


Introduction
Family caregivers provide the majority of care for individuals with life-limiting illnesses (Fast et al., Reference Fast, Duncan, Keating and Kim2024). In Canada, over one-quarter of adults are caregivers to a loved one (Canadian Centre for Caregiving Excellence, 2022). High-intensity caregivers (those who provide more than 20 hours of care per week) face disproportionate risks of burnout, income loss, and social isolation (Lee et al., Reference Lee, Baik, Becker and Cheon2022; Schulz & Sherwood, Reference Schulz and Sherwood2008). The undervaluation of care work disproportionately impacts women who comprise the majority of the caregiving labour force, reinforcing gendered expectations regarding the division of labour (Heger & Korfhage, Reference Heger and Korfhage2020). Despite the essential role they play in sustaining health care systems, many caregivers receive limited formal support, prompting calls for policy responses that recognize unpaid care work. One such intervention is direct financial remuneration, which has been adopted across many nations as a policy response to support the financial burden incurred by intensive caregivers (Rocard & Llena-Nozal, Reference Rocard and Llena-Nozal2022). Current research regarding the impact of direct remuneration programs demonstrates benefits such as enhanced financial stability, reduced stress, and increased feelings of recognition (Giesbrecht et al., Reference Giesbrecht, Crooks and Williams2010; Simon-Rusinowitz et al., Reference Simon-Rusinowitz, Mahoney, Loughlin and Sadler2005). However, much of this research focuses on program outcomes rather than the firsthand experiences of the caregivers navigating and receiving these benefits (Leger, 2021; Mihailescu, Reference Mihailescu2021). This study contributes to this body of knowledge by exploring how caregivers receiving Nova Scotia’s Caregiver Benefit perceive its value, limitations, and role in supporting their caregiving responsibilities.
Nova Scotia’s Caregiver Benefit program (also referred to as the Benefit) was created in 2009. The program represents a material and symbolic recognition in the landscape of family caregiving. It is the first Canadian program to provide a monthly allowance to family caregivers in support of their caregiving roles and to enhance their material capacity to provide care for their loved one(s) (O’Hara, Reference O’Hara2014). The Benefit is administered by Continuing Care, a branch of the Nova Scotia Department of Health and Wellness. The Benefit offers caregivers $400 per month if both the caregiver and the care recipient adhere to the following eligibility criteria: both the caregiver and the care recipient must be at least 19 years of age and a resident of Nova Scotia; and the caregiver must provide at least 20 hours of care per week through self-reporting and verified through a home care assessment. It is needs-based in accordance with the care recipient’s annual income, which must be less than $31,661 for a single caregiver or $46,662 for those who are married or partnered (Nova Scotia Department of Health and Wellness, 2025). The care recipient and the caregiver may reside within the same household, with eligibility extending to co-residing spousal caregivers. As of April 2025, 3,303 caregivers have received the Caregiver Benefit (Caregivers Nova Scotia, 2025).
The stated goal of the Benefit is to recognize the contribution of caregivers by ‘assist[ing] the caregiver in sustaining the support they provide’ (Government of Nova Scotia, 2021). However, this objective is articulated in broad terms. It is unclear whether the program is intended primarily as a symbolic recognition or a mechanism to enhance affordability. This ambiguity reflects the use of generalized policy language that offers limited insight into the program’s underlying purpose. Access to services such as the Caregiver Benefit is restricted through referrals and care recipient evaluations to receive access, and these restrictions can prevent caregivers from receiving subsequent supports (Flood et al., Reference Flood, DeJean, Doetter, Quesnel-Vallée and Schut2021). This lack of communication and information sharing between different organizations translates into a fragmented patchwork of supports that are inaccessible to caregivers (Canadian Centre for Caregiving Excellence, 2022; Leger, 2021). A 2021 study estimated that only 13 per cent of Nova Scotian caregivers have received the Caregiver Benefit (Leger, 2021), indicating limited access from its intended audience.
The experiences of caregiver advocates indicate that the program’s adoption required sustained grassroots effort, reflecting decades of mobilization to gain recognition within Nova Scotia’s policy agenda. The Benefit has persisted in spite of changes in government and the varying priorities of different political parties, yet the monthly financial payment amount has remained unchanged since 2009. This is reflective of fiscal conservatism and a limited political will to expand direct financial support for caregivers (Mihailescu, Reference Mihailescu2021). These historical and political dynamics position the Caregiver Benefit not only as a material support mechanism but also as a discursive object. The program’s language, eligibility criteria, and structure function as a symbolic text through which societal recognition of caregiving labour is articulated, representing the assumptions and values engrained within policy design. As a text, the Benefit communicates both acknowledgement of caregiving and the constraints imposed by broader political and fiscal priorities, demonstrating the existing tension between symbolic recognition and practical support.
To date, no research has been conducted on how caregivers experience the Caregiver Benefit in relation to their caregiving duties (O’Hara, Reference O’Hara2014). This study aims to fill this knowledge gap by exploring the experiences of high-intensity caregivers in Nova Scotia who receive the Caregiver Benefit to gain insight into how they conceive of the program’s impact. By situating caregiver experiences within both the operational and discursive dimensions of the Benefit, this study provides a nuanced lens for understanding the implications of the Caregiver Benefit for high-intensity caregivers. As other provinces and jurisdictions consider the development of their own direct remuneration programs for caregivers (e.g., Prince Edward Island’s At Home Caregiver Benefit, established in 2024), this study offers transferability in its findings regarding the advantages, barriers, and opportunities offered through Nova Scotia’s longstanding program.
Methodology
Study design
This study uses a qualitative descriptive approach. This design enables direct descriptions of experiences and phenomena that are easily understood and adopted by a wide variety of stakeholders, particularly those situated within the policy realm (Sandelowski, Reference Sandelowski2010). The emphasis on practical findings is appropriate for this study as it aims to highlight real-world implications of the Caregiver Benefit in its current state and identifies areas for improvement that are reflected in the lived experiences of caregivers.
Sample
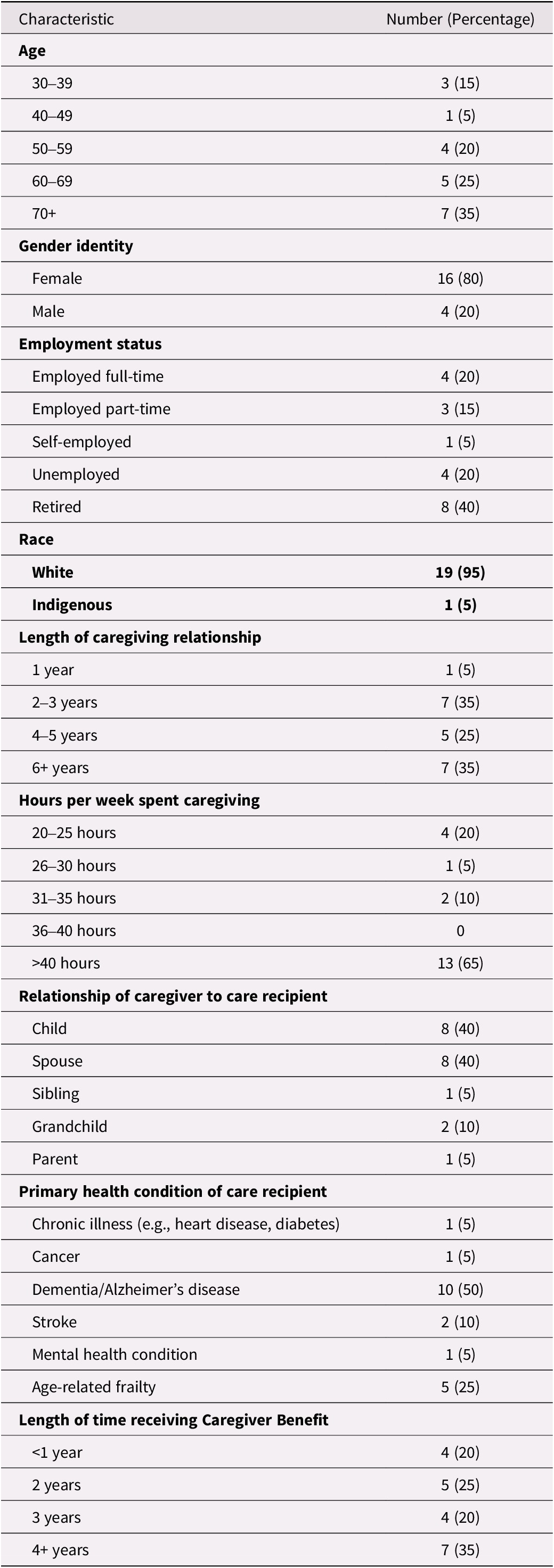
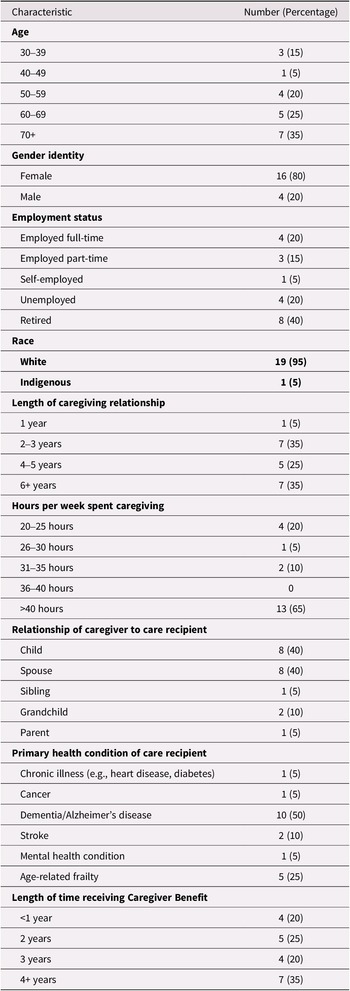
Our sample was composed of 20 current or former beneficiaries of the benefit (see Table 1 for a full description of demographic characteristics). Purposive sampling was used, including criteria and snowball sampling. The inclusion criteria of this study are as follows: (a) caregivers who are 19 years of age or older, (b) reside in Nova Scotia, (c) provide greater than or equal to 20 hours of care per week to a family member or loved one, (d) are currently receiving or have previously received the Caregiver Benefit, and (e) are fluent in English.
