


Medical education is fundamental to healthcare, shaping clinical competence and the quality of patient care. In the UK, it is delivered through a complex framework involving the General Medical Council (GMC), NHS England, Royal Colleges, universities and NHS trusts. Reference Patel1 Mental health trusts are uniquely positioned to offer valuable psychiatric training, but face challenges such as limited resources, recruitment issues and persistent stigma around mental illness. Reference Best2
Despite the growing emphasis on quality improvement in training, evidence suggests that psychiatric education often lags behind other specialties in perceived value and structure. Reference Menon, Winston and Sullivan3,Reference Vassilas and Berrisford4 For example, inconsistencies in induction processes, limited access to psychotherapy supervision and variable teaching quality have all been reported as factors contributing to residents’ dissatisfaction. Reference Carson and Clark5–Reference Shanley, Jones and Reddi7 There is also a duty to provide appropriate induction for international medical graduates (IMGs) and to orient them to the NHS and postgraduate medical education in the UK. 8 The COVID-19 pandemic accelerated the shift to online and hybrid teaching, raising concerns about learner engagement, peer support and equitable access. Simultaneously, curricula must now incorporate non-clinical skills including leadership, medico-legal knowledge and digital literacy. 9
This study explores the experiences of medical students and psychiatry residents within a large London mental health trust. Through qualitative focus groups, it identifies key challenges and suggests improvements, contributing to ongoing efforts to enhance psychiatric education and align it more closely with learners’ real-world needs.
Method
Focus group methodology was selected as an appropriate approach to explore the experiences of medical students and residents. The focus group format enabled a deeper understanding of participants’ experiences, capturing the nuances and emotional significance of the issues discussed. The study involved four separate focus groups categorised by the participants’ level of training: medical students, foundation year doctors, core psychiatry residents (CPRs) and higher-specialty residents (HSRs). Participants were recruited through an internal mass email distributed to all medical students and residents within the trust, inviting them to join the study.
All focus groups were conducted online via Microsoft Teams, with the exception of the group of doctors in their first year after medical school (foundation doctors), which took place in person. Each session was facilitated by a single moderator from the same training grade; however, the foundation doctors group was facilitated by a senior resident due to limited facilitator availability. A standardised topic guide (see Box 1) was used across all sessions to maintain consistency and support structured discussion. Each participant was given sufficient time to respond following the open discussion, which helped prevent any single individual from dominating and allowed balanced input before moving to the next topic. Prior to the start of each session, participants’ verbal consent for their participation in the focus group, and for the use of their data in subsequent publications, was formally obtained and recorded. Anonymity was ensured. Formal ethical approval was not required, because the project was conducted as part of a quality improvement initiative to support the development of an educational strategy for the trust.
Topic guide
-
(a) Current challenges in medical education within our trust: let’s discuss the issues and challenges currently experienced in the delivery of medical education or training within our trust.
-
(b) Enhancing the quality of medical education: how can we improve and elevate the quality of medical education? Let’s explore strategies and opportunities for enhancement.
-
(c) Ideas for future medical education delivery: what innovative and forward-thinking ideas do you have for the future of medical education delivery within our trust? Please share your insights.
(Prompts to use for each question: onboarding, training, resources, getting support)
In the data analysis, a meticulous and methodologically sound approach was adopted to ensure both the replicability and validity of the findings. Although all focus groups were audio-recorded for accuracy, one group was documented via written detailed notes because one participant opted out of audio-recording. The analysis followed a thematic approach, informed by Braun and Clarke’s thematic analysis, while incorporating some mechanical organising techniques for practical convenience. The data-set was first read repeatedly to develop strong familiarity. Coding involved identification of meaningful segments of text, supported by colour-coding for visual grouping of related ideas. A scissors-and-sort method was used as an additional organisational aid, allowing extracts with shared features to be collated to support deeper reflection on patterns within the data. These organisational tools were used solely to manage the material efficiently; theme development itself was interpretive rather than mechanical. Candidate themes were then reviewed, refined and clearly defined to ensure that they represented coherent patterns of meaning across the data-set.
