


Sexual violence is a serious and pervasive form of harm, with profound consequences for those affected. It is consistently linked to increased risk for, and severity of, a wide range of mental disorders. Reference Dworkin, Menon, Bystrynski and Allen1 Mental health service users report disproportionately high rates of sexual violence victimisation. Reference Kaul, Connell-Jones, Paphitis and Oram2,Reference Khalifeh, Oram, Osborn, Howard and Johnson3 Whereas there is growing recognition of these impacts, less attention has been paid to how mental health services may themselves be sites of risk.
Sexual violence has, however, been documented in mental healthcare settings. In one study, more than one in ten psychiatric in-patients engaged in some type of sexual behaviour during the first 2 weeks of admission, with indecent exposure and non-consensual sexual touching most frequently reported. Reference Bowers, Ross, Cutting and Stewart4 An analysis of incident reports on UK National Health Service (NHS) Trust mental health wards by the Care Quality Commission found that more than a third of reported sexual incidents involved sexual assault or harassment, with most occurring in communal areas and the majority of perpetrators being male and victims female. 5 Investigations by Rape Crisis England & Wales have highlighted further safeguarding failures and serious failures in psychiatric in-patient settings, echoing the concerns raised in the earlier Care Quality Commission report. 6
Despite growing documentation of sexual violence within psychiatric in-patient settings, far less is known about how patients themselves experience these incidents. Psychiatric in-patient settings should be places of safety, providing therapeutic care for people in acute mental distress. Reference Thompsell, Pratap, Lovelock, Clement, Haydon and King7,Reference McGarry8 However, for some patients these settings are unsafe or even harmful. Reference Jones, Nolan, Bowers, Simpson, Whittington and Hackney9 Safety is not only about protection from physical violence but also encompasses emotional, psychological and relational dimensions. Reference Stenhouse10 When patients witness sexual violence, it can create a pervasive sense of fear and vulnerability; when they are directly subjected to it, the experience may be deeply traumatising, violating both personal and institutional boundaries. Such incidents can shatter trust in staff, fellow patients and the therapeutic function of the in-patient environment itself. Institutional failure to prevent or respond adequately to such incidents can represent a profound breach of trust – what has been termed institutional betrayal – and may compound trauma, reduce patients’ motivation to engage in treatment or follow therapeutic guidance and hinder recovery. Reference Lewis, Lee, Zabelski and Shields11 Understanding the lived experience of sexual violence in these settings is critical to improving practice and restoring safety.
Findings from a qualitative synthesis further highlight the risk of re-traumatisation for patients with prior lived experiences of sexual violence during in-patient stay, which may have a detrimental impact on their existing mental health condition and recovery. Reference Hennessy, Hunter and Grealish12
This systematic review aimed to synthesise qualitative evidence on how patients experience and understand sexual violence – whether directly experienced or witnessed – during psychiatric in-patient stays. It also examined patients’ perceptions of institutional responses to sexual violence within this setting.
Method
Protocol and registration
This systematic review follows Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines, Reference Page, McKenzie, Bossuyt, Boutron, Hoffmann and Mulrow13 and was prospectively registered with PROSPERO (no. CRD42024595945).
Databases and search strategy
We searched MEDLINE, Embase and PsycINFO via Ovid from their respective start dates to 14 October 2024. The search strategy used combinations of text-word terms and Medical Subject Headings terms for sexual violence (e.g. sexual harassment, unwanted or inappropriate touching, indecent exposure, image-based sexual abuse, sexual assault, rape and professional sexual misconduct) and psychiatric in-patient settings (e.g. psychiatric hospital, secure or locked mental health units, forensic psychiatry and psychiatric intensive care unit). The complete search strategy is provided in Supplementary Table 1. Additionally, for the included studies, J.B. and Y.D. conducted reference list screening and forward citation tracking using Web of Science and Google Scholar.
