


Cognitive analytic therapy (CAT) was developed in the 1980s by the general practitioner Anthony Ryle Reference Ryle, Kellet, Hepple and Calvert1 as a time-limited (16–24 sessions, with follow-up), integrative psychotherapy deliverable within a resource-limited National Health Service. Reference Ryle, Kellet, Hepple and Calvert1,Reference Ryle and Kerr2 CAT integrates both cognitive and analytical models, and provides an accessible, relational and collaborative approach to exploring the development of the socially formed self and problematic patterns of relating that potentially result in psychopathology. Reference Ryle, Kellet, Hepple and Calvert1
Drawing on object relations and sociocultural theories, Reference Vygotsky3,Reference Leiman4 CAT understands that internalised representations of the self, others and the world are informed by early attachment experiences with significant others. The representations of reciprocal interactions are internalised as ‘reciprocal roles’, from which patterns develop to protect the self from anticipated stress (e.g. reject self or others) or to seek fulfilment of unmet needs from others (e.g. perfect care). Behaviours are known within CAT as procedures, or as reciprocal role procedures (RRPs) when linked directly with a reciprocal role. Reference Ryle, Kellet, Hepple and Calvert1 Ryle identified three procedures:
-
• traps: circular procedures where negative perceptions, behaviours or beliefs lead to further negative experiences, reinforcing the original problem;
-
• dilemmas: procedures with binary polarised behavioural options;
-
• snags: where desired outcomes are avoided because they are feared or not felt to be deserved.
With explicit use of transference and countertransference, CAT adopts a three-phased approach: reformulation, recognition and revision. Reference Ryle, Kellet, Hepple and Calvert1
Reformulation involves supporting patients in exploring how their early development and resulting survival patterns may be influencing their patterns of behaviour and relationships in adulthood. Reference Ryle, Kellet, Hepple and Calvert1,Reference Ryle and Kerr2 Therapist and patient jointly create a reformulation letter and sequential diagrammatic reformulation (SDR) (colloquially known as the ‘map’) based on identified reciprocal roles and problematic RRPs.
Recognition involves diary keeping and exploration of RRPs, using the SDR and in-therapy reciprocal roles to support recognition. This phase is supported by noticing and naming potential enactments occurring both inside and outside therapy.
Revision involves noticing and trialling RRP ‘exits’, which may offer alternative ways of relating. Therapist and patient consider therapy endings, acknowledging this in goodbye letters and planning follow-up sessions. Reference Ryle, Kellet, Hepple and Calvert1
CAT is predominantly offered to individuals with complex and enduring psychological difficulties. Reference Simmonds-Buckley, Osivwemu, Kellett and Taylor5 Effectiveness studies have included individuals with personality disorder, trauma, anxiety, depression and eating disorders. Reference Ryle, Kellet, Hepple and Calvert1,Reference Owen, Laphan, Gee and Lince6,Reference Hallam, Simmonds-Buckley, Kellett, Greenhill and Jones7 Large pre–post reductions in global functioning and depression outcomes, plus moderate to large reductions in interpersonal problems, were reported. Reference Simmonds-Buckley, Osivwemu, Kellett and Taylor5 Meta-analysis of randomised controlled trials (RCTs) of CAT in over-16-year-olds reported mean drop-out rates of 16% Reference Hallam, Simmonds-Buckley, Kellett, Greenhill and Jones7 and 18.69%. Reference Simmonds-Buckley, Osivwemu, Kellett and Taylor5 This is comparable to other psychotherapeutic modalities. Reference Simmonds-Buckley, Osivwemu, Kellett and Taylor5 Use of CAT in child and adolescent mental health services (CAMHS) is increasing, with recent descriptions of services and work with young people. Reference Crothers and Barnes8 Effectiveness and feasibility of CAT within CAMHS is not clear.
Aims
This paper aims to collate all published literature discussing the use of CAT with under-18-year-olds. A secondary aim is to establish whether CAT is feasible and effective in this cohort.
Method
A search was undertaken in the following databases: MEDLINE (Healthcare Databases Advanced Search (HDAS), the Health Education England/National Institute for Health and Care Excellence platform, 1946–), PsycINFO (HDAS, 1806–) and CINAHL. These searches were run on 31 August 2023 and repeated in March 2025. There were no search date limitations. A combination of subject headings and keyword terms were used (supplementary material, available online at https://doi.org/10.1192/bjb.2026.10218). The search strategy was developed initially in MEDLINE and tested for sensitivity using a pool of relevant references found via hand-searching.
The initial database search (Search 1) found limited articles (n = 72). To capture all literature on CAT with under-18-year-olds, a subsequent hand-search (Search 2) of the Association of Cognitive Analytic Therapy (ACAT) website bibliography was completed. This bibliography contains expert opinion and service provision articles. 9 Articles are reviewed by newsletter editors but are not peer reviewed.
All articles commenting on CAT with under-18-year-olds were included. Owing to the limited published literature on this topic, broad inclusion criteria were chosen, including expert opinion, service description and quantitative articles. Literature reviews, book chapters and articles referring to studies or services already identified were excluded. References from eligible articles and relevant reviews were scrutinised for further potential articles.
In Search 2, Part A the following keywords were searched in the ACAT bibliography search function: young, child, children, parent, adolescent, teenager, youth.
Following deduplication, articles were screened by one author and three authors independently assessed full texts for eligibility.
