


Introduction
The COVID-19 pandemic not only severely impacted the physical health of the population (Islam et al Reference Islam, Jdanov, Shkolnikov, Khunti, Kawachi, White, Lewington and Lacey2021) but also their mental health (Santomauro et al Reference Santomauro, Mantilla Herrera, Shadid, Zheng, Ashbaugh, Pigott, Abbafati, Adolph, Amlag, Aravkin, Bang-Jensen, Bertolacci, Bloom, Castellano, Castro, Chakrabarti, Chattopadhyay, Cogen, Collins, Dai, Dangel, Dapper, Deen, Erickson, Ewald, Flaxman, Frostad, Fullman, Giles, Giref, Guo, He, Helak, Hulland, Idrisov, Lindstrom, Linebarger, Lotufo, Lozano, Magistro, Malta, Månsson, Marinho, Mokdad, Monasta, Naik, Nomura, O’Halloran, Ostroff, Pasovic, Penberthy, Reiner, Reinke, Ribeiro, Sholokhov, Sorensen, Varavikova, Vo, Walcott, Watson, Wiysonge, Zigler, Hay, Vos, Murray, Whiteford and Ferrari2021). Social isolation and lack of interaction due to lockdowns as well as economic uncertainty were key drivers of increased stress, anxiety, and depression among the general population (Ernst et al Reference Ernst, Niederer, Werner, Mikton, Ong, Rosen, Brähler and Beutel2022; Fetzer et al Reference Fetzer, Hensel, Hermle and Roth2021). Moreover, some occupational groups such as healthcare professionals faced extremely high levels of stress and anxiety due to work-related factors (work overload, resource shortages, extended shifts), social and familial issues (social distancing, fear of infecting loved ones, social stigma), and patient circumstances (high mortality rates, ethical dilemmas) (Al Maqbali et al Reference Al Maqbali, Alsayed, Hughes, Hacker and Dickens2024; Sachdeva et al Reference Sachdeva, Nandini, Kumar, Chawla and Chopra2022). Other essential workers in non-healthcare fields (agriculture, food industry, supermarkets, maintenance services, social care, etc.) experienced stress and anxiety levels sometimes surpassing those of frontline healthcare workers due to inadequate training, lack of personal protective equipment (PPE), and insufficient employer support (Chowdhury et al Reference Chowdhury, Kainth, Godlu, Farinas, Sikdar and Turin2022; Schou-Bredal et al Reference Schou-Bredal, Bonsaksen, Ekeberg, Skogstad, Grimholt and Heir2022).
Despite growing literature on COVID-19 and workers’ mental health, little is known about whether, and how, worker representation mitigates workers’ concerns about contagion and transmission in the workplace. This article addresses the following research question: Is the active participation of worker representatives in negotiating and implementing COVID-19 protective measures associated with lower levels of concern among workers about contracting or transmitting the virus?
This study contributes to research on COVID-19 in the workplace, worker representation, and occupational health by focusing on psychological concerns and fear rather than physical outcomes such as infection or mortality. It further extends the literature by distinguishing between the mere presence of worker representatives and their active participation in protective decision-making processes. The paper also documents inequalities in access to representative protection and shows how concern about infection is concentrated among workers who are most exposed to risk and least protected from an institutional standpoint. The COVID-19 pandemic constitutes a critical case for examining how worker voice and representation function in contexts of heightened risk to mental health and psychosocial protection at work. Understanding these mechanisms remains highly relevant both for addressing future public health emergencies and for the broader literature on occupational health governance and industrial democracy. The article is structured as follows. First, an overview is made of the existing literature on the psychological consequences of the fear of contracting or transmitting COVID-19 and the possible role that worker representation can play in its mitigation. This overview highlights the research gap in this area. The methodology is then detailed, followed by a description of the results, which are presented in two sections differentiating between concern about contracting and transmitting the virus. Finally, the discussion section integrates the findings with previous literature, emphasising their theoretical and practical implications, as well as the limitations of the study and potential future research areas.
Fear of contracting or transmitting COVID-19 in the workplace
Various factors have been linked to augmented mental health issues during the pandemic. Among these, fear of contracting COVID-19 at work and/or transmitting the disease was associated with increased anxiety, stress, depression, insomnia, and decreased psychological well-being in the general population (Alimoradi et al Reference Alimoradi, Ohayon, Griffiths, Lin and Pakpour2022; Luo et al Reference Luo, Ghanei Gheshlagh, Dalvand, Saedmoucheshi and Li2021). Fear is understood as ‘an anticipatory emotion triggered when a situation is perceived as threatening to our safety or that of others’ (Garcia Reference Garcia2017, 462). During the pandemic, this fear extended beyond concerns of personal illness to worries about infecting loved ones and uncertainty about the severity of the disease (Han et al Reference Han, Mahendran and Yu2021). The coexistence of fear and concern was evident in phenomena such as coronaphobia, defined as ‘an excessive response triggered by fear of contracting the virus causing COVID-19, leading to excessive worry about physiological symptoms and significant stress from personal and occupational losses’ (Arora et al Reference Arora, Jha, Alat and Das2020, 2). Accordingly, some studies employed indicators of worry about coronavirus to measure fear (Ahorsu et al Reference Ahorsu, Lin, Imani, Saffari, Griffiths and Pakpour2022; Mertens et al Reference Mertens, Gerritsen, Duijndam, Salemink and Engelhard2020).
Mental health issues derived from fear of contracting or transmitting COVID-19 were amplified among workers in both essential and non-essential sectors, because workplace conditions were often conducive to COVID-19 transmission. This includes conditions such as close physical proximity and frequent social interactions with colleagues, supervisors, clients, students, or patients (Giorgi et al Reference Giorgi, Lecca, Alessio, Finstad, Bondanini and Lulli2020). To curb virus transmission and alleviate psychological consequences, the Spanish government, like many others, established occupational risk prevention protocols. COVID-19 protective measures were introduced at personal (use of PPE), collective (disinfectant gel, dividers, maintaining social distancing), and organisational levels (introduction of telework, work schedule reorganisation, tasks and workplaces reassignment) (Ministerio de Sanidad 2021).
From an organisational psychology perspective, studies using the Job Demands–Resources model have considered how COVID-19 protective measures are workplace resources that mitigate the relationship between perceived infection risk (a job demand) and psychological distress or burnout. These studies also consider the impact of communication systems and participatory decision-making (Eguchi et al Reference Eguchi, Hino, Inoue, Tsuji, Tateishi, Ando, Nagata, Matsuda and Fujino2021; Falco et al Reference Falco, Girardi, Dal Corso, Yıldırım and Converso2021). Occupational health and safety research has yielded mixed results. Some studies found a positive correlation between the number of preventive measures and increased fear of infection, suggesting that such measures heighten risk awareness (Sasaki et al Reference Sasaki, Kuroda, Tsuno and Kawakami2020). Others report protective effects on fear and distress (Asaoka et al Reference Asaoka, Sasaki, Imamura, Kuroda, Tsuno and Kawakami2022; Chaudhry et al Reference Chaudhry, Rasool, Raza, Mhelska and Ur Rehman2023). There is little research on the specific effectiveness of different COVID-19 protective measures in reducing fear. Although some evidence suggests that personal protective measures are most effective (Asaoka et al Reference Asaoka, Sasaki, Imamura, Kuroda, Tsuno and Kawakami2022), other points to collective and organisational measures (Chaudhry et al Reference Chaudhry, Rasool, Raza, Mhelska and Ur Rehman2023) so further exploration is needed to address this gap.
The role of worker representatives’ participation in implementing COVID-19 preventive measures
The positive impact of worker participation on occupational health and safety is well-established (Graham and Walters Reference Graham and Walters2021; Gunningham Reference Gunningham2008; Walters and Nichols Reference Walters and Nichols2007). This participation can be direct, involving employees in decision-making about their work and safety through team meetings or quality circles. It can also be indirect, via formal structures of representation often channelled or backed by trade unions, such as health and safety representatives or health and safety committees (García-Miguélez Reference García-Miguélez2009; Menéndez et al Reference Menéndez, Benach and Vogel2009). Although studies have shown the benefits of direct worker participation in areas such as ergonomics (Rivilis et al Reference Rivilis, Van Eerd, Cullen, Cole, Irvin, Tyson and Mahood2008), improved psychosocial health (Llorens-Serrano et al Reference Llorens-Serrano, Salas-Nicás, Navarro-Giné and Moncada Lluís2022), and reduced absenteeism (Payá Castiblanque Reference Payá Castiblanque2020a), this research focuses on indirect participation, collective, and representative. The present study adopts a critical perspective on labour relations, which holds that workers’ participation ‘cannot be separated from the problems of power, authority, legitimacy, and control; it is inevitable that it involves a political aspect’ (Boix and Vogel Reference Boix, Vogel, Ruiz-Frutos, Delclòs and Ronda2013, 151). Within the framework of industrial democracy, participation should be understood as an extension of workers’ power and control in decision-making, allowing them to influence the technical-productive behaviour of the company. This vision stands in contrast to the economistic approach, where ‘cosmetic’ participation predominates, based on the manipulation of workers’ motivations to align them with corporate objectives (Martín Reference Martín1995, 371).
Literature examining the various repercussions of worker representatives’ actions in relation to workplace matters – including occupational health – often refers to the ‘union effect’. Historically, the presence of worker representatives has been shown to improve preventive management standards (risk assessment and prevention action planning) in different institutional contexts (Coutrot Reference Coutrot2009; Jirjahn et al Reference Jirjahn, Mohrenweiser and Smith2022; Ollé-Espluga et al Reference Ollé-Espluga, Vergara-Duarte, Belvis, Menéndez-Fuster, Jódar and Benach2015; Payá Castiblanque Reference Payá Castiblanque2023; Walters et al Reference Walters, Nichols, Connor, Tasiran and Cam2005; Yassi et al Reference Yassi, Lockhart, Sykes, Buck, Stime and Spiegel2013). During the pandemic context, the presence and intervention of worker representatives has been associated with the implementation of COVID-19 protective measures, either personal (provision of disinfectant gel, gloves, masks, and uniforms) (Dean et al Reference Dean, Venkataramani and Kimmel2020; Moore et al Reference Moore, Ball, Cai, Flynn and Mulkearn2021; Ollé-Espluga et al Reference Ollé-Espluga, Payá Castiblanque, Llorens-Serrano, Esteve-Matalí and Navarro-Giné2024), collective (ventilation systems) (Crowell et al Reference Crowell, Hanson, Boudreau, Robbins and Sokas2021), and organisational, to ensure physical distancing (introducing telework, changing shifts or working days) (Moore et al Reference Moore, Ball, Cai, Flynn and Mulkearn2021; Ollé-Espluga et al Reference Ollé-Espluga, Payá Castiblanque, Llorens-Serrano, Esteve-Matalí and Navarro-Giné2024).
