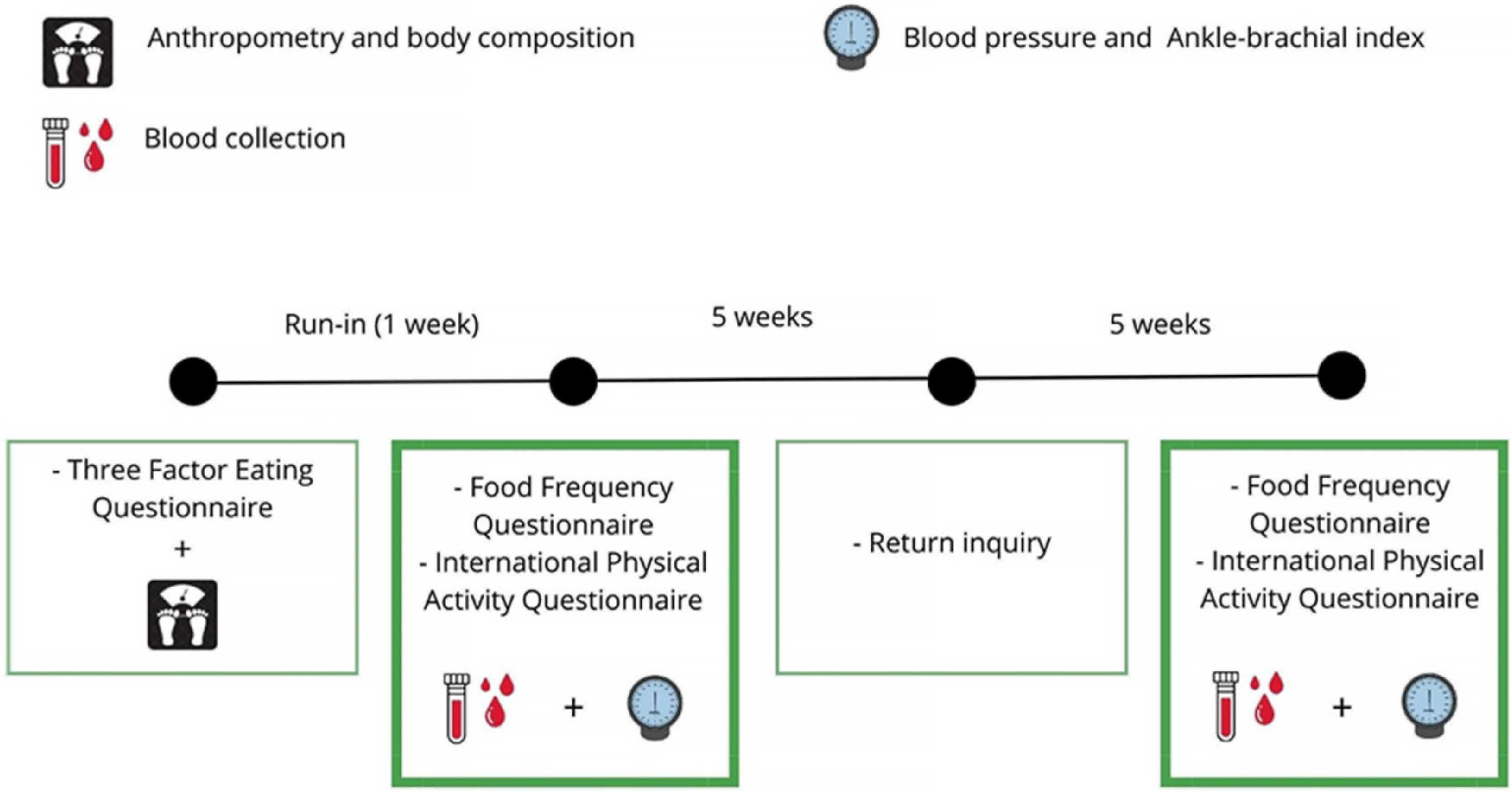
At the beginning of the study, all participants filled out the Three-Factor Eating Questionnaire (TFEQ) and were measured for anthropometry and body composition markers. After this moment, all participants were under a one-week run-in period to assess possible adherence to the study protocol. During this period, participants had to maintain stability in their usual weight, with less than < 2 % variations, and could not consume teas and fermented foods. Those who met the initial requirements participated in the initial blood collection and brachial and peripheral blood pressure measurements to measure the ABI. After 5 weeks of study, participants responded to a return questionnaire to assess adherence to the protocol. At the end of the study, a new blood collection and blood pressure measurement were performed (Figure 1).
Experimental design of the study.

