


Emotional instability and difficulties in emotion regulation (ER), defined as problems with the processes of “monitoring, evaluating, and modifying emotional reactions” (Thompson, Reference Thompson1994, pp. 27–28), are core symptoms of Borderline Personality Disorder (BPD; Bud et al., Reference Bud, Nechita and Szentagotai Tatar2023; D’Aurizio et al., Reference D’Aurizio, Di Stefano, Socci, Rossi, Barlattani, Pacitti and Rossi2023). This is supported by meta-analytical findings showing a strong association between ER difficulties and BPD symptoms (Bud et al., Reference Bud, Nechita and Szentagotai Tatar2023; Daros & Williams, Reference Daros and Williams2019; Putnam & Silk, Reference Putnam and Silk2005), and by a developmental trajectory study in children and adolescents linking increased ER difficulties to higher borderline symptoms over time (Vogel et al., Reference Vogel, Geselowitz, Tillman, Barch, Luby and Whalen2024). However, little is known about how and when these difficulties manifest in early developmental stages, particularly in children at elevated risks, despite their potential role as early indicators of later psychopathology.
Research on developmental pathways provides evidence for a transgenerational transmission of BPD and its core symptomatology. Family studies have reported a 4- to 20-fold increased risk of BPD in first-degree relatives compared to the general population (Barnow et al., Reference Barnow, Spitzer, Grabe, Kessler and Freyberger2006; Zanarini et al., Reference Zanarini, Gunderson, Marino, Schwartz and Frankenburg1988), with even stronger familial clustering for core symptoms (Silverman et al., Reference Silverman, Pinkham, Horvath, Coccaro, Klar, Schear, Apter, Davidson, Mohs and Siever1991). According to Linehan’s biosocial theory, BPD develops through the interaction of an invalidating environment, mismatched parental responses to the child’s emotions, and the child’s emotional vulnerability (Lieb et al., Reference Lieb, Zanarini, Schmahl, Linehan and Bohus2004; Linehan, Reference Linehan1987). A growing body of evidence supports this parent–child pathway, linking parents’ ER difficulties to the development of ER difficulties and related psychopathology in their children, both in clinical and non-clinical samples (Feng et al., Reference Feng, Shaw and Silk2008; Han & Shaffer, Reference Han and Shaffer2013; Li et al., Reference Li, Li, Wu and Wang2019; Loechner et al., Reference Loechner, Sfärlea, Starman, Oort, Thomsen, Schulte-Körne and Platt2020; Luczejko et al., Reference Luczejko, Werkmann, Hagelweide, Stark, Weigelt, Christiansen, Kieser, Otto, Reck, Steinmayr, Wirthwein, Zietlow and Schwenck2024; Powers et al., Reference Powers, Stevens, O’Banion, Stenson, Kaslow, Jovanovic and Bradley2022; Shortt et al., Reference Shortt, Stoolmiller, Smith-Shine, Mark Eddy and Sheeber2010). However, most clinical research has examined parental ER in the context of anxiety or depressive disorders (Loechner et al., Reference Loechner, Sfärlea, Starman, Oort, Thomsen, Schulte-Körne and Platt2020; Riva Crugnola et al., Reference Riva Crugnola, Ierardi, Ferro, Gallucci, Parodi and Astengo2016; Sanders et al., Reference Sanders, Zeman, Poon and Miller2015), while studies focusing on children of parents with BPD are comparatively scarce (e.g., Dittrich et al., Reference Dittrich, Boedeker, Kluczniok, Jaite, Hindi Attar, Fuehrer, Herpertz, Brunner, Winter, Heinz, Roepke, Heim and Bermpohl2018; Kohlhoff et al., Reference Kohlhoff, Cibralic, Wallace, Morgan, McMahon, Hawkins, Eapen, Briggs, Huber and McNeil2020; Silk et al., Reference Silk, Shaw, Skuban, Oland and Kovacs2006).
Although limited, initial findings suggest that children of mothers with BPD show difficulties in ER at various stages of development and in different contexts. For example, an observational study has shown that three-year-old children of mothers with BPD display lower self-soothing abilities during mother–child interactions compared to children of mentally healthy mothers and those whose mothers have depressive disorders (White et al., Reference White, Flanagan, Martin and Silvermann2011). In an open-ended narrative paradigm, children aged four to seven years were presented with emotionally charged story stems and asked to complete them; children of mothers with BPD demonstrated fewer ER strategies in their responses than children of mentally healthy mothers (Macfie et al., Reference Macfie, Swan, Fitzpatrick, Watkins and Rivas2014; Macfie & Swan, Reference Macfie and Swan2009). In a community sample, adolescent daughters of mothers with BPD reported reduced self-control and increased negative affectivity on temperament questionnaires (Zalewski et al., Reference Zalewski, Stepp, Scott, Whalen, Beeney and Hipwell2014). Overall, these studies have focused primarily on habitual ER rather than spontaneous, state-level strategies in emotionally challenging contexts, and they employed heterogeneous assessment methods. Most research on children of parents with BPD relies on maternal reports, self-reports, or clinician ratings and is further limited to a narrow age range (Gratz et al., Reference Gratz, Myntti, Kiel, Kurtz and Tull2024; Macfie et al., Reference Macfie, Swan, Fitzpatrick, Watkins and Rivas2014; Whalen et al., Reference Whalen, Kiel, Tull, Latzman and Gratz2015; Zalewski et al., Reference Zalewski, Stepp, Scott, Whalen, Beeney and Hipwell2014). Comparative studies of children of mothers with BPD versus other maternal psychopathologies are scarce, limiting our understanding of whether observed ER difficulties are specific to BPD or reflect broader transdiagnostic effects.
A related unresolved question, in both childhood and adulthood, concerns which ER strategies are associated with BPD and under which situational conditions. In the adult literature, ER strategies are typically classified as adaptive (e.g., problem-solving, cognitive reappraisal) or maladaptive (e.g., rumination, suppression; Aldao & Nolen-Hoeksema, Reference Aldao and Nolen-Hoeksema2012), with adaptive strategies supporting effective regulation and maladaptive strategies reflecting difficulties that contribute to the development and maintenance of psychopathology (Aldao et al., Reference Aldao, Nolen-Hoeksema and Schweizer2010; Dryman & Heimberg, Reference Dryman and Heimberg2018; Lincoln et al., Reference Lincoln, Schulze and Renneberg2022). More recent work highlights that ER effectiveness depends on context, emphasizing the importance of flexible strategy use (Aldao et al., Reference Aldao, Sheppes and Gross2015; Navas-Casado et al., Reference Navas-Casado, García-Sancho and Salguero2023; Pruessner et al., Reference Pruessner, Barnow, Holt, Joormann and Schulze2020). Consistent with these perspectives, our study provides an initial approach to the concept of regulatory flexibility by examining children’s ER variability together with their use of adaptive and maladaptive strategies. To our knowledge, this situation-specific, state-level assessment has not previously been applied to young children at elevated risk, such as offspring of mothers with BPD. Although this operationalization does not capture contextual flexibility per se, it offers a first step toward understanding early forms of regulatory adaptability in this population and helps address the gap in situation-specific assessments of ER. Accordingly, ER behaviors in this study were categorized as adaptive or maladaptive based on their situation-specific adaptiveness.