Classic studies on industrial safety and hygiene emphasise that worker representatives play a key role not only in improving preventive management standards but also in reducing health damage from injuries and accidents (Shannon et al Reference Shannon, Mayr and Haines1997). The effectiveness of worker representation systems depends on the level of participation by elected representatives. Workplaces where representatives actively negotiate preventive measures (active participation) achieve greater health damage reduction than those where representatives are merely informed or consulted (passive participation) (Nichols et al Reference Nichols, Walters and Tasiran2007; Payá Castiblanque Reference Payá Castiblanque2020b; Robinson and Smallman Reference Robinson and Smallman2013). Thus, the mere presence of worker representatives does not guarantee improvements in safety and health standards; their active involvement in designing and implementing preventive measures is crucial. However, participation levels are unequal, conditioned by factors such as workplace size, the economic sector of the company or its financial situation (Menéndez et al Reference Menéndez, Benach and Vogel2009; Walters and Wadsworth Reference Walters and Wadsworth2014). The increasing precariousness of employment and deterioration of working conditions in Western economies in recent decades have restricted, if not prevented, access to the protection offered by representatives for a growing number of workers. From a sociodemographic perspective, employment precariousness particularly affects certain groups, such as women, young people, migrants, and those in low-skilled manual jobs (Matilla-Santander et al Reference Matilla-Santander, Martín-Sánchez, González-Marrón, Cartanyà-Hueso, Lidón-Moyano and Martínez-Sánchez2021; van Barneveld et al Reference van Barneveld, Quinlan, Kriesler, Junor, Baum, Chowdhury, (Raja), Clibborn, Flanagan, Wright, Friel, Halevi and Rainnie2020). In terms of business characteristics, companies in the private and primary sectors concentrate the highest indicators of low job quality (Murtin et al Reference Murtin, Arnaud, Le Thi and Parent-Thirion2022).
As with classic studies linking active worker representative participation to reduced accidents and occupational illnesses, the pandemic revealed a similar relationship: workplaces with active participation by worker representatives showed lower COVID-19 positivity rates (Crowell et al Reference Crowell, Hanson, Boudreau, Robbins and Sokas2021) and mortality rates (Dean et al Reference Dean, Venkataramani and Kimmel2020). However, these studies primarily focused on the physical effects (positivity and mortality) of COVID-19, neglecting the potential role that worker representatives may play in mental health, particularly in reducing fear of contracting or transmitting COVID-19. In the present study, this gap is addressed by exploring the relationship between the presence and active participation of worker representatives in the design and implementation of protective measures and workers’ levels of concern about contracting or transmitting COVID-19. Therefore, this research contributes to the literature by expanding the evidence and offering new empirical insights into the relationship between worker representation and psychological concerns during the pandemic. It also broadens the analytical scope by shifting the focus from traditional physical outcomes to psychosocial consequences. Furthermore, it sheds light on inequalities in workers’ access to protective and representative mechanisms across different segments of the labour market.
To do so, the research question guiding this study is: Is active participation by worker representatives in COVID-19 prevention management associated with lower levels of concern about COVID-19 contraction or transmission in the workplace? To address this question, the study examines the relationship between such participation – particularly in the negotiation and implementation of protective measures, whether organisational, collective, or personal – and the level of concern expressed by workers regarding the risk of contagion or transmission in their work environment.
Materials and methods
Study design, data source, and sample
This is a cross-sectional study using microdata from the second wave of the online survey ‘Working Conditions and Health in the Context of COVID-19 in Spain’ (hereafter referred to as COTS2) (Llorens-Serrano et al Reference Llorens-Serrano, Navarro-Giné, Salas-Nicás and Moncada Lluís2021), conducted between April 26 and May 24, 2021. It was distributed among members of Comisiones Obreras (CCOO), Spain’s largest labour union. As of 2023, CCOO represents 1,087,714 members and includes 104,200 elected representatives (35% of the national total) (CCOO 2024).
The target population for the COTS2 survey was workers residing in Spain who were employed when the state of alarm was declared (14 March 2020). For this study, we selected those workers who were salaried employees at the time the survey was administered, including those affected by a reduction-time. The final sample consisted of 19,452 salaried employees, 52.9% of whom were women.
Dependent variables
The two questions related to fear of contracting or transmitting COVID-19 included in the COTS2 questionnaire were:
-
Are you concerned about the possibility of becoming infected with COVID-19 at work?
-
Are you concerned about the possibility of transmitting COVID-19 to someone else?
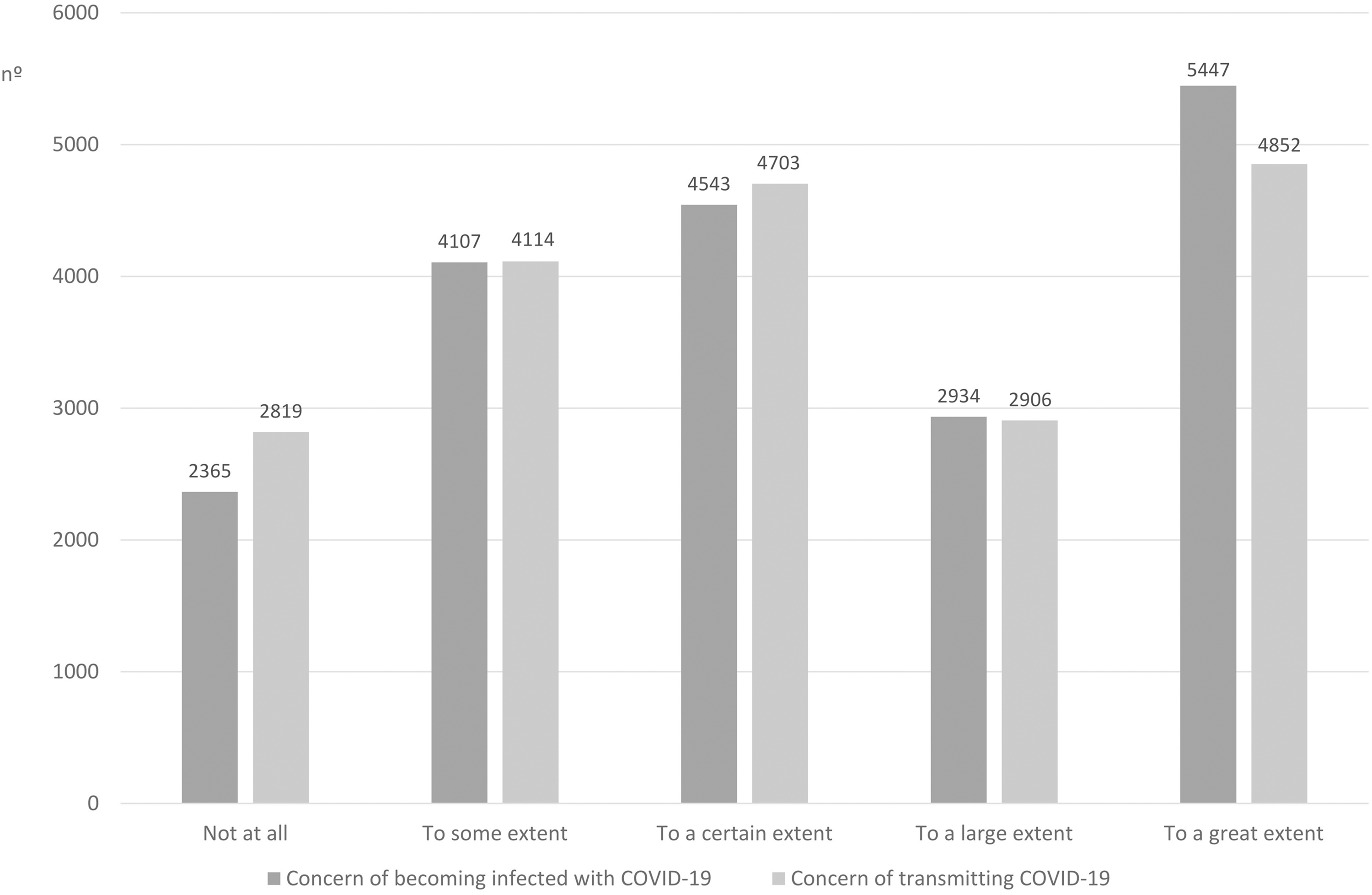
In both cases, a Likert scale with five response options was used, ranging from ‘not at all’ to ‘to a great extent’ (see Figure 1). Responses were dichotomised by considering those workers who answered ‘to a large extent’ or ‘to a great extent’ as concerned.
Levels of concern about contracting or transmitting COVID-19.

