Inflammation is a natural defence against injury or infection, but chronic inflammation can lead to diseases like cardiovascular issues, type 2 diabetes and cancer by damaging tissues and unhealthy changes in the metabolism(Reference Minihane, Vinoy and Russell1). Conditions such as obesity and cardiovascular diseases are associated with a state of low-grade chronic inflammation, a condition involving the constant release of systemic inflammatory markers, such as TNF, IL-6, and most notably, C-reactive protein (CRP)(2–Reference Ramos, Pellanda and Gus4)
Under normal conditions, CRP levels are below 1 mg/l, in individuals with obesity or metabolic syndrome CRP concentrations often range from 3 to 10 mg/l, indicating a state of low-grade systemic inflammation. However, in chronic diseases such as CVD, chronic obstructive pulmonary disease or cancer, CRP concentrations can exceed 40 mg/l(Reference Karadag, Kirdar and Karul5). Individually, CRP measurement aids in predicting cardiovascular risk and, consequently, in its prevention(2). However, few studies have investigated emerging risk factors for inflammation, such as the consumption of ultra-processed foods (UPF), among young people.
UPF are industrially manufactured products that contain minimal to no whole foods and are primarily composed of ingredients like oils, fats, sugars, starches and proteins that are synthetically produced in laboratories. These products often include additives such as preservatives, colorants and flavour enhancers, designed to improve or replicate the sensory characteristics of natural foods(Reference Monteiro, Cannon and Levy6). The consumption of UPF has been steadily rising, replacing more nutritious meals both at home and in food service settings(Reference Souza, Barufaldi and Abreu7,Reference Bielemann, Motta and Minten8) . On average, UPF have a higher energy density, containing elevated levels of saturated fats, trans fats, free sugars and Na, while being low in essential nutrients such as fibre and vitamins. Excessive intake of these components can lead to metabolic dysregulation, elevating levels of free fatty acids and postprandial glucose, which in turn activate inflammatory pathways through oxidative stress and the release of pro-inflammatory cytokines, contributing to low-grade chronic inflammation(Reference Louzada, Martins and Canella9–Reference de Moura Antunes, Rossi and Inoue11).
Data from the Brazilian Family Budget Survey indicate a significant shift in dietary patterns between 2002–2003 and 2017–2018, with a decline in the consumption of in natura or minimally processed foods and an increase in UPF(Reference Rodrigues, Souza and Bezerra12). In 2017–2018, UPF accounted for 26·7 % of adolescents’ total energy intake(13). Observational studies suggest that diets high in fats and sugars, typical of UPF consumption, are associated with elevated CRP concentrations in adolescents(Reference Oddy, Allen and Trapp14–Reference Khayyatzadeh, Bagherniya and Fazeli16). Furthermore, low-grade chronic inflammation during adolescence has been associated with the development of CVD(Reference Santos, Mesquita and Vieira3,Reference Hertiš Petek, Petek and Močnik17) , metabolic syndrome(Reference Damiani, Kuba and Cominato18), type 2 diabetes(Reference De Albuquerque Melo, Miranda Tassitano and De Moraes Vasconcelos Petribú19) and obesity(Reference Bragança, Mendes and Costa20).
Despite growing evidence of the harmful effects of UPF consumption in adults(Reference Mendoza, Smith-Warner and Rossato21,Reference Hu, Yao and Ge22) , research exploring this association in adolescents remains limited, particularly in relation to inflammatory processes. This study aims to address this gap by evaluating the association between total UPF consumption, as well as specific UPF groups such as sugary beverages and processed meats, with CRP concentrations in Brazilian adolescents.
Methods
Study design and sample
This study utilised data from the Study of Cardiovascular Risk in Adolescents (ERICA), a nationwide, cross-sectional, school-based study aimed at estimating the prevalence of metabolic syndrome and other cardiovascular risk factors in Brazilian adolescents aged 12–17 years. Data collection for ERICA was conducted by trained researchers between February 2013 and November 2014.
The sample was divided into thirty-two strata, comprising the capitals of the twenty-seven Brazilian states and other cities with more than 100 000 inhabitants in each of the five geographical regions of the country. After geographical stratification, the following selection steps were performed: school selection (proportional to the number of enrolled students from the seventh grade of elementary school to the last grade of high school and inversely proportional to the distance between the school and the state capital), three combinations of eligible classes and shifts (morning and afternoon) were randomly chosen. All adolescents in the selected classes were invited to participate in the study. More details about the sampling process were described previously(Reference Bloch, Szklo and Kuschnir23).
