


Introduction
Substance use disorders (SUDs) remain a leading cause of preventable morbidity and mortality worldwide, with opioids [1, Reference Wilson, Kariisa, Seth, Smith and Davis2], alcohol [Reference Rehm and Shield3, 4], cocaine [Reference Kariisa, Scholl, Wilson, Seth and Hoots5, Reference Peacock, Tran, Larney, Stockings, Santo and Jones6], and tobacco [7, 8] accounting for a substantial share of health loss and service utilization. Clinical interest in cannabinoids has risen rapidly alongside shifting policies and widespread real-world use [Reference Boehnke, Gangopadhyay, Clauw and Haffajee9, Reference Freeman, Hindocha, Green and Bloomfield10], yet evidence on whether cannabis or cannabinoid formulations improve SUD outcomes is mixed [Reference Black, Stockings, Campbell, Tran, Zagic and Hall11,Reference Bahji, Vazquez and Casey12]. Trials and observational studies vary markedly in exposure definitions, comparators, and outcome windows [Reference Solmi, De Toffol and Kim13], and many reports privilege short-horizon laboratory or symptom readouts that may not translate into durable clinical benefit [Reference Nielsen, Sabioni and Trigo14, Reference Metrik, Aston and Gunn15]. Outcomes across this literature are also ascertained in very different ways. Some are confirmed objectively, through biochemical testing or administrative records, while others rest on participant self-report, which is more vulnerable to recall, expectancy, and social desirability bias. Because a finding supported by objective verification carries more evidential weight than one resting on self-report alone, the method of ascertainment is itself relevant to how cannabinoid effects should be judged. At the same time, patients and addiction treatment services need pragmatic answers about whether cannabinoids reduce relapse or improve retention in treatment programs [Reference Volkow and Weiss16, Reference Hindocha, Cousijn and Ranaldi17], yet actionable, disorder-specific guidance remains limited [Reference Allan, Ramji, Perry, Ton, Beahm and Crisp18].
Previous systematic reviews have either addressed cannabinoids within broad psychiatric or health syntheses where SUDs occupied a secondary role, represented by small subsets of studies heavily skewed toward cannabis use disorder (CUD), or focused on SUDs but with fragmented evidence bases constrained to single disorders or narrow populations. None has synthesized the full breadth of human evidence across the principal SUDs within a single design-weighted framework calibrated to distinguish symptomatic targets from sustained therapeutic outcomes. Each element of this gap matters for a different reason, and each may contribute to the apparent inconsistency of the literature. Breadth across disorders is important because the contexts, mechanisms, and treatment goals of opioid, alcohol, cocaine, tobacco, and methamphetamine use disorders differ, so a cannabinoid effect present in one disorder need not generalize to another. Reviews confined to single disorders or skewed toward CUD cannot reveal such variation, and reading their conclusions side by side can make coherent patterns at the disorder level appear as unexplained disagreement. The design-weighted element matters in a different way, because studies of unequal internal validity are otherwise treated as interchangeable, even though weaker designs are more exposed to confounding and selection effects that tend to favor positive signals. When beneficial results cluster in lower-tier designs and null results in stronger ones, an unweighted reading registers the field as mixed when the discrepancy in fact tracks evidential strength. The distinction between symptomatic and sustained outcomes is no less consequential because a treatment can ease short-term symptoms without altering the longer-term course of a disorder. Where these two classes of endpoint are pooled together, a benefit on craving or withdrawal sitting alongside an absent effect on retention or abstinence reads as contradiction rather than as a coherent divergence by outcome horizon. Meanwhile, adequately powered randomized controlled trials (RCTs) within individual SUDs remain too few to define clinical efficacy independently, and the heterogeneity of the evidence base makes conventional meta-analysis unsuitable. A cross-SUD synthesis that integrates diverse designs while weighting conclusions by evidential strength can therefore yield a more clinically informative picture than any prior review.
We, therefore, synthesized human studies encompassing opioid, alcohol, cocaine, tobacco, and methamphetamine use disorders to determine whether cannabis or specific cannabinoid formulations confer clinically meaningful benefit across SUDs. Studies were classified and interpreted according to design quality and internal validity, and results were organized by SUD endpoint so that stronger designs and sustained therapeutic outcomes informed the overall conclusions. This endpoint-centered, tiered structure preserves methodological transparency and enables inferences that inform clinical practice while acknowledging where mechanistic or intermediate signals point to plausible pathways that require confirmatory trials targeting sustained clinical outcomes.
Methods
Search strategy and selection criteria
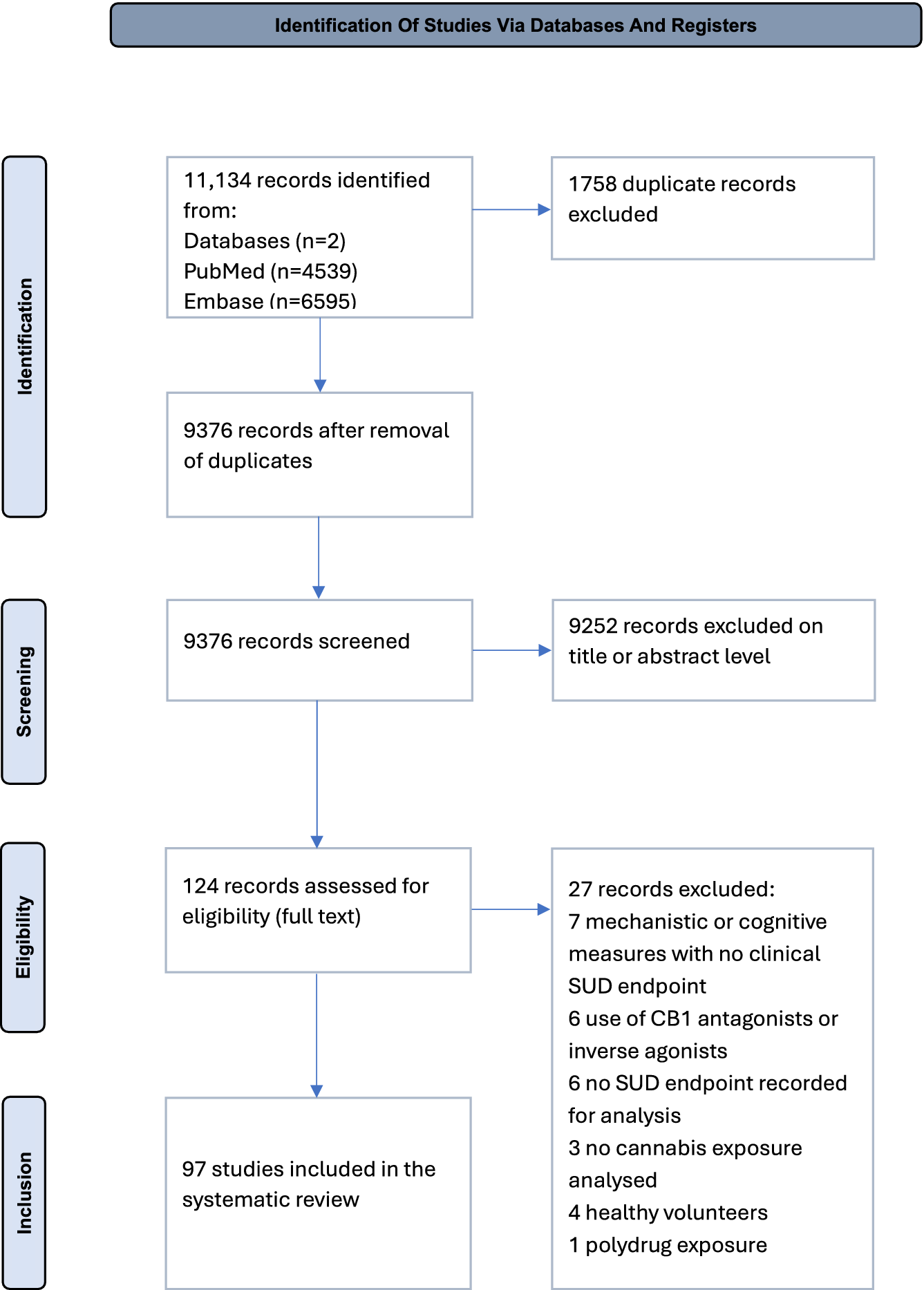