Participants
The study included men and women aged 18 and 45 years, with excess body weight, assessed by body mass index (BMI) ≥ 27 kg/m2, body fat percentage > 25 % for men and > 30 % for women, and waist circumference ≥ 94 cm for men and ≥ 80 cm for women. Participants were recruited from the local community of Viçosa (Minas Gerais, Brazil) and underwent online and in-person screening to assess inclusion criteria. Individuals with chronic diseases such as diabetes, high blood pressure, and cardiovascular diseases did not participate in the study. Those who had acute infectious or inflammatory conditions in the last three months and those who had eating disorders, pregnancy, menopause, were smokers, athletes, vegans, or were in the lactation period were also not included. Individuals who already regularly consumed teas, supplements, or fermented foods were also not included.
Sample calculation and randomization
The sample size calculation for this study was performed using G * Power software (version 3.1.9.6), based on an effect size of 0·8 between two independent means of total serum antioxidant levels following green tea supplementation in individuals with obesity(Reference Suliburska, Bogdański and Szulinska32). A statistical power of 95 % and a significance level of 5 % were applied. The minimum required sample size was 30 individuals per group.
The randomization of participants who were included in the study was carried out using the minimization method, in a 1:1 ratio, in MinimPy software, version 0.2 (Copyright, Mahmoud Saghaei, 2010–2011), considering sex, age, and BMI as prognostic factors(Reference Abramson33). Additionally, allocation concealment was implemented to minimize selection bias.
Interventions
Both groups followed healthy diets individually planned by a nutritionist, considering the distribution of macronutrients and micronutrients necessary for health, and applying a caloric prescription of (–500 kcal/d) in the values calculated by the Estimated Energy Requirement (EER) for individuals with excess body weight(Reference Trumbo, Schlicker and Yates34). In addition, all participants received nutritional guidance, five menus with a list of substitutions, and a recipe book with the preparations presented on the menus. Furthermore, everyone was advised to maintain their usual level of physical activity.
In addition, participants in the kombucha group received seven 200 ml bottles of kombucha weekly and were instructed to keep them refrigerated and ingest them with a main meal (lunch or dinner) due to the acidity of the beverage. The 200 ml dose was established considering the safety profile demonstrated in previous studies conducted by our research group(Reference Fraiz, Bonifácio and Lacerda31,Reference Costa, da Silva Duarte and Fraiz35) . Kombucha was also produced weekly, with green tea from the Amaya brand, grown in the city of Registro (São Paulo, Brazil). The tea was prepared by infusion, as recommended by the manufacturer’s instructions. The 30 g/l of a biofilm of bacteria and yeast and a previously produced kombucha were added until the pH reached 4·4. Incubation for kombucha fermentation occurred for 5 d at 25°C.
At the end of preparation, through Ultra-high performance liquid chromatography-MSE (UPLC - MSE) analysis, it was possible to determine that kombucha presented 92 phenolic compounds, mostly from the flavonoid class (70·7 %), phenolic acids (25 %), lignans (2·2 %) and other polyphenols (1·1 %). Among the most abundant phenolic compounds in the beverage are gallocatechin, catechin 5-O-gallate, epicatechin, epigallocatechin, 5-O-galloylquinic acid, catechin, 5-p-coumaroylquinic acid, quercetin 3-O-rutinoside, and niricetin 3-O-glycoside. Furthermore, it exhibited a total phenolic content of 0·32 ± 0·003 mg GAE/ml (in gallic acid equivalents), antioxidant capacity of 3·24 ± 0·43 μmol TE/ml, pH of 3·41 ± 0·09, and total acidity of 0·20 ± 0·02 (w/v acetic acid).
Assessments and measurements
At the beginning of the study, weight and body composition were assessed using the tetrapolar electrical bioimpedance technique (Tetrapolar Bioimpedance, Inbody, model Y230). The participants’ food consumption was assessed using a food frequency questionnaire (FFQ), which was digitized in ERICA-REC24h, which uses the food composition table developed by the Brazilian Institute of Geography and Statistics (IBGE)(36). All food consumption data were adjusted for thousand kilocalories. Physical activity was assessed using the short version of the International Physical Activity Questionnaire (IPAQ), validated for the Brazilian population(Reference Matsudo, Araújo and Matsudo37), and presented in metabolic equivalent task (MET).
On the initial and final experimental days, participants came to the laboratory, fasting for 10 h, to collect blood and measure brachial and peripheral blood pressure. The day before the experimental day, all participants were instructed to eat a standard dinner, as determined by the study. The blood was collected by a trained professional and centrifuged to separate the plasma fractions for analysis of the markers in the focus of this study. To this end, the samples were stored in an ultrafreezer at −80°C until analysis.