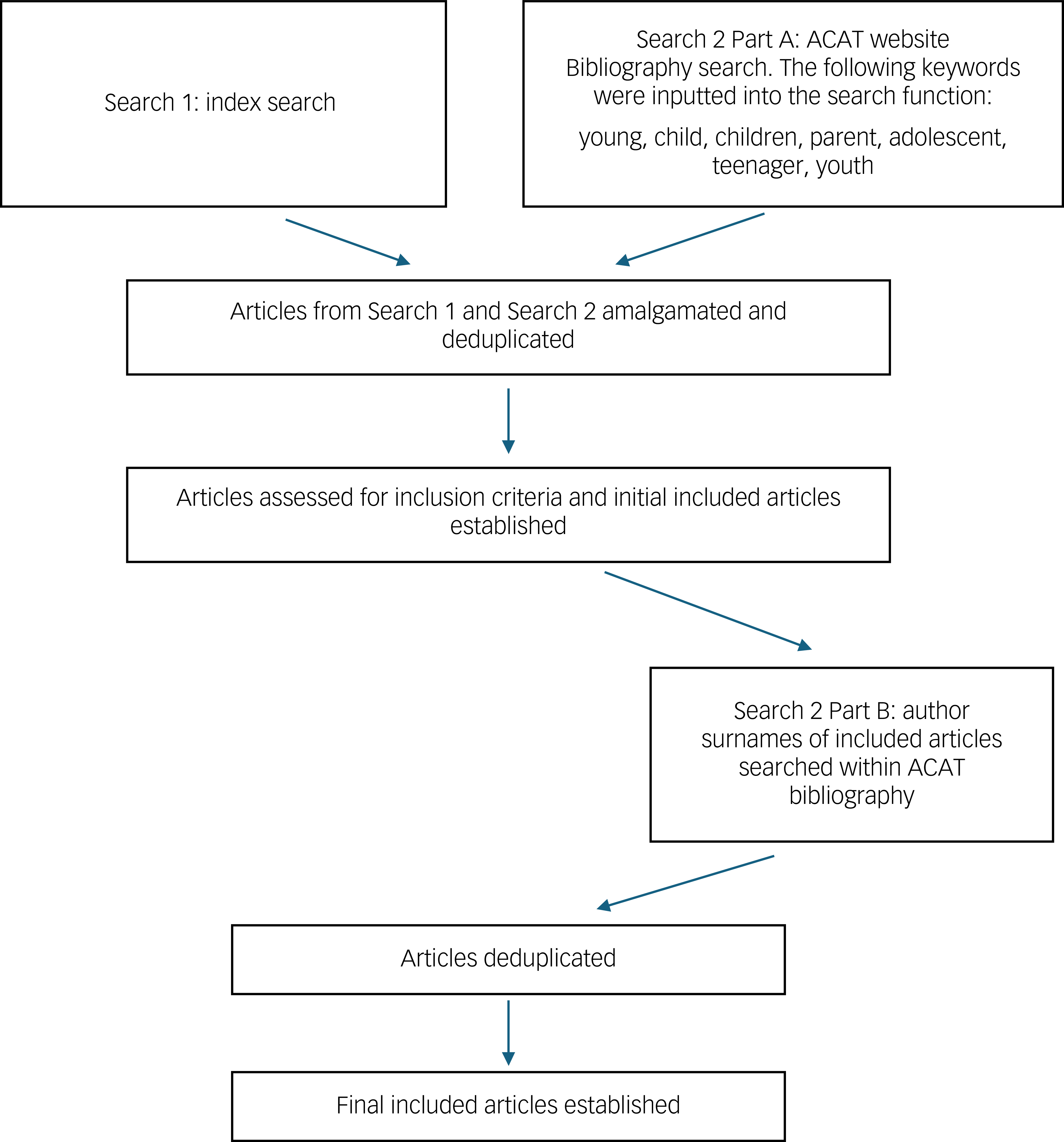
Author surnames of eligible articles were then searched in the ACAT bibliography search function (Search 2, Part B). Articles were screened and assessed for eligibility. No author disagreements occurred over included articles, probably because of the broad inclusion criteria. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the search is shown in Fig. 1. Figure 2 shows a simplified flow chart of the search methods.
PRISMA flow diagram. ACAT, Association of Cognitive Analytic Therapy.

Flowchart of simplified process for Search 1 and Search 2. ACAT, Association of Cognitive Analytic Therapy.

Each author independently reviewed included articles against the Oxford Centre for Evidence-Based Medicine Levels of Evidence criteria to decide evidence level. 10 Further author discussion was required to reach consensus for five papers. Reference Gersh, Hulbert, McKechnie, Ramadan, Worotniuk and Chanen11–Reference Turley, Faulkner, Tunbridge, Regan and Knight15
Quantitative studies were reviewed for quality by two authors (M.C., F.R.), with findings summarised. In line with this paper’s aim, a thematic summary is provided in the absence of thematic analysis for reflective and service description papers.
Results
In total, 37 articles met the inclusion criteria. Articles were categorised into quantitative (n = 11), service descriptions (n = 12) and reflective (n = 14) articles.
Quantitative articles
Table 1 gives a summary of the 11 quantitative articles. Nine (82%) quantitative papers focused on CAT interventions with young people; Reference Gersh, Hulbert, McKechnie, Ramadan, Worotniuk and Chanen11–Reference Daly, Llewelyn, McDougall and Chanen13,Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16–Reference Haw, Marsden, Hartley, Turpin and Taylor21 one (9%) investigated outcomes with families; Reference Russell-Carroll and Gordon22 one (9%) reviewed opinions of CAT with staff members. Reference Turley, Faulkner, Tunbridge, Regan and Knight15
Summary of quantitative articles involving cognitive analytic therapy (CAT) interventions with under-18-year-olds

RCT, randomised controlled trial; BPD, borderline personality disorder; HYPE, Helping Young People Early; GCC, good clinical care; SCID-II, Structured Clinical Interview for DSM-IV Axis II Disorders; YSR, Youth Self-Report; YASR, Young Adult Self Report; SOFAS, Social and Occupational Functioning Assessment Scale; YMHS, youth mental health service; SDQ, Strengths and Difficulties Questionnaire; FEP, first-episode psychosis; SFET, specialised FEP treatment; SCID-I, Structured Clinical Interview for DSM-IV Axis I Disorders; MADRS, Montgomery–Åsberg Rating Scale for Depression; BPRS, Brief Psychiatric Rating Scale; SANS, Scale for the Assessment of Negative Symptoms; AIAQ, Anger, Irritability, and Assault Questionnaire; OAS-M, Overt Aggression Scale Modified; ASSIST, Alcohol, Smoking and Substance Involvement Screening Test; AUDIT, Alcohol Use Disorders Identification Test; SDS, Severity of Dependence Scale; MARS, Medication Adherence Report Scale; BPDS-IV, Borderline Personality Disorder Severity Index IV; 3RS, Rupture Resolution Rating System; SAS-SR, Social Adjustment Scale Self Report; H-TAU, historical treatment as usual; GP, general practitioner; PSQ, Personality Structure Questionnaire; CTQ, Childhood Trauma Questionnaire; ADES-II, Adolescent Dissociative Experience Scale Second Edition; SDP, States Description Procedure; SEQ, Session Evaluation Questionnaire; ARM, Agnew Relationship Measure; CGI-I, Clinical Global Impression Improvement Scale; NSSI, non-suicidal self-injury; CATCH-Y, Cognitive Analytic Therapy for Containing Self-Harm in Young People; SITBI, Self-Injurious Thoughts and Behaviors Interview; ABUSI, Alexian Brothers Urge to Self-Injure Scale; MYTS, Motivation for Youth Treatment Scale; PHQ-9A, Patient Health Questionnaire-9 modified for adolescents.
Recruitment for six studies came from the Helping Young People Early (HYPE) treatment programme. Reference Gersh, Hulbert, McKechnie, Ramadan, Worotniuk and Chanen11,Reference Daly, Llewelyn, McDougall and Chanen13,Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16–Reference Chanen, Jackson and McCutcheon19 HYPE is an early intervention programme for borderline personality disorder (BPD) in youth, based on CAT and developed in Melbourne, Australia. Reference Chanen, Jackson and McCutcheon19 The programme supports 15- to 25-year-olds with BPD. HYPE-based trials comprised 66.7% of the included quantitative research on CAT in under-18-year-olds.
Two HYPE-based papers provide RCT data on treatment outcomes from CAT for under-18-year-olds with BPD. Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16,Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17 In a 2008 study, Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16 86 participants were randomised to CAT or good clinical care (GCC). GCC involved standardised team-based care. Both treatment groups showed improvements for outcomes of BPD dimensional total scores, internalising and externalising psychopathology, parasuicidal behaviour and global functioning, suggesting that early intervention is feasible and effective in BPD. CAT showed slightly faster rates of improvement in internalising (s.d. = −0.29; 95% CI −0.67 to 0.10) and externalising (s.d. = −0.50; 95% CI −0.97 to −0.04) pathologies compared with GCC over 24 months.