Independent variables
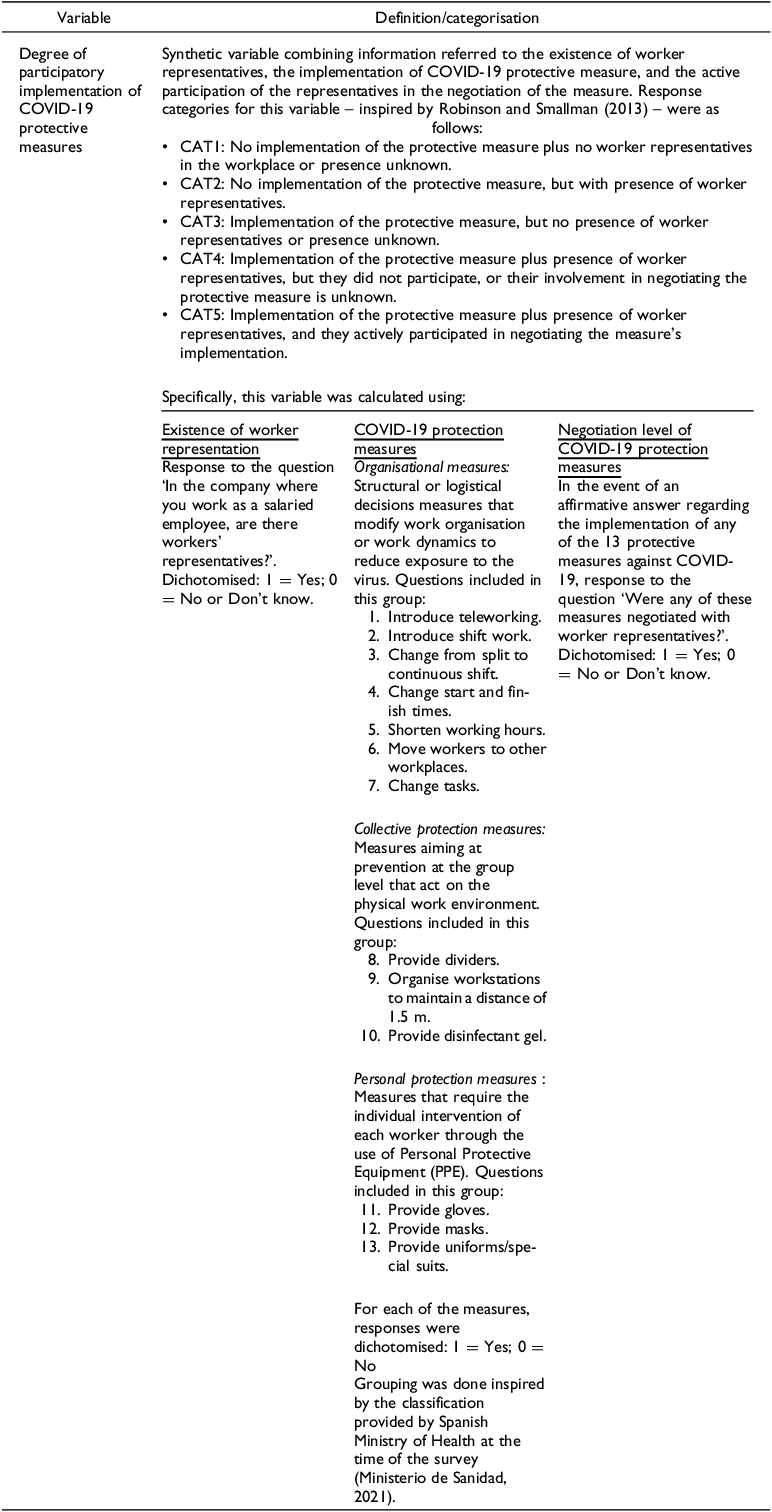
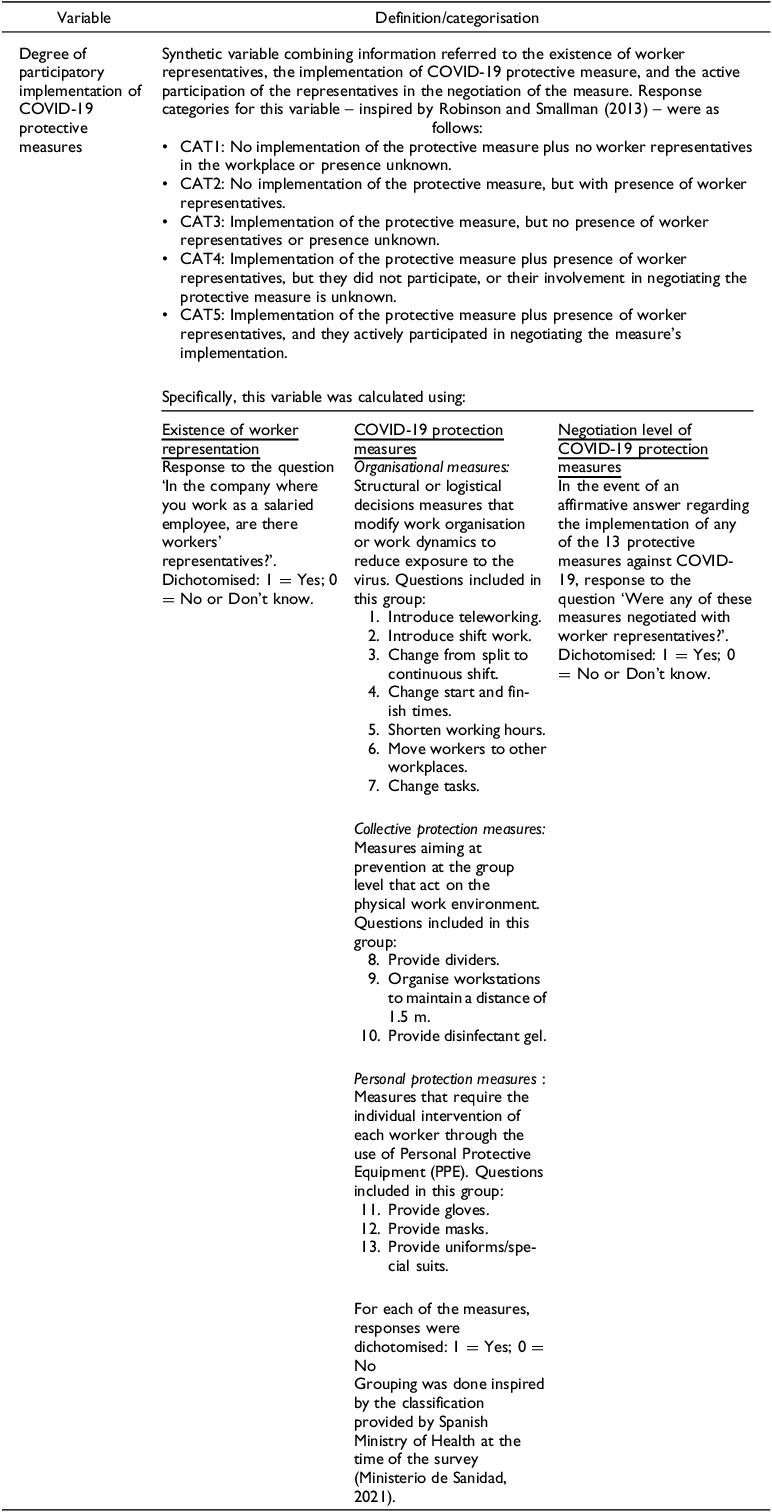
A synthetic indicator on the degree of participatory implementation of COVID-19 protective measures was used as the independent variable (Table 1 summarises this indicator and the variables from which it is derived).
Definition of the independent variable
Sociodemographic and occupational covariates
The following sociodemographic and occupational covariates were selected to adjust the analyses:
-
age (16–34 years, 35–49 years, 50 or older)
-
gender identity (woman, man, non-binary)
-
nationality (Spanish, non-Spanish)
-
occupational social class (manual, non-manual)
-
type of contract (permanent, temporary, no contract)
-
company ownership (public sector, private sector)
-
economic activity, adapted using the codes from the Statistical Classification of Economic Activities in the European Community (NACE Rev. 2). It includes: Primary (Agriculture, livestock, forestry and fishing); Industry; Education; Health activities; Care; Social Work; Construction; Wholesale and retail trade; Transportation and storage; Hospitality (Catering; Hotels and restaurants); Financial, insurance and real estate activities; Administrative and related services; Information and communications; Professional, scientific and technical activities; Sanitation, waste management and remediation activities; Cleaning of buildings and premises; Private security; Others.
Selection of covariates was based on a dual vulnerability criterion: exposure to COVID-19 (Williams Reference Williams2020) and the probability of having worker representatives in the workplace (Matilla-Santander et al Reference Matilla-Santander, Martín-Sánchez, González-Marrón, Cartanyà-Hueso, Lidón-Moyano and Martínez-Sánchez2021; Menéndez et al Reference Menéndez, Benach and Vogel2009; Murtin et al Reference Murtin, Arnaud, Le Thi and Parent-Thirion2022; Ollé-Espluga et al Reference Ollé-Espluga, Payá Castiblanque, Llorens-Serrano, Esteve-Matalí and Navarro-Giné2024; Walters and Wadsworth Reference Walters and Wadsworth2014). In this regard, the literature extensively documents that workers in precarious or atypical employment arrangements, such as the self-employed and digital platform workers, faced high levels of exposure, low levels of protection (including the need to resort to individual self-protection strategies), and limited institutional support. This was also true for those in specific occupational groups, including seafarers and transport workers, highlighting a situation of marked structural vulnerability. (Devereux and Wadsworth Reference Devereux and Wadsworth2022; Qureshi et al Reference Qureshi, Harris, Jegasothy, Seale, Chughtai and Quinlan2024; Ruiz et al Reference Ruiz, Vives, Alvarez, Diaz and Zaupa2022). In addition, young people experienced poorer mental health during COVID-19, largely due to their lower resilience and less effective coping strategies compared with adults (Na et al Reference Na, Yang, Mezo and Liu2022). The persistence of gender inequalities in the distribution of domestic and care work had significant effects on emotional exhaustion (Bartolj et al Reference Bartolj, Murovec and Polanec2022). Of the key determinants of the worker representatives’ presence, size of the company/workplace is the only variable not available in the COTS2 database.
Expected relationships and hypotheses
To empirically capture the relationships identified in the research question, the study distinguishes five analytical categories (CAT1–CAT5). These categories combine the implementation of COVID-19 protective measures with the presence and degree of participation of workers’ representatives, as detailed in Table 1. Based on the literature reviewed in the theoretical framework of this study (Nichols et al Reference Nichols, Walters and Tasiran2007; Payá Castiblanque Reference Payá Castiblanque2020b; Robinson and Smallman Reference Robinson and Smallman2013), a hierarchical ordering of these categories is assumed. Compared to CAT1, workers’ levels of concern are expected to progressively decrease as workplaces move from the non-application or non-participatory implementation of protective measures (CAT2–CAT4) to scenarios characterised by the active participation of workers’ representatives (CAT5). This active participation is expected to enhance the effectiveness of protective measures by increasing their suitability to specific working conditions, boosting confidence in preventive management, and reinforcing workers’ perceptions of control and voice (Eguchi et al Reference Eguchi, Hino, Inoue, Tsuji, Tateishi, Ando, Nagata, Matsuda and Fujino2021; Falco et al Reference Falco, Girardi, Dal Corso, Yıldırım and Converso2021). These factors shape both the objective quality of prevention and workers’ subjective risk perceptions.
Considering the research question and previous literature, this study formulates the following hypotheses: (a) Lower concern about contracting or transmitting COVID-19 is reported among workers in workplaces with protective measures (CAT2–CAT5) than among workers in workplaces without protective measures (CAT1); (b) Protective measures against COVID-19 are more likely to be implemented in workplaces with worker representation (CAT2, CAT4, and CAT5) than in workplaces without representation (CAT1 and CAT3); (c) Workers’ concern about contracting or transmitting COVID-19 is reduced when protective measures are negotiated and implemented with the active participation of worker representatives (CAT5) than when measures are implemented without their active participation (CAT3 and CAT4), reflecting the role of participatory processes in enhancing procedural legitimacy and contextual adaptation; and (d) Access to the most protective settings (particularly CAT5) is uneven across different occupational and sociodemographic groups. Consequently, higher levels of concern are expected to cluster among workers with the greatest infection risk and the least access to participatory forms of worker representation.
Statistical analyses
First, univariate analyses were performed to describe the dependent variables. Then, a bivariate analysis was performed to explore the associations between concern of contracting or transmitting COVID-19 and the sociodemographic and occupational covariates (see Table 2). This bivariate analysis was replicated for the presence or absence of workers’ representatives in the workplaces (see Table 3) and the implementation of the 13 protection measures against COVID-19 (see Table 4). Chi-square test was used to calculate p-values. The type I error was set at α = 0.05.