Results
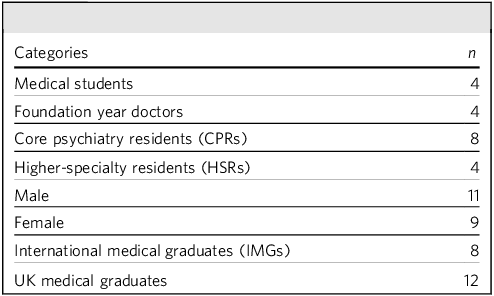
A total of 20 participants were included in the study (Table 1). The sample demonstrated a broadly representative distribution with respect to gender, country of primary medical qualification and level of training. The themes identified from all the focus groups included induction, accessible information, rota issues, facilities, psychotherapy and other training requirements, clinical and non-clinical teachings and supervision and support.
Participant information

Induction
An induction to the role is a structured programme designed to introduce new personnel to their work environment, the policies and procedures of the NHS and the specific duties of their roles. The medical students found the induction beneficial but too lengthy, taking almost an entire week; they felt that this extended duration significantly reduced their clinical time. It was suggested that some parts of the induction could be offered beforehand as pre-recorded sessions, allowing students to watch them at their convenience:
‘I think the induction was well organised, but the kind of the first week felt like a little bit of a write-off. So basically, I just don’t think it should be dragged out that whole week.’ (Medical student 1)
Foundation doctors and CPRs had no concerns regarding the quantity or quality of their induction, which usually lasts for 3 days in the trust. However, foundation doctors suggested that a broader orientation covering different services, therapy options and referral pathways within the trust would be beneficial. Although CPRs and HSRs typically have experience with several inductions before starting their current post, this may be the first induction for foundation doctors. As a result, the latter need clearer orientation on how services operate within the NHS, particularly within mental health trusts:
‘I think the induction was quite good actually.’ (Foundation year doctor 4)
HSRs felt that their induction was appropriate. However, IMGs found their induction inadequate, expressing a need for more shadowing experiences and specific training sessions. They particularly noted the difficulty of handling on-calls immediately after starting. Adjusting to an unfamiliar healthcare system can be demanding for IMGs, and this transition can significantly affect their confidence and performance:
‘I’m an IMG, so when I arrive to this country, I didn’t get much understanding and I wasn’t explained while it was a complete mess for at least last first four months.
I didn’t know even a single thing about system, so I was just sitting. Ideally, I don’t know anything, so it was very difficult for me to get into the system.’ (HSR2)
Accessible information
All groups emphasised the importance of having written guidance, policies and protocols available in various areas; these documents should be easily accessible and up to date.
Residents, in particular, highlighted the need for information on local guidance, booking leave and claiming study budgets. Foundation group doctors, who are rotated every 4 months, found written information on local guidelines and referral pathways to be especially helpful. CPRs expressed the need for written guidance outlining teaching hours and educational opportunities as part of their training. Given the intensity of their training and the frequency of transitions, it is unrealistic to expect doctors to retain everything from induction alone. Having accessible written guidance provides a reliable reference point when they need clarity or support:
‘You don’t feel very well supported. You don’t. I don’t know who to contact for anything.’ (Foundation year doctor 2)
‘We need a comprehensive information pack for trainees including all the information.’ (HSR4)
Rota issues
Participants shared their experiences and suggestions regarding placement, rotation and on-calls. Medical students felt that the current placement allocation results in significant disparities in gaining clinical experience and knowledge. They emphasised the importance of designing placements to ensure exposure to both wards and community services. The specialist visits, where students independently chose to attend a preferred service on a designated day, were identified as a positive aspect of the placement experience. However, they noted that the psychiatric placement experience did not match the learning opportunities of other specialties:
‘Again, I understand that’s a challenge of a placement and having the resources to allocate students all these things, but I think. Seeing a memory clinic for four or five weeks probably isn’t the best use of four or five weeks.’ (Medical student 2)
‘… specialist visit, I thought they were real positive to the placement’. (Medical student 3)
Foundation year doctors expressed a preference for exposure to different settings rather than remaining in a single job for the entire rotation, because this approach does not provide a comprehensive insight into psychiatry and its services. In the trust, foundation doctors are not required to do on-calls, which was seen as a positive aspect. Although this was viewed positively, it does come with reduced learning opportunities and a financial impact:
‘So, whether it’s some time spent around seeing other things as well. You know, we know the medical side of things, but there’s it’s quite difficult to get to grips with the breadth of community services and sort of non-pharmacological intervention in psychiatry.’ (Foundation year doctor 3)
CPRs voiced concerns about rota gaps, increased workload and last-minute notices to cover different sites. They suggested improvements such as including foundation group doctors in the rota, redesigning the rota and considering alternative staffing solutions, including external locums or adjusted locum pay arrangements:
‘Across all on-call types, significant rota gaps exist. Trainees face challenges with being informed at the last minute about the need to transfer to a different site due to rota gaps.’ (CPR1)
Rota gaps for duty doctors also negatively affect HSRs, who often have to step down, resulting in lost training opportunities.