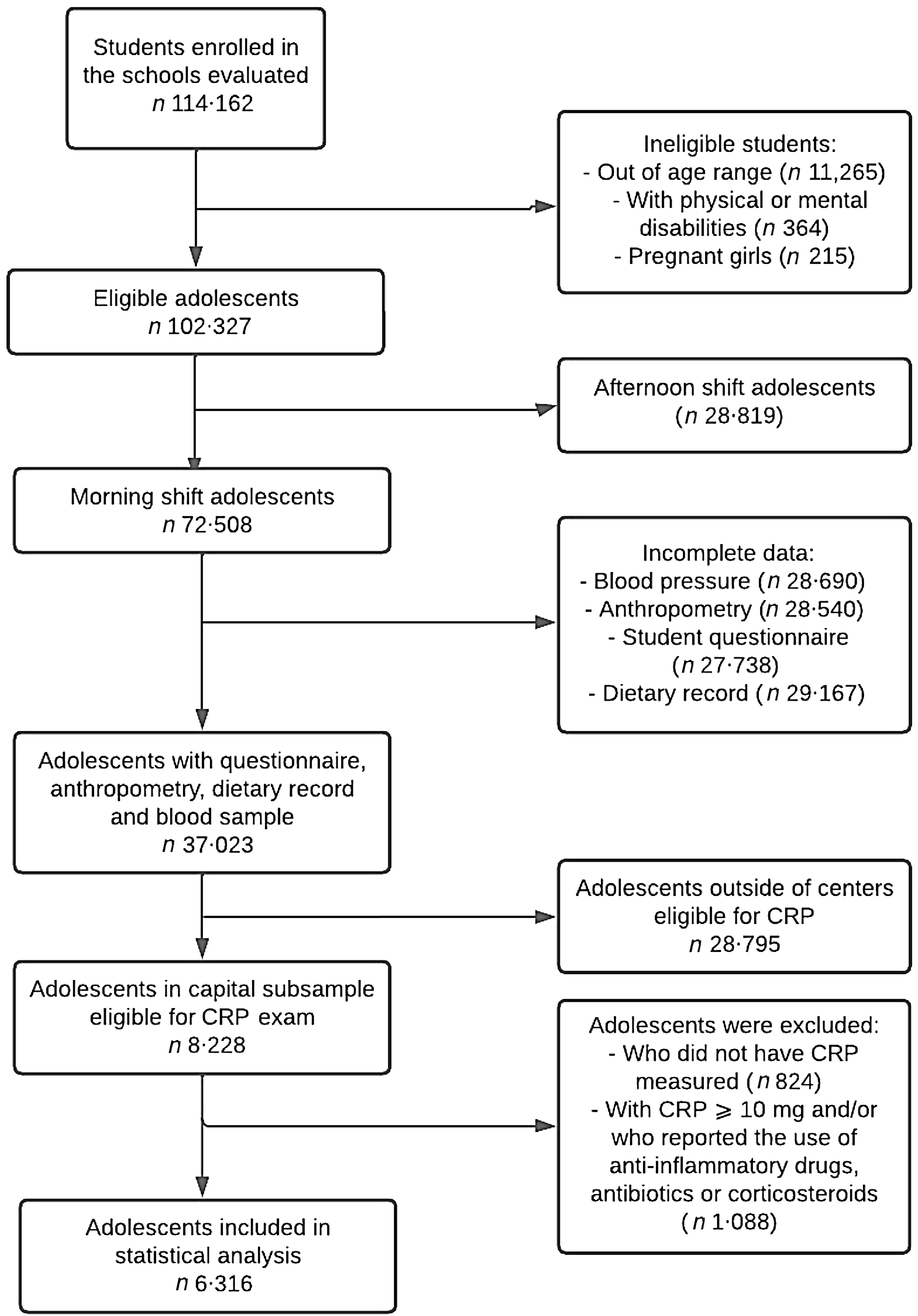
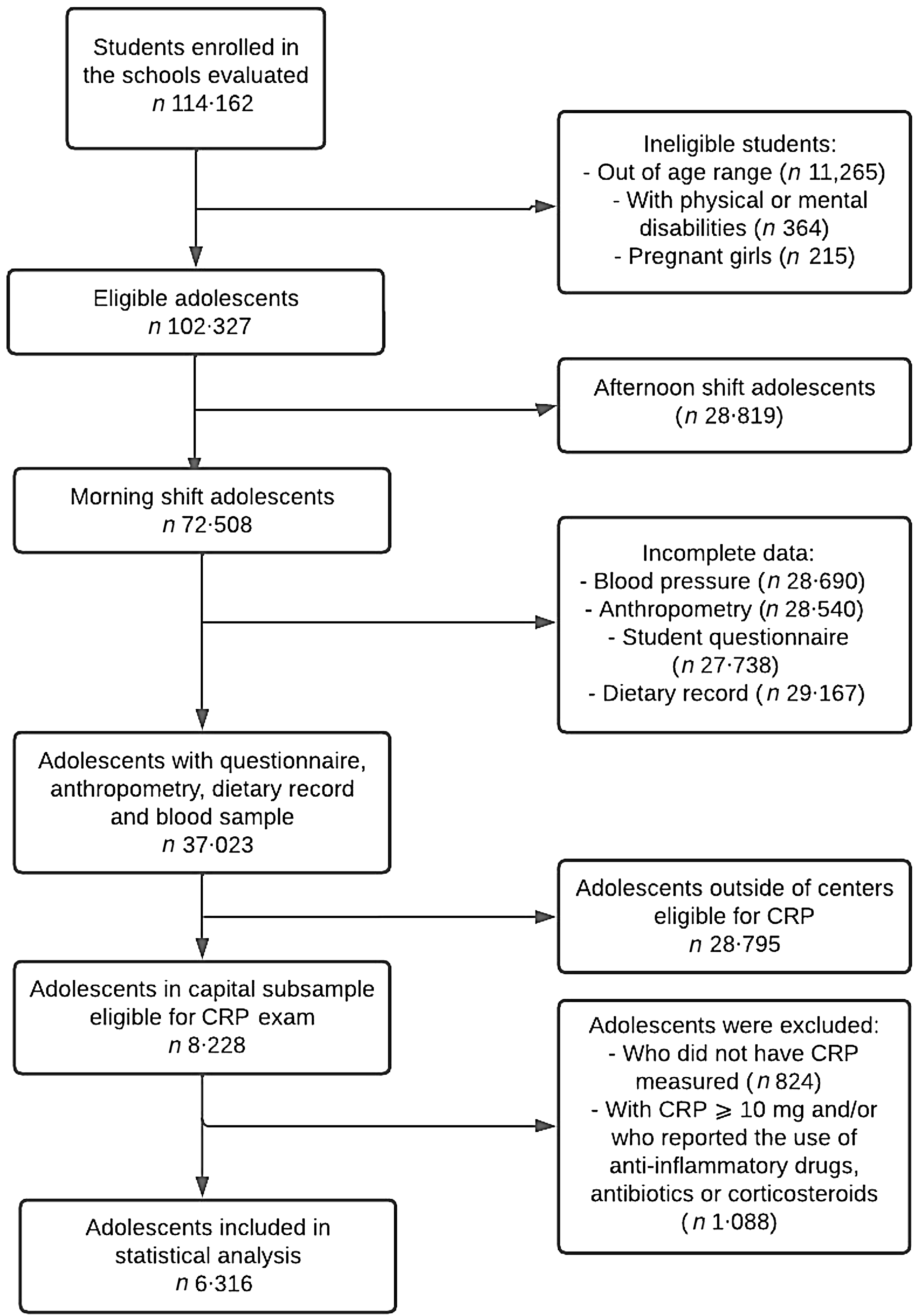
In this study, the analysed sample comprised 6316 adolescents aged 12–17 attending morning classes in schools in six capitals: Brasília, Fortaleza, João Pessoa, Manaus, Porto Alegre and Rio de Janeiro, where CRP concentrations were measured. Adolescents who reported the use of corticosteroids, anti-inflammatory drugs and antibiotics, pregnant individuals and those with CRP concentrations ≥ 10 mg/l (to exclude cases of acute inflammation)(Reference DeBoer24) were excluded. The study entry flowchart is presented in Figure 1.
Flowchart of eligible adolescents in the ERICA study, 2013–2014.
This study was conducted following the ethical principles outlined in the Declaration of Helsinki and was approved by the Research Ethics Committee of the Institute of Public Health Studies, Federal University of Rio de Janeiro (IESC/UFRJ). Approval was also obtained from the ethics committees of each participating study centre. The signed informed consent form from parents or guardians was required for all students participating in the study.
C-reactive protein
Blood samples were collected after a 12-hour fast to obtain CRP measurements. The decision to measure only CRP as an inflammatory marker was mainly due to the limited additional predictive value for cardiovascular risk from the inclusion of other markers(2), as well as logistical and budgetary difficulties at the