Beyond this, notable gaps remain in the literature, particularly regarding the use of behavioral observation methods and the examination of ER across a broader age range in young children (cf. Gratz et al., Reference Gratz, Kiel, Latzman, Elkin, Moore and Tull2014; White et al., Reference White, Flanagan, Martin and Silvermann2011). Addressing these gaps is important, as observational approaches can provide insights beyond self- and other-report measures. Examining ER across a broad age range of early developmental stages in children of parents with BPD, when mental disorders are still relatively rare, may help identify ER patterns that serve as early indicators of later BPD-related psychopathology.
To pursue this aim, the present multicenter study used behavioral observation methods to assess ER in children of mothers with BPD aged six months to six years. This age range was selected to allow the observational task to be implemented as early as possible, while ensuring it remained feasible and comparable across younger and older children. ER was compared among children of mothers with BPD (C-BPD) to children of mothers with anxiety and/or depressive disorders (C-AD/D) and to children of mentally healthy mothers (C-CON). Based on prior findings (Barnow et al., Reference Barnow, Spitzer, Grabe, Kessler and Freyberger2006, Reference Barnow, Aldinger, Arens, Ulrich, Spitzer, Grabe and Stopsack2013; Bartsch et al., Reference Bartsch, Roberts, Davies and Proeve2015; Gratz et al., Reference Gratz, Kiel, Latzman, Elkin, Moore and Tull2014, Reference Gratz, Myntti, Kiel, Kurtz and Tull2024; Weiss et al., Reference Weiss, Zelkowitz, Feldman, Vogel, Heyman and Paris1996), we hypothesized that (1) C-BPD would exhibit more unfavorable ER strategies than C-AD/D and C-CON and (2) that C-AD/D would also display more unfavorable ER strategies than C-CON. These hypotheses were preregistered at the German Clinical Trials Register (DRKS; ID: DRKS00020460, Link: https://drks.de/search/de/trial/DRKS00020460) prior to data collection.
Methods
Study design
The data originates from the longitudinal, multicenter, randomized controlled trial “ProChild” (study protocol: Rosenbach et al., Reference Rosenbach, Heinrichs, Kumsta, Schneider and Renneberg2022), which aims to prevent child maltreatment and promote mental health in children of mothers with BPD through the parenting intervention “Parenting Skills for Mothers with BPD” (Rosenbach et al., Reference Rosenbach, Buck-Horstkotte and Renneberg2020), designed for mothers of children up to six years old. The data in this study comprises the cross-sectional results of the ER task. Data were managed using REDCap hosted at Charité-BIH Clinical Study Center (Harris et al., Reference Harris, Taylor, Thielke, Payne, Gonzalez and Conde2009, Reference Harris, Taylor, Minor, Elliott, Fernandez, O’Neal, McLeod, Delacqua, Delacqua, Kirby and Duda2019). Ethical approval was sought by the German Society for Psychology (German abbreviation: DGPs; No. RennebergBabette2019-07-29VADM).
After recruitment, mothers were first contacted for a telephone screening to assess inclusion and exclusion criteria for both mother and child. Eligible dyads then provided informed consent before participating in a clinical interview, during which sociodemographic information and maternal and child’s psychopathology were assessed. Subsequently, mothers and children attended a laboratory session where they completed the ER task.
Recruitment
Recruitment took place via social media and flyers handed out in psychiatric hospitals and various medical practices across the Berlin, Bochum, Bremen, and Bielefeld regions. Mothers and their children were included if the child was between six months and six years of age, and the mother met one of the following criteria: A current or lifetime diagnosis of BPD, a current or lifetime (up to the birth of the index child) anxiety and/or depressive disorder, or no mental disorder. If mothers with BPD also met criteria for current or lifetime anxiety and/or depressive disorders, they were included only in the BPD group. Additional inclusion criteria were regular weekly contact between mother and child and sufficient German language proficiency. Mothers with BPD had to have already completed therapy or had to be currently in therapy for their BPD symptoms. Children had to be able to sit independently and grasp objects purposefully. Exclusion criteria for mothers included endangerment of the child’s welfare, acute suicidality, psychotic symptoms, alcohol or drug dependency, or a diagnosed intellectual disability. Children with motor or vision-related disabilities were also excluded.
Participants
A total of 351 German speaking mother–child dyads were included in the study. For 31 dyads (8.8%), no video recordings were available due to participant dropout prior to the ER task. Additionally, two dyads were excluded because the child was older than six years at the time of inclusion. The final sample consisted of N = 318 mother–child dyads (n = 158 in the C-BPD group, n = 64 in the C-AD/D group, and n = 96 in the C-CON group). A post-hoc power analysis for a one-way MANOVA was performed in G*Power 3.1. The model included 12 dependent variables (duration, frequency, latency × four strategies) and three groups. A multivariate effect size of f = 0.10, α = 0.0167, and power = 0.90 were assumed, resulting in a total required sample size of N = 180 (60 per group).
Within the recruited sample, mothers had a mean age of 33.60 years (SD = 5.93; range: 17–52 years). Children had a mean age of 39.41 months (SD = 22.16; range: 6–84 months). Of the children, 53.5% were female, with no significant differences between groups (Appendix, Table 1). Mothers with BPD were significantly younger than mentally healthy mothers. Both clinical groups showed lower educational levels compared to the mentally healthy group (Appendix, Table 2).
Material
Sociodemographic information
To assess sociodemographic information, we used the sociodemographic section of the German diagnostic interview for mental disorders in toddlers (German abbreviation: Kleinkind-DIPS; Schneider et al., in preparation). For this study, the variables child gender, child age, maternal age, and maternal education were used.
Maternal psychopathology
Mothers were assigned to diagnostic groups (mothers with BPD, mothers with AD/D or mentally healthy mothers) based on a structured diagnostic interview (Structured Clinical Interview for DSM 5; SCID-5-CV and SCID-5-PD; Beesdo-Baum et al., Reference Beesdo-Baum, Zaudig and Wittchen2019). In addition, maternal psychopathology was assessed using the German version of the Brief Symptom Inventory (BSI; Derogatis, Reference Derogatis1975; Franke, Reference Franke2000), which includes items such as “the feeling of being worthless” or “the feeling of being tense or excited,” the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, Reference Gratz and Roemer2004), with items such as “when I have negative feelings, I lose control,” and the short version of the BPD-specific Questionnaire of Thoughts and Feelings (QTF, Renneberg & Seehausen, Reference Renneberg and Seehausen2010) with items such as “close interpersonal relationships are threatening”.
For further analyses of the BSI, we used the Global Severity Index (GSI) as it is considered the most sensitive indicator of psychological distress (Franke, Reference Franke2000). The GSI reflects overall symptom distress and has shown good reliability and validity in German clinical samples (Crameri et al., Reference Crameri, Schuetz, Andreae, Koemeda, Schulthess, Tschuschke and von Wyl2016; Franke et al., Reference Franke, Ankerhold, Haase, Jäger, Tögel, Ulrich and Frommer2011, Reference Franke, Jaeger, Glaesmer, Barkmann, Petrowski and Braehler2017; Piersma et al., Reference Piersma, Reaume and Boes1994; Sadlonova et al., Reference Sadlonova, Löser, Celano, Kleiber, Broschmann and Herrmann-Lingen2022). In our sample, Cronbach’s alpha for the BSI scales ranged from acceptable to good (α = .711 to .854), except for the additional items, showing poor reliability (α = .629).