Physical facilities
Participants emphasised the importance of adequate facilities in enhancing their learning and training experience. Medical students reported issues with access, because they did not have access cards to enter certain buildings, making them feel restricted and isolated. Participants noted the lack of a dedicated space for students for resting and having lunch, which they felt was essential for their well-being during long shifts:
‘I think it would be nice somewhere else to actually eat lunch, because I went in there once as well with my lunch to try and heat up. I couldn’t warm my lunch up anywhere as well because there was no common room to do it.’ (Medical student 2)
Residents echoed these concerns, highlighting the absence of a dedicated physical space for medical education. This lack of space hinders the organisation of teaching sessions, mock examinations, simulations and other educational events, thereby impacting the quality of their training:
‘There is no doctors’ mess on site or dedicated space for medical education.’ (HSR2)
Additionally, there were also issues with the local taxi service contract, which often caused significant delays when travelling to different sites. To address this, residents proposed using the ride-hailing service via the trust account to facilitate faster and more reliable transport:
‘You have to wait sometimes for one hour, so I thought it’s… but normal thing in the trust and it takes long time for taxi to come so. Yeah, it is actually waste of time, especially when you have three or four MHA assessments at night.’ (HSR3)
Psychotherapy competency requirements
Medical students and foundation group doctors do not have psychotherapy training requirements. Psychiatry residents expressed significant anxiety about achieving the necessary competencies in psychotherapy. They noted a lack of clear guidance and a standardised approach within the trust, making it challenging to meet these requirements in a timely manner:
‘Lack of psychotherapy supervision groups, leading to trainees needing to extend their training.’ (CPR3)
Residents highlighted the need for more supervision groups and a broader scope for long cases to help them fulfil their competencies effectively. The provision of additional support and structured guidance would alleviate worry and ensure that residents can achieve their psychotherapy competencies as required:
‘There is a problem with the psychotherapy training. We don’t get enough psychotherapy training. There is not [sic] enough trainers or supervisors for psychotherapy cases, especially for HSRs.’ (HSR3)
Training requirements
Obtaining the required workplace-based assessments (WPBAs) is a concern across all groups. Participants noted that securing direct supervision for these assessments is not always possible. Foundation group doctors felt that WPBAs could be made more meaningful and aligned with the quality observed in other specialties. High service pressures further limit opportunities for supervisors to observe clinical encounters and provide timely, constructive feedback, ultimately affecting the educational value of these assessments:
‘It would be good to have a quality and meaningful WPBA.’ (Foundation year doctor 3)
CPRs found it challenging to achieve their portfolio competencies, suggesting that protected self-development time, similar to that provided for foundation years, would be beneficial. Additionally, residents expressed the need to use academic programme time for self-development when no sessions are scheduled, which would help them meet their training requirements more effectively. They have an added requirement to complete Membership of the Royal College of Psychiatrists (MRCPsych) examinations that further intensified the strain, leaving them feeling short on time and stretched across competing demands:
‘Difficulty in completing numerous portfolio and training requirements during regular working hours due to the demands of the daily workload.’ (CPR6)
Clinical teaching
Medical students felt that some sessions were too long and difficult to focus on, especially when conducted via Microsoft Teams with the camera and microphone off. They missed the bedside teaching aspect of psychiatry and proposed more simulation training with individual feedback. They emphasised that all teaching should align with the curriculum and focus on core skills. They preferred more small-group teachings and called for greater consistency and effectiveness in clinical problem-based learning sessions. Sessions involving people with lived experience were highly valued by the students. All the groups expressed a desire for advanced teaching incorporating artificial intelligence and virtual reality technologies:
‘They had like good content. But I think they just ran on for too long. It’s quite hard. It’s quite hard to engage you, especially when you’re just listening for the three hours, you just have to turn your mics and cameras off and just listen.’ (Medical student 1)
Foundation group doctors felt that the psychiatric teaching available to them was not sufficiently tailored to their stage of training. They expressed a strong interest in attending the local psychiatric academic programme alongside their mandatory foundation teaching:
‘General sort of teaching and learning. I think I would say it’s probably one of the best rotations I’ve been on the terms of that.’ (Foundation year doctor 4)
CPRs were concerned about the inconsistency of protected teaching time, and expressed general dissatisfaction with MRCPsych examination preparation teaching. They called strongly for a restructured programme with more practical, simulated and interactive sessions:
‘Inconsistencies across their teams in having protected time in order to attend the academic programme, which has affected ability to attend, even remotely.’ (CPR5)
HSRs preferred having a refresher course on relevant physical health and medical emergencies tailored for their level. They highly valued the registrar teaching day and preferred these events to be held face to face:
‘It would be good to have sessions with patients sharing their lived experiences, providing valuable insights for trainees.’ (HSR1)
Clinical teachings often reflect a clinician-centred perspective and do not fully convey the patient’s journey through the system. Opportunities to hear directly from patients about their perspective can be meaningful.