time of data collection. Blood samples were collected via venipuncture using appropriate tubes for biochemical analysis. Immediately after collection, the samples were centrifuged at 3000 rpm for 10 min to separate the serum. The serum was then either analysed or transferred to cryogenic tubes for storage. Throughout the process, the samples were kept refrigerated to ensure the preservation of the biomarkers(Reference Cureau, Bloch and Henz25). The analysis was conducted in two laboratories using the same technology (immunoturbidimetry - Kit Bio Systems), brand and equipment model (Siemens, Munich, Germany, Advia 2400 Chemical Analyzer). For the centres in Fortaleza, João Pessoa and Manaus, the CRP analysis was performed by a reference laboratory, where the test was conducted immediately after collection. For Brasília, Rio de Janeiro and Porto Alegre, the analysis was conducted in another laboratory, using serum samples stored at a temperature of –80°C. The observed agreement in a sample of tests performed in both laboratories was 0·94 (Bland-Altman test), and when classified as > 3 mg/l, the Kappa of the subsample with the experimental dose was 0·86. For the purposes of analysis in this study, CRP was classified as ≤ 3 mg/l, indicating the absence, or > 3 mg/l indicative of the presence of low-grade inflammation(26). This decision was made to use reference values for adults since there are no specific reference values for adolescents.