Demographic characteristics of participants (n = 20)
The theory of information power was used to determine data sufficiency (Malterud et al., Reference Malterud, Siersma and Guassora2016). According to this theory, the more information relevant to the study aim contained within the sample, the smaller number of participants are required. This is informed by five key elements: (a) the study aim, with narrower aims requiring fewer participants, (b) sample specificity, where highly specific and information-rich samples reduce the need for further sampling, (c) the application of established theory, which can support a smaller sample when guiding analysis, (d) the quality of dialogue, with rich interviews contributing to higher informational power, and (e) the analysis strategy, where in-depth analyses require fewer participants than broader cross-case comparisons (Malterud et al., Reference Malterud, Siersma and Guassora2016). Given our study’s narrow aim, recruitment of a specific sample of high-intensity caregivers with direct experience receiving the Caregiver Benefit, and the application of Pearlin’s stress process model for caregiving (Pearlin et al., Reference Pearlin, Mullan, Semple and Skaff1990), 20 participants provided a sufficient sample size to address the research question. The informational power of the data was continuously assessed concurrent with the interviews and analysis. In alignment with the tenets of this theory, a small sample size was anticipated due to the narrow aim of this study, the specificity of participant experiences, and the extensive and robust nature of participant dialogue.
Recruitment
Caregivers were predominantly recruited through digital media postings and listserv email distributions of the recruitment poster by care coordinators at Caregivers Nova Scotia. A social media post was also shared by the Alzheimer’s Society of Nova Scotia. Snowballing was also used in instances where participants had peers who they felt could impart valuable insights towards the study.
Data collection
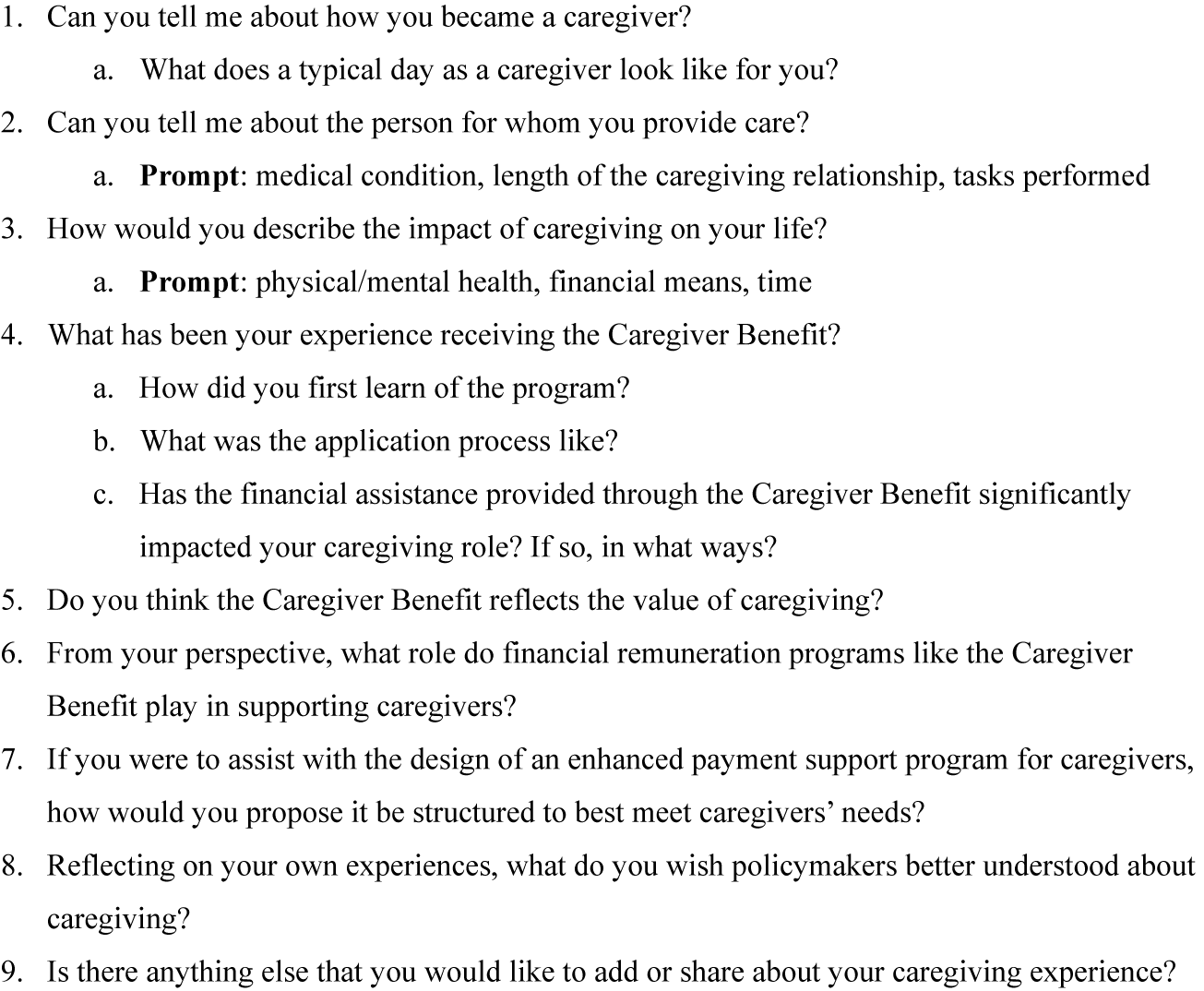
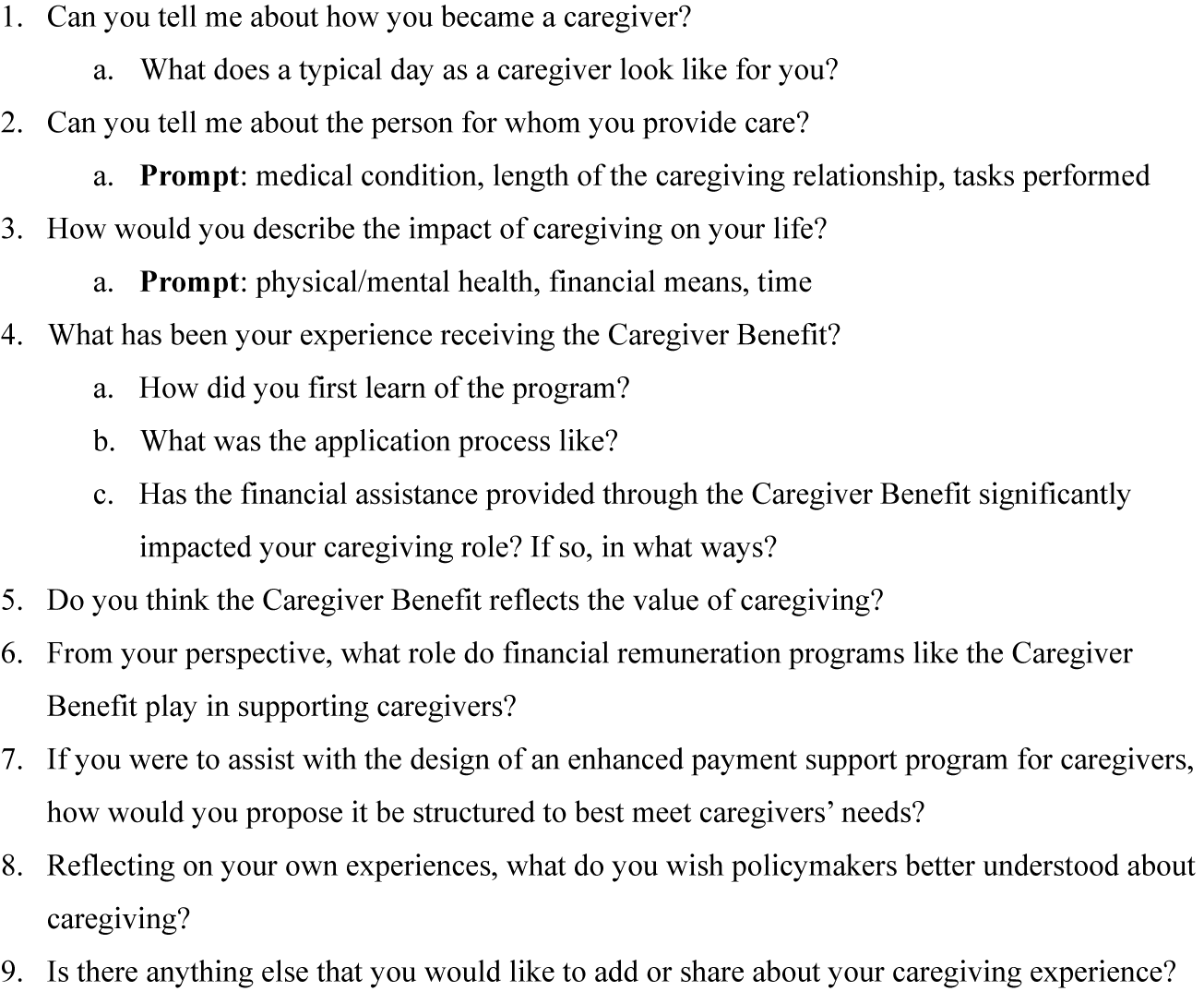
Data collection occurred from March 2025 to June 2025. Demographic data were collected via LimeSurvey, including age, sex, racialization, length of caregiving relationship, employment status, hours of care provided per week, relationship between caregiver and care recipient, and health condition of the care recipient. The interview guide was developed through collaborative dialogue between the first and last author and through consultations with connections at Caregivers Nova Scotia (see Figure 1 for the interview guide). This review process ensured that questions were reflective of the goals of the study and elicited information about caregiver experiences in an open way, while also attending to their emotional realities, enabling a compassionate approach to data collection.
Semi-structured interview guide.