We conducted a systematic review aligned with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow19], with a structured narrative synthesis following Synthesis Without Meta-analysis (SWiM) guidance [Reference Campbell, McKenzie, Sowden, Katikireddi, Brennan and Ellis20]. The protocol was prospectively registered with PROSPERO (CRD420251151193). Searches covered PubMed and Embase from 1 January 1975 to 30 June 2025. These two databases were selected because they jointly provide near-complete coverage of the biomedical and clinical addiction literature, complemented by the additional backward and forward citation searching undertaken for all included records. Full strategies, field tags, and de-duplication procedures are reported in the Supplement. Two reviewers (DZD, AAZD) independently screened titles and abstracts, followed by full-text screening in duplicate. Inter-rater reliability for eligibility decisions was high (Cohen’s κ = 0.88, 96.0% agreement), and remaining disagreements were resolved by consensus. Trial registries were checked for ongoing or unpublished trials. No language restrictions were applied. Translations were arranged when required. No artificial intelligence tools were used at any stage of searching, screening or data extraction. In total, 124 full-text articles were assessed for eligibility, and 97 studies were included (Figure 1).
PRISMA 2020 flow diagram for the systematic review. PubMed: 4,539 records; Embase: 6,595 records; total: 11,134; duplicates removed: 1,758; records screened: 9,376; records excluded: 9,252; full-text articles assessed: 124; articles excluded with reasons: 27; studies included: 97.

Figure 1. Long description
The flowchart is organized into four vertical stages labeled on the left.
1. Identification: The top box shows 11,134 records identified from two databases: PubMed (n=4539) and Embase (n=6595). An arrow points right to a box indicating 1,758 duplicate records were excluded. A downward arrow leads to a box with 9,376 records remaining after duplicate removal.
2. Screening: A downward arrow leads to a box showing 9,376 records screened. An arrow points right to a box indicating 9,252 records were excluded at the title or abstract level.
3. Eligibility: A downward arrow leads to a box showing 124 records assessed for eligibility via full text. An arrow points right to a box listing 27 records excluded for specific reasons: 7 for mechanistic or cognitive measures with no clinical S U D endpoint, 6 for use of C B 1 antagonists or inverse agonists, 6 for no S U D endpoint recorded for analysis, 3 for no cannabis exposure analyzed, 4 for healthy volunteers, and 1 for polydrug exposure.
4. Inclusion: A final downward arrow leads to the bottom box indicating 97 studies were included in the systematic review.
Eligible studies were original human research evaluating cannabis or cannabinoids as a specific exposure in relation to clinically relevant outcomes for SUDs. We considered randomized and non-randomized interventional designs and observational designs, provided that cannabis exposure was analyzed as a distinct variable rather than embedded in an undifferentiated illicit drugs composite. Observational eligibility was not restricted by subtype, and case–control designs were therefore admissible. One identified study [Reference Li, Milivojevic, Constable and Sinha21] carried a case–control descriptor and was the only study so described. Because its groups were defined by cannabis exposure status rather than by outcome, and all measures were obtained concurrently at a single time point, it constitutes an analytical cross-sectional comparison rather than a case–control study in the epidemiological sense. It was accordingly classified within the cross-sectional stratum and appraised with the Joanna Briggs Institute (JBI) analytical cross-sectional tool. Studies without a cannabis-specific analysis were excluded. Where reports addressed several substances, a study was included for a given SUD only if that SUD had an analyzable cannabis-SUD endpoint association. We excluded animal and in-vitro studies, studies centered on cannabinoid receptor type 1 (CB1) antagonists or inverse agonists, healthy-volunteer experiments lacking SUD relevance, studies reporting only cognitive or laboratory measures without SUD endpoints, studies in which cannabis exposure could not be separated from polydrug exposure, narrative reviews, editorials, and protocols. When multiple publications described the same cohort, we linked them at the cohort level to avoid double counting.
Outcomes and data extraction
Primary outcomes, prespecified and coded uniformly across designs following the SUD framework, were treatment retention, relapse, abstinence, craving, withdrawal severity, and consumption. Each outcome was mapped to its target SUD. Laboratory or mechanistic readouts were recorded for context but did not determine study-level efficacy unless designated as primary clinical endpoints by the original authors. For interventional trials, we extracted allocation, masking, intervention, comparator, timing, and outcome definitions. For observational studies, we captured the exposure definition and verified that cannabis was modeled as a separate exposure. Two reviewers (DZD, AAZD) independently extracted data with a piloted form and cross-checked entries. Inter-rater reliability for the coding of eligible studies was high (Cohen’s κ 0.84, 90.2% agreement), and discrepancies were resolved by discussion. Extracted items included study identifiers, setting and population, design, sample size, SUD category, exposure and outcome definitions, verification methods, follow-up duration, and statistical approach.
Data analysis
Given substantial heterogeneity in design, exposure definitions, comparators, and timing, meta-analysis was not undertaken. Instead, synthesis proceeded narratively using prespecified disorder and endpoint strata. To retain quantitative detail without pooling incommensurable estimates, the effect sizes and confidence intervals reported by individual studies, where available, are compiled at the study level in a supplementary table organized by disorder and endpoint. Direction-of-effect classifications, reported as Beneficial, No Significant Effect, Mixed/Partial, or Harmful/Inferior, were applied consistently across studies, and findings were integrated within an endpoint-centered framework that incorporates design-based weighting for figures and summaries. Where studies reported on participants who used more than one substance, we extracted and synthesized the analysis isolating cannabis exposure from the other substances, in order to minimize confounding from polysubstance use.