At the beginning of the study, an analysis of the inflammatory profile, including complement component C3 and C-reactive protein (CRP), and liver enzymes, such as aspartate aminotransferase (AST), alanine aminotransferase (ALT), and gamma-glutamyl transferase (GGT), was carried out to characterize the participants about variables that may interfere with oxidative stress and endothelial health. For these analyses, the UV kinetic method was applied using the Mindray BS-200® Chemistry Analyzer (Shenzhen, China), following the procedures outlined by the commercial kit from Bioclin Bioquímica (Belo Horizonte, Minas Gerais, Brazil).
The markers ICAM, VCAM, oxidized low-density lipoprotein (ox-LDL), CD36, glutathione peroxidase (GPx), and glutathione reductase (GR) were analyzed using the enzyme-linked immunosorbent assay (ELISA) technique. The kits used were: “Human ICAM/CD54” (E-EL-H6114), “Human VCAM/CD106” (E-EL-H5587), and “Human OxLDL’ (E-EL-H6021) from Elabscience Biotechnology; and “Human Cluster of Differentiation 36’ (MBS166979), ‘Human Glutathione Peroxidase 3’ (MBS2704850), and ‘Human Glutathione Reductase’ (MBS2703164) from MyBioSource®, all following the manufacturers’ recommended protocols.
The activity of superoxide dismutase (SOD), hydrogen peroxide (H2O2), iron-reducing antioxidant power (FRAP), malondialdehyde (MDA), and nitric oxide (NO) was determined using plasma samples in colorimetric assays. SOD was determined considering the capacity to catalyze the reaction of superoxide (O2) into H2O2, which was also evaluated through the oxidation of substrate by a peroxidase(Reference Marklund and Marklund38,Reference Nahum, Wood and Sznajder39) . At the same time, FRAP analysis considered reducing ferric ions to ferrous ions by adding a sample with reducing activity(Reference Benzie and Strain40). MDA dosage measured lipid peroxidation through thiobarbituric acid reactive species (TBARS)(Reference Buege and Aust41). The NO was considered a standard curve with known sodium nitrite concentrations ranging from 0–125 µM(Reference Grisham, Johnson and Lancaster42).
Brachial blood pressure was measured in participants in both arms, and in case of differences, the arm with the highest value was measured again, and the average between the values was considered(43). To do this, the participants were seated, with their legs uncrossed, feet flat on the floor, with an empty bladder, free of clothing on their arms, palms facing upwards, and arms at heart level(Reference Barroso, Rodrigues and Bortolotto44).
To assess the ABI, a portable vascular Doppler (MEDMEGA®, DV 610B) was used, associated with a sphygmomanometer, measuring systolic blood pressure (SBP) on the right and left sides of the brachial, dorsal foot, and posterior tibial arteries. The ratio between the highest SBP of the lower limb (dorsal foot or posterior tibial artery) and the brachial SBP of the corresponding side was calculated, and the ABI value that presented the lowest value between the right and left sides was adopted(Reference Kim, Wattanakit and Gornik45).
The primary outcomes of this study are oxidative stress markers such as SOD, FRAP, GPx, GR, oxLDL, MDA, ON, and H₂O₂, while the secondary outcomes are endothelial markers ICAM, VCAM, CD36, ABI, SBP, and DBP.
Statistical analyses
Statistical analyses and graphical representations were performed using SPSS (version 25.0) and GraphPad Prism (version 10.0) software, respectively. The studies were performed according to the per-protocol principle. The Shapiro-Wilk and Levene tests were used to assess the normality of variables and the homoscedasticity of variances, respectively. Baseline participant characteristics were analyzed using the independent samples t test or the Mann–Whitney U test, according to normality. A repeated measures analysis of variance (ANOVA), based on Wilks’ Lambda from the multivariate test, was conducted to evaluate the interaction between time and condition. Correlations between variables were estimated using Pearson’s or Spearman’s correlation coefficients, depending on data distribution. Results are expressed as mean (standard deviation) or median (minimum-maximum value), with a statistical significance of 5 %.
Results
A total of 500 individuals were recruited, and 75 met the inclusion criteria and began the study. Throughout the study, 21·33 % of participants were lost to follow-up, who were discontinued for personal reasons or non-adherence to the study protocol.(Reference Fraiz, Bonifácio and Lacerda31) After 10 weeks, 59 people completed the study, 29 from the control group (17 women and 12 men) and 30 from the kombucha group (18 women and 12 men). When comparing baseline markers, there was no significant difference between those initially randomized (n 75) and those who completed the study (n 59).