Semi-structured, one-on-one interviews were held with each participant and facilitated by the first author via Zoom (n = 15) or by telephone (n = 5). To mitigate the risk of fraudulent participation, participants were screened during recruitment to confirm their eligibility for the Caregiver Benefit and their caregiving role, and interviews included contextual questions about their caregiving experiences that verified the authenticity of participant accounts. Interview length ranged from 35 minutes to 2 hours (average interview length: 65 minutes). Written and verbal consent was obtained for audio recording. The first author transcribed all interviews verbatim to ensure that participant data were accurately captured and subsequently de-identified for purposes of participant confidentiality.
Data analysis
Data analysis was conducted using NVivo software (version 15) for coding, thematic analysis, and data management. The six stages of thematic analysis as outlined by Braun and Clarke were followed: (a) gaining familiarity with data, (b) coding, (c) theme location, (d) reviewing themes, (e) developing a definition for themes, and (f) developing a report (Clarke & Braun, Reference Clarke and Braun2014). Interview transcriptions were reviewed twice by the first author prior to coding to become familiar with the data, and initial impressions and key ideas were captured through reflexive notes. Constant comparative analysis was used to highlight convergences and divergences across participant experiences and responses, aligning with the principles of the qualitative descriptive methodology. Themes were identified by the first author through initial codes to capture important patterns across interviews. Subsequently, preliminary themes were reviewed and discussed among all authors to reach a shared understanding.
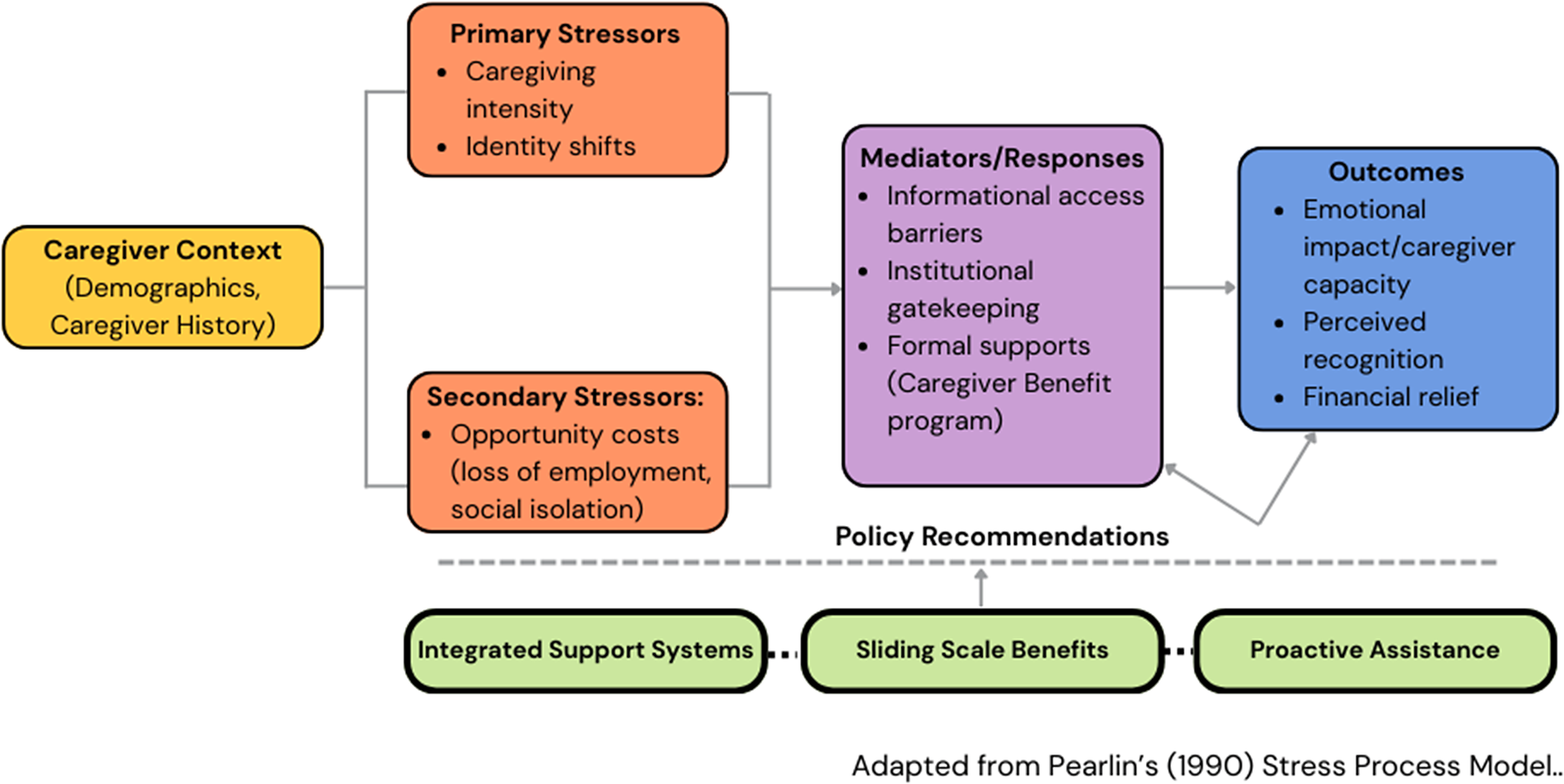
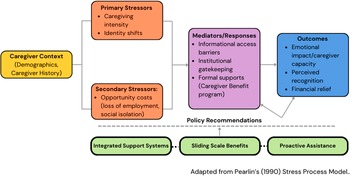
This study uses an integrated framework based around the Pearlin’s stress process model for caregiving (Pearlin et al., Reference Pearlin, Mullan, Semple and Skaff1990) alongside policy-as-text analysis. In this approach, caregiving intensity, identity shifts, and foregone opportunities are conceptualized as stressors that shape caregivers’ expectations of support (Pearlin et al., Reference Pearlin, Mullan, Semple and Skaff1990). These factors interact with policy dimensions, such as the Benefit’s perceived value, access barriers, and payment amount. Pearlin’s model explains how intensive caregiving catalyses role strain, which influences how caregivers consider the $400 per month benefit (see Figure 2 for a visual adaptation of Pearlin’s model). Concurrently, policy-as-text analysis evaluates the Benefit’s design and language as communicating societal recognition of caregiving, subject to constraints such as policy fragmentation and a lack of outreach, stringent eligibility rules, and funding limits. Together, these approaches demonstrate how structural factors and caregiver stressors jointly influence considerations of supports like the Caregiver Benefit.