In a 2022 study, Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17 participants were randomised to three treatment arms: HYPE + CAT; HYPE + befriending; a general youth mental health service (YMHS) + befriending. The researchers considered treatment ‘completed’ if eight (50% of total offered) CAT or befriending sessions were attended. Participants assigned to HYPE + CAT attended significantly more individual psychotherapy sessions than those assigned to befriending (Kruskal–Wallis χ 2 = 13.6; P < 0.001) and completed treatment more than those assigned to befriending (χ 2 = 8.3; P = 0.004). Of the 46 assigned to HYPE + CAT, 24 received more than eight CAT sessions. Drop-out was due to not attending beyond 6 weeks (n = 8), voluntary discontinuation (n = 6), moving catchment area (n = 4), developing psychosis/mania (n = 3) and suicide (n = 1). Three participants (two in the HYPE + CAT group) died by suicide (one during treatment and two before follow-up). Between baseline and 12 months, HYPE + CAT was not superior to befriending for interpersonal problems (Inventory of Interpersonal Problems Circumplex Version (IIP-C), t 99.73 = −0.87; P = 0.39) or social adjustment (Social Adjustment Scale Self-Report (SAS-SR), t 110.36 = −0.753; P = 0.45). HYPE was not superior to YMHS + befriending for interpersonal problems (IIP-C, t 96.12 = 0.80; P = 0.43) or social adjustment (SAS-SR, t 106.68 = 0.06; P = 0.95). Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17
Gleeson et al (2012) completed a pilot RCT comparing HYPE + specialised first-episode psychosis treatment (SFET) against SFET alone. Reference Gleeson, Chanen, Cotton, Pearce, Newman and McCutcheon18 Recruitment involved collaboration between HYPE and an early psychosis prevention and intervention centre. Eight patients were randomised to each trial arm. Four completed HYPE + SFET; five completed SFET alone. Following treatment, the HYPE + SFET group had fewer psychotic, depressive and irritability symptoms, better functioning and were more likely to continue medication than the SFET group. HYPE + SFET appeared safe and feasible for first-episode psychosis with BPD in under-18-year-olds. Reference Gleeson, Chanen, Cotton, Pearce, Newman and McCutcheon18
A quasi-experimental approach was used in comparing CAT and GCC groups from the 2008 HYPE study with a non-randomised, historical treatment as usual (H-TAU) cohort. Reference Chanen, Jackson and McCutcheon19 All groups showed improvement. The CAT and GCC groups showed greater improvements than the H-TAU on four outcome measures. Standardised rates of improvements in internalising (s.d. = −0.72; 95% CI −1.18 to −0.26) and externalising (s.d. = −0.69; 95% CI −1.19 to −0.18) psychopathologies were quicker for CAT than for H-TAU. The H-TAU cohort had 50% fewer care contacts per week, compared with the CAT or GCC cohorts, potentially confounding outcomes.
The importance of the therapeutic alliance, regardless of modality, is evidenced. Reference Martin, Garske and Davis23 Repair of a ruptured patient–therapist alliance can solidify the therapeutic relationship. Mechanisms and consequences of rupture repair are poorly understood. Reference Eubanks, Muran and Safran24 Gersh et al (2017) Reference Gersh, Hulbert, McKechnie, Ramadan, Worotniuk and Chanen11 used a HYPE RCT sample. Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16 They examined pre–post outcome assessments and alliance processes in two groups presenting with BPD randomised to 16 sessions of CAT or befriending treatment. The number of ruptures did not differ significantly between groups. The CAT group completed more stages of resolution (t = 2.7, P = 0.2), in greater depth (t = 2.61, P = 0.2). Early therapy ruptures were associated with significantly poorer outcomes (0.32 correlation with the social adjustment scale, P < 0.5); resolution of ruptures later in therapy was associated with better outcomes (−0.11 correlation with the Borderline Personality Disorder Severity Index, P < 0.5). Early ruptures were more withdrawal-based and later ruptures more confrontational. There was no significant association between rupture repair and treatment outcome. Reference Gersh, Hulbert, McKechnie, Ramadan, Worotniuk and Chanen11
Daly et al (2010) Reference Daly, Llewelyn, McDougall and Chanen13 aimed to validate a nine-stage CAT rupture resolution model with youth with BPD. They applied the model Reference Bennett, Parry and Ryle25 to 18 ruptures across sessions rated as ‘good’ (n = 3) and ‘bad’ (n = 2) by patients. Sessions were part of the HYPE RCT comparing CAT with GCC. Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16 A significant association was found (P = 0.02) between the number of model stages progressed through and rupture resolution, and between the number of model stages progressed through and positive treatment outcome (P = 0.02). Unresolved ruptures tended to miss the later model stages. Reference Daly, Llewelyn, McDougall and Chanen13
Hessels et al (2021) reviewed 22 participants (from a total of n = 29) receiving on average 15 CAT sessions within a HYPE-inspired programme in The Netherlands. Reference Hessels, Dijk and Aken20 They aimed to assess treatment programme feasibility through attendance, and group mean scores for pre-treatment (baseline) and post-treatment (6 months) psychosocial assessments. All 29 participants completed the treatment programme, but 7 (24.1%) did not attend the second measurement point and were excluded from analysis. The mean score for ‘total difficulties experienced’ was lower at the second than first wave (on a 0–40 scale, mean 0.23, 95% CI 0.40–3.15; t(21) = 2.68, P < 0.05). Prosocial behaviour did not significantly change between the two measurement points (on a 0–10 scale, mean 1.77, 95% CI −0.71 to 0.08; t(21) = −1.67, P = 0.11). The emotional problems score was higher at the second wave (on a 0–10 scale, mean 0.82; 95% CI 0.01–1.62; t(21) = 2.11, P < 0.05). Self-harming was lower at the second wave (on a 0–4 scale, mean 0.50, 95% CI = 0.05–0.95; t(21) = 2.318, P < 0.05). There was no significant change in problems with alcohol use across measurement points (on a 0–6 scale, mean 0.14, 95% CI −0.36 to 0.64; t(21) = 0.568, P = 0.576) or drug use problems (on a 0–6 scale, mean −0.18, 95% CI = −0.44 to 0.08; t(7.397) = 0.932, P = 0.381).
Ougrin et al (2008) examined the effect of CAT-informed therapeutic assessments on treatment adherence. Reference Ougrin, Ng and Low12 Two groups with self-harm were compared. Participants received assessment as usual or CAT-informed therapeutic assessment. Participants who received therapeutic assessment were significantly more likely to attend their first community follow-up (χ2 = 3.89, P < 0.05) and engage with services (χ 2 = 4.49, P < 0.05). This study was not randomised: allocation was dependent on which staff member a young person was allocated. Young people in the therapeutic assessment group were more likely to have been referred to tertiary CAMHS, suggesting potential confounding factors contributing to increased follow-up attendance. Reference Ougrin, Ng and Low12
Haw et al (2024) assessed whether a five session CAT-informed therapy called CAT for Containing Self-Harm in Young People (CATCH-Y) was feasible and acceptable for reducing non-suicidal self-injury (NSSI) in youth. Reference Haw, Marsden, Hartley, Turpin and Taylor21 The study recruited 13 participants from two CAMHS teams in the Northwest of England; 11 participants completed all five sessions; 2 dropped out (one for escalated risk and one withdrew) pre-intervention. Ten participants provided pre–post data. Five showed improved depression scores (Patient Health Questionnaire for Adolescents) and two deteriorated. Four had improved sense of recovery (Recovery Questionnaire for Young People) and one deteriorated. Equal numbers demonstrated improvements (n = 3) and deteriorations (n = 3) in urge to self-harm (Alexian Brothers Urge to Self-Injure Scale). Reference Haw, Marsden, Hartley, Turpin and Taylor21 Mean imputed data were used for one missing data point in one case. Researchers completing the assessments were also the therapists, introducing potential bias. Clinicians were not formally trained in CAT, but were familiar with the CAT framework and skills/tools. The small sample size, missing data and no comparator negate ability to draw inferences from pre–post assessment findings. This early-stage feasibility study provides a baseline for further evaluation of CATCH-Y as an approach to NSSI in under-18-year-olds. Reference Haw, Marsden, Hartley, Turpin and Taylor21
Russell-Carroll & Gordon used a CAT perspective to compare relational patterns in six families displaying emotional dysregulation versus six non-dysregulated families. Reference Russell-Carroll and Gordon22 Interviews of families responding to critical, ambiguous and empathic vignettes were analysed. Families with emotional dysregulation described significantly fewer ‘OK’ relational patterns (U = 4.0, P = 0.02, r = 0.67) when discussing parental relationships and significantly more ‘abusing’ patterns (U = 6, P = −0.05, r = 0.5) in response to a critical vignette. Incidence of trauma and ‘victim-abusing’ relational patterns were similar in both groups. Reference Russell-Carroll and Gordon22
Articles giving service descriptions
The 12 articles discussing CAT-based services are summarised in Table 2.