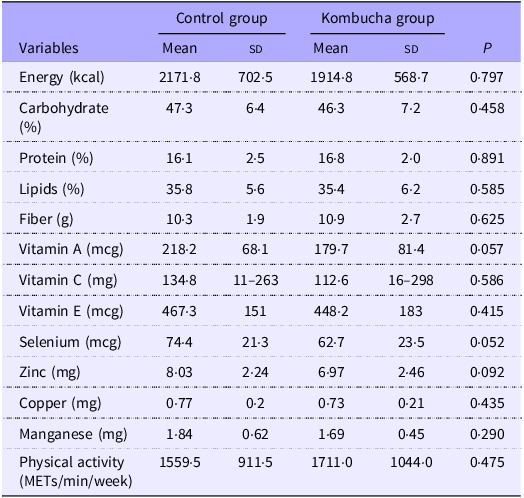
Furthermore, during the study, there was a similarity between the control and kombucha groups regarding consumption of energy, grams of carbohydrates, proteins, lipids, and fibers, as well as in relation to the level of physical activity practiced. Similarly, the consumption of micronutrients with antioxidant potential also did not differ between groups, as shown in Table 1.
Self-Reported food consumption and physical exercise practice at baseline

Values are presented as mean (standard deviation) or median (minimum–maximum value). The P-values represent the results obtained by the independent samples t test or Mann–Whitney U test. %: percentage; g: grams; kcal: kilocalories; mcg: microgram; mg: milligram; MET: Metabolic equivalent of task; min: minutes.
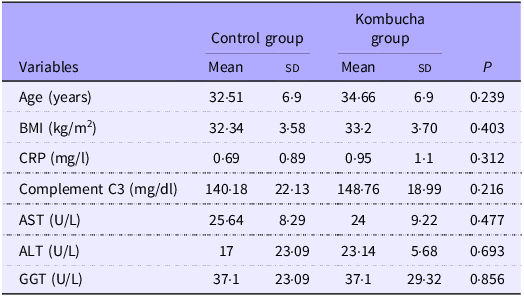
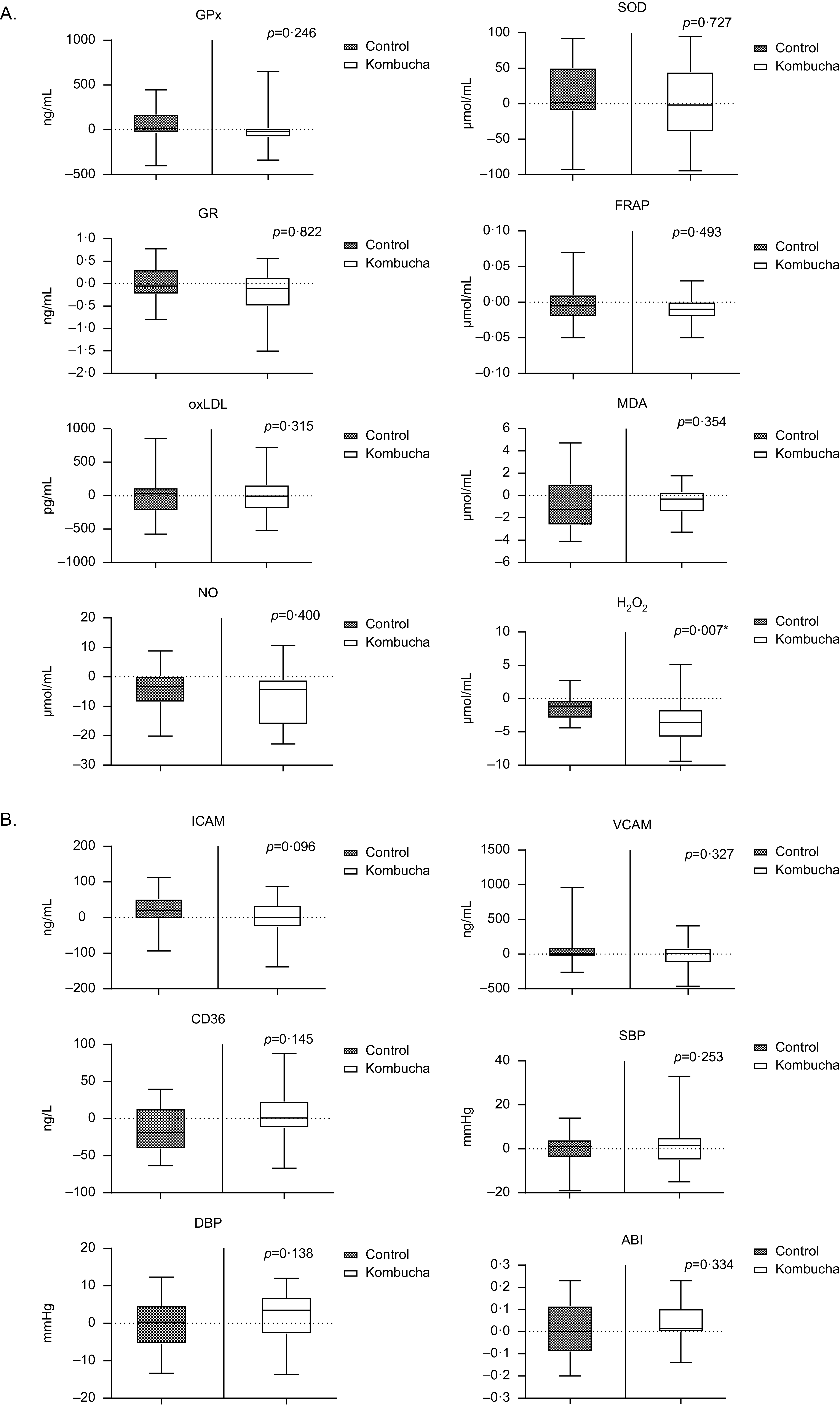
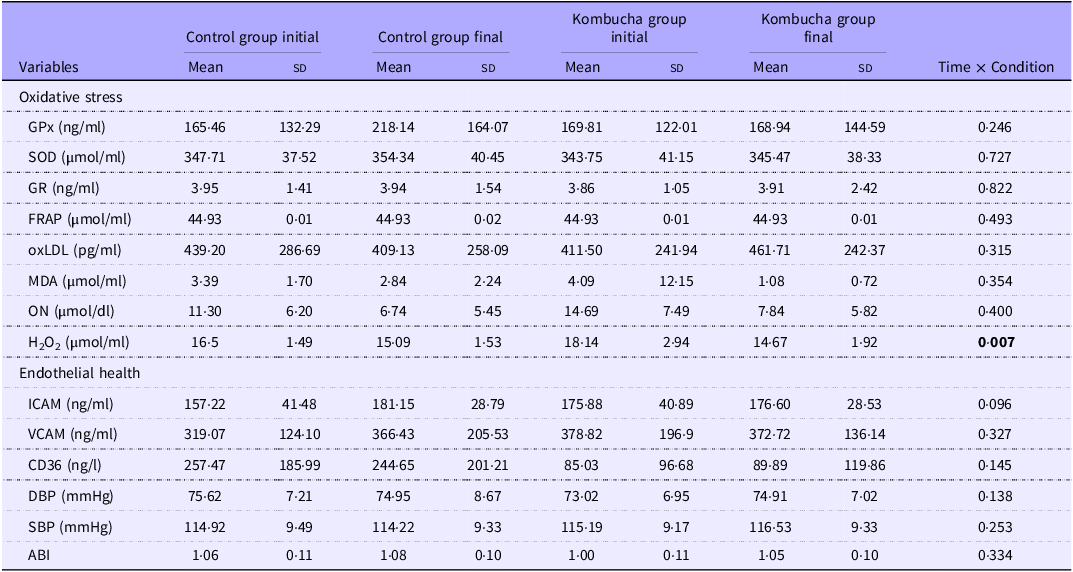
At baseline, age, BMI, inflammatory profile, and liver enzymes did not differ between groups (Table 2). Additionally, at the start of the study, the groups were similar regarding markers of oxidative stress and endothelial health. After 10 weeks of intervention, the H2O2 marker showed a significantly greater reduction (P = 0·007) in the kombucha group (18·14 v. 14·67 µmol/ml), compared to the control group (16·5 v. 15·09 µmol/ml) (Figure 2). The other markers of oxidative stress and endothelial health did not differ between the groups in the analysis of the Time × Condition interaction (Table 3).
