


Diabetes is becoming an increasingly pressing issue worldwide. Reference Ong, Stafford, McLaughlin, Boyko, Vollset and Smith1 In 2021, there were an estimated 539 million (95% uncertainty interval 500–564 million) people living with diabetes across the globe, with a corresponding global age-standardised total diabetes prevalence of 6.1% (95% uncertainty interval 5.8–6.5). Reference Ong, Stafford, McLaughlin, Boyko, Vollset and Smith1 Around 11% of Indian people are diagnosed with diabetes, with a higher burden in urban compared with rural regions (16 v. 8%). Reference Anjana, Unnikrishnan, Deepa, Pradeepa, Tandon and Das2 With changes in lifestyle and food habits, this increasing prevalence of diabetes among Indian people shows no sign of slowing down. Reference Ranasinghe, Jayawardena, Gamage, Sivanandam and Misra3 Inadequate glycaemic control, adhering to the prescribed diet and lifestyle to manage diabetes, the risk of developing comorbidities and the financial burden of managing the condition affect the individual’s psychological well-being, leading to distress and affecting quality of life. Reference Jena, Kalra and Yeravdekar4 Although medical management in this group of people is well established, psychological support is inadequate, resulting in poor quality of life and generalised well-being. Reference Peyrot, Rubin, Lauritzen, Snoek, Matthews and Skovlund5
Psychological challenges in people with diabetes
Psychological challenges linked to diabetes include depression, anxiety, eating disorders, schizophrenia, affective disorders, Alzheimer’s disease and phobic reactions. Reference Nouwen, Winkley, Twisk, Lloyd, Peyrot and Ismail6–Reference Al Hayek, Robert, Babli, Almonea and Al Dawish11 The prevalence of depression has been reported to be 22% in type 1 and 19% in type 2 diabetes, and varied based on factors such as study setting, care type and economic status. Reference Farooqi, Gillies, Sathanapally, Abner, Seidu and Davies12 Generalised anxiety disorder had a prevalence rate of almost three times higher than that reported in general population, and about 12–40% of people with type 2 diabetes had an eating disorder. Reference Expert13,Reference García-Mayor and García-Soidán14 People with diabetes also have a higher incidence of cognitive decline and an increased risk of developing Alzheimer’s disease. Reference Akomolafe, Beiser, Meigs, Au, Green and Farrer15
Another challenge among people with diabetes is diabetes distress. The term diabetes distress refers to the emotional state in which individuals experience stress, guilt, or denial caused by the daily demands of living with diabetes. Reference Kreider16 It is different from clinical depression, but can have similar effects on a person’s mental well-being. People with severe diabetes distress had associated matching symptoms with mild depression based on Beck Depression Inventory scores. Reference Roy, Sengupta, Sahana, Das, Talukdar and Baidya17 Patients with diabetes distress avoid self-care tasks like taking medications, self-monitoring of blood glucose or attending medical appointments. Reference Abd El Kader, Ibrahim, Mohamed and Osman18 Diabetes distress can also manifest as unhealthy behaviour, elevated haemoglobin A1c and impaired relationships with healthcare professionals, partners, family or friends. Reference Peyrot, Rubin, Lauritzen, Snoek, Matthews and Skovlund5,Reference Fisher, Mullan, Arean, Glasgow, Hessler and Masharani19 Diabetes distress prevalence rates have been reported to range from 18 to 35% among people with diabetes globally. Reference Fisher, Skaff, Mullan, Arean, Mohr and Masharani20 Despite such a high burden, information on the prevalence and impact of diabetes distress among this subset of patients is minimal in many countries.
Diabetes distress and its prevalence in different populations in India
The pooled prevalence of diabetes distress in India was estimated at 33%. Reference Sinha, Priya, Sinha and Hifz Ur Rahman21 However, studies conducted in India have reported a wide prevalence of diabetes distress of between 8.45 and 61.48%. Reference Sinha, Priya, Sinha and Hifz Ur Rahman21 The prevalence of diabetes distress among patients with type 2 diabetes in one of the states of India (Haryana, population 25 million) was 38%. Reference Ranjan, Rajput, Sachdeva, Saha and Yadav22 A study from Chennai (population 7 million), the state capital of Tamil Nadu, India, reported the prevalence of diabetes distress to be 61.3%. Reference Natesan, Aravamuthan and Venkatraman23 However, there is relatively no data on the prevalence of diabetes distress among patients with type 2 diabetes from tier 2 cities in India (tier 2 cities are characterised by improving infrastructure, urbanisation, industrialisation and a growing middle class).
