


Antipsychotic medications are central to treating severe mental illness (SMI), but significantly increase the risk of metabolic syndrome, such as weight gain, dyslipidaemia, type 2 diabetes and hypertension, Reference Carli, Kolachalam, Longoni, Pintaudi, Baldini and Aringhieri1 which contributes to higher mortality from heart disease and diabetes-related causes, Reference Li, Chen, Peng, Lu, Kwan and Tse2 highlighting the need to address these risks. Predicting which patients will develop severe adverse outcomes is difficult, although a weight increase of 4% or more within the first month of treatment strongly predicts long-term weight gain and metabolic risks, Reference Vandenberghe, Najar-Giroud, Holzer, Conus, Eap and Ambresin3,Reference Strassnig, Miewald, Keshavan and Ganguli4 making early weight change a key marker for timely intervention.
Management strategies include both pharmacological and non-pharmacological approaches: drugs such as ephedrine, sibutramine, orlistat and topiramate show limited benefit, Reference Faulkner and Tony5,Reference Baptista, ElFakih, Uzcátegui, Sandia, Tálamo and de Baptista6 but metformin helps regulate weight and body mass index (BMI), Reference Wu, Zhao, Guo, He, Fang and Guo7,Reference Chen, Chiu, Huang, Wu, Liu and Lu8 with greater effects when combined with non-pharmacological methods such as exercise, diet and psychological programmes. Reference Plourde and Prud’homme9 These interventions, ranging from education to motivation-enhancing programmes, Reference Verhaeghe, De Maeseneer, Maes, Van Heeringen and Annemans10,Reference Fernández-San-Martín, Martín-López, Masa-Font, Olona-Tabueña, Roman and Martin-Royo11 generally reduce weight or BMI, Reference Bruins, Jorg, Bruggeman, Slooff, Corpeleijn and Pijnenborg12 but it remains unclear which elements are most effective. Evidence suggests that the first 6 months are most critical, with a weight loss of 5–9% typically achieved then, followed by 3–6% thereafter, Reference Franz, VanWormer, Crain, Boucher, Histon and Caplan13 reinforcing the importance of early, tailored interventions for those receiving antipsychotics for SMI.
Although the UK government allocated £100 million in 2021–2022 to support weight management in the general population, 14 limited National Health Service resources and a lack of SMI-specific initiatives leave those taking antipsychotics for SMI underserved. This systematic review and meta-analysis therefore aims to identify the most effective purely non-pharmacological components for reducing weight and/or BMI in people with SMI on antipsychotic therapy, focusing on interventions within the first 6 months, when impact is greatest.
Method
Search strategy and study selection
A comprehensive literature search with no language restrictions was conducted in five databases: PubMed, Cochrane Library, CINAHL, PsycInfo and Embase. The strategy combined controlled vocabulary and keywords across four concept groups: severe mental illness (e.g. severe mental illness, schizophreni*, bipolar), antipsychotic medications (e.g. antipsychotic, anti-psychoti*), metabolic outcomes (e.g. weight, BMI, hypertension, insulin resistance, dyslipidaemia, stroke) and modifiable cardiometabolic risk factors (e.g. modifiable*, changeable risk factor). Boolean operators and truncation symbols were applied to capture variations in relevant terminology. The search covered content from the inception of each database and the last search was on 30 October 2024. Full search strings are presented in Appendix 1 of the supplementary material, available online at https://doi.org/10.1192/bjb.2026.10216.
Studies were eligible if they involved participants with a diagnosis of SMI and evaluated non-pharmacological interventions delivered alongside antipsychotic treatment. Trials using a range of antipsychotic medications were included to support a more generalised understanding of intervention effects on weight and BMI. Both randomised controlled trials (RCTs) and non-randomised controlled trials (NRCTs) with a comparator group (standard care, alternative intervention or no intervention) were eligible. Studies were required to report either weight or BMI as an outcome. Studies involving individuals prescribed antipsychotics for dementia were excluded, as current evidence is inconclusive regarding whether metabolic changes in this population are attributable to antipsychotic treatment alone. Reference Atti, Ferrari Gozzi, Zuliani, Bernabei, Scudellari and Berardi15 Similarly, studies including individuals with intellectual disabilities (also known as learning disabilities) were excluded because this group has distinct support needs and requires different approaches to non-pharmacological weight interventions, limiting direct comparability with the general SMI population. Reference Smith, Stogios, Au, Maksyutynska, De and Ji16,Reference Jinks, Cotton and Rylance17 Including dementia and intellectual disability populations would therefore reduce the applicability of lifestyle interventions and the comparability of metabolic outcomes to the broader SMI group.
Titles and abstracts were screened for eligibility by two reviewers (S.A. and S.S.) independently. Discrepancies between the reviewers were planned to be resolved via a third reviewer (H.S.), but this was not required as there were no discrepancies between reviewers. Eligible studies were then screened in full text (by S.A. and S.S.).