Our newer ways of working have reduced in-person contact with colleagues, making them appreciate the social and professional connection provided by in-person sessions. For these reasons, they may favour face-to-face teaching.
Non-clinical skills development
Residents’ groups emphasised the importance of having opportunities for audit and quality improvement projects, noting that there needs to be more support and promotion from the trust for these activities.
CPRs highlighted the necessity of training for writing tribunal reports, attending tribunals, giving witness testimony in coroner’s court, understanding the Mental Health Act assessments and handling the responsibilities of a registrar on call:
‘Include teaching sessions covering practical skills, transitioning to SPR [skills for psychological recovery] training and improving proficiency in various computer/IT applications and offer teaching sessions focusing on soft skills like team management.’ (CPR8)
HSRs felt that the trust should do more to prepare them for consultant roles through both formal and informal training, indicating this as a neglected area of their training. Providing these opportunities would ensure that residents are well equipped with essential non-clinical skills, preparing them comprehensively for their future roles.
The current programme provides limited attention to non-clinical skill development, leaving residents concerned about their readiness for future roles. They expressed a clear need for targeted training to support their transition into senior clinician positions.
Supervision and support
All groups expressed concerns about the inconsistency of supervision. Although some consultants provide protected supervision time, others do not, leading to a variable experience across the board. Supervision is essential for residents, providing a containing space where their concerns, uncertainties and developmental needs can be understood and addressed.
Residents felt that their skills and contributions are not sufficiently valued, particularly when compared with other specialties, where resident doctors have more autonomy in their practice:
‘Sometimes feel a bit like, you know, we’re not allowed to make any decisions, which is quite different from other jobs.’ (Foundation year doctor 2)
There was a strong call from residents for the trust to more proactively promote doctors’ well-being and provide additional support. They suggested the implementation of a mentorship or buddy scheme to support everyone, with IMGs feeling especially desperate for such support. HSRs indicated that having peer groups for higher-specialty residents would be beneficial:
‘Mentorship, it’s an informal type of mentoring, and we find it more comfortable. Yeah, it’s more comfortable for a newcomer.’ (HSR2)
Participants also highlighted the importance of appreciating doctors’ work and fostering a culture that values rotational doctors. They suggested the establishment of an annual doctors’ day to give awards and showcase their work. Additionally, providing certificates of participation or appreciation for volunteer roles or extra work was recommended. It was emphasised that team members should take every opportunity to thank and recognise each other’s efforts:
‘So, I was just going to say that that my previous Trust uh, we used to have a Trainees conference like within the trust.’ (HSR3)
Furthermore, participants suggested organising more social and face-to-face events to enhance connection and foster a sense of belonging among the team. This approach would help build a supportive and appreciative working environment, improving overall morale and job satisfaction.
There was a general sense of not feeling valued or appreciated. This can be partly linked to the rotational nature of training, which limits the time available to build relationships and develop a sense of belonging.
Discussion
The current study explores the experiences of psychiatry residents from a medical education perspective. It provides valuable insights into the experiences of psychiatry residents and medical students during their psychiatric placements, and outlines key areas for improvement in the quality of medical education delivery by mental health trusts.