According to the Metabolic Non-communicable Disease Health Report of India – 2023, the state of Tamil Nadu in India (population: 72 million) had a 14.4% prevalence of diabetes, which is higher than the national average (11.4%). Reference Anjana, Unnikrishnan, Deepa, Pradeepa, Tandon and Das2 The recognition and understanding of diabetes distress by physicians in diabetes care is a crucial step toward endorsing support that is not simply prescriptive, but also person-centred and collaborative. Reference Peyrot, Rubin, Lauritzen, Snoek, Matthews and Skovlund5
The current study explores the burden of diabetes distress and the factors contributing to this condition among individuals living with diabetes attending a tertiary care hospital, in a tier 2 city in the state of Tamil Nadu.
Method
The study was conducted by following the Strengthening and Reporting of Observational Studies in Epidemiology (STROBE) guidance for cross-sectional studies (Supplementary File 1 available at https://doi.org/10.1192/bjo.2026.11020).
Survey tool
Diabetes distress was defined as a negative emotional state where people experience feelings such as stress, guilt or denial that arise from living with diabetes and the burden of self-management. Reference Peyrot, Rubin, Lauritzen, Snoek, Matthews and Skovlund5,Reference Kreider16 We selected the Diabetes Distress Scale 17 (DDS-17) to assess the distress levels in the participants. Reference Polonsky, Fisher, Earles, Dudl, Lees and Mullan24 The DDS-17 scale consists of 17 questions and is measured by a six-point Likert-style scoring. The DDS-17 scale measures four dimensions of distress, which are emotional burden, physician-related distress, regimen-related distress and diabetes-related interpersonal distress. The scoring ranges from 1 (never) to 6 (always) for each item (Supplementary File 2). A mean item score <2 is considered as no/low diabetes distress and a mean item score of ≥2 is considered as moderate-to-high diabetes distress. The scale was translated to Tamil (native language of Tamil Nadu) and validated (Supplementary File 3). The cut-off value for diabetes distress in the Tamil version is the same as of the original scale.
A structured questionnaire was prepared on the demographic and clinical profile, including age, gender, duration of diabetes, type of diabetes, education level, occupation, marital status, insurance coverage, type of medication intake, comorbidities (systemic hypertension, dyslipidaemia, hypothyroidism, coronary artery disease, stroke and chronic kidney disease) exercise, practising yoga, smoking and alcohol intake (as self-reported by the participants). Participants completed the questionnaire and DDS-17 scale.
Ethical considerations
The authors assert that all procedures contributing to this work comply with the ethical standards of the Kauvery Institutional Ethics Committee (registration number ECR/966/INST/TN2017/RR-21), which is in keeping with the Helsinki Declaration of 1975, as revised in 2013. Informed written consent was secured from all participants before enrolment in the study.
Study setting and population
Tamil Nadu is the tenth largest state in India with an area of 130 060 km2 and a population of 72.1 million. 25,26 Tiruchirappalli is a major tier 2 city in Tamil Nadu, with a estimate population of 1 239 000 in 2025. 25 The Kauvery hospital’s diabetic out-patient department caters to over 1 04 730 patients, and the diabetic diabetic out-patient department serves about 16 800 patients annually.
This prospective, observational study was conducted across a period of 3 months at the diabetic out-patient department of Kauvery Hospital, Tiruchirappalli, Tamil Nadu, India.
Inclusion and exclusion criteria
Inclusion criteria encompassed adults aged 18 years and above, diagnosed with type 1 or type 2 diabetes or gestational diabetes, and willingness to provide informed consent. Exclusion criteria included individuals with a diagnosis or a history of a major mental health disorder such as psychosis, bipolar disorder or major clinical depression or cognitive impairment (obtained by reviewing medical history) or taking psychiatric drugs, and those not willing to participate in the study.
