


Highlights
-
• Ultra-early microdiscectomy (≤12 h) accelerates early neurological recovery and shortens hospital stay.
-
• Surgery within 48 h remains the critical threshold for favorable long-term outcomes in acute lumbar disc herniation with deficits.
-
• No increase in complications or recurrence with ultra-early versus later (≤48 h) surgery.
Introduction
Lumbar disc herniation is a common cause of surgical referral, particularly when neurological deficits such as motor weakness or features of cauda equina syndrome (CES) are present. Reference Rosner, Glynn and Lee1 While many cases of radiculopathy improve with conservative treatment, substantial or progressive motor impairment and bowel/bladder dysfunction warrant prompt decompression to limit irreversible deficits. Reference Rosner, Glynn and Lee1
The optimal timing of decompression remains debated. Guidelines endorse “early” surgery for CES and motor deficits, yet “early” spans 6–48 h across studies. Some reports suggest advantages to ultra-early intervention (≤12 h), whereas others find comparable outcomes across the ≤48 h window; real-world logistics may also constrain ultra-early access. Reference Paternostro-Sluga, Grim-Stieger and Posch2,Reference Sabnis and Diwan3
High-quality comparative data within the first 48 h are limited, and the interaction between pre-hospital symptom duration and in-hospital surgical delay is poorly characterized across outcomes such as motor recovery, pain, complications and length of stay (LOS). Reference Ramakonar and Fehlings4,Reference Lavy, Marks, Dangas and Todd5
Hence, we analyzed a large retrospective cohort undergoing emergency microdiscectomy for acute disc herniation with motor weakness and/or CES, comparing outcomes among ≤12 h, 12–24 h, 24–48 h and >48 h from presentation. We further assessed whether symptom duration before presentation modifies timing–outcome relationships.
Methods
We conducted a single-center retrospective cohort study of adults (≥18 y) undergoing emergency lumbar microdiscectomy (2015–2025). Inclusion required MRI-confirmed lumbar disc herniation with significant compression on corresponding nerve roots or cauda equina that is causing motor weakness and/or CES. Exclusions were prior surgery at the same level, multilevel discectomy or incomplete records. Patients were grouped by time from presentation to incision: ≤12 h, >12–≤24 h, >24–≤48 h and >48 h. Symptom duration was recorded as the number of days from the onset of weakness or cauda equina symptoms to presentation, with a full cohort range of 0–62 days. For analytic purposes and consistent with prior literature and the observed cohort distribution, we categorized duration as ≤2 days, 3–5 days and ≥6 days, with the latter representing cases of chronic/subacute presentation.
Surgical indication and MRC grading
During the study period, surgery was indicated for CES, rapidly progressive motor deficits or moderate-to-severe weakness (typically Medical Research Council [MRC] ≤3/5) causing functional limitation. Patients with isolated, nonprogressive MRC 4/5 weakness were generally managed conservatively or by elective microdiscectomy unless deterioration occurred or disabling functional impact was evident. Motor strength for major myotomes (dorsiflexion, plantarflexion, EHL, knee/hip flexion–extension) was graded on the MRC scale at presentation and follow-up.
Clinical data were extracted from electronic medical records, including age, sex, duration of symptoms prior to presentation, level of disc herniation and neurological findings at presentation. Primary outcome measures included postoperative motor improvement, assessed using the MRC scale, and subjective pain resolution. Secondary outcomes included the presence of urinary/fecal incontinence at presentation, length of hospital stay (LOS), postoperative complications (such as dural tears, wound infections, hematomas and discitis), recurrent emergency department (ED) visits and recurrent disc herniation confirmed by MRI. Follow-up neurological assessments were conducted immediately postoperatively, at 2 weeks and at 3 months.
Descriptive and inferential statistics were used in the analysis of the collected data. Continuous variables were summarized as means with standard deviations, while categorical variables were presented as frequencies and percentages. The Kruskal–Wallis test was employed to compare differences in continuous variables across the different time of surgery categories. For categorical variables, Chi-square and Fisher’s exact tests were used to assess associations between time of surgery and other categorical variables. To analyze changes in muscle power (assessed using the MRC scale) over four time points (at presentation, 1 day after surgery, 2 weeks after surgery and 3 months after surgery), the Friedman test was used for overall differences, followed by Wilcoxon Signed-Rank tests for post hoc pairwise comparisons when significant. To evaluate factors associated with recurrent disc herniation, recurrent ED visits and weakness improvement after surgery, logistic regression analysis was conducted, with results reported as odds ratios with 95% confidence intervals and p-values. The Hosmer–Lemeshow test was used to assess model fit, and collinearity was examined to ensure model stability. The significance of the results was measured using a p-value of <0.001. All statistical analyses were carried out in R software version 4.4.2 (Vienna).