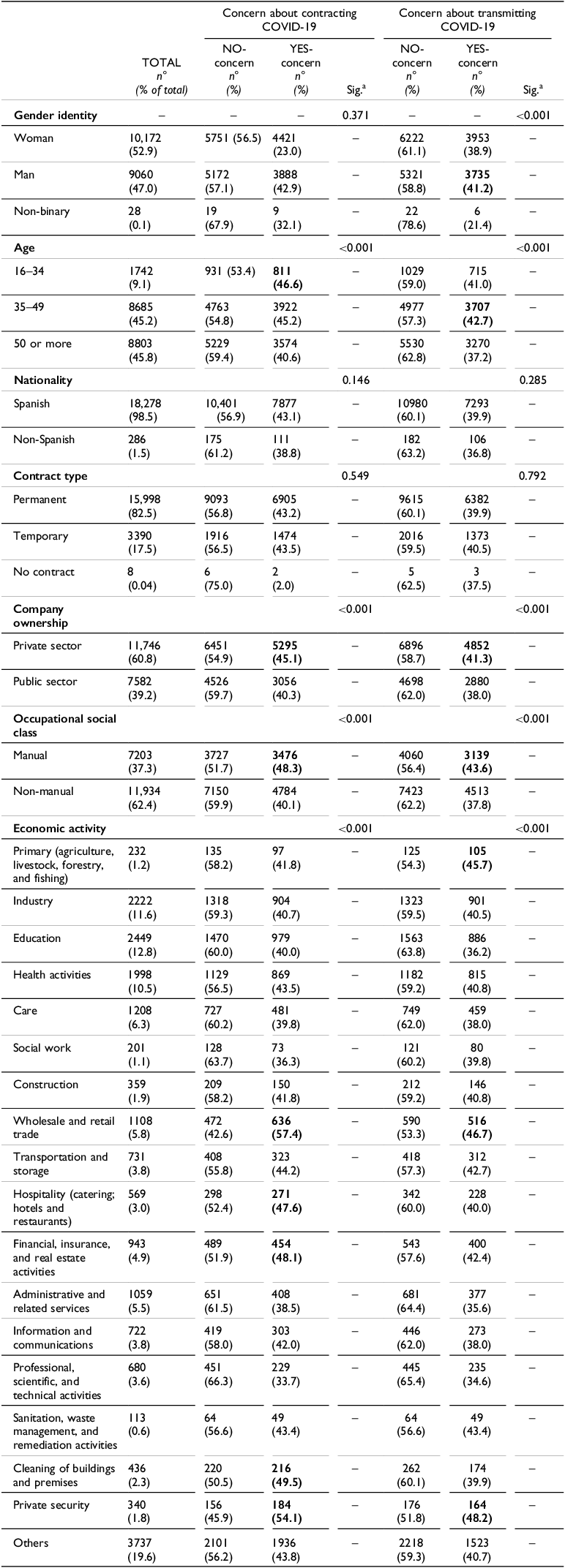
Concern about contracting and transmitting COVID-19 according to sociodemographic and occupational characteristics
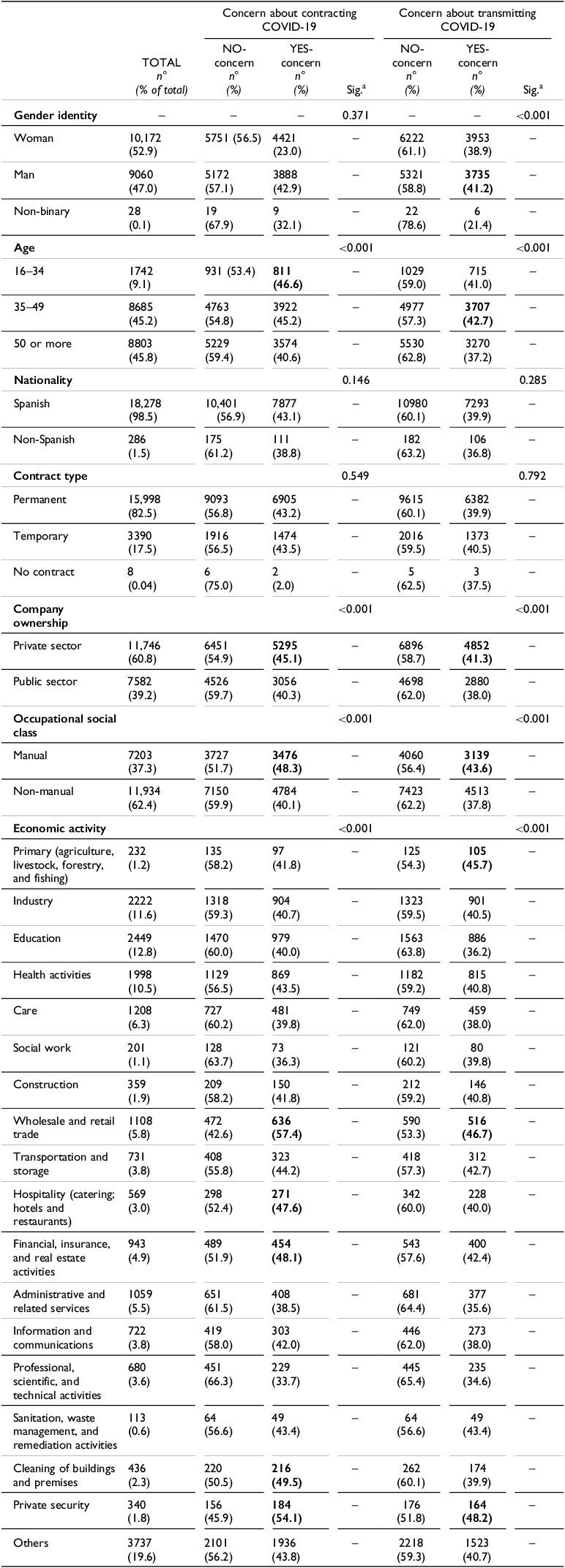
a p-Value determined by chi-square test.
Bold values indicate the highest percentages within each category for concern about contracting and transmitting COVID-19.
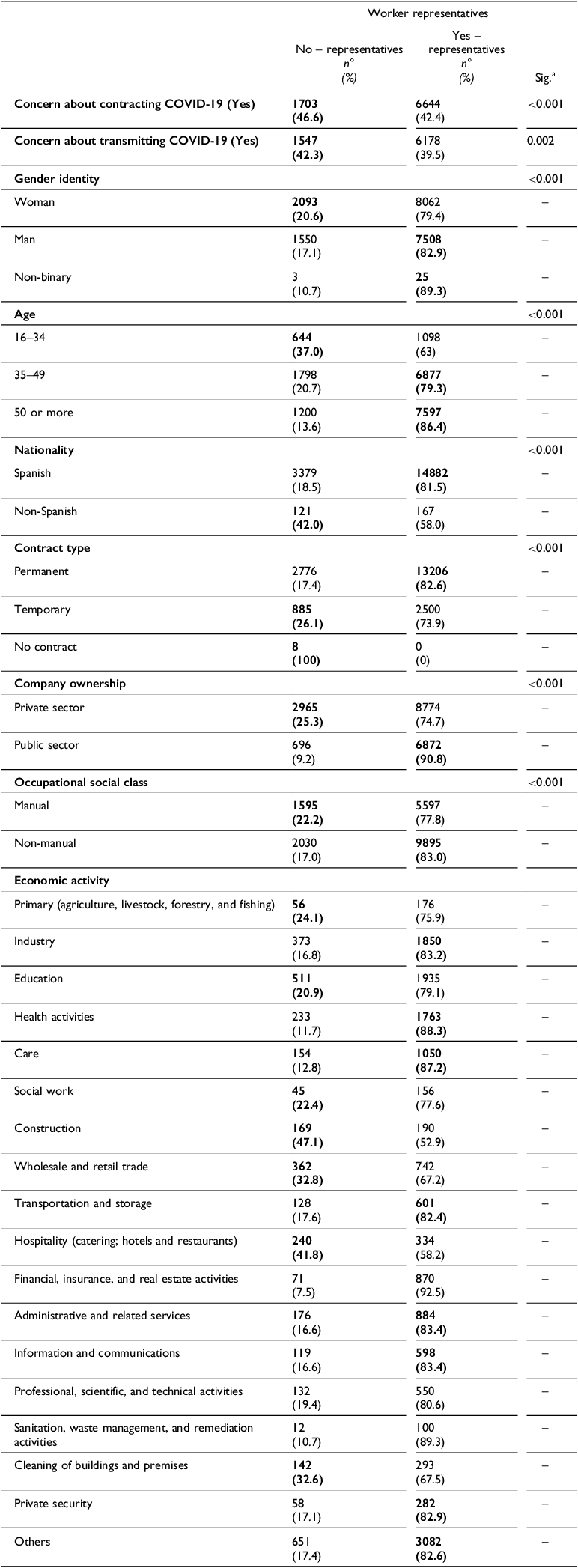
Presence of worker representatives in the workplace according to concern about contracting and transmitting COVID-19 and sociodemographic and occupational characteristics
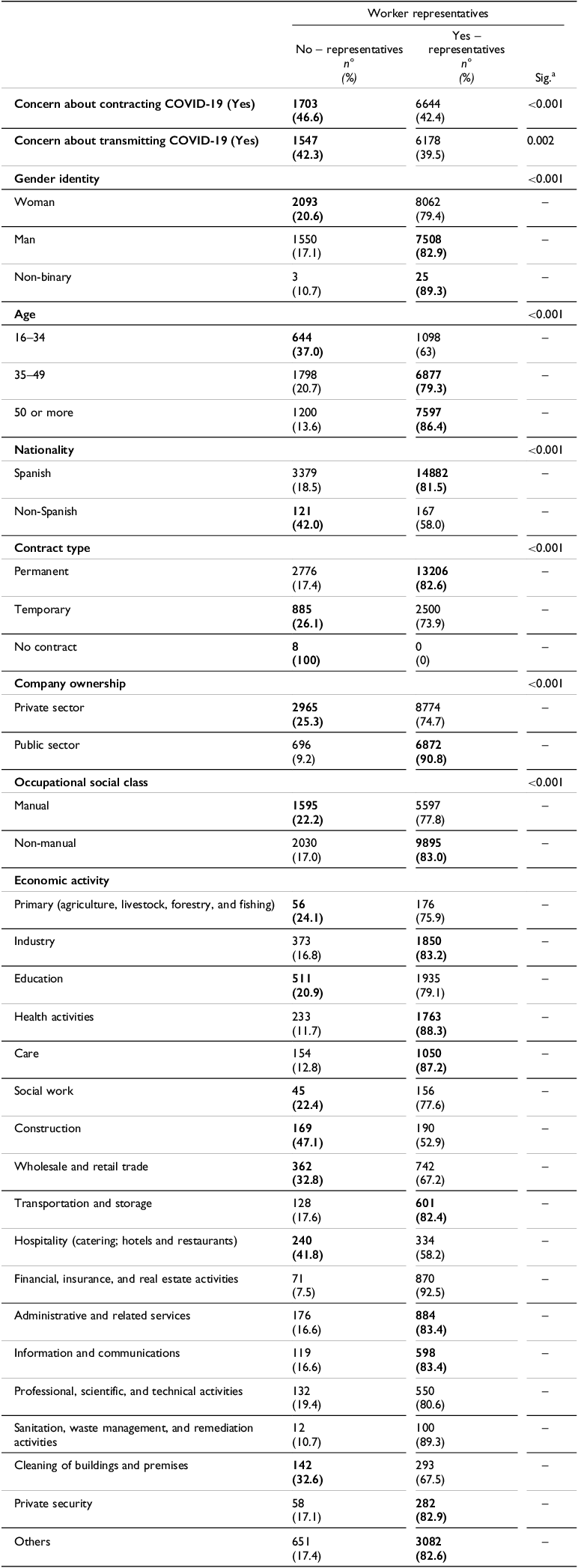
a p-Value determined by chi-square test.