For further analyses of the DERS, we used the total score, as it is commonly employed in clinical samples (Erez & Gordon, Reference Erez and Gordon2025; Hallion et al., Reference Hallion, Steinman, Tolin and Diefenbach2018; Harrison et al., Reference Harrison, Sullivan, Tchanturia and Treasure2010; Haynos et al., Reference Haynos, Roberto and Attia2015; Staples & Mohlman, Reference Staples and Mohlman2012), including samples of participants with BPD (Osborne et al., Reference Osborne, Michonski, Sayrs, Welch and Anderson2017). Cronbach’s alpha for the DERS subscales in our sample ranged from good to excellent (α = .820 to .932), with the total score demonstrating excellent internal consistency (α = .970).
The QTF is designed to capture the characteristic cognitions and feelings of individuals with BPD (Renneberg et al., Reference Renneberg, Schmidt-Rathjens, Hippin, Backenstrass and Fydrich2005). In the present sample, internal consistency was excellent (Cronbach’s α = .94).
Children’s mental health
Children’s mental health was assessed using the Kleinkind-DIPS (Schneider et al., in preparation), a structured clinical interview for mental disorders in toddlers that combines the Kinder-DIPS (Schneider et al., Reference Schneider, Pflug, In-Albon and Margraf2017) and the Baby-DIPS (Popp et al., Reference Popp, Fuths, Seehagen, Bolten, Gross-Hemmi, Wolke and Schneider2016). Previous studies of both source interviews reported good to excellent interrater reliability, as well as moderate to good agreement with clinical judgments for the Kinder-DIPS (Neuschwander et al., Reference Neuschwander, In-Albon, Adornetto, Roth and Schneider2013; Popp et al., Reference Popp, Fuths, Seehagen, Bolten, Gross-Hemmi, Wolke and Schneider2016; Weber et al., Reference Weber, Christiansen and Chavanon2020). The interview evaluates common mental health problems in children up to six years; in the present study, assessments were based on maternal report. Interviewers were advanced Master’s students in clinical psychology or psychologists in postgraduate training toward licensure as psychotherapists. All interviewers received structured training in the administration of the instrument, including reliability checks; certification required agreement on diagnosis and severity in two interviews. Any diagnostic questions or uncertainties were continuously supervised during the study. For the present exploratory analyses, the categorical variable (diagnosis vs. no diagnosis) was used.
Behavioral observation task
To measure ER, age-specific tasks were adapted from the Laboratory Temperament Assessment Battery (Lab-TAB; Goldsmith et al., Reference Goldsmith, Reilly, Lemery and Longley1999; Goldsmith & Rothbart, Reference Goldsmith and Rothbart1999). For children aged six months to three years, we used the Toy Retraction Task (Lab-TAB Prelocomotor Version 3.1; Goldsmith & Rothbart, Reference Goldsmith and Rothbart1999, Figure 1a) while children were sitting in a high-chair. For children aged three years and one month to six years, we developed a new task called Toy in Glass, inspired by the Attractive Toy in a Transparent Box Task (Lab-TAB, Preschool Version; Goldsmith et al., Reference Goldsmith, Reilly, Lemery and Longley1999; Figure 1b). Both tasks were based on the same core principle: During a waiting phase, the children’s preferred toy was placed within sight but out of reach, creating negative emotions to trigger ER strategies. The purpose of the tasks was not further explained to the child to create a higher potential for frustration. According to previous literature, the younger age group waited for three minutes, the older group for six minutes (Gagne et al., Reference Gagne, van Hulle, Aksan, Essex and Goldsmith2011; Thacker, Reference Thacker2011)
Emotion regulation tasks for children form six months to six years. Notes. Figure (a) shows the ER task Toy Retraction (Lab-TAB Prelocomotor Version 3.1.; Goldsmith & Rothbart, Reference Goldsmith and Rothbart1999). Figure (b) shows the ER task Toy in Glass (adapted from Lab-TAB, Preschool Version; Goldsmith et al., Reference Goldsmith, Reilly, Lemery and Longley1999).

Procedure
Each behavioral observation task took place in the laboratory and was recorded with four cameras, positioned at the front, back, side, and on the ceiling. Sessions began with a warm-up phase, during which the mother and child played together with age-appropriate toys to help the child become comfortable. During the ER task, the mother was seated with her back to the child and instructed to appear occupied by completing questionnaires. She was asked to respond to the child’s bids for attention with neutral phrases such as “I can’t right now” or “I’m busy right now.” This setup was designed to capture children’s own ER strategies, rather than those shaped by maternal co-regulation. The experimenter remained in the control room during the waiting phase.
Before the waiting phase, the experimenter presented the child with two toy options and asked which one they preferred (Appendix, Figure 1). The selected toy was then placed out of reach. PhD students and postdoctoral researchers from the department with children in the age range of those included in the study were consulted in advance to ensure that the toys were developmentally appropriate and appealing.
Coding of emotion regulation
During the warm-up phase, children’s affect and interest in the preferred toy were globally coded, meaning a single overall score was assigned for the entire phase. In the subsequent waiting phase, affect and ER were assessed and coded separately, second-by-second (Braungart-Rieker et al., Reference Braungart-Rieker, Garwood, Powers and Wang2001). After the waiting phase, children’s interest in the preferred toy was again globally coded. For the second-by-second data, duration, latency, and frequency of each affect and ER strategy were calculated.
Coders were blind to maternal diagnostic group membership, measurement time point, research center, and hypotheses. The coding system was adapted from prior literature (Bolten et al., Reference Bolten, Nast, Skrundz, Stadler, Hellhammer and Meinlschmidt2013; Diener et al., Reference Diener, Mangelsdorf, McHale and Frosch2002; Ekas et al., Reference Ekas, Braungart-Rieker, Lickenbrock, Zentall and Maxwell2011; Möller et al., Reference Möller, Majdandžić and Bögels2014). Coders underwent training until they achieved an inter-rater reliability above 85%. Coders were the first author and Master’s degree students. In total, 42.73% of the 318 videos were double-coded. Coding was carried out using Mangold INTERACT for second-by-second and global coding (Mangold, Reference Mangold, Böttger, Jensen and Jensen2018).
Affect coding
During the waiting phase, positive affect was coded second-by-second when the child appeared satisfied (intensity level one), smiled (intensity level two), or showed excitement (intensity level three). Negative affect was coded second-by-second when the child appeared dissatisfied (intensity level one), moaned or whined (intensity level two), cried (intensity level three), or lost control (intensity level four; Appendix, Table 3). The waiting phase was terminated if the child displayed 20 seconds or more of negative affect at intensity level three and/or five seconds or more at intensity level four. During the warm-up phase, positive, negative, and neutral affect were coded as global codes using the same intensity levels. Cohen’s Kappa for global affect coding during the warm-up phase indicated almost perfect agreement (κ = .916; Landis & Koch, Reference Landis and Koch1977). For affect coding during the waiting phase, ICC values ranged from .673 to 1.00, indicating good to excellent reliability based on Cicchetti (Reference Cicchetti1994) guidelines.
Emotion regulation coding
For ER, we developed a descriptive coding system based on Braungart-Rieker et al. (Reference Braungart-Rieker, Garwood, Powers and Wang2001) and Perry et al. (Reference Perry, Calkins and Bell2016). ER was coded second-by-second during the waiting phase when the children oriented toward the mother (mother orientation), themselves (self-orientation), the preferred toy (toy orientation), or the environment (environmental orientation). All strategies were categorized as either adaptive or maladaptive according to their situation-specific adaptiveness (Appendix, Table 4). This categorization was conducted to capture child behaviors related to difficulties in ER as described in BPD, which are characterized by situationally inappropriate or intense expressions of anger and thus reflect maladaptive regulation in the given context. In the context of the ER task, in which children were required to wait for a desirable toy, maladaptive behaviors included, for example, maladaptive mother-oriented behaviors, such as verbal expressions of intense frustration or anger directed toward the mother. In contrast, adaptive behaviors in this situation included, for example, seeking support from the mother (see Appendix, Table 4). To test our hypotheses, unfavorable strategies are conceptualized as the more frequent and prolonged use of maladaptive ER strategies.