Induction to a new role is crucial for patient safety and employee satisfaction. However, the study reveals that NHS inductions are often uninspiring and perceived as mere tick-box exercises. Reference McMenamin, Blencowe and Roland10 Neither online nor classroom inductions were generally well received by residents. Effective socialisation was identified as critical, and the provision of all necessary information for residents, Reference Goodall, Boyle and MacKenzie11 including training and support details, is essential. In our study, participants were generally satisfied with the induction process. However, they highlighted a clear need for substantial improvement in induction for IMGs. National reviews have already recognised that inadequate induction contributes to challenges for IMGs, who are disproportionately referred to the GMC. Reference Wise12 Consequently, both the NHS and GMC now provide standardised professional practice induction to better prepare IMGs for their roles. 13
In our study, core psychiatry residents expressed particular concern about rota gaps. Previous research has identified rota gaps and inadequate facilities as significant issues. Reference Clarke14,Reference Forsythe and Suttie15 Rota gaps not only increase workload and stress but also reduce training opportunities and can impact patient care. Brexit, coupled with the exodus of doctors, has further exacerbated the shortage of doctors and intensified staffing gaps in medical rotas. Reference Milner, Nielsen and Verdery16 NHS restrictions on external locums have added further pressure on resident doctors, contributing to overall dissatisfaction. Reference Allen, Ashcroft, Ferguson, Grigoroglou, Kontopantelis and Stringer17 Similarly, adequate rest facilities are important for both students and residents because these are linked to staff recruitment and retention. 18 In our study, participants raised concerns about the adequacy of these facilities, highlighting their impact on well-being and overall training experience.
Achieving psychotherapy competency is a significant challenge for psychiatry residents. They face difficulties in finding cases due to dropouts and other in-session issues. Similar challenges have been reported in other studies, such that of Carson and Clark, indicating a broader systemic problem. Reference Carson and Clark5,Reference Shanley, Jones and Reddi7 In our study, residents described significant worry about meeting psychotherapy requirements, driven by limited guidance, difficulty accessing cases and inconsistent supervision. Baban et al reported the same pattern in a London-wide qualitative study; despite these barriers, residents consistently described psychotherapy training as one of the most enriching components of their education, helping re-humanise psychiatric practice and deepen their engagement with patients. Reference Baban, Hillen, Story, Burn and Curtis19 Residents and students also noted that WPBAs could be improved in terms of accessibility and effectiveness, rather than being seen as a tick-box exercise, and reflecting a broader issue within medical training. Reference Menon, Winston and Sullivan3 The Assessment Strategy Review by RCPsych highlights significant inconsistencies in the quality of WPBAs. Although these play a vital role in assessing day-to-day behaviours, communication, patient-centred care and teamwork, many supervisors struggle to deliver high-quality assessments due to time pressures. As a result, feedback often becomes a tick-box exercise rather than specific, constructive guidance. Reference Dave20
The shift to online teaching post-pandemic has posed challenges, Reference Mian and Khan21 despite its efficiency. In our study, medical students found it difficult to concentrate and engage with virtual teaching, and residents miss the opportunity to interact with their peers and develop a sense of colleagueship. Reference McMenamin, Blencowe and Roland10 In-person teaching helps foster socialisation and a sense of belonging. Spencer reports that small-group teaching and constructive feedback were highly valued by medical students, but consultant supervision and teaching time were limited due to increased workloads. Reference Spencer22
In the current study, core psychiatry residents appreciate specific teaching for their MRCPsych examinations, Reference Vassilas and Berrisford4 although there is a need for continuous feedback and improvement. There is a growing demand for non-clinical skills training, Reference Husnain and Hussain23,Reference Higgins, Gallen and Whiteman24 such as leadership, medico-legal knowledge and ‘soft’ skills. Higher-specialty residents feel that more should be done to prepare them for consultant roles, because current training is heavily focused on clinical skills with insufficient emphasis on leadership and management. Residents also see potential in using advanced technology such as artificial intelligence and virtual reality simulation in psychiatric teaching, which some NHS trusts are already implementing to prepare residents for on-calls. Reference Mudunkotuwe, Henry, Clift and Strickland25 Digital psychiatry is rapidly becoming a core part of modern practice, and its adoption is essentially unavoidable. Future psychiatrists need to be prepared not only to use these tools, but to critically understand their safety, ethical implications and real-world limitations. 26