Results
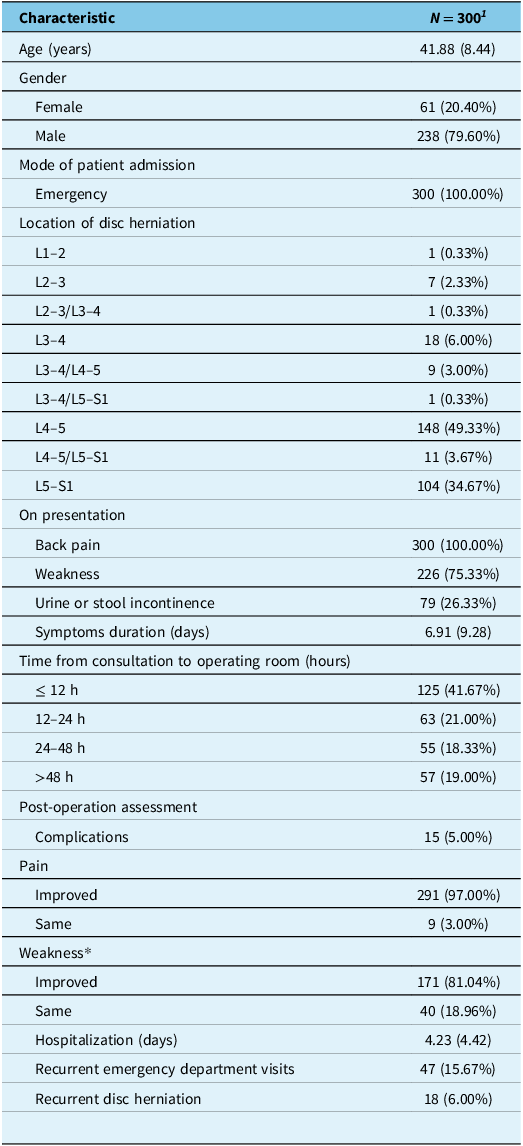
We included 300 patients (mean age 41.9 y; 79.6% male). Levels were mainly L4–5 (49.3%) and L5–S1 (34.7%) (Table 1). At presentation, 75.3% had motor weakness, and 26.3% had urinary/fecal incontinence. Mean symptom duration before presentation was 6.9 days. Surgical timing groups were ≤12 h (41.7%), 12–24 h (21.0%), 24–48 h (18.3%) and >48 h (19.0%).
Baseline characteristics, presentation and outcomes of patients undergoing microdiscectomy for acute disc herniation. P-values reflect comparisons across all four timing groups (≤12 h, 12–24 h, 24–48 h, >48 h) unless otherwise specified. Post hoc pairwise comparisons are shown where appropriate

1 Mean (SD); n (%).
*Missing data.
Delays beyond 48 h were most often due to prolonged symptom history or chronic presentation (41.1%) and patient-related factors such as reluctance or delayed consent (21.4%). Other contributors included absence of neurological deficits at presentation (14.3%), medical clearance requirements (7.1%), lack of documentation (5.4%), additional investigations (5.4%), conservative management attempts (3.6%) and operating room unavailability (1.8%).
Preoperative neurological status
A total of 11 patients presented with complete paralysis (MRC 0/5) in at least one myotome; 8 (72.7%) underwent ultra-early decompression (≤12 h), and the remainder were treated within 24–48 h. Early postoperative flicker (MRC 1) developed in five patients, but only two patients (18.1%) achieved meaningful recovery (≥MRC 3) by 3 months, consistent with the limited reversibility of complete paralysis even when decompressed rapidly. In keeping with this pattern of more severe neurological injury, patients treated ≤12 h also more frequently presented with incontinence (46.3%) and plantarflexion weakness (59.2%), while other myotome deficits were similar across groups.