ER variability was calculated for adaptive strategies by examining how many different strategies (mother-, self-, toy-, or environment orientation) a child displayed during the waiting phase. Interrater reliability for coding adaptive ER was high, with ICC values for ER strategies ranging from .845 to .988. Interrater reliability for coding maladaptive ER could not be interpreted due to an insufficient number of observed maladaptive ER cases.
Manipulation check
In addition to affect and ER codes, interest in the preferred toy was globally coded before and after the waiting phase. Interest was classified as approach or avoidance (Appendix, Table 5). Cohen’s kappa indicated perfect interrater reliability (κ = 1.00) for interest ratings before and after the waiting phase.
Affect and interest codes served as manipulation checks to assess whether the task induced negative affect and whether the child was interested in the preferred toy. In addition, mothers reported whether the child was already familiar with the desirable toy and whether the child showed interest. After warm-up and waiting phases, mothers also completed questionnaires on mood and arousal for themselves and their child on the Self-Assessment-Manikin-Scales (SAM; Bradley & Lang, Reference Bradley and Lang1994).
Analyses
Statistical analyses
All analyses were conducted using SPSS Statistics, Version 29. Covariates were included in the statistical models if they differed significantly between maternal diagnostic groups (BPD, AD/D, and CON). The initial analyses served as manipulation checks, assessing affect, mood, and arousal during the waiting phase, as well as interest in and familiarity with the preferred toy. Each of these variables were analyzed using t-tests. To account for varying wait times, the percentage of time and relative frequency of each affect expression and ER strategy were calculated based on the actual task duration. In cases of early termination, durations were adjusted accordingly.
To examine whether children who terminated the ER task early or reached the toy differed from those who completed it, regression analyses were conducted using sociodemographic variables and maternal diagnostic group as predictors.
To test hypotheses (1) and (2) regarding children’s use of ER strategies in relation to maternal psychopathology, separate MANCOVAs were conducted for the duration, latency, and frequency of ER strategies, with Holm-Bonferroni corrected p-values. Additionally, an ANCOVA was performed to examine differences in children’s variable use of ER strategies across maternal diagnostic groups. Before analyses, intercorrelations among the dependent variables were examined. None exceeded the critical threshold (r > .90; Tabachnick et al., Reference Tabachnick, Fidell and Ullman2019), suggesting that the dependent variables are unlikely to be redundant. Regarding the covariates, collinearity statistics showed no indication of multicollinearity (all VIFs < 2).
For exploratory, non–pre-registered analyses, the models were repeated using categorical measures of maternal psychopathology derived from cutoffs on dimensional scales, categorical measures of children’s mental health and children’s age group as independent variables.
The data, codebook, and analysis scripts are publicly available in the PsychArchives repository (Bunz, Reference Bunz2026; Bunz et al., Reference Bunz, Derhardt, Seehagen, Heinrichs, Kumsta, Renneberg and Schneider2026).
Missing values
Due to missing data, complete video recordings of all ER task phases were unavailable for 52 of 318 mother–child dyads (16.3%). In five cases (1.6%), video data were available only for the warm-up phase, but not for the waiting phase. In 47 cases (14.8%), the waiting phase was terminated prematurely. Among these, 29 cases (9.1%) ended early due to the child displaying strong negative affect. In 10 cases (3.1%), the child managed to reach the toy before the waiting time had elapsed. In four cases (1.3%), the experimenter ended the task prematurely by mistake, and in another four cases (1.3%), the child left the room or tried to leave the chair, leading to early task termination for safety. None of these cases were excluded; instead, available phases or shortened waiting durations were coded accordingly.
Results
Missing data analyses
To examine whether sociodemographic variables (child’s and mother’s age, child’s gender, and maternal education) and maternal diagnostic group were associated with termination of the ER task due to elevated negative affect during the waiting phase, two logistic regression analyses were conducted. Separate models were estimated for child age and diagnostic group, as these variables are confounded (see Appendix, Table 1). To account for multiple testing across the two models, p-values were adjusted using the Bonferroni–Holm correction. Only the model including child age as a predictor was statistically significant (child age: χ 2(7) = 65.53, p < .001, Nagelkerke R 2 = .41; diagnostic group: χ 2(8) = 9.33, p = .315, Nagelkerke R 2 = .06). Within this model, children’s age emerged as a significant negative predictor, indicating that younger children were more likely to have the task terminated by the experimenter due to elevated negative affect (Appendix, Table 6).
Manipulation check
According to affect duration and frequency, children exhibited significantly longer and more negative than positive affect during the waiting phase (duration: t(312) = 14.631, p < .001, Cohen’s d = .827; frequency: t(312) = 13.13, p < .001; Cohen’s d = .742; Appendix, Table 7). They showed more approach than avoidance before (97.2% vs. 1.9%) and after (90.6% vs. 1.3%) the waiting phase. According to mothers, 69.2% of the children did not know the toy before the study, while 16% of the children were only slightly familiar with it. Regarding toy attractiveness, 56.3% of mothers rated the toy as very attractive, 34.6% as somewhat attractive, and 5.7% as not attractive.
Regarding the mood and arousal ratings of the SAM-Scales, mothers rated their child’s mood as more positive before the waiting phase than after (t(301) = –14.673, p < .001, Cohen’s d = –.844). They rated their child’s arousal as higher after the waiting phase than before (t(296) = 7.765, p < .001, Cohen’s d = .451). The same pattern was found for mothers’ own ratings of mood (t(300) = –10.448, p < .001, Cohen’s d = –.602), and arousal (t(292) = 8.200, p < .001, Cohen’s d = .479; Appendix, Table 8).