Characteristics of participants at baseline, according to allocation group

Values are presented as mean (standard deviation) or median (minimum–maximum value). The P-values represent the results obtained by the independent samples t test or Mann–Whitney U test. ALT: alanine aminotransferase; AST: aspartate aminotransferase; BMI: body mass index; GGT: gamma-glutamyl transferase; kg: kilograms; kg/m2: kilograms per square meter; mg/l: milligrams per liter; mg/dl: milligrams per deciliter; U/L: units per liter.
Markers of oxidative stress and endothelial health in the comparison between the control and kombucha group. (a) refers to markers of oxidative stress and (b) refers to markers of endothelial function. The values presented in the graphs represent the deltas (final – initial) for both groups, whereas the P-value refers to the results of the repeated measures ANOVA for the Time × Condition interaction. ABI = ankle-brachial index; BPS = systolic blood pressure; BPD = diastolic blood pressure; CD36 = scavenger receptor B2; FRAP = iron-reducing antioxidant power; GPx = glutathione peroxidase; GR = glutathione reductase; H2O2 = hydrogen peroxide; ICAM = intracellular adhesion molecule; MDA = malondialdehyde; NO = nitric oxide; oxLDL = oxidized low-density lipoprotein; SOD = superoxide dismutase; VCAM = vascular cell adhesion molecule.