To enhance interpretability across heterogeneous designs, we applied a tier-weighting framework, where each study received a base weight by tier type: RCT (1.00), prospective cohort (0.70), retrospective cohort (0.60), cross-sectional (0.45), case series (0.35), and qualitative (0.25). These values reflect the conventional evidence hierarchy [Reference Murad, Asi, Alsawas and Alahdab22], with decrements calibrated to the progressive loss of internal validity from randomization through self-selected exposure to cross-sectional measurement. The specific weights were compiled by the authors for this review and have not been formally validated as an instrument. They function as ordinal scaling aids for synthesis and figure construction, not as probability-based analytic weights, and do not replace study-level results. For each disorder and endpoint, the tier-weighted total within a direction-of-effect category was obtained by assigning each contributing endpoint instance the base weight of its study design and summing these weights across the instances in that category. Raw instance counts were retained alongside these totals and, to enable comparison across disorders, the direction-of-effect distribution within each disorder was additionally expressed as a percentage of that disorder’s total endpoint instances. We mapped designs to risk of bias (RoB) tools, applying RoB 2 to RCTs [Reference Sterne, Savović, Page, Elbers, Blencowe and Boutron23], Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I) to non-randomized comparative and cohort studies [Reference Sterne, Hernán, Reeves, Savović, Berkman and Viswanathan24], JBI Cross-Sectional to analytical cross-sectional studies [Reference Moola, Munn, Tufanaru, Aromataris, Sears, Sfetcu, Aromataris and Munn25], JBI Case Series to case series [Reference Munn, Barker, Moola, Tufanaru, Stern and McArthur26], and JBI Qualitative to qualitative designs [Reference Lockwood, Munn and Porritt27]. Confidence in the evidence for each disorder and endpoint was summarized using a simplified assessment appropriate to narrative synthesis without pooling, combining the strength of the contributing study designs, the risk of bias, and the consistency of the direction of effect, and it is reported with the risk of bias assessments in the Supplement [Reference Campbell, McKenzie, Sowden, Katikireddi, Brennan and Ellis20, Reference Murad, Asi, Alsawas and Alahdab22]. Where overlapping cohorts produced multiple reports, we kept analytically distinct, non-overlapping outcomes while assigning cohort-level participant counts to the most comprehensive report.
Role of the funding source
None to declare.
Results
After full-text assessment of 124 records, 97 studies met inclusion criteria (Figure 1), describing 41,954 unique participants (35.1% female). Publications spanned 1991–2025 and comprised 17 RCTs, 31 prospective cohort studies, 16 retrospective cohort studies, 20 cross-sectional studies, 4 case reports, and 9 qualitative studies (Table 1). These 97 studies contributed 195 endpoint instances across the six prespecified SUD endpoints. Of these, 89 (45.6%) were classified as Beneficial, 80 (41.0%) as No Significant Effect, 12 (6.2%) as Mixed/Partial, and 14 (7.2%) as Harmful/Inferior.
Characteristics of included studies

Table 1. Long description
The table is organized into seven columns: Study, Study design, Sample size (female percentage), Mean age (S D) in years, Form, dose, route, Direction-of-effect: S U D endpoint (S U D), and Outcome.
Key entries include:
* Gossop et al. [28]: Cross-sectional retrospective survey of 50 participants (30% female). Outcome: Mixed/Partial effect on withdrawal severity in O U D. 22 participants used cannabis; 12 reported it made withdrawal worse, 6 said it reduced distress.
* Saxon et al. [29]: Retrospective analysis of 98 participants (0% female). Outcome: No significant effect on abstinence or retention in O U D.
* Wasserman et al. [33]: Prospective observational study of 74 participants (40.5% female). Outcome: Harmful/Inferior effect on relapse in O U D. Baseline cannabis use significantly increased heroin lapse risk.
* Best et al. [34]: Cross-sectional survey of 200 participants (30% female). Outcome: Beneficial effect on consumption in O U D. Daily users reported fewer days of heroin use.
* Labigalini et al. [35]: Prospective case series of 25 participants (0% female). Outcome: Beneficial effect on abstinence, craving, and withdrawal in Co U D. 68% ceased crack use.
* Dreher [37]: Qualitative ethnographic study of 33 females (100%). Outcome: Beneficial effect on craving, relapse, and abstinence in Co U D. 92.8% attributed stopping crack use to ganja.
* Morgan et al. [59]: R C T pilot of 24 participants (50% female) using C B D inhalers. Outcome: Beneficial effect on consumption in T U D. C B D group reduced cigarettes by approximately 40%.
* Hurd et al. [88]: R C T of 42 participants (16.7% female) using Epidiolex. Outcome: Beneficial effect on craving in O U D. Lower cue-induced craving persisting 7 days post-dose.
* Lake et al. [110]: Prospective cohort of 1389 participants (41% female). Outcome: Beneficial effect on consumption in O U D. Daily cannabis use buffered the risk of daily opioid use associated with low methadone doses.
Abbreviations used: S U D (substance use disorder), O U D (opioid use disorder), A U D (alcohol use disorder), Co U D (cocaine use disorder), T U D (tobacco use disorder), M U D (methamphetamine use disorder), N A (not available), N S (not significant).
Abbreviations: SUD, substance use disorder; OUD, opioid use disorder; AUD, alcohol use disorder; CoUD, cocaine use disorder; TUD, tobacco use disorder; MUD, methamphetamine use disorder. NA, not available. NS, not significant. HR, hazard ratio. OR, odds ratio.
a Calculated on 176 first admission patients, excluding 20 re-entering.
b Median (IQR)
Of the 17 RCTs, 12 were rated low risk of bias on RoB 2, 4 raised some concerns, and 1 was rated high risk (eFigures 1a–h). Among the 47 cohort studies assessed with ROBINS-I, 11 were rated low risk, 27 moderate, 7 serious, and 2 critical, with bias due to confounding the most frequently flagged domain. Of the 33 studies assessed with JBI checklists (20 cross-sectional, 4 case series, 9 qualitative), 21 were rated as low concern, 11 as moderate concern, and 1 as high concern.