In our study, medical students and foundation residents generally found psychiatry to be a pleasant and supportive environment. However, there is a need to foster a culture that values resident doctors more. The rotational nature of training can disadvantage residents in various ways, Reference Best2 and supervision was found to be inconsistent. Consultant interest in residents greatly influences their satisfaction. Reference Spencer22,Reference Varvari, Debell, Harrison and Ranjith27 Varvari et al report that residents internalise their supervisors’ behaviours, using these as templates for their own future consultant practice and leadership, and therefore supervisors should be conscious role models. Reference Varvari, Debell, Harrison and Ranjith27 There is a call from our participants for more structured mentorship and buddying systems. Social events, awards and recognition can help residents feel valued and appreciated. With increasing evidence of burnout and stress among doctors and medical students, there is a pressing need for enhanced support for well-being and mental health. Reference Clark6
The concerns highlighted in our study are not new. Similar issues have been recognised across multiple specialties and NHS trusts, indicating that the challenges we identify are part of a wider systemic problem rather than one confined to a single organisation. The recent Medical Training Review: Phase 1 Diagnostic Report, Reference Powis28 by Professors Whitty and Powis, reflects this national picture, outlining many of the same themes. The report describes supervision quality as highly variable, effectively a ‘postcode lottery’, and emphasises how service pressures undermine clinical training, supervision and teaching. It also draws attention to variations in departmental culture and the limited support available to resident doctors. Crucially, the reviewers conclude that incremental adjustments will not address these entrenched issues; instead, a fundamental redesign of medical training is required. They advocate for more stable team structures to enable consistent supervision, mentorship, continuity and support, and call for training models that embed core generalist skills, digital capability and leadership development.
Overall, this study highlights key areas for improving psychiatric training, including better induction, accessible information and rota gap solutions. Enhancing facilities, structured support for psychotherapy competencies and clinical and non-clinical training are essential. These improvements will enrich the learning environment and elevate the quality of psychiatric education for medical students and residents within the mental health trust.
Strengths and limitations
This study examines psychiatric residents’ and medical students’ experiences from a medical education perspective. Using qualitative focus groups, it captures detailed participant perspectives, providing valuable insights into their experiences and challenges. The inclusion of diverse resident groups ensures a broad understanding of issues across training stages, but we had only limited numbers in the groups of medical students, foundation doctors and higher-specialty residents. The study has several limitations. It did not include GP residents on psychiatric rotations or examine psychiatry subspecialties, which may involve different training experiences. Because the study was conducted within a single trust, its findings may not generalise to other trusts or regions of the UK. Focus groups also carry inherent constraints: participants may feel hesitant to share negative experiences, and discussions can be shaped disproportionately by more dominant voices despite efforts to ensure balanced participation. Finally, the participants may not reflect the wider workforce, because only a limited number took part despite invitations being extended to all residents and students. Those who chose to participate may represent individuals particularly motivated to share their views, and their experiences or preferences may differ from those who did not take part.
This study highlights key areas for improvement in psychiatric training in the UK, including better induction, accessible information and rota gap solutions. Enhancing facilities, structured support for psychotherapy competencies and clinical and non-clinical training are essential. These improvements will enrich the learning environment and elevate the quality of psychiatric education for medical students and residents within the mental health trust.
About the authors
Bruce Tamilson is a consultant neuropsychiatrist based at St George’s Hospital, London, UK and South West London and St George’s Mental Health NHS Trust, London, UK. He also holds academic roles as an honorary senior clinical lecturer at St George’s, University of London, London, UK and as a senior lecturer at University College London, London, UK. Michelle Keag is a higher trainee in psychiatry at South West London and St George’s Mental Health NHS Trust, London, UK, with a particular interest in medical education. This project was undertaken as part of the Royal College of Psychiatrists (RCPsych) Leadership and Management Fellowship Programme (2023–2024).
Data availability
The materials supporting this study’s findings are not publicly available due to privacy constraints; however, de-identified materials can be shared upon request to the corresponding author.
Author contributions
Both authors contributed to all stages of the project, including study design, data collection, analysis and manuscript preparation.
Funding
This project received no external funding.
Declaration of interest
None.

 Open access
Open access
eLetters
No eLetters have been published for this article.