


Non-suicidal self-injury (NSSI) is defined as individuals directly and intentionally harming their own bodies for socially unacceptable reasons, without the intent to die. NSSI is not only a clinical problem that has been increasing over the years, but also a public health issue. Reference Nock1 Reports suggest that its prevalence is about 6.2% before adolescence, Reference Liu, Walsh, Sheehan, Cheek and Sanzari2 and rises to nearly 22% during the adolescent years. Reference Xiao, Song, Huang, Hou and Huang3 Owing to the challenges in defining NSSI and the recognition that it represents a unique clinical phenomenon, the DSM-5 has listed it under conditions that require further study, which has helped shape the theoretical background for ongoing research. 4
Pain perception emerges as an important biological component in understanding the mechanisms influencing the onset and maintenance of NSSI. Studies conducted in this context have revealed that individuals exhibiting NSSI demonstrate a higher pain threshold, greater pain tolerance compared with healthy controls. Reference Koenig, Thayer and Kaess5 Another study conducted with adolescents found that pain hyposensitivity was significantly associated with the frequency of self-harm, and that the pressure pain threshold (PPT) had significant specificity and sensitivity for the frequency of NSSI. Reference Cummins, English, Minnis, Stahl, O’Connor and Bannister6
These differences in pain perception have been reported in various studies to manifest not only subjectively but also at the physiological level. In one study, significant increases in systolic blood pressure (SBP), diastolic blood pressure (DBP) and heart rate were observed following a painful stimulus in terms of the physiological response to pain for the entire sample (NSSI and control group combined). Furthermore, an increased severity of NSSI was associated with a decreased heart rate response to pain and an increased heart rate variability response. These findings suggest that the autonomic nervous system response to pain is associated with decreased sympathetic and increased parasympathetic activity as a result of higher severity NSSI. Reference van der Venne, Mürner-Lavanchy, Höper, Koenig and Kaess7 Unlike studies that employ continuous heart rate monitoring to capture moment-to-moment autonomic fluctuations, the present study relied on pre–post cuff-based measurements of blood pressure and heart rate. Although this method offers a practical and non-invasive way to assess physiological responses to pain, it provides discrete snapshots rather than continuous trajectories and may partially reflect measurement-related arousal. Therefore, interpretations regarding autonomic reactivity should take into account the temporal limitations of this approach.
In addition to physiological processes, various psychological and psychopathological risk factors also play a role in the onset of NSSI. A meta-analysis study found that the presence of depression increased the risk of NSSI by 1.98 times, while the presence of anxiety increased the risk of NSSI by 1.19 times. Reference Fox, Franklin, Ribeiro, Kleiman, Bentley and Nock8 Another meta-analysis examining changes in pain perception in patients with depression and anxiety disorders found that patients with depression had a higher pain threshold, while patients with anxiety had a lower pain threshold. Reference Scaini, Davies, De Francesco, Pelucchi, Rubino and Battaglia9 It has been shown that adolescents with depressive disorders have lower pain sensitivity compared with healthy adolescents, and this lower pain sensitivity has also been found to be positively correlated with suicidal thoughts. Reference Shen, Qing, Yunxiao, Yingao, Jingwen and Xiaoping10 However, recent large-scale research has also reported no meaningful association between psychological symptoms – including depression and anxiety – and experimentally assessed pain thresholds, indicating that these relationships may not be consistent across studies. Reference Böhme, Banellis, Vejlø, Allen and Fardo11
Impaired emotion regulation skills are another fundamental factor frequently emphasised in the psychological basis of NSSI. Emotion regulation is defined as an individual’s capacity to observe, evaluate and regulate their emotional responses, particularly the intense and transient nature of these responses, in order to achieve their goals. Reference Thompson12 Results from longitudinal studies conducted with both adolescents and young adults have revealed that experiencing difficulty in regulating emotions predicts greater participation in NSSI. Reference Duggan, Heath and Hu13,Reference Heffer and Willoughby14 As a result of a study, it was found that emotion dysregulation is associated with reduced pain perception, independent of individuals’ history of NSSI. It was also noted that emotion dysregulation has a partial mediating effect on the relationship between NSSI and pain tolerance. Reference Franklin, Aaron, Arthur, Shorkey and Prinstein15
In light of these findings, NSSI must be approached in a multidimensional manner, not only through psychological foundations but also within the context of interactions between pain perception, physiological response patterns and emotion regulation skills. However, studies evaluating these variables together are quite limited in the literature. Accordingly, the present study aims to contribute to the field by examining the biopsychological processes accompanying NSSI in adolescents from a holistic perspective, particularly by revealing the relationships between PPT, autonomic responses and psychological variables.