Ultra-processed food consumption
To assess the consumption of UPF, a 24-hour dietary recall (R24h) was conducted. The choice of a dietary recall method was made with the intention of capturing the wide dietary diversity of the Brazilian population across different regions, including UPF. The multipass method(Reference Barufaldi, Abreu and Veiga27) was employed for this purpose, which involves a guided interview in five stages aiming to reduce underreporting of food consumption. The five stages that guide the interview are based on the following steps: (1) quick listing of the foods and beverages consumed; (2) questions about foods that are usually omitted; (3) the time each food was consumed; (4) detailed description of the foods and their respective quantities, reviewing the information on the time and occasion of consumption and (5) final review of the information and probing for any foods that were consumed but not reported.
The R24h was conducted directly on notebooks using the software developed for the study, ERICA-REC24h(Reference Barufaldi, Abreu and Veiga27), for entering dietary data. The software includes lists of foods constructed from the food and beverage database from the Brazilian Family Budget Survey 2008–2009, conducted by the Brazilian Institute of Geography and Statistics(28). To assess portion sizes, researchers referred to photographic records in the software related to household measurements. Foods reported by adolescents that were not included in the ERICA-REC24h database were manually added by researchers.
To calculate the energy consumption of each adolescent, consumption estimates were converted to grams and associated with the Brazilian table of food composition(28). For the classification of foods according to their degree of processing, the NOVA classification was used, dividing foods into four groups: (1) Unprocessed or minimally processed foods: foods obtained directly from plants or animals without undergoing any alteration (e.g. fruits, vegetables, eggs, meats) or that have undergone minimal changes such as cleaning, fermentation, pasteurisation, removal of inedible parts and refrigeration (e.g. dried or polished grains, flours, pasteurised milk, yoghurt, nuts, coffee, chilled or frozen meats); (2) Culinary ingredients: natural ingredients like sugar, salt, oils and fats used to add flavour to preparations and do not contain food additives; (3) Processed: foods in which salt, sugar or other culinary ingredients are added during their manufacturing process (canned vegetables, cereals or legumes, tomato extract or concentrate with salt, salted, dried and smoked meats, fish preserved in oil or water and salt, candied or crystallised fruits, cheeses, bread made with flour, yeast, water and salt); 4) Ultra-processed: foods from industrial formulations, highly processed with a variety of exclusively industrial chemicals. UPF are rich in sugar, fat, Na or artificial sweeteners. UPF uniquely contain food substances with no or rare culinary use (invert sugar, fructose, corn syrup, gluten, soluble or insoluble fibre, maltodextrin, isolated soy protein, interesterified oil) and/or cosmetic food additives (colourings, flavourings, flavour enhancers, emulsifiers, thickeners, sweeteners)(Reference Monteiro, Cannon and Levy6).
Culinary preparations reported in the R24h were disaggregated, and ingredients were classified according to the above categories. The classification was performed by two independent investigators, and disagreements were resolved by a third investigator(Reference Rocha, Gratão and Carmo29). In addition to the variable of the percentage of total daily energetic intake from UPF in the diet, variables were also constructed for the percentage of daily caloric intake from the following groups of UPF: rich in carbohydrates (mass-produced packaged bread and cakes, instant ‘seasoned and packaged’ noodles, cakes and cake mixes, ‘ready-to-heat’ products, including ready-made pies, pizzas and pasta preparations); dairy beverages (fruit yoghurts, chocolate-flavoured milk and other dairy derivatives with added colourings and flavourings); sodas and sugary beverages (nectars, processed juices and ultra-processed energy drinks); processed meats (sausages, burgers, and other reconstituted meat products); sweets (ice cream, chocolate, other confectionery); margarine and sauces and snacks. Finally, the percentage of caloric intake from UPF was estimated as a percentage of daily caloric consumption.
Covariates
Covariates were obtained through a self-reported structured questionnaire by adolescents, entered into an electronic data collector (Personal Digital Assistant - PDA). The investigated socio-demographic variables included sex (female/male), age (12–17 years-old), study centre (Manaus, Fortaleza, Brasília, João Pessoa, Rio de Janeiro, Porto Alegre), type of school (public or private) and self-reported skin colour (categorised according to the definition adopted by the Brazilian Institute of Geography and Statistics - IBGE - white, brown, black, yellow/indigenous). Socio-economic concentration was assessed according to the Brazil Criterion of the Brazilian Association of Research Companies, which considers ownership of goods and the presence of a domestic employee. Its score can range from 0 to 46. For this study, the total score was divided into tertiles, considering adolescents classified in the highest tertile as having a higher socio-economic level.