Summary of articles describing cognitive analytic therapy (CAT)-based service descriptions for under-18-year-olds

n.a., not applicable; CAMHS, child and adolescent mental health services; MDT, multidisciplinary team; HCA, healthcare assistants; PICU, psychiatric intensive care unit.
CAT with young people
CAT appears adaptable in terms of modality, Reference Barnes26 being used with individuals Reference Barnes26–Reference Elia and Jenaway29 and groups. Reference Barnes26,Reference Mulhall30–Reference Mulhall32
Individual CAT – reflections on how to best benefit the young person
Engaging adolescents in the therapeutic process is important. One study of young people receiving CAT found a 47% drop-out rate. Reference Jenaway and Mortlock27 Youth tend to prefer shorter treatment processes. Reference Chanen, McCutcheon, Germano, Nistico, Jackson and McGorry28 Flexible and transparent engagement approaches appear beneficial. Responsibility for attendance being progressively handed over to the young person appears beneficial, with support for organisation and structure of initial sessions being led by the clinician. Reference Chanen, McCutcheon, Germano, Nistico, Jackson and McGorry28 CAT tools were deemed helpful for adolescents. Reference Jenaway and Mortlock27 Visual representations of reciprocal roles appeared more accessible to adolescents than words. Rating scales were considered least helpful. Reference Jenaway and Mortlock27 Young people found identifying reciprocal roles via creative means (drama, film, music) to be less threatening than identifying them within themselves. Emotional expression within film is likely exaggerated for effect, therefore supporting emotionally distant patients to recognise and acknowledge feelings and reciprocal roles. Reference Elia and Jenaway29 The six-part story method (6PSM) has also been helpful in discussing reciprocal roles and procedures ‘at a distance’ with young people. Reference Mulhall30
When working with young people, parents’ feelings were considered when writing reformulation letters, reducing critical reciprocal roles; one paper stated there were no complaints from parents regarding reformulation letters for individual CAT with under-18-year-olds. Reference Jenaway and Mortlock27
CAT with under-18-year-olds is not limited to individual therapy
CAT-informed community services included a CAT-informed film creation and a film series for a school group, with the aim of supporting emotional distress. Reference Barnes31 Direct work with under-18-year-olds showed improvement in self–self, self–other and other–self relationships and improved prosocial behaviour in adolescents with interpersonal difficulties. Reference Barnes31 Traumatised young people in ‘stuck’ positions with grief were able to move forwards with their lives following a CAT-informed group-based intervention. Reference Barnes31
Two papers describe patient group work in CAMHS in-patient wards. Reference Mulhall30,Reference Mulhall32 Groups were CAT-informed. Flexibility with CAT tools was required to adapt to context. Groups highlighted commonly repeated reciprocal roles. Locked in-patient units can bring about controlled reciprocal roles in young people and thereafter defiant/rebelling procedures, which can affect group productivity. Reference Mulhall32 Young people who align with the group purpose risk peer-berating outside of sessions. Themes from CAT in-patient groups included safety, fun, psychoeducation, mental health and relational awareness, positivity and change. Reference Mulhall32
Open groups are complicated by changing zones of proximal development Reference Vygotsky3 and attendance. Closed groups are another option. Inclusion criteria may include mid-stay, psychologically ready, unlikely to be discharged mid-group, and reasonable peer compatibility. Feedback from a closed six-session CAT group suggests this is acceptable to adolescents as a therapeutic intervention. Reference Mulhall30
CAT with parents
Four papers described CAT-informed care with parents of adolescents. Reference Barnes26,Reference Chanen, McCutcheon, Germano, Nistico, Jackson and McGorry28,Reference Barnes31,Reference Bernardy-Arbuz33 CAT-informed family sessions are used in holistic care programmes. Reference Chanen, McCutcheon, Germano, Nistico, Jackson and McGorry28 One service involved five-session integrated individual CAT for parents, focusing on recognition of their responses in the child–parent relationship, linking how this may affect their children’s behaviours. Reference Barnes31 Knowing parents are holding them in mind can be valuable for ‘non-engaging’ young people. Reference Barnes31 One author reflects on benefits of CAT parenting guidance: if parents cannot ‘repair’, they may ‘repeat’ unhelpful patterns of relating and struggle to internalise and embed skills learned in parenting groups. Reference Bernardy-Arbuz33 Using CAT language in parenting groups provides a relational view of parenting skills. Reference Bernardy-Arbuz33 In one service, 11 parents (50%) dropped out, 8 with no explanation, 2 with inconsistent attendance and 1 for medical reasons. The author proposes individual CAT with parents before group sessions, to improve engagement. Reference Bernardy-Arbuz33
CAT with staff members
Six papers described CAT-informed services for staff members. Reference Priddy, Kellett, Goodall and Cotton14,Reference Elia and Jenaway29,Reference Barnes31,Reference Potter, Bernardy-Arbuz, Regan and Barnes34–Reference Crothers, Edwards and Radford36
CAT-informed supervision
CAT-informed supervision of staff working with adolescents may increase understanding of relationships within peer mentoring schemes, and support scheme success. Reference Barnes31 When reformulation was offered within staff supervision sessions, young people were observed to transition from ‘disengaging–disengaged’ to ‘appreciating–valued’ and ‘remembering–acknowledged’. Reference Barnes31 The Teaching for Holistic, Relational and Inclusive Early Childhood Education (THRIECE) project involved CAT-informed care in educational settings. Reference Potter, Bernardy-Arbuz, Regan and Barnes34 The project aimed to increase relational awareness among primary school teachers. Post-project thematic analysis revealed increased relational awareness, self-reflection and creation of ‘common language’ for relationships. Increases in psychological safety and improved staff relationships were found.
CAT-informed reflective groups
Mulhall (2021) set up a staff CAT-informed reflective group. Reference Mulhall35 Owing to staff workload, attendance varied. Flexibility and regular supervision were essential for facilitators to prevent rejecting–rejected reciprocal roles during times of reduced attendance. Reference Mulhall35 Broad group themes included service improvement, noticing push–pull dynamics, increasing understanding and professional growth.