Adaptation of Pearlin’s stress process model for caregiving.
To validate the robustness and trustworthiness of this study, the first author maintained a reflexive journal which was used following each interview to document initial responses and identify how previous experiences may colour such reactions. The trustworthiness criteria outlined by Lincoln and Guba were followed through the duration of this study (Lincoln & Guba, Reference Lincoln and Guba1985). Credibility was fostered through open collaboration and discussion regarding thematic findings with co-authors versed in caregiving, policy research, and/or qualitative methods.
Ethical considerations
Ethics approval for this study was received from the Research Ethics Board (#17869). Prospective participants spoke with the first author prior to scheduling an interview to review an informed consent document and demographic survey (collected via LimeSurvey). This discussion allowed for a conversation regarding the study’s goals, data handling procedures, and the voluntary and ongoing role of consent. All interview transcriptions were completed verbatim by the first author. Transcriptions were stored on an encrypted device accessible only by the first author. Participants were provided with an anonymized version of their interview transcription for their reference and to allow for the opportunity to add or redact any comments. An incentive of a $50 gift card was provided to caregivers who participated in the study in appreciation of their time.
Reflexivity
As health services researchers, our interest in financial remuneration for family caregivers is informed by both academic and experiential perspectives. Our prior experiences and research knowledge examining caregiver burden, including economic strain and gendered labour patterns, have influenced our underlying assumption that caregiving is a systematically undervalued pursuit which would benefit from formal compensation mechanisms. This perspective influenced the study’s emphasis on quantifying out-of-pocket expenditures in addition to the inclusion of gender and socioeconomic variables. Simultaneously, the research team remained attentive to alternative interpretations of the data, including the potential that financial remuneration has diverse impacts across caregiver groups. To ameliorate potential bias, we employed standardized analytic approaches and interpreted findings in ways that recognize both supporting and conflicting evidence within the literature.
Results
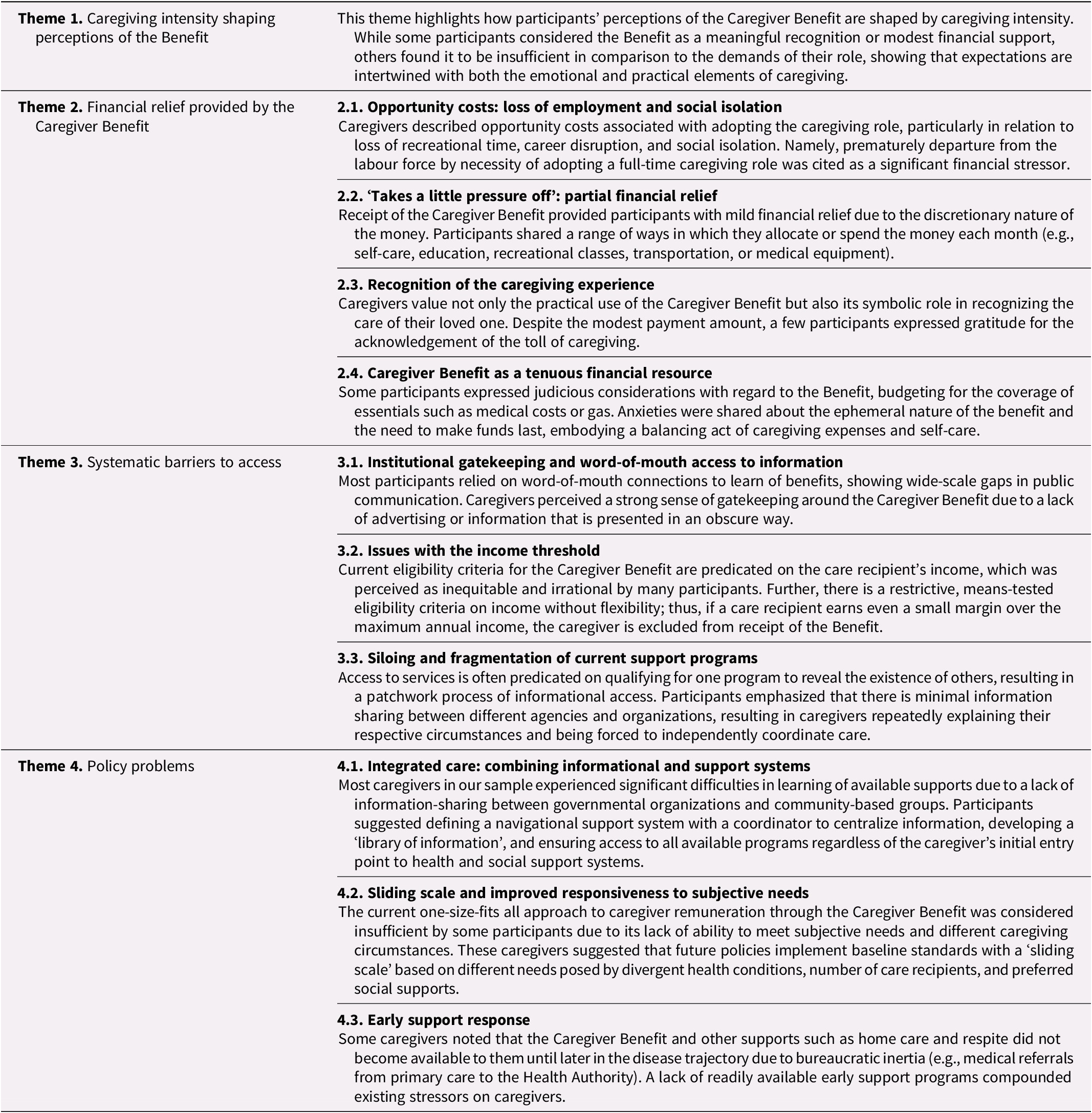
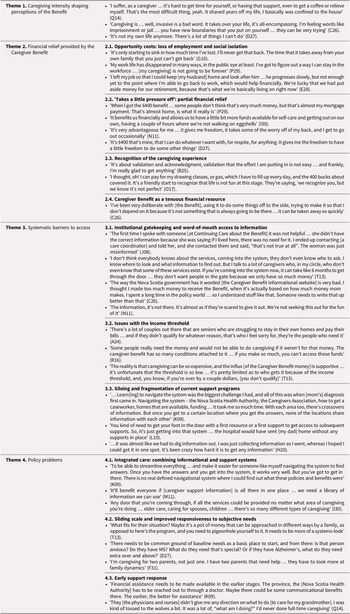
Twenty family caregivers participated in this study. The majority of the sample (n = 16) included female caregivers providing care to a parent or spouse with dementia or Alzheimer’s disease. Although 53 per cent of caregivers in Nova Scotia are women (Research on Aging Policies and Practice, 2020), 80 per cent of our study sample identify as women. Similar to the demographic profile of Nova Scotia, our sample is predominantly comprised caregivers of a parent with dementia and/or age-related frailties (Leger, 2021). Over half of the sample identified as full-time intensive caregivers who provide more than 40 hours of care per week. A survey of Nova Scotian caregivers measured the provincial average at 40 hours of care provided per week (Leger, 2021). The most recent data provided by Nova Scotia Continuing Care estimate the average age of Benefit recipients to be 68 (Government of Nova Scotia, 2013), whereas the average age of this sample was 61. Four themes and 10 sub-themes were identified (see Table 2 for a detailed summary of main findings and Table 3 for key illustrative quotes from participants). Though most participants in this study have received the Caregiver Benefit for less than 3 years, a few participants (n = 3) started receiving the Benefit shortly after its inception.