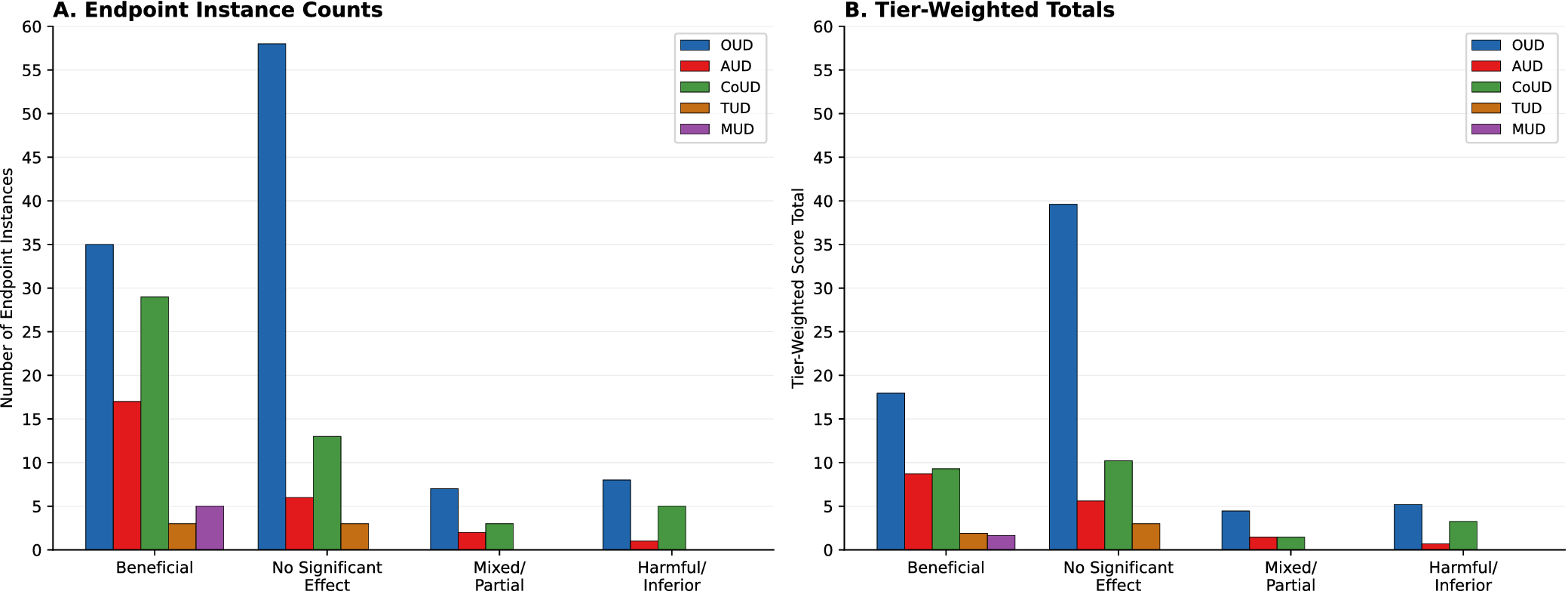
Opioid use disorder (OUD) dominated the evidence base, contributing 108 of 195 endpoint instances (55.4%), followed by cocaine use disorder (CoUD; 50, 25.6%), alcohol use disorder (AUD; 26, 13.3%), tobacco use disorder (TUD; 6, 3.1%), and methamphetamine use disorder (MUD; 5, 2.6%). Nine studies contributed to more than one SUD, and 49 contributed to more than one endpoint instance. The distribution of direction-of-effect categories varied markedly by disorder (Figure 2; Table 2). Most No Significant Effect instances arose in OUD (58/80; 72.5%), and OUD also accounted for the largest share of Harmful/Inferior instances (8/14; 57.1%). In contrast, for all other SUDs, Beneficial classifications outnumbered non-Beneficial ones, predominantly accounted for by short-term SUD endpoints craving, withdrawal severity, and consumption. For MUD, all five instances were Beneficial, though numbers were small. Expressed as a percentage of each disorder’s total endpoint instances, the direction-of-effect distributions were directly comparable across disorders (full distributions in Table 2). No Significant Effect predominated only in OUD, at 53.7% of its instances, against 23.1% in AUD and 26.0% in CoUD. Beneficial classifications represented 65.4% of AUD, 58.0% of CoUD, and all five MUD instances, compared with 32.4% in OUD, while TUD was evenly split at 50.0%.
SUD endpoint instance counts and tier-weighted totals by direction-of-effect category and substance use disorder. Panel A shows raw endpoint instance counts; Panel B shows tier-weighted score totals. SUD indicates substance use disorder; OUD, opioid use disorder; AUD, alcohol use disorder; CoUD, cocaine use disorder; TUD, tobacco use disorder; MUD, methamphetamine use disorder.

Figure 2. Long description
Panel A, titled Endpoint Instance Counts, has a y-axis labeled Number of Endpoint Instances ranging from 0 to 60. The x-axis lists four categories: Beneficial, No Significant Effect, Mixed forward slash Partial, and Harmful forward slash Inferior. Each category contains a cluster of five colored bars representing O U D in blue, A U D in red, Co U D in green, T U D in orange, and M U D in purple. In the Beneficial category, O U D is highest at 35, followed by Co U D at 29. In the No Significant Effect category, O U D peaks at 58.
Panel B, titled Tier-Weighted Totals, has a y-axis labeled Tier-Weighted Score Total ranging from 0 to 60. The x-axis categories and legend remain the same as Panel A. The overall trends are similar but the magnitudes are lower. In the Beneficial category, O U D is approximately 18, while Co U D and A U D are around 9. In the No Significant Effect category, O U D remains the highest peak at approximately 40. For both panels, T U D and M U D consistently show the lowest counts and scores across all effect categories.
SUD endpoint instances and tier score totals, with breakdown per direction-of-effect category and SUD endpoints for each SUD

Table 2. Long description
The table is organized into four primary sections based on direction-of-effect. Each section lists six endpoints: Retention, Relapse, Abstinence, Craving, Withdrawal, and Consumption, followed by a section total.
1. Beneficial Effect Section:
- O U D: Total n = 35, Sigma Tier = 17.95. Highest endpoint is Craving (n = 11, Sigma Tier = 6).
- A U D: Total n = 17, Sigma Tier = 8.7. Highest endpoint is Consumption (n = 5, Sigma Tier = 2.8).
- Co U D: Total n = 29, Sigma Tier = 9.3. Highest endpoint is Craving (n = 10, Sigma Tier = 2.8).
- T U D: Total n = 3, Sigma Tier = 1.9.
- M U D: Total n = 5, Sigma Tier = 1.65.
2. No Significant Effect Section:
- O U D: Total n = 58, Sigma Tier = 39.6. Highest endpoint is Retention (n = 20, Sigma Tier = 13.6).
- A U D: Total n = 6, Sigma Tier = 5.6.
- Co U D: Total n = 13, Sigma Tier = 10.2.
- T U D: Total n = 3, Sigma Tier = 3.
- M U D: Total n = 0, Sigma Tier = 0.
3. Mixed/Partial Effect Section:
- O U D: Total n = 7, Sigma Tier = 4.45.
- A U D: Total n = 2, Sigma Tier = 1.45.
- Co U D: Total n = 3, Sigma Tier = 1.45.
- T U D and M U D: All values are 0.
4. Harmful/Inferior Effect Section:
- O U D: Total n = 8, Sigma Tier = 5.2.
- A U D: Total n = 1, Sigma Tier = 0.7.
- Co U D: Total n = 5, Sigma Tier = 3.25.
- T U D and M U D: All values are 0.
Abbreviations used: O U D (Opioid Use Disorder), A U D (Alcohol Use Disorder), Co U D (Cocaine Use Disorder), T U D (Tobacco Use Disorder), M U D (Methamphetamine Use Disorder).