Emotion regulation
Adaptive and maladaptive strategies
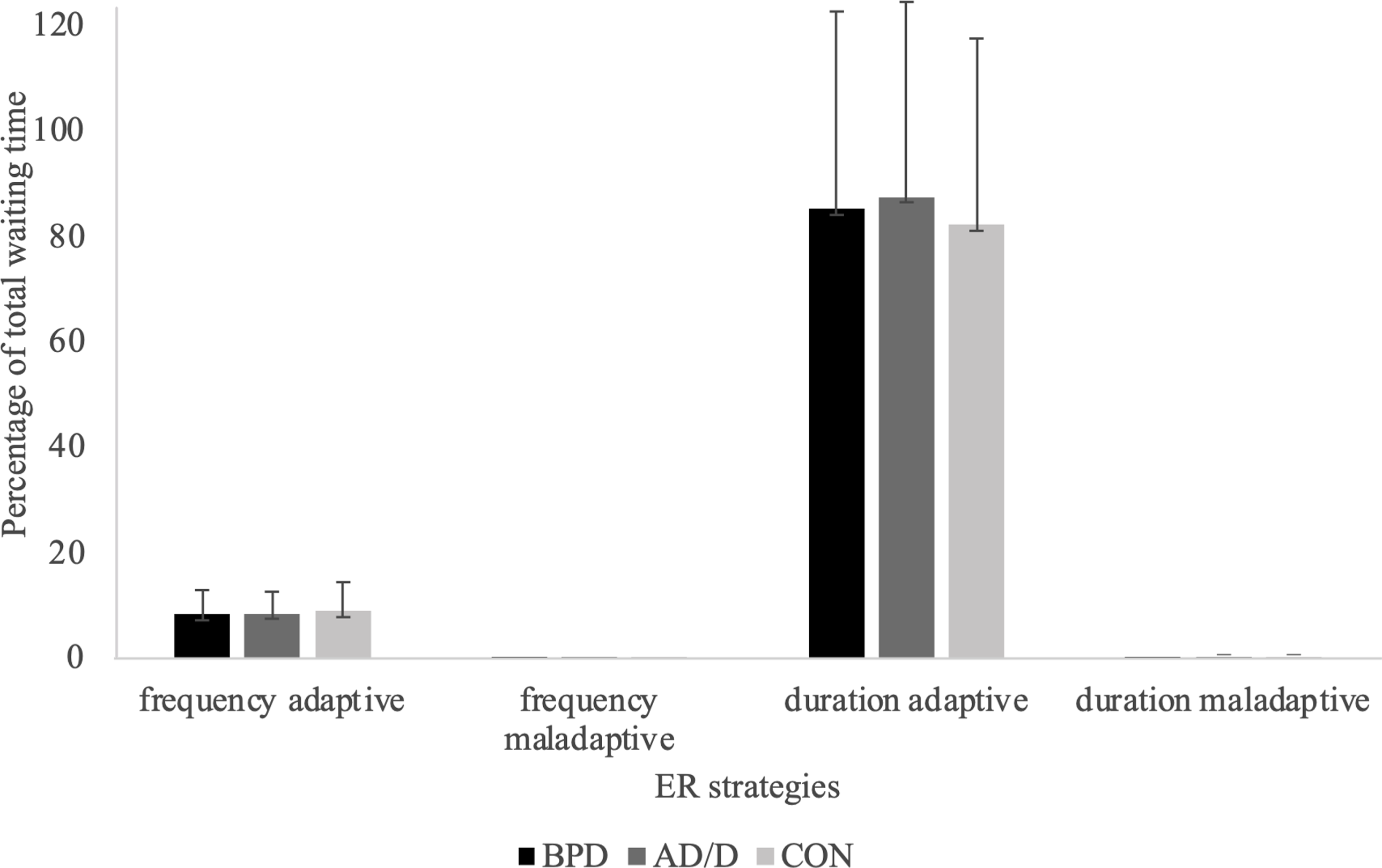
Based on the classification of ER strategies as adaptive and maladaptive, children predominantly used adaptive strategies during the waiting phase (M = 84.60%, SD = 36.74), whereas maladaptive strategies were almost absent (M = 0.03%, SD = 0.32) across all maternal diagnostic groups (Figure 2). Similarly, the average relative frequency of adaptive strategies was 8.42 (SD = 4.76), while maladaptive strategies were rarely used (M = 0.01, SD = 0.06; Figure 2). Due to this insufficient data for maladaptive strategies, the following analyses focused on children’s adaptive ER strategies.
Duration and frequency of emotion regulation strategies across maternal diagnostic groups. Notes. The standard deviation exceeds 100% because multiple strategies could be used simultaneously, resulting in overlapping percentages.
To examine group differences in adaptive strategy use, three MANCOVAs with Holm-Bonferroni correction were conducted. Dependent variables were the duration, latency, and frequency of adaptive mother-, self-, toy-, and environment-oriented strategies. Maternal diagnostic group was the independent variable; maternal and child age were entered as covariates due to significant group differences (Appendix, Tables 1 and 2). Maternal education was included as a fixed factor because it was categorical.
Results revealed no significant main effects of maternal diagnostic group on children’s duration, latency, and frequency of adaptive ER strategies. The covariate children’s age had a significant main effect on these measures, indicating a moderate to large effect size (Cohen, Reference Cohen2009; Appendix, Tables 9 and 10). The covariates did not significantly interact with maternal diagnostic group (Appendix, Table 10).
Emotion regulation variability
To examine the effect of maternal diagnostic group on children’s variable use of adaptive ER strategies, an ANCOVA was conducted. Children’s and mother’s age were included as covariates, and maternal education as a fixed factor. Consistent with findings on duration, latency, and frequency, no significant differences between maternal diagnostic groups emerged in the variable use of adaptive ER strategies. A small but significant main effect of children’s age was found (Cohen, Reference Cohen2009; Appendix, Table 11).
In light of these findings, hypotheses 1 and 2, which proposed that ER strategies of C-BPD would differ from those of C-AD/D and C-CON, with both clinical groups displaying more frequent and prolonged maladaptive strategies, were not supported. Children showed almost no maladaptive strategies across all groups. No group differences were found in the use of adaptive ER strategies, neither in duration, frequency, latency, nor variability of strategy use. Only significant age effects were observed for these variables.
Explorative analyses
Categorical maternal psychopathology (based on dimensional cutoffs)
Exploratorily, we examined whether categorical measures of maternal psychopathology derived from cutoffs on dimensional scales would produce different results for children’s ER strategies compared to the prior categorical diagnostic groups. To this end, we used the Global Severity Index (GSI) from the Brief Symptom Inventory (Franke, Reference Franke2000), the overall score from the Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, Reference Gratz and Roemer2004) and the cutoff score of the Questionnaire of Thoughts and Feelings (QTF; Renneberg & Seehausen, Reference Renneberg and Seehausen2010; descriptive statistics on group differences are displayed in Appendix, Table 12). As specified in the BSI manual, T-scores ranged from 20 to 80. Participants were grouped by GSI T-scores into below average (20–49), average (50–60), and above average (>60; clinically significant). Separate Holm-Bonferroni corrected MANCOVAs for duration, latency, and frequency of adaptive ER strategies showed no effects of GSI groups. Consistent to the main analyses, children’s age affected duration, latency, and frequency, with a moderate to large effect size (Cohen, Reference Cohen2009; Appendix, Table 13).
In the absence of standardized clinical cutoffs for the DERS, prior studies suggest a clinical range for the total score between 80 and 127 (Harrison et al., Reference Harrison, Sullivan, Tchanturia and Treasure2010; Haynos et al., Reference Haynos, Roberto and Attia2015; Staples & Mohlman, Reference Staples and Mohlman2012). Additionally, samples with BPD often exceed scores of 100 (Osborne et al., Reference Osborne, Michonski, Sayrs, Welch and Anderson2017). Based on this, participants were categorized into low (<80) and high (>80) emotional dysregulation groups. Separate Holm-Bonferroni corrected MANCOVAs showed no significant effect of maternal DERS group on children’s adaptive ER strategies. However, children’s age had a significant moderate to large effect on duration, latency, and frequency of these strategies (Cohen, Reference Cohen2009; Appendix, Table 14).
According to the QTF, participants were categorized based on the provided cutoff score of 2.68 for suspected BPD, resulting in two groups: below and above the cutoff. Separate Holm–Bonferroni corrected MANCOVAs for duration, latency, and frequency revealed no significant effects of the QTF groups. Consistent with the main analyses, children’s age significantly affected duration, latency, and frequency, with moderate to large effect sizes (Cohen, Reference Cohen2009; Appendix, Table 15).
Categorical measures of children’s mental health
In addition to maternal psychopathology, we exploratively examined whether children’s adaptive ER was associated with the presence or absence of a diagnosis, as assessed by the Kleinkind-DIPS. In our sample, 28.6% of the children met diagnostic criteria (see Appendix, Table 16 for frequencies of specific diagnoses). However, Holm-Bonferroni–corrected MANCOVAs revealed no significant associations between children’s diagnostic status and the duration, latency, or frequency of adaptive ER strategies. Significant effects were observed only for children’s age, with medium to large effect sizes for latency and frequency measures (Appendix, Table 17).