Descriptions of themes
Key participant quotes
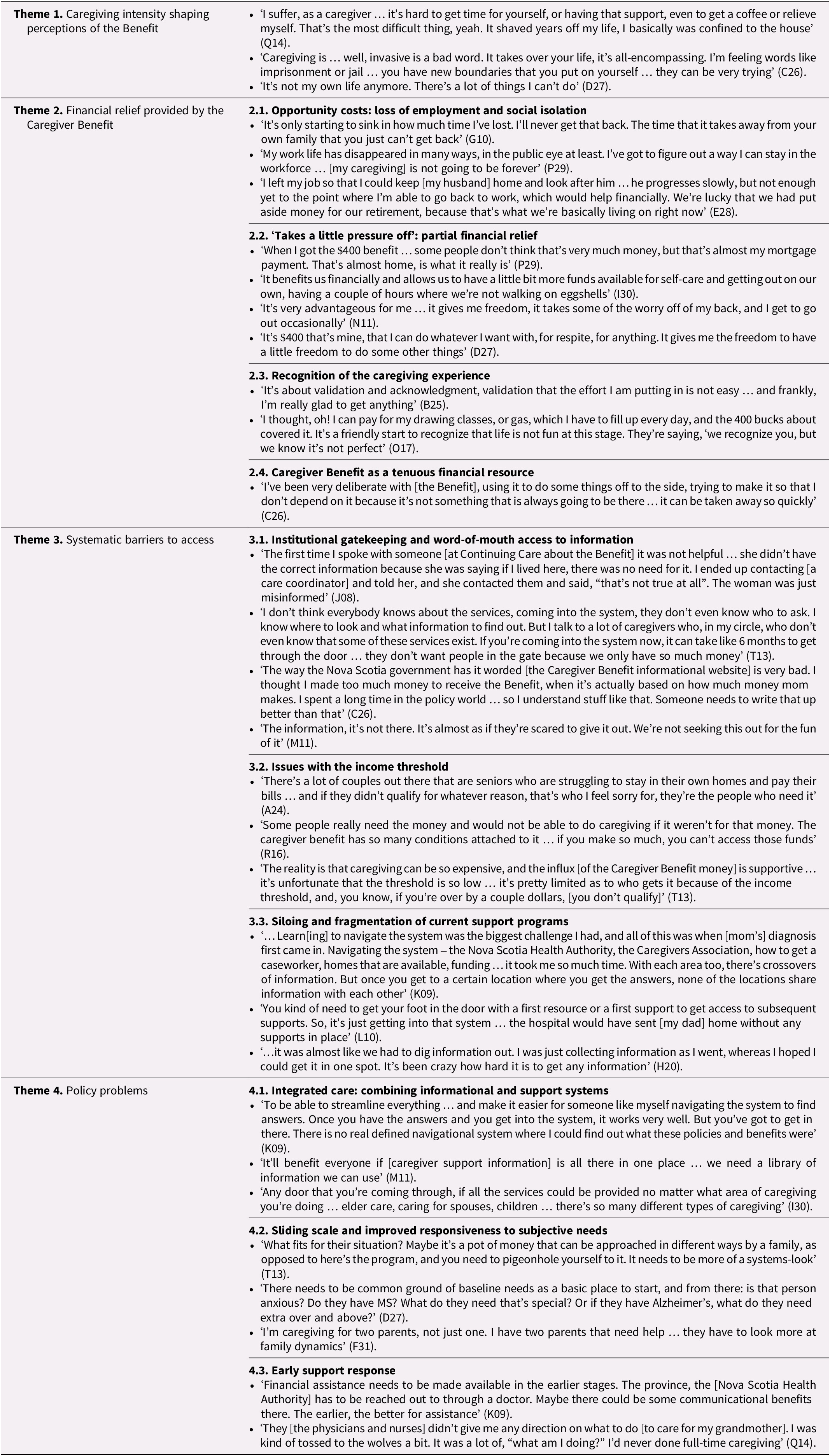
The goal of this study is to explore the experiences of high-intensity caregivers in Nova Scotia who are recipients of the Caregiver Benefit in order to elucidate their perspectives of the program’s impact. The themes illustrate how caregivers interpret the Caregiver Benefit within the broader context of intensive caregiving and navigating support systems. Participants’ experiences of caregiving intensity shaped how they understood the purpose and adequacy of the Benefit. These interpretations were closely related to the financial pressures associated with caregiving, in addition to the systemic barriers encountered when trying to access formal supports. Participants reflected on how current policy structures could be modified to better respond to the needs of caregivers.
Theme 1: Caregiving intensity shaping perceptions of the benefit
This theme examines the daily realities that impacted participants’ caregiving roles and subsequently informed their experiences and perceptions of the Caregiver Benefit. Perceptions of the Benefit were not formed in isolation, but were shaped by the intensity, identity shifts, and lost opportunities associated with caregiving. The intensity of the caregiving role on participants’ lives shaped expectations of the Benefit, varying from symbolic recognition, partial compensation for lost employment, or an insufficient response to the scope of their responsibilities.
Many participants described caregiving as redefining their sense of self, autonomy, and daily life as they had to reassess other elements of their personal and professional lives to accommodate the intensity of the caregiving role. Caregiving responsibilities often evolved into an all-encompassing role, which one participant described as ‘feeling so tied’ (A24) to their caregiving responsibilities. Several caregivers noted the challenge of maintaining ‘a life beyond [the] caregiving situation’ (C26) or preserving any real ‘freedom of action’ (O17). The totalizing nature of this shift left one participant feeling as though there was ‘nothing outside of it’ (E28). These experiences demonstrate that caregiving is not experienced as a set of duties but rather as a totalizing role that necessitates a reorganization of time and personal identity.
For caregivers who felt that caregiving had become a central part of their identity, the Benefit was often perceived as a modest but valued form of recognition. One participant emphasized appreciation simply for the availability of the program: ‘it’s not a lot of money … [but] we’re so blessed to have what we have…I know how hard this can be on some people’ (L10). Contrarily, others described the Benefit as disproportionately low considering the totalizing nature of the caregiving role: ‘it’s so low, if that’s your [only source] of pay … it lasts for no time, it’s so sad. Nobody can live off [that]’ (G10). Simultaneously, some caregivers described caregiving as intrinsically meaningful regardless of its intensity due to self-discovery and enhanced closeness with the care recipient: while the role comprises of ‘a mountain of work, I was changed, and it was really rewarding’ (Q14). These positive identifications sometimes moderated expectations of the Benefit, with participants framing it less as compensation and more as a supportive mechanism that eased the weight of their duties. These accounts emphasize how perceptions of the Caregiver Benefit are shaped by an interplay between the monetary value and the broader emotional shifts associated with the intensive caregiving role.
Theme 2: Financial relief provided by the Benefit
One of the central motivators underpinning this study was to determine the extent to which the Caregiver Benefit offers a form of meaningful financial support and recognition towards the labour of caregivers. This theme explores how caregivers perceive the Benefit with regard to relieving the financial pressures of caregiving, appreciation for the existence of such a program in Nova Scotia, and how caregivers make determinations about budgeting and expenditures.
Sub-theme 2.1. Opportunity costs: Loss of employment and social isolation
Forfeitures in personal lives were central to how caregivers considered the Benefit. Participants described significant opportunity costs associated with caregiving; notably, a loss of employment and constrained social capacity. Due to the full-time nature of caregiving and how it permeates other elements of the caregivers’ lives, several participants discussed an inability to retain their social lives, job prospects, and other aspects of personal autonomy. Some working-age participants reported resigning from the workforce prematurely due to the intensity of their caregiving demands. One respondent resigned from employment so that her spouse could remain at home, despite anticipation of financial hardship: ‘he [didn’t] want to do that [live in long-term care], and I [didn’t] want to do that’ (E28), showing how caregiver decision making is often shaped by relational and moral commitments rather than economic rationale. Another participant noted that 6 years outside of the workforce resulted in her ‘work life … disappear[ing]’ (P29), citing limited opportunities flexible enough to accommodate full-time caregiving responsibilities.
For those who were unable to balance their caregiving responsibilities alongside workforce involvement, the Benefit was often interpreted as a small but necessary supplement to provide economic support: ‘the $400 a month is definitely helpful, but … how can I go back to work, how can we make this work financially? We just don’t bring in enough money’ (E28), referring to the structural tension between caregiving responsibilities and labour market participation. Caregivers experiencing significant social disruption often found the Benefit insufficient without provision of broader structural supports such as respite services or peer support to mitigate feelings of isolation: ‘I have so much support, and even I feel isolated … [we need] peer support groups available for caregivers too’ (I30). These experiences suggest that while the Benefit provides a minor amount of financial relief, it does not address the opportunity costs implicit in caregiving that extend beyond income loss to social disconnection and constrained life opportunities.