Risk of bias, quality assessment and level of evidence
The methodological quality of each study was assessed using the Cochrane Collaboration’s risk of bias tools, with ROBINS-I applied to NRCTs, for which it is specifically designed, and RoB 2 applied to assess risk of bias in RCTs, for which it is the recommended instrument. Reference Sterne, Hernán, Reeves, Savović, Berkman and Viswanathan18,Reference Sterne, Savović, Page, Elbers, Blencowe and Boutron19 These tools were used independently by the researchers, assigning scores for low risk of bias, high risk of bias or some concerns (Appendices 3a and 3b in the supplementary material). These results were then discussed to come to a consensus. There were also no discrepancies identified by researchers when assessing quality. Studies with rated as being at high risk of bias were assessed with caution but not excluded.
Data extraction
Data extraction was completed by two researchers (S.A. and S.S.). Data were first extracted on 30 October 2024. The data extracted included the nature of the intervention (exercise, nutrition, education, screening, monitoring and psychological components), the treatment format (group versus individual), participant characteristics (demographic data and diagnosis) and the comparison intervention. Data were extracted only for participants receiving antipsychotic treatment at the time of the intervention. Detailed information on the specific antipsychotic used, its dosage and any changes in medication during the study period was not extracted. This approach aligned with the aim of the review, which was to obtain a generalised understanding of the effects of weight or BMI reduction interventions among individuals undergoing antipsychotic therapy, rather than to analyse outcomes by specific medication type or regimen.
Statistical analysis
All data points were initially converted to metric units (lb to kg). To conduct the meta-analysis, the mean change in weight and BMI were calculated for the intervention and control groups from available data at baseline and at 6-months into the intervention. Standard deviations were calculated from the standard errors and confidence intervals. A random-effects model was used when calculating the weighted mean difference, with 95% confidence intervals (CI). Heterogeneity was quantified using the I 2-statistic to identify the level of heterogeneity between studies.