Bold values indicate the highest percentages within each category for concern about contracting and transmitting COVID-19.
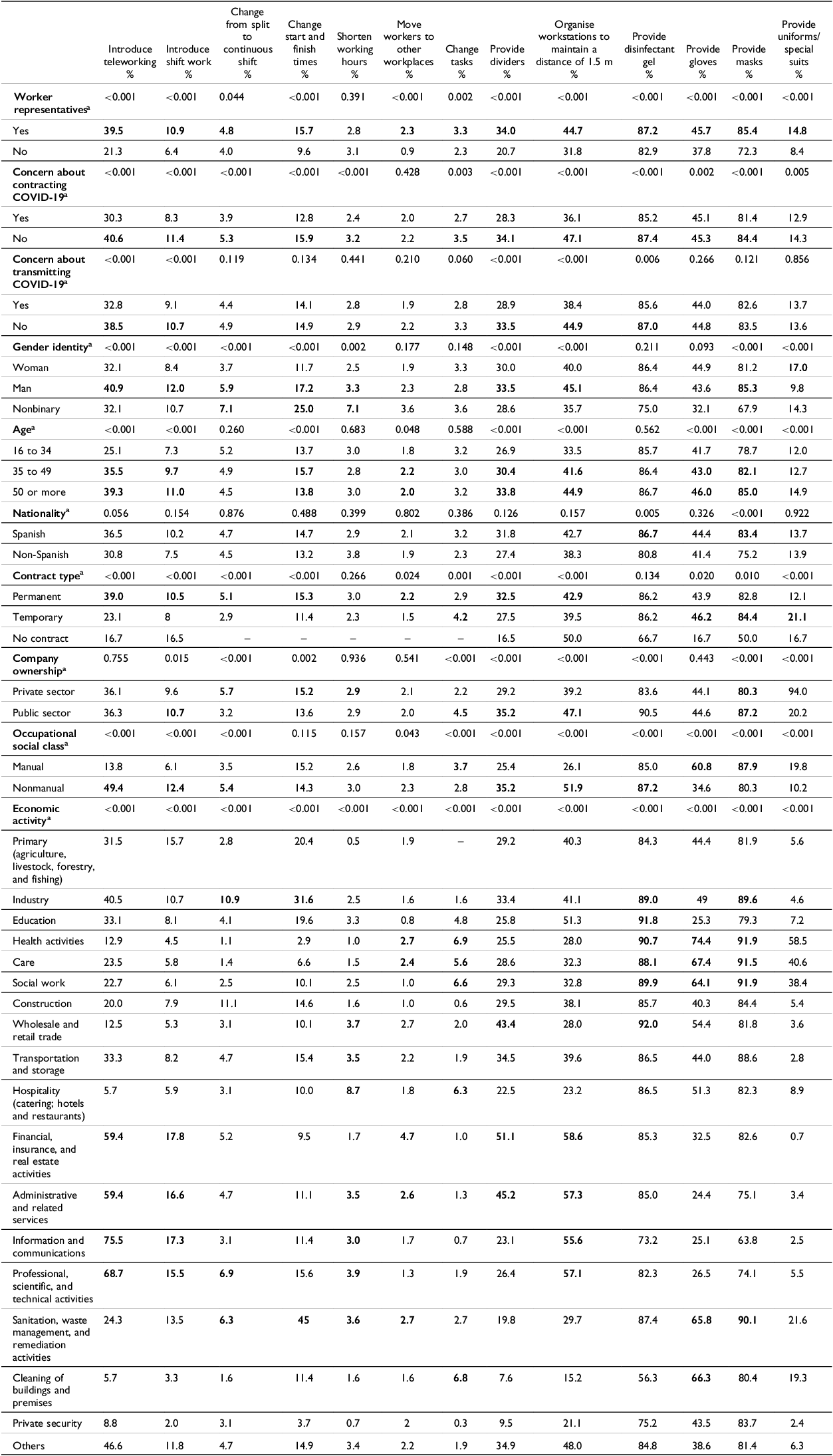
Implementation of protective measures according to the presence of workers’ representatives in the workplace, concern about contracting and transmitting COVID-19, and sociodemographic and occupational characteristics
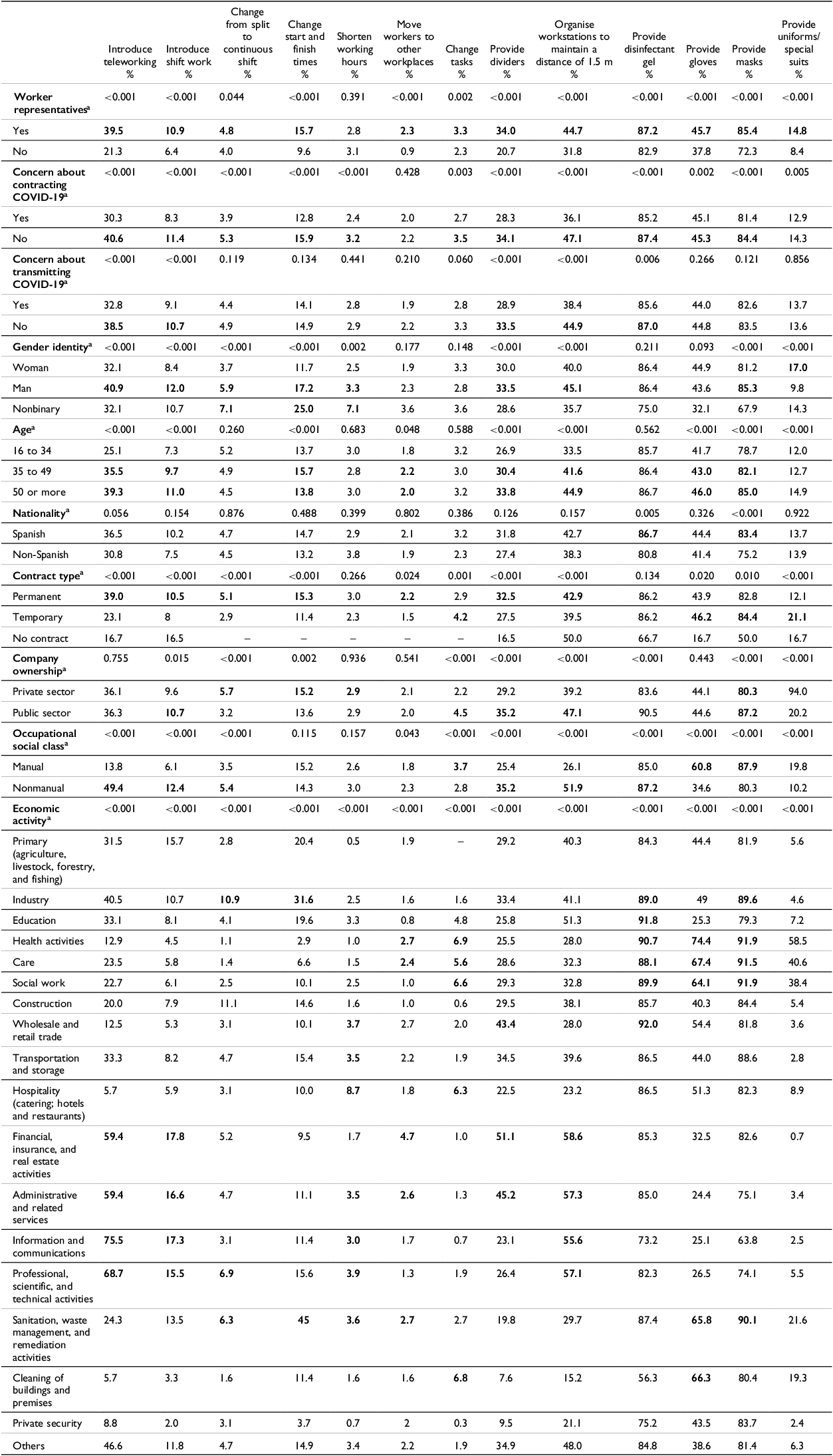
a p-Value determined by chi-square test.
Bold values indicate the highest percentages within each category for concern about contracting and transmitting COVID-19.
Finally, a multivariate analysis (logistic regression modelsFootnote 1 ) was employed to estimate the relationship between the degree of participatory implementation of COVID-19 protective measures and concern of COVID-19 contraction or transmission. Crude odds ratios (cOR) and adjusted odds ratios (aOR) accounting for the covariates were calculated for each dependent variable, with 95% confidence intervals. Absence of concern was established as the reference category for the dependent variables (see Tables 5 and 6). The independent variables were the synthetic indicators constructed for each of the 13 COVID-19 protective measures. We used CAT1 as reference category for these indicators (no implementation of the protective measure plus no worker representatives in the workplace or presence unknown). Participants not answering the question(s) were excluded from the calculation of each indicator. Individual and multivariate logistic regression models were performed using IBM SPSS Statistics software, version 28.