Our hypotheses developed in this context are presented below:
-
(a) It is expected that the PPT in the case group consisting of adolescents exhibiting NSSI will be higher than in the control group.
-
(b) It is expected that the amount of change in physiological measurement parameters in response to pain stimuli will be lower in the case group consisting of adolescents exhibiting NSSI compared with the control group.
-
(c) Depression and anxiety scores are expected to be higher in adolescents exhibiting NSSI compared with the control group.
-
(d) Adolescents who exhibit NSSI are expected to have more difficulty regulating their emotions compared with the control group.
-
(e) In adolescents exhibiting NSSI, a negative relationship is expected between the amount of change in physiological measurement parameters and pain threshold values.
-
(f) A positive correlation is expected between depression scores and PPT values in the case group consisting of adolescents exhibiting NSSI.
-
(g) A negative correlation is predicted between anxiety scores and PPT values in the case group consisting of adolescents exhibiting NSSI.
-
(h) A positive correlation is expected between emotion regulation difficulties and PPT values.
Method
Research design
This research employed a single-centre, cross-sectional and non-matched case–control design. Although individual matching was not performed, participants were recruited with the aim of achieving demographic comparability, particularly with respect to age and gender. Before data collection, power analysis was conducted with the G*Power software (G*Power version 3.1.9.6 for macOS; Düsseldorf; https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower), using effect size derived from previous research Reference Franklin, Aaron, Arthur, Shorkey and Prinstein15 (d = 0.84). Accordingly, it has been calculated that a sample of at least 64 participants (at least 32 participants for each group) was required to achieve 80% power at a 95% CI. This power analysis was conducted based on the study’s a priori determined hypothesis (a) (the assumption that the NSSI group has a higher pain threshold than the control group). Therefore, the calculated sample size is based on the effect size required to detect the difference in pain threshold between the two groups. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human patients were approved by the Pamukkale University Faculty of Medicine Non-Interventional Clinical Research Ethics Committee with E-60116787-020-690590 number. Written informed consent was obtained from both the adolescents and their parents or legal guardians prior to participation. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Reference Von Elm, Altman, Egger, Pocock, Gøtzsche and Vandenbroucke16 guidelines for case–control research, and the completed STROBE checklist is provided as Supplementary Table 1 available at https://doi.org/10.1192/bjo.2026.10997.
Participants and psychiatric assessment
The study population consisted of adolescents aged 14–18 who visited the Child and Adolescent Psychiatry Outpatient Clinics at Pamukkale University Faculty of Medicine Hospital for any reason. Among these, 34 adolescents who met the DSM-V diagnostic criteria for NSSI were included in the case group of our study. Thirty-four adolescents without any physical or mental illness diagnosis were included in the control group. All adolescents included in the study and their families were informed about the study and were included in the study groups after obtaining their written consent.
Adolescents and their parents underwent detailed diagnostic interviews based on DSM-V to evaluate their diagnoses. For both study groups, exclusion criteria included refusal to participate, intellectual disability, autism spectrum disorder and psychotic disorders. For the control group, additional exclusion criteria were the presence of a history of NSSI and/or suicide, as well as any psychiatric or physical illness.
Data collection tools
Sociodemographic Data Form (SDF)
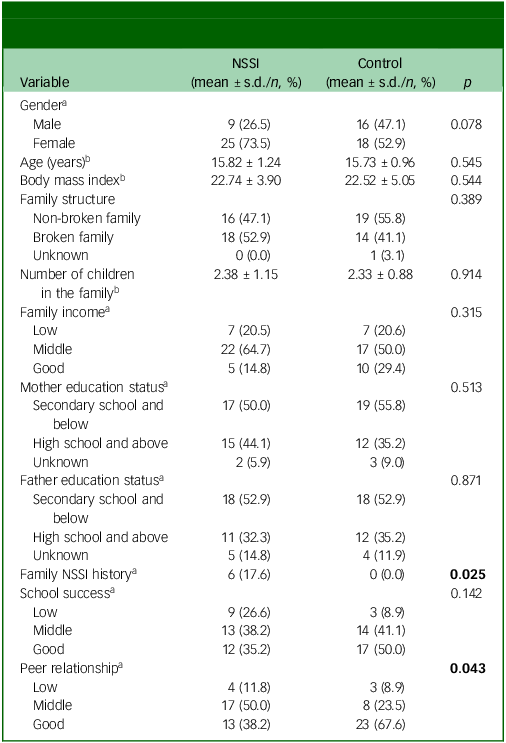
The SDF was developed by the researchers to collect basic descriptive information. The form included gender assigned at birth, age, BMI, family structure, number of children, family income level, parental education levels, family history of NSSI, perceived school success and quality of peer relationships. Descriptive statistics for all variables are presented in Table 1.