Meta-analysis was conducted specifically for BMI and weight changes. The meta-analysis compared interventions that were group based, individual based or combined (both group and individual). It also compared weight/BMI reduction between interventions that had a psychological component and those that did not. Additionally, weight/BMI reduction was compared for interventions with one component (e.g. exercise, nutrition, education, screening, monitoring, a psychological component) against interventions with more than one component if more than one interventional component was included.
Publication bias was assessed using a funnel plot. Statistical analysis was conducted using Stata version 18 for Windows 10.
Registration of protocol
This systematic review was registered with PROSPERO on 24 August 2023 (CRD42023457376) before the searches and review had been completed.
Results
Study overview
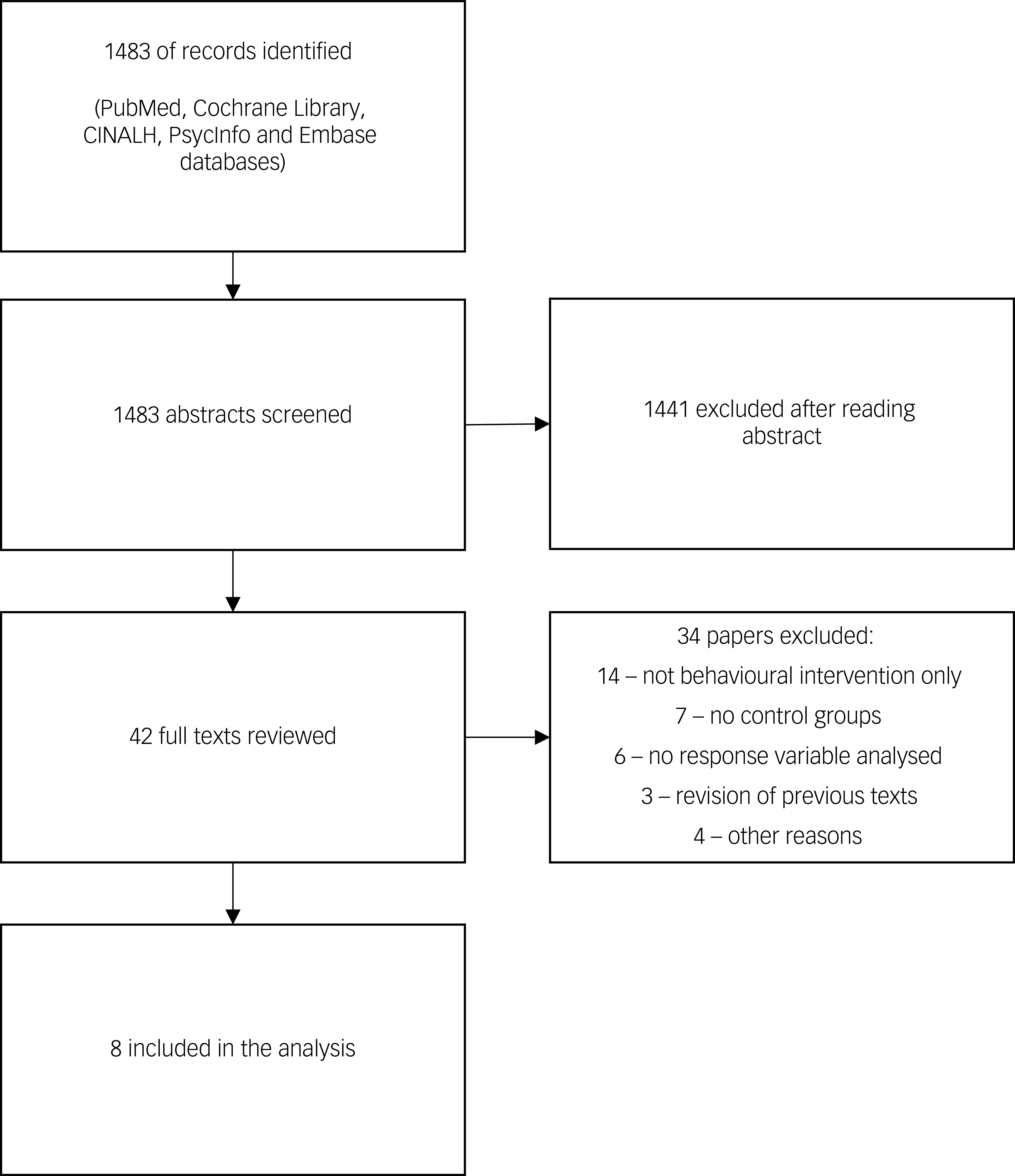
The initial search generated 1483 results from the five databases. Screening of article abstracts and references gave 42 potentially eligible studies. After full text review of these studies, eight were identified for inclusion in the analysis (Fig. 1). Seven of these Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20–Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 reported both body weight and BMI changes, and one Reference Scheewe, Backx, Takken, Jorg, van Strater and Kroes27 reported BMI change only. Five of the studies Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20,Reference Alvarez-Jimenez, Gonzalez-Blanch, Vazquez-Barquero, Perez-Iglesias, Martinez-Garcia and Perez-Pardal22,Reference Weber and Wyne25–Reference Scheewe, Backx, Takken, Jorg, van Strater and Kroes27 reported on RCTs, and the remaining three Reference Vreeland, Minsky, Menza, Rigassio Radler, Roemheld-Hamm and Stern21,Reference Poulin, Chaput, Simard, Vincent, Bernier and Gauthier23,Reference Blouin, Binet, Bouchard, Roy, Despres and Almeras24 were on NRCTs.
Selection of studies in different stages of review.

Description of the studies
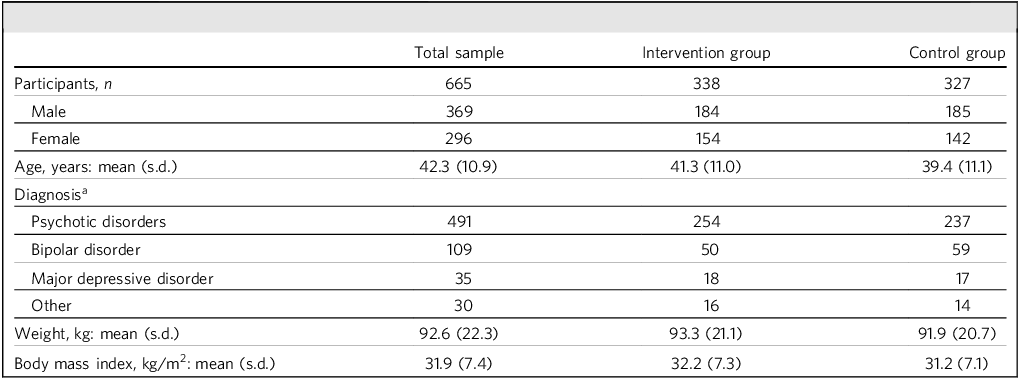
A total of 643 participants were included in the meta-analysis. All participants had a diagnosis of SMI and were receiving antipsychotic therapy. All included studies had similar population demographics, including age and gender. Participants had various SMI, such as bipolar affective disorder and psychotic disorders (schizophrenia, schizophreniform disorder, schizoaffective disorder, delusional disorder, brief reactive psychosis, or psychosis not otherwise specified) (Table 1). There were significant variations between the papers in terms of sample size and the type of intervention administered.
Demographic data for participants in the meta-analysis

a. Diagnosis shows the number of included patients receiving antipsychotic medication for the listed ICD-10 or DSM-IV diagnoses.