Abbreviations: n, number of SUD endpoint instances; ΣTier, tier score total. Tier weights: RCT (1.00), prospective cohort (0.70), retrospective cohort (0.60), cross-sectional (0.45), case series (0.35), qualitative (0.25).
Abbreviations: OUD, opioid use disorder; AUD, alcohol use disorder; CoUD, cocaine use disorder; TUD, tobacco use disorder; MUD, methamphetamine use disorder.
Tier-weighted totals (Figure 2B) recalibrated the apparent distribution of findings. In OUD, the Beneficial tier-weighted sum (17.95) was substantially lower than the No Significant Effect sum (39.60), because the Beneficial signal derived partly from lower-tier designs whose contributions were proportionally reduced. The same pattern was visible across all SUDs when raw counts (Figure 2A) were compared with tier-weighted totals (Figure 2B). In AUD, however, the Beneficial sum (8.70) still exceeded No Significant Effect (5.60) after weighting, suggesting a more robust symptomatic signal. In CoUD, the balance shifted. Raw Beneficial instances outnumbered No Significant Effect (29 vs. 13), but tier-weighted totals reversed this (9.30 vs. 10.20), indicating that much of the CoUD Beneficial signal came from lower-evidence designs. TUD (1.90 Beneficial, 3.00 No Significant Effect) and MUD (1.65 Beneficial, all weighted evidence) contributed few but directionally notable instances.
The 195 SUD endpoint instances comprised 29 retention, 23 relapse, 31 abstinence, 46 craving, 36 withdrawal severity, and 30 consumption. Two patterns were consistent across SUDs (Table 2; Figure 3). Patient-reported symptom endpoints, craving and withdrawal severity, displayed the highest Beneficial counts, with craving contributing 46 instances and withdrawal severity 36, the majority classified Beneficial. The highest Beneficial peaks arose from craving, withdrawal severity, and consumption in OUD, AUD, and CoUD. In contrast, retention, relapse, and abstinence aggregated in non-Beneficial categories. Within OUD, retention showed marked No Significant Effect dominance (Beneficial: 2, 1.30; No Significant Effect: 20, 13.60; Mixed/Partial: 1, 0.70; Harmful/Inferior: 4, 2.50). Abstinence (Beneficial: 4, 1.75; No Significant Effect: 13, 8.30; Mixed/Partial: 2, 1.40; Harmful/Inferior: 1, 0.70) and relapse (Beneficial: 2, 0.70; No Significant Effect: 6, 4.10; Mixed/Partial: 1, 0.45; Harmful/Inferior: 3, 2.00) demonstrated the same pattern. Unlike in OUD, CoUD, and TUD, cannabinoid exposure studies in AUDs presented a higher tier total score for Beneficial (8.70) than for No Significant Effect (5.60). In CoUD, SUD endpoints were higher by instance count in the Beneficial category, 29, however, when considering tier scores, the No Significant Effect direction-of-effect registered the highest total value (10.20).
Tier-weighted SUD endpoint total scores grouped by direction-of-effect category (A, Beneficial; B, No Significant Effect; C, Mixed/Partial; D, Harmful/Inferior), color-coded by substance use disorder.

Figure 3. Long description
A four-panel set of bar charts labeled A through D. Each chart shares a Y-axis titled Tier-Weighted Score Total ranging from 0.0 to 14.0 in increments of 0.5. The X-axis lists six endpoint categories: Retention, Relapse, Abstinence, Craving, Withdrawal Severity, and Consumption. A legend in each panel identifies five substance use disorders: O U D in blue, A U D in red, C o U D in green, T U D in orange, and M U D in purple.
* Panel A, Beneficial: O U D shows the highest scores in Craving at 6.0 and Withdrawal Severity at 5.0. Other categories remain below 3.5.
* Panel B, No Significant Effect: This panel contains the highest overall values. O U D peaks at 13.5 for Retention and 8.3 for Abstinence. Craving and Withdrawal Severity for O U D are around 4.3 and 6.0 respectively.
* Panel C, Mixed or Partial: All scores are significantly lower, with no bar exceeding 1.5. O U D and A U D show small peaks in Craving and Abstinence.
* Panel D, Harmful or Inferior: Scores are also low, with O U D peaking at 2.5 for Retention and 2.0 for Relapse. C o U D shows values between 1.0 and 1.5 for Craving and Withdrawal Severity.
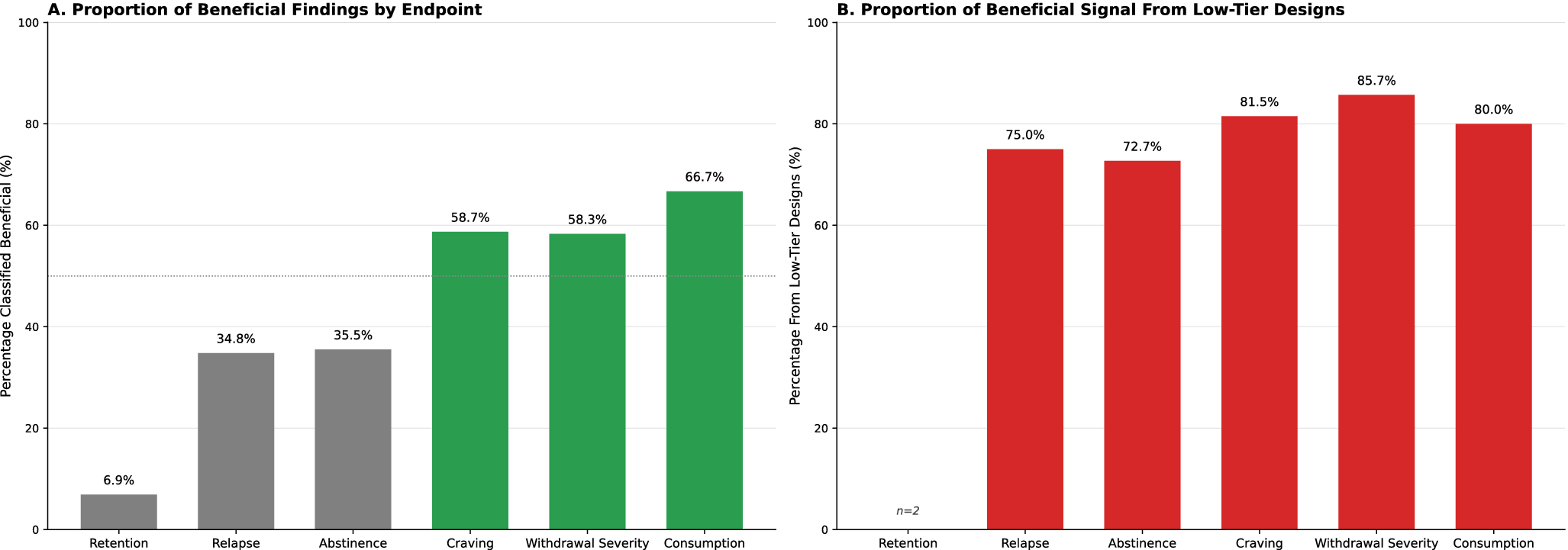
Across designs, outcome verification varied from objective measures to self-report. Objective verification, using biochemical testing or administrative records, was most common for the three sustained outcome endpoints, namely retention, relapse, and abstinence. For each of these SUD endpoints, the majority of instance counts were classified in non-Beneficial direction-of-effect categories (retention: 27/29 [93.1%]; relapse: 15/23 [65.2%]; abstinence: 20/31 [64.5%]) (Table 2), and nearly all of these non-Beneficial findings were extracted from higher-tier designs, including RCTs, prospective and retrospective studies (retention: 27/27 [100%]; relapse: 14/15 [93.3%]; abstinence: 18/20 [90.0%]) (Table 1). The inverse is noticeable for shorter-term SUD endpoints that deal with a more immediate context post-intervention. A higher percentage of studies for craving, withdrawal severity, and consumption report SUD endpoint instance counts that cluster in the Beneficial category (craving: 27/46 [58.7%]; withdrawal severity: 21/36 [58.3%]; consumption: 20/30 [66.7%]), but the overwhelming majority are derived from low-evidence studies, including qualitative, cross-sectional, and case studies (craving: 22/27 [81.5%]; withdrawal severity: 18/21 [85.7%]; consumption: 16/20 [80.0%]). This inverse relationship between endpoint horizon and evidence tier is a defining feature of the data set (Figure 4). The outcomes for which cannabinoids appear most consistently beneficial are precisely those supported by the weakest designs, while the outcomes most relevant to sustained recovery are evaluated by stronger designs that predominantly find no effect.