Comparison of sociodemographic characteristics between non-suicidal self-injury (NSSI) and control groups

a. Chi-square test.
b. Mann-Whitney U test.
Statistically significant values (p < 0.05) are shown in bold.
Inventory of Statements About Self-Injury (ISAS)
The ISAS, a measurement tool that provides a detailed assessment of an individual’s self-harming behaviour, was developed by Klonsky and Glenn in 2009. Reference Klonsky and Glenn17 The scale consists of two sections, ‘Behaviors’ and ‘Functions,’ and allows for the participant’s self-report evaluation. The first section, ‘Behaviors,’ inquires about NSSI methods and how many times these methods were performed. The second section, ‘Functions,’ has two subscales: intrapersonal functions and interpersonal functions, and evaluates the functions of NSSI with 39 questions. The Turkish adaptation and psychometric evaluation of the scale were conducted by Bildik et al in a sample of high school students. Reference Bildik, Somer, Kabukçu Başay, Başay and Ozbaran18 In our study, the Cronbach’s α coefficient for the total intrapersonal functions score was determined to be 0.863, and the Cronbach’s α coefficient for the total interpersonal functions score was determined to be 0.914.
Revised Child Anxiety and Depression Scale – Child Version (RCADS)
This is a clinical symptom screening scale developed to assess depression and anxiety disorders in young people. Developed by Chorpita et al, Reference Chorpita, Yim, Moffitt, Umemoto and Francis19 the scale consists of 47 items and 6 subscales. The scale is a 4-point Likert scale, and each item is scored on a scale of 0–3. The subscales assessed by the scale are separation anxiety, social phobia, obsessive–compulsive disorder, panic disorder, generalised anxiety disorder and major depressive disorder. Eight different total scores can be obtained from the scale. Six of these are scores obtained from the sum of the subdimensions, while the other two are the anxiety total score and the anxiety-depression total score, i.e. the total score of the scale. The validity and reliability of the scale for children and adolescents in Turkish were established by Görmez et al. Reference Gormez, Kılınçaslan, Orengul, Ebesutani, Kaya and Ceri20 In our study, the Cronbach’s α coefficient for the total scale score was determined to be 0.969.
Difficulties in Emotion Regulation Scale-16 (DERS-16)
The scale, developed by Biureberg et al Reference Bjureberg, Ljótsson, Tull, Hedman, Sahlin and Lundh21 as a short form of the DERS scale, consists of 16 items and allows participants to be assessed through self-reporting. The scale has a 5-point Likert structure. It consists of five subscales: non-acceptance, goal, impulsivity, strategy and openness. Subscale scores are obtained by summing the relevant subscale items, while the total of all items constitutes the total scale score. The validity and reliability study of the scale for the adolescent age group in Turkish was conducted by Demirpençe Seçinti and Şen. Reference Demirpence Secinti and Sen22 In our study, the Cronbach’s α coefficient for the total scale score was determined to be 0.944.
Measures
PPT measure
PPT measurements were performed under the same environmental conditions and by the same researcher using a digital algometer device (Jtech Echo Algometer, USA). The algometer used in the study has a maximum measurement capacity of 11.3 kg. Participants were informed about the procedure prior to the test. They were asked to inform the examiner at the first moment they felt pain during the pressure application. Participants were seated during the procedure. PPT measurement was performed by applying pressure to the third finger pulp of the participants’ dominant hand using the device. The dominant hand was chosen because it is typically used to perform NSSI rather than being injured itself, reducing the likelihood of confounding effects from local tissue damage or altered nociception. Measurements were repeated three times at 1-min intervals, and the average of the three measurements was recorded as the participants’ PPT in kg/cm2. To evaluate whether a 1-min interval between repeated PPT measurements was sufficient to prevent carry-over or temporal summation effects, a repeated-measures analysis of variance (ANOVA) was conducted on the three PPT trials. No significant differences were observed across the three measurements (p = 0.539, partial η 2 = 0.009), indicating that the 1-min interval successfully minimised carry-over effects.
Blood pressure and heart rate measure
After a minimum 10-min rest period prior to the PPT measurement, blood pressure and pulse measurements were taken from the participants’ left arm using a digital upper-arm blood pressure monitor (WOHLER JPD-HA200, Shenzhen Jumper Medical Equipment Co. Ltd., China). After the PPT measurement, blood pressure and pulse values were measured again in the same manner. All measurements were conducted while participants remained seated throughout the entire procedure. Post-PPT blood pressure and heart rate measurements were taken after the PPT assessment without any change in body position to avoid postural or movement-related confounding. Changes in SBP/DBP and pulse were recorded for each participant.
Analytic plan and statistical approach
This study was not pre-registered; therefore, the distinction between confirmatory and exploratory analyses is detailed in this section to enhance the transparency of the study.