Effects of children’s age
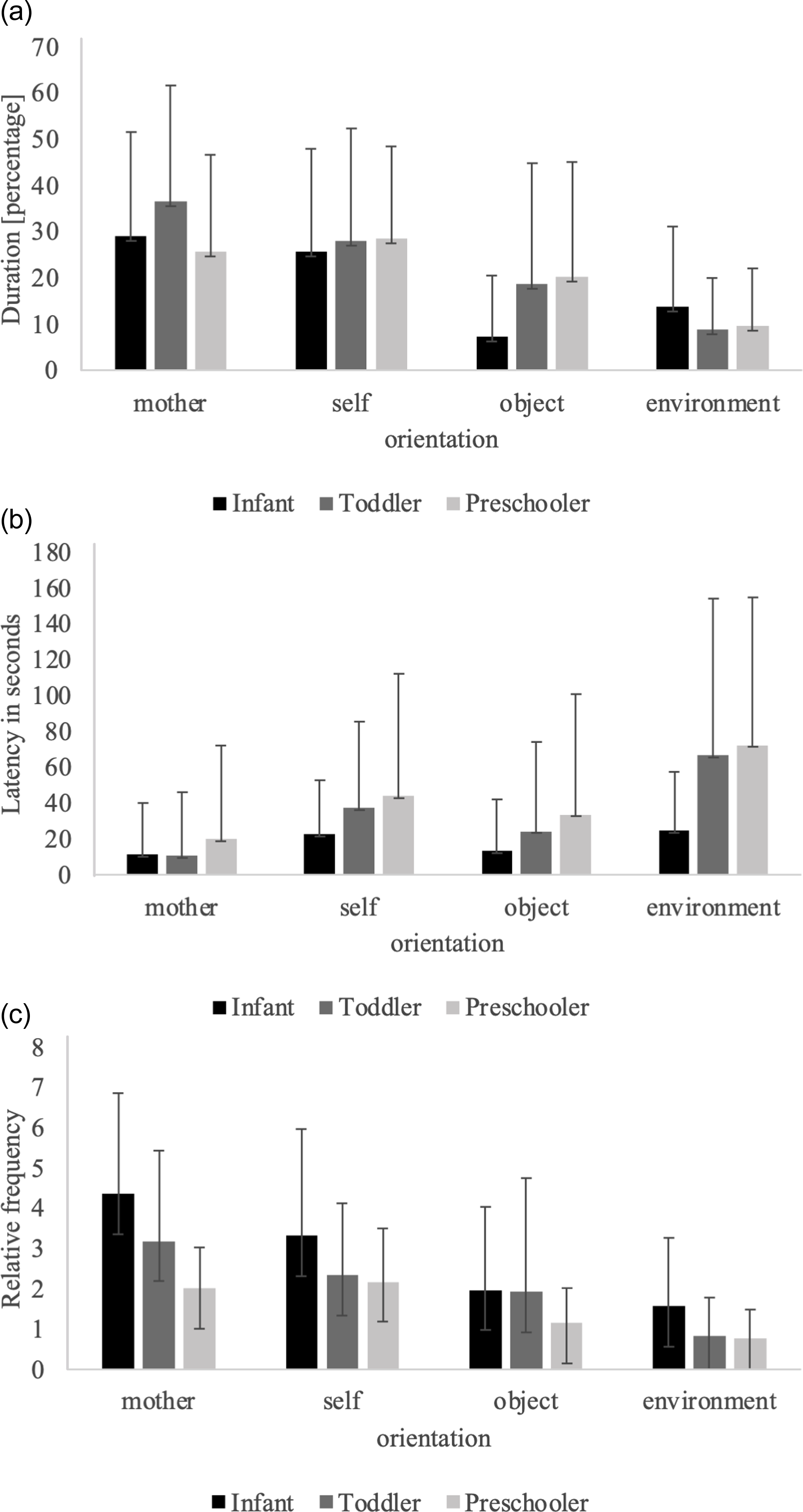
Due to the main effects of children’s age on duration, latency, and frequency of adaptive ER strategies, the effect of age was further explored. Children were categorized into three age groups with approximately equal frequencies: Infants (up to 23 months), toddlers (>23 months up to 48 months), and preschool aged children (>48 months up to 84 months; Appendix, Table 18). Three separate Holm-Bonferroni corrected MANOVAs with Games-Howell post-hoc tests were conducted for duration, latency, and frequency of adaptive ER strategies, using children’s age groups as independent variable. Results showed significant effects of age group on all three measures (Appendix, Table 19). Post-hoc tests for duration showed that toddlers spent significantly more time oriented toward their mother than preschoolers, while toddlers and preschoolers spent more time oriented toward the preferred toy (Figure 3a, Appendix, Table 20). Older children had significantly longer latencies than younger children in self-, environment-, and toy-oriented behaviors (Figure 3b, Appendix, Table 20). Frequency analyses revealed that younger children displayed significantly more frequent mother-, self-, toy-, and environment-oriented behaviors than older children (Figure 3c, Appendix, Table 20).
Duration, latency, and frequency of adaptive emotion regulation strategies across age groups. Notes. Figure (a) displays the duration of adaptive emotion regulation strategies across age groups, expressed as a percentage of total waiting time. Figure (b) shows the latency of adaptive emotion regulation strategies across age groups. Figure (c) presents the frequency of adaptive emotion regulation strategies across age groups.
An exploratory ANOVA with Games-Howell post-hoc tests was conducted to examine ER variability across age groups (Appendix, Table 21). Results indicated a small but significant main effect of age on ER variability (F(2, 310) = 3.795, p = .024, η2 = .024). Post-hoc tests revealed that preschoolers exhibited significantly more ER variability than infants (MD = .294, SE = .117, p = .034, 95%-CI [.018, .571]).
Discussion
This study aimed to investigate ER in young children of mothers with BPD as a potentially disorder-specific, transgenerationally transmitted pattern. We compared ER in C-BPD with that in children of mothers with anxiety/depressive disorders and mentally healthy mothers using negative emotions inducing behavioral observation tasks.
Task validation
Manipulation checks on interest, mood, arousal, toy attractiveness ratings and affect coding indicated that the ER tasks successfully induced negative affect and that the children were engaged with and found their desirable toy attractive. Delay of gratification tasks like these are commonly used in ER research to examine behavioral responses to negative emotions in young children (Bunz et al., under review; Planalp et al., Reference Planalp, Van Hulle, Gagne and Goldsmith2017), but, to our knowledge, they have not previously been employed to assess ER in offspring of mothers with BPD.
Demographic patterns
Beyond ER, demographic analyses showed that mothers with BPD were younger than mentally healthy mothers. This aligns with research indicating that teenage and unplanned pregnancies are more common among individuals meeting BPD criteria compared to those without such diagnoses (De Genna et al., Reference De Genna, Feske, Larkby, Angiolieri and Gold2012) and may be related to impulsivity and risk-taking behaviors, including unprotected sex (Barker et al., Reference Barker, Romaniuk, Cardinal, Pope, Nicol and Hall2015; Sansone et al., Reference Sansone, Barnes, Muennich and Wiederman2008).