Behavioural variables encompassed smoking, passive exposure to tobacco, alcohol consumption, physical activity and screen time. For the tobacco-related variable, definitions from the Centers for Disease Control and Prevention of the USA (CDC) on the Global Youth Tobacco Surveillance(Reference Warren, Jones and Asma30) were adopted. Adolescents answered questions about smoking and environmental exposure to tobacco smoke. Active smokers were those who reported smoking cigarettes on at least one day in the last 30 d. Regarding passive smoking, the following questions were asked: (1) Do you come into contact with the smoke from cigarettes (or cigars, pipes, cigarillos) of other people in the home where you live? (2) Do you come into contact with the smoke from cigarettes (or cigars, pipes, cigarillos) of other people outside the home (at school, parties, bars, work or other places) to the point of smelling it? For these questions, responses were dichotomous (yes/no). Alcohol consumption was assessed through the following question: in the last 30 d, on how many days did you have at least one glass or dose of alcoholic beverage? Adolescents who had consumed at least one glass of alcohol in the last 30 d were considered alcohol consumers(Reference Ryan and Kokotailo31).
To determine physical activity time, an adaptation of the Self-Administered Physical Activity Checklist(Reference Farias Júnior, Lopes and Mota32) was used. This questionnaire is widely utilised in research with adolescents, featuring a list of 24 activities with the option to include other activities if not listed. It allows adolescents to report how often (days) and the duration (hours and minutes) they engaged in moderate to vigorous physical activity during leisure time over the past week. The questionnaire has acceptable reproducibility (intra-class correlation coefficient = 0·88; 95 % CI: 0·84, 0·91, with 52 % agreement on meeting the recommended physical activity level) and validity (Spearman’s ρ for total minutes of physical activity per week was 0·62 compared to four 24-hour recalls) in Brazilian adolescents(Reference Farias Júnior, Lopes and Mota32). Adolescents who did not accumulate at least 420 min/week of moderate and vigorous physical activity were considered insufficiently active in leisure time(33).
Screen time refers to the time respondents spend watching TV, using computers, and playing video games, assessed through a single question: on a normal weekday, how many hours do you spend watching TV, using a computer or playing video games? The obtained response was categorised based on recommendations to limit adolescents’ screen time to a maximum of 2 h/d(34).
Anthropometric variables included weight and height measurements, used to determine BMI and waist circumference (WC), were performed by trained researchers according to standardised procedures(Reference Bragança, Mendes and Costa20). Body weight was measured on an electronic scale (Líder, Araçatuba, São Paulo, Brazil, model P200M), with a capacity of 200 kg and precision of 50 g(Reference Lohman, Martorell and Roche35). Height was measured with 0·1 cm accuracy using a portable stadiometer (Alturexata, Belo Horizonte, Minas Gerais, Brazil). BMI was calculated by dividing weight by height squared, thereafter classified according to the curves proposed by the WHO. Adolescents with a Z-score < 1 were classified as ‘normal weight,’ Z-score ≥ 1 and < 2 as ‘overweight,’ and those with a Z-score ≥ 2 were classified as ‘obese.’ WC was measured with the aid of an inelastic measuring tape (Sanny, São Bernardo do Campo), with 0·1 cm precision, twice, obtaining the average between them. The measurement was taken with participants standing, arms at their sides, feet slightly apart and the abdomen relaxed, at the midpoint between the lower ribs and the upper edge of the iliac crest(36). A maximum variation of 1 cm between the two measurements was allowed; if the difference exceeded this value, the WC measurement was repeated.
Statistical analysis
All studied variables were described using mean or proportion with their respective 95 % 95 % CI. The UPF was evaluated as a percentage of the total daily energetic intake and categorised into quartiles (Q1 ≤ 13·9 % kcal/d; Q2 = 14·0 % to 28·1 % kcal/d; Q3 = 28·2 % to 44·8 % kcal/d; Q4 ≥ 44·9 % kcal/d). In addition, UPF subgroups were dichotomised based on the median consumption in the sample to identify adolescents with higher consumption of these products, due to the absence of normative consumption values.
Heterogeneity or linear trend in the results was assessed by the Wald’s test. Poisson regression models with robust variance were used to assess the association of UPF consumption quartiles with relatively high CRP values. Prevalence ratios and their respective 95 % CI were presented in hierarchical models of three concentrations adjusted for gender, age, type of school, region, skin colour and socio-economic status (Model 1); Model 1 + physical activity, active and passive smoking, screen time, alcohol consumption and total energetic intake (Model 2); Model 2 + WC in centimetres (Model 3). The selection of variables included in the models was based on the literature; after inclusion, variables were kept in the models, and those from the next levels of adjustment were added.
All analyses were performed in Stata version 14.0 (StataCorp). The ‘svy’ command set was used to consider the complex sample design and represent the entire population of studied adolescents. All tests were two-tailed, and a P-value less than 0·05 was statistically significant.