Nature of interventions
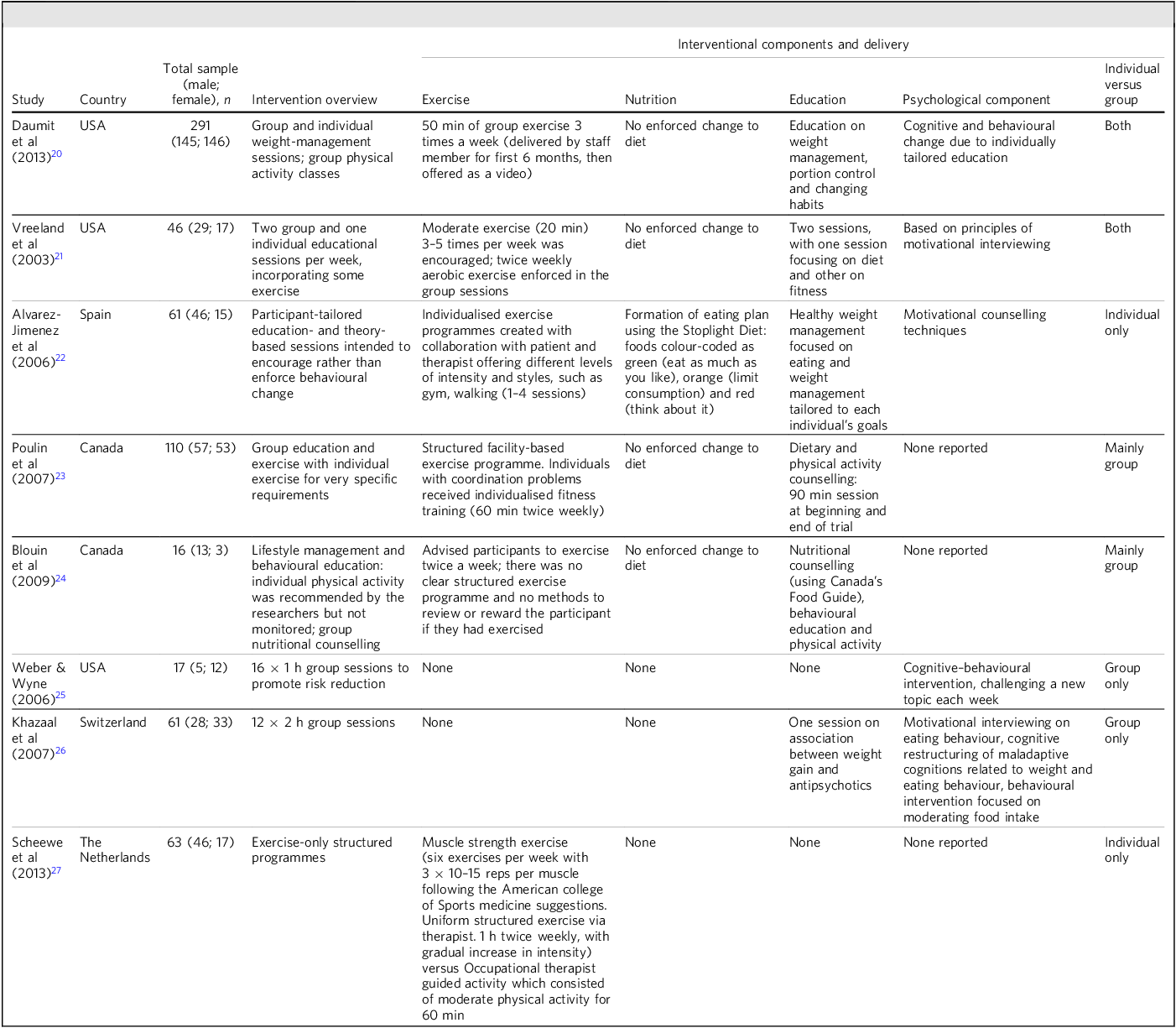
The studies were categorised based on the nature of their behavioural intervention (exercise, nutrition, education, psychological component), whether they included screening pre-intervention and monitoring other than weight and BMI, and whether they were group or individual interventions or both (Table 2). Our key findings were as follows.
Included studies and their interventional components

Finding 1: All interventions showed weight or BMI reduction
The overall findings indicated that the interventions led to some weight loss and a reduction in BMI (Fig. 2). Although some studies showed particularly strong results, such as Daumit et al Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20 (significant weight loss of −1.5 kg (95% CI −2.49 to −0.51 kg) and significant BMI reduction of −0.5 (95% CI −0.86 to −0.14)), Alvarez-Jimenez et al Reference Alvarez-Jimenez, Gonzalez-Blanch, Vazquez-Barquero, Perez-Iglesias, Martinez-Garcia and Perez-Pardal22 (significant weight loss of −2.8 kg (95% CI −4.93 to −0.67 kg) and significant BMI reduction of −0.99 (95% CI −1.71 to −0.27)), Vreeland et al Reference Vreeland, Minsky, Menza, Rigassio Radler, Roemheld-Hamm and Stern21 (significant BMI reduction of −2.2 (95% CI −4.29 to −0.11)) and Khazaal et al Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 (the highest significant BMI reduction, of −6.2 (95% CI −9.61 to −2.79)). Other studies Reference Poulin, Chaput, Simard, Vincent, Bernier and Gauthier23–Reference Weber and Wyne25,Reference Scheewe, Backx, Takken, Jorg, van Strater and Kroes27 showed some weight loss or BMI reduction, but the effects were not statistically significant due to crossing the line of effect.