Children’s emotion regulation strategy use
Association with maternal psychopathology
Regarding our main research question, and contrary to previous literature (Macfie et al., Reference Macfie, Swan, Fitzpatrick, Watkins and Rivas2014; White et al., Reference White, Flanagan, Martin and Silvermann2011; Zalewski et al., Reference Zalewski, Stepp, Scott, Whalen, Beeney and Hipwell2014), our findings did not reveal a BPD-specific ER pattern in offspring. Additionally, no general association was found between maternal psychopathology and children’s ER strategies. This was true for both categorical measures of maternal psychopathology, as well as across ER measures including duration, latency, frequency, and variability. The null findings remained consistent whether ER strategies were analyzed broadly (adaptive and maladaptive) or in finer subcategories (mother-, self-, toy-, environment-oriented strategies).
Some previous studies have likewise reported no significant associations between children’s ER and maternal BPD diagnosis (Gratz et al., Reference Gratz, Kiel, Latzman, Elkin, Moore and Tull2014; Wilson & Durbin, Reference Wilson and Durbin2012). However, the main body of literature suggests a positive association between children’s ER difficulties and parental BPD psychopathology (cf. Eyden et al., Reference Eyden, Winsper, Wolke, Broome and MacCallum2016). These inconsistencies may reflect differences in how ER is measured and conceptualized, as it overlaps with coping and temperament concepts (Mazefsky et al., Reference Mazefsky, Conner, Breitenfeldt, Leezenbaum, Chen, Bylsma and Pilkonis2021). In children of mothers with BPD, ER has predominantly been assessed as a trait construct, using parent–child interactions or self- and parent reports (e.g., Abela et al., Reference Abela, Skitch, Auerbach and Adams2005; Barnow et al., Reference Barnow, Spitzer, Grabe, Kessler and Freyberger2006, Reference Barnow, Aldinger, Arens, Ulrich, Spitzer, Grabe and Stopsack2013; White et al., Reference White, Flanagan, Martin and Silvermann2011). The present study adds new insights by observing children’s state-based ER strategies in an emotionally challenging situation. By restricting parent–child interactions, the task highlights children’s own use of ER strategies, which may help explain the absence of group differences observed in our study, compared to previous research that focused on ER within parent–child interactions (cf. White et al., Reference White, Flanagan, Martin and Silvermann2011). Another possible explanation for the lack of association between maternal psychopathology and children’s ER in this study may be related to differences in measurement, as children’s ER was assessed as a state measure, while maternal psychopathology was assessed as a trait. Consistent with this, Nolen-Hoeksema et al. (Reference Nolen-Hoeksema, Wolfson, Mumme and Guskin1995) found that the mother’s negative affect state during a mother–child task, but not her (trait) psychopathology as measured by self-reports, was related to the preschool child’s behavior and affect during this task.
Building on this, it is important to note that we examined ER in an at-risk sample rather than in clinically diagnosed children. Although offspring of parents with mental disorders are generally considered at increased risk, the absence of an association between maternal psychopathology and children’s ER in our study may reflect resilience processes that buffer against this risk. Protective factors, such as supportive caregiving, a positive family climate, or low negative reactivity in the child, may buffer against negative effects, allowing children to develop adaptive ER despite exposure to maternal symptoms (Morris et al., Reference Morris, Silk, Steinberg, Myers and Robinson2007). This interpretation is supported by previous research showing that more than half of offspring of parents with mental disorders do not develop psychosocial difficulties (Mowbray et al., Reference Mowbray, Lewandowski, Bybee and Oyserman2004; van Santvoort et al., Reference van Santvoort, Hosman, Janssens, van Doesum, Reupert and van Loon2015). Regression analyses further showed that the emotion-inducing task was challenging for all children, regardless of maternal diagnosis, suggesting that the task’s demanding nature may have constrained group differences, potentially limiting statistical power to detect subtle effects.
Adaptive and maladaptive emotion regulation
Beyond the null finding regarding the association between children’s ER and maternal psychopathology, a central result of this study is that children showed almost no maladaptive ER strategies. This expands ER literature in early childhood and in children of mothers with BPD in particular, where the distinction between adaptive and maladaptive strategies has rarely been examined (Braet et al., Reference Braet, Theuwis, Van Durme, Vandewalle, Vandevivere, Wante, Moens, Verbeken and Goossens2014; Eyden et al., Reference Eyden, Winsper, Wolke, Broome and MacCallum2016). In our negative emotion-induction task, maladaptive ER were defined as aggressive expressions of ER strategies, conceptually derived from the symptom of inappropriate anger regulation in BPD, and reflecting the accepted view that aggression indicates maladaptive regulation (Calkins et al., Reference Calkins, Gill, Johnson and Smith1999; Gerstein et al., Reference Gerstein, Pedersen y Arbona, Crnic, Ryu, Baker and Blacher2011; Kerr & Schneider, Reference Kerr and Schneider2008). In comparison, the Feel-KJ questionnaire (Grob & Smolenski, Reference Grob and Smolenski2005), classifies adaptive and maladaptive ER strategies based on the strategy itself rather than the observable expression. Another possibility is an outcome-driven interpretation, for example in the coding scheme by Nolen-Hoeksema et al. (Reference Nolen-Hoeksema, Wolfson, Mumme and Guskin1995), higher frequencies of frustration and lower engagement in task persistence or problem-solving are interpreted as indicators of maladaptive regulation. These differing definitions of adaptivity may partly explain inconsistent findings regarding children’s ER across studies, highlighting the need for further conceptual and empirical research in this area (cf. Braet et al., Reference Braet, Theuwis, Van Durme, Vandewalle, Vandevivere, Wante, Moens, Verbeken and Goossens2014).
Since children in our study displayed almost no maladaptive ER strategies, further analyses focused on adaptive strategies. In adult populations, frequent use of maladaptive strategies such as rumination and suppression has been consistently linked to psychopathology, with medium to large effect sizes, whereas less frequent use of adaptive strategies like reappraisal and acceptance showed only small to medium effects (Aldao et al., Reference Aldao, Nolen-Hoeksema and Schweizer2010; Conklin et al., Reference Conklin, Cassiello-Robbins, Brake, Sauer-Zavala, Farchione, Ciraulo and Barlow2015; Lincoln et al., Reference Lincoln, Schulze and Renneberg2022). Although some evidence suggests that, for example, rumination may predict depression (Rood et al., Reference Rood, Roelofs, Bögels, Nolen-Hoeksema and Schouten2009), it remains unclear whether maladaptive ER is a cause or consequence of psychopathology, particularly given the prevalence of cross-sectional designs (Aldao et al., Reference Aldao, Nolen-Hoeksema and Schweizer2010). Some evidence suggests that effortful control, a temperamental factor supporting ER, may moderate the relationship between parenting and later adolescent rumination (Hilt et al., Reference Hilt, Armstrong and Essex2012); but more longitudinal research is needed to clarify these dynamics. This is relevant to our study, as maladaptive ER strategies may not yet have been observable and ER did not differ by children’s diagnostic status. Given that this is the first study to assess ER across an early developmental period, such difficulties may emerge later, potentially alongside more severe or persistent forms of psychopathology.
Emotion regulation variability
Recent adult studies define adaptive and maladaptive strategies based on situational demands, an approach conceptualized as ER flexibility, with initial evidence suggesting that more flexibility is associated with lower levels of psychopathology (Aldao & Nolen-Hoeksema, Reference Aldao and Nolen-Hoeksema2012; Aldao et al., Reference Aldao, Sheppes and Gross2015; Pruessner et al., Reference Pruessner, Barnow, Holt, Joormann and Schulze2020). In children, research on ER flexibility remains limited, focusing mainly on methodological questions and physiological correlates (Myruski & Dennis-Tiwary, Reference Myruski and Dennis-Tiwary2021; Parsafar et al., Reference Parsafar, Fontanilla and Davis2019). Definitional challenges persist, as many child studies assess variability rather than true flexibility, which requires integrating contextual shifts into both design and analysis (Aldao et al., Reference Aldao, Sheppes and Gross2015). Building on these conceptual considerations, the present study investigates ER variability in an at-risk sample as an initial step toward incorporating contextual factors into research on children’s ER.