Results
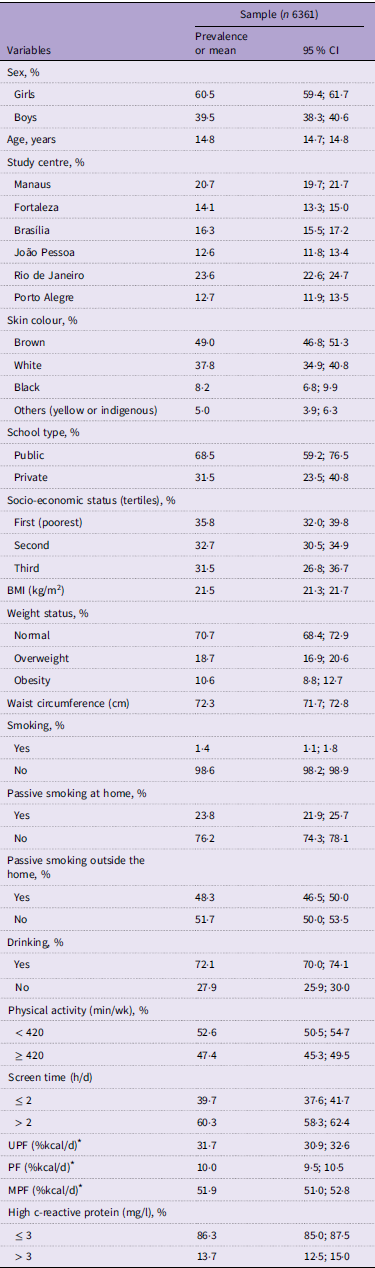
A total of 6316 participants were included in the analysis. The sample description is presented in Table 1. We observed that the majority of adolescents were female (60·5 %), with brown skin colour (49 %) and attending public schools (68·5 %). The prevalence of overweight/obesity in the sample was 29·3 %. Despite the low occurrence of smoking (1·4 %), many adolescents reported passive smoking outside (48·3 %) or inside the home (23·8 %). Most of the adolescents (52·6 %) were classified as physically inactive, and 60·3 % reported excessive screen time. The mean of UPF consumption was 523 g (95 % CI: 500, 546), which represents 31·7 % of the total daily energy intake.
Characteristics of adolescents included in the study sub-sample, ERICA 2013–2014
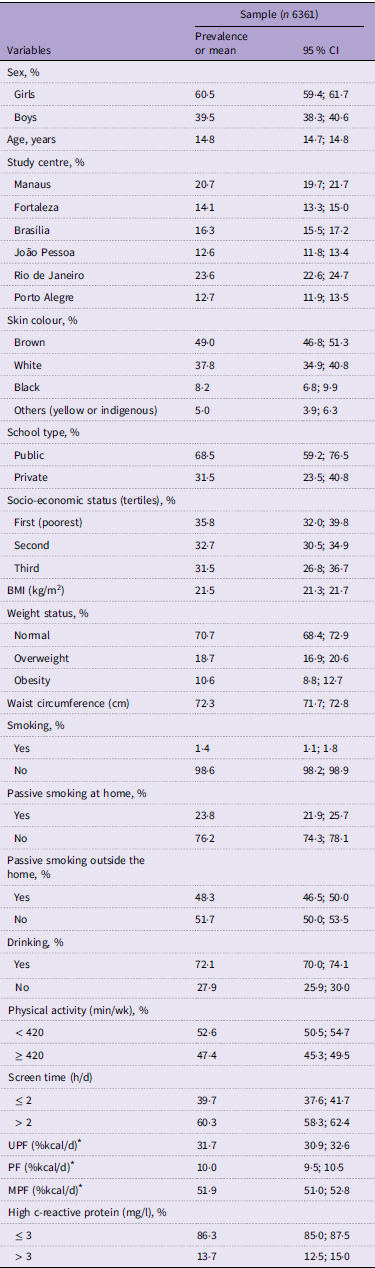
UPF, ultra-processed foods; PF, processed foods; MPF, minimally processed foods.
* The classification of the degree of food processing was done according to the NOVA classification.
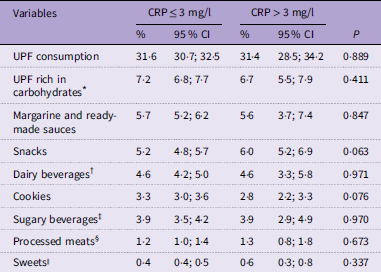
The prevalence of elevated CRP was 13·7 %. The median of CRP was stable through the quartiles of UPF consumption (median (p25–p75): 1st = 0·20 (0·12–0·98); 2nd = 0·20 (0·12–1·12); 3rd = 0·20 (0·12–0·91) and 4th quartile = 0·23 (0·12–1·05)). Table 2 presents the consumption of different groups of UPF according to the classification of CRP concentration. Overall, the most consumed UPF were those with high carbohydrate content, snacks and sweetened beverages. When analysing the UPF consumption, no differences were observed in total consumption and subcomponents, according to CRP concentrations.
Percentage of caloric contribution from UPF stratified by CRP concentration among adolescents, ERICA 2013/2014
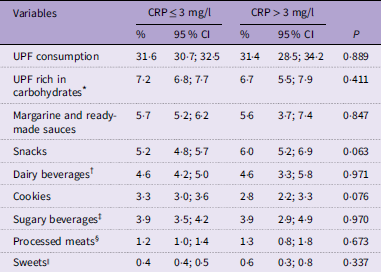
UPF, ultra-processed foods; CRP, C-reactive protein.