Priddy et al (2025) completed a grounded theory study of cognitive analytic reflective practice (CARP) groups with staff in a secure residential home for (often traumatised) young people. Reference Priddy, Kellett, Goodall and Cotton14 This CAT-informed reflective practice was found to widen ‘awareness of the self, other, and system’ and ‘change relational dynamics and establish exits’. Review of the CARP groups also revealed improve team cohesiveness, as evidenced by increased scores on the Group Entitativity Measure–Group Psychotherapy (H(1) = 4.18, P = 0.04). Coding of Helpful Aspects of Therapy questionnaire scores showed no significant difference in helpfulness/unhelpfulness (H(7) = 10.75, P = 0.15). Reference Priddy, Kellett, Goodall and Cotton14
CAT-informed consultation
CAT’s framework can support professional understanding of patient formulation while inviting professionals to explore personal emotional responses. Reference Crothers, Edwards and Radford36 During monthly 2 h CAT-informed consultation, increased relational understanding of cases by staff was observed, alongside recognition of re-enacting unhelpful reciprocal roles. Staff form a ‘common language’ when discussing cases. Reference Crothers, Edwards and Radford36 Using CAT language for multi-agency communication can reduce ‘splits’, minimise collusion with unhelpful relational patterns, and aid patient-centred understanding of the formulation and care plan. Reference Chanen, McCutcheon, Germano, Nistico, Jackson and McGorry28
Reflective articles
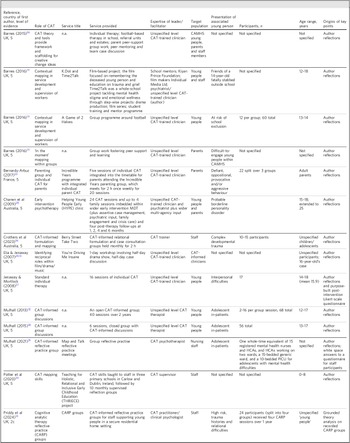
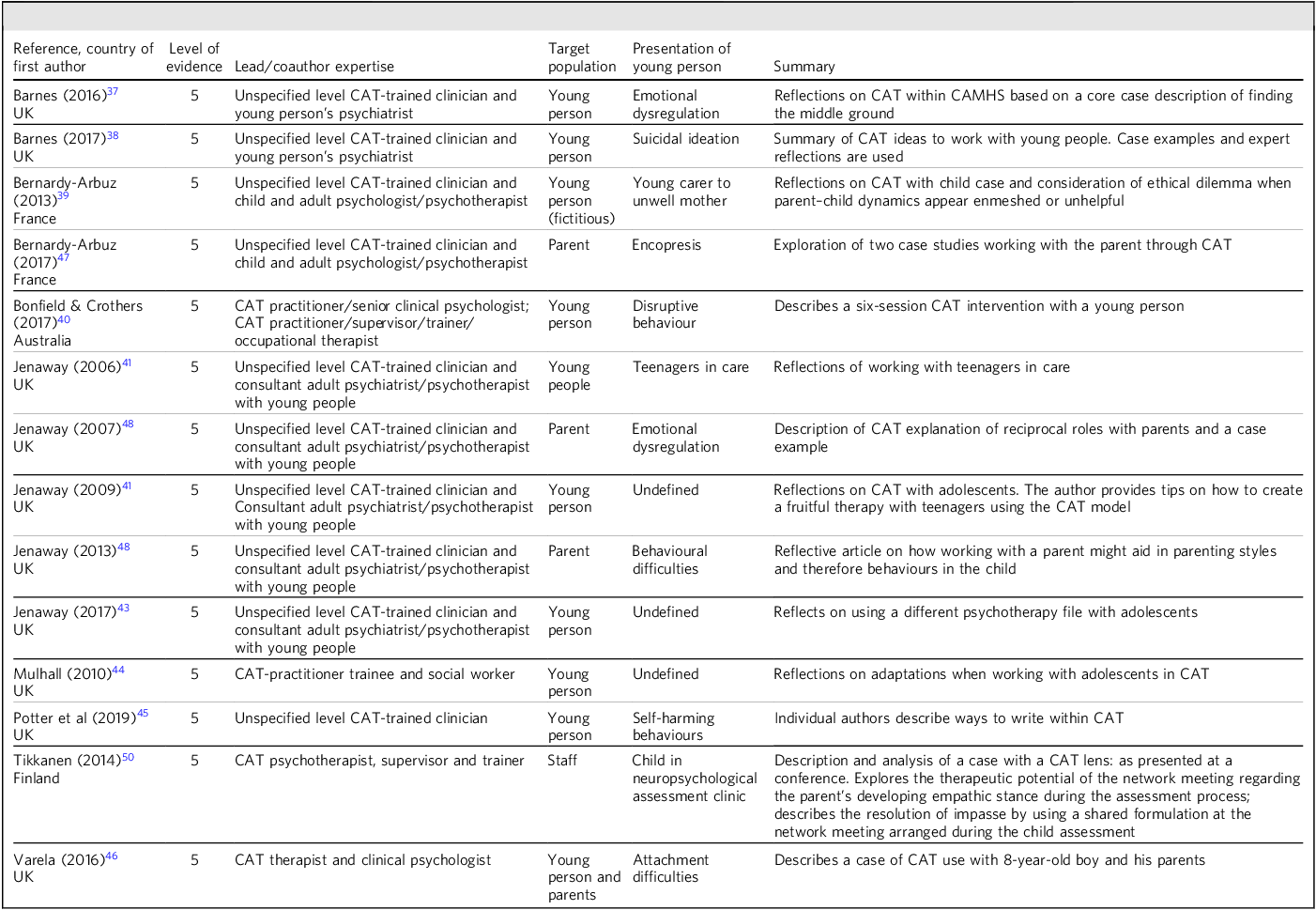
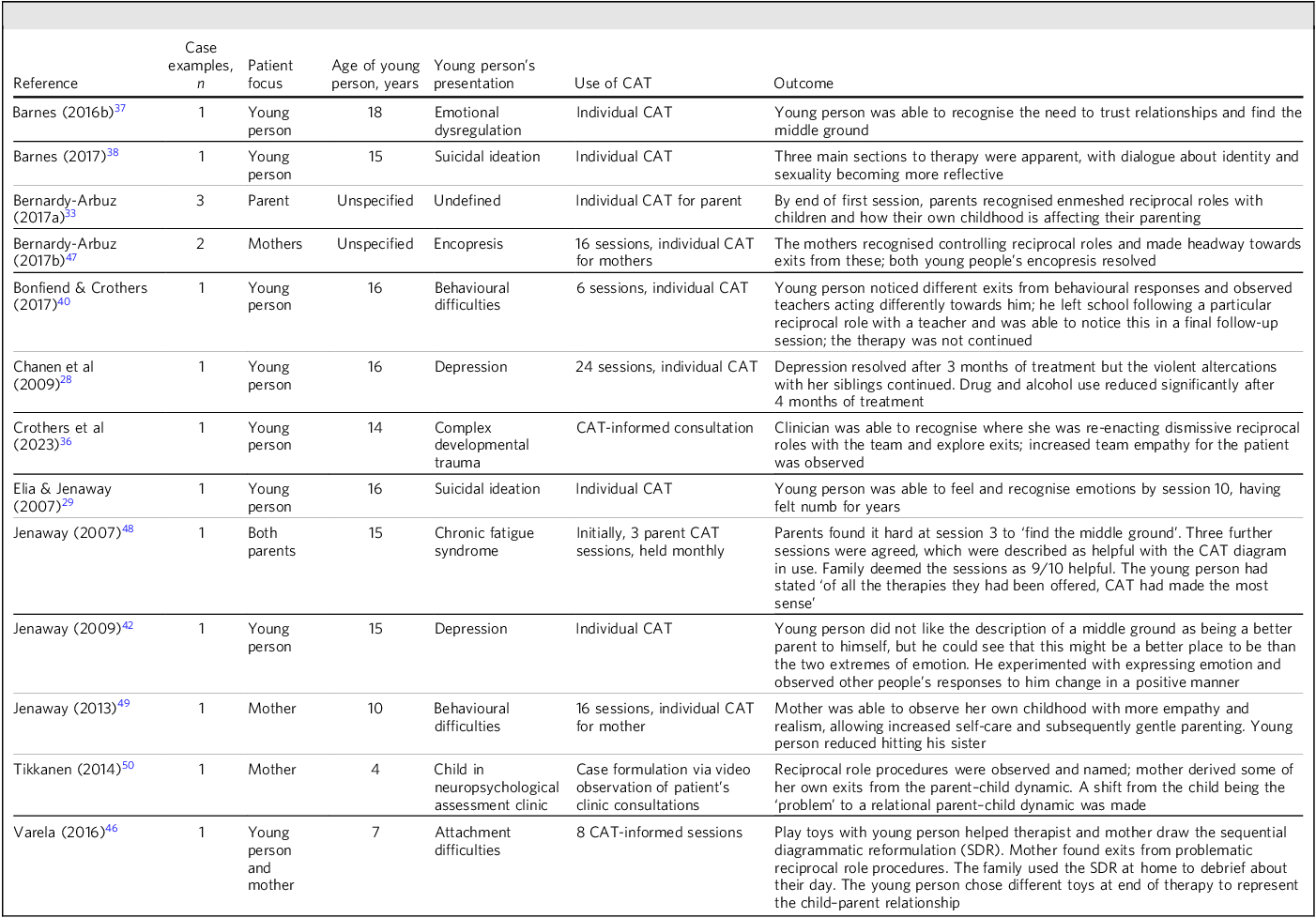
The 14 reflective articles are summarised in Table 3. Case examples described in the literature are detailed in Table 4.
Summary of reflective and expert-opinion articles discussing cognitive analytic therapy (CAT)-based interventions for under-18-year-olds

CAMHS, child and adolescent mental health services.
Summary of case examples described in articles discussing cognitive analytic therapy (CAT)-based interventions for under-18-year-olds

CAT with under-18-year-olds means adapting for under-18-year-olds
Regarding individual work with under-18-year-olds, Reference Barnes37–Reference Varela46 authors commented on the helpfulness of the model supporting change through collaborative understanding, fostering agency and mastery in young people who otherwise experience limited control and limited financial, decision-making and social power. Reference Barnes37,Reference Barnes38,Reference Jenaway42 Working with a young person’s resources and following their agenda, rather than insisting on CAT’s agenda, is important. Offering fewer sessions with co-agreed extensions may enable patient control/autonomy. Reference Jenaway41
Reference was made to working in the ‘middle ground’ with under-18-year-olds, Reference Barnes37,Reference Barnes38,Reference Jenaway42 a place of negotiation between extreme polarisations where emotions can be felt and contained, and where self-compassion, integration and self-parenting are explored. The importance of prioritising intrapersonal self-parenting exits, rather than potentially less safe interpersonal changes within an unsafe system (e.g. seeking validation from parents), is highlighted. Reference Barnes37,Reference Barnes38
Youth may find exploring past traumas unbearable. Reference Jenaway41 One adaptation considers working in the ‘here and now’, guided by principles of solution-focused therapy to identify exits encompassing the young person’s resources and strength. Focusing on the present, aspirations and solutions can support engagement. Reference Jenaway41