Evidence quality gradient across SUD endpoints. Panel A shows the proportion of endpoint instances classified as Beneficial for each of the six prespecified endpoints, with bars colored green where most instances were Beneficial (above the 50% reference line) and gray where fewer than half were Beneficial. Panel B shows the proportion of those Beneficial findings derived from lower-tier designs (cross-sectional, case series, and qualitative), shown in red. Retention is based on only two Beneficial instances (n = 2).

Figure 4. Long description
A two-panel figure analyzing S U D endpoints.
Panel A, titled Proportion of Beneficial Findings by Endpoint, has a y-axis labeled Percentage Classified Beneficial percent ranging from 0 to 100. A horizontal dashed reference line is at 50 percent. Six bars from left to right are:
* Retention: 6.9 percent (gray)
* Relapse: 34.8 percent (gray)
* Abstinence: 35.5 percent (gray)
* Craving: 58.7 percent (green)
* Withdrawal Severity: 58.3 percent (green)
* Consumption: 66.7 percent (green)
Panel B, titled Proportion of Beneficial Signal From Low-Tier Designs, has a y-axis labeled Percentage From Low-Tier Designs percent ranging from 0 to 100. Six bars from left to right are:
* Retention: No bar shown, labeled with n equals 2
* Relapse: 75.0 percent (red)
* Abstinence: 72.7 percent (red)
* Craving: 81.5 percent (red)
* Withdrawal Severity: 85.7 percent (red)
* Consumption: 80.0 percent (red)
Discussion
This review set out to determine whether cannabis or specific cannabinoid formulations confer clinically meaningful benefit across opioid, alcohol, cocaine, tobacco, and methamphetamine use disorders, classifying studies by design quality and organizing findings by endpoint so that stronger designs and sustained outcomes carried the greatest weight in the conclusions. Against that aim, the central finding is a consistent divergence between symptomatic and sustained therapeutic outcomes of cannabinoid exposure across SUDs. Short-term endpoints (craving, withdrawal severity, and consumption) cluster in the Beneficial direction with comparatively higher tier-weighted totals, while long-term endpoints (retention, relapse, and abstinence) predominantly populate the No Significant Effect category, most strikingly in OUD (Figures 2–4; Table 2). This divergence reflects the inverse relationship between endpoint horizon and evidence tier established in the Results, whereby the most consistent benefits attach to the outcomes assessed by the weakest designs. Together, these findings support a cautious interpretation. Cannabinoid strategies may improve short-horizon symptoms but the current evidence base does not demonstrate that such improvement translates into durable changes in treatment trajectory.
In OUD, where the evidence base is largest, the asymmetry between short-term and long-term SUD endpoints is especially clear, with the heaviest No Significant Effect weights falling on retention and abstinence and exceeding the corresponding symptomatic weights (Table 2). Several methadone and clinic cohorts that verified exposure by urinalysis and tracked administrative retention found no association between cannabis use and illicit opioid use or treatment retention once core clinical covariates were included. In these analyses, cannabis coefficients typically attenuated to null or fluctuated inconsistently after adjustment for factors such as opioid agonist dose, baseline severity, and visit adherence [Reference Saxon, Calsyn, Greenberg, Blaes, Haver and Stanton29, Reference Budney, Bickel and Amass32, Reference Epstein and Preston38, Reference Weizman, Gelkopf, Melamed, Adelson and Bleich39, Reference Scavone, Sterling, Weinstein and Van Bockstaele61, Reference Bisaga, Sullivan, Glass, Mishlen, Pavlicova and Haney67, Reference Håkansson, Widinghoff, Abrahamsson and Gedeon75, Reference Klimas, Nosova, Socías, Nolan, Brar and Hayashi85, Reference Naji, Rosic, Sanger, Dennis, Hillmer and Hudson105]. Consistently, across OUD studies, dose, treatment assignment, and engagement emerged as the dominant drivers of retention and abstinence, and the apparent cannabis signal diminished when these determinants were modeled explicitly [Reference Peles, Schreiber and Adelson42, Reference Chaudhry, Umeed, De Silva, Al-Adwani, Sultan and Alam54, Reference Hill, Bennett, Griffin, Connery, Fitzmaurice and Subramaniam57, Reference Abrahamsson, Widinghoff, Lilliebladh, Gedeon, Nilvall and Hakansson66, Reference Levine, Lundahl, Ledgerwood, Lisieski, Rhodes and Greenwald71, Reference Peles, Schreiber, Sason and Adelson86, Reference Shulman, Choo, Ohrtman, Pavlicova, Rotrosen and Nunes122]. Relapse in OUD demonstrated a similar pattern, with the highest registered tier scores in the No Significant Effect [Reference Epstein and Preston38, Reference Aharonovich, Liu, Samet, Nunes, Waxman and Hasin40, Reference Lions, Carrieri, Michel, Mora, Marcellin and Morel63, Reference Bunting, Krawczyk, Choo, Pavlicova, McNeely and Tofighi104, Reference Naji, Rosic, Sanger, Dennis, Hillmer and Hudson105, Reference Shulman, Choo, Ohrtman, Pavlicova, Rotrosen and Nunes122] and Harmful/Inferior [Reference Wasserman, Weinstein, Havassy and Hall33, Reference Roux, Carrieri, Cohen, Ravaux, Spire and Gossop53, Reference Proctor, Copeland, Kopak, Hoffmann, Herschman and Polukhina77] direction-of-effect categories, with a smaller Beneficial component [Reference Lucas, Reiman, Earleywine, McGowan, Oleson and Coward58, Reference Lau, Sales, Averill, Murphy, Sato and Murphy70].