Statistical analysis
Statistical analysis was performed using GraphPad PRISM software (version 11 for Windows; GraphPad, Boston, Massachusetts, USA; https://www.graphpad.com/features). Categorical variables were expressed as numbers (percentages) and continuous variables were expressed as mean ± s.d. Before applying parametric tests, data for continuous variables were tested for normality using the Shapiro–Wilk test. Variables following a normal distribution were analysed using parametric tests (Student’s t-test), whereas non-normally distributed variables, if any, were compared using Mann–Whitney U-test. Based on DDS-17 score, participants were classified into two groups: no diabetes distress group (DDS score <2) and diabetes distress group (DDS score ≥2). Differences in demographic and clinical parameters were observed between the groups. A correlation analysis was conducted to examine the relationship between the DDS-17 score and the demographic and clinical variables. Comparisons between the groups were conducted using chi-squared tests for categorical variables and t-tests for continuous variables. A P-value of <0.05 was considered statistically significant.
Results
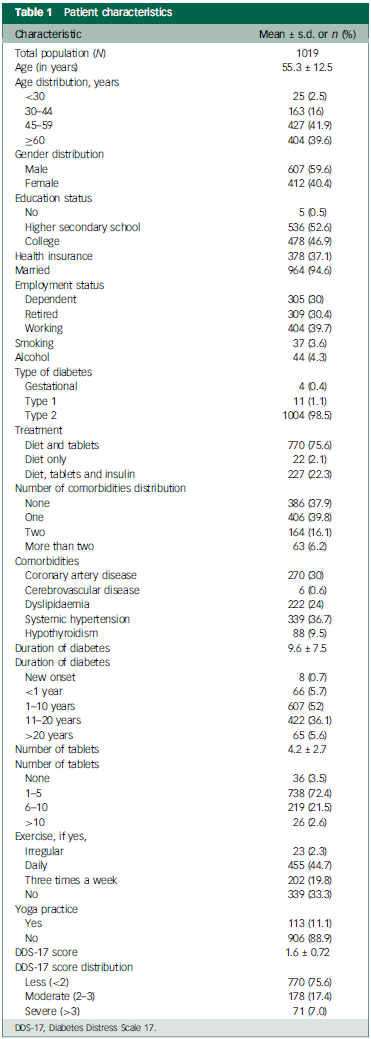
A total of 1250 consecutive patients were screened for the study, out of which 231 patients were excluded as they did not satisfy the inclusion criteria. The remaining 1019 patients were included in the study. Table 1 summarises the demographic characteristics and profile along with other comorbid health conditions.
Patient characteristics

DDS-17, Diabetes Distress Scale 17.
Of the included 1019 patients with diabetes, a predominant majority (98.5%, n = 1004) had type 2 diabetes. The average age of participants was 56 years (59.6% male, 40.4% female). Over four-fifths of respondents (81.5% n = 831) were over 45 years of age.