In this study, hypotheses (a)–(h) were determined prior to the data collection process. Hypotheses (a) and (b) are between-group hypotheses comparing pain threshold and physiological response changes between the NSSI and control groups. Hypotheses (c) and (d) are between-group hypotheses comparing psychopathology (depression and anxiety levels) and emotion regulation difficulties between the two groups. Hypotheses (e), (f) and (g) are within-group hypotheses tested only in the NSSI group (hypothesis (e): relationship between the amount of physiological change and pain threshold; hypothesis (f): relationship between depression and pain threshold; hypothesis (g): relationship between anxiety and pain threshold). Hypothesis (h) aims to evaluate the relationship between emotion regulation difficulties and pain threshold at the level of the entire sample. Within the confirmatory hypotheses, between-group differences in pain threshold (a) and physiological response (b) were designated as the primary study outcomes. All remaining confirmatory hypotheses (c)–(h) were treated as secondary study outcomes.
Analyses beyond these hypotheses – those examining relationships between NSSI functions (ISAS subscales) and pain threshold – were not planned prior to the study and are therefore classified as exploratory analyses. Their results are presented separately from hypothesis-based analyses in the results section.
Statistical evaluation
The data were analysed using the SPSS program (IBM SPSS Statistics for macOS, Version 27.0. Armonk, NY: IBM; https://www.ibm.com/products/spss-statistics#pricing). Continuous variables are presented as mean ± s.d. and categorical variables as frequency and percentage. Prior to conducting parametric analyses, the assumption of normality was evaluated using the Kolmogorov–Smirnov and Shapiro–Wilk tests. When parametric assumptions were met, independent sample t-tests were used; otherwise, Mann–Whitney U tests were applied. Relationships between continuous variables were examined using Pearson or Spearman correlations (partial correlations when covariates were included), and categorical differences were assessed with chi-square tests. For comparing changes in physiological variables (SBP, DBP and heart rate) between groups, a mixed (repeated measures) ANOVA was conducted. In this model, time (pre–post PPT) served as the within-subject factor and group (NSSI versus control) as the between-subject factor. The group × time interaction term tested whether physiological responses differed between groups. Adjusted models included age, gender and BMI as covariates due to known influences on cardiovascular reactivity. Group comparisons of pain threshold and psychological variables were conducted without covariates, as these analyses represented primary hypothesis-driven contrasts. This analytic approach was adopted to ensure transparency and consistency across models.
Results
There were no missing data for any study variables; all participants had complete observations across physiological, psychological and pain measures.
Sociodemographic data
The study included 34 cases with NSSI and 34 healthy control participants. The mean ages of the participants were 15.82 ± 1.24 and 15.73 ± 0.96, respectively, and no statistically significant difference in age was found between the two groups (p = 0.545). The gender assigned at birth distribution was 73.5% female and 26.5% male in the case group and 52.9% female and 47.1% male in the control group; no significant difference was observed between the groups in terms of gender (p = 0.078). Detailed sociodemographic data for the participants are presented in Table 1.
Group comparisons (hypotheses (a)–(d))
Hypothesis (a): group differences in PPT
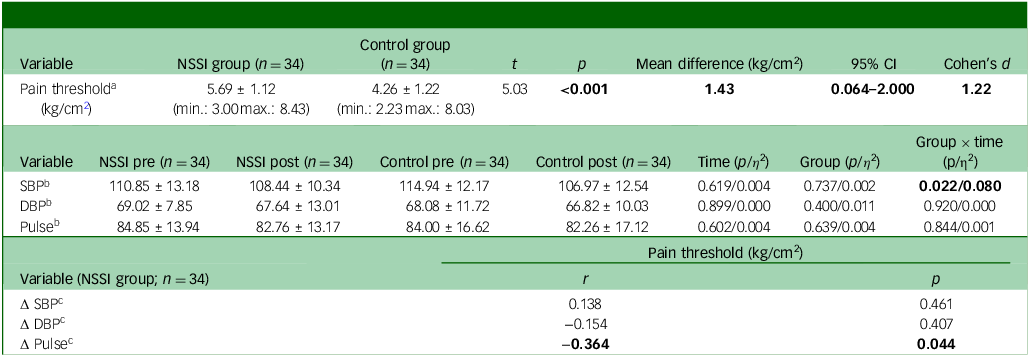
A significant difference in PPT was found between the groups. The mean PPT for the NSSI group was 5.69 ± 1.12 kg/cm2, while the mean for the control group was 4.26 ± 1.22 kg/cm2. This difference was considered statistically significant (p < 0.001) (Table 2). None of the participants’ PPT values reached the maximum measurable limit of the algometer (11.3 kg).