Effect sizes comparing intervention group to control group on (a) weight reduction (kg) and (b) BMI reduction (kg/m2). The effect size of each study is represented by a single square (θ i) and horizontal lines are 95% CIs. The diamond represents the overall effect size of the meta-analysis (θ). The vertical line represents the line of no effect (θ 0). The weight (%) column indicates the relative contribution of each study to the overall meta-analysis.

Finding 2: Group-based interventions were more effective at BMI reduction
The analysis of weight reduction interventions based on group, individual or combined approaches showed varying results (Fig. 3). The largest pooled effect size (φ) was for individual interventions, with a reduction of φ = −2.80 kg (95% CI −4.93 to −0.67 kg), although this was based on a single study. Reference Alvarez-Jimenez, Gonzalez-Blanch, Vazquez-Barquero, Perez-Iglesias, Martinez-Garcia and Perez-Pardal22 Group interventions (n = 4 studies) Reference Poulin, Chaput, Simard, Vincent, Bernier and Gauthier23–Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 had a pooled effect size of φ = −2.73 kg (95% CI −5.64 to 0.17 kg), but this result was not statistically significant. Combined group and individual interventions (n = 2) Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20,Reference Weber and Wyne25 showed a smaller but statistically significant effect size of φ = −1.54 kg (95% −2.53 to −0.56 kg).
Effect sizes of (a) weight reduction (kg) and (b) body mass index reduction (kg/m2) between the intervention groups and control groups, further subcategorised by the method of intervention delivery. B, both group and individual interventions; G, group-only interventions; I, individual interventions. The effect size of each study is represented by a single square (θ i) and horizontal lines are 95% CIs. The diamond represents the overall effect size of the meta-analysis (θ). The vertical line represents the line of no effect (θ 0). The weight (%) column indicates the relative contribution of each study to the overall meta-analysis.

Further analysis of studies with different intervention types (group, individual or both) revealed that group interventions had the largest effect on BMI reduction (φ = −2.17 (95% CI −4.28 to −0.06)), Reference Poulin, Chaput, Simard, Vincent, Bernier and Gauthier23–Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 followed by individual interventions (φ = −0.98 (95% CI −1.69 to −0.27)). Reference Sterne, Savović, Page, Elbers, Blencowe and Boutron19,Reference Blouin, Binet, Bouchard, Roy, Despres and Almeras24 Interventions that included both group and individual components had a pooled effect size of φ = −1.03 (95% CI −2.57 to 0.51), indicating non-significant BMI reduction. Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20,Reference Vreeland, Minsky, Menza, Rigassio Radler, Roemheld-Hamm and Stern21
Finding 3: Interventions with psychological components were more effective at weight and BMI reduction
The pooled effect size for weight loss for interventions without psychological components (φ = −4.88 kg (95% CI −10.81 to 1.05 kg)) (n = 2) Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20,Reference Vreeland, Minsky, Menza, Rigassio Radler, Roemheld-Hamm and Stern21 was greater than for those with psychological components (φ = −1.78 kg (95% CI −2.65 to −0.91 kg)) (n = 5) Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20–Reference Alvarez-Jimenez, Gonzalez-Blanch, Vazquez-Barquero, Perez-Iglesias, Martinez-Garcia and Perez-Pardal22,Reference Weber and Wyne25,Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 (Fig. 4). However, the effect size for interventions with psychological components does not cross the line of no effect.
Effect sizes of (a) weight reduction (kg) and (b) body mass index reduction (kg/m2) between the intervention groups and control groups, further subcategorised by presence (Y) or absence (N) of a psychological component in the intervention. The effect size of each study are represented by a single square (θ i) and horizontal lines are 95% confidence intervals (CIs). The diamond represents the overall effect size of the meta-analysis (θ). The vertical line represents the line of no effect (θ 0). The weight (%) column indicates the relative contribution of each study to the overall meta-analysis.

When comparing BMI reduction in the studies with and without psychological components, the pooled effect size for studies without psychological components (n = 3) Reference Poulin, Chaput, Simard, Vincent, Bernier and Gauthier23,Reference Blouin, Binet, Bouchard, Roy, Despres and Almeras24,Reference Scheewe, Backx, Takken, Jorg, van Strater and Kroes27 was φ = −1.54 (95% CI −3.17 to 0.08), whereas that for with psychological components (n = 5) Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20–Reference Alvarez-Jimenez, Gonzalez-Blanch, Vazquez-Barquero, Perez-Iglesias, Martinez-Garcia and Perez-Pardal22,Reference Weber and Wyne25,Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 was φ = −1.41 (95% CI −2.59 to −0.23). The studies without psychological components showed non-significant results, as they crossed the line of no effect.