Eligibility criteria
Studies were eligible for inclusion if they: (a) used qualitative study designs (e.g. in-depth or semi-structured interviews, focus group discussions); (b) described patients’ experiences of sexual violence, witnessing sexual violence or managing the risk of sexual violence within psychiatric in-patient settings, as described directly by patients; and (c) were published as peer-reviewed studies in English, French or Chinese. Studies were excluded if they: (a) used quantitative or mixed-method designs without extractable qualitative data; (b) were case studies, case file reviews or reports based on Freedom of Information Act requests (or non-UK equivalents); (c) were published in non-peer-reviewed formats (e.g. theses, dissertations, reports or conference abstracts); (d) did not report on patient experiences of sexual violence, witnessing sexual violence or managing risk of sexual violence within psychiatric in-patient settings; (e) reported on patient experiences second-hand (e.g. from staff rather than from patients directly); (f) included reports on patient experiences from settings other than psychiatric in-patient settings, or from mixed settings without separate analysis; and (g) included samples in which more than 25% of participants were under the age of 18 years.
Study selection
J.B. and Y.D. screened titles and abstracts against the inclusion criteria, independently dual-screening a random 20% of records with >90% agreement. The remaining records were split for screening, followed by dual-independent, full-text screening. Discrepancies were resolved through discussion or, if needed, consultation with senior author S.O.
Quality appraisal
Study quality was appraised using the widely used Critical Appraisal Skills Programme (CASP) qualitative studies checklist. 14 J.B. and Y.D. independently assessed all included studies using the CASP checklist, and any discrepancies were resolved through discussion and consensus.
Data extraction
Data were extracted into MS Excel for Windows (2019; Microsoft Corporation, Redmond, WA, USA) by Y.D., including bibliographic information, geographical information, study design, analytical methods, sample characteristics, settings, type of ward (mixed- or single-gender) and relevant participant quotes (treated as primary constructs), and also author interpretations of these quotes (treated as secondary constructs).
Data synthesis
Data were synthesised using interpretative meta-synthesis, drawing on the principles of thematic synthesis. Reference Thomas and Harden15 This approach involved interpretation of primary constructs across studies to generate new theoretical insights that moved beyond the findings of individual studies, to develop a more in-depth, comprehensive understanding of how patients experience sexual violence and safety within psychiatric in-patient settings. This method was chosen for its transparency and systematic nature, as well as its capacity to produce findings that are both analytically rigorous and relevant to informing clinical practice and policy.
The synthesis process was conducted by Y.D., and proceeded through six key stages: (a) primary constructs underwent line-by-line coding using open, descriptive codes; (b) codes were grouped into conceptual categories to identify patterns across the data; (c) interpretative categories were developed into candidate themes to the research questions; (d) themes were refined and defined through reviewing and checking to ensure that each was coherent, distinct and supported by primary constructs; (e) themes were contextualised by identifying variations and contradictions both across studies and within individual studies (e.g. conflicting accounts within the same data-set); and (f) final themes were synthesised into a coherent narrative that connects the findings to relevant theoretical frameworks and the broader literature. Codes, categories and themes were discussed, refined and reorganised by S.O. Contradictions and discrepancies – both intra- and inter-study – were identified and interrogated.
Results
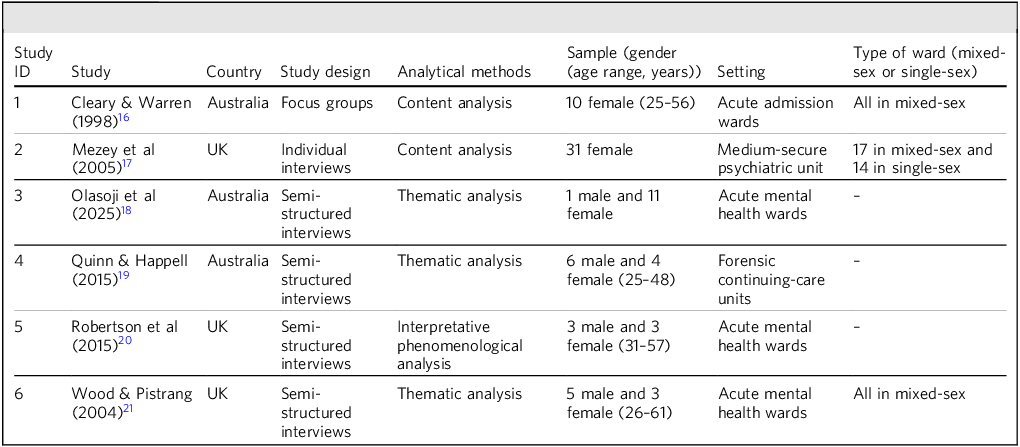
The complete study selection process is shown in Fig. 1. The reasons for the exclusion of each study reviewed at the full-text stage are shown in Supplementary Table 2. Six studies describing 78 participants were included in this review, with 63 identified as female (80.8%) and 15 as male (19.2%). Studies dated from 1998 to 2025. The characteristics of individual studies are described in Table 1.
Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flowchart.

Study characteristics

Themes, subthemes and studies

Across all six studies, accounts of sexual violence and safety concerns in psychiatric in-patient settings were provided, largely by female patients. A broad spectrum of harmful experiences was described: verbal harassment and sexualised abuse; Reference Cleary and Warren16,Reference Robertson, Pote, Byrne and Frasquilho20,Reference Wood and Pistrang21 sexual coercion and intimidation; near-sexual coercion, intimidation and exploitation; Reference Cleary and Warren16,Reference Mezey, Hassell and Bartlett17,Reference Quinn and Happell19–Reference Wood and Pistrang21 near-miss sexual assaults Reference Cleary and Warren16,Reference Mezey, Hassell and Bartlett17 ; and sexualised physical violence. Reference Mezey, Hassell and Bartlett17
All six studies were determined to be broadly methodologically sound. One study Reference Quinn and Happell19 met all ten CASP criteria; two studies Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18,Reference Robertson, Pote, Byrne and Frasquilho20 met nine out of the ten criteria and three Reference Cleary and Warren16,Reference Mezey, Hassell and Bartlett17,Reference Wood and Pistrang21 met eight out of the ten criteria. None but the highest-ranking study were judged to have adequately considered relationships between participants and researchers, and ethical issues were not judged to have been fully taken into account in three studies. Reference Cleary and Warren16,Reference Mezey, Hassell and Bartlett17,Reference Wood and Pistrang21 Full-quality appraisal details are provided in Supplementary Table 3.
Themes
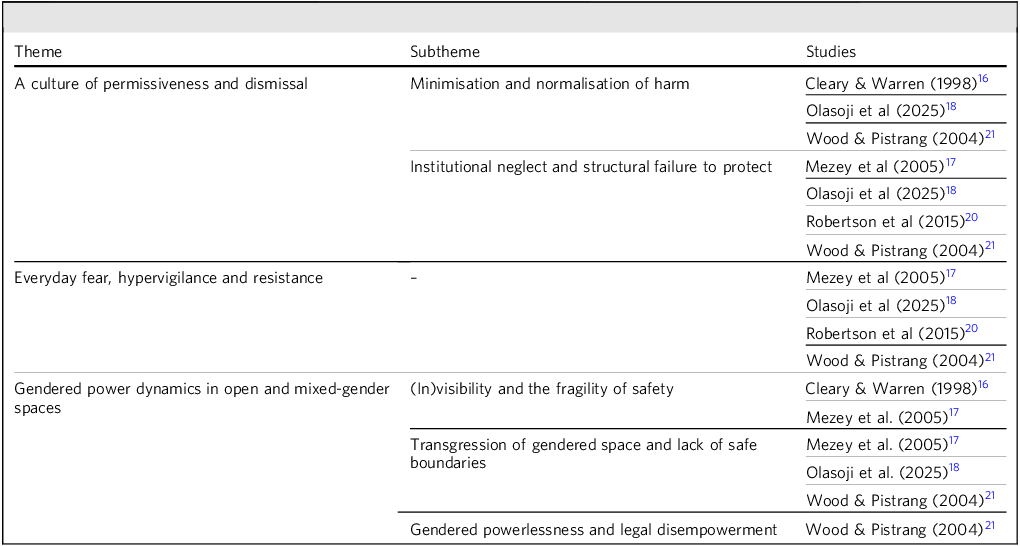
We developed three higher-order analytical themes that capture patients’ subjective experiences and the impact of experiencing or witnessing sexual violence, as well as their accounts of how sexual violence and associated risks are managed and responded to within psychiatric in-patient settings (see Table 2).