Three-quarters of the population were on lifestyle management and oral antidiabetic drugs (75.5%, n = 770), and just over a fifth of people were on insulin treatment (22.2%, n = 227). The remaining patients (n = 20) were on lifestyle management and not on any medication.
Nearly two-thirds of participants (62.2%, n = 633) had at least one or more comorbidities, with hypertension (30%, n = 270) and coronary artery disease (36.7%, n = 339) being the two most common. Just over half of the population were exercising or practising yoga daily or regularly (55.7%, n = 568).
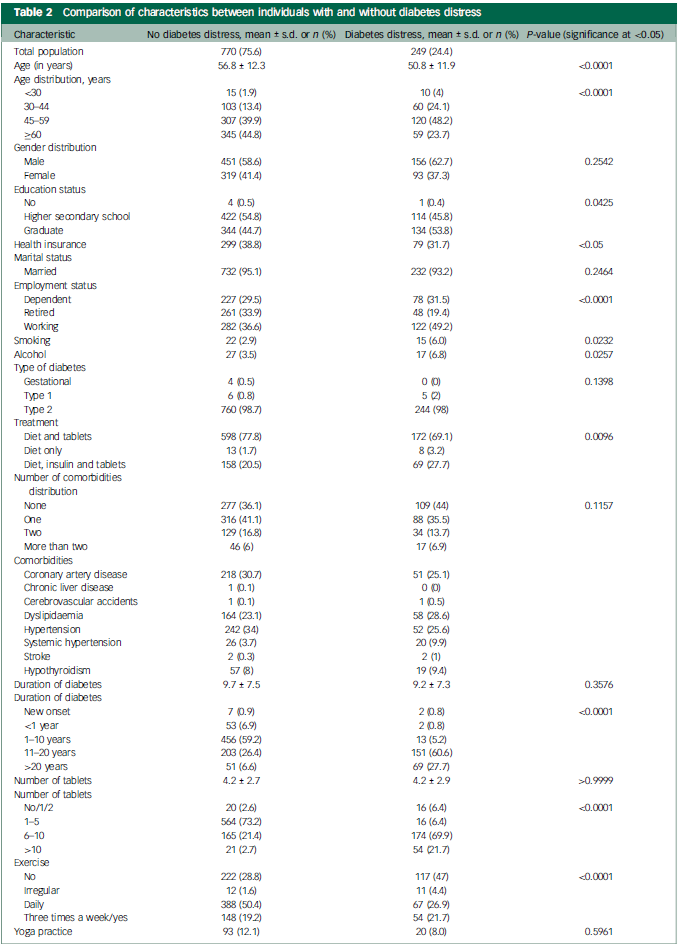
Nearly a quarter of all respondents reported diabetes distress (24.4%, n = 249). Table 2 provides details of comparison between those with and without diabetes distress. Individuals with diabetes distress were significantly more likely to be younger (<45 years of age) compared with the no diabetes distress group (28.1 v. 15.3%; P < 0.0001). The prevalence of smoking and alcohol consumption were significantly higher among those with diabetes distress (P < 0.05). Individuals with diabetes distress were significantly more likely to have long-standing diabetes (>10 years) compared with the no diabetes distress group (88 v. 33%; P < 0.0001). Individuals in the diabetes distress group were significantly less likely to exercise compared with the non-diabetes distress cohort (47 v. 28.8%; P < 0.001). In this study, the term exercise refers to any planned, structured and repetitive physical activity of at least 30 minutes a day. Participants who exercised were sorted into three groups based on their frequency: daily, three times a week and irregular/inconsistent (Table 1).
Comparison of characteristics between individuals with and without diabetes distress
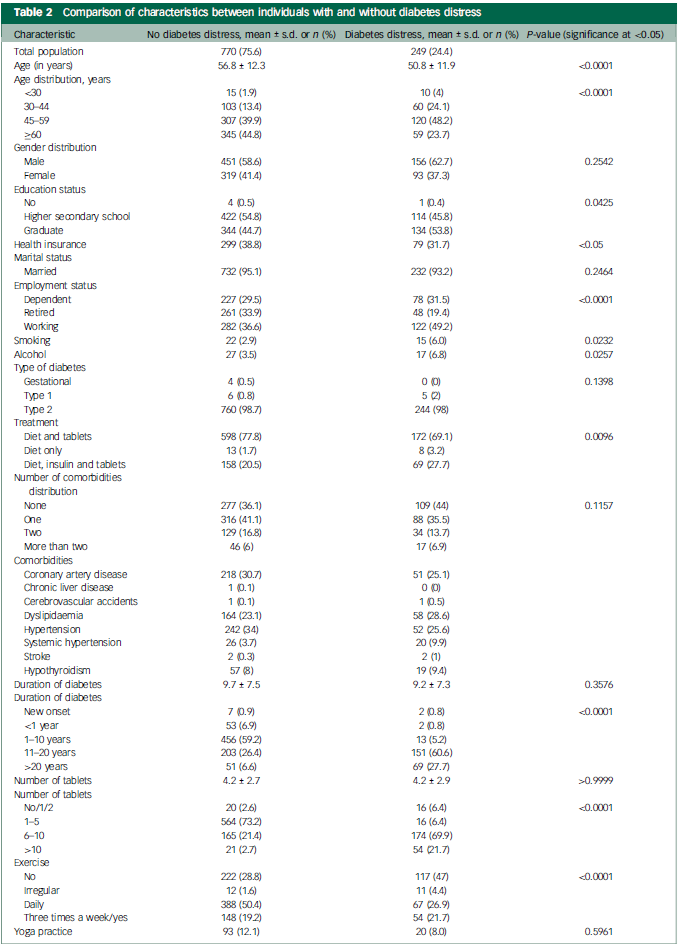
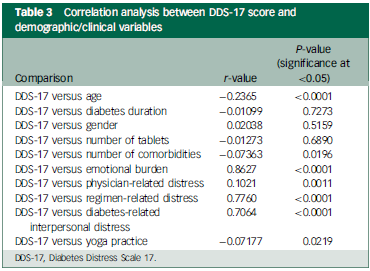
A negative correlation was identified between diabetes distress score on the DDS-17, age (r = −0.2365; P < 0.0001) and number of comorbidities (r = −0.07363; P = 0.0196) (Table 3).