Pain threshold and autonomic response indicators: group comparisons and correlations

NSSI, non-suicidal self-injury; SBP, systolic blood pressure; DBP, diastolic blood pressure.
a. Independent samples t test.
b. Mixed analysis of variance analysis.
c. Partial correlation.
Statistically significant values (p < 0.05) are shown in bold.
Hypothesis (b): group × time differences in physiological reactivity
Pain-induced changes in SBP, DBP and heart rate were analysed using mixed (repeated-measures) ANOVA with age, gender and BMI entered as covariates.
SBP
The main effect of time (p = 0.619, η 2 = 0.004) and group (p = 0.737, η 2 = 0.002) were not significant but the group × time interaction was significant (p = 0.022, η 2 = 0.080). This indicates that the SBP change pattern differed between groups. SBP decreased by 2.41 mmHg in the NSSI group (110.85 → 108.44 mmHg), whereas the control group showed a larger decrease of 7.97 mmHg (114.94 → 106.97 mmHg). The resulting interaction contrast was 5.56 mmHg, reflecting a noticeably blunted physiological response in the NSSI group.
DBP
Time (p = 0.899, η 2 = 0.000), group (p = 0.400, η 2 = 0.011) and group × time interaction (p = 0.920, η 2 = 0.000) were not significant. Small and similar decreases in DBP values were observed in both groups (NSSI: 69.02 → 67.64 mmHg; control: 68.08 → 66.82 mmHg) (Table 2).
Heart rate
Time (p = 0.602, η 2 = 0.004), group (p = 0.639, η 2 = 0.004) and group × time interaction (p = 0.844, η 2 = 0.001) were not significant. Heart rate change showed a similar decrease in both groups (NSSI: 84.85 → 82.76; control: 84.00 → 82.26) (Table 2).
Hypotheses (c)–(d): group differences in depression, anxiety and emotion regulation
According to the results obtained from the RCADS and DERS-16 scales, the psychopathology levels of the NSSI group are significantly higher than those of the control group. The major depression subscale score was significantly higher in the case group (p < 0.001). Similarly, the total anxiety score (p < 0.001) and the RCADS total scale score (p < 0.001) were also significantly higher in the NSSI group compared with the control group. The DERS-16 total score, which assesses difficulties in emotion regulation, was also found to be statistically significantly higher in the case group (p < 0.001) (Table 3).
Comparison of depression, anxiety and emotion regulation difficulties between non-suicidal self-injury (NSSI) and control groups

RCADS, Revised Child Anxiety and Depression Scale; DERS-16, Difficulties in Emotion Regulation Scale.
a. Independent samples t test.
Statistically significant values (p < 0.05) are shown in bold.
Relationships in the NSSI group (hypotheses (e)–(g))
Hypothesis (e): within-NSSI association between physiological change and PPT
In the NSSI group, a significant negative association was found between heart rate change (Δheart rate) and PPT after adjusting for age, gender and BMI (partial r = –0.364, p = 0.044). No significant associations were observed between pain threshold and changes in SBP or DBP (partial r = 0.138, p = 0.461; partial r = –0.154, p = 0.407, respectively) (Table 2).
Hypotheses (f)–(g): within-NSSI association between depression, anxiety and PPT
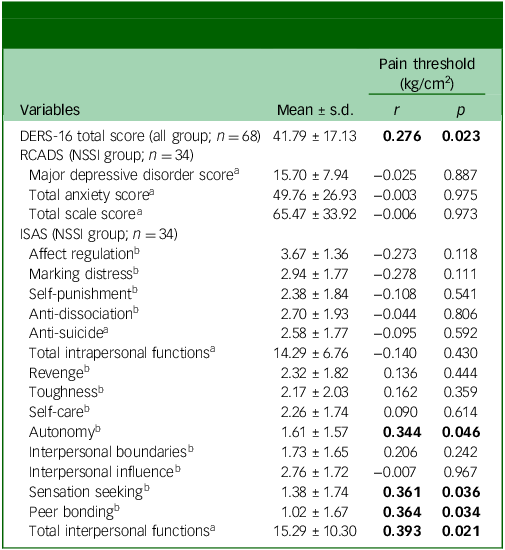
No significant relationship was found between the RCADS scale depression subscale, total anxiety subscale and total scale score and the PPT in the NSSI group (all p > 0.05) (Table 4).
Correlations between pain threshold, psychological scale scores and non-suicidal self-injury (NSSI) functions

DERS-16, Difficulties in Emotion Regulation Scale; RCADS, Revised Child Anxiety and Depression Scale; ISAS, Inventory of Statements About Self-Injury.
a. Pearson correlation.
b. Spearman correlation.
Statistically significant values (p < 0.05) are shown in bold.