Sub-theme 2.2. ‘Takes a little pressure off’: Partial financial relief
Over half of participants found that the monthly receipt of the Caregiver Benefit provided some sense of financial solace, often described as modest but meaningful relief within otherwise constrained financial circumstances. Participants shared perspectives such as ‘it takes a little pressure off, it’s a little extra money for something else’ (B25) and ‘it helps you kind of go, okay, there’s one less thing I need to worry about’ (C26), suggesting that the Benefit functioned to alleviate immediate financial stressors rather than fundamentally altering the caregivers’ economic situations. For others, this relief was tied to the ability to cover specific, recurring expenses, with one participant noting that ‘it takes care of a bill that we don’t have to worry about … it gives us a little bit more discretionary funds to pay down debts’ (I30), showing how the Benefit provided limited financial flexibility and reallocation of resources.
Considering the financial costs incurred by the scope of caregiving responsibilities, two participants discussed the ‘importance … of that extra money to be able to buy diapers, to not have to scrape to buy diapers’ (D27) and affording ‘medications … they are atrocious right now … [the Benefit] comes in handy’ (M11). In this way, the Benefit was experienced as a mechanism that ameliorated day-to-day financial precarities, allowing caregivers to manage standard caregiving-related expenses with slightly enhanced stability. For some, this buffering effect extended to larger life decisions. One participant shared that ‘[is] that extra buffer that has allowed me to not really look for employment outside … without it, I probably would have had to find work, somehow’ (E28), showing that modest financial supports may still influence labour market participation and caregiver capacity. Others found that the Benefit allowed them an ability to regain some level of control over their personal lives outside of their caregiving role, using the funds as ‘a little bit extra … to pay off my student loans’ (S19) or to ‘pay the hotel and gas to [visit my children]’ (I30). These experiences suggest that although the Benefit is not financially substantial, it provided caregivers with a level of financial agency that allowed them to navigate competing demands and regain control over caregiving-related costs and personal expenditures.
Sub-theme 2.3. Recognition of the caregiving experience
Regardless of divergent opinions regarding the financial sufficiency of the Caregiver Benefit, some participants emphasized its importance, framing it as a critical support within an otherwise absent arrangement of caregiver financial supports. Some described it as ‘crucial … it’s crucial. Not only for me, but for my spouse, my loved one. It’s vital that it’s provided. Without it … something very serious is going to happen’ (K09), and as something that ‘it gave me some light to keep on going … it has bought me a little bit of time to restructure [our] finances’ (P29). This suggests that the Benefit was experienced as a stabilizing mechanism by which caregivers were able to sustain their roles during periods of heightened emotional and financial strain. For others, the Benefit was considered in relation to broader system-level factors, with a participant noting that he would be ‘lost [without it] … I struck gold. This is basically more economical for them to give me financial assistance than to keep her in the hospital … it’s very much appreciated’ (N11). This perspective reflects an awareness of the cost-saving mechanism of caregiving, locating the Benefit as a broad exchange between caregivers and the health care system. There was also a sense of pride and appreciation that Nova Scotia was the first province to offer a direct financial benefit to caregivers (and the sole one, until 2024): ‘I am so thankful for what the government does here for us in Nova Scotia, I say it all the time’ (C26), and ‘when they gave me [that] pot of money … it was something. I can’t believe Nova Scotia would be that progressive’ (H20). Many participants highlighted the flexibility of the Benefit, noting that the absence of spending restrictions allowed them to allocate the funds towards needs that were most pertinent to their own caregiving experiences: These reflections represent the symbolic importance of the Benefit beyond the monetary value, contributing to perceptions of social recognition. Other participants discussed the flexibility of the Benefit, noting the lack of spending restrictions which allowed them to allocate funds to their own self-assessed needs. For some, this extended beyond immediate caregiving expenses to include aspects of self-care and preservation of personal identity, such as ‘I thought … I can pay for my drawing classes [which] I quit [when] I was focused on [my husband’s care]’ (O17), showing that the Benefit could facilitate self-reclamation within the intensive caregiving context. Given the often taken-for-granted and hidden nature of caregiving through the vantage point of the policy realm, some caregivers found the element of recognition important on its own: ‘it’s about validation and acknowledgment … the degree of validation that the effort I’m putting in is not easy’ (B25), ‘the acknowledgment is that we’re going to use it for something that will bring us, hopefully, some peace’ (T13). Collectively, these accounts underscore the role of the Benefit as both a material support and a symbolic acknowledgement of caregiving labour, with perceived value encompassing validation and a sense of being seen within health and social support systems.
Sub-theme 2.4. Caregiver benefit as a tenuous financial resource
A few participants shared that they exercise a strong degree of judiciousness when allocating the Benefit towards their monthly budgets, reflecting an underlying sense of uncertainty regarding the position’s continuity. This was linked to the conditional nature of eligibility, especially if the care recipient transitioned into institutional care. One participant explained ‘I don’t depend on it because it’s not something that is always going to be there’ (C26), showing that the perceived transient nature of the Benefit shaped conservative financial decision making and limited integration into long-term planning. For others, this caution was exacerbated by previous experiences with government programs, which resulted in apprehension towards future financial penalties. Another participant worried that future ineligibility could result in a repayment onus she would be unable to meet: ‘I almost didn’t apply for the Caregiver Benefit [because] when the CERB [Canada Emergency Response Benefit] program had happened, I had to pay that back … I didn’t want to mess with the government [and] I knew I couldn’t afford to pay money back [again]’ (P29). This experience shows how trust in public programs and previous interactions with them can influence perceptions of the Benefit and apprehensions caregivers may have around uptake.
Although the Benefit provided modest financial relief for many participants, these accounts showed that its impact was often constrained by broader structural challenges within caregiving support systems.
Theme 3: Systemic barriers to access
Caregivers consistently encountered structural and systematic barriers that limited their ability to access supports such as the Caregiver Benefit. These challenges reflect a form of administrative burden; specifically, the learning and psychological costs individuals experience when interacting with complex publicly administered programs. Participants described significant efforts taken to locate information, navigate eligibility requirements, and coordinate across fragmented social support systems.
Sub-theme 3.1. Institutional gatekeeping and word-of-mouth access to information
Difficulties gaining entry and access to the Caregiver Benefit and supplemental caregiving supports were the most widely shared experience among all participants. Many participants felt that this was not coincidental and was instead by design to restrict numbers and keep people out of the system: ‘the government makes everything so difficult for people to apply’ (A24), ‘[the government], they’re gatekeepers, they don’t want people on the gate, ‘we only have so much money, let’s keep them out’ (T13), and ‘it’s almost as if they’re scared to give it [the Caregiver Benefit] out’ (M11). These perceptions suggest that program accessibility was interpreted both as an administrative challenge and as an expression of resource constraints and prioritization decisions. As a result, many participants only learned of the Caregiver Benefit and started to receive it due to word-of-mouth communications from peers and colleagues, indicating a reliance on social networks to navigate access. Participants described learning about the program through peers: ‘my sister … told me the [province] gave something to people who support’ (C26), ‘I reached out to friends and I got the right information and I started putting things together’ (K09), ‘I didn’t even know about it until my colleague mentioned it to me’ (Q14), and ‘I learned about the program because of a … support group’ (P29). This reliance on family networks demonstrates inequities in access, in which caregivers without strong social or informational networks could remain unaware of available support benefits. A handful of participants found that Continuing Care was not forthcoming about the existence of the Benefit, and that it is not widely advertised: ‘our continuing care worker didn’t tell us about it … I told her about it, [and] I had to dig it out of her’ (H20), reinforcing perceptions of opacity within formal support systems.