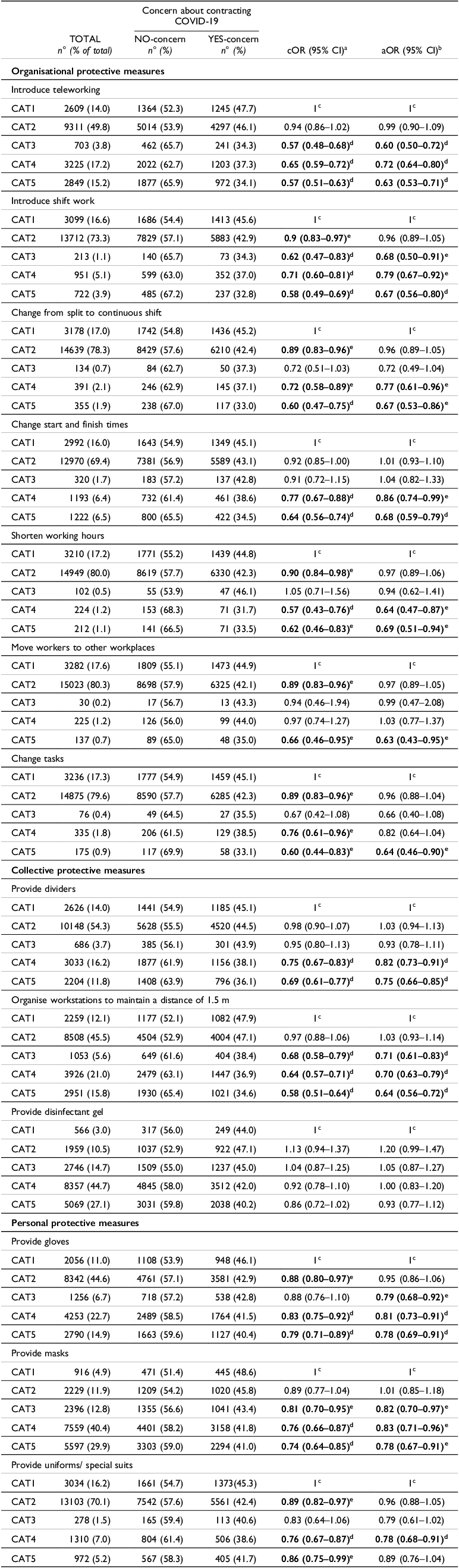
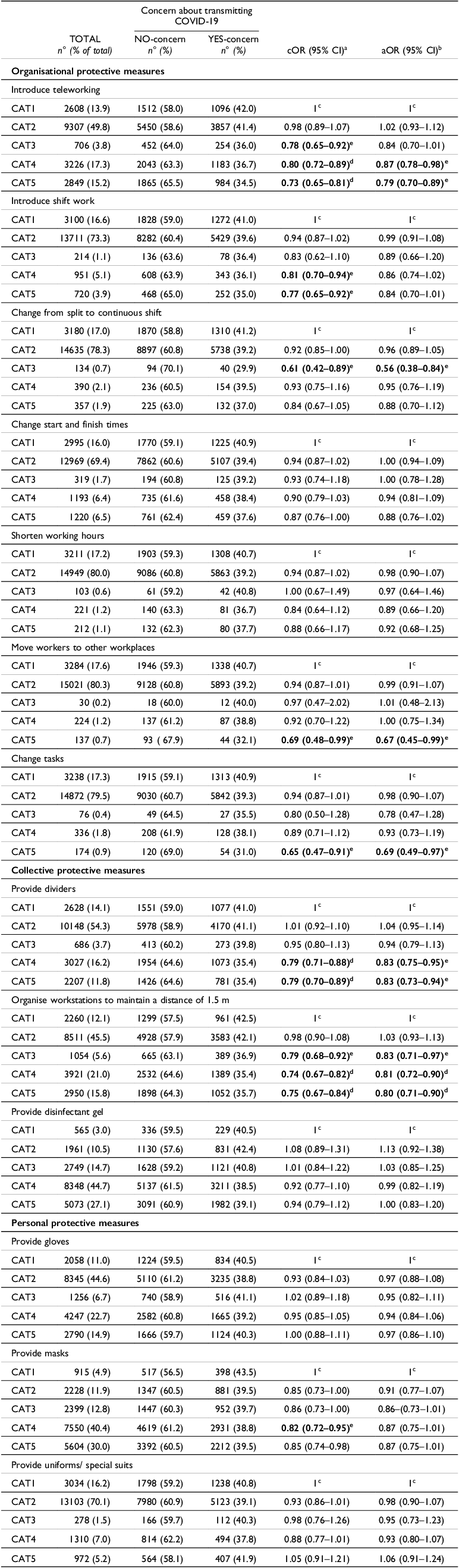
Concern about contracting COVID-19 according to the degree of participatory implementation of protective measures
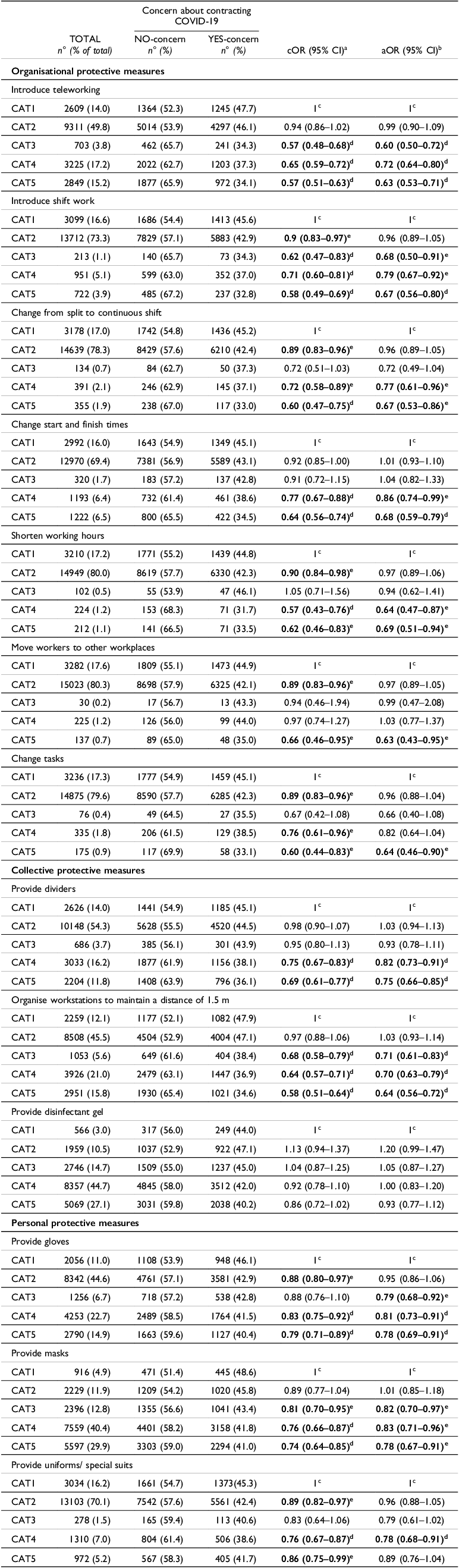
a cOR: crude odds ratio. 95% CI: 95% confidence interval. No concern of contracting COVID-19 was the reference category.
b aOR: adjusted odds ratio by gender identity (reference category: women); age (reference category: 16-34); nationality (Spanish); contract type (permanent); company ownership (private sector); occupational social class (manual); and economic activity (primary).
c For each of the 13 COVID-19 protective measures, an indicator with five differentiated occupational risk prevention categories (hereinafter CAT) was constructed, where CAT1 was the reference category in the regression analysis. Categories are defined as CAT1: No implementation of the protective measure plus no presence of worker representatives in the workplace or presence unknown; CAT2: No implementation of the protective measure, but with presence of worker representatives; CAT3: Implementation of the protective measure, but no presence of worker representatives or presence unknown; CAT4: Implementation of the protective measure plus presence worker representatives, but they did not participate, or their involvement in negotiating the protective measure is unknown; and CAT5: Implementation of the protective measure plus presence of worker representatives, and they actively participated in negotiating the measure’s implementation.
d p < 0.001.
e p < 0.05.
Bold values indicate the highest percentages within each category for concern about contracting and transmitting COVID-19.
Concern about transmitting COVID-19 according to the degree of participatory implementation of protective measures
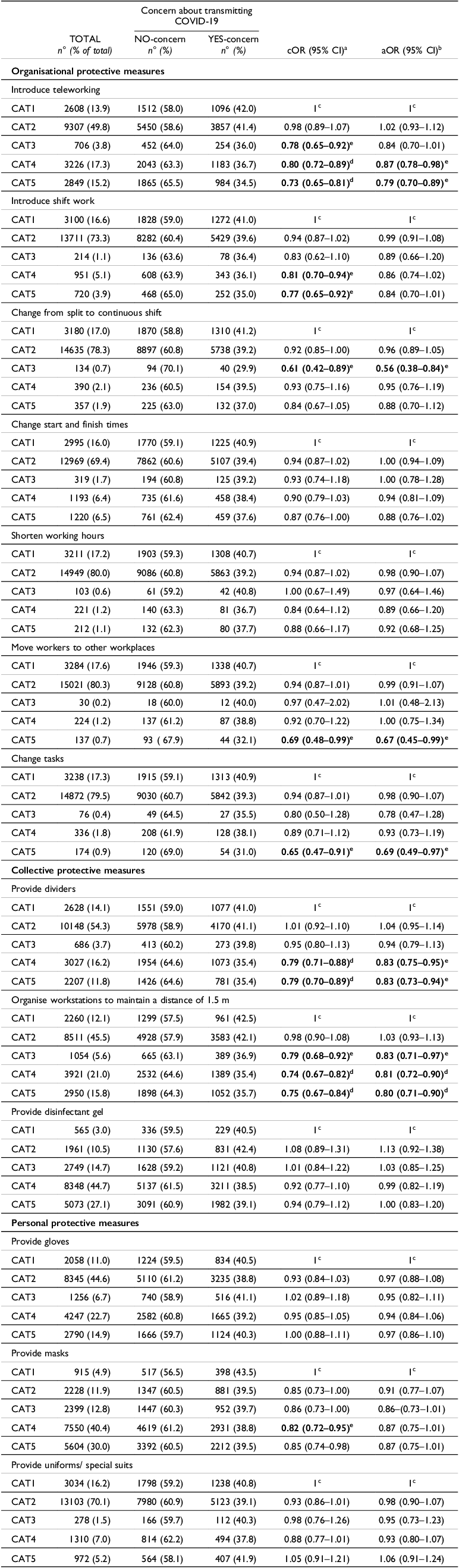
a cOR: crude odds ratio. 95% CI: 95% confidence interval. No concern of transmitting COVID-19 was the reference category.
b aOR: adjusted odds ratio by gender identity (reference category: women); age (reference category: 16-34); nationality (Spanish); contract type (permanent); company ownership (private sector); occupational social class (manual); and economic activity (primary).
c For each of the 13 COVID-19 protective measures, an indicator with five differentiated occupational risk prevention categories (hereinafter CAT) was constructed, where CAT1 was the reference category in the regression analysis. Categories are defined as CAT1: No implementation of the protective measure plus no presence of worker representatives in the workplace or presence unknown; CAT2: No implementation of the protective measure, but with presence of worker representatives; CAT3: Implementation of the protective measure, but no presence of worker representatives or presence unknown; CAT4: Implementation of the protective measure plus presence of worker representatives, but they did not participate, or their involvement in negotiating the protective measure is unknown; and CAT5: Implementation of the protective measure plus presence of worker representatives, and they actively participated in negotiating the measure’s implementation.
d p < 0.001.
e p < 0.05.
Bold values indicate the highest percentages within each category for concern about contracting and transmitting COVID-19.