Muscle strength recovery over time
Motor strength improved significantly in patients treated ≤12 h, with rapid early gains in plantarflexion and dorsiflexion and more gradual recovery in other myotomes (Table 2, Figure 1A–F).
Box plot showing muscle power improvement over time for patients who underwent surgery within 12 h: Friedman test results. (A) hip flexion, (B) extensor hallucis longus, (C) plantarflexion, (D) dorsiflexion, (E) knee flexion, (F) knee extension.

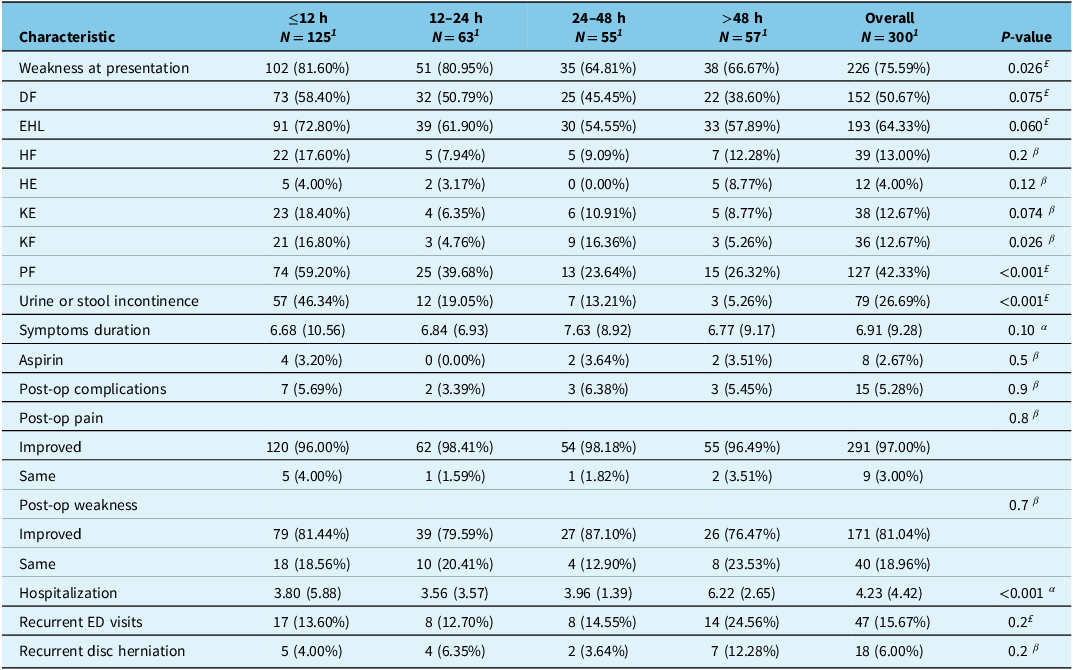
Comparison of patient characteristics and outcomes based on time to surgery. P-values reflect comparisons across all four timing groups (≤12 h, 12–24 h, 24–48 h, >48 h) unless otherwise specified. Post hoc pairwise comparisons are shown where appropriate

DF = dorsiflexion; ED = emergency department; EHL = extensor hallucis longus; HF = hip flexion; HE = hip extension; KE = knee extension; KF = knee flexion; PF = plantarflexion.