AUD and CoUD display related but not identical patterns. In AUD, Beneficial tier weight is concentrated in craving [Reference Lucas, Reiman, Earleywine, McGowan, Oleson and Coward58, Reference Lau, Sales, Averill, Murphy, Sato and Murphy70, Reference Mueller, Hooper, Ellingson, Olsavsky, Rzasa-Lynn and Bryan121, Reference Zimmermann, Teetzmann, Baeßler, Schreckenberger, Zaiser and Pfisterer123], consumption [Reference Reiman44, Reference Reiman48, Reference Lucas, Baron and Jikomes89, Reference Karoly, Mueller, Andrade and Hutchison96, Reference Mok, Milloy, Grant, Lake, DeBeck and Hayashi100], and withdrawal severity [Reference Reiman44, Reference Reiman48, Reference Lucas, Reiman, Earleywine, McGowan, Oleson and Coward58, Reference Mok, Milloy, Grant, Lake, DeBeck and Hayashi100]. No Significant Effect appears most in craving [Reference Karoly, Drennan, Prince, Zulic and Dooley109, Reference Hurzeler, Logge, Watt, McGregor, Suraev and Haber119, Reference Kirkland, Browning, Meredith, Robertson, Herring and Tomko120] and consumption [Reference Kirkland, Browning, Meredith, Robertson, Herring and Tomko120, Reference Mueller, Hooper, Ellingson, Olsavsky, Rzasa-Lynn and Bryan121] within AUD, while harmful signals are scarce [Reference Aharonovich, Liu, Samet, Nunes, Waxman and Hasin40]. In CoUD, the Beneficial signal again concentrates in short-term SUD endpoints and derives predominantly from qualitative, cross-sectional, and case study designs rather than controlled ones (Table 2), with smaller low-evidence contributions to relapse and abstinence. Qualitative and field investigations consistently describe intentional, post-crack cannabis use to manage the “come down,” reducing agitation, dysphoria, and urges across multiple settings. In mixed methods and longitudinal work, reductions in crack use are sometimes observed in the period after these cannabis substitution episodes rather than during use, suggesting a temporal asymmetry that is mechanistically plausible and clinically testable. This pattern warrants targeted prospective designs that anchor exposure, symptom trajectories, and subsequent consumption temporally to determine whether post-episode mitigation translates into reproducible reductions in stimulant use.
Cannabinoid exposure in CoUD does exhibit a notable non-beneficial footprint. No Significant Effect totals are distributed across all six SUD endpoints [Reference Li, Milivojevic, Constable and Sinha21, Reference Epstein and Preston38, Reference Aharonovich, Liu, Samet, Nunes, Waxman and Hasin40, Reference Alessi, Rash and Petry50, Reference Oliveira, Gonçalves, Ometto, Santos, Malbergier and Amaral90, Reference Meneses-Gaya, Crippa, Hallak, Miguel, Laranjeira and Bressan98, Reference Mongeau-Pérusse, Brissette, Bruneau, Conrod, Dubreucq and Gazil101, Reference Reddon, Socias, DeBeck, Hayashi, Walsh and Milloy116], while the Harmful/Inferior category includes SUD endpoints in specific observational contexts [Reference Viola, Tractenberg, Wearick-Silva, Rosa, Pezzi and Grassi-Oliveira65, Reference Giasson-Gariépy, Potvin, Ghabrash, Bruneau and Jutras-Aswad80, Reference Viola, Sanvicente-Vieira, Kluwe-Schiavon, Rothmann, Mélo-Pereira and Bicca95]. Inpatient detox cohorts indicate a correlation between earlier initiation of cannabis and long-duration or heavy use with higher withdrawal scores, more intense craving, and increased re-hospitalizations during CoUD detox, delineating an adverse clinical phenotype within that context [Reference Viola, Tractenberg, Wearick-Silva, Rosa, Pezzi and Grassi-Oliveira65, Reference Viola, Sanvicente-Vieira, Kluwe-Schiavon, Rothmann, Mélo-Pereira and Bicca95]. This inpatient signal coexists with the community “come down” narrative, implying that setting, exposure history, and severity shape directionality in CoUD. Future studies should stratify by age of cannabis onset and cumulative exposure to clarify when cannabis use is palliative versus prognostically unfavorable. TUD and MUD contribute far fewer instances overall. Signals trend Beneficial mostly for craving, withdrawal severity, and consumption, with fewer non-beneficial weight recorded [Reference Morgan, Das, Joye, Curran and Kamboj59, Reference Hindocha, Freeman, Grabski, Stroud, Crudgington and Davies84, Reference Lucas, Baron and Jikomes89, Reference Valleriani, Haines-Saah, Capler, Bluthenthal, Socias and Milloy94, Reference Reddon, Socias, DeBeck, Hayashi, Walsh and Milloy116], but numbers are small and should be read as preliminary.
Taken together, these disorder-specific patterns converge on a single overarching observation. Although cannabinoids may reduce uncomfortable or motivating symptoms in the near term, there is little consistent evidence that such modulation translates into improved treatment course or attainment of sustained non-use. The relative consistency of Beneficial symptom signals suggests that cannabinoids may have a role as adjuncts for short-horizon symptom targets, reducing distressing cravings, mitigating withdrawal experiences, and diminishing overall short-term consumption, at times when such effects can meaningfully support patient engagement or comfort. Such short-term relief from craving, withdrawal, and consumption may itself be valued by patients, even where it does not translate into longer-term treatment benefit. Conversely, the preponderance of No Significant Effect for sustained SUD endpoints, especially in OUD, argues against extrapolating those short-term benefits into assumptions about enduring treatment success. Within the scope of this review, symptom relief is not shown to bridge into sustained therapeutic trajectory or verified non-use at scale.
The tier-weighted framework explains why the short-term/long-term divergence holds even when unweighted counts appear encouraging. By assigning greater weight to randomized and prospective designs, it shows that sustained outcomes are evaluated mainly in higher-tier studies clustering in No Significant Effect, while symptomatic benefits rest disproportionately on lower-tier designs. The few low-tier signals of mild gain in sustained outcomes do not subvert this trend.
This concentration of benefit in the weaker designs is the review’s second principal message, and it carries a specific interpretive risk. Most lower-tier studies are open-label, observational, or qualitative and lack the blinding and placebo control needed to separate a pharmacological effect from expectancy. Cannabinoids are known to produce substantial placebo and expectancy responses. A meta-analysis of double-blind randomized trials in clinical pain found that placebo produced pain reduction comparable to the active cannabinoid [Reference Gedin, Blomé, Pontén, Lalouni, Fust and Raquette124], and balanced placebo experiments show that the expectancy of having received THC alters subjective and behavioral responses independently of the drug itself [Reference Metrik, Kahler, Reynolds, McGeary, Monti and Haney125]. Because craving and withdrawal severity, the endpoints where benefit is most consistent, are largely self-reported and particularly sensitive to expectancy, the symptomatic gains seen in uncontrolled and lower-tier studies may partly reflect these mechanisms rather than a specific cannabinoid action. Caution is, therefore, warranted in attributing even short-term symptom relief to cannabinoids until it is confirmed in adequately powered, placebo-controlled, blinded trials.