With under-18-year-olds, keeping things focused and straightforward is particularly helpful. Reference Barnes37,Reference Jenaway42 Focusing on one procedure is recommended. Reference Jenaway42 The SDR is recognised as most helpful, given adolescents’ propensity to be visually minded. Reference Mulhall44 Two cases demonstrate the power of mapping alongside patients to understand unhelpful patterns at extreme ends, and gently exploring the middle ground, allowing reflection, self-care and development of trusting relationships. Reference Barnes37 ‘Relationship cards’ might help adolescents consider key relationships visually. Reference Mulhall44 CAT is described as feasible for adolescents, being met with commitment and enthusiasm. Reference Mulhall44 Blocking and protective sentences when working with a 16-year-old are discussed. Reference Potter, Amleh, Crothers, Bernardy and Cutler45 Use of protective sentences allowed the young person to open up and talk about associated feelings.
Barnes (2017) offers insight into more systemic, context-aware relational approaches. Reference Barnes38 He recommends using CAT theory within community resources. CAT enables an integrated, young person-centred way of working, prioritising collaborative exploration to promote a sense of agency (reduce power imbalance) for young people. Reference Barnes38 The CAT model reminds clinicians of the adolescent’s zone of proximal development, highlighting the importance of working with young people ‘where they are at’, not where services wish them to be. Reference Barnes38
CAT-informed care does not have to be 16 sessions
Shortened CAT therapies have been described, including a six-session CAT intervention for disruptive behaviour within a school system. Reference Bonfield and Crothers40 Mapping allowed the young person to feel open and encouraged, alongside supporting trusted teachers to demonstrate alternative ways of responding. Different responses by teachers allowed the young person to take alternative exits, resulting in several situations being defused. Important aspects of change processes (e.g. co-creation, creativity, formulation and inviting a parent and child to be active and curious participants) are well supported by CAT. Reference Varela46 Adaptations are likely required for CAT to be accessible for children, such as shorter therapy and using toys and ‘sculpts’ to support discussion of reciprocal roles and create maps. Reference Varela46
CAT with parents and staff
Under-18-year-olds do not exist in isolation: they are surrounded by adults
School and parental involvement is often required to support reciprocal role changes. Reference Bonfield and Crothers40 When working with children, exploring parents’ own RRPs can aid in understanding and resolving the child’s RRPs. Reference Bernardy-Arbuz47 In two cases, exploring how parent RRPs might inadvertently be repeated/triggered with their daughter resulted in resolution of child encopresis. A developmental explanation of parent–child reciprocal roles can aid exploration of a parent’s own RRPs. Reference Jenaway49 Work with parents has helped them find the middle ground of their own behaviours rather than ‘trying to control’ children’s behaviours. Reference Jenaway48 With use of CAT tools, talking about a parent’s early life and relationships can support exploration of evolving patterns with their own children in a safe, non-judgemental manner. This can aid engagement and exits. Reference Jenaway48
CAT with parents is recommended as a prelude to parenting programmes, whereby parents might revise some of their own procedures before working on supporting their child. Reference Jenaway49 One parent described child therapy, her own CAT therapy and parenting interventions as a ‘triangle’ of care. Reference Jenaway49
CAT conceptual tools have been reported as being of use in a neurology clinic. Reference Tikkanen50 Tikkanen (2014) analysed videorecorded child neurological assessment processes, with coercion and oppositional interactions observed. Reference Tikkanen50 Sharing the formulation with parents helped recognition and subsequent resolution of the impasse created by this re-enactment of the problematic RRP.