A culture of permissiveness and dismissal
This theme illustrates how sexual violence can become normalised within psychiatric in-patient settings through the interplay of patients’ internalisation of harm and institutional inaction.
Minimisation and normalisation of harm
Several female participants described experiences of sexual harassment and non-physical sexualised behaviours, but participants often minimised or downplayed the threat and impacts associated with these experiences. Reference Cleary and Warren16,Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18,Reference Wood and Pistrang21 Participants also reported that behaviours such as sexual comments and lewd gestures were routinely dismissed as harmless or insignificant by staff.
Institutional neglect and structural failure to protect
Several participants reported that staff ignored, dismissed or delayed responding to their concerns about the perceived risks and incidents of sexual violence or harassment. Reference Mezey, Hassell and Bartlett17,Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18,Reference Robertson, Pote, Byrne and Frasquilho20,Reference Wood and Pistrang21 Participants described how nurses responded to their need for a safe space by allowing them to move their mattresses to a meeting room near the nursing station, rather than by addressing the risk. Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18
Beyond neglectful responses, some participants explicitly reported staff misconduct, including inappropriate physical contact and violations of personal boundaries. Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18,Reference Wood and Pistrang21
Everyday fear, hypervigilance and resistance
This theme emphasises the persistent sense of threat, the need for self-protection and the emotional distress associated with the perception of sexual violence risks and experiences of sexual violence during psychiatric in-patient care. Participants described an enduring state of hypervigilance shaped by both direct experiences and the perceived risk of sexual harm. Within this context, many of them engaged in active strategies to protect themselves and reassert personal boundaries, navigating a constant tension between vulnerability and resistance.
Many participants described taking steps to resist harm and assert personal boundaries, such as verbally confronting sexually inappropriate behaviour, avoiding contact with patients who made participants feel unsafe and locking bedroom doors at night. Reference Mezey, Hassell and Bartlett17,Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18,Reference Wood and Pistrang21 Despite these self-protective strategies, the ongoing risk of sexual violence was itself a source of significant emotional and psychological harm. Some participants also experienced sexual violence directly, with both the violence and subsequent institutional neglect leading to fear, disgust and chronic distress. Reference Mezey, Hassell and Bartlett17,Reference Robertson, Pote, Byrne and Frasquilho20,Reference Wood and Pistrang21 For some, these impacts manifested as hypervigilance, immobility, dissociation and emotional withdrawal. Reference Mezey, Hassell and Bartlett17,Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18,Reference Robertson, Pote, Byrne and Frasquilho20
Gendered power dynamics in open and mixed-gender spaces
Women’s safety in psychiatric in-patient settings was shaped by staff visibility, the conduct of others and the absence of protected female-only spaces. Although staff presence could offer reassurance, its absence created fears of undetected harm and, in some cases, staff themselves perpetrated abuse. Legal detention intensified power imbalances and, due to the inability to leave sites of harm, intensified feelings of vulnerability.