Effect of control and kombucha interventions on oxidative stress and endothelial health

Values are presented as mean (standard deviation). The term Time × Condition refers to the P–values obtained from the repeated measures ANOVA interaction effects. µmol/ml = micromole per milliliter; µmol/dl = micromole per deciliter; ABI = ankle-brachial index; CD36 = scavenger receptor B2; DBP = diastolic blood pressure; FRAP = iron-reducing antioxidant power; GPx = glutathione peroxidase; GR = glutathione reductase; H2O2 = hydrogen peroxide; ICAM = intracellular adhesion molecule; MDA = malondialdehyde; mmHg = millimeters of mercury; ng/ml = nanograms per milliliter; ng/l = nanogram per liter; NO = nitric oxide; oxLDL = oxidized low-density lipoprotein; pg/ml = picogram per milliliter; SBP = systolic blood pressure; SOD = superoxide dismutase; VCAM = vascular cell adhesion molecule.
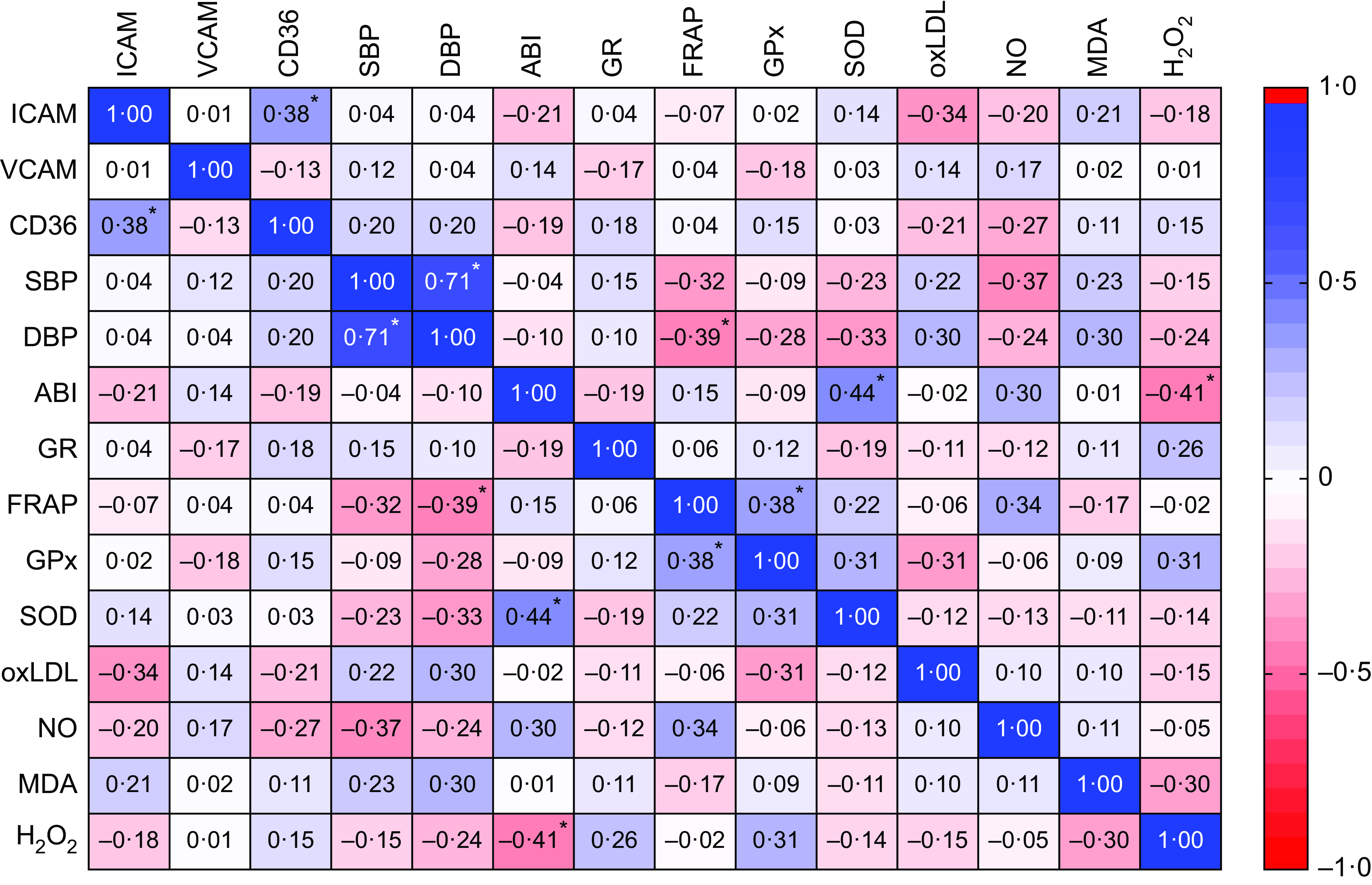
Through correlation analyses, it was possible to observe direct, moderate, and significant correlations between ICAM and CD36, SOD and ABI, and GPx and FRAP, while inverse, moderate, and significant correlations were presented between FRAP and diastolic blood pressure (DBP), and H2O2 and ABI. A direct, strong, and significant correlation was also observed between SBP and DBP (Figure 3).