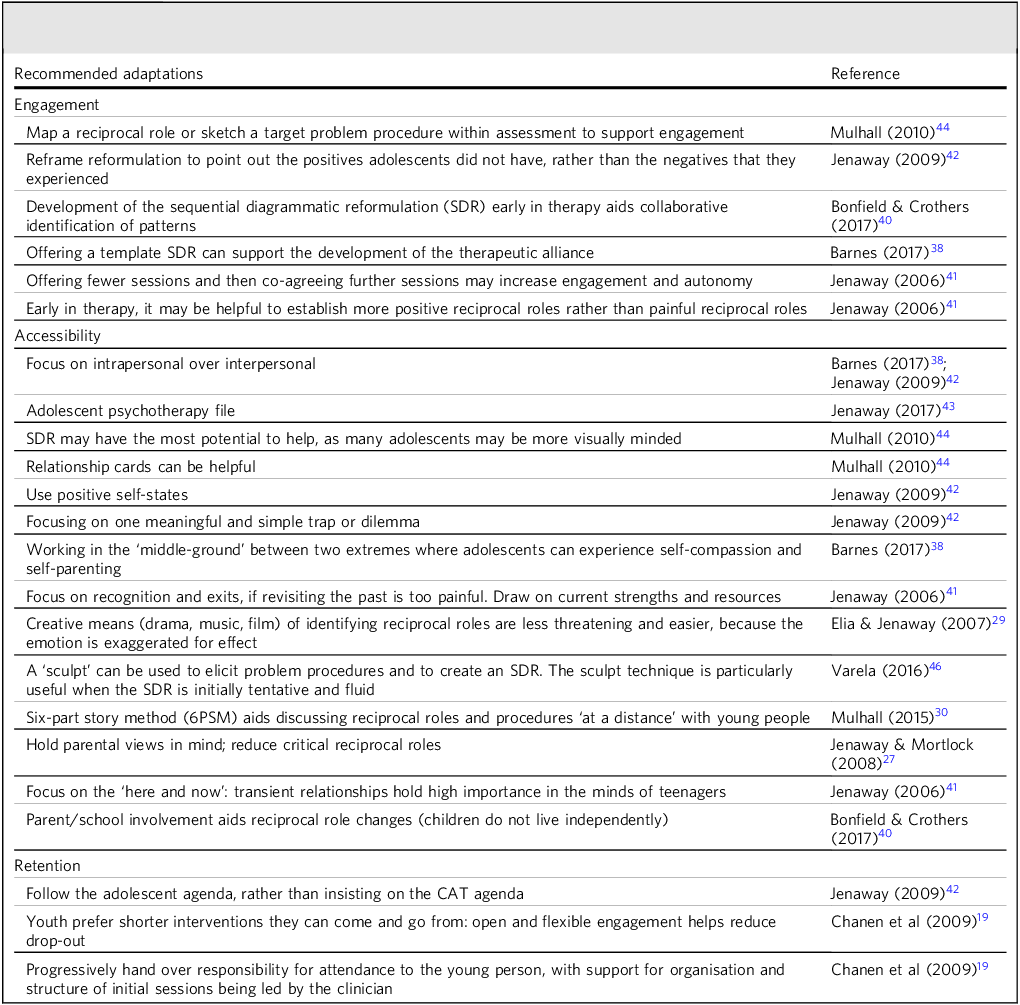
Adaptations to support adolescent engagement with CAT are summarised in Table 5.
Recommended adaptations to consider when using cognitive analytic therapy (CAT)-based Interventions with under-18-year-olds

Discussion
This review aimed to collate the growing evidence, both grey and published, on the use of CAT with under-18-year-olds, with secondary aims of establishing whether CAT is feasible and effective in this cohort. Limited evidence exists for CAT with adolescent populations. Results demonstrate the utility of CAT as an individual therapy and within surrounding systems. Although CAT exists as a therapeutic modality, it also offers a lens to explore individual, family and therapeutic dynamics. Under-18-year-olds can face extraordinary pressures with little resources or social power, potentially forming reciprocal roles around powerlessness and control. Inevitably, surrounding systems may enact unhelpful patterns of responding that can sustain distress for young people. Reflective articles comment positively on the use of CAT. There is a theme of focusing collaboratively on the ‘middle ground’, increasing self-compassion and self-parenting abilities. With young people, focusing on the intrapersonal may feel safer than the interpersonal, particularly if surrounding environments and attachments feel unsafe.
Feasibility
Outcome studies for CAT treatment programmes are feasible to recruit to. Reference Gleeson, Chanen, Cotton, Pearce, Newman and McCutcheon18,Reference Haw, Marsden, Hartley, Turpin and Taylor21 Studies and expert reflections suggest CAT is feasible with under-18-year-olds. CAT theory, particularly Vygotsky’s zone of proximal development, Reference Vygotsky3 may be extended to include environment and geography: to work where a young person ‘is at’. Reference Barnes26 CAT is used flexibly in CAMHS, with individuals, parents, care staff and educational settings.
Case studies comment on the use and acceptability (a generic term for whether the therapy had a low drop-out rate, was easy to understand and was felt helpful to the patient) of CAT in under-18-year-olds and CAT’s diversity with parents and case formulation. CAT appears acceptable to adolescents, Reference Haw, Marsden, Hartley, Turpin and Taylor21 even those with complex comorbidities such as BPD and first-episode psychosis. Reference Gleeson, Chanen, Cotton, Pearce, Newman and McCutcheon18
Limited data exist on drop-out from CAT among under-18-year-olds. CAT treatment programmes studied show good adherence from participants, Reference Hessels, Dijk and Aken20 better than comparable controls. Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16 One paper reported 47% drop-out rate, mainly due to practical attendance difficulties. Reference Jenaway and Mortlock27 In Chanen et al (2008), 15 (37%) completed treatment in the HYPE + CAT arm, with 26 (63%) discontinuing at various points of treatment. There were no significant differences compared with controls; 10 (38%) of those who discontinued treatment negotiated an early termination because they felt they did not require more treatment. Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16
Chanen et al (2022) found better treatment completion for HYPE + CAT compared with HYPE + befriending (24/46 (52.2%) v. 29/93 (31.2%)), with better median psychotherapy session attendance: median 12 (IQR = 16.5) v. 3 (IQR = 9.8) sessions. Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17 With HYPE + SFET, the average number of sessions was 9.5/16, and 5 participants (83%) reached reformulation. Reference Gleeson, Chanen, Cotton, Pearce, Newman and McCutcheon18
Smaller pilot studies showed good attendance. Zero participants dropped out of the treatment programme in Hessels et al (2021). Reference Hessels, Dijk and Aken20 In Haws et al (2024), 11 participants (85%) attended all five CAT sessions. Zero participants dropped out once commencing CAT. Reference Haw, Marsden, Hartley, Turpin and Taylor21
Adaptations for improving engagement with under-18-year-olds is discussed in reflective articles. Adult patients can find the SDR and reformulation letter helpful, yet they may elicit powerful, painful emotions. Reference Balmain, Melia, Dent and Smith51 Emotion regulation is still refining itself in adolescence, Reference Young, Sandman and Craske52 therefore CAT may pose threat to adolescents’ emotional balance. CAT’s adaptability appears to allow for this. Jenaway (2006, 2009) Reference Jenaway41,Reference Jenaway42 recommends focus on positive, less painful reciprocal roles. Similarly, adaptations found to improve CAT’s acceptability to adolescents include techniques for ‘distancing’ emotions, such as using film Reference Elia and Jenaway29 or the six-part story method. Reference Mulhall30 The observations by Gersh et al (2017) regarding therapeutic ruptures may also be useful for clinicians looking to engage under-18-year-olds therapeutically. Reference Gersh, Hulbert, McKechnie, Ramadan, Worotniuk and Chanen11
Effectiveness
Five quantitative articles, Reference Daly, Llewelyn, McDougall and Chanen13,Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16–Reference Chanen, Jackson and McCutcheon19 including two robust RCTs, Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16,Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17 provide outcome data for under-18-year-olds attending 16-session CAT. This low percentage (13.5% of the total included articles) mirrors research in broader age groups, where most research involves practice-based evidence with pre–post outcome measures being assessed, and case studies. Reference Taylor and Hartley53 No clinically significant benefit from CAT over high-quality holistic biopsychosocial intervention was found. Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17 HYPE + CAT showed slightly faster improvements in internalising and externalising psychopathologies, versus HYPE + GCC. Reference Tikkanen50 RCTs ensured integrity of CAT delivery, Reference Daly, Llewelyn, McDougall and Chanen13 suggesting good validity of studies. The largest study in this review randomised 139 participants, Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17 demonstrating overall low-power samples. No studies observed outcome effects beyond 24 months: longitudinal studies are warranted to ascertain longer-term outcomes of CAT.