Age effect on children’s emotion regulation
An additional key finding, revealed by the exploratory analyses, was that ER strategies varied as a function of age. Older children exhibited longer latencies in self-, environment-, and toy-oriented behaviors, indicating better waiting abilities and greater self-control, consistent with the emergence of effortful control in the preschool years (Kochanska et al., Reference Kochanska, Murray and Harlan2000; Zentner & Shiner, Reference Zentner and Shiner2012). They may also have employed cognitive ER strategies not directly observable, explaining these longer latencies. This aligns with evidence that children around five to six years increasingly use cognitive reappraisal as an intentional ER strategy (Willner et al., Reference Willner, Hoffmann, Bailey, Harrison, Garcia, Ng, Cipriano and Brackett2022). Regarding maternal orientation, preschoolers showed descriptively longer latencies than toddlers and infants, suggesting reduced reliance on maternal support. Duration-based analyses similarly indicated that younger children oriented more toward their mothers, while older children focused longer on the preferred toy, reflecting increasing independence and self-regulation as predicted by developmental models (Bornstein & Esposito, Reference Bornstein and Esposito2023; Holodynski & Friedlmeier, Reference Holodynski and Friedlmeier2006) and the emergence of toy exploration in toddlerhood (Grolnick et al., Reference Grolnick, Bridges and Connell1996). The greater reliance on co-regulation in younger children may also explain why task termination due to intense negative affect occurred mainly in this group, likely reflecting distress from the limited maternal interaction in the experimental setup.
Based on both frequency and variability measures, our study found that infants, while showing higher frequency scores across all four strategy categories, used significantly fewer distinct strategies than preschoolers, indicating a more frequent but less varied ER pattern. This is consistent with literature showing that older children possess a broader ER repertoire and can flexibly select strategies according to contextual demands (Calkins & Hill, Reference Calkins and Hill2007; Ponzetti et al., Reference Ponzetti, Spinelli, Coppola, Lionetti, D’Urso, Shah, Fasolo and Aureli2023). It also aligns with adult research linking higher emotional intensity to a higher frequency of ER strategies (Barrett et al., Reference Barrett, Lane, Sechrest and Schwartz2000; Dixon-Gordon et al., Reference Dixon-Gordon, Aldao and De Los Reyes2015; Kozubal et al., Reference Kozubal, Szuster and Wielgopolan2023).
Overall, the similarities between our results and previous developmental studies in healthy populations suggest that our study successfully replicates established findings in an at-risk sample, thereby supporting the validity of our ER tasks, an important prerequisite of the interpretation of our results.
Strengths and limitations
This study has several strengths. We used behavioral observations and employed well-established tasks based on the Lab-TAB protocol, allowing for objective, state-level assessment of ER across a broad range of strategies. Additionally, the ER tasks were consistent with the most widely used definition of ER (Thompson, Reference Thompson1994), as emotions were induced before measuring ER, confirmed by manipulation checks, and goal-directed behaviors were assessed. Age-related differences in ER further supported task validity. Coding was based on previously used coding schemes (Braungart-Rieker et al., Reference Braungart-Rieker, Garwood, Powers and Wang2001; Perry et al., Reference Perry, Calkins and Bell2016) and focused on observable behaviors rather than inferred intent. ER was measured using multiple indices (frequency, latency, duration, and variability), which allowed for a more precise assessment of ER. The relatively large sample, inclusion of both clinical and healthy controls, and wide age range enhanced generalizability and allowed for the assessment of ER as an early predictor of BPD-specific psychopathology.
However, several limitations should be considered. The sample included mothers with both current and lifetime BPD diagnoses, which may have increased heterogeneity within this diagnostic group and thereby attenuated differences between groups. Nevertheless, descriptive statistics on categorical measure of maternal psychopathology derived from cutoffs on a dimensional scale showed that mothers with BPD exhibited the highest levels of psychological stress, ER difficulties, and BPD-specific thoughts and feelings compared with the clinical and healthy control groups, while showing only slightly higher ranges and standard deviations than the clinical control group (Appendix, Table 12). Moreover, contextual factors known to influence children’s emotional development (e.g., paternal mental health, family dynamics, or environmental stressors), were not assessed (Basu & Banerjee, Reference Basu and Banerjee2020; Fisher, Reference Fisher2017; Kvalevaag et al., Reference Kvalevaag, Ramchandani, Hove, Assmus, Eberhard-Gran and Biringer2013). These may partly explain the lack of association between children’s ER and maternal psychopathology. Additionally, differences in measurement, maternal psychopathology assessed as a trait variable and children’s ER assessed as a state variable, may also explain the null findings. Finally, the ER task restricted maternal interaction, which may have disproportionately stressed younger children by limiting access to age-appropriate co-regulation strategies, potentially reducing group differences related to maternal psychopathology due to age-related developmental variations in ER.
Future directions
Future research should further examine the classification of ER strategies as adaptive or maladaptive in (early) childhood and more clearly distinguish between ER variability and flexibility. As in the present study, future work should consider multiple ER indices (e.g., duration, latency, frequency, variability, and flexibility) to better capture the complexity of children’s regulatory behavior, while also accounting for important contextual and protective factors. Longitudinal studies are needed to elucidate how children’s ER develops in the context of parental psychopathology, how and when early ER patterns relate to later mental health and psychopathology outcomes.
Conclusion
Although maternal psychopathology was not directly associated with children’s ER, the study revealed meaningful age-related differences and distinct pattern in the use of adaptive versus maladaptive strategies in children of mothers with BPD. These findings provide an initial step in applying the concepts of ER adaptiveness and ER variability to this population, exploring ER patterns as early predictors of later BPD specific psychopathology. Thus, the study contributes to the transdiagnostic RDoC framework of ER patterns (Michelini et al., Reference Michelini, Palumbo, DeYoung, Latzman and Kotov2021) and underscores the importance of further longitudinal research in at-risk samples.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579426101345.
Data availability statement
The data and code necessary to reproduce the analyses presented in this study are publicly available at PsychArchives. The analysis code is available at https://doi.org/10.23668/psycharchives.21655, and the data set including the codebook can be accessed at https://doi.org/10.23668/psycharchives.21656.
Acknowledgments
We would like to thank all mothers and children who participated in the ProChild study. We are also grateful for our collaboration with Prof. Dr. Charlotte Rosenbach, Jana Zitzmann, and Anne Jung who have coordinated the study and administered the data assessment at their sites.
Funding statement
The ProChild study was funded by the Federal Ministry of Education and Research, Germany, the data rely on the subproject 2 “Mental Health”, funding ID: 01KR1805B.
Competing interests
The authors declare none.
Pre-registration statement
Preregistration of the study’s hypotheses and analysis plan is available at the German Clinical Trials Register. Active link: https://drks.de/search/en/trial/DRKS00020460. Date of stamp: 2020-02-19. Deviation: The recruitment status was updated continuously, and the hypotheses were expanded to include the assumption that unfavorable emotion regulation strategies are associated with unfavorable mental health (i.e., more diagnoses and/or greater severity of diagnoses).




 Open access
Open access