(In)visibility and the fragility of safety
Participants’ experiences of safety were linked to the visibility and proximity of staff and the presence of other patients. In a study by Cleary and Warren, Reference Cleary and Warren16 one participant described how the visibility provided by staff presence and the openness of the ward yielded a sense of safety. From the same study, another participant described how a sexual advance was interrupted by staff intervention, potentially preventing an assault. However, participants across two studies also expressed fear that staff might not be present at critical moments, or that incidents could occur without detection. Reference Cleary and Warren16,Reference Mezey, Hassell and Bartlett17
Transgression of gendered space and lack of safe boundaries
Across two studies, participants described male patients entering female patients’ sleeping areas without permission, usually at night, a period marked by heightened vulnerability and fear. Further intrusive behaviours, such as sitting on or approaching female patients in their beds and sexual threats, were also described. Reference Mezey, Hassell and Bartlett17,Reference Wood and Pistrang21
Beyond the actions of other patients, the presence and conduct of male staff also contributed to female patients’ vulnerability. In the study of Wood and Pistrang, Reference Wood and Pistrang21 one participant described how the presence of male staff at night, including when undressing, made her feel exposed, powerless and sexually vulnerable. In the same study, and in a second study, participants described staff behaviour that crossed professional boundaries, including unwanted and inappropriate physical contact. Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18,Reference Wood and Pistrang21
Gendered powerlessness and legal disempowerment
One participant described feeling especially powerless when subjected to sexual misconduct by staff while detained, because the legal constraints of their section status meant that they could not leave the institution or remove themselves from unsafe situations. Reference Wood and Pistrang21
Contradictory constructs
Our analysis identified both intra- and inter-study contradictions. In one study, a female patient described that she had never heard of, let alone encountered, the sexual intimidation of female patients by males within an in-patient setting. Reference Quinn and Happell19 Within the same study, however, one male patient described how men within the setting had forced themselves on female patients and had given them money in exchange for sex. Male and female patients in other studies also reported experiencing or witnessing sexual violence within in-patient settings. This contradiction might be due to individual differences in experiencing or observing sexual violence or could, alternatively, be attributable to differences in the extent to which sexual violence is minimised or normalised, or the willingness to talk about it.
Discussion
This review synthesises qualitative evidence on patients’ experiences of sexual violence in psychiatric in-patient settings, drawing on six studies published between 1998 and 2025. Most accounts came from women, who described a continuum of harmful behaviours, from verbal harassment to sexualised physical violence, perpetrated by both staff and other patients. These experiences occurred in environments where the visibility of staff was inconsistent, gendered spaces were permeable and the constraints of legal detention removed the possibility of leaving unsafe situations. Together, these conditions created a sense of threat, undermining trust in the ward as a therapeutic space.
These findings correspond with long-standing concerns about mixed-gender psychiatric wards. Several governments have sought to reduce mixed accommodation due to heightened vulnerabilities for women, 22,Reference Hoare, Murphy, O’Donoghue, Allen and Duffy23 and more recent reviews continue to emphasise the importance of gender-sensitive ward design. Reference Rodriguez-Labajos, Kinloch, Grant and O’Brien24,Reference Abel and Newbigging25
Participants’ accounts suggest that sexual violence was often minimised – by patients themselves but also by staff. Some patients seemed to downplay non-physical harassment as a means of coping with a hostile environment, whereas others reported that staff had dismissed their concerns. This pattern echoes the concept of institutional betrayal, where trusted institutions fail to protect or validate individuals, thereby compounding harm. Reference Smith and Freyd26 Comparable dynamics have been observed in healthcare settings more broadly, where staff-perpetrated misconduct and dismissive responses to patient reports have been identified. Reference Bismark, Studdert, Morton, Paterson, Spittal and Taouk27
Even when safeguards were present, these were inconsistently applied. Staff visibility sometimes offered reassurance and, on occasions, directly interrupted harmful behaviour. However, participants described incidents occurring at moments of staff absence, particularly in private or poorly monitored spaces. In some cases, staff were themselves identified as perpetrators of sexual misconduct, highlighting the dual role of staff as potentially both protectors and sources of harm. This duality, combined with the closed nature of in-patient environments, left detained women especially vulnerable, echoing wider concerns about coercion and loss of autonomy in mental health detention.
Participants described adopting their own safety strategies – locking doors, avoiding certain peers or confronting inappropriate behaviour. Although these actions reflect the boundary-setting and heightened vigilance described in trauma theory, Reference Herman28 they also signal a transfer of responsibility for safety from the institution to the individual. Such reliance on patient-led resistance risks exacerbating emotional strain, as indicated by accounts of chronic fear, hypervigilance, dissociation and withdrawal. Over time, this constant self-monitoring may erode the intended therapeutic function of in-patient care.