Sub-theme 3.2. Issues with the income threshold
Income-based restrictions for the Caregiver Benefit proved to be a significant pain point for many participants; namely, that receipt of the Benefit is predicated on the care recipient’s income rather than that of the caregiver. Participants frequently interpreted this as a disjuncture between policy intention and the lived experiences of caregivers. A participant argued that ‘it really shouldn’t have anything to do with mom because the money isn’t going to mom, it’s going to the person that’s looking after her … those kinds of things are very frustrating’ (A24), while another stated that ‘it doesn’t make sense that it’s based on [mom’s] income … her income doesn’t support me … I don’t know why it’s based on that’ (H20). These accounts indicate that the current eligibility criteria ignore the economic vulnerability of caregivers by predicating access to supports on the financial status of another individual. Skepticism was shared regarding the motive behind basing eligibility on the care recipient’s income, with some interpreting it as a mechanism to systematically exclude caregivers: ‘I’ve always kind of questioned [that] … anybody who has a pension is not going to be eligible right off the bat, [and] that doesn’t acknowledge the caregiver’ (T13). The current income threshold was described by some participants as extremely low and strictly enforced, with one caregiver sharing that their parent had been rejected from receipt of the Benefit the first time due to surpassing the means assessment by less than 100 dollars. Such experiences highlight how tightly defined eligibility criteria can result in exclusion of caregivers at the margins, validating perceptions that the program does not consider the financial realities faced by caregivers.
Sub-theme 3.3. Siloing and fragmentation of current support programs
A lack of integration between current support programs was described as a significant obstacle by over half of participants, complicating access to the Caregiver Benefit and other support resources. One participant characterized the system as disconnected and fragmented ‘they’re all their own separate things, like two doors across the hallway. No communication … it’ll benefit everyone if [all information] is all out there in one place’ (M11), demonstrating how institutional silos result in inefficiencies for caregivers in need of supports. Participants described navigating multiple organizations as there is no central conduit for support information, and that this required a substantial time cost: ‘each [organization] provides new information … once you have the answers and you get into the system; it works very well … but you’ve got to get in’ (K09). This distinction shows how the burden of informational navigation falls on caregivers who already lack an abundance of time due to the demands of their caregiving circumstances. In some cases, clinicians and allied health professionals also lacked the insight to assist with navigation efforts: ‘a lot of times, people don’t know about services … the social worker didn’t say, “we got this program”. They didn’t know about the program!’ (P29), gesturing to systemic gaps in coordination across sectors.
These barriers collectively shaped how caregivers ultimately appraised the usefulness of the Caregiver Benefit, revealing that the effectiveness of the program is mediated by both the financial value and the broader systems in which they are accessed and delivered. The experiences of these caregivers influenced their proposals regarding improvements which could be made to the Caregiver Benefit and other supports in the future.
Theme 4: Policy problems
Reflecting on the barriers and obstacles encountered when navigating the caregiving support system, participants often proposed policy modifications that could improve the responsiveness of the Caregiver Benefit and related programs. Three core suggestions arose among participants: (a) integrated care through the combination of current informational and support systems, (b) implementation of a sliding scale to better respond to the subjective needs of caregivers, and (c) the importance of support response early in the caregiving journey as a proactive policy measure.
Sub-theme 4.1. Integrated care: Combining informational and support systems
In response to the aforementioned systematic barrier of siloed resources, multiple caregivers suggested that current organizations (e.g., governmental agencies such as the Health Authority as well as community-based organizations) aggregate their information to provide caregivers with a full range of support options. As stated by one caregiver, ‘to be able to streamline everything … it would make it so much easier for someone like [me] navigating the system to find answers … maybe the provincial government could centralize some of these agencies into one or two departments [to] make it easier for us’ (K09), emphasizing how system-level coordination could reduce informational barriers and improve access to supports. Several participants noted that local community and advocacy organizations were more transparent and simpler to navigate in exploring available supports compared to governmental agencies. Other participants proposed the hiring of ‘a [provincial] care navigator … making sure anybody who’s receiving anything … knows about other services [too]’ (I30). This recommendation reflects a macro-level need for continuity and coordination of care, positioning navigational support as a crucial component of effective policy implementation.
Sub-theme 4.2. Sliding scale and improved responsiveness to subjective needs
A central recurring issue with the Benefit is the flat-rate payment without accommodation for personal contexts of the caregiving dynamic. In its current state, the program was found to be ‘a one-size-fits-all … it’s not taking into account where people’s pressures are, what might be a pressure for us may not be a pressure for another family’ (T13), indicating a disjuncture between standardized policy design and the diversity of caregiving experiences. While the minimum threshold to qualify for the Benefit entails a weekly caregiving equivalent to that of a part-time job, some caregivers felt that this amount should be scaled incrementally for different caregiving loads. One caregiver noted ‘I was spending over 100 hours a week [caring for my sibling] … there should be a difference based on the number of hours you commit’ (H20), underscoring how a flat-rate financial support obscures significant variation in caregiving labour. Three participants were simultaneously caregiving for both of their parents and thereby suggested that the greater number of care recipients should be accommodated: ‘when you multiply it by 2, it gets even worse’ (R16), ‘how many people would you be taking care of before they could say, “well, maybe we need to add a little bit more [to the Benefit payment]?”’ (C26). Participants also discussed the financial strain associated with complex medical needs, and that out-of-pocket expenses are variable and can often be substantial. One caregiver shared that ‘we paid for [so much] out of pocket … I bought a chair that was like, $2000 [and] the government didn’t do anything’ (S19), showing how a fixed Benefit payment fails to account for episodic expenditures. These accounts suggest that a more flexible model may better align financial supports with caregiving intensity and needs, improving the perceived fairness of the program.
Sub-theme 4.3. Early support response
Access to the Caregiver Benefit and other support programs was not immediately available at the outset of the caregiving trajectory for many participants, which was a significant source of stress. As a result, some participants stressed the importance of meeting caregivers with available support resources as early as possible to reduce anxieties and financial burden. As one participant stated, ‘the earlier the better when it comes to assistance … without it, something very serious is going to happen’ (K09). Speaking about their own onerous journey with applying for the Caregiver Benefit, one participant stated, ‘it should be more proactive versus reactive … [the Benefit] needs better structure, better rollout, to be better for the caregiver’ (Q14). This participant shared that due to a long waiting period, they did not receive the Caregiver Benefit until several months into their caregiving journey despite early application and persistent follow-up. Participants suggested that earlier and more structured provision could ease the transition into caregiving, with one caregiver proposing that agencies develop a resource guide outlining available resources from the outset: ‘[caregiving] agencies could design a booklet, say “this [is] the beginning of the process … so we have to be prepared” (M11). These recommendations reflect a need for anticipatory policy design that recognizes caregiving as an evolving trajectory rather than a static state.
These findings suggest that caregivers interpret the Caregiver Benefit as both a symbolic recognition of the caregiving role and a small financial support. However, its perceived adequacy is shaped by caregiving intensity and the broader policy environment within which caregivers must navigate to access supports.
Discussion
This qualitative descriptive study explored the perspectives of 20 family caregivers with experience receiving the Caregiver Benefit in Nova Scotia. As a whole, participants recognized and appreciated the novelty of this program in comparison to other Canadian jurisdictions. Though the sum of $400 per month was generally found to be low considering cost-of-living expenditures and care-related expenses, receiving the Benefit fostered feelings of appreciation and intrinsic recognition among our sample. Our findings also highlight the inadequacy of this amount relative to the extensive economic and social impacts of intensive caregiving. Since the Benefit has remained static since its introduction in 2009 underscores the political and fiscal context wherein family caregiving largely subsidizes the health care system at minimal personal cost to the government. Participant gratitude for the Benefit thus coexists with a recognition that the program provides a symbolic acknowledgement of caregiving labour rather than as a full compensation for the opportunity costs, lost income, and systemic vulnerabilities caregivers’ experience. This observation situates the Caregiver Benefit within the political economy of care, emphasizing both the reliance of health and social systems on family care and the need for more robust support policies for family caregivers. On the matter of the Benefit’s design, caregivers appreciated its self-directed nature as they were able to utilize funds in accordance with their own personal needs. This finding is consistent with current research evaluating the benefits of self-directed programs in support of caregivers (Milliken et al., Reference Milliken, Mahoney and Mahoney2020; Simon-Rusinowitz et al., Reference Simon-Rusinowitz, Mahoney, Loughlin and Sadler2005). Many caregivers in our study shared the financial toll of caregiving, including transportation expenses, pharmaceutical costs, and home care. Such out-of-pocket expenses are pervasive and commonly experienced by caregivers (Hastert et al., Reference Hastert, Kyko, Ruterbusch, Robinson, Kamen, Beebe-Dimmer, Nair, Thompson and Schwartz2024).