The study adhered to current legislation and received approval from the Ethics Committee of the university affiliated with the research group conducting the study (CEEAH-5470). All participants provided online informed consent before participating in the study.
Robustness check
To test the robustness of the analyses performed, complementary analyses were carried out. Given the lack of specificity of our dependent variables, the Spanish version of the Mental Health Inventory-5 (MHI-5) was used as an alternative dependent variable somehow related to fear (Vilagut et al Reference Vilagut, Ferrer, Rajmil, Rebollo, Permanyer-Miralda, Quintana, Santed, Valderas, Ribera, Domingo-Salvany and Alonso2005). This is a subscale included within a broader instrument known as SF-36 Health Questionnaire which assesses feelings of nervousness, anxiety, depression, and psychological well-being during the previous month. In analyses not shown, a chi-square test was first performed to examine whether the dependent variables measuring concern about contracting or transmitting COVID-19 were related to mental health. 52.2% of those who reported being concerned about contracting COVID-19 in the workplace were at high risk of poor mental health (MHI-5), compared to 29% of those who did not report such concern. These differences are statistically significant (p < .001). Results were similar for the dependent variables related to concern about transmitting COVID-19. Then, the Mental Health Inventory-5 was used as a dependent variable in a regression analysis (see Table 1 in the Appendix), obtaining homogeneous results that reinforce the validity of the dependent variables used in the present study.
Despite regressions being performed adjusting for sociodemographic and occupational covariates, stratified analyses were also carried out according to occupational social class, type of contract, and a proxy of essential workersFootnote 2 (see Tables 3, 4, and 5 in the Appendix, respectively). This was done to consider the identified double vulnerability factor and reinforce the robustness of the overall results.
Results
Descriptive analysis
Concern about contracting the virus was slightly higher (8381 individuals, 43.2% of the sample) than about transmission (7758 individuals, 40%) (Figure 1). The distribution of concern across different socio-demographic and occupational groups (see Table 2) shows that younger individuals (46.6%), manual workers (48.3%), and those working in private companies (45.1%) report higher levels of concern about contracting COVID-19. This is particularly evident in sectors characterised by high exposure and less protection, such as retail and wholesale trade (57.4%), building cleaning (49.5%), and private security (54.1%). A similarly elevated level of concern about transmitting COVID-19 was observed among manual workers (43.6%) and in sectors such as the primary sector (45.7%), cleaning (39.9%), and hotel and catering (40%). No statistically significant differences were detected according to nationality or type of contract.
The role played by the presence or absence of worker representatives is the focus of Table 3. Compared to workers with representation, those without representatives expressed statistically significantly greater concern about both contracting COVID-19 (46.6% vs. 42.4%) and transmitting it (42.3% vs. 39.5%). The average representation in the sample as a whole is 80.7%, although there are inequalities in access to worker representatives. Groups with less access included young people (63%), those on temporary contracts (74%), immigrants (58%), and individuals employed in sectors such as hospitality (58.2%), wholesale and retail trade (67.2%), and cleaning (67.5%). The groups reporting the most concern about contracting or transmitting the virus are also those with the least union or institutional coverage, as these results illustrate.
Table 4 shows the implementation of protective measures according to the presence of worker representatives in the workplace, concerns about COVID-19 contraction and transmission, and workers’ sociodemographic and occupational characteristics. The presence of representatives is associated with a greater implementation of protective measures. For example, 39.5% of those with representatives could telework, compared to 21.3% of those without; 44.7% experienced reorganisations of workstations to maintain distancing, compared to 31.8%; and 85.4% received face masks, compared to 72.3%. Similarly, concern about contraction was significantly higher among those without access to such measures. Only 30.3% of those concerned about becoming infected could telework, compared to 40.6% of those who were not. Lower rates of distribution of gel, gloves, and masks were observed among concerned workers. Although differences were less pronounced regarding concern about COVID-19 transmission, the pattern holds. Overall, the descriptive results underline a dual axis of vulnerability: certain groups face greater exposure to infection risk due to their employment conditions (e.g. young age, manual occupations, private sector, or high-exposure sectors) while simultaneously having less access to protective resources such as worker representation or effective implementation of protective measures. This dual pattern is consistently linked to greater concern about contracting and transmitting COVID-19.
Regression analysis on concern about contracting COVID-19
The logistic regression analyses in Table 5 generally reveal a positive association between the implementation of COVID-19 protective measures in workplaces and reduced employee concern about contracting the disease. This relationship is observed in 12 out of 13 indicators of the three categories involving application of protective measures (CAT3, CAT4, and CAT5). For instance, compared to those without telework or representatives (CAT1), employees with telework options through negotiations with worker representatives (CAT5) show 1.59 times lower odds of expressing concern about contracting COVID-19: CAT5; aOR = 0.63; 95% CI: 0.53–0.71.Footnote 3 This signals an initial ‘union effect’, as workplaces with worker representatives are more likely to implement COVID-19 protective measures (see Table 2 in the Appendix)
Regarding the type of protective measure implemented, more sophisticated organisational measures are related to 1.56 times lower odds of individuals reporting concern about contracting COVID-19. For example: shorten working hours – CAT4 (aOR = 0.64; 95% CI: 0.47–0.87); move workers to other workplaces – CAT5 (aOR = 0.63; 95% CI: 0.43–0.95); and change tasks – CAT5 (aOR = 0.64; 95% CI: 0.46–0.90). In contrast, personal protective measures show a slightly weaker positive association, corresponding to 1.28 times lower odds: gloves – CAT5 (aOR = 0.78; 95% CI: 0.69–0.91); masks – CAT5 (aOR = 0.78; 95% CI: 0.67–0.91); and uniforms – CAT4 (aOR = 0.78; 95% CI: 0.68–0.91). Despite the greater association with more sophisticated organisational measures, these are rarely implemented, with working hours reduced in only 2.9% of cases and task changes or relocation in 2.1% and 3.1% or cases, respectively (see Table 3; and Table 2 in the Appendix).
A second ‘union effect’ emerges, characterised by a more pronounced reduction in concern about contracting COVID-19 when worker representatives actively negotiated and participated in the implementation of COVID-19 protective measures (CAT5), compared to scenarios with no participation of representatives (CAT4) or with implementation of the protective measures but without worker representation or unawareness of it (CAT3). Notably, the positive association is statistically significant only for the more sophisticated organisational measures when negotiated by worker representatives: moving workers to other workplaces – CAT5 (aOR = 0.63; 95% CI: 0.43–0.95); and changing tasks – CAT5 (aOR = 0.64; 95% CI: 0.46–0.90). However, this ‘union effect’ faced barriers due to the low participation rates of worker representatives (see the ‘YES-Rep Participate’ column of Table 2 in the Appendix).
The robustness of the results obtained is supported by complementary analyses. For example, when replacing the dependent variable with the Mental Health Inventory-5, a consistent association was observed between the participatory implementation of measures and better mental health (see Table 1 in the Appendix). For most of the analysed measures, the CAT5 category was associated with a significant reduction in the risk of poor mental health. In contrast, measures implemented without union participation (CAT3 and CAT4 categories) showed weaker effects. This suggests that measures that reduced concern about contraction also contributed to improved mental health, thus highlighting the beneficial role of worker representation.
Stratification analyses (see Appendix Tables 3, 4, and 5) reinforce this finding. The benefits of participatory measures were significant for both manual and non-manual workers (see Appendix Table 3). For manual employment specifically, the magnitude of the effect was slightly higher for organisational measures such as shift change (CAT5: aOR = 0.68) and task change (CAT5: aOR = 0.64). Therefore, worker representation may mitigate inequalities, as manual workers experience more pronounced reductions in concern when active bargaining occurs (CAT5).
At the same time, limitations to the participation of representatives can be identified in our analyses. For instance, supplementary Table 4 shows that workers with permanent contracts had consistently lower aOR for most CAT5 measures (11 out of 13) of becoming infected with SARS-CoV-2, contrasting with temporary workers (4 out of 13). This suggests implementation barriers in groups with lower representation as already illustrated in Tables 3, 4 of the descriptive analyses. A similar picture appears when analysing the association between concern and measures according to our proxy of essential jobs (assessed by the level of worker representation and sectoral concern about transmission in Appendix Table 5). Sectors with high worker representation and low concern (industry; administrative and related services; information and communications; professional, scientific and technical activities) showed the most consistent and significant protective effects. In this group, negotiated telework (CAT5) was associated with an aOR of 0.57 and change of tasks with an aOR of 0.53. In contrast, in sectors with low representation and high concern (wholesale and retail trade; hotels and catering; cleaning of buildings and premises), associations were weak or not significant, confirming the limitations of the union effect in precarious, poorly institutionalised and under-represented contexts.
Regression analysis on concern about transmitting COVID-19
Compared to concern about contracting COVID-19, the results show a lower frequency of statistically significant association between implementation of COVID-19 protective measures and reduced concern about transmitting the disease (Table 6). Only 6 of the 13 indicators show this relationship, involving the implementation of four organisational measures (introduce teleworking, change from split to continuous shift, move workers to other workplaces, and change tasks) and two collective measures (provide dividers and organise workstations to maintain a 1.5-metre distance). As with concern about contracting COVID-19, negotiating more sophisticated organisational measures with worker representatives is more strongly associated with reduced concern of transmitting it: move workers to other workplaces – CAT5 (aOR = 0.67; 95% CI: 0.45–0.99); and change tasks – CAT5 (aOR = 0.69; 95% CI: 0.49–0.97).
Discussion and conclusions
This research examined the relationship between worker representatives’ active participation in the negotiation and implementation of COVID-19 protective measures and worker concerns about contracting or transmitting the disease as a proxy of fear. From a multivariate analysis on a sample of wage earners affiliated to CCOO, two distinct ‘effects’ linked to union representation were identified. First, the results generally support that active participation of workers’ representatives in the negotiation of COVID-19 protective measures (in the present analysis, CAT5) is associated with less concern about contraction or transmission. It is true that the mere existence of COVID-19 protective measures, even without the active involvement of worker representatives in their implementation, also reduces concern about becoming infected (CAT4) compared to their absence (CAT1). However, this reduction is less pronounced when workers’ representatives are not involved in the negotiation and implementation of these measures, consistent with the analyses of Robinson and Smallman (Reference Robinson and Smallman2013). Thus, the results obtained confirm and support the initial hypotheses of the present study.