Finding 4: Interventions with more than one component showed greater BMI reduction
Further to this, the BMI meta-analysis was able to compare a group that included more than one intervention (e.g. exercise, nutrition, education, screening, monitoring, psychological component) against a group that only used one of these interventions (Fig. 5). The pooled effect of having multiple interventions (n = 6) Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20–Reference Blouin, Binet, Bouchard, Roy, Despres and Almeras24,Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 was much greater and significant (φ = −1.58; 95% CI −2.7 to −0.47) compared with having a single intervention (n = 2) Reference Weber and Wyne25,Reference Scheewe, Backx, Takken, Jorg, van Strater and Kroes27 (φ = −0.70; 95% CI −1.83 to 0.42).
Effect sizes of body mass index reduction only (kg/m2) between the intervention groups and control groups, further subcategorised by presence or absence of multiple interventional components. N, only one intervention component; Y, more than one intervention component. The effect size of each study are represented by a single square (θ i) and horizontal lines are 95% confidence intervals (CIs). The diamond represents the overall effect size of the meta-analysis (θ). The vertical line represents the line of no effect (θ 0). The weight (%) column indicates the relative contribution of each study to the overall meta-analysis.

Publication bias
The funnel plots for both BMI and weight reduction (supplementary material, Appendix 2a and 2b respectively) show some asymmetry, which was expected given that most interventions resulted in weight and BMI reduction. The funnel plot for weight reduction suggests that the studies included in the meta-analysis had effect sizes not indicative of publication bias. However, the funnel plot for BMI reduction indicated that the study by Khazaal et al Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 may be subject to publication bias. Despite this, when the meta-analysis was repeated with that study removed, the effect size for BMI reduction remained statistically significant (φ = −0.78; 95% CI −1.21 to −0.36), suggesting that the overall findings are robust.
Risk of bias
We rated five papers as having low risk of bias, Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20,Reference Alvarez-Jimenez, Gonzalez-Blanch, Vazquez-Barquero, Perez-Iglesias, Martinez-Garcia and Perez-Pardal22–Reference Blouin, Binet, Bouchard, Roy, Despres and Almeras24,Reference Scheewe, Backx, Takken, Jorg, van Strater and Kroes27 two as having some concerns Reference Weber and Wyne25,Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 and one as having moderate concerns. Reference Vreeland, Minsky, Menza, Rigassio Radler, Roemheld-Hamm and Stern21 Of the studies assessed using RoB 2, Weber & Wyne Reference Weber and Wyne25 raised some concerns owing to small sample size, unclear handling of missing outcome data, and potential lack of masking (‘blinding’). Khazaal et al Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 raised some concerns because of small sample size, potential randomisation limitations, missing outcome data and the subjective nature of outcomes (e.g. eating-related cognitions and binge-eating). Of the studies assessed using ROBINS-I, Vreeland et al Reference Vreeland, Minsky, Menza, Rigassio Radler, Roemheld-Hamm and Stern21 was rated moderate risk owing to potential confounding and selection bias of participants in the weight-management programme, because they may have been more motivated or health-oriented than controls, and non-randomised, clinic-based recruitment with self-selection raises concerns that baseline differences, rather than the intervention itself, could partly explain observed weight changes.
Discussion
Mental health services remain under pressure, so with the limited resources, it is important to establish the most cost-effective interventions. Patients on antipsychotic treatment experience the greatest reduction in weight and BMI during the first 6 months of weight management interventions, highlighting this period as a critical window for impact. Therefore, it is important to establish which weight and BMI reduction intervention works best and what combinations of components are most cost-effective.
This review highlights the benefits of non-pharmacological interventions in regulating antipsychotic-induced weight gain in people with SMI. The studies included in the current meta-analysis Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20–Reference Scheewe, Backx, Takken, Jorg, van Strater and Kroes27 show weight or BMI decrease throughout, and focus on different non-pharmacological components to achieve this loss. We found that interventions that consisted of two components, one of which was psychological, provided the greatest weight and BMI reduction within 6 months of initiating antipsychotic medication.
Role of group intervention
Our analysis reveals that the greatest effect sizes for BMI reduction were observed in people who were able to participate in group interventions. Additionally, the greatest effect size for weight reduction was seen in interventions with combined group and individual components. Studies by Daumit et al Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20 and Vreeland et al Reference Vreeland, Minsky, Menza, Rigassio Radler, Roemheld-Hamm and Stern21 yielded particularly strong results suggesting that the benefits are best when interventions adopted both group and individual components. These combined formats provide extensive contact time with instructors, which may be the critical factor in promoting weight loss or reduction in BMI.
Our findings align with previous meta-analyses, although these are on studies in the general population. Reference Abbott, Smith, Tighe and Lycett28 One possible explanation, echoed across the literature, is that group settings offer increased instructor time and foster supportive group dynamics that enhance attendance, adherence and overall engagement. Reference Poulin, Chaput, Simard, Vincent, Bernier and Gauthier23–Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 The role of such psychological factors is especially relevant for individuals with SMI, who often experience challenges in maintaining consistent participation, thereby worsening physical health outcomes. 29
Although individual interventions offer a more personalised approach, they may lack the extended exposure and peer support that group formats naturally provide. Therefore, future interventions might benefit from adopting hybrid models that integrate both group and individual components, ensuring both tailored support and sufficient instructor engagement time. This strategy could be particularly effective for people with SMI, addressing both their physical and motivational barriers to participation.