1 Mean (SD); n (%), α Kruskal–Wallis rank sum test, £ Pearson’s Chi-squared test, β Fisher’s exact test.
Motor recovery stratified by symptom duration
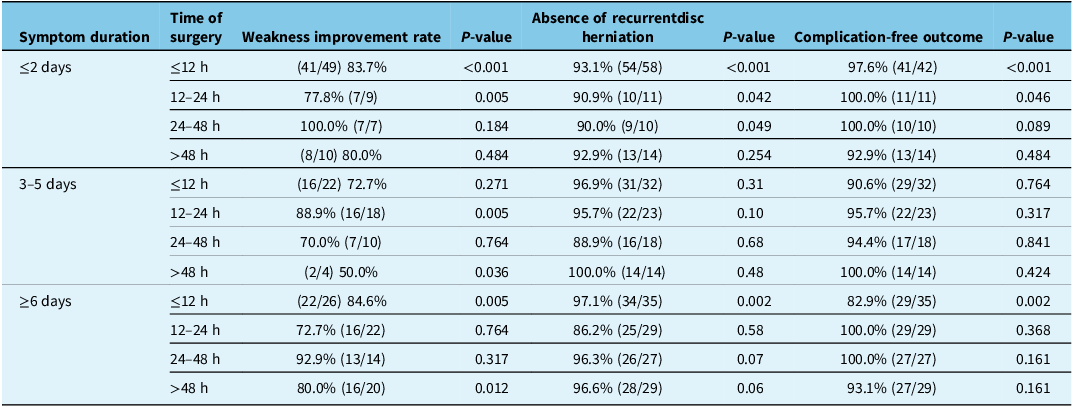
Symptom duration markedly modified postoperative outcomes. Patients with ≤2-day symptoms derived the greatest benefit from ultra-early decompression (≤12 h), showing the highest rates of motor improvement, pain resolution and continence recovery. Those with 3–5 days of symptoms performed similarly across all ≤48 h surgical intervals, suggesting a broader therapeutic window. In contrast, patients with ≥6-day (chronic) symptoms exhibited substantially lower rates of early motor recovery, reflecting longer-standing deficits at baseline; although ≤12 h decompression produced some early gains, overall recovery in this subgroup was less reliable, and modestly delayed surgery occasionally showed fewer complications. These findings illustrate distinct timing–duration interactions and underscore symptom duration as a major modifier of surgical timing effects (full range 0–62 days; subgroup outcomes summarized in Table 3).
Post hoc analysis of post-operation outcomes by symptom duration and time from ER admission to surgery. P-values reflect comparisons across all four timing groups (≤12 h, 12–24 h, 24–48 h, >48 h) unless otherwise specified. Post hoc pairwise comparisons are shown where appropriate

Hospitalization
LOS followed a consistent pattern across all symptom-duration strata: patients operated ≤12 h had the shortest stays (mean 3.6 days), while those treated >48 h had significantly longer hospitalization (mean 6.1 days). These patterns persisted after stratifying by symptom duration.
Recurrent herniation, complications and secondary outcomes
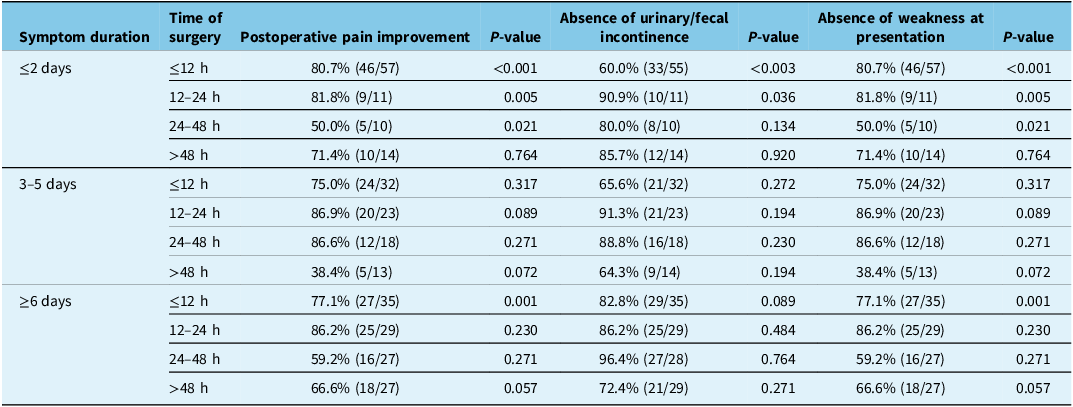
Table 4 summarizes the secondary functional outcomes – pain improvement, continence preservation and weakness resolution – and shows that the interaction between symptom duration and surgical timing extends across these domains. Pain improvement was highest with ≤12 h surgery among acutely presenting patients, whereas continence outcomes were most sensitive to early timing only in the ≤2-day group. Recurrent herniation (6%) and overall complication rates were similar across timing categories; however, acute patients treated ≤12 h experienced fewer recurrences, while chronic patients undergoing ultra-early surgery occasionally demonstrated slightly higher complication rates. These patterns indicate that symptom duration continues to modify the benefits of early decompression, with ultra-early surgery favoring acute presentations but sometimes yielding comparable or better outcomes with moderate delays in chronic cases.