Second, workplaces with worker representation (CAT4) tend to implement more protective measures than those without (CAT3). This aligns with both classic studies on occupational health (Coutrot Reference Coutrot2009; Jirjahn et al Reference Jirjahn, Mohrenweiser and Smith2022; Ollé-Espluga et al Reference Ollé-Espluga, Vergara-Duarte, Belvis, Menéndez-Fuster, Jódar and Benach2015) and specific research focused on the pandemic context (Crowell et al Reference Crowell, Hanson, Boudreau, Robbins and Sokas2021; Dean et al Reference Dean, Venkataramani and Kimmel2020; Moore et al Reference Moore, Ball, Cai, Flynn and Mulkearn2021;Ollé-Espluga et al Reference Ollé-Espluga, Payá Castiblanque, Llorens-Serrano, Esteve-Matalí and Navarro-Giné2024). Existing research relates the implementation of COVID-19 protective measures to reduced psychological distress (Asaoka et al Reference Asaoka, Sasaki, Imamura, Kuroda, Tsuno and Kawakami2022; Chaudhry et al Reference Chaudhry, Rasool, Raza, Mhelska and Ur Rehman2023). This study adds to literature about worker representation by highlighting that representatives not only enhance the implementation of such measures but also potentially act as a protective factor for mental health. Thus, the combination of safety measures plus the involvement of worker representatives in decision-making may mitigate the relationship between perceived risk of infection in the workplace and mental health outcomes (Eguchi et al Reference Eguchi, Hino, Inoue, Tsuji, Tateishi, Ando, Nagata, Matsuda and Fujino2021; Falco et al Reference Falco, Girardi, Dal Corso, Yıldırım and Converso2021). By providing reliable information, facilitating access to negotiated preventive measures, and fostering safer work environments, representatives can help reduce uncertainty and, consequently, psychological distress (Eguchi et al Reference Eguchi, Hino, Inoue, Tsuji, Tateishi, Ando, Nagata, Matsuda and Fujino2021; Falco et al Reference Falco, Girardi, Dal Corso, Yıldırım and Converso2021). Furthermore, being concerned about contracting or transmitting the virus is associated with poorer mental health. When mental health is used as an alternative dependent variable (see Table 1 in the Appendix), the results obtained are comparable to those found when concern is the main variable. This reinforces the underlying relationships between the presence of worker representatives, their negotiated participation, and the mitigation of both anticipatory worry and the risk of poor mental health.
Consistent with Chaudhry et al (Reference Chaudhry, Rasool, Raza, Mhelska and Ur Rehman2023), in the present study stronger associations with reduced concern about contracting COVID-19 are found when implementing more sophisticated organisational measures than the provision of personal protective equipment. This could be explained by the fact that organisational measures ensure physical distancing while the effectiveness of personal protective measures depends on individual compliance (Chaudhry et al Reference Chaudhry, Rasool, Raza, Mhelska and Ur Rehman2023). In contrast, Asaoka et al (Reference Asaoka, Sasaki, Imamura, Kuroda, Tsuno and Kawakami2022) found that individual prevention measures (such as hydroalcoholic gel, gloves, and masks) provided the greatest psychological protection. In our study, only the stratified analysis by occupation type (see Appendix Table 3) showed that the use of PPE was associated with reduced concern about COVID-19 contraction among manual workers, but not among non-manual workers. As COVID-19 protective measures were mandatory when determined by a risk assessment (Ministerio de Sanidad 2021), it is likely that risk assessments for manual jobs mainly recommended the use of personal protective equipment (PPE), whereas those for non-manual jobs tended to recommend organisational measures, such as teleworking or task restructuring. This remains a subject for future study.
Despite the positive implications of worker representation, several barriers limiting its scope have been identified. The low level of participation of worker representatives in the negotiation of protective measures (see Table 2 in the Appendix) reinforces the argument of Boix et al (Reference Boix, Vogel, Ruiz-Frutos, Delclòs and Ronda2013) that labour representation should not be viewed solely as a technical or functional mechanism. Rather, it is an asymmetrical power relationship between capital and labour within the framework of industrial democracy. In the Spanish case, the unions’ limited structural market power – closely linked to employment precariousness – restricts representatives’ lobbying and bargaining power. Our results also confirm a pattern of double vulnerability in terms of contracting and transmitting COVID-19 (see Tables 2– 4). While certain groups of workers (i.e. young people, manual workers, employees in the private sector, and in sectors such as commerce, cleaning, or private security) show significantly higher levels of concern about contracting COVD-19, this does not translate into greater organisational protection. This dynamic reproduces what Williams (Reference Williams2020) called the ‘coronavirus class divide’, in which workers with less structural power face higher risks of exposure. Concurrently, access to both worker representation and preventive measures is not homogeneous in our results, as previously pointed out in Menéndez et al (Reference Menéndez, Benach and Vogel2009) and Walters and Wadsworth (Reference Walters and Wadsworth2014). Once again, groups such as young people, migrants, those with temporary contracts, and those working in sectors such as cleaning and hospitality are less likely to have worker representation and effective protection measures. This finding indicates a process of cumulative exclusion, where greater exposure to risk is combined with weak institutional protection, thus reproducing structural logics of inequality (Devereux and Wadsworth Reference Devereux and Wadsworth2022; Qureshi et al Reference Qureshi, Harris, Jegasothy, Seale, Chughtai and Quinlan2024; Ruiz et al Reference Ruiz, Vives, Alvarez, Diaz and Zaupa2022). Indeed, stratified regression analyses confirm that negotiated representative participation (category CAT5) shows no or very weak statistically significant associations among temporary workers or workers in sectors with low representation and high contagion concerns (see Tables 4 and 5 in the Appendix). This result stresses the structural limitations of union action in contexts of precariousness and the low institutionalisation of labour representation.
Additionally, the negotiated implementation of protective measures was less effective in reducing concerns about COVID-19 transmission than contraction, which might reflect factors that go beyond the workplace, such as personal circumstances or family vulnerability (Chowdhury et al Reference Chowdhury, Kainth, Godlu, Farinas, Sikdar and Turin2022). Further research is needed on those factors limiting the scope and effectiveness of worker representatives in this area. For example, delving into those factors facilitating the most favourable and less frequent scenarios for workers, such as active participation of worker representatives in the negotiation and implementation of organisational measures.
Policy and practice recommendations
The following recommendations can be derived from the results of the study. Firstly, regulatory and organisational mechanisms should be established to guarantee the presence of workers’ representatives in workplaces, particularly in sectors with high-risk exposure and low union coverage, such as cleaning, hospitality, retail, and private security. To this end, incentives could be offered to encourage the constitution of representative bodies in small companies, and reforms could be introduced to facilitate union action in fragmented or precarious work environments by implementing territorial safety representatives (Payá Castiblanque Reference Payá Castiblanque2020a). Secondly, the active role of representatives in planning, designing, and implementing prevention measures must be strengthened, moving beyond an approach limited to mere consultation or information. Regulatory frameworks could be established that require the negotiation and co-management of preventive protocols with representatives on health and safety committees. The third proposal is to include workers’ representation in the planning of health emergencies to systematically integrate representative participation as a key player in the development of contingency plans, risk assessment, and the implementation of occupational health measures. Fourthly, given the dual pattern of vulnerability identified in the study, occupational health and safety policies should pay particular attention to young people, migrants, temporary contract workers, and manual labourers. Measures could include specific preventive audits in underrepresented sectors, union and labour rights training campaigns targeting underrepresented groups, and the inclusion of equity clauses in collective bargaining agreements to ensure effective access to protection. A final recommendation is aimed at labour authorities to develop specific indicators to evaluate not only the formal existence of worker representation, but also the degree of effective participation in occupational health decision-making processes.
Limitations
The study, based on a cross-sectional survey among members of the CCOO union, has its limitations. In addition to the cross-sectional design of the research, the sample used may overestimate the presence of workers’ representatives in workplaces. 80.7% of respondents reported having such representation, compared to around 50% in Spain as a whole (Jódar et al Reference Jódar, Alós, Beneyto and Vidal2018). The use of a non-representative sample could constitute a serious limitation if our objective were to estimate population parameters. In the present study, however, the focus lies on examining the association between the degree of implementation of protective measures and workers’ concern about COVID-19 contraction and transmission. In such cases, sample representativeness is not a prerequisite (Rothman et al Reference Rothman, Gallacher and Hatch2013), as valid inferences about associations between exposure and outcome can still be drawn, provided that potential confounders are adequately controlled. To this end, our analysis incorporated covariates identified in the existing literature, and a multivariate analysis technique was employed to control for confounding factors. The only variable included in the regression analysis was the firm/work centre size, as this information was not included in the survey. Nonetheless, the exclusion of this variable might not have a substantial impact, given its interrelation with both the presence of worker representatives and the implementation of preventive measures. Indeed, as observed in a previous study conducted in Spain, the presence of worker representatives may reflect the effect of organisational size (Ollé-Espluga et al Reference Ollé-Espluga, Vergara-Duarte, Belvis, Menéndez-Fuster, Jódar and Benach2015). Moreover, additional stratified analyses by occupation type, contract type, and a proxy for the essential nature of work have allowed us to test the robustness of the analyses from the perspective of potential biases by further restricting the study populations.
The dependent variables used in this study to capture concern about COVID-19 contraction and transmission were created ad hoc for the COTS2 questionnaire and did not directly contain the word ‘fear’ in their wording, as in other published studies (Ahorsu et al Reference Ahorsu, Lin, Imani, Saffari, Griffiths and Pakpour2022; Mertens et al Reference Mertens, Gerritsen, Duijndam, Salemink and Engelhard2020) that use ‘worry’ as a proxy for fear. To overcome this limitation, a complementary analysis was undertaken with another dependent variable included in the survey indirectly reporting on fear and unrest, the Mental Health Inventory-5 (Vilagut et al Reference Vilagut, Ferrer, Rajmil, Rebollo, Permanyer-Miralda, Quintana, Santed, Valderas, Ribera, Domingo-Salvany and Alonso2005). The results with this additional variable were in line with those referred to concern.
Conclusions
This paper offers a significant contribution to the literature on occupational health and worker representation. It presents novel empirical evidence on the association between worker representatives’ active involvement in negotiating COVID-19 protective measures and lower levels about concern of contraction and transmission. This emotional dimension – closely linked to mental health – has been largely overlooked in prior research on workplace representation. Thus, the findings broaden classic occupational safety literature by showing that the protective role of worker representation extends beyond physical harm reduction to include psychosocial risks, especially in times of public health crisis. In doing so, the study underscores the structural importance of worker voice in industrial democracy. The findings also reveal inequalities in access to protection. Precarious workers – those on temporary contracts, in low-skilled manual jobs, or in poorly unionised sectors – are both more concerned about becoming infected and less likely to benefit from protective measures negotiated by representatives. This dual pattern of vulnerability calls for targeted policy responses.
Future research could explore how worker representation shapes fear and perceived safety over time using longitudinal designs. Qualitative and comparative studies may also offer deeper insights into the mechanisms of representative participation across different institutional and sectoral settings. Ensuring not just the presence but the active participation of worker representatives is essential to safeguarding both physical and mental well-being in present and future workplace crises.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/elr.2026.10069.
Funding Statement
The authors received no financial support for the research, authorship, and/or publication of this article.
Competing interests
None.




 Open access
Open access