The physical and organisational structure of wards emerged as central to both vulnerability and protection. Mixed-gender accommodation, unprotected female sleeping areas and staffing practices that did not account for gendered needs all contributed to risk. These findings align with long-standing policy debates in the UK and elsewhere about eliminating mixed-gender psychiatric wards 29,Reference Hide30 and implementing gender-sensitive design. Evidence from service evaluations and policy reviews suggests that female-only wards and gender-specific safety protocols can reduce risk and improve patients’ perceptions of safety. Reference Dixon, Petrakis, Fossey, Sim and Barclay31,Reference Kulkarni, Gavrilidis, Lee, Van Rheenen, Grigg and Hayes32
Overall, the synthesis points to a convergence of structural, cultural and interpersonal factors that, together, shape the risk and experience of sexual violence in psychiatric in-patient settings. Minimisation of harm, inconsistent protection and the structural disempowerment of detained women create conditions in which sexual violence can occur and persist. Addressing these risks requires more than physical redesign: it necessitates institutional cultures that actively prevent, recognise and respond to sexual violence, alongside policy frameworks that embed gender-sensitive, trauma-informed practice as a core component of in-patient mental healthcare.
Strengths and limitations
To our knowledge, this is the first systematic review and qualitative synthesis to focus specifically on patients’ subjective experiences of sexual violence within psychiatric in-patient settings. We used a robust search strategy comprising searches of three major databases, reference list screening and citation tracking. Dual screening and quality appraisal reduced the risk of bias and error. The six included studies, published between 1998 and 2025, provided both historical and contemporary perspectives. Interpretative synthesis allowed us to identify recurring patterns and conceptual themes not apparent within individual studies.
Despite comprehensive searches, only a small number of studies were identified and, in most cases, sexual violence was not their primary focus. This probably reflects the neglect of this topic in the research, but may also relate to our decision to exclude non-peer-reviewed literature. Most studies focused on female patients, with very limited data on male patients and none on transgender or non-binary individuals. Similarly, few data were available on sexual minority patients, with only one study specifically examining lesbian, gay, bisexual, transgender and queer/questioning experiences. Reference Robertson, Pote, Byrne and Frasquilho20 This narrow demographic representation restricts the scope of the findings and underscores the need for more inclusive research. All studies were conducted in Western, English-speaking countries, raising questions about the global generalisability of the findings, particularly given the variations in in-patient care. Finally, although the synthesis was informed by the interpretative ethos of meta-ethnography, it did not apply all formal procedures such as reciprocal translation or line-of-argument synthesis, Reference Sattar, Lawton, Panagioti and Johnson33 due to the limited number and depth of the available participant quotations. Instead, analysis involved combining, interpreting and reinterpreting study findings to develop new conceptual insights, while attending to both thematic convergence and interpretative tensions. Reference Aguirre and Bolton34
Implications for research, services and policy
There is an urgent need for empirical research that examines patients’ subjective experiences of sexual violence in psychiatric in-patient settings, using intersectional approaches to capture how gender, sexuality, race, disability and detention status shape both harm and institutional response. Evidence from non-Western, non-English-speaking and low- and middle-income countries is also critical to understanding how cultural and systemic contexts influence patient safety, with comparative studies offering insight into the impact of differing policies, gender norms and healthcare systems.