* UPF rich in carbohydrates = packaged breads and cakes produced on a large scale, ‘tempered and packaged’ instant noodles, cakes and cake mixes, ‘ready-to-heat’ products, including ready-made pies, pizzas and pasta preparations.
† Dairy beverages = fruit yoghurts, flavoured milk and other dairy derivatives.
‡ Sugary beverages = soda, nectars, juices and ultra-processed energy drinks.
§ Processed meats = sausages, hamburgers and other reconstituted meat products.
|| Sweets = ice cream, chocolate, other confectionery and culinary ingredients.
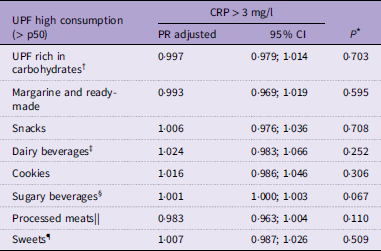
The association between the consumption of UPF and relatively high CRP is presented in Table 3. High consumption of UPF (highest quartile, ≥ 44·9 % kcal/d) was modestly associated with a relatively high CRP after adjusting for potential confounders (prevalence ratio = 1·039; 95 % CI: 1·006, 1·073), compared with those reporting lower consumption of these foods. This association was also observed, but with an even lower magnitude, among adolescents in the third quartile of UPF consumption (28·2 % to 44·8 % kcal/d). However, when evaluating different types of UPF separately, such as UPF rich in carbohydrates, margarine and ready-made sauces, snacks, cookies, dairy beverages, sugary beverages, processed meats and sweets, no associations were observed between high consumption of these UPF – represented by values above the median consumption in the sample – and elevated CRP concentrations (Table 4).
Association of UPF consumption with altered concentrations of CRP in adolescents, ERICA 2013/2014

UPF, ultra-processed foods; CRP, C-reactive protein.
Model 1: adjusted for sex, age, region, skin colour, school type and economic status.
Model 2: adjusted for Model 1 plus active and passive smoking, alcohol consumption, physical activity and total energetic intake.
Model 3: Model 2 plus waist circumference.
* Wald’s test for trends.
Association of high consumption, above the median, of UPF subcomponents with altered CRP, ERICA 2013/2014
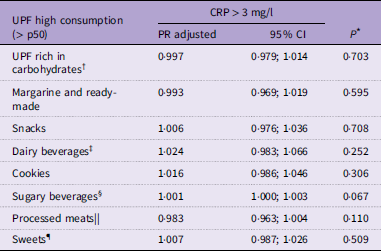
UPF, ultra-processed foods; CRP, C-reactive protein.
Adjusted PR for: sex, age, region, skin colour, school type, economic status, active and passive smoking, alcohol consumption, physical activity, calorie intake, minimally processed food consumption and waist circumference.
* Wald’s test for heterogeneity.
† UPF rich in carbohydrates = packaged breads and cakes produced on a large scale. ‘tempered and packaged’ instant noodles, cakes and cake mixes. ‘ready-to-heat’ products, including readymade pies, pizzas and pasta preparations.
‡ Dairy beverages = fruit yoghurts, flavoured milk and other dairy derivatives.
§ Sugary beverages = soda, nectars, juices and ultra-processed energy drinks.
|| Processed meats = sausages, hamburgers and other reconstituted meat products.
¶ Sweets = ice cream, chocolate and other confectionery and culinary ingredients.
Discussion
This study aimed to evaluate the association between UPF consumption and CRP concentrations, a marker of low-grade systemic inflammation, in adolescents. We observed a modest positive association between UPF consumption and relatively high CRP concentrations (≥ 3 mg/l). However, when analysing different UPF groups separately – such as carbohydrate-rich UPF, margarine and ready-made sauces, snacks, cookies, dairy beverages, sugary beverages, processed meats and sweets – no significant associations with elevated CRP were found.
The percentage of energetic contribution from UPF observed in the diet of adolescents in this study (31·7 %) was similar to the 27 % found in the Brazilian Family Budget Survey 2017–2018(Reference Rodrigues, Souza and Bezerra12) and lower than the UPF consumption of 39·7 % observed in the National School Health Survey conducted in 2012(Reference Costa, Flores and Wendt37). These levels of consumption can be considered high, and it is associated with chronic low-grade inflammation(Reference da Costa Louzada, Baraldi and Steele38–Reference Tavares, Fonseca and Rosa40).
Our analyses showed a modest association between higher total consumption of UPF (≥ 44·9 % kcal/d) and elevated CRP concentrations. Martins et al. (Reference dos Santos Martins, da Cunha França and Viola41) also observed that adolescents (n 391), aged 17–18 years from a northeastern Brazilian city with higher UPF consumption had higher concentrations of IL-8 (β = 0·58; 95 % CI: 0·12, 1·00). However, they did not find an association with CRP levels (β = 0·26; 95 % CI: –0·12, 0·64). Our results extend previous findings among Brazilian adolescents by studying a broader age range of adolescents, as well as a large sample from centres across the entire country, which consequently provides greater variability in dietary consumption habits nationwide.