A cautious, adjunctive stance appears warranted. The review’s results speak to clinical expectations rather than to the specifics of how cannabinoids should be administered. Where cannabinoids are considered, they are best framed as additions to evidence-based care directed at explicit short-term symptom targets, the only domain in which benefit was observed, and not as a means of improving retention, abstinence, or relapse prevention, for which the present literature shows no consistent effect, particularly in OUD. The non-beneficial and occasionally harmful signals seen in some observational contexts warrant monitoring rather than a presumption of safety. For services and policy makers, these results argue against blanket endorsement while leaving room for methodologically structured exploration where symptom burdens are high and conventional options are constrained.
These findings extend and sharpen themes identified by prior disorder-specific and cannabinoid-specific reviews. In OUD, previous syntheses have reported reductions in craving and anxiety [Reference Shafie, Ing, Rostam-Abadi, Weleff, Griffin and Ranganathan126], benefit in withdrawal settings on nausea and muscle spasms [Reference Kudrich, Hurd, Salsitz and Wang127], and modest opioid withdrawal alleviation by dronabinol within a narrow dose range [Reference Bahji, Gómez and Sofuoglu128]. CBD has been characterized as showing some indication of benefit on opioid craving and anxiety [Reference Lo, MacCallum, Nanson, Koehn, Mitchell and Milloy129], and a cross-SUD review reported beneficial CBD effects in TUD and OUD [130]. Mechanistic syntheses have invoked CBD effects on stress reactivity, sleep, and cue processing to justify adjunctive use [Reference Alencar Rodrigues, Silva Caroba, Taba, Filev and Gallassi131]. However, when attention shifts from proximal symptoms to sustained outcomes, prior evidence becomes more neutral. Meta-analysis of longitudinal OUD data found no significant cannabis association with mitigating non-medical opioid use [Reference Costa, Nunes, Heringer, Anand and De Aquino132], and skepticism persists regarding cannabinoid efficacy on stimulant use outcomes [Reference Paulus, Billieux, Benyamina and Karila130, Reference Daldegan-Bueno, Maia, Glass, Jutras-Aswad and Fischer133, Reference Tang, Tonkovich and Rudisill134]. Our tiered synthesis renders those differences visible by disaggregating endpoints and weighting designs within the largest evidence base yet considered, clarifying why mechanistic plausibility should not be conflated with clinical durability.
This review’s principal strengths are its cross-disorder scope and systematic coverage, yielding the largest eligible corpus of human studies on cannabinoid exposure across five SUDs. Careful SUD endpoint mapping upholds the distinction of patient-oriented symptom experience from longer-horizon clinical outcomes and verified use. The tier-weighted scheme privileges controlled designs while incorporating observational and lived-experience evidence, permitting a wide-angle view of efficacy while guarding against overinterpretation of acute laboratory signals.
Several limitations warrant consideration. The corpus remains heterogeneous across exposure definitions, time horizons, outcome definitions, and measurement methods. Many studies rely on self-report for exposure and sometimes for outcomes, complicating dose–response inference. Objective verification, when present, is most common for outcomes such as administrative retention or biochemically verified use, but even then, follow-up durations and analytic choices vary. Observational designs frequently face residual confounding, including time-varying co-use and symptom severity, and selection mechanisms that can make cannabis exposure a marker of underlying risk rather than a modifiable driver of outcomes. Few randomized trials have sufficient size or duration to test whether acute symptom relief mediates clinically meaningful change over the months in which relapse and sustained non-use are decided. Publication bias is plausible, particularly for early-phase symptom results, and may overstate the apparent consistency of Beneficial findings for craving and withdrawal severity. Representativeness is uneven. Opioid medication programs figure prominently in the OUD evidence, while alcohol and cocaine cohorts often come from inpatient or post-discharge settings. Tobacco and methamphetamine domains are comparatively sparse and geographically constrained. In addition, the tier-weighting framework was compiled by the authors for this review and has not been independently validated, so the tier-weighted values should be read as ordinal scaling aids rather than as validated quantitative estimates.
Future research should close three gaps. First, adequately powered, longer-follow-up RCTs that integrate cannabinoids as adjuncts to standard care, with biochemically verified outcomes, time-horizon stratification to map short-term symptom change onto medium-term outcomes, clear specification of product class, dose, route, the cannabidiol (CBD) and tetrahydrocannabinol (THC) ratio (CBD:THC ratio), and systematic monitoring of adverse effects. These trials should be placebo-controlled and blinded, and given the prominence of expectancy in cannabinoid research, future work should also characterize the placebo and expectancy contribution to the SUD-relevant outcomes reported here, across both symptomatic and sustained endpoints, for example, through balanced placebo designs that separate pharmacological from expectancy effects. Second, real-world studies should embrace target-trial emulation, time-varying confounding control, and transparent exposure characterization, acknowledging policy heterogeneity and product variability that plausibly moderate effects. Third, a harmonized endpoint framework, adopted prospectively across disorders, would improve comparability and facilitate the kind of cross-SUD synthesis attempted here.
When disorder, endpoint, and design are considered together, the evidence from 97 studies encompassing 41,954 participants supports a selective conclusion. Cannabinoid strategies most consistently favor symptom relief, targeting craving, withdrawal severity, and reduction of consumption in the acute treatment stage. The firmest conclusions concern OUD, where the eligible literature is by far the most extensive and cannabinoids are predominantly ineffective for enduring clinical outcomes such as retention, relapse, and abstinence. For AUD, CoUD, TUD, and MUD, far fewer studies met eligibility, with TUD and MUD represented by only a handful of instances, so the findings there, in either direction, should be read as preliminary rather than definitive. This disparity reflects the state of the published evidence rather than any restriction of scope, since all studies meeting the prespecified criteria were included. Within the scope and limits of this review, cannabinoids might be considered for short-horizon symptom targets under protocolized conditions, recognizing that even this short-term benefit rests largely on weaker designs, but they should not be assumed to improve long-term treatment trajectory without further evidence. This interpretation integrates the strengths of a tier-aware synthesis with the discipline of endpoint-specific reporting and is offered to inform clinical decision making, service planning, and the design of next-generation trials aligned to sustained therapeutic outcomes.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1192/j.eurpsy.2026.12236.
Data availability statement
Data extracted and synthesized for this review are reported in the manuscript, tables, and supplementary material. Any additional data can be made available by the corresponding author upon reasonable request.
Acknowledgments
We are indebted to Christopher Zammit Dimech for the invaluable assistance in the formatting and presentation of the figures utilized in the study.
Financial support
None to declare.
Competing interests
None to declare.






 Open access
Open access
Comments
No Comments have been published for this article.