Findings of our study suggest that caregivers experience the program as both a symbolic recognition of the caregiving role and a formal mechanism to offset the financial toll of caregiving, with a more pronounced emphasis on the former. Participants often expressed appreciation for the Benefit as an indication that their caregiving work was acknowledged by the government; however, many caregivers emphasized that the fixed amount of $400 per month without adjustments for particular contexts of caregiving was insufficient to address the financial costs associated with caregiving. Such fiscal constraints and the consequent limited material impact of the Benefit have previously been studied (Mihailescu, Reference Mihailescu2021). Consequently, the Caregiver Benefit functions largely as a symbolic gesture of recognition accompanied by modest financial relief rather than as a comprehensive mechanism to address the economic impact of caregiving. This finding aligns with participant ideas that the current program could be strengthened through greater responsiveness to caregiving intensity, such as sliding scale payments to accommodate for different income brackets or specialized medical devices necessitated by the health condition of the care recipient. Clarification of the policy’s intent may also improve transparency and provide greater alignment between caregivers’ expectations and program design.
Pearlin’s stress process model for caregivers provides a useful framework for interpretation of our findings. Within this model, caregiving responsibilities described by participants constitute primary stressors, while the financial strain, employment disruption, and out-of-pocket costs identified reflect secondary stressors which are exacerbated over time. The Caregiver Benefit can be understood as a mediating resource within this process, intended to alleviate financial strain and reduce potential downstream effects on caregiver well-being. However, our findings indicate that while the Benefit offers symbolic recognition of caregivers and a modest form of financial relief, the fixed value restricts its potential to meaningfully disrupt the stress proliferation process. Importantly, our findings extend the application of the model through emphasizing the role of direct financial policy interventions as structural mediators within the caregiving stress process. Though the model has historically emphasized psychosocial resources (Pearlin et al., Reference Pearlin, Mullan, Semple and Skaff1990), our results suggest that the accessibility and adequacy of financial supports are critical determinants of caregiver outcomes. This highlights the importance of considering how policy interventions can be improved upon to more effectively target secondary stressors such as financial burden to alleviate cumulative disadvantage among caregivers.
Many participants expressed difficulties gaining information about the Caregiver Benefit and available supports due to bureaucratic gatekeeping and fragmentation of resources across different organizations. Current research has found that despite the push towards health systems reforms, caregiver programs continue to operate in silos and rely heavily on gatekeeping mechanisms to reduce expenditures (Funk, Reference Funk2019; Magnaye et al., Reference Magnaye, Fast, Eales, Stolow and Leslie2020; Parmar et al., Reference Parmar, Anderson, Abbasi, Ahmadinejad, Brémault-Phillips, Chan, Charles, Dobbs, Khera, Stickney-Lee and Tian2020). This finding is echoed in international caregiving research, highlighting the importance of streamlining support systems to enable policy proactivity and reduce administrative barriers (Berry et al., Reference Berry, Dalwadi and Jacobson2017; Pieper et al., Reference Pieper, Kasdorf, Voltz and Strupp2025; Strommen et al., Reference Strommen, Fuller, Sanders and Elliott2020). Integrated care models have been found to reduce navigational burden on caregivers and reduce system complexity (Kim et al., Reference Kim, Wister, O’dea, Mitchell, Li and Kadowaki2023; Sadler et al., Reference Sadler, Potterton, Anderson, Khadjesari, Sheehan, Butt, Sevdalis and Sandall2019). Caregivers favour centralized information repositories to access service information, a relatively inexpensive and feasible policy option to enhance support access and uptake (Funk, Reference Funk2019; Ogilvie et al., Reference Ogilvie and Eggleton2016). Restrictive eligibility criteria is a demonstrated barrier in the caregiving literature, alongside the time–cost burden borne by caregivers forced to navigate convoluted informational systems (Funk, Reference Funk2019; Funk et al., Reference Funk, Dansereau and Novek2017).
There was a strong aspiration across our sample to engage in collaboration with governmental agencies to amend the Caregiver Benefit and current support programs to better meet their needs, sharing ideas such as better integrated care systems and a sliding-scale payment model to respond to diverse circumstances. With regard to the latter, there is a newly established precedent for this model of program in Canada. Prince Edward Island developed a direct remuneration program (the At Home Caregiver Benefit) that operates on a sliding scale based on a care recipient’s annual income (Prince Edward Island, 2025). Participants in our study found that the information they required to access the Benefit and other programs existed as fragments across numerous sources, resulting in frustration and confusion regarding eligibility criteria. Evidence shows that a lack of inclusion of caregiver perspectives in program design causes service gaps in caregiver support (Schulz et al., Reference Schulz, Beach, Friedman, Martsolf, Rodakowski and James2017; Tracy et al., Reference Tracy, Nickell and Upshur2019). Minimal consultations with the target population of caregivers were conducted prior to the establishment of the Caregiver Benefit (Nova Scotia Legislature, 2010), thus restricting its ability to meaningfully reflect the needs of the population it aims to serve. Collaboration and co-design of support programs offer a way to validate caregiver experiences, promote community engagement, and verify program appropriateness to practical contexts (Parmar et al., Reference Parmar, L’Heureux, Lewanczuk, Lee, Charles, Sproule, Henderson, Chaudhuri, Berry, Shapkin, Powell, Nicholas, Tarnowski, Leslie, Lobchuk, Kaattari, Porter, Ewa, Podlosky and Anderson2025).
This study offers key insights into the current policy conversations regarding the development of caregiver remuneration programs. While prior research has examined the effectiveness of caregiver support programs such as the Canadian Compassionate Care Benefit (Williams et al., Reference Williams, Eby, Crooks, Stajduhar, Giesbrecht, Vuksan, Cohen, Brazil and Allan2011), these studies have primarily focused on program outcomes and labour market consequences rather than on the lived experiences of caregivers navigating policy supports (Flood et al., Reference Flood, DeJean, Doetter, Quesnel-Vallée and Schut2021; Mihailescu, Reference Mihailescu2021). Similarly, policy analyses of caregiver financial benefits have highlighted structural constraints such as limited payment amounts, restrictive eligibility criteria, and administrative complexity, yet they have not systematically explored how these policies are experienced by caregivers firsthand (Mihailescu, Reference Mihailescu2021). In contrast, our study contributes to the literature in three distinct ways. First, by centring caregiver narratives within Nova Scotia’s Caregiver Benefit, this research provides in-depth qualitative insights as to how caregivers interpret the meaning and utility of direct financial support, identifying dimensions that quantitative metrics alone do not capture. Second, our findings show how caregiving intensity and opportunity costs influence how benefits are perceived, revealing that financial supports are considered through both material and symbolic lenses. Third, this study highlights implementation gaps that are underexplored in existing evaluations of caregiver benefits by documenting firsthand policy navigation challenges to advance an understanding of how program design shapes real-world accessibility. To our knowledge, this research is the first to qualitatively explore firsthand perspectives of a direct financial support program for caregivers in a Canadian context. In doing so, we seek to fill a gap in the literature by providing rich insights into how financial supports are experienced, perceived, and navigated in current caregiving contexts.
Limitations
While this study sought to elicit the firsthand perspectives of Caregiver Benefit beneficiaries, this study does not claim to be representative of the entire population of caregivers in Nova Scotia. Foremost, participants were recruited through caregiver focused organizations (Caregivers Nova Scotia and the Alzheimer Society of Nove Scotia), which may have influenced the composition of the sample. Further, participants connected to these organizations may be more aware of available supports or have greater access to informational resources than caregivers who lack affiliation with such networks. Only English language speaking caregivers were included in the sample, thus potentially restricting the reflectiveness of these findings to caregivers of other cultures. Further, all participants with one exception identified a white, which may inadvertently mask or restrict the unique experiences of racialized caregivers. Given that our sample primarily revolved around the experiences of dementia caregivers, further research should be conducted to explore the different experiences of those providing care for other health conditions. It is possible that the perspectives of underrepresented groups of caregivers (e.g., young caregivers, rural-dwelling caregivers, or rare disease caregivers) are not adequately captured across this sample. Future research should examine the experiences of caregivers across diverse demographic and geographic contexts.
Conclusion
This study provides novel insights as to how intensive family caregivers (those providing greater than or equal to 20 hours of care per week) in Nova Scotia experience direct financial support through the Caregiver Benefit. While participants expressed appreciation for the program’s symbolic recognition and flexibility, they also identified significant barriers related to payment adequacy, systemic access obstacles, and a lack of tailored support mechanisms. Caregivers advocated for policy innovations including integrated care navigation, sliding-scale payments, and earlier intervention of supports in the caregiving trajectory to better meet subjective needs. As other jurisdictions consider adopting caregiver remuneration programs, our findings demonstrate the importance of caregiver-centred policy design to ensure that programs are reflective of practical caregiver needs. Future research should explore how direct financial support programs can be optimized to enhance caregiver capacity.


 Open access
Open access