A hypothesis for the occurrence of this association derives from the fact that UPF is rich in sugar, refined carbohydrates and saturated fatty acids, which may trigger a heightened inflammatory response in the body. For instance, excessive intake of simple carbohydrates and sugars can rapidly alter circulating glucose and insulin concentrations, leading to postprandial hyperglycaemia, which may induce endothelial dysfunction, increased production of free radicals and pro-inflammatory cytokines, thereby generating a pro-atherosclerotic state(Reference Giugliano, Ceriello and Esposito42,Reference Santos, Gagliardi and Xavier43) . Furthermore, these foods are low in fibre and antioxidants, nutrients that could play an anti-inflammatory role and, consequently, reduce the risk of developing chronic inflammation(Reference Navarro, De Dios and Jois44).
However, when evaluating different UPF groups individually (carbohydrate-rich UPF, margarine and ready-made sauces, snacks, cookies, dairy beverages, sugary beverages, processed meats and sweets), no associations with CRP > 3 mg/l were found. This may suggest that the overall quantity of UPF consumed is more important than specific UPF groups. Juul et al. (Reference Juul, Deierlein and Vaidean45) found that beyond changes in nutritional composition (macro- and micronutrients), food (ultra)processing can alter the physical structure and chemical composition, including the addition of artificial sweeteners and the presence of neo-formed contaminants, posing health risks. This suggests, hypothetically, that the cumulative effect of different UPF components may contribute to increased chronic inflammation. However, experimental data to support this hypothesis are still limited. Moreover, some authors propose that such components may exacerbate biological pathway alterations (e.g. increased oxidative stress, inflammation, dysglycemia and hypertension) and facilitate changes in gut microbiota due to the increased circulation of lipopolysaccharides from dysbiotic bacteria (metabolic endotoxemia)(Reference Juul, Deierlein and Vaidean45,Reference Guerville, Leroy and Sinquin46) . Future research, including experimental studies, is needed to investigate the causal relationship between UPF consumption and chronic inflammation and to elucidate the underlying biological mechanisms.
The findings of this study reinforce the recommendations of the official guidelines from the Brazilian Ministry of Health, which advocate prioritizing nature and minimally processed foods and culinary preparations while avoiding UPF(47). Previous studies based on health education interventions targeting adolescents to increase knowledge about food classification, limit UPF consumption and promote the consumption of in natura and minimally processed foods have shown promising results in increasing vegetable intake, reducing overall UPF and soda consumption and improving cardiometabolic health indicators(Reference Fonseca, Bertolin and Gubert48–Reference Marques, Ferreira and Santos50).
Some limitations should be considered when interpreting the results of this study. Firstly, data from only one dietary recall were utilised, potentially leading to differences between actual habitual intake and the reported intake. Additionally, weekend dietary intake was not assessed, possibly underestimating UPF consumption. The classification of foods according to the NOVA framework occurred after data collection, potentially leading to misclassification and impacting the assessment of UPF subgroups. In this study, we assessed only CRP as an inflammatory marker, which limits our findings. However, it is a first-line clinical marker that allows for comparisons with previous studies. Due to the cross-sectional design, causal relationships cannot be established, and the possibility of reverse causality cannot be entirely ruled out. Among the strengths of this study are the sample size, data collection by a trained researcher team, laboratory tests conducted in certified and comparable facilities and the inclusion of adolescents from all regions of Brazil.
Conclusion
In this study, we observed a modest association between higher UPF consumption and relatively high concentrations of CRP (> 3 mg/l) in a large sample of Brazilian adolescents. However, no association was found between specific UPF groups and elevated CRP. These findings suggest a potential association between overall UPF consumption and early signs of low-grade inflammation in adolescents. Experimental and cohort studies are needed to further explore the role of UPF in inflammatory processes and their potential health consequences from adolescence to adulthood.
Acknowledgements
Not applicable.
The ERICA project was financed by the Department of Science and Technology of the Department of Science and Technology and Strategic Inputs of the Ministry of Health (Decit /SCTIE/MS) and the Health Sector Fund (CT –Saúde) of the Ministry of Science, Technology and Innovation (MCTI) by the Innovation and Research Financing Agency (FINEP: protocol 01 090 421), and the National Council for Scientific and Technological Development (CNPq: protocols 565037/2010–2, 405009/2012–7 and 457050/2013–6). We thank the Research Incentive Fund at the Hospital de Clínicas de Porto Alegre (FIPE-HCPA –20090098, 20150400 and 20200522). This work was supported by the Coordination for the Improvement of Higher Education Personnel –Brazil (CAPES) –Financing Code 001.
Conceptualisation: G. R. d. S., N. N. F. M., P. B. Z. R. e F. V. C. Formal analysis: F. V. C. Supervision: B. D. S., F. V. C. Writing – original draft: G. R. d. S. Writing – review and editing: L. L. M., A. S. d. C., B. D. S., F. V. C.
All authors declare that they have no potential conflicts of interest.