Relationships in the entire sample (hypothesis (h))
Hypothesis (h) : full-sample association between DERS and PPT
When examining the correlations between the PPT and DERS-16 total score, a positive and significant relationship was found between the DERS-16 total score and PPT in the entire sample (r = 0.276, p = 0.023) (Table 4).
Exploratory analyses: relationships between pain thresholds and NSSI functions
The analyses presented in this section were not pre-specified and are exploratory in nature. Given the large number of comparisons, the risk of false-positive findings is increased; therefore, these results should be interpreted with caution.
When examining the ISAS subscales that assess NSSI functions, significant positive correlations were found between the PPT and the functions of autonomy (r = 0.344, p = 0.046), sensation seeking (r = 0.361, p = 0.036) and peer bonding (r = 0.364, p = 0.034). Furthermore, a significant positive relationship was observed between the total interpersonal functions score and PPT (r = 0.393, p = 0.021) (Table 4).
Discussion
In this study, it was found that individuals with NSSI had a significantly higher PPT compared with the control group. Similarly, a recent meta-analysis also showed that adolescents and young adults with NSSI had a higher pain threshold than healthy controls. Reference Pontén, Lee, Khoo, Nilsson, Nevin and Walldén23 This result suggests that these individuals may perceive and process pain differently. According to Nock’s ‘pain analgesia hypothesis,’ individuals with low sensitivity to expected pain are more likely to exhibit NSSI. Reference Nock1 Additionally, Kao et al suggested that the pain threshold may return to normal with a decrease in NSSI frequency and therefore may serve as a ‘state marker’. Reference Kao, Mürner-Lavanchy, von Stosch, Josi, Berger and Koenig24 In another study conducted using machine learning, low pain sensitivity was identified as one of the strongest predictors of NSSI. Reference Mürner-Lavanchy, Koenig, Reichl, Josi, Cavelti and Kaess25 All these findings suggest that pain perception may be an important component in clinical assessment and intervention processes. However, further research is needed to explain the psychological and biological mechanisms underlying the increased PPT, particularly in adolescents.
In our study, when examining pre- and post-pain physiological responses, only a significant time effect and time × group interaction were detected for SBP. Following pain, SBP decreased in both groups, but this decrease was more pronounced in the control group and remained limited in the NSSI group. This suggests that autonomic response patterns accompanying pain may differ in individuals with NSSI and that alternative mechanisms may be involved in regulating physiological responses to acute stressors. The literature reports increased cortisol response after pain, decreased parasympathetic activity and delayed recovery in adolescents with NSSI. Reference Koenig, Rinnewitz, Warth, Hillecke, Brunner and Resch26 Furthermore, it has been demonstrated that as NSSI frequency increases, cortisol and α-amylase responses change, heart rate response becomes weaker and sympathetic response components differ. Reference van der Venne, Mürner-Lavanchy, Höper, Koenig and Kaess7 These findings suggest that autonomic regulation can be reshaped not only at the basal level but also in terms of dynamic responses to stressors. The limited SBP change observed in our study may also be part of a desensitisation pattern. Furthermore, the persistence of the group × time interaction despite the disappearance of the time effect when age, gender, and BMI covariates were added suggests that the SBP’s NSSI-specific differentiation may be related to biological processes independent of developmental factors. However, supporting our findings with larger samples and longitudinal designs will allow for stronger and more generalisable conclusions about the nature of this relationship. In this context, considering the limited number of studies conducted specifically in the adolescent age group, future longitudinal studies with larger samples will contribute to a more detailed understanding of this autonomic response pattern in a developmental context.
Although significant changes were observed in SBP in our study, the fact that no significant differences were found between groups in DBP and pulse changes can be considered a physiologically expected situation. Since SBP is more sensitive to acute changes in cardiac output and sympathetic nervous system activity, it can respond quickly to short-term stressors; DBP is primarily determined by peripheral vascular resistance, and changes in this resistance are related to slower vascular processes. Reference Shahoud, Sanvictores and Aeddula27 The pulse response is regulated via the baroreflex, and this regulation can show significant differences between individuals. Indeed, the literature reports that sympathetic nervous system activity in healthy individuals can vary by a factor of 7–10 between individuals, and that baroreflex sensitivity can differ both between individuals and over time. Reference Charkoudian and Rabbitts28 Given that DBP typically shows less reactivity to acute nociceptive or stress-related stimuli than SBP, the absence of significant DBP changes in our results is consistent with expected physiological response patterns. Therefore, the observation of significant changes in SBP in response to a short-term and controlled stressor, coupled with more limited responses in DBP and heart rate, can be considered a physiologically based outcome.