Addition on of psychological interventions
Our meta-analysis found that psychologically based interventions had a small but statistically significant impact on BMI reduction and weight loss in people with SMI treated with antipsychotics. In contrast, the benefit of non-psychological interventions, although showing some positive trends, did not reach statistical significance. The variability in outcomes across studies may be attributed to the heterogeneity in psychological methods applied, including motivational interviewing techniques, Reference Rollnick30 cognitive–behavioural therapy (CBT) or a blend of both. Although the positive trends may well be clinically significant even if they did not reach the threshold of statistical significance, it is possible that future larger studies may demonstrate statistical significance. However, recruitment into mental health studies and clinical studies is often difficult owing to the nature of the population studied and hence results need to be interpreted with that in mind.
Among the psychological interventions, the study by Khazaal et al Reference Khazaal, Fresard, Rabia, Chatton, Rothen and Pomini26 demonstrates the greatest reduction in BMI (−6.2), possibly owing to its integrated use of motivational interviewing at the outset, followed by CBT. This hybrid approach targeted maladaptive eating behaviours, binge eating and cognitive distortions related to food and body image. This suggests that interventions combining motivational strategies with structured cognitive–behavioural techniques may offer superior outcomes, although further research in larger trials is needed to confirm this.
The effectiveness of motivational counselling is reinforced by studies such as those by Vreeland et al Reference Vreeland, Minsky, Menza, Rigassio Radler, Roemheld-Hamm and Stern21 and Alvarez-Jimenez et al, Reference Alvarez-Jimenez, Gonzalez-Blanch, Vazquez-Barquero, Perez-Iglesias, Martinez-Garcia and Perez-Pardal22 both of which reported greater BMI reductions compared with control groups. These interventions emphasised the importance of assessing participants’ motivation, reinforcing behavioural change through repetition and homework, and addressing eating behaviours such as stimulus control and the speed of eating. Such findings echo broader trends reported in the literature, where motivational interviewing has demonstrated efficacy in the general population and also in primary care, with one systematic review Reference Barnes and Ivezaj31 finding that in 54.2% of primary care studies using motivational interviewing participants achieved at least 5% weight loss. However, that review did not adequately address maladaptive eating behaviours or motivational barriers specific to SMI populations.
In our review, CBT-based interventions also showed promising outcomes. Daumit et al Reference Daumit, Dickerson, Wang, Dalcin, Jerome and Anderson20 employed a model rooted in social cognitive and behavioural theories, incorporating psychiatric rehabilitation principles. Their programme, which included psychoeducation, behavioural modification and cognitive adaptations such as environmental prompts and reinforcement strategies, resulted in significant weight and BMI reduction. Notably, their approach improved treatment adherence, which is a critical challenge in SMI populations. This was consistent with a broader review of 40 RCTs that supports the role of psychoeducation in reducing psychiatric relapse and improving medication adherence. Reference Mueser, Corrigan, Hilton, Tanzman, Schaub and Gingerich32
Weber & Wyne Reference Weber and Wyne25 implemented a CBT-only intervention over 16 weeks for participants being treated with antipsychotics, using a curriculum modelled on the Diabetes Prevention Program lifestyle intervention for the general public. 33 Although the content focused effectively on self-monitoring and behaviour change, the study did not find statistically significant results, likely owing to small sample sizes. Despite this, the structured, generalisable format of the programme holds promise if adapted to the specific cognitive and motivational needs of SMI populations.
Taken together, our findings suggest that psychological interventions, especially those that integrate motivational interviewing with CBT and provide tailored, supportive environments, are more likely to produce meaningful weight-related outcomes in people with SMI. Future studies should prioritise these combined approaches, ensuring that interventions address both behavioural habits and cognitive barriers while offering sufficient intensity and duration to support lasting change.
Multiple-component as opposed to single-component interventions
Our meta-analysis found that interventions incorporating multiple components, such as exercise, nutrition, education, psychological support, screening and monitoring, were significantly more effective in reducing BMI among individuals with SMI than those using a single component. Specifically, the effect size for BMI change in multi-component interventions was large and statistically significant (φ = −1.58; 95% CI −2.7 to −0.47) compared with a non-significant effect size for single-component interventions (φ = 0.70; 95% CI −1.83 to 0.42). This strongly supports the superiority of multi-component approaches in improving weight loss outcomes in this population.
In contrast, studies using single-component interventions showed some weight and/or BMI reduction but failed to reach statistical significance. For example, Weber & Wyne’s Reference Weber and Wyne25 CBT intervention focused solely on education, and Scheewe et al Reference Scheewe, Backx, Takken, Jorg, van Strater and Kroes27 applied an exercise-only programme that emphasised mental health benefits rather than weight loss as a primary outcome. These findings suggest that although individual components may offer modest benefits, when used in isolation they are insufficient for achieving meaningful weight loss in SMI populations.