Correlation matrix between markers of oxidative stress and endothelial health. The values presented are the Pearson or Spearman correlation coefficients. * Indicate statistical significance. ABI = ankle-brachial index; CD36 = scavenger receptor B2; DBP = diastolic blood pressure; FRAP = iron-reducing antioxidant power; GPx = glutathione peroxidase; GR = glutathione reductase; H2O2 = hydrogen peroxide; ICAM = intracellular adhesion molecule; MDA = malondialdehyde; NO = nitric oxide; oxLDL = oxidized low-density lipoprotein; SBP = systolic blood pressure; SOD = superoxide dismutase; VCAM = vascular cell adhesion molecule.

Discussion
This is the first clinical study specifically evaluating the effect of green tea kombucha consumption on markers of oxidative stress and endothelial health. After 10 weeks of intervention, participants in the kombucha group exhibited a significant reduction in H₂O₂ compared to the control group. However, kombucha consumption did not significantly alter other oxidative stress markers, including antioxidant enzymes and pro-oxidant radicals. Concerning endothelial health, no significant differences were observed between the groups.
The green tea used to produce kombucha has complex polyphenols that are degraded by bacterial and yeast enzymes during the fermentation process, increasing the content of phenolic compounds and increasing the bioavailability and antioxidant capacity of the beverage(Reference Bhattacharya, Gachhui and Sil46,Reference Gaggìa, Baffoni and Galiano47) . The kombucha used in this study had a total phenolic content of 0·32 mg GAE/ml (in gallic acid equivalents) and an antioxidant capacity of 3·24 μmol TE/ml. Evidence also points out that kombucha is a beverage that contains vitamin C and antioxidant minerals such as copper, manganese, and zinc, which are capable of neutralizing free radicals(Reference Júnior, Meireles Mafaldo and de Lima Brito48,Reference Costa, Vilela and Fraiz49) . This rich composition of the beverage possibly contributed to the reduction of the pro-oxidant radical H2O2.
Previous in vitro and experimental animal studies have shown the potential of kombucha for reducing oxidative stress(Reference Gaggìa, Baffoni and Galiano47,Reference Sai Ram, Anju and Pauline50–Reference Cardoso, Moreira and de Campos Costa53) , a fact justified by the presence of phenolic compounds, such as verbascoside(Reference Cardoso, Moreira and de Campos Costa53). In the present study, both groups were able to reduce H2O2. However, the kombucha group showed a significantly greater reduction in this marker. H2O2 occurs in normal metabolism and is responsible for detecting, signaling, and regulating detox in humans. Increased concentrations of this marker cause tissue and cellular damage, promoting changes in cell shape, proliferation, and recruitment of immune cells(Reference Sies54). For these reasons, H2O2 has stood out as a marker with a dual causal role in atherosclerosis induced by oxidative stress, causing damage to the vascular wall and activating the signaling of the cascade of thrombogenic events(Reference Mercier and Bäck55). Therefore, reducing this marker represents a clinically relevant benefit of kombucha, as the accumulation of this molecule is intrinsically linked to the development of obesity-related comorbidities, particularly cardiovascular diseases(Reference Lismont, Revenco and Fransen56,Reference Shimokawa57) .
Although no antioxidant enzyme studied was altered by kombucha consumption, the literature indicates that the beverage’s action against oxidative stress may occur through the inhibition of reactive oxygen and nitrogen species and also through the activation of antioxidant enzymes(Reference Yang, Ji and Zhou58). The kombucha used in this study presented the main phenolic compounds gallocatechin, catechin 5-O-gallate, epicatechin, epigallocatechin, and catechin. These compounds are capable of activating cysteine thiol oxidation of human Kelch-like ECH-associated protein 1 (KEAP-1), which causes nuclear factor erythroid 2-related factor 2 (Nrf2) to be released, causing the transcription of antioxidant enzymes to be activated(Reference Costa, Vilela and Fraiz49).