Although our study did not reveal a significant group × time interaction in terms of heart rate at the group level, correlation analyses performed only in the NSSI group showed a significant difference. A significant and negative relationship was found between the amount of heart rate change (Δheart rate) and PPT; this relationship was maintained even when covariates were controlled. Accordingly, as the PPT increases, the heart rate response after a painful stimulus decreases, meaning that the cardiovascular response is more blunted. This finding is consistent with studies reporting that physiological responses in NSSI generally occur at lower intensities. Koenig et al found that adolescents with NSSI exhibited a less pronounced increase in heart rate and a smaller decrease in heart rate variability following stress exposure, reflecting attenuated autonomic reactivity. Reference Koenig, Lischke, Bardtke, Heinze, Kröller and Pahnke29 In this regard, our findings indicate that NSSI-specific regulation exists not only at the group level but also in terms of individual physiological patterns. Our results suggest that NSSI may be shaped not only by psychological processes but also by interactions with autonomic nervous system responses and pain-related physiological factors. However, further studies with larger samples and longitudinal designs are needed to better understand the nature of this relationship.
In our study, depression, anxiety and emotion regulation difficulties were higher in the NSSI group compared with the controls. However, these differences likely reflect the expected clinical profile of adolescents who engage in NSSI rather than representing a study-specific effect, given that such characteristics are commonly reported in this population and were partly reflected in the inclusion criteria. Therefore, these findings should be interpreted primarily as descriptive indicators of sample characteristics. Meta-analytic studies consistently show that depressive and anxious symptoms are associated with NSSI and contribute to the onset and maintenance of the behaviour. Reference Fox, Franklin, Ribeiro, Kleiman, Bentley and Nock8,Reference Shi, Gao, Zhou and Huang30,Reference Guan, Liu, Li, Cai, Bi and Zhou31 Similarly, the higher level of emotion regulation difficulties observed in our NSSI group aligns with prior literature; for example, Wolff et al reported a moderate association between emotion regulation difficulties and NSSI. Reference Wolff, Thompson, Thomas, Nesi, Bettis and Ransford32 Taken together, although these psychological differences do not constitute novel findings, they reinforce the multidimensional nature of NSSI and underscore the importance of assessing depression, anxiety and emotion regulation skills in clinical practice. Future longitudinal studies will be essential for clarifying the causal roles of these processes.
Our study’s analyses conducted at all participant levels revealed a positive and significant relationship between difficulties in emotion regulation and PPT. This finding suggests that individuals with weak emotion regulation skills may have a higher PPT. Indeed, emotion dysregulation has been shown to be associated with reduced pain perception, independent of individuals’ history of NSSI. Reference Franklin, Aaron, Arthur, Shorkey and Prinstein15 The literature demonstrates that pain and emotion regulation processes operate through shared neurobiological mechanisms and interact with each other. According to Bresin and Gordon’s model, the experience of pain is not only a physiological response but can also contribute to the emotional regulation process. In this context, it is suggested that NSSI, which emerges during periods of intense negative emotion, may serve a regulatory function at both the physiological and emotional levels through pain. Reference Bresin and Gordon33 However, it is important to note that not all studies have reported an association between emotion regulation and pain perception. For example, Lalouni et al Reference Lalouni, Fust, Bjureberg, Kastrati, Fondberg and Fransson34 found no significant link between emotion regulation difficulties and pain sensitivity, indicating that findings in this domain remain mixed. Although emotion regulation difficulties were positively associated with PPT in the full sample, this relationship may partly reflect underlying group differences, as both emotion regulation difficulties and PPT were significantly higher in the NSSI group compared with the controls. Therefore, this association should be interpreted with caution. While our findings are generally consistent with much of the existing literature, further studies with larger samples and longitudinal designs are needed to understand the causal aspects and developmental dynamics of this relationship.
Our study found no significant relationship between RCADS depression and anxiety scores and PPT. Although this finding may appear to contradict the literature at first glance, it is consistent with the complex picture presented by current research. Meta-analyses show that the direction and magnitude of this relationship may vary depending on the clinical characteristics of the sample and the type of pain stimulus. For example, Thompson et al found no difference between depressed and control groups in high-intensity noxious stimulation but detected a higher pain threshold in depressed individuals in low-intensity noxious stimulation. Furthermore, it has been reported that the cutaneous pain threshold increases in depression, while it decreases for ischaemic stimulation. Reference Thompson, Correll, Gallop, Vancampfort and Stubbs35 A 2025 meta-analysis also shows that depression is associated with a higher pain threshold and anxiety with a lower pain threshold, and that the severity of depression is moderately correlated with the pain threshold. In addition, it is noted that the results vary depending on the type of pain. Reference Salas-González, Heredia-Rizo, Fricke-Comellas, Chimenti and Casuso-Holgado36 However, there may be various methodological and sample-based reasons why our study does not fully align with the literature. Some of these include the limited sample size, targeting the NSSI group rather than a clinically diagnosed population with depression or anxiety and measuring the PPT using only a single type of stimulus (pressure). Therefore, further studies with larger samples, covering different pain modalities and focusing on clinical diagnosis groups are needed to better understand the relationship between depression and anxiety levels and PPT.