Correlation analysis between DDS-17 score and demographic/clinical variables
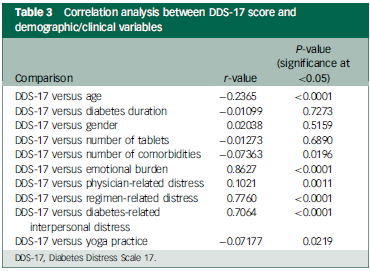
DDS-17, Diabetes Distress Scale 17.
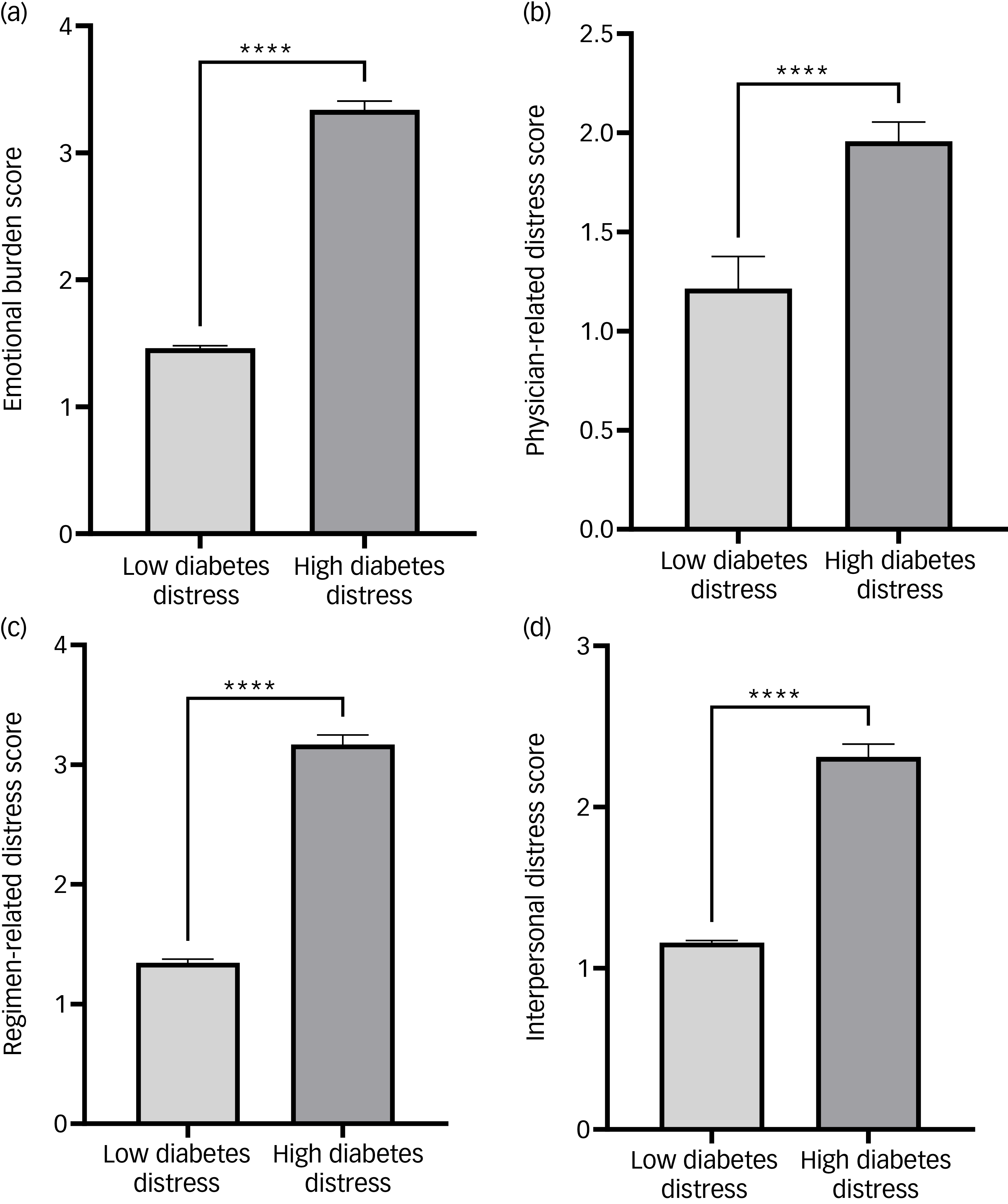
The subdomain scores of emotional burden, physician-related distress, regimen-related distress and diabetes-related interpersonal distress were all significantly higher among those with diabetes distress than those with no diabetes distress (Fig. 1). A significant positive correlation was observed between diabetes distress scores and domains of emotional burden (r = 0.8627; P < 0.0001), physician-related distress (r = 0.1021; P = 0.0011), regimen-related distress (r = 0.7760; P < 0.0001) and diabetes-related interpersonal distress (r = 0.7064; P < 0.0001) (Table 3).