Post hoc analysis of postoperative pain improvement, continence preservation and weakness at presentation by symptom duration and time from ER admission to surgery. Chi-square test, number of improved/total cases in that cell. Postoperative pain improvement, continence preservation and weakness resolution stratified by symptom duration and surgical timing. This table illustrates how symptom duration modifies the effect of surgical timing on functional outcomes. P-values reflect comparisons across all four timing groups (≤12 h, 12–24 h, 24–48 h, >48 h) unless otherwise specified. Post hoc pairwise comparisons are shown where appropriate

Logistic regression
Multivariable analysis showed that gender, but not surgical timing, predicted recurrence and ED visits: males had lower odds of both outcomes. Neither timing nor symptom duration independently predicted motor recovery (Table 5).
Logistic regression analysis of factors associated with post-operation outcomes. P-values reflect comparisons across all four timing groups (≤12 h, 12–24 h, 24–48 h, >48 h) unless otherwise specified. Post hoc pairwise comparisons are shown where appropriate

Discussion
Key findings
Ultra-early surgery (≤12 h) was associated with faster early motor recovery and shorter hospital stay. However, long-term motor outcomes were comparable across the ≤48 h window. These findings indicate that the main clinical breakpoint remains within 48 h, with ultra-early decompression offering primarily an acceleration of recovery rather than superior long-term outcomes.
Comparison with prior literature
Our results confirm earlier evidence that delays beyond 48 h are consistently linked to worse functional outcomes and longer hospitalizations. Reference Ahn, Ahn, Buchowski, Garrett, Sieber and Kostuik6–Reference Hogan, Kuris, Durand, Eltorai and Daniels10 While prior studies generally assessed 24–48 h thresholds, our analysis provides additional granularity, suggesting that ultra-early surgery may accelerate neurological recovery in acute cases. Importantly, all patients in our cohort had MRI-confirmed compression, ensuring that decompression was clinically warranted.
Prior reports, including Reference Jerwood and Todd11,Reference DeLong, Polissar and Neradilek12 , showed improved bladder outcomes with earlier surgery but did not stratify motor recovery within narrower windows. Our data extend this by showing that plantarflexion and dorsiflexion strength improved most rapidly when decompression occurred ≤12 h, although long-term recovery rates converged across the ≤48 h groups. This observation is consistent with trends noted in Reference Todd13,Reference Thakur, Storey and Kalakoti14 , as well as Kögl et al. (2021), Reference Kögl, Brawanski, Girod, Petr and Thomé15 which supported early decompression but did not explicitly examine ultra-early intervals.
Among patients presenting with bowel dysfunction, only a minority recovered even when decompressed within 12 h. This finding mirrors prior literature, where bowel symptoms are consistently the least likely to improve after surgery. Reference Jerwood and Todd11,Reference Siccoli, Staartjes, de Wispelaere and Schröder16
Influence of symptom duration
A major contribution of this study is the joint analysis of pre-hospital symptom duration and surgical delay. Patients with ≤2-day symptoms showed the most consistent early motor gains and shortest hospital stays with ultra-early decompression, while those with 3–5-day symptoms achieved similarly favorable outcomes as long as surgery occurred within 48 h. In contrast, patients presenting with ≥6-day (chronic) symptoms demonstrated less predictable improvement irrespective of timing; in this subgroup, ultra-early surgery was not uniformly advantageous, and modest delays occasionally yielded fewer complications and better continence outcomes. These findings likely reflect the impact of prolonged neural compression and potential irreversible changes, aligning with evidence that recovery potential diminishes as symptom duration increases. Notably, our 3-month follow-up may partially underestimate later recovery in the ≥6-day group, as delayed improvement trajectories have been reported in subacute and chronic deficits.
Pain and complications
Pain improvement was high overall (97%), consistent with earlier literature. Reference Albert, Lange, Brawanski and Schebesch17,Reference Siccoli, de Wispelaere, Schröder and Staartjes18 Acute patients operated on ≤12 h had slightly lower pain improvement, a finding that may reflect transient postoperative irritation. Complication rates were low (5%) overall and not significantly influenced by timing. However, in patients with chronic symptoms, ultra-early surgery was sometimes associated with slightly higher complication rates, underscoring the need for careful patient selection in this subgroup.