Preventing sexual violence in psychiatric in-patient settings requires whole-ward culture change, in which staff and patients develop a shared understanding of safety and security and critically routine practices that normalise risk, and commit to proactive safeguarding. 5,Reference Hughes, Lucock and Brooker35–Reference Rahman, Khwaja, Balachandra, Khwaja and Tyrer37 Participants’ accounts underline the need for trauma-informed care, recognising that wards can be sites of both first-time trauma and re-traumatisation. Reference Sweeney, Filson, Kennedy, Collinson and Gillard38
Gender-sensitive care should be standard. This includes the provision of women-only areas or wards, staffed appropriately and designed to protect spatial boundaries through secure bedroom corridors, lockable doors and monitored access. Reference Copperman and Knowles39,Reference Morton, McKenzie, Cooper, Every-Palmer and Jenkin40 Safety planning should begin before admission, with comprehensive risk assessments that address both perpetration and victimisation histories, and be reviewed regularly. Ward protocols should ensure prompt, consistent responses to incidents, underpinned by clear reporting and investigation processes. Safeguarding conversations should be normalised and supported by practical measures such as panic alarms and bedroom doors that can be locked from the inside. Reference Muir-Cochrane, van der Merwe, Nijman, Haglund, Simpson and Bowers41 Staff training should focus on recognising, preventing and responding to sexual violence, initiating respectful discussions about sexual well-being and boundaries Reference Wilson, Eaton, Foye, Ellis, Thomas and Simpson42,Reference Foye, Wilson, Jepps, Blease, Thomas and McAnuff43 and addressing harmful behaviour in ways that resolve underlying causes rather than displacing the problem. Reference Olasoji, Powell, Gazula, Layne, Hui and Adamson18
Body-worn cameras (BWCs) have been proposed as a means of deterring violence, improving incident documentation and increasing accountability. Evidence from acute care and criminal justice contexts suggests that BWCs may reduce some forms of aggression and support transparent investigation processes. Reference Kroger, van Baarle, Widdershoven, Bal and Weenink44 However, their application in mental healthcare raises distinctive ethical and practical concerns, including the potential to heighten surveillance anxiety among patients, exacerbate mistrust in staff–patient relationships and infringe privacy in therapeutic interactions. Participants in one qualitative study expressed mixed views, with some valuing the perceived increase in safety and others perceiving cameras as intrusive or coercive. Reference Wilson, Foye, Thomas, Chadwick, Dodhia and Allen-Lynn45 The effectiveness of BWCs in preventing sexual violence specifically remains untested, and any adoption should be co-produced with patients and staff, guided by clear governance on consent, data use and storage, and integrated within a broader culture of respect and safeguarding rather than used as a standalone measure.
Mental health services should adopt a zero-tolerance framework for sexual violence, with policies that clearly define unacceptable behaviour, specify immediate safeguarding actions and require timely, transparent investigation, including police referral where thresholds are met. Reference Lawn and McDonald46 Accountability can be strengthened by appointing named safeguarding leads, auditing responses and publishing anonymised annual data on incidents and outcomes.
Implementation should draw on established frameworks, such as the Sexual Safety Collaborative’s Standards and Guidance to Improve Sexual Safety on Mental Health and Learning-Disability Inpatient Pathways 47 and the Royal College of Psychiatrists’ Culture of Care Programme, 48 and be supported by confidential, accessible reporting systems for current and historical disclosures. Reference Ashmore, Spangaro and McNamara49
Although further research is urgently needed to inform prevention and response, action cannot wait. Addressing the risks of sexual violence in psychiatric settings requires immediate steps towards sustained cultural change, gender-sensitive design and policies that translate zero-tolerance commitments into consistent safeguarding practice. Embedding trauma-informed, inclusive principles, strengthening accountability and creating safe spaces for disclosure are essential to restoring wards as genuinely therapeutic environments.
About the authors
Yue Deng is a psychology undergraduate student in the Department of Psychology, King’s College London, London, UK. Joanne Butler is a psychiatry registrar at South London and Maudsley NHS Foundation Trust, London, UK. Sian Oram is Professor of Trauma and Recovery in the Department of Health Services and Population Research, King’s College London, London, UK.
Supplementary material
The supplementary material for this article is available online at https://doi.org/10.1192/bjb.2026.10222
Data availability
No new data were created in this study. The data cited can be found in the original articles listed in the references.
Author contributions
J.B. and S.O. conceptualised the study design. J.B. developed and registered the protocol in PROSPERO. J.B. and Y.D. jointly conducted the study selection and quality appraisal. Y.D. led the data curation, coding and analysis, with S.O. providing supervision and guidance. All authors contributed to refining the analysis. Y.D. drafted the original manuscript, and all authors contributed to reviewing and editing it.
Funding
This research was supported by the BECS Foundation and the UK Prevention Research Partnership (Violence, Health, and Society, no. MR-VO49879/1), an initiative funded by the UK Research and Innovation Councils, the Department of Health and Social Care (England) and the UK devolved administrations, and leading health research charities.
Declaration of interest
None.




 Open access
Open access
eLetters
No eLetters have been published for this article.