These conclusions are reinforced from broader literature. A meta-analysis of 49 RCTs involving people with type 2 diabetes reported that combining education with dietary modification led to greater BMI reductions than education alone. Reference Maula, Kai, Woolley, Weng, Dhalwani and Griffiths34 Similarly, studies in the general population show that integrated interventions (diet plus exercise) resulted in significantly higher odds of weight loss (OR = 17.5) compared with diet-only (OR = 7.2) or exercise-only (OR = 5.2) approaches. Reference Elliot and Hamlin35
Overall, these findings indicate that effective weight management interventions for individuals with SMI should include at least two core components, typically a combination of dietary, exercise, educational or psychological strategies. Future research and clinical programme design should prioritise multi-component frameworks to enhance outcomes.
Screening and other forms of monitoring
The study by Alvarez-Jimenez et al Reference Alvarez-Jimenez, Gonzalez-Blanch, Vazquez-Barquero, Perez-Iglesias, Martinez-Garcia and Perez-Pardal22 produced the most significant weight and BMI reduction among participants with SMI. A key differentiating factor in this study was its participant-centred screening process, which focused on assessing everyone’s willingness to change. Importantly, the treatment rationale was clearly explained to participants, ensuring they understood the purpose and goals of the intervention, an element largely absent from other studies in our meta-analysis.
This approach of targeting willingness to change is supported by broader research on treatment expectations. An RCT investigating individuals with depression demonstrated that outcomes were significantly improved when participants were given a treatment-congruent explanation of their illness. Specifically, those who received a psychological explanation for depression responded better to psychological treatments, whereas those who received a biological explanation responded more favourably to biological treatments. Reference Henrich, Wilhelm, Lange and Rief36 This suggests that aligning the explanation of the illness with the intended treatment can positively influence participants’ expectations and, in turn, enhance treatment outcomes.
Our findings and the existing literature highlight the importance of incorporating a clear, personalised explanation of treatment rationale in non-pharmacological interventions for weight loss in SMI populations. Doing so may strengthen participant engagement, align expectations and ultimately improve intervention effectiveness. Future programme designs should consider this strategy as a foundational component to enhance the impact of behavioural and psychological interventions.
Limitations
Across the included studies, there were only a total of 338 participants in the intervention groups and 327 participants in the control groups. Many studies, particularly in the subgroup analyses (e.g. psychological versus non-psychological interventions, group versus individual formats), had small sample sizes, resulting in limited statistical power to detect meaningful differences between intervention types. This lack of power increases the risk of type II errors and may explain why some interventions did not reach statistical significance despite showing positive trends. Reference Akobeng37 Additionally, most intervention components were evaluated in observational contexts. Future research should prioritise adequately powered RCTs with sufficient participants in each intervention subgroup to robustly evaluate the relative effectiveness of psychological versus non-psychological, and single- versus multi-component interventions.
Clinical and research implications
Interventions that were in a group format and incorporated at least two components, one of which was a psychological element, consistently yielded the most substantial improvements in weight and BMI reduction. These multifaceted, group-based approaches are particularly effective when implemented within the first 6 months of antipsychotic initiation, suggesting a critical window for early intervention. Targeting this early phase with comprehensive, psychologically informed group programmes may be essential for mitigating the metabolic side-effects of antipsychotic therapy and improving long-term physical health outcomes in individuals with SMI.
Future research should prioritise evaluating and optimising a non-pharmacological intervention that incorporates a multi-component and psychologically informed group programme, with a focus on integrating this approach into standard psychiatric care.
About the authors
Shahbaz Abdullah is an old age psychiatry higher trainee doctor with Leicestershire Partnership Trust, Leicester, UK, and Academic Clinical Fellow at the University of Leicester, UK. Elizabeta Mukaetova-Ladinska is Professor of Old Age Psychiatry in the School of Psychology and Vision Sciences, University of Leicester, UK, and an old age psychiatry consultant with Leicestershire Partnership NHS Trust, Leicester, UK. Samreen Samad is a consultant in general adult psychiatry with Leicestershire Partnership NHS Trust, Leicester, UK. Hari Subramaniam is a consultant in old age psychiatry with Leicestershire Partnership NHS Trust, Leicester, UK.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjb.2026.10216
Data availability
The data that support the findings of this study are available from the corresponding author, S.A., on reasonable request.
Author contributions
S.A. and S.S. were responsible for the initial acquisition of data. S.A., E.M.-L. and H.S. were responsible for analysis, along with the drafting of the manuscript. All authors made substantial contributions to the conception, design and interpretation of data and revising the work for important intellectual content. All approved the final version to be published and agree to be accountable for all aspects of the work in ensuring accuracy and integrity.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.







 Open access
Open access
eLetters
No eLetters have been published for this article.