Predictors of outcomes
Logistic regression showed that gender, but not timing, was significantly associated with recurrence and ED revisits, with females having higher odds. While the cause is unclear, biomechanical differences, disc properties or activity patterns may contribute and merit further investigation. Reference Saeed, Mukherjee, Chaudhuri, Kerry, Ahuja and Pal19 Neither age, surgical delay, nor symptom duration independently predicted long-term motor outcomes. This supports the interpretation that ultra-early surgery primarily accelerates neurological recovery and discharge, rather than altering durable functional results. Nevertheless, some patients did not improve despite ultra-early surgery, likely reflecting irreversible deficits at presentation in cases of established CES. Reference Woodfield, Hoeritzauer and Jamjoom20,Reference Surjanovic and Loughin21
Before vs. after 48 h
When dichotomized at 48 h, outcomes clearly diverged: patients treated later had longer hospitalizations and more recurrent ED visits, while those treated ≤48 h – regardless of exact timing – had similar motor and pain recovery. Thus, while ≤12 h may expedite recovery in selected acute cases, the strongest evidence continues to support the ≤48 h threshold as the critical determinant of neurological outcomes. This reinforces prior meta-analyses and cohort studies highlighting the importance of maintaining the 48-h surgical window for optimal results. Reference Ahn, Ahn, Buchowski, Garrett, Sieber and Kostuik6,Reference Kohles, Kohles, Karp, Erlich and Polissar7,Reference Hogan, Kuris, Durand, Eltorai and Daniels10,Reference Kögl, Brawanski, Girod, Petr and Thomé15,Reference Costa, Oertel, Zileli, Restelli, Zygourakis and Sharif22
Clinical implications and MRC clarification
Our findings support current recommendations for early decompression in CES and significant motor weakness. Reference Costa, Oertel, Zileli, Restelli, Zygourakis and Sharif22 Importantly, we clarify that our results should not be generalized to all patients with minimal weakness (stable MRC 4/5). In our practice, surgery was indicated for CES, rapidly progressive deficits or moderate-to-severe weakness (MRC ≤3/5). Conservative management remains appropriate for mild, nonprogressive deficits, which can improve without surgery. This distinction is crucial to prevent overextension of surgical indications.
Limitations and future directions
This study is limited by its retrospective, single-center design, which introduces potential selection bias and restricts generalizability. Symptom onset was based on clinical documentation and may be imprecise, and treatment decisions were influenced by surgeon judgment, operating room availability and patient factors, creating potential unmeasured confounding. Although a stringent p-value threshold was applied, this may have reduced sensitivity to smaller effects. Additionally, the 3-month follow-up interval may underestimate later neurological recovery, particularly in patients with longer preoperative symptom duration; prior studies indicate that patients with deficits lasting more than 1 week may continue improving for 6–12 months, which could partly account for the lower recovery rates observed in the ≥6-day subgroup.
Future multicenter, prospective studies are needed to validate the ≤12 h window, explore cost-effectiveness and stratify outcomes by symptom duration and severity. Biomarker studies may also help guide individualized surgical timing. Reference Ramakonar and Fehlings4
Conclusion
For acute lumbar disc herniation with neurological deficits, surgery within 48 h remains the central benchmark for favorable outcomes. Ultra-early intervention (≤12 h) can accelerate early neurological recovery and reduce LOS in selected acute presentations, but long-term motor outcomes appear similar across other ≤48 h windows. These data support prioritizing early access, while reserving ultra-early activation for patients with CES, rapid progression or more-than-mild motor deficits. Prospective, multicenter studies should validate timing strategies stratified by symptom duration and deficit severity.
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank all colleagues who contributed to discussions that improved this work.
Author contributions
AI, OS and AM conceptualized the study and designed the methodology. AI, OS, SE, MH, FA, NS, AB, AT and AEM contributed to data collection and patient follow-up. AI and OS performed data analysis and interpretation. AI drafted the manuscript. SB supervised the study, provided critical revisions and approved the final version. All authors reviewed and approved the final manuscript.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Competing interests
The authors declare that they have no conflicts of interest relevant to this work.
Ethical standard
This study was approved by the Medical Research Committee at Hamad Medical Corporation and was conducted in accordance with the Declaration of Helsinki. Informed consent was waived for retrospective analysis.
Consent for publication
Not applicable.



 Open access
Open access