All included case examples revealed positive clinical outcomes. Although this may suggest positive implications for CAT, publication bias should be acknowledged.
Strengths
To our knowledge, this is the first paper to collate published literature on CAT within CAMHS and summarise recommendations for adaptations to CAT work with under-18-year-olds.
Limitations
Heterogeneity of the few articles published on CAT within CAMHS limits this paper to summation and descriptions of findings. Six (54.5%) of the quantitative studies give evidence for CAT as part of HYPE, Reference Gersh, Hulbert, McKechnie, Ramadan, Worotniuk and Chanen11,Reference Daly, Llewelyn, McDougall and Chanen13,Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16–Reference Chanen, Jackson and McCutcheon19 with two articles Reference Chanen, Jackson, McCutcheon, Jovev, Dudgeon and Yuen16,Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17 providing participants for three other studies. Reference Gersh, Hulbert, McKechnie, Ramadan, Worotniuk and Chanen11,Reference Daly, Llewelyn, McDougall and Chanen13,Reference Chanen, Jackson and McCutcheon19 This homogeneity reduces generalisability of results.
Three studies in this review include participants up to 25 years of age. Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17,Reference Gleeson, Chanen, Cotton, Pearce, Newman and McCutcheon18,Reference Hessels, Dijk and Aken20 The average age of participants in the three studies was 17.27 years (s.d. = 2.31), Reference Hessels, Dijk and Aken20 18.4 years (s.d. = 2.9) Reference Gleeson, Chanen, Cotton, Pearce, Newman and McCutcheon18 and 19.1 years (s.d. = 2.8). Reference Chanen, Betts, Jackson, Cotton, Gleeson and Davey17 It is not clear whether study findings relate to this review’s age range or are skewed towards older cohorts.
Medical evidence preferences clinical trials, which often use diagnoses to establish inclusion criteria. Diagnoses facilitate succinct patient descriptions, guiding management and categorising cases for research purposes. Reference Cook and Décary54 The HYPE studies included young people matching various numbers of criteria for the DSM-IV definition of BPD. BPD is a controversial diagnosis in under-18-year-olds who present with complex interplays of systemic, relational and psychological distress. Reference Johnstone55 Further work is needed to understand which profiles of under-18-year-olds might benefit most from CAT.
Publications for CAT within CAMHS are predominantly lower-level evidence. 10 Of the total, 27 articles (73%) include author reflections and service descriptions, including 1 grounded theory. Reference Priddy, Kellett, Goodall and Cotton14 Although it is assumed the authors are experienced CAT clinicians, only 10 articles (37%) include explicit statements of authors’ or service providers’ expertise in CAT, reducing evidence reliability and possibility of accurate replications of services.
Inherent bias likely exists for the positive effects of CAT within CAMHS in expert-opinion articles and, by extension, this scoping review. The thematic summary of reflective articles was informed by the author’s (S.A.) clinical experience of CAT with under-18-year-olds. The author viewed CAT as beneficial for under-18-year-olds. To minimise bias, the thematic summary was reviewed by co-authors.
Calvert & Kellett (2014) offer ideas for future CAT research. Reference Calvert and Kellett56 Owing to the limited number of studies, with often small sample sizes, evidence-based practice and practice-based evidence are often considered equally. Similar observations are made in this review. The lack of substantive empirical evidence for CAT with under-18-year-olds should not be misinterpreted as lack of effectiveness. Practice-based evidence is acknowledged in mental healthcare and the ‘development of evidence is not a simple linear process, but a cycle of ongoing development and evaluation’. Reference Taylor and Hartley53,Reference Craig, Dieppe, Macintyre, Michie, Nazareth and Petticrew57 Although high-value evidence, RCTs may overlook complex interpersonal dynamics within the therapist–patient relationship. Future CAT research with under-18-year-olds needs to balance evidence-based practice and practice-based evidence. Research strategies, including single diagnostic category studies, large-scale pragmatic trials and single-case experimental design studies, should be considered with under-18-year-olds to determine cost and clinical effectiveness of CAT.
About the authors
Emma Salter is a child and adolescent consultant psychiatrist in Avon and Wiltshire Mental Health Partnership NHS Trust, Bristol, UK. She is a cognitive analytic therapy (CAT)-trained practitioner. Matthew Carr is a psychiatry resident working in CAMHS in Avon and Wiltshire Mental Health Partnership NHS Trust, Bristol, and a child and adolescent psychodynamic psychotherapy student at the Tavistock and Portman NHS Foundation Trust, London, UK. Frank Reakes is a child and adolescent consultant psychiatrist in Oxford Health NHS Foundation Trust, Oxford, UK. Scott Ankrett is a principal clinical psychologist and CAT practitioner with the CAMHS, Somerset NHS Foundation Trust, Wells, UK.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjb.2026.10218.
Data availability
Data availability is not applicable to this article as no new data were created or analysed in this study.
Acknowledgement
We thank Steven Walker, Avon and Wiltshire Mental Health Trust Library Service, for support in discussing and finalising the search criteria and providing Research Information Systems (RIS) files to faciliate initial screening.
Author contributions
E.S. was involved in initiation of the project, approval of search criteria for the methods, initial screening of articles and further review of inclusion criteria for the paper. She wrote the background and methods. She analysed and wrote the results for service description articles and discussion. M.C. was involved in initiation of the project and further review of inclusion criteria for the paper. He analysed and wrote the results for quantitative articles and discussion. F.R. was involved in review of the methodology and further review of inclusion criteria for the paper. He analysed and wrote the results for quantitative articles and discussion. S.A. was involved in initiation of the project and further review of inclusion criteria for the paper. He analysed and wrote the results for expert reflection articles and discussion. All authors were involved in editing and approving the final article for submission.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.





 Open access
Open access
eLetters
No eLetters have been published for this article.