Comparison of emotional burden, physician-related distress, regimen-related distress and diabetes-related interpersonal distress scores between patients with type 2 diabetes with and without diabetes distress, according to DDS-17 scores. DDS-17, Diabetes Distress Scale 17. ****P <0.0001.

Discussion
Our study highlights the high prevalence of psychological distress in the form of diabetes distress, and its associated factors, in middle-aged patients with type 2 diabetes in a tier 2 city in India. Our study observed the prevalence of diabetes distress in about a fourth of the study population compared with the 33% pooled prevalence of diabetes distress identified by a systematic review and meta-analysis pooled prevalence of diabetes distress of Indian patients with diabetes. Reference Sinha, Priya, Sinha and Hifz Ur Rahman21 It could be that the discrepancies in economic and health care resources across India play a role in the heterogeneity of prevalence findings. However, it still highlights the significant burden diabetes distress brings to people with diabetes in India. Addressing diabetes distress is critical for improving self-management and health outcomes among individuals with diabetes.
One finding of our study was that individuals with diabetes distress had long-standing diabetes. A study (N = 142) done in another region of India, using the same DDS-17 and study duration, showed a significant increase in the total diabetes distress scores and the subscores with increasing diabetes duration as seen in our study. Reference Sumana, Ruman, Beatrice Anne and Katkam27
Another aspect of our findings was that those with diabetes distress are relatively younger. Similarly, a study (N = 438) found nearly a quarter (24%) of individuals with young-onset diabetes reported high levels of diabetes distress, including emotional burden and regimen-related distress. Reference Trief, Uschner, Tung, Marcus, Rayas and MacLeish28 Young adults often grapple with feelings of being overwhelmed, anxious and defeated because of the constant demands of managing their condition. Factors contributing to this distress include regimen-related concerns, emotional burdens and interpersonal issues related to diabetes management. Reference Hagger, Lake, Singh, Hamblin and Rasmussen29,Reference Luzuriaga, Leite, Ahmed, Saab and Garg30 All of these were supportive of our findings in relation to the subdomains of the DDS-17. In addition, young individuals may struggle with dietary restrictions that interfere with social activities or career advancement opportunities, leading to feelings of isolation and frustration. Young adults are typically navigating significant life transition such as pursuing education or starting career while simultaneously managing a chronic condition. Reference Farooqi, Gillies, Sathanapally, Abner, Seidu and Davies12 Young adults experiencing diabetes distress often report higher haemoglobin A1c levels, indicating suboptimal blood glucose management and increased risk of comorbidities. Reference Sinha, Priya, Sinha and Hifz Ur Rahman21,Reference Trief, Uschner, Tung, Marcus, Rayas and MacLeish28,Reference Hagger, Lake, Singh, Hamblin and Rasmussen29
Patients on more complicated regimens often report feeling overwhelmed, which can lead to poor adherence to treatment protocols and ultimately worsen their glycaemic control. Reference Luzuriaga, Leite, Ahmed, Saab and Garg30 The analysis in our study revealed that individuals with diabetes distress had a higher number of medications compared with those with no or low diabetes distress. Studies have shown that emotional distress, including diabetes distress, is a significant predictor of medication adherence behaviour among patients with type 2 diabetes. Reference Hoogendoorn, Krause-Steinrauf, Uschner, Wen, Presley and Legowski31 Those experiencing high levels of distress are less likely to adhere to their prescribed medication regimens, which can result in a cycle of worsening health outcomes and increased medication needs. Reference Hoogendoorn, Krause-Steinrauf, Uschner, Wen, Presley and Legowski31,Reference Kretchy, Koduah, Ohene-Agyei, Boima and Appiah32
With urbanisation and industrial development, there has been an increase in sedentary lifestyle in India, especially given the growth of number of tier 2 cites. Reference Mohanty, Sahoo, Epari, Ganesh and Panigrahi33 A third of individuals with diabetes distress in our study reported that they did not exercise. Sedentary lifestyle is attributed to various health complications, including cardiovascular disease and risk for mortality. Individuals who sit for long periods without adequate physical activity face a 73% higher risk of early death compared with their more active counterparts. Reference Dai and Albrecht34 Therefore, engaging in regular physical activity not only helps mitigate these risks, but also contributes to improved mental health and overall well-being, reinforcing the importance of movement in daily routines.