Moreover, it was possible to notice a positive effect of the energy-restricted diet on the reduction of oxidative stress markers such as NO and H2O2 in both groups. The literature is clear about the effectiveness of a healthy, properly planned, energy-restricted diet in reducing concentrations of free radicals in the human body and increasing longevity(Reference Mladenovic Djordjevic, Loncarevic-Vasiljkovic and Gonos59,Reference Green, Lamming and Fontana60) . For these reasons, energy-restricted diets are often incorporated into studies on nutritional supplements in individuals with excess body weight, as they may potentiate the beneficial effects of these interventions(Reference Darvish Damavandi, Shidfar and Najafi25,Reference Sharifi-Zahabi, Rezvani and Hajizadeh-Sharafabad61,Reference Zhao, Duan and Zhang62) . In this context, it was expected that the diet would also promote benefits to the vascular endothelium. However, ICAM and VCAM unexpectedly increased, mainly in the control group. These molecules play a fundamental role in mediating inflammation in the vascular endothelium and are increased in pathological cases of inflammation, such as obesity(Reference Singh, Kaur and Kumari63). Possibly, the participants in this study already showed a tendency to increase this marker due to the low-grade inflammation caused by the accumulation of abdominal fat and visceral adiposity. Therefore, the energy-restricted diet for 10 weeks was insufficient to minimize this impact related to excess weight.
The correlations presented between the baseline markers of the participants in this study are in line with information previously established in the literature. The ICAM and CD36 molecules showed a direct, moderate, and significant correlation, and evidence indicates that both favor the formation of atheroma plaque(Reference Shu, Peng and Hang11,Reference Singh, Kaur and Kumari63) . Furthermore, the direct, moderate, and significant association between SOD and ABI, as well as the inverse, moderate and significant association between FRAP and BPD, happens due to the already-established role of antioxidants on blood pressure(Reference Ortiz, Manriquez and Romero64,Reference Salonen, Salonen and Ihanainen65) . Similarly, the direct and significant associations of GPx and FRAP (moderate), BPS and BPD (strong) depict congruence between markers with similar functions(Reference Gawlik, Naskalski and Fedak66,Reference Thompson and McEvoy67) .
The strengths of this study include the similarity between the control and kombucha groups in terms of baseline characteristics, such as age, BMI, inflammatory profile, and also characteristics during the study, such as consumption of macronutrients and fiber, antioxidant micronutrients, and practice of physical activity. Furthermore, the control for this study was an energy-restricted diet, which is considered the gold standard intervention related to improving cardiovascular risk factors in apparently healthy individuals with excess body weight. However, this study had a limited intervention time, apparently insufficient for greater health benefits.
In conclusion, daily consumption of 200 ml green tea kombucha for 10 weeks proved effective in reducing the pro-oxidant H2O2 radical, which suggests a promising effect on the health of individuals with excess body weight. The other markers of oxidative stress and endothelial health were similar between the control and kombucha groups. As this beverage is still little studied, new clinical studies are needed to elucidate other possible beneficial effects on health.
Acknowledgments
We thank the Federal University of Viçosa, Università degli Studi di Padova, National Council for Scientific and Technological Development (CNPq), Minas Gerais State Research Support Foundation (FAPEMIG), and Coordination for the Improvement of Higher Education Personnel (CAPES - code 001) for supporting this research.
This study was funded by FAPEMIG (grant number: APQ-00035-20).
D. B. B.: Conceptualization, Methodology, Formal analysis, Investigation, Writing - original draft, Visualization. G. M. F.: Methodology, Investigation, Writing - review & editing, Visualization. U. V. L.: Methodology, Investigation. R. R. C.: Conceptualization, Investigation, Writing - review & editing. A. C. P. K.: Methodology, Investigation. V. C.: Methodology, Resources, Project administration, Funding acquisition. A. G.: Methodology, Resources, Project administration, Funding acquisition. F. A. R. B.: Conceptualization, Methodology, Resources, Writing - review & editing, Supervision, Project administration, Funding acquisition. J. B.: Conceptualization, Methodology, Resources, Writing – review & editing, Supervision, Project administration, Funding acquisition.
The authors of this article declare that there is no conflict of interest.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects/patients were approved by the National Research Ethics Commission (CAAE: 25880819.3.0000.5153; number: 6.197.412). Written informed consent was obtained from all subjects/patients. Furthermore, this study was registered in the Brazilian Clinical Trials Registry (number: RBR-9832wsx).