Our study found significant positive correlations between PPT and certain functions of NSSI. As the PPT increased, the frequency of use of the behaviour’s functions of sensation seeking, peer bonding and autonomy was also found to increase. This finding shows that NSSI is not limited to the function of reducing internal tension or regulating negative emotions; the experience of pain may also be linked to different functions of the behaviour. According to the Benefits and Barriers Model, NSSI is shaped not only by internal (self-punishment, emotional relief) and external (bonding with peers, social acceptance and communication) reinforcers, but also by the interaction of factors that sustain and inhibit behaviour. Reference Hooley and Franklin37 In this model, barriers are defined as obstacles that make it difficult for the behaviour to emerge. A high pain threshold can contribute to the behaviour becoming easier to engage in by weakening this physical barrier. This situation can increase the likelihood of NSSI emerging, particularly in individuals who are sensation seeking. Reference Kentopp, Conner, Fetterling, Delgadillo and Rebecca38 Additionally, it has been reported that individuals who continue to engage in NSSI generally have a higher pain threshold Reference Glenn, Michel, Franklin, Hooley and Nock39 and tend to form more relationships with peers who exhibit this behaviour. Reference Heath, Ross, Toste, Charlebois and Nedecheva40 Our findings suggest that the function of gaining autonomy may also be related to the PPT. A high pain threshold may strengthen an individual’s perception of control over their behaviour and transform self-harm into an experience associated with a sense of ‘regaining control’ or ‘being effective’ over their body. Reference Nock1 This situation can be considered as one of the possible psychological mechanisms underlying the relationship between PPT and the autonomy function of behaviour. On the other hand, considering that the relationship between PPT and NSSI functions has not been directly addressed in the literature, our finding contributes uniquely to the existing body of knowledge. Further research involving larger samples and different pain modalities is needed to elucidate the underlying processes of this relationship in greater detail. However, because the associations between NSSI functions and pain threshold were derived from exploratory analyses and involved multiple comparisons, these findings should be interpreted cautiously due to the increased risk of false positives.
This study should be evaluated in light of several important limitations. First, although the power analysis indicated that the sample size was sufficient for detecting the primary outcome – group differences in pain threshold – it should be acknowledged that secondary analyses (e.g. physiological responses and within-group correlations) may not have had adequate power to detect smaller effect sizes. Accordingly, non-significant results in these analyses should be interpreted with caution. The absence of significant associations between psychopathology and pain outcomes is more likely attributable to limited statistical power within the NSSI group. In addition, although the difference in gender distribution between groups did not reach statistical significance (p = 0.078), the absolute imbalance (73.5 v. 52.9% female) indicates that the study may not have been sufficiently powered to detect gender-specific effects. Given prior evidence that gender may influence pain threshold, autonomic reactivity and psychopathology, the potential contribution of gender to some findings cannot be fully ruled out. Future studies with larger and more balanced samples are needed to clarify these effects. Another limitation is that some participants in the NSSI group had comorbid psychiatric diagnoses, which may complicate interpretations regarding processes specific to NSSI. Furthermore, pain threshold was assessed using only one type of noxious stimulus (pressure), limiting the generalisability of the results to other pain modalities. The cross-sectional design of the study also prevents causal inferences. Another limitation is the use of a non-matched case–control design. Although the groups were statistically comparable in age and gender, the absence of individual matching may limit control over unmeasured confounding variables. Additionally, physiological measurements were restricted to acute responses, and long-term autonomic regulatory processes were not assessed. Finally, given the large number of comparisons – particularly in exploratory analyses – there is an increased risk of false-positive findings. Because of the limited sample size and theoretical intercorrelation among subscales, applying a formal multiple comparison correction (e.g. Holm–Bonferroni) would likely be overly conservative. Therefore, exploratory results are interpreted with caution and should not be considered confirmatory.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.10997
Data availability
The data supporting this study’s findings are available on request from the corresponding author. The data are not publicly available due to preserving the privacy of research participants.
Acknowledgements
We thank all participants and their families who participated in the study. The authors acknowledge the use of ChatGPT 5.2 for grammatical corrections and language editing during the drafting of this manuscript.
Author contributions
The study was designed with the contributions of all authors. N.E.G. collected the data. E.G.G. performed the data analysis. E.G.G. prepared the first draft. E.G.G., N.E.G., B.K.B., Ö.B., A.B. and M.A.T. interpreted the data, contributed to the writing and revision of the manuscript and approved the final version to be published.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.