Our study suggests that as diabetes distress increases, the emotional burden experienced by individuals also intensifies. This relationship underscores the psychological impact of diabetes management, where the demands of self-care can lead to heightened feelings of stress and anxiety. These correlations further illustrate how diabetes distress is intricately linked to the practical aspects of daily diabetes management, including treatment regimens and the overall impact on one’s life.
Limitations
Our study is a cross-sectional study, and thus has the limitations that such cross-sectional studies bring in principle, in that they focus on association and not causation. We cannot claim our sample to be representative of the diabetes population, as the participants belonged to a single centre. Therefore, the results may not be able to be applied to broader populations because of differences in demographic and social factors. This could be considered a convenience sample. Additionally, the absence of biochemical parameters to determine the extent of glycaemic and blood pressure control and lipid levels limits the understanding of the relationship between physiological health and diabetes distress. Additionally, by excluding individuals with a history of diagnosed mental health disorders and/or cognitive impairments, we cannot determine if some people in the excluded cohort had a higher psychological burden of diabetes distress and who may be at higher risk of diabetes distress by virtue of their pre-existing mental health and/or cognitive problems.
Future implications
Our study suggests that younger individuals are more likely to experience diabetes distress. This subset of people should be regularly screened and appropriately treated for reducing the psychological burden and to promote generalised well-being. We suggest large-scale interventional studies to further clarify the risk factors associated with diabetes distress.
In summary, our study is a relatively large-scale study of >1000 participants selected continuously (subject to inclusion criteria being met), highlighting, for the first time, the association of psychological distress with diabetes in a tier 2 city hosting an emergent middle-class urban population. The high burden of diabetes distress highlighted in our study underscores the critical need for a holistic approach to diabetes management. There is a need to recognise the emotional and psychological challenges faced by individuals with diabetes by healthcare providers, and develop comprehensive care strategies that address both physical and mental health. This integrated approach may improve clinical outcomes and foster a supportive environment that prioritises the overall well-being of individuals with diabetes. Ultimately, these strategies can lead to enhanced quality of life and better adherence to diabetes management plans, paving the way for more effective and compassionate care.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjo.2026.11020
Data availability
The data that support the findings of this study are available from the corresponding author, R.S., upon reasonable request.
Author contributions
All authors satisfy the International Committee of Medical Journal Editors guidance by substantially contributing to the design, analysis and interpretation of the work, drafting of the manuscript, final approval of the manuscript and all agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work is appropriately investigated and resolved. G.P.: conceptualisation, formal analysis, investigation, methodology, project administration, validation, visualisation, writing – original draft, writing – review and editing. L.S.N.: conceptualisation, formal analysis, investigation, methodology, project administration, validation, visualisation, writing – review and editing. S.R.K.: conceptualisation, formal analysis, funding acquisition, investigation, methodology, project administration, validation, visualisation, writing – review and editing. A.S.: project administration, validation, visualisation, writing – review and editing. K.A.G.: investigation, project administration, writing – original draft, writing – review and editing. D.T.: investigation, project administration, validation, visualisation, writing – review and editing. S.T.: project administration, validation, visualisation, writing – review and editing. R.S.: conceptualisation, formal analysis, investigation, methodology, project administration, validation, visualisation, writing – review and editing.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Declaration of interest
S.J.T. and R.S. are members of the BJPsych Open Editorial Board. They did not take part in the review or decision-making process of this paper. R.S. has received institutional and research support from LivaNova, Union Chimique Belge, Eisai, Veriton Pharma, Neuraxpharm, Bial, Angelini, UnEEG and Jazz Pharma outside the submitted work. He holds grants from National Institute for Health and Care Research, Small Business Research Initiative and other funding bodies all outside this work. No other author has any declared conflict of interest related to this paper.



 Open access
Open access
eLetters
